A new treatment approach for severe Legg-Calvé-Perthes ... · The FHRO surgery starts with an expo...
5
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2018 A new treatment approach for severe Legg-Calvé-Perthes deformity based on computer simulation and surgical navigation Ackermann, Joelle ; Ganz, Reinhold ; Fuernstahl, Philipp Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: https://doi.org/10.5167/uzh-166619 Journal Article Published Version Originally published at: Ackermann, Joelle; Ganz, Reinhold; Fuernstahl, Philipp (2018). A new treatment approach for severe Legg-Calvé-Perthes deformity based on computer simulation and surgical navigation. Leading opinions. Orthopädie Rheumatologie:6-9.
Transcript of A new treatment approach for severe Legg-Calvé-Perthes ... · The FHRO surgery starts with an expo...

Zurich Open Repository andArchiveUniversity of ZurichMain LibraryStrickhofstrasse 39CH-8057 Zurichwww.zora.uzh.ch
Year: 2018
A new treatment approach for severe Legg-Calvé-Perthes deformity basedon computer simulation and surgical navigation
Ackermann, Joelle ; Ganz, Reinhold ; Fuernstahl, Philipp
Posted at the Zurich Open Repository and Archive, University of ZurichZORA URL: https://doi.org/10.5167/uzh-166619Journal ArticlePublished Version
Originally published at:Ackermann, Joelle; Ganz, Reinhold; Fuernstahl, Philipp (2018). A new treatment approach for severeLegg-Calvé-Perthes deformity based on computer simulation and surgical navigation. Leading opinions.Orthopädie Rheumatologie:6-9.

6 Orthopädie & Rheumatologie 4 / 2018
Referat
HÜFTE
A new treatment approach for severe Legg-Calvé-Perthes deformity based on computer simulation and surgical navigationLegg-Calvé-Perthes is a hip disorder occurring in children, which causes deformity of the femoral head. For the surgical treatment of severe cases, a so-called femoral head reduction osteotomy (FHRO) can be performed in which a wedge needs to be resected to restore the sphericity of the joint. Although very good outcomes after FHRO have been reported, the surgery is rarely performed because preoperative planning and surgical execution are very challenging. Due to advances in computer-assisted surgery, new treatment concepts for FHRO could be developed which enable safer and more precise execution.L egg-Calvé-Perthes (LCP) is a relatively common orthopaedic disease in paedi-atric hip disorders, with a prevalence of 1 case per 1200 children.1 It has an onset between 5–10 years of age and it is caused by a disturbance of perfusion of the femo-ral head, leading to avascular necrosis (death of bone tissue) and deformations of the femoral head.2 Revascularisation is slow and the necrotic bone undergoes fa-tigue fracturing, leading to flattening of the contour to an ellipsoid shape with an extra-large horizontal and a small vertical diameter. The femoral deformity initiates a reactive adaptation of the ace-tabulum. Traditional treatment con-cepts for LCP range from con-servative methods trying to keep the deformation as small as possible with mechanical unloading the joint,3 to surgi-cal methods trying to improve containment and therewith enlarge the load distribution area.4 Possible conservative treat-ments are adductor tenotomy, bracing and physical therapy. Traditional surgical methods, in turn, are femoral varus os-teotomy, which realigns the
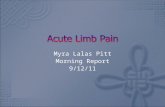
femoral head relative to the hip socket, as well as pelvic osteotomies, to achieve ade-quate coverage of the femoral head. In one-third of the cases, however, the defor-mity of the head and the reactive acetabu-lar deformity are too large and exceed the possibilities of traditional treatment con-cepts. Deeper understanding of blood supply in the femoral head encouraged the deve-lopment of a more effective surgical tech-nique,5 which permits to directly correct the femoral head morphology, rather than indirectly compensating overall joint func-tionality by altering the femoral shaft or pelvis. The so-called femoral head re-duction osteotomy (FHRO) allows reshaping the head to its anatomical spherical shape by resection of the necrotic or deformed cen-tral part (Fig. 1).6 The de-termination of the optimal correction, however, inclu-ding definition of the seg-ment to be removed and direction of the cuts to achieve the resection, des-cribes an exceedingly dif-ficult 3D (three dimensio-nal) geometrical problem. Conservative preopera-tive planning, which is based on analysis of plain
P. Fürnstahl, Zürich
Fig. 1: Schematic view of a femoral head resection (FHRO) (modified from Ganz et al. 2009)6
KEYPOINTS●● Computer-assisted surgery can even drive the development of completely new treatment concepts such as for LCP. ●● The computer-assisted treat-ment approach comprises a 3D preoperative planning stage in which the surgery is simulated in a patient-specific fashion. ●● Based on the simulated surgery, patient-specific navigation in-struments can be designed and 3D-printed. ●● The instruments permit a more precise and safer execution of the surgery. Therewith it may help to further improve the results and hopefully encoura-ges a more prevalent future employment of the FHRO worldwide.
