A Network Meta-Analysis of Long-Acting Muscarinic ... · The Author(s) 2017. This article is an...
20
ORIGINAL RESEARCH A Network Meta-Analysis of Long-Acting Muscarinic Antagonist (LAMA) and Long-Acting b 2 -Agonist (LABA) Combinations in COPD Katya Y. J. Sion . Eline L. Huisman . Yogesh S. Punekar . Ian Naya . Afisi S. Ismaila Received: April 19, 2017 / Published online: August 22, 2017 Ó The Author(s) 2017. This article is an open access publication ABSTRACT Introduction: Comparative data on the effica- cies of long-acting muscarinic antagonist (LAMA) and long-acting b 2 -agonist (LABA) combinations for the treatment of moder- ate-to-very-severe chronic obstructive pul- monary disease (COPD) are limited. The aim of this Bayesian network meta-analysis (NMA) is to assess the relative efficacies of available open combinations (delivered via separate inhalers) and fixed-dose combinations (FDCs, delivered via a single inhaler). Methods: We conducted a systematic literature review with the aim of identifying randomized controlled trials (RCTs) of C8-week duration in adults aged C40 years with COPD that com- pared LAMA ? LABA combinations with each other, with tiotropium (TIO), or with placebo. Data on changes from baseline in trough forced expiratory volume in 1s (FEV 1 ) and on St George’s Respiratory Questionnaire (SGRQ) total score, the Transition Dyspnea Index (TDI) focal score, and rescue medication use at 12 and 24 weeks were extracted from these RCTs and analyzed using a NMA in a Bayesian framework. Results: Data from 44 RCTs were included in the NMA. All FDCs showed improvements Enhanced Content To view enhanced content for this article go to http://www.medengine.com/Redeem/ 72E8F06066607981. Electronic supplementary material The online version of this article (doi:10.1007/s41030-017-0048-0) contains supplementary material, which is available to authorized users. K. Y. J. Sion Á E. L. Huisman Real World Strategy and Analytics, Mapi Group, Houten, The Netherlands Y. S. Punekar ViiV Healthcare, GlaxoSmithKline, Brentford, Hounslow, Middlesex, UK I. Naya Respiratory Medicine Development Centre, GlaxoSmithKline, Brentford, Hounslow, Middlesex, UK A. S. Ismaila (&) Value Evidence and Outcomes, GlaxoSmithKline, 5 Moore Drive, PO Box 13398, Research Triangle Park, NC 27709-3398, USA e-mail: afi[email protected] A. S. Ismaila Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, ON, Canada Present Address: K. Y. J. Sion Care and Public Health Research Institute, Maastricht University, Maastricht, The Netherlands Present Address: E. L. Huisman Novo Nordisk, Alphen aan den Rijn, The Netherlands Pulm Ther (2017) 3:297–316 DOI 10.1007/s41030-017-0048-0
Transcript of A Network Meta-Analysis of Long-Acting Muscarinic ... · The Author(s) 2017. This article is an...

ORIGINAL RESEARCH
A Network Meta-Analysis of Long-Acting MuscarinicAntagonist (LAMA) and Long-Acting b2-Agonist(LABA) Combinations in COPD
Katya Y. J. Sion . Eline L. Huisman . Yogesh S. Punekar . Ian Naya .
Afisi S. Ismaila
Received: April 19, 2017 / Published online: August 22, 2017� The Author(s) 2017. This article is an open access publication
ABSTRACT
Introduction: Comparative data on the effica-cies of long-acting muscarinic antagonist(LAMA) and long-acting b2-agonist (LABA)combinations for the treatment of moder-ate-to-very-severe chronic obstructive pul-monary disease (COPD) are limited. The aim ofthis Bayesian network meta-analysis (NMA) is toassess the relative efficacies of available open
combinations (delivered via separate inhalers)and fixed-dose combinations (FDCs, deliveredvia a single inhaler).Methods: We conducted a systematic literaturereview with the aim of identifying randomizedcontrolled trials (RCTs) of C8-week duration inadults aged C40 years with COPD that com-pared LAMA ? LABA combinations with eachother, with tiotropium (TIO), or with placebo.Data on changes from baseline in trough forcedexpiratory volume in 1 s (FEV1) and on StGeorge’s Respiratory Questionnaire (SGRQ)total score, the Transition Dyspnea Index (TDI)focal score, and rescue medication use at 12 and24 weeks were extracted from these RCTs andanalyzed using a NMA in a Bayesian framework.Results: Data from 44 RCTs were included inthe NMA. All FDCs showed improvements
Enhanced Content To view enhanced content for thisarticle go to http://www.medengine.com/Redeem/72E8F06066607981.
Electronic supplementary material The onlineversion of this article (doi:10.1007/s41030-017-0048-0)contains supplementary material, which is available toauthorized users.
K. Y. J. Sion � E. L. HuismanReal World Strategy and Analytics, Mapi Group,Houten, The Netherlands
Y. S. PunekarViiV Healthcare, GlaxoSmithKline, Brentford,Hounslow, Middlesex, UK
I. NayaRespiratory Medicine Development Centre,GlaxoSmithKline, Brentford, Hounslow, Middlesex,UK
A. S. Ismaila (&)Value Evidence and Outcomes, GlaxoSmithKline,5 Moore Drive, PO Box 13398, Research TrianglePark, NC 27709-3398, USAe-mail: [email protected]
A. S. IsmailaDepartment of Clinical Epidemiology andBiostatistics, McMaster University, Hamilton,ON, Canada
Present Address:K. Y. J. SionCare and Public Health Research Institute,Maastricht University, Maastricht, The Netherlands
Present Address:E. L. HuismanNovo Nordisk, Alphen aan den Rijn,The Netherlands
Pulm Ther (2017) 3:297–316
DOI 10.1007/s41030-017-0048-0

relative to placebo in terms of trough FEV1,SGRQ total score, and TDI focal score aboveclinically relevant thresholds, with the excep-tion of TIO/olodaterol and aclidinium/formoterol, both of which failed to show clini-cally relevant improvements in SGRQ score at24 weeks. All FDCs demonstrated reduced res-cue medication use versus placebo. Open com-binations demonstrated improved efficacy in alloutcomes versus placebo, but these improve-ments did not consistently exceed clinicallyrelevant thresholds for SGRQ and TDI scores. Allonce-daily FDCs showed improved efficacyversus TIO, but improvements were less consis-tently observed versus TIO with open dualcombinations and combinations containingformoterol or salmeterol administered twicedaily. Relative probabilities of improvementbetween FDCs highlighted potential between-class differences for trough FEV1 but suggestedlittle potential for differences in patient-reported outcomes.Conclusion: LAMA ? LABA combinations gen-erally showed improved outcomes versus pla-cebo and TIO. FDCs appeared to perform betterthan open dual combinations. A potentialeffectiveness gradient was observed betweenFDCs for objectively assessed functional out-comes, although further prospective trials arerequired to confirm these findings.Funding: GSK.
Keywords: Bayesian analysis; Combinationbronchodilator; Comparative efficacy; COPD;Indirect treatment comparison; LABA; LAMA;Meta-analysis
INTRODUCTION
Bronchodilators, particularly long-acting mus-carinic antagonists (LAMAs) and long-actingb2-agonists (LABAs), have become the mainstayof pharmacological therapy for chronicobstructive pulmonary disease (COPD) [1–3].Despite the well-demonstrated utility of LABAs[4–7] and LAMAs [8–11] as maintenance ther-apy, a high number of patients with moderateor severe COPD receiving LABA or LAMAmonotherapy can fail to achieve adequate
control of symptoms [12]. A combination of aLAMA and a LABA maintenance therapy is alogical therapeutic option to improve symptomcontrol for such patients [13]. In the last decade,multiple randomized controlled trials (RCTs)have reported that improvements in lungfunction and patient-reported outcomes (PROs)can be achieved with LAMA ? LABA combina-tions compared with the componentmonotherapies for patients with stable COPD,with no differences in safety [14–20].
LAMA? LABA combinations can be adminis-tered as open dual combinations (using separateprescribed inhalers for each bronchodilator) andfixed-dose combinations (FDCs; use of a singleinhaler delivering a fixed dose of each bron-chodilator). Several options are available withineach class; in the last few years, several FDCLAMA/LABA therapies have been approved asonce-daily (OD) or twice-daily (BID) maintenancetherapies for COPD, including glycopyrronium/indacaterol (GLY/IND) 110/50 mcg OD (outsidethe USA) [21] and 27.5/15.6 mcg BID (USAonly) [22], umeclidinium/vilanterol (UMEC/VI)62.5/25 mcg OD [23, 24], aclidinium/formoterol(ACL/FOR) 400/12 mcg BID [25], and tiotropium/olodaterol (TIO/OLO) 5/5 mcg OD [26, 27]. Withthe increasing range of LAMA? LABA therapiesthat have become available, it is desirable to assesstheir comparative efficacies and characteristics.Limited data are currently available fromdirect comparisons between FDC LAMA/LABAtherapies or of FDC therapies with open dualLAMA? LABA combinations. There is therefore aneed to synthesize the available data from RCTsto enable comparisons to be made betweentherapies.
The aim of this Bayesian networkmeta-analysis (NMA) was to compare the effi-cacy of available FDC and open dualLAMA ? LABA bronchodilators in patients withmoderate-to-very-severe COPD, based on a sys-tematic literature review (SLR) up to October2015. The NMA reported here contains a further18 trials that were not previously available in anearlier NMA based on the literature up to theend of 2014 [28]. A novel aspect of this NMAcompared with other NMAs in the area is thepotential to examine differences in efficacybetween FDCs and open dual LAMA ? LABA
298 Pulm Ther (2017) 3:297–316

