A novel presentation of HechtBeals trismus
5
A novel presentation of HechtBeals trismus pseudocamptodactyly syndrome: Review of literature and holistic management Partha Chattopadhyay, Cyriac Abby Philips, Debargha Dhua, Prabir Kumar Josh, Prasanta Mukhopadhyay ABSTRACT Introduction: HechtBeals Trismus Psuedocamptodactyly syndrome, a rare autosomal dominant inherited disease encompass a variety of genotypic and phenotypic verges that affects members of a family. Case Report: Here we report a patient, who presented with congenital coal black hyperpigmentation of the skin with progressive trismus. Conclusion: With emergence of new reports, the mutational and expressive variations of this disease is becoming more enigmatic. Our tidings shed light on a novel clinical association with coal black skin pigmentation in whom trismus was dealt successfully through operative methods. Further mutational analysis and clinical probing would help in concreting a definite categorization of this diseases that lie between these gamuts. Keywords: Trismus, Masseter Spasm, Hypermelanosis ***** Chattopadhyay P, Philips CA, Dhua D, Josh PK, Mukhopadhyay P. A novel presentation of HechtBeals trismus pseudocamptodactyly syndrome: Review of literature and holistic management. International Journal of Case Reports and Images 2012;3(3):1923. ********* doi:10.5348/ijcri201203101CR6 INTRODUCTION Trismus is a condition in which there is inability to normally open the mouth due to varied reasons, commonly tetanus, sub mucosal fibrosis, condylar fracture, temporomandibular joint dysfunction, neuroleptic syndromes, peritonsillar abscess and ankylosis of temporomandibular joint. Trismus can also be part of a rare syndrome complex known as the TrismusPsuedoCamptodactyly Syndrome [1]. Here we present a patient who presented to us with Trismus PsuedoCamptodactyly Syndrome, in whom congenital progressive diffuse coal black hyperpigmentation was a striking feature, with mild affection of his elder brother (coal black pigmentation to a lesser degree with mild trismus). Corrective surgical procedure of the trismus and microstomia resulted in betterment and quality of life of our patient without any recurrence even after nine months. CASE REPORT A 17yearold male, presented to us with progressive difficulty in opening the mouth for two years, associated with bony deformities of skull and extremities and www.ijcasereportsandimages.com
Transcript of A novel presentation of HechtBeals trismus

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 3, March 201 2. ISSN – [0976-31 98]
A novel presentation of HechtBeals trismuspseudocamptodactyly syndrome: Review of literatureand holistic managementPartha Chattopadhyay, Cyriac Abby Philips, Debargha Dhua,Prabir Kumar Josh, Prasanta Mukhopadhyay
ABSTRACTIntroduction: HechtBeals TrismusPsuedocamptodactyly syndrome, a rareautosomal dominant inherited diseaseencompass a variety of genotypic andphenotypic verges that affects members of afamily. Case Report: Here we report a patient,who presented with congenital coal blackhyperpigmentation of the skin with progressivetrismus. Conclusion: With emergence of newreports, the mutational and expressivevariations of this disease is becoming moreenigmatic. Our tidings shed light on a novelclinical association with coal black skinpigmentation in whom trismus was dealtsuccessfully through operative methods.Further mutational analysis and clinical probingwould help in concreting a definitecategorization of this diseases that lie betweenthese gamuts.
Keywords: Trismus, Masseter Spasm,Hypermelanosis*****
Chattopadhyay P, Philips CA, Dhua D, Josh PK,Mukhopadhyay P. A novel presentation of HechtBealstrismus pseudocamptodactyly syndrome: Review ofliterature and holistic management. InternationalJournal of Case Reports and Images 2012;3(3):1923.*********
doi:10.5348/ijcri201203101CR6
INTRODUCTIONTrismus is a condition in which there is inability tonormally open the mouth due to varied reasons,commonly tetanus, sub mucosal fibrosis, condylarfracture, temporomandibular joint dysfunction,neuroleptic syndromes, peritonsillar abscess andankylosis of temporomandibular joint. Trismus can alsobe part of a rare syndrome complex known as theTrismusPsuedoCamptodactyly Syndrome [1]. Here wepresent a patient who presented to us with TrismusPsuedoCamptodactyly Syndrome, in whom congenitalprogressive diffuse coal black hyperpigmentation was astriking feature, with mild affection of his elder brother(coal black pigmentation to a lesser degree with mildtrismus). Corrective surgical procedure of the trismusand microstomia resulted in betterment and quality oflife of our patient without any recurrence even afternine months.