© Universitätsklinik Balgrist

Orthopädie & Rheumatologie 4 / 2018 7
Referat
HÜFTEradiographs or single computed tomogra-phy (CT) scans, cannot sufficiently cap-ture the 3D problem. Moreover, it lacks appropriate tools for precise surgical im-plementation of the planned correction. These may be reasons why the number of cases treated with FHRO remains world-wide low considering the prevalence of LCP.4Our previous work on computer-assis-ted surgery methods for complex orthopa-edic interventions in upper7-11 and lower12 extremities paved the ground for the de-velopment of a new computer-assisted FH-RO treatment method. We would like to describe the computer-assisted FHRO treatment approach on the basis of an ex-ample case of a LCP patient with severe deformation on the left femoral head. The patient was a 15-year-old female pupil. The severe deformity of her femoral head caused pain and forced her to give up rhythmic gymnastics, which she did semi-professionally since the age of 6 (Fig. 2A, B).The treatment involves two compo-nents, computer-assisted preoperative planning in which every step of the FHRO is computer-simulated in 3D, and intraope-rative navigation through patient-specific instruments (PSI) permitting a precise realisation of the planned correction. Preoperative planningIn a first step, a 3D reconstruction of the pathological bone is obtained by seg-menting CT data (Fig. 2B) using a com-mercial software (Mimics, Version 19; Materialise, Leuven, Belgium). The resul-ting 3D model (Fig. 2C) can then be im-ported into our in-house developed pre-operative planning software CASPA (Com-puter Assisted Surgical Planning Applica-tion, Version 5; Balgrist CARD AG, Zurich, Switzerland), which is capable of precise-ly simulating each step of the surgical pro-cedure in 3D. Thereby, the optimal osteo-tomy parameters can be established in a quantitative and objective fashion.As shown in Fig. 3, the planning proce-dure is composed of the following steps: the placement of the osteotomy planes (Fig. 3A) such that the wedge (red) can be resected and the lateral fragment (purple) can be mobilized (Fig. 3B). The reduction of the mobile fragment to achieve a sphe-
rical femoral head is shown in Fig. 3C. In this example case, we used a mirror-model of the healthy contralateral femur as a cor-rection goal (Fig. 3D). In case of bilateral deformities, we employ so-called statisti-cal shape models (SSMs) to predict the pre-morbid anatomy. A SSM is built from femora models from a representative set of individuals in order to learn the anato-mical variation between different subjects. This summation of all possible shapes can then be fitted to a new patient for predic- ting the healthy shape of the femoral head without pathological deformation. Resto-ring the sphericity of the femoral head is the main objective in the preoperative planning. Another challenge is to define the osteotomy planes without compromi-sing the blood supply of the femoral head.5 Additionally, a decent remaining neck dia-meter on the femoral shaft, approximately 1/3 of the pathological neck diameter, needs to be considered as well to ensure overall stability (Fig. 3C). Fig. 4: A) 3-D printed PSI and true-size replica of the pathological femur. B) Verification of the PSI on the replica of the pathological femur. C) Postoperative femur model