combinations, and between once- and twice-daily therapies. An added feature was to exploresubgroup analyses where possible to observe theimpact of severity of lung function impairmentand use of concurrent inhaled corticosteroids(ICS) across different trials on the relative effi-cacies of bronchodilators.
METHODS
Data Sources
This article is based on a synthesis of previouslyconducted studies and does not involve anynew studies of human or animal subjects per-formed by any of the authors.
A SLR was performed to identify RCTs com-paring open or FDC LAMA ? LABA therapieswith each other, with TIO monotherapy, orwith placebo in adult patients with COPD. Abroad search strategy was utilized to include allavailable LAMAs, LABAs, and LAMA ? LABAcombinations. No time restrictions wereemployed. Several databases and trial registrieswere searched, including MEDLINE�, Embase�,and clinicaltrials.gov, in October 2015 usingpre-defined search strategies specifically tailoredto each platform [details on the data sourcesand search strategies are presented in ElectronicSupplementary Material (ESM) Tables S1, S2].
Inclusion Criteria and Study SelectionProcess
Abstracts were screened independently by tworeviewers, with any discrepancies resolved byconsensus. RCTs included in the NMA werethose published in English or German, ofC8 weeks’ duration, involving adults ofC40 years of age with COPD as defined by theGlobal Initiative for Chronic Obstructive LungDisease (GOLD) guidelines [1].
Only RCTs involving FDC LAMA/LABAs oropen dual LAMA ? LABA combinations, TIO18 mcg OD (TIO 18), TIO 5 mcg OD (TIO 5), orplacebo were included in the NMA. TIOmonotherapy was included as a comparator as itwas used as the principal comparator instead of
placebo in several studies. Studies comparingTIO with placebo were also included tostrengthen the network.
Included trials were required to report out-comes within a 4-week window at 12 (8–16)weeks and/or 24 (20–28) weeks. Outcomes ofinterest were: trough forced expiratory volumein 1 s (FEV1), and the subjective PROs ofbreathlessness assessed by the Transition Dysp-nea Index (TDI) focal score, health-relatedquality of life (HRQoL) assessed by the StGeorge’s Respiratory Questionnaire (SGRQ)total score, and rescue short-acting b2-agonistmedication use (puffs/day).
Data Extraction and Quality Assessment
Data extraction was performed by oneresearcher and reviewed by a second. Key datafrom each eligible study, including study char-acteristics, patient characteristics at baseline,and outcomes of interest, were extracted byrecording data from the original report into astandard data extraction form. For the out-comes of interest, the mean or least squaresmean difference in change from baseline (CFB)between the arms of interest, and associated95% confidence intervals (95% CIs), standarderror (SE), or standard deviation (SD), wereabstracted. If not reported, the difference in CFBwas calculated based on the CFB in each treat-ment arm, and the SE was imputed using theuncertainty of other trials in the network [29]. Achecklist for assessing the risk of bias in RCTsbased on guidance from the Institute for Qual-ity and Efficiency in Health Care was employed[30].
To reduce the risk of imbalances in effectmodifiers (any characteristic of patients orstudies which would influence the treatmenteffect) across studies and obtaining biased out-comes in the NMA, the similarity of studies wasassessed by evaluating the distribution ofpatient characteristics and study designs acrossthe direct comparisons in the network. If anymajor differences were detected, subgroupanalysis was used to evaluate the impact of thedifference on treatment effect. Subgroup anal-yses were performed for four patient subgroups:
Pulm Ther (2017) 3:297–316 299

ICS users and non-users, and patients withmoderate or severe disease (as reported in theindividual study publications). These analyseswere only feasible for the outcome of troughFEV1 due to the limited data available for theother outcomes. It was not feasible to usemeta-regression techniques to adjust for varia-tions due to the relatively limited number ofstudies available in the network.
Bayesian NMA
A NMA was performed within a Bayesianframework [31–33] to analyze the extracted dataand thereby synthesize the results of the inclu-ded studies and assess relative treatment effects.The details of this framework have been pre-sented previously [28]; briefly, a generalizedlinear model with identity link and a normallikelihood distribution was employed, withnon-informative prior distributions assumed forall outcomes.
For each outcome, fixed- and random-effectsmodels were evaluated. The most appropriatemodel for each outcome was identified by cal-culating the Deviance Information Criterion, ameasure of goodness of fit based on the poste-rior mean residual deviance. The parameters ofthe different models were estimated within aBayesian framework using a Markov ChainMonte Carlo method implemented in the R andOpenBUGS software packages (Foundation forStatistical Computing, Vienna, Austria). TheOpenBUGS codes were based on those pre-sented by Dias et al. [34].
The Bayesian NMA provides posterior distri-butions of the relative treatment effectsbetween different therapies for each outcome ofinterest. The posterior distributions are sum-marized using the median (reflecting the mostlikely value of the estimate) and the 2.5 and97.5 percentiles to capture the 95% credibleinterval (95% CrI), with the latter representingthe range of true underlying effects with aprobability of 95%. For each endpoint, theprobability that each treatment is better than acertain comparator is presented; the probabilityof the comparator being better than the initialtreatment is the difference between 100 and the
original probability. Studies reporting meanvalues without any measure of uncertainty (SE,SD, 95% CI) were included in the base caseanalysis with imputed SE values but excludedfrom scenario analyses [29]. A separate analysiswithout imputation was also performed. A sce-nario analysis was conducted to evaluate theimpact of pooling TIO 18 and TIO 5 on therelative effects on trough FEV1.
RESULTS
Study Selection
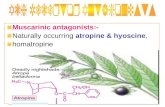
Of a total of 4493 abstracts identified in theinitial literature search, 510 (11.4%) wereassessed to be of interest (Fig. 1). After exclusionof 256 articles, and the addition of fourGlaxoSmithKline (GSK) clinical study reportsand an additional article retrieved by scanningreferences, 259 citations were included in theSLR. Parallel online searches of trial registriesidentified 5838 relevant records. After exclusionof 5650 registries (2304 based on study design,611 based on population, 997 based on inter-vention, 79 based on comparator, 12 based onoutcomes, 13 based on language, and 1634duplicates), 188 registries were suitable forinclusion in the SLR. After merging the searchesand excluding trials involving non-relevantcomparators, we identified a total of 95 cita-tions related to 44 RCTs which were included inthe NMA.
Characteristics of the included RCTs are pre-sented in ESM Table S3, and the results of theassessment for risk of bias are summarized inESM Table S4. Most studies were randomized,double-blind, multicenter trials. Trough FEV1
was the most commonly reported outcome,while rescue medication use was the least com-mon (Table 1). The majority of trials comparedTIO [either TIO 18 (18 trials) or TIO 5 (6 trials)]with placebo. Most trials had a duration of either12–13 weeks (16 trials) or approximately26 weeks (15 trials). Nine trials had a duration ofapproximately 1 year, while three trials werelonger: the SPARK trial (duration 64 weeks [35]),the TIOSPIR� trial (duration 2.3 years [36]), and
300 Pulm Ther (2017) 3:297–316