CASE REPORTA 17yearold male, presented to us with progressivedifficulty in opening the mouth for two years, associatedwith bony deformities of skull and extremities and
CASE REPORT OPEN ACCESS
Partha Chattopadhyay1 , Cyriac Abby Phil ips2, DebarghaDhua2, Prabir Kumar Josh3, Prasanta Mukhopadhyay4
Affi l iations: 1Professor, General Medicine, College ofMedicine & Sagar Dutta Hospital, Kamarhati, Kolkata-58,West Bengal - 70001 4, India; 2Junior Resident, GeneralMedicine, Nilratan Sircar Medical College and Hospital,Kolkata, West Bengal - 70001 4, India; 3AssociateProfessor, Plastic Surgery, Calcutta National MedicalCollege & Hospital, Kolkata West Bengal - 70001 4, India;4Professor, General Medicine, Nilratan Sircar MedicalCollege and Hospital, Kolkata, West Bengal - 70001 4,India.Corresponding Author: Dr. Partha Chattopadhyay, WestJagtala - Batamore, P.O - Maheshtala South 24-Parganas,Kolkata - 7001 41 ; West Bengal, India; Ph: +91 -33-249031 76, Mob: 09830391 922; Fax: +91 -33-23587282; Email :drpartha73@gmail .com
Received: 1 2 August 2011Accepted: 1 3 February 201 2Published: 31 March 201 2
IJCRI 201 2;3(3):1 9-23.www.ijcasereportsandimages.com Chattopadhyay et al. 1 9

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 3, March 201 2. ISSN – [0976-31 98]
Chattopadhyay et al. 20
progressive hyperpigmentation of the skin since birth.There was no relevant history of infections in childhood,drug intake by the mother of the patient duringpregnancy, drug intake in the patient, trauma, surgeriesor similar complaints in the family members. Onexamination, the patient was found to have features ofmacrocephaly, micrognathia with microstomia,arachnodactyly, trismus, pseudocamptodactyly (flexioncontractures of the distal joints of the hands oncomplete dorsiflexion), a broad stout neck, with low setears, scoliosis and diffuse melanotic hyperpigmentationof the whole body, including palms and soles, withlinear melanonychia, without any pigmentary changesof the orogenital mucosal surfaces (figures 1A, B).Systemic examination revealed no abnormalities, exceptfor an irregularly irregular pulse rate. A completehemogram, liver function test, renal function testincluding serum electrolytes along with thyroid functiontesting fasting blood glucose levels and a routine urineanalysis were well within normal limits.Roentgenograms of the skull showed features of diploicspace expansion along with premature sinuses withfrontal and occipital bossing and that of the peripheralbones and the knee joints revealed cortical wideningwith delayed fusion of the epiphyses. An oralpantomogram revealed features suggestive of aprobable mandibular condylar dysplasia, as interpretedby our consultant radiologist (figure 2). Theelectrocardiogram revealed features suggestive ofventricular premature beats. A Computed Tomographyof the abdomen and a Magnetic Resonance Imaging ofthe Brain revealed no significant abnormalities. AnEchocardiogram performed was within normal limits.Based on the specific clinical findings, a diagnosis ofArthrogryposis, distal type 7, also known as HechtBeal’s Trismus Pseudocamptodactyly Syndrome wasmade.The patient had painless restriction of mouthopening beyond 20 mm. A Computerized Tomography
of the skull bones revealed normal condyles and thetemporomandibular joints on either side with bilateralmandibular coronoid hyperplasia (figure 3). Theseenlarged coronoids was impinging on the posterioraspect of the zygoma causing trismus and hence abilateral coronoidectomy procedure was planned.The patient was successfully intubated using an adultfibreoptic bronchoscope under intravenous anesthesia.Difficulty in intubation was anticipated and equipmentpertaining to emergency jet ventilator and tracheostomywas kept ready. The intraoperative interincisor(distance between the upper and lower incisors) mouthopening was found to be 35 mm. The access wasthrough a preauricular incision. The hyperplasticcondyles and the normal temporomandibular joint,was exposed and a coronoidectomy, performed oneither side. After proper haemostasis, the operative sitewas closed with drains in place. The postoperativeperiod was uneventful. An intraoral device (figure 4)was used in the immediate postoperative period in orderto maintain mouth opening with physiotherapy sessionsto prevent secondary scarring and fibrosis. In thesubsequent days, the inter incisor mouth openinggradually improved to 45 mm (figure 5). Afterwards, hewas discharged from the hospital with an advice tocontinuing orthopedic rehabilitation and maintenanceof oral hygiene. At consequent monthly follow up evenafter ten months revealed maintenance of mouthopening with no features of a relapse.