A B CFig. 3: Simulated outcome of the FHRO using computer-assisted preoperative planning, anterior-posterior view. A) Definition of osteotomy planes (cyan). Stable fragment (orange), mobile fragment (pink) and wedge to be resected (red). B) A sufficiently large remaining neck diameter must be con-sidered (indicated by arrow). C) Final position of the mobile fragment, achieving a spherical femoral head. D) Mirror-model of contralateral femur, used as correction goal (green)
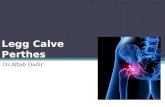
A B C DFig. 2: A) X-ray image of the example case suffering LCP. A blue arrow indicates the location of the necrosis and the severe deformation of the femoral head. B) CT scan showing the pathological bone. C) 3D simulation permits examination of the bone form every perspective, hence provides more information of the pathology
A B C

8 Orthopädie & Rheumatologie 4 / 2018
Referat
HÜFTE
Patient-specific navigation instruments and surgical executionThe CASPA software additionally per-mits the design of PSI which guarantee a very precise execution of surgical tasks such as drilling, cutting, and reduction (Fig. 4). Each PSI is represented as 3D mo-del and has a dedicated position and func-tion in the preoperative planning. For in-stance, the PSI for guiding the osteotomies of the FHRO are located anteriorly on the proximal femur shaft. They integrate a cutting slit in which the sawblade can be entered to perform the osteotomy exactly as planned. They key idea of PSI is the undersurface of the instrument base, which guarantees to place the instruments in the surgery on the bone exactly on the same position as preoperatively planned. This can be achieved by computer algo-rithms which are capable of moulding the undersurface as a negative of the bone surface. Afterwards, a selective laser-sin-tering device (3D printer) is used to ma-nufacture the PSI as CE-conform medical products (manufacturer: Medacta SA, Castel San Pietro, Switzerland). A biocom-patible polyamide PA2200 is used as the raw material for printing. Before surgery, the PSI are verified on a true-size replica of the pathological fe-mur (see Fig. 4B) and sterilised with con-ventional steam pressure sterilisation. The FHRO surgery starts with an expo-sure of the hip using the surgical disloca-tion approach,13 including a trochanteric osteotomy, which enables full access to the joint. The trochanter and hence muscles and ligaments are reattached after the re- section. The first PSI is then applied to the femoral shaft and shifted proximally until the optimal position can be found (Fig. 5). The first osteotomy is performed by inser-ting the saw blade into the slit of the PSI (lateral cut, Fig. 5A). Afterwards, the se-cond PSI is applied to complete the wedge resection (medial cut, Fig. 5B), followed by the reduction of the mobile fragment to its planned position (Fig. 5D). The frag-ment is secured with three lag screws to the medial part, while two further screws secure the trochanter fragment (Fig. 6).