Search on 2 October 2015MEDLINE® (n=933), Embase® (n=1651),
Cochrane: CENTRAL (n=1810), CDSR (n=23),DARE (n=47), HTA database (n=29)
Title / abstract screening n=4493
Full text screening n=510
Included in SLR: 259 citations related to 133 trials
Included in NMA: 95 citations related to 44 trialsFull text articles, n=42
Conference abstracts, n=49 CSRs, n=4
Abstracts excluded: n=3983Patient population not of interest (180)Intervention not of interest (300)Comparator not of interest (160)Outcomes not of interest (0)Study design not of interest (1699)Language (23) Duplicate (1214) Conference prior to 2009 (407)
Articles excluded: n=256Patient population out of scope (9)Intervention out of scope (12)Comparator out of scope (16)Outcomes out of scope (134)Study design out of scope (80)Language (2) Not retrievable (3)
Articles added: n=5CSRs from GSK studies (4)Articles retrieved byscanning references (1)
Not relevant: n=164Investigating only monotherapiesother than TIO (159)Investigating LAMA/LABA-basedtriple therapy (11)Population out of scope (2)
Fig. 1 PRISMA flow diagram of study selection process.CDSR Cochrane Database of Systematic Reviews, CSRclinical study report, DARE Database of Abstracts ofReviews of Effects, GSK GlaxoSmithKline, HTA Health
Technology Assessment, LABA long-acting b2-agonist,LAMA long-acting muscarinic antagonist, NMA Networkmeta-analysis, SLR systematic literature review, TIOtiotropium
Pulm Ther (2017) 3:297–316 301

Table1
Resultsof
thebase
case
Bayesiannetworkmeta-analysis:placebo-adjusted
levelsof
efficacyof
each
differentbronchodilator
Outcomeof
interest
Num
ber
ofRCTs
analyzed
Mon
otherapy
(inmcg)a
Opendu
alcombination
s(inmcg)a
TIO
5or
18TIO
181
FOR12
bTIO
181
IND
150
TIO
181
OLO
5TIO
181
FOR10
bTIO
181
SAL50
c
TroughFE
V1at
12weeks
(CFB
,mL)
33114.70
(106.20,
123.40);[99%
151.60
(118.80,
183.10);[99%
188.60
(170.20,
207.30);[99%
165.70
(145.30,
186.20);[99%
NA
NA
TroughFE
V1at
24weeks
(CFB
,mL)
24110.90
(102.90,
118.90);[99%
113.50
(76.33,
150.40);[99%
NA
NA
NA
123.60
(39.40,
215.90);[99%
SGRQ
totalscoreat
12weeks
(CFB
)
17-2.97
(-3.41,
-2.53);[99%
-3.99
(-6.94,
-1.03);[99%
NA
-4.82
(-5.82,
-3.82);[99%
NA
NA
SGRQ
totalscoreat
24weeks
(CFB
)
20-2.53
(-2.94,
2.12);[99%
NA
NA
NA
-3.18
(-5.46,
-0.89);[99%
-4.00
(-5.42,
-2.59);[99%
TDIfocalscoreat
12weeks
140.79
(0.52,
1.06);
[99%
0.86
(-0.12,
1.85);96%
NA
NA
NA
NA
TDIfocalscoreat
24weeks
150.83
(0.65,
1.01);
[99%
0.93
(0.41,
1.44);
[99%
NA
NA
NA
0.41
(-0.46,
1.27);82%
Rescuemedicationuseat
12weeks
(CFB
)
11-0.29
(-0.64,
0.06);95%
-0.54
(-1.26,
0.17);93%
-1.16
(-1.58,
-0.74);[99%
NA
NA
NA
Rescuemedicationuseat
24weeks
(CFB
)
9-0.65
(-1.26,
-0.11);99%
NA
NA
NA
NA
NA
Outcomeof
interest
Fixed-do
secombination
s(inmcg)a
ACL/FOR
400/12
dTIO
/OLO
5/5
GLY/IND
27.5/15.6d
GLY/IND
110/50
UMEC/V
I62.5/25
TroughFE
V1
at12
weeks
(CFB
,mL)
135.90
(110.60,
160.80;)[99%
170.20
(153.50,
186.90)[
99%
222.20
(193.30,
250.90);[99%
205.10
(185.70,
224.00);[99%
208.10
(187.90,
228.20);[99%
TroughFE
V1
at24
weeks
(CFB
,mL)
138.20
(117.90,
158.30);[99%
172.10
(152.70,
191.70);[99%
NA
181.80
(162.50,
200.90);[99%
195.80
(174.80,
217.30);[99%
SGRQ
totalscore
at12
weeks
(CFB
)
NA
-4.90
(-6.10,
-3.68);[99%
-4.97
(-6.42,
-3.52);[99%
-4.89
(-5.98,
-3.80);[99%
-4.70
(-5.72,
-3.68);[99%
302 Pulm Ther (2017) 3:297–316

Table1
continued
Outcomeof
interest
Fixed-do
secombination
s(inmcg)a
ACL/FOR
400/12
dTIO
/OLO
5/5
GLY/IND
27.5/15.6d
GLY/IND
110/50
UMEC/V
I62.5/25
SGRQ
totalscore
at24
weeks
(CFB
)
-2.80
(-4.37,
-1.22);[99%
-3.76
(-4.92,
-2.60);[99%
NA
-4.29
(-5.34,
-3.23);[99%
-4.11
(-5.23,
-2.99);[99%
TDIfocalscoreat
12weeks
NA
1.50
(1.01,
2.00);[99%
1.62
(1.07,
2.17);[99%
1.34
(0.67,
1.99);[99%
1.24
(0.77,
1.73);[99%
TDIfocalscoreat
24weeks
1.37
(0.98,
1.76);[99%
1.19
(0.87,
1.51);[99%
NA
1.31
(1.03,
1.58);[99%
1.01
(0.66,
1.36);[99%
Rescuemedicationuse
at12
weeks
(CFB
)
NA
-0.97
(-1.38,
-0.56);[99%
-1.19
(-1.45,
-0.93);[99%
NA
-0.84
(-1.19,
-0.49);[99%
Rescuemedicationuse
at24
weeks
(CFB
)
-0.66
(-1.75,
0.44);92%
-1.28
(-2.52,
-0.12);98%
NA
-1.09
(-2.07,
-0.12);98%
-1.13
(-1.86,
-0.46);[99%
Resultsin
tablearereported
asthemeanim
provem
entwiththe95%credibleinterval(95%
CrI)in
parenthesis,followed
bythepercentage
probabilityof
improved
outcom
eversus
placebo
ACLaclidinium,C
FBchange
from
baselin
e,CrIcredibleinterval,F
EV1forced
expiratory
volumein
1s,FO
Rform
oterol,G
LYglycopyrronium
,IND
indacaterol,
NA
data
notavailable,NMA
networkmeta-analysis,OLO
olodaterol,RCT
rand
omized
controlledtrial,SA
Lsalmeterol,SG
RQ
StGeorge’sRespiratory
Ques-
tionnaire,TDITransitionDyspn
eaIndex,TIO
tiotropium
,UMECum
eclidinium,V
Ivilanterol
aNum
bersfollowingdrug
arethedose.S
ee‘‘Introduction’’for
amoredetailedexplanation.
Note:un
lessindicatedotherwise,alldosesweretakenonce
daily.
bForm
oterol
dose
takentwicedaily
cSalmeterol
dose
takentwicedaily
dCom
bineddose
takentwicedaily
Pulm Ther (2017) 3:297–316 303