DISCUSSIONTrismus – Psuedocamptodactyly Syndrome is a rareautosomal dominant disease affecting multiple familymembers, which manifests as inability to open themouth (most likely due to masseteric fibrous bands andcoronoid hyperplasia, which lead to molding deformitiesand developmental hypoplasia of the bones of
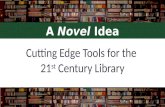
Figure 1: A, B) Features of psuedocamptodactyly (flexion contractures of the distal joints of the hands) with dysmorphic facialfeatures including microagnathia, low set ears and macrocephaly. Features of Trismus (difficulty in opening the mouth), withdiffuse hypermelanotic pigmentation of palms along with arachnodactyly.
IJCRI 201 2;3(3):1 9-23.www.ijcasereportsandimages.com

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 3, March 201 2. ISSN – [0976-31 98]
Chattopadhyay et al. 21
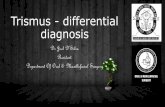
Figure 2: An oral pantomogram showing features of condylardysplasia, (right > left) (yellow arrows).
Figure 3: Computed tomography scan reveal bilateral coronoidhyperplasia (yellow arrows).
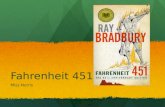
Figure 4: The intra oral device used to maintaining mouthopening and for orthopedic rehabilitation.
mandible), flexion contractures of the fingers (apparenton dorsiflexion), with facial dysmorphism in the form ofmacrocephaly, facial asymmetry, downslantingpalpebral fissures, micrognathia, long philtrum, low setears, arachnodactyly, and chest wall deformities [1, 2].Trismus – Pseudocamptodactyly Syndrome can also beassociated with the Carney Complex Variant in whichspotty hyperpigmentation or lentiginosis occurs alongwith distal arthrogryposis and cardiac myxomas. Hechtand Beal in 1969, described this rare occurrence in afather and his four children (two sons, two daughters)who presented with problems in mastication and shortfinger flexor shortening leading to camptodactyly [3].Jong (1971), Ter Haar and Vanhoof (1974) and Mabry etal (1974) associated the complex of Trismus withPsuedocamptodactyly in a large number of familiesfrom Denmark and also in a kindred with severefeatures who was traced back to a Dutch girl whomigrated to Tennessee soon after the American
Revolution, and hence came a new nomenclature, theDutchKentucky Syndrome [4, 5, 6].Mabry et al. 1974; Lefaivre and Aitchison, 2003 [7],Veugelers et al. 2004 [8] identified an arginine 674toglutamine mutation in the MYH8 gene (which was infact previously found to be associated with the Carneycomplex) leading to this autosomal dominant disease.Toydemir et al. (2006) identified the R674Q mutationin the MYH8 gene in all affected members of fourfamilies with trismuspseudocamptodactyly syndrome,including descendants of the Dutch family reported byTer Haar and Van Hoof (1974) [9]. Bamshad et al.(1996) in a revised and extended classification schemeof the distal arthrogryposis, referred to this disorder asdistal arthrogryposis type 7 (DA7) [10].In 1992, Chen et al. and in 2008, MinzerConzetti etal. broadened the phenotype of TrismusPsuedocamptodactyly Syndrome by adding furtherfindings into the clinical spectrum of the disease andalso showed that trismus and camptodactyly can occureven as isolated events in some cases [11, 12 ].Hence, these case reports suggest that TrismusPsuedocamptodactyly Syndrome is an autosomaldominant disease that runs in many generations of thefamily.Hyperpigmentation can be of localized and diffusetype. Diffuse hyperpigmentation occurring since birth isa very rare abnormality and can be seen with CongenitalAdrenal Hypoplasia (coalblack pigmentation), and withother rare dermatological conditions like MelanosisUniversalis Hereditaria, Diffuse Congenital Melanosis,Familial Progressive Hyperpigmentation, Generalized
IJCRI 201 2;3(3):1 9-23.www.ijcasereportsandimages.com

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 3, March 201 2. ISSN – [0976-31 98]
Chattopadhyay et al. 22
Figure 5: A, B) Improvement in mouth opening, post surgical on follow up (A anterior view, B lateral view).