Discussion and outlookThe progress in technology, especially in computer simulation and 3D printing, has enabled the application computer-as-sisted preoperative planning and surgical navigation in hip surgery. Above all, we see the benefits particularly for FHRO: The precise planning of the osteotomies, which are required to reconstruct the sphericity of the head, is hardly possible on conventional, plain radiographs or sin-gle CT scans due to the limitations of 2D based methods. To date, the proposed computer-assisted treatment approach has been successfully applied in five LCP ca-ses. Furthermore, we have initiated a com-prehensive clinical trial to investigate the effectiveness of the method more systema-tically and in a larger setting.Previous studies have already shown that the application of PSI can result in a significantly improved surgical execution compared to the freehand technique.10 Therefore, we strongly expect to observe equivalently high precision in PSI-naviga-ted FHRO. Moreover, the more controlled execution of the osteotomies reduces tech-nical failures, which is particularly advan-tageous in complex interventions. Further-more, the application of PSI has shown to reduce surgery time,10 which is beneficial for the patient and reduces costs. However, there are also limitations to this method. The preoperative time effort to create the 3D simulation and to design the PSI is - with up to 5 hours on average - still very high. Consequently, costs for PSI design amount up to 3000 EUR and manufacturing costs of 600 EUR have to be considered as well. Unfortunately, in-surance companies do not reimburse the-se expenses, because the tariff structure in the Swiss health care system is not yet prepared to consider costs of innovative, new technology within a reasonable time. Another drawback is the long production
Fig. 5: A) Navigated osteotomy using the first PSI (lateral cut). B) Navigated osteotomy using the second PSI, resulting in a medical cut such that the wedge can be resected. In C) the result after the osteotomies is shown. D) Result after wedge resection and fixation of the fragment in the planned position Fig. 5: A) Navigated osteotomy using the first PSI (lateral cut). B) Navigated osteotomy using the second PSI, resulting in a medical cut such that the wedge can be resected. In C) the result after the osteotomies is shown. D) Result after wedge resection and fixation of the fragment in the planned position Fig. 6: Post-operative radiographs 7 weeks after the FHRO. A reorientation of the acetabu-
lum was additionally performed in this case to achieve optimal joint congruency
A B C D

Orthopädie & Rheumatologie 4 / 2018 9
Referat
HÜFTElead time of 2 weeks, required for 3D prin-ting of the PSI.Future work will address the develop-ment of computer algorithms to automate the planning process such that planning times and costs can be reduced. Further-more, the consideration of additional image modalities such as MRI will enable the integration of cartilage models into preoperative planning. The herein presented new computer-based treatment concept for LCP permits sophisticated 3D preoperative planning and a simpler, safer and more precise sur-gical execution. nAuthors: Joëlle Ackermann1, 2 Reinhold Ganz3 Philipp Fürnstahl2 1 Laboratory for Orthopaedic Biomechanics, ETH Zurich, Zurich, Switzerland;
2 Computer Assisted Research and Development Group, Balgrist University Hospital,
University of Zurich, Zurich, Switzerland; 3Faculty of Medicine, University of Berne, Berne, Switzerland Corresponding author:Dr. Sc. Philipp Fürnstahl
E-Mail: [email protected] References:
1 Wada I et al.: [Bone disease with pain. Legg-Calvé-Per-thes' disease (LCPD)]. Clin Calcium 2008; 18(29): 239-48 2 Ziebarth K et al.: Residual Perthes deformity and surgi-cal reduction of the size of the femoral head. Oper Tech Orthop 2013; 23(3): 134-9 3 Wild A et al.: Die nichtopera-tive Therapie des Morbus Perthes. Orthopäde 2003; 32(2): 139-45 4 Siebenrock KA et al.: Head reduction os-teotomy with additional containment surgery improves sphericity and containment and reduces pain in Legg-Calvé-Perthes disease. Clin Orthop Relat Res 2015; 473(4): 1274-83 5 Gautier E et al.: Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br 2000; 82(5): 679-83 6 Ganz R et al.: Extended retinacular soft-tissue flap for intra-articular hip