the UPLIFT trial (duration 4 years [11]). Nearly allof the trials (40/44) allowed concomitant ICSuse; concurrent LABA therapy was allowed ineight trials which compared TIO with placebo,but was not allowed in the trials involvingLAMA? LABA therapy.
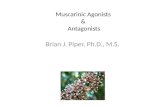
Patient Characteristics
Patient characteristics for all included RCTsare presented in Fig. 2. The mean age ofpatients ranged between 60.5 and 67.9 years,with the percentage of males ranging between49.5 and 98.5%. The increased variability ingender was largely attributable to three trialscomparing TIO with placebo, one of whichrecruited patients from medical centers forveterans, who are predominantly male.
Patients were current smokers (range26.4–59.5%) or former smokers at study entry,all with a smoking history of [10 pack-years.Most trials included patients with both mod-erate and severe COPD (GOLD stages II andIII); some also included patients with verysevere disease (GOLD stage IV). The SPARKtrial was a notable exception as it includedonly patients with severe or very severe COPD,with 76% of patients enrolled using concur-rent ICS, and all patients having reported atleast one moderate/severe exacerbation in theprevious year (Fig. 2) [35].
Bayesian NMA
Because many studies used TIO 18 or TIO 5 asa comparator arm instead of placebo, the base
Garcia 2007Moita 2008
ANHELTO 1ANHELTO 2Aaron 2007
Covelli 2005Chan 2007OTEMTO 1
FLIGHT 1&2TIOSPIR
OTEMTO 2Donohue 2010
GLOW2Abrahams 2013Bateman 2010a
Casaburi 2000Casaburi 2002
INTRUST-2QUANTIFY
Tashkin 2009ZEP117115DB2113374INTRUST-1
Troosters 2014AUGMENT COPD
DB2113360TONADO-1DB2113373TONADO-2
Donohue 2002UPLIFT
ACLIFORM COPDSHINE
Bateman 2010bBeeh 2006
SPARKVoshaar 2008
Brusasco 2003ENLIGHTEN
Vogelmeier 2008TIPHON
Verkindre 2006Niewoehner 2005
% Male
0 50%% Male
100%
Garcia 2007Moita 2008
Verkindre 2006Troosters 2014
Beeh 2006ZEP117115
ENLIGHTENDB2113373DB2113360
Vogelmeier 2008QUANTIFYINTRUST-2
AUGMENT COPDFLIGHT 1&2
SPARKTONADO-1INTRUST-1
GLOW2Donohue 2010
TONADO-2Tashkin 2009
SHINEBateman 2010a
ANHELTO 2Brusasco 2003
Abrahams 2013ACLIFORM COPD
TIPHONANHELTO 1Covelli 2005OTEMTO 2DB2113374
Bateman 2010bVoshaar 2008
OTEMTO 1Casaburi 2000Casaburi 2002
UPLIFTDonohue 2002
TIOSPIRChan 2007Aaron 2007
Niewoehner 2005
Age and COPD duration
0 40 6020Age (years)
80
Garcia 2007Beeh 2006
Vogelmeier 2008Donohue 2010Brusasco 2003Casaburi 2000Casaburi 2002Donohue 2002
Moita 2008TIPHON
Aaron 2007Verkindre 2006
Niewoehner 2005UPLIFT
Chan 2007TONADO-2
Voshaar 2008TIOSPIR
ACLIFORM COPDBateman 2010b
SPARKINTRUST-1
Covelli 2005TONADO-1
SHINEINTRUST-2DB2113374
Bateman 2010aENLIGHTEN
GLOW2Abrahams 2013
OTEMTO 2ANHELTO 2
Tashkin 2009AUGMENT COPD
OTEMTO 1QUANTIFYDB2113360ANHELTO 1FLIGHT 1&2DB2113373ZEP117115
Troosters 2014
Current smokers (%)
0 30%% Current smokers
60%
Garcia 2007Vogelmeier 2008
Brusasco 2003Casaburi 2000
Moita 2008Verkindre 2006
AUGMENT COPDTroosters 2014
Tashkin 2009Aaron 2007
ANHELTO 1TIPHON
Donohue 2010ANHELTO 2OTEMTO 2QUANTIFYOTEMTO 1Beeh 2006
Casaburi 2002ENLIGHTEN
TONADO-2DB2113360
FLIGHT 1&2TONADO-1DB2113373
ACLIFORM COPDDB2113374
GLOW2INTRUST-1
Abrahams 2013ZEP117115INTRUST-2
Voshaar 2008Bateman 2010aBateman 2010b
Covelli 2005SHINE
Niewoehner 2005TIOSPIR
UPLIFTDonohue 2002
Chan 2007SPARK
ICS use (%)
0 40%% ICS use
80%
Garcia 2007Moita 2008
Tashkin 2009Verkindre 2006
Niewoehner 2005Casaburi 2000Casaburi 2002Brusasco 2003
Chan 2007Covelli 2005
Donohue 2002Aaron 2007Beeh 2006
Voshaar 2008Bateman 2010bAbrahams 2013Bateman 2010a
Vogelmeier 2008Donohue 2010
GLOW2Troosters 2014
ENLIGHTENOTEMTO 1
SHINEOTEMTO 2
FLIGHT 1&2ANHELTO 1
AUGMENT COPDANHELTO 2QUANTIFY
ACLIFORM COPDTONADO-2TONADO-1
TIOSPIRDB2113360
UPLIFTINTRUST-1DB2113373DB2113374INTRUST-2ZEP117115
TIPHONSPARK
Disease severity and FEV1
0 50% 100%
Age, mean/yearsCOPD duration, mean/years
% Severe or very severe COPDFEV1 % predicted
Fig. 2 Patient characteristics in the randomized controlledtrials included in the NMA. Values are weighted means ofthe patient populations included in the NMA. Zero valuesindicate that data were not reported. COPD chronic
obstructive pulmonary disease, FEV1 forced expiratoryvolume in 1 s, ICS inhaled corticosteroids, NMA networkmeta-analysis
304 Pulm Ther (2017) 3:297–316

case was performed with studies comparing aLAMA ? LABA intervention of interest toanother LAMA ? LABA intervention of inter-est or to TIO 18 or TIO 5, or placebo. It wasassumed that the results from TIO 18 and TIO5 were sufficiently similar to be pooled toge-ther: similar efficacy and safety have beenreported for both doses in a previous NMA [37]and study [38]. A scenario analysis was con-ducted for trough FEV1 at 12 and 24 weeksto evaluate the impact of pooling the twodoses.
The overall networks of studies for the basecase analysis for each outcome of interest at24 weeks are presented in Fig. 3. The individual
study results for each outcome of interest arepresented in ESM Table S5.
Results are presented for each of the fouroutcomes of interest (trough FEV1, SGRQ totalscore, TDI focal score and rescue medicationuse) for each time point (12 and 24 weeks). Foreach set of results, results of the base case NMA(with imputation) are presented first, compar-ing the active therapies with placebo, then thedual therapies with TIO, and finally the dualtherapies with each other. Results obtainedwithout imputation of SEs are then brieflysummarized, followed by results of the scenarioanalysis, where applicable. Finally, results of thesubgroup analyses are presented.
TIO/OLO5/5
ACL/FOR400/12
TIO 18 +SAL 50
TIO 5or 18PBO
UMEC/VI62.5/25
UPLIFTNiewoehner 2005Brusasco 2003Donohue 2002Donohue 2010SHINEGLOW2Troosters 2014Abrahams 2013Bateman 2010aBateman 2010bCasaburi 2002
GLY/IND110/50
TIO 18 +FOR 12
ACLIFORMAUGMENT
QUANTIFY
Aaron 2007
SHINE
DB2113374
DB2113360
ZEP117115
ENLIGHTEN
SHINESPARK
DB2113
373
TIO/OLO5/5
ACL/FOR400/12
TIO 18 +SAL 50
TIO 5or 18PBO
UMEC/VI62.5/25
TIPHONUPLIFTBrusasco 2003Donohue 2010SHINEGLOW2Vogelmeier 2008Bateman 2010aAbrahams 2013Donohue 2002Casaburi 2002
GLY/IND110/50
TIO 18 +FOR 10
ACLIFORMAUGMENT
TONADO-1TONADO-2
TONADO-1TONADO-2
SHINE SHINESPARK
Aaron 2007
Vogelmeier 2008
DB2113374
DB2113360
ZEP117115
Vogelm
eier 2
008
DB2113
373
a b
TIO/OLO5/5
ACL/FOR400/12
TIO 18 +SAL 50
TIO 5or 18PBO
UMEC/VI62.5/25
Brusasco 2003Casaburi 2002Donohue 2010SHINEGLOW2Abrahams 2013Donohue 2002
GLY/IND110/50
TIO 18 +FOR 12
ACLIFORMAUGMENT
QUANTIFY
Aaron 2007
SHINE
DB2113374
DB2113360
SHINE
DB2113
373
TIO/OLO5/5
ACL/FOR400/12
TIO 5or 18PBO
UMEC/VI62.5/25
Donohue 2010SHINEDonohue 2002
GLY/IND110/50
ACLIFORM
TONADO-1TONADO-2
TONADO-1TONADO-2
SHINE
DB2113374
DB2113360
ZEP117115
SHINE
DB2113
373
c d
Fig. 3 Overall network of studies in the base case NMA ofLAMA? LABA combination therapies evaluated at 24 weeksfor trough FEV1 (a), St George’s Respiratory Questionnaire(SGRQ) total score (b), TransitionDyspnea Index (TDI) focalscore (c), and rescue medication use (d). Studies in blue textrepresent those that reported mean values without standarderrors/standard deviations/confidence intervals. Blue dotted
lines represent relationships for which errors were calculated byimputation. ACL aclidinium, FEV1 forced expiratory volumein 1 s, FOR formoterol, GLY glycopyrronium, IND inda-caterol, LABA long-acting b2-agonist, LAMA long-actingmuscarinic antagonist, NMA network meta-analysis, OLOolodaterol, PBO placebo, SAL salmeterol, TIO tiotropium,UMEC umeclidinium, VI vilanterol
Pulm Ther (2017) 3:297–316 305