Acanthosis Nigricans [13]. Lentigenes have beendescribed with TrismusPsuedocamptodactylySyndrome before, in the form of spotty pigmentationalong with Carney Complex.The treatment options for PsuedocamptodactylySyndrome are bleak. The main target is alleviation ofsymptoms, mainly Trismus, by operative procedures,since pharmacological management is of little help.Even then, any possible surgical therapy must beundertaken in these patients to relieve trismus so muchso, that, most of these patients suffer fromcomplications of malnutrition.Our patient presented with typical features oftrismuspseudocamptodactyly syndrome and previouslyunidentified phenotype of diffuse cutaneous melanocytichyperpigmentation, but lacked the Carney Complexabnormalities. His elder brother had same features butto a much lesser degree and was asymptomatic and thusoblivious of the potential peril. Diffuse cutaneous coalblack pigmentation without carney complex associatedwith trismus–pseudocamtodactyly syndrome has notbeen documented before in peer reviewed literature.Surgical management of TrismusPsuedocamptodactyly syndrome has been glorified veryseldom in medical literature. Almost all the casesreported before involved correction of coronoidhyperplasia by a respective procedure, followed byorthopedic rehabilitation and timely oral deviceapplication. Lefaivre and Aitchison in 2003 firstreported the surgical management of this disease intheir seminal report that highlighted the correction oftrismus in a 28monthold man who had a mouthopening of 6 mm. The man had initial endoscopiccorrective procedure resulting in an early relapse at sixweeks, which was then definitively corrected byextensive sub periosteal mandibular resection and
coronoidectomy with a final mouth opening at 25 mm at12 month follow up Gasparini et al. (2008) reported thesurgical correction in a girl at four years of age by meansof coronoidectomy which subsequently relapsed aftersix years and was then managed with a second definitivesurgery without further relapse [14]. Another casereport highlighted a single corrective bilateralcoronoidectomy that provided normal mouth opening ina patient with an initial opening of 25 mm [15]. Promptand complete early correction of coronoid hyperplasiain HechtBeal Syndrome along with timely applicationof oral devices, orthopedic physiokinetic therapy andmaintenance of oral hygiene proves to be gladdening inmanagement of this curious and difficult to treat diseaseentity.
CONCLUSIONHecht Beal Syndrome encompasses a variety ofgenotypic and phenotypic verges in a patient. As moreawareness transpire, with an extensive armada ofnonpareil diagnostics, the mutational and expressivevariations of this disease is becoming more curious andobvious. In our patient, trismus was a main concern,which was dealt successfully through surgery. The caseunder scrutiny here brings forth avantgarde clinicalassociation debut of coal black skin pigmentation andtrismus in a patient of Hecht Beal Syndrome in whomsurgical correction of lock jaw (addressed less in otherreports) resulted in an improvement in quality of life,pushing further insights into novel representations ofthis group of diseases.