surgery: surgical technique, indications, and results of ap-plication. Instr Course Lect 2009; 58: 241-55 7 Vla-chopoulos L et al.: Three-dimensional corrective osteoto-mies of complex malunited humeral fractures using pati-ent-specific guides. J Shoulder Elbow Surg 2016; 25(12): 2040-7 8 Vlachopoulos L et al.: Computer-assisted plan-ning and patient-specific guides for the treatment of mids-haft clavicle malunions. J Shoulder Elbow Surg 2017; 26(8): 1367-73 9 Schweizer A et al.: Three-dimensional correction of distal radius intra-articular malunions using patient-specific drill guides. J Hand Surg Am 2013; 38(12): 2339-47 10 Schweizer A et al.: Computer-assisted 3-di-mensional reconstructions of scaphoid fractures and non-unions with and without the use of patient-specific gui-des: early clinical outcomes and postoperative assess-ments of reconstruction accuracy. J Hand Surg Am 2016; 41(1): 59-61 11 Vlachopoulos L et al.: Three-dimensional postoperative accuracy of extra-articular forearm osteo-tomies using CT-scan based patient-specific surgical gui-des. BMC Musculoskelet Disord 2015; 16: 336 12 Wirth S et al.: Computer aided three-dimensional surgical plan-ning with patient-specific instruments for accurate correc-tion of malaligned bones of the foot and ankle. Fuss und Sprunggelenk 2015; 13(2): 123-32 13 Ganz R et al.: Surgi-cal dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001; 83(8): 1119-24
Neue Ansätze im Kampf gegen infizierte ImplantateImplantatassoziierte Infektionen waren ein Schwerpunktthema auf der Agenda des Deutschen Kongresses für Orthopädie und Unfallchirurgie (DKOU) 2018. Unter anderem wurden neue Ansätze zur Vorbeugung und Behandlung dieser Komplikation diskutiert.Wundinfektionen nach einer Operati-on gehören zu den gefürchtetsten Komplikationen in allen chirurgischen Fächern. Auf Implantaten können Bakte-rien eine dünne Schleimschicht, den soge-nannten Biofilm, bilden, der sie vor An-griffen des Immunsystems oder Antibioti-ka schützt. Ohne Behandlung droht eine Blutvergiftung. «Patienten, die nach einer Operation starke Schmerzen im Wundbe-reich oder Fieber haben, müssen deshalb so schnell wie möglich untersucht und behandelt werden», betonte Prof. Dr. med. Joachim Windolf, einer der Kongressprä-sidenten des DKOU 2018. Meist sind dann mehrere Operationen notwendig, bei de-nen das Implantat entfernt und die Ein-griffsstelle von Keimen befreit werden muss. Bei den besonders schwerwiegen-den Formen der bakteriellen Entzündung des Knochens (Osteomyelitis) ist ein inter- disziplinärer Therapieansatz erforderlich. «Der Operateur sollte dazu einen Infektio-logen, Mikrobiologen und gegebenenfalls einen plastischen Chirurgen mit in die Behandlung einbeziehen», sagt Windolf. Dies empfiehlt auch die aktuelle Leitlinie der Deutschen Gesellschaft für Unfallchi-rurgie (DGU).1 Um das Risiko für Infektionen so gering wie möglich zu halten, empfiehlt Windolf folgende Massnahmen: ein Vorab-Scree-ning auf multiresistente Erreger (z.B. MRSA), strenge Hygiene nicht nur im OP, sondern im gesamten Krankenhaus und möglichst gewebeschonende Operations-techniken. Eine weitere Präventionsmass-nahme ist etwa die Verwendung antimik-robiell beschichteten Fadenmaterials oder spezieller antibiotikahaltiger Knochenze-mente für die Verankerung der Kunstge-lenke. Studien zeigen, dass dieser das In- fektionsrisiko deutlich verringert, vor al-lem bei den besonders risikoreichen Kor-rektur- oder Wechseloperationen.2 Für Platten und Nägel, die bei offenen und somit stark infektionsgefährdeten Knochenbrüchen eingesetzt werden, gibt es Beschichtungen, die die Ansiedlung von Keimen verhindern sollen. In Laborversu-chen wird zudem die gezielte Anwendung von Viren, welche sich auf die Zerstörung von Bakterien spezialisiert haben (Bakte-riophagen), untersucht. Diese sind in der Lage, in den bakteriellen Biofilm einzu-dringen und diesen zu zerstören. (red) nQuelle:
Pressemitteilung zum DKOU 2018, 23.–26. Oktober 2018, BerlinLiteratur: 1 Tiemann A et al.: Leitlinie der DGU 2017; AWMF-Nr. 012-033; www.awmf.org 2 Wang J et al.: PLoS ONE 2013; 8(12): e82745
NEWS