NMA Results: Trough FEV1
12 WeeksThe base case analysis results at 12 weeksshowed that all active therapies achievedimprovements in trough FEV1 versus placebo,with probabilities improved outcomes of[99%(Table 1). All improvements were greater thanthe minimal clinically important difference(MCID) of 100 mL [39]. In comparison withTIO, all combination therapies were superior,with probabilities of improved outcomes ofC94% (ESM Table S6).
Comparing the combination therapies, theopen combination TIO 18 OD ? IND 150 OD(TIO ? IND) and the FDCs UMEC/VI andGLY/IND (both doses) all had high probabilities(C94%) of improved outcomes versus the othertherapies [TIO 18 OD ? FOR 12 BID, ACL/FOR,TIO 18 OD ? OLO 5 OD (TIO ? OLO) andTIO/OLO]. Between these three therapies, theFDCs appeared to be superior to the opencombination, with probabilities of improvedoutcomes of C91%. The probability of improvedoutcomes using GLY/IND versus UMEC/VI was78% for the comparison with GLY/IND27.5/15.6, but only 42% for the comparisonwith GLY/IND 110/50 (ESM Table S6).
Results using data without imputed SEs weregenerally similar to the base case results, withonly small differences (\5 mL) in changes inFEV1 for most comparisons except those withTIO/OLO for which differences were larger(\15 mL; data not shown). Comparisons withACL/FOR were not included as these data wereobtained by imputation.
In the scenario analysis, separating TIO 18and TIO 5 had little impact on the base caseresults (data not shown).
24 WeeksThe base case analysis results at 24 weeksshowed that all active therapies achievedimprovements in trough FEV1 versus placebogreater than the 100 mL MCID with probabili-ties of improved outcomes of [99% (Table 1;Fig. 4a). In comparison with TIO, all FDCsdemonstrated superiority, with probabilities ofimproved outcomes of [99% (ESM Table S7).
However, the probabilities of improvementversus TIO for the open dual therapies [TIO 18OD ? salmeterol (SAL) 50 BID (TIO ? SAL) andTIO 18 ? FOR 12] were lower (61% and 56%,respectively).
Comparing the combination therapies, theOD FDCs (UMEC/VI, TIO/OLO, and GLY/IND110/50) showed the greatest improvementsversus placebo and had high probabilities(C85%) of improved outcomes versus the othertherapies (TIO ? SAL, TIO 18 ? FOR 12, andACL/FOR). Between the OD FDCs, UMEC/VIhad a high probability of improved outcomesversus TIO/OLO (96%; mean difference23.74 mL; 95% CrI -3.31 to 50.73) and versusGLY/IND 110/50 (84%; mean difference13.87 mL; 95% CrI -12.98 to 41.33) (ESMTable S7).
Results using data without imputed SEs weresimilar to the base case results, with only smalldifferences (\5 mL) in changes in FEV1 for allcomparisons (data not shown). Results of thescenario analysis (separating TIO 18 and TIO 5)were in line with the base case results, althoughthe probability of improved outcomes withACL/FOR versus TIO 5 was lower (75%; meandifference 12.57 mL; 95% CrI -22.83 to 49.43)than for the comparison with TIO 5 or 18([99%; mean difference 27.33 mL; 95% CrI 5.65to 48.95).
NMA Results: HRQoL Assessed Using SGRQTotal Score
12 WeeksThe base case analysis results at 12 weeksshowed that all active therapies achievedimprovements in HRQoL, as shown by decrea-ses in the SGRQ total score, versus placebo, withprobabilities of improved outcomes of [99%(Table 1). These decreases were clinically rele-vant (greater than the MCID of 4 units [40]) forthe combination therapies, with the exceptionof TIO 18 ? FOR 12. In comparison with TIO, alltherapies showed improvements in HRQoL,with decreases in the SGRQ score of \4 unitsand probabilities of improved outcomes of[99%, with the exception of TIO 18 ? FOR 12(probability of an improved outcome 75%;
306 Pulm Ther (2017) 3:297–316

mean difference -1.01 units; 95% CrI -3.94 to1.89) (ESM Table S8).
Comparing the combination therapies, theprobabilities of improved outcomes using theFDCs (TIO/OLO, both doses of GLY/IND, andUMEC/VI) and the open dual combinationTIO ? OLO versus TIO 18 ? FOR 12 were rela-tively high (C68%). Reductions in the SGRQscore were similar between all FDCs andTIO ? OLO, with the probabilities of improvedoutcomes for comparisons ranging from 38% to57% (ESM Table S8).
Results with data without imputed SEs weregenerally similar to the base case results, withrelatively small differences (\0.5 units) in
changes in the SGRQ score for most compar-isons except for those with GLY/IND 110/50, forwhich differences were greater (\1.1 units; datanot shown). Comparisons with TIO 18? FOR 12were not included as these data were obtained byimputation.
24 WeeksThe base case analysis results at 24 weeksshowed that all active therapies achievedimprovements in HRQoL, as shown by decrea-ses in the SGRQ total score, versus placebo, withprobabilities of improved outcomes of [99%;these decreases were clinically relevant([4 units) for GLY/IND 110/50 and UMEC/VI
a195.80 (174.80, 217.30),>99%
181.80 (162.50, 200.90),>99%
172.10 (152.70, 191.70),>99%
138.20 (117.90, 158.30),>99%
113.50 (76.33, 150.40),>99%
123.60 (39.40, 215.90),>99%
110.90 (102.90, 118.90),>99%
UMEC/VI 62.5/25
GLY/IND 110/50
TIO/OLO 5/5
ACL/FOR 400/12a
TIO 18 + FOR 12b
TIO 18 + SAL 50c
TIO 5 or 18
Mean difference (95% CrI) in CFB in trough FEV1 vs placebo (mL)0 50 100 150 200 250
c1.01 (0.66, 1.36),>99%
1.31 (1.03, 1.58),>99%
1.19 (0.87, 1.51),>99%
1.37 (0.98, 1.76),>99%
0.93 (0.41, 1.44),>99%
0.41 (−0.46, 1.27),82%
0.83 (0.65, 1.01),>99%
UMEC/VI 62.5/25
GLY/IND 110/50
TIO/OLO 5/5
ACL/FOR 400/12a
TIO 18 + FOR 12b
TIO 18 + SAL 50c
TIO 5 or 18
Mean difference (95% CrI) in TDI focal score vs placebo−0.5 0.0 0.5 1.0 1.5 2.0
d−1.13 (−1.86, −0.46),>99%
−1.09 (−2.07, −0.12),98%
−1.28 (−2.52, −0.12),98%
−0.66 (−1.75, 0.44),92%
−0.65 (−1.26, −0.11),99%
UMEC/VI 62.5/25
GLY/IND 110/50
TIO/OLO 5/5
ACL/FOR 400/12a
TIO 5 or 18
Mean difference (95% CrI) in CFB in rescue medication use vs placebo (puffs/day)
−3 −2 −1 0 1
b−4.11 (−5.23, −2.99),>99%
−4.29 (−5.34, −3.23),>99%
−3.76 (−4.92, −2.60),>99%
−2.80 (−4.37, −1.22),>99%
−4.00 (−5.42, −2.59),>99%
−3.18 (−5.46, −0.89),>99%
−2.53 (−2.94, −2.12),>99%
UMEC/VI 62.5/25
GLY/IND 110/50
TIO/OLO 5/5
ACL/FOR 400/12a
TIO 18 + SAL 50c
TIO 18 + FOR 10b
TIO 5 or 18
Mean difference (95% CrI) in CFB in SGRQ total score vs placebo−7.5 −5.0 −2.5 0.0
Fig. 4 Forest plots showing differences for active treat-ments versus placebo in outcomes at 24 weeks. a CFBmean trough FEV1, b CFB mean SGRQ total score,c mean TDI focal score, d CFB mean rescue medicationuse (puffs/day). Results are reported as the mean with the95% credible interval (Crl) in parenthesis, followed by thepercentage probability of improved outcome versusplacebo. Black dotted lines represent MCID values. aCom-bined dose taken twice daily, bFOR dose taken twice daily,
cSAL dose taken twice daily. All other doses are taken oncedaily. ACL aclidinium, CFB change from baseline, CrIcredible interval, FEV1 forced expiratory volume in1 second, FOR formoterol, GLY glycopyrronium, INDindacaterol, MCID minimal clinically important differ-ence, OLO olodaterol, SAL salmeterol, SGRQ St George’sRespiratory Questionnaire, TDI transition dyspnea index,TIO tiotropium, UMEC umeclidinium, VI vilanterol
Pulm Ther (2017) 3:297–316 307