*********
IJCRI 201 2;3(3):1 9-23.www.ijcasereportsandimages.com

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 3, March 201 2. ISSN – [0976-31 98]
Author ContributionsPartha Chattopadhyay – Analysis and interpretation ofdata, Drafting the article, Final approval of the versionto be publishedCyriac Abby Philips – Conception and design, Analysisand interpretation of data, Drafting the article, Criticalrevision of the article, Final approval of the version to bepublishedDebargha Dhua – Acquisition of data, Critical revisionof the article, Final approval of the version to bepublishedPrabir Kumar Josh – Analysis and interpretation ofdata, Drafting the article, Final approval of the versionto be publishedPrasanta Mukhopadhyay – Analysis and interpretationof data, Critical revision of the article, Final approval ofthe version to be publishedGuarantorThe corresponding author is the guarantor ofsubmission.Conflict of InterestAuthors declare no conflict of interest.Copyright© Partha Chattopadhyay et al. 2012; This article isdistributed under the terms of Creative Commonsattribution 3.0 License which permits unrestricted use,distribution and reproduction in any means providedthe original authors and original publisher are properlycredited. (Please see www.ijcasereportsandimages.com/copyrightpolicy.php for more information.)
REFERENCES1. Yamashita DD, Arnet GF. Trismuspseudocamptodactyly syndrome. J Oral Surg1980;38:62530.2. Robertson RD, Spence MA, Sparkes RS, NeiswangerK, Field LL. Linkage analysis with the trismuspseudocamptodactyly syndrome. Am J Med Genet1982;12:11520.3. Hecht F, Beals RK. New syndrome of congenitalcontractural arachnodactyly originally described byMarfan in 1896. Pediatrics 1972 Apr;49(4):5749.4. Mabry CC, Barnett IS, Hutcheson MW, SorensonHW. Trismus pseudocamptodactyly syndrome:DutchKentucky syndrome. J Pediat 1974;85:5038.5. Ter Haar BGA, Van Hoof RF. The TrismusPseudocampylodactyly Syndrome. J Med Genet1974;11:419.6. Jong JGY. A family showing strongly reduced abilityto open the mouth and limitation of somemovements of the extremities. HUMAN GENETICS1971;13(3)2107.7. Lefaivre JF, Aitchison MJ. Surgical correction oftrismus in a child with Hecht syndrome. Ann PlastSurg 2003 Mar;50(3):3104.8. Veugelers M, Bressan M, McDermott DA, et al.Mutation of perinatal myosin heavy chain associatedwith a Carney complex variant. N Engl J Med 2004Jul 29;351(5):4609.
Chattopadhyay et al. 23
9. Toydemir RM, Chen H, Proud VK, et al. Trismuspseudocamptodactyly syndrome is caused byrecurrent mutation of MYH8. Am J Med Genet PartA 2006 Nov 15;140(22):238793.10. Bamshad M, Jorde LB, Carey JC. A revised andextended classification of the distal arthrogryposes.Am J Med Genet 1996;65:27781.11. Chen H, Fowler M, Hogan Genome Res, et al.Trismuspseudocamptodactyly syndrome: Report ofa family and review of literature with specialconsideration of morphologic features of themuscles. Dysmorph Clin Genet 1992;6:16574.12. MinzerConzetti K, Wu E, Vargervik K, Slavotinek A.Phenotypic variation in trismuspseudocamptodactyly syndrome caused by arecurrent MYH8 mutation. Clin Dysmorph2008;17:14.13. Verbov J, Hereditary diffuse hyperpigmentation.Clinical and Experimental Dermatology1980;5:227–34.14. Gasparini G, Boniello R, Moro A, Zampino G, Pelo S.Trismuspseudocamptodactyly syndrome: casereport ten years after. Eur J Pediatri Dent 2008Dec;9(4):199203.15. Carlos R, Contreras E, Cabrera J. Trismuspseudocamptodactyly syndrome (Hecht–Bealssyndrome): case report and literature review. OralDis 2005 May;11(3):186–9.
IJCRI 201 2;3(3):1 9-23.www.ijcasereportsandimages.com