only (Table 1; Fig. 4b). In comparison with TIO,all therapies showed improvements in HRQoL,with decreases in the SGRQ score of \4 units;the probability of improved outcomes wasC98% for all therapies except for TIO 18? FOR 10 (71%; mean difference -0.64 units;95% CrI -2.93 to 1.64) and ACL/FOR (63%;mean difference -0.27 units; 95% CrI -1.89to 1.36) (ESM Table S9).
Comparing the combination therapies,TIO ? SAL and the OD FDCs (TIO/OLO,GLY/IND 110/50, and UMEC/VI) showed rela-tively high probabilities of improved outcomesversus ACL/FOR (C83%) and TIO 18 ? FOR 10(C68%). Improvements using TIO ? SAL andthe FDCs were similar, although relatively highprobabilities of improved outcomes were shownversus TIO/OLO with GLY/IND 110/50 (76%;mean difference -0.53 units; 95% CrI -2.00 to0.95) and UMEC/VI (67%; mean difference-0.35 units; 95% CrI -1.87 to 1.17).
Results with data without imputed SEs weregenerally similar to the base case results, withsmall differences (\0.2 units) in changes in theSGRQ score for most comparisons except thosewith ACL/FOR, for which differences were greater(\2.3 units; data not shown). With non-imputeddata, the probabilities of improvement usingACL/FOR were considerably lower versus placebo(70%; mean difference -0.65 units; 95% CrI-3.07 to 1.80), TIO (8%; mean difference 1.78units; 95% CrI -0.68 to 4.25) and all othercombination therapies (\1–6%) than with impu-ted data. These differences are due to the inclu-sion of only a single trial reporting outcomes withACL/FOR versus placebo in the non-imputed data(the ACLIFORM trial [41]) which reported a meanchange from baseline in the SGRQ score of -0.65units; however, the base case analysis also inclu-ded the AUGMENT trial [42], which reported aconsiderably larger mean change from baseline of-4.36 units.
NMA Results: Breathlessness Assessedby TDI Focal Score
12 WeeksThe base case analysis results at 12 weeksshowed that all active therapies achieved
increases in TDI focal score versus placebo withprobabilities of improved outcomes of C96%(Table 1). These increases were clinically rele-vant (greater than the MCID of 1.0 unit [43]) forthe FDCs (TIO/OLO, both GLY/IND doses, andUMEC/VI) but not for TIO alone or TIO 18? FOR 12. In comparison with TIO, the FDCsshowed increases in the TDI focal score of\1.0unit, with high probabilities of improved out-comes (C96%), while the probability of animproved outcome with TIO 18 ? FOR 12 waslower (56%; mean difference 0.07 units; 95%CrI -0.88 to 1.02) (ESM Table S10).
Comparing the combination therapies, theFDCs showed high probabilities of improvedoutcomes (C77%) versus the only open dualtherapy assessed (TIO 18 ? FOR 12). TIO/OLOshowed a high probability of improvementversus UMEC/VI (80%); the probability ofimprovement was also high versus UMEC/VI forGLY/IND 27.5/15.6 (86%) but was lower forGLY/IND 110/50 (61%) (ESM Table S10). Noimputation analysis was necessary for thesedata.
24 WeeksThe base case analysis results at 24 weeks showedthat all active therapies achieved increases in TDIfocal score versus placebo; the probability ofimproved outcomes was[99% for all therapiesexcept TIO ? SAL (82%; mean difference 0.41units; 95% CrI -0.46 to 1.27) (Table 1; Fig. 4c).These improvements were clinically relevant([1.0 unit) for the FDCs (TIO/OLO, GLY/IND110/50, ACL/FOR, and UMEC/VI) but not forTIO alone or in open dual combination therapy.In comparison with TIO, the FDCs showedincreases in TDI focal score of \1.0 unit, withhigh probabilities of improved outcomes(C85%); the probabilities with open dual com-binations were lower (65% for TIO 18? FOR 12;16% for TIO? SAL) (ESM Table S11).
Comparing the combination therapies, theFDCs and TIO 18 ? FOR 12 all showed highprobabilities (C85%) of improved outcomesversus TIO ? SAL. ACL/FOR and GLY/IND110/50 showed high probabilities of improvedoutcomes versus TIO 18 ? FOR 12 (91%; meandifference 0.44 units; 95% CrI -0.21 to 1.09;and 96%; mean difference: 0.38 units; 95% CrI:
308 Pulm Ther (2017) 3:297–316

-0.06 to 0.82, respectively). ACL/FOR andGLY/IND 110/50 also showed high probabilitiesof improved outcomes versus UMEC/VI (91%and 92%, respectively) (ESM Table S11).
Results with data without imputed SEs weresimilar to the base case results, with only smalldifferences (B0.08 units) in changes in TDIscore for all comparisons (data not shown).With non-imputed data, the probabilities ofimprovement using ACL/FOR were slightlylower versus TIO (94%; mean difference 0.48units; 95% CrI -0.12 to 1.07) and all combi-nation therapies (49–96%) than with imputeddata.
NMA Results: Puffs/day of RescueMedication
12 WeeksThe base case analysis results at 12 weeksshowed that all active therapies achieveddecreases in rescue medication use versus pla-cebo, with probabilities of improved outcomesof C93% (Table 1). In comparison with TIO,combination therapies showed decreases inrescue medication use; the probabilities ofimproved outcomes were[99% for all therapiesexcept TIO 18 ? FOR 12 (78%; mean difference-0.25 puffs/day; 95% CrI -0.87 to 0.37) (ESMTable S12).
Comparing the combination therapies,TIO ? IND and the FDCs (TIO/OLO, GLY/IND27.5/15.6, and UMEC/VI) showed high proba-bilities of improved outcomes (C82%) versusTIO 18 ? FOR 12. TIO ? IND showed a highprobability of improvement versus TIO/OLO(88%), while both TIO ? IND and GLY/IND27.5/15.6 showed high probabilities ofimprovement versus UMEC/VI (98% and 94%,respectively) (ESM Table S12). However, a sub-sequent direct comparison of TIO ? IND withUMEC/VI found no significant difference inrescue medication use [44].
Results with data without imputed SEs hadno differences from the base case results (datanot shown). Comparisons with TIO 18 ? FOR12 and TIO/OLO were not included as thesedata were obtained by imputation.
24 WeeksThe base case analysis results at 24 weeksshowed that all active therapies achieveddecreases in rescue medication use versus pla-cebo with probabilities of improved outcomesC92% (Table 1; Fig. 4d). In comparison withTIO, the OD FDCs (TIO/OLO, GLY/IND 110/50,and UMEC/VI) showed decreases in rescuemedication use with high probabilities (C87%)of improved outcomes; the probability ofimprovement with ACL/FOR was lower (51%;mean difference -0.01 puffs/day; 95% CrI-1.22 to 1.26).
Comparing the combination therapies, theOD FDCs showed relatively high probabilities ofimproved outcomes (C78%) versus ACL/FOR.Reductions in rescue medication use were sim-ilar between the OD FDCs, with the probabili-ties of improved outcomes for comparisonsranging from 34% to 55% (ESM Table S13).
Results with data without imputed SEs weresimilar to the base case results, with small dif-ferences (B0.2 puffs per day) in changes inrescue medication use for all comparisons. Theprobability of an improved outcome usingGLY/IND 110/50 versus TIO was higher ([99%;mean difference -0.51 puffs/day; 95% CrI-0.91 to -0.10) than with imputed data.Comparisons with ACL/FOR and TIO/OLOwere not included.
Subgroup Analysis
The relative effects of different therapies ontrough FEV1 at 12 and 24 weeks were assessed insubgroups of patients using and not using ICS,and in those with moderate disease or severe/very severe disease. Due to the limited dataavailable for these subgroups, only some thera-pies could be compared. Differences in troughFEV1 at 24 weeks in favor of dual combinations[TIO 18 ? FOR 12 and the FDCs (TIO/OLO,GLY/IND 110/50 and UMEC/VI)] versus placebowere greater for patients without ICS use (range162–280 mL) than for patients with ICS use(range 118–180 mL; ESM Table S14) and forpatients with moderate disease (range147–276 mL) than patients with severe disease
Pulm Ther (2017) 3:297–316 309

(58–119 mL; ESM Table S15). The probabilitiesof improved outcomes using TIO/OLO orUMEC/VI versus TIO 18 ? FOR 12, andUMEC/VI versus TIO/OLO or GLY/IND 110/50,were higher in subgroups without ICS use andin those with moderate disease than in thosewith ICS use and with severe disease, respec-tively. However, the probabilities of improvedoutcomes using TIO 18 ? FOR 12 versus TIOand GLY/IND 110/50 versus TIO/OLO werehigher in subgroups with ICS use and withsevere disease than in patients without ICS useor those with moderate disease, respectively.
DISCUSSION
In this study, the relative efficacy ofLAMA? LABA combination bronchodilators wasevaluated in patients with moder-ate-to-very-severe COPD using data from 44RCTs on four outcomes of interest reported at 12and/or 24 weeks after randomization: troughFEV1, SGRQ total score, TDI focal score, and dailyrescue medication use. These outcomes wereselected in accordance with the bulk of availabledata for RCTs involving dual bronchodilators.
Clinically relevant improvements wereobserved versus placebo over the 12- and/or24-week time frame in trough FEV1 (improve-ments of C100 mL [39]), SGRQ total score (im-provements of C4 units [40]), and TDI focalscore (improvements of C1 unit [43]) with allFDC therapies, with the exception of TIO/OLOand ACL/FOR, both of which failed to showclinically relevant improvements in SGRQ totalscore at 24 weeks. Although no MCID has beenestablished for rescue medication use,improvements were observed with all FDCsversus placebo at 12 and 24 weeks, with proba-bilities of improved outcomes of C92%. Withopen dual combinations of TIO with LABAtherapies, improvements were observed versusplacebo in all outcomes, but while improve-ments in trough FEV1 were clinically relevant,the magnitudes of treatment benefits for thePROs of SGRQ total score and TDI focal scorewere often below clinically relevant thresholds.These results are not surprising given the his-torical emphasis on improving lung function in
the development of therapies for COPD [45].The findings suggest that there may be a greaterlikelihood of a clinically important patientresponse with FDC bronchodilators comparedwith open dual regimens, particularly whencomparing once- versus twice-daily treatments.To the best of our knowledge, comparativeoutcomes between FDCs and open dual com-binations have not been assessed in otherNMAs, and direct evidence in support of thisclaim is available from only one 6-month RCTthat reported improvements in pre-bron-chodilator FEV1 and forced vital capacity, and asignificantly higher percentage of patientsachieving a clinically relevant improvement inTDI, using GLY/IND 110/50 compared with TIO18 ? FOR 12 [46].
Once-daily FDCs showed consistentimprovements versus TIO monotherapy in lungfunction, HRQoL, and rescue medication useafter 12 and 24 weeks of treatment, with prob-abilities of better outcomes of C87% in all cases.However, less certainty of improvement wasapparent with FDCs or open dual combinationscontaining FOR or SAL taken twice daily. Whenthe TDI focal score was examined, improve-ments were observed with all FDCs versus TIOat 12 and 24 weeks, with probabilities ofimprovement of C85%, while the probability ofimprovement using open dual combinationswas lower (16–65%). In contrast to improve-ments in trough FEV1 and SGRQ total score, nopotential for efficacy differences emergedbetween once- or twice-daily regimens for theTDI assessments. The improvements observedusing LAMA ? LABA combination therapycompared with TIO monotherapy are consistentwith results from several RCTs which directlycompared various LAMA ? LABA therapies withTIO [14–20]. This observation is therefore notunexpected and could be attributed to thedirect agonist effect of the added LABA, as wellas possible synergistic effects [13]. Some RCTshave reported improved lung function out-comes using LAMA ? LABA therapies comparedwith LABA monotherapy; [15–17] these findingsare consistent with the conclusions of tworecent NMAs, which performed slightly differ-ent analyses to that presented in this study[47, 48].
310 Pulm Ther (2017) 3:297–316

It was notable that for most dual bron-chodilators assessed at both time points, agreater magnitude of benefit in TDI focal scoreand SGRQ total score was observed at 12 com-pared with 24 weeks, but this diminution ofresponse with time was not consistentlyobserved for FEV1 and rescue medication use.This result may indicate that some PROs may bemore subject to recall bias, as patients arerequired to recall their previous state in order toestimate changes [49], making them potentiallyless effective in discriminating between differ-ent active therapies over time, and suggests thatshorter assessments may be more reliable forwithin-class comparisons. However, alternativeapproaches, such as comparing responder ratesbetween two regimens, which has previouslyidentified efficacy differences between dualbronchodilators, may be equally valid [46].
In this study, improvements in SGRQ totalscore and TDI focal score were never greaterthan the proposed MCIDs of 4 units [40] and1 unit [43], respectively, when comparisonswere made between active regimens. This find-ing highlights that dual combination therapywas associated with an incremental efficacygain in PROs compared with standard of caremonotherapy, a finding concordant with thatreported in other meta-analyses comparingFDCs with their individual component LAMAor LABAs [47, 48]. By contrast, the magnitude oflung function benefit using FDCs comparedwith placebo was often twofold higher thanthat seen with TIO monotherapy. The currentNMA identified a potential gradient of effec-tiveness emerging between the once-daily FDCsand those including twice-daily LABAs, partic-ularly with regards to improvements in troughFEV1: at 12 weeks, GLY/IND and UMEC/VIdemonstrated the greatest improvements, fol-lowed by TIO ? IND, while improvements withACL/FOR, TIO/OLO, TIO ? OLO, and TIO 18? FOR 10 were lower; at 24 weeks, UMEC/VIdemonstrated the greatest improvement,followed by GLY/IND, then TIO/OLO, withACL/FOR and the open dual combinationsshowing lower improvements. However, furthertrials are required to confirm these findings.Head-to-head trials of FDCs with results yet to bereported include two trials comparing GLY/IND
with UMEC/VI (NCT02487446 andNCT02487498) and one trial comparingUMEC/VI with TIO/OLO (NCT02799784).
It is worth noting that the effectiveness of aninhaled therapy could potentially be affected bythe delivery device used [50]. While severalinhaler types are available, dry powder inhalers(DPIs) have become increasingly common forCOPD therapies due to their multiple advan-tages over the more traditional pressurizedmetered-dose inhalers (pMDIs) [51]. However,different classes of DPIs are available, withongoing debate about their relative advantages[51]. Of the therapies assessed in this NMA,most were delivered by either single-dose DPIs(TIO 18, IND, FOR 12, and the combined ther-apy GLY/IND) or multi-dose DPIs (FOR 10 andthe combined therapies ACL/FOR and UMEC/VI).The exceptions were SAL, which was deliveredby a pMDI, and TIO 5, OLO, and TIO/OLO,which were delivered by soft mist inhalers [52].However, as the majority (40/44) of the studiesincluded in the NMA were blinded, it is unlikelythat these differences in inhaler type would bereflected in the results. Currently, while severalstudies have identified patient preferencesbetween different inhaler types [53–55], there islimited evidence to demonstrate any differencesin efficacy outcomes [56, 57]. Further research istherefore required to inform optimal devicedesign, improve compliance, reduce handlingerrors and, ultimately, improve outcomes.
This NMA is an updated extension of ourpreviousNMAcomparing the efficacyofUMEC/VIwith other dual bronchodilators, TIO, or pla-cebo [28]. The previous review included 26RCTs of C10 weeks’ duration, published inEnglish up to April 2014. The expanded inclu-sion criteria in this update allowed the inclu-sion of a further 18 RCTs and enabled analysisof additional combination bronchodilators(TIO ? OLO, TIO/OLO, GLY/IND 27.5/15.6, andACL/FOR); also, TIO 5 was not included as acomparator in the previous analysis. However,the principal observation of similar efficacybetween available combination bronchodilatorswith regards to PROs remained the same forboth analyses. Improvements in trough FEV1
using different combination therapies were lesssimilar; here, the magnitude of some of the
Pulm Ther (2017) 3:297–316 311

differences between therapies were beyondaccepted non-inferiority margins used forwithin-class comparisons (C50 mL or C50% ofthe proposed MCID [8, 58]). Scenario analysisseparating TIO 18 and TIO 5 showed that theaddition of TIO 5 to the analysis had a negligi-ble effect on measured outcomes. In this upda-ted NMA we also performed subgroup analysisto examine potential confounding due to dis-ease severity and concurrent therapy. Theresults highlight some additional differences inthe magnitudes of improvements in lung func-tion between therapies in patient subgroupswith differing capacities for bronchodilation.
Two other recent NMAs have examined thecomparative effects of available FDCs on lungfunction and PROs; neither included open dualcombination therapies [48, 59]. The NMA bySchlueter et al. included 27 RCTs of C20 weeks’duration, published up to September 2014, andassessed outcomes at 24 and 48 weeks [59]. RCTswere excluded based on concomitant treatments,and meta-regression rather than subgroup analy-sis was performed to assess the effects of baselinedisease severity and concomitant ICS use onoutcomes [59]. The NMA by Calzetta et al.included 22 RCTs of C3 months’ duration, pub-lished up to October 2015, and assessed outcomesfor FDC LAMA/LABA combinations versus theircomponent monotherapies when they werereported for each study; RCTs without compar-isons of the dual therapy to a componentmonotherapy were excluded [48]. Despite thedifferences in inclusion criteria and analysismethods, the results obtained in both NMAs wereconsistent with those for the current analysis.Both NMAs assessed differences in SGRQ totalscore and TDI focal score using the percentage ofresponders, rather than the calculated differencesin scores as in the present NMA; however, inaccordance with our results, neither study repor-ted any significant difference in these outcomesbetween FDCs [48, 59]. Both previous NMAsreported differences between the FDCs for troughFEV1. Schlueter et al. reported improvements withTIO/OLO, GLY/IND 110/50, and UMEC/VI abovethose seen with ACL/FOR that were of similarmagnitudes to the improvements observed in thepresent study at the same time point (approxi-mately 24 weeks) [59]. Calzetta et al. reported a
similar potential gradient of effectiveness to thatpresented here, with UMEC/VI and GLY/IND27.5/15.6 demonstrating the greatest improve-ments, followed by GLY/IND 110/50, TIO/OLO,then ACL/FOR [48].
A potential limitation of this and otherNMAs of FDC bronchodilators is the low num-ber of studies involving some treatments andthe scarcity of direct comparisons of these withother active treatments. In particular, of theFDCs, only two studies presenting data forACL/FOR were eligible for inclusion; both ofthese were ‘large’ trials (each with[300 patientsreceiving ACL/FOR [41, 42], considerablygreater than the previously proposed cut-off forlarge trials of 100 patients [60]), thereby reduc-ing the likelihood of any distortion of resultsdue to a small study effect [61]. However, theheterogeneity of the studies included in thisNMA was not assessed, so the extent of distor-tion is not known. Additionally, comparisons inthis study were frequently calculated indirectly,so there is some uncertainty in the estimatedefficacies. As with all meta-analyses, the poten-tial influence of confounders constitutes a lim-itation. Due to the low number of studiesinvolved, meta-regression to adjust for anyconfounders was infeasible, so subgroup analy-sis was performed. The greatest improvementsin lung function were observed in non-ICS usersand patients with moderate disease for allcombination therapies versus placebo. How-ever, it is still unclear whether any greatermagnitude of difference in lung functionbetween the therapies in these subgroups islikely to be matched by clinically importantchanges in PROs. Another limitation of thisstudy is that the outcomes analyzed wererestricted to those investigated in multiple RCTsof 12 or 24 weeks’ duration; other relevantendpoints that have been less commonly orinconsistently reported, such as exacerbationrate or time to first event in patients of varyingexacerbation risk, were excluded.
CONCLUSIONS
In an indirect treatment comparison using aBayesian NMA, most but not all dual
312 Pulm Ther (2017) 3:297–316

combination therapies showed improved out-comes versus placebo and versus TIOmonotherapy at 12 and/or 24 weeks. The like-lihood of improved outcomes appeared to begreater with FDCs compared with open dualcombinations. The relative probabilities ofimprovement between available FDCs suggestedbroadly similar efficacy when assessed using thePROs of SGRQ total score, TDI focal score, andrescue medication use, while some differencesbetween bronchodilators were observed forobjective assessments using trough FEV1. Whilehead-to-head RCTs would be required to pro-vide robust evidence of efficacy differencesbetween LAMA ? LABA bronchodilators, indi-rect comparisons such as the present NMA allowthe existing volume of RCT data to be employedto generate data which may be of use tohealthcare payers and providers.
ACKNOWLEDGEMENTS
This study was funded by GSK (study number:200167). The funders of the study had a role instudy design, data analysis, data interpretation,writing of the report, and payment of the articleprocessing charges. The corresponding authorhad full access to all the data and bears the finalresponsibility for submission of the study forpublication. The authors gratefully acknowl-edge Andreas Karabis for his contributions tothe study design, data acquisition, and analysis,and Patricia Guyot for her assistance in dataverification. Editorial assistance in the prepara-tion of this manuscript was provided by Eliza-beth Jameson, PhD, of Fishawack Indicia Ltd,UK and was funded by GSK. All named authorsmeet the International Committee of MedicalJournal Editors (ICMJE) criteria for authorshipfor this manuscript, take responsibility for theintegrity of the work as a whole, and have givenfinal approval to the version to be published.
Disclosures. YS Punekar is an employee ofGSK and hold stocks/shares in GSK. I Naya is anemployee of GSK and hold stocks/shares in GSK.AS Ismaila is an employee of GSK and holdstocks/shares in GSK. AS Ismaila is also an
unpaid faculty member at McMaster University.At the time of the study, KYJ Sion was anemployee of Mapi, who was contracted by GSKto provide data analysis for the study. At thetime of the study, EL Huisman was an employeeof Mapi, who was contracted by GSK to providedata analysis for the study. Authors from Mapiwere not paid for manuscript development.
Compliance with ethics guidelines. Thisarticle is based on a synthesis of previouslyconducted studies, and does not involve anynew studies of human or animal subjects per-formed by any of the authors.
Data availability. The datasets generatedand analyzed during the current study areavailable from the corresponding author onreasonable request.
Open Access. This article is distributedunder the terms of the Creative CommonsAttribution-NonCommercial 4.0 InternationalLicense (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercialuse, distribution, and reproduction in anymedium, provided you give appropriate creditto the original author(s) and the source, providea link to the Creative Commons license, andindicate if changes were made.
REFERENCES
1. Global Initiative for Chronic Obstructive LungDisease. Global Strategy for the Diagnosis, Man-agement and Prevention of Chronic ObstructivePulmonary Disease. Updated 2016. Available athttp://goldcopd.org. Accessed 17 Oct 2016.
2. Tashkin DP, Cooper CB. The role of long-actingbronchodilators in the management ofstable COPD. Chest. 2004;125(1):249–59.
3. Cazzola M, Page C. Long-acting bronchodilators inCOPD: where are we now and where are we going?Breathe. 2014;10(2):111–20.
4. Appleton S, Poole P, Smith BJ, et al. Long-actingbeta2-agonists for poorly reversible chronicobstructive pulmonary disease (Review). CochraneDatabase Syst Rev. 2006;3:CD001104. doi:10.1002/14651858.CD001104.pub2.
Pulm Ther (2017) 3:297–316 313

5. Man WD, Mustfa N, Nikoletou D, et al. Effect of sal-meterol on respiratory muscle activity during exercisein poorly reversible COPD. Thorax. 2004;59(6):471–6.
6. O’Donnell DE, Voduc N, Fitzpatrick M, Webb KA.Effect of salmeterol on the ventilatory response toexercise in chronic obstructive pulmonary disease.Eur Respir J. 2004;24(1):86–94.
7. Sin DD, McAlister FA, Man SF, Anthonisen NR.Contemporary management of chronic obstructivepulmonary disease: scientific review. JAMA.2003;290(17):2301–12.
8. Feldman G, Maltais F, Khindri S, et al. A random-ized, blinded study to evaluate the efficacy andsafety of umeclidinium 62.5 lg compared withtiotropium 18 lg in patients with COPD. Int JChron Obstr Pulm Dis. 2016;11:719–30.
9. Kerwin E, Hebert J, Gallagher N, et al. Efficacy andsafety of NVA237 versus placebo and tiotropium inpatients with COPD: the GLOW2 study. Eur RespirJ. 2012;40(5):1106–14.
10. O’Donnell DE, Fluge T, Gerken F, et al. Effects oftiotropium on lung hyperinflation, dyspnoea andexercise tolerance in COPD. Eur Respir J.2004;23(6):832–40.
11. Tashkin DP, Celli B, Senn S, et al. A 4-year trial oftiotropium in chronic obstructive pulmonary dis-ease. N Engl J Med. 2008;359(15):1543–54.
12. Dransfield MT, Bailey W, Crater G, Emmett A,O’Dell DM, Yawn B. Disease severity and symptomsamong patients receiving monotherapy for COPD.Prim Care Respir J. 2011;20(1):46–53.
13. Cazzola M, Molimard M. The scientific rationale forcombining long-acting beta2-agonists and mus-carinic antagonists in COPD. Pulm Pharmacol Ther.2010;23(4):257–67.
14. Tashkin DP, Pearle J, Iezzoni D, Varghese ST. For-moterol and tiotropium compared with tiotropiumalone for treatment of COPD. COPD.2009;6(1):17–25.
15. van Noord JA, Aumann JL, Janssens E, et al. Com-bining tiotropium and salmeterol in COPD: effectson airflow obstruction and symptoms. Respir Med.2010;104(7):995–1004.
16. Bateman ED, Ferguson GT, Barnes N, et al. Dualbronchodilation with QVA149 versus single bron-chodilator therapy: the SHINE study. Eur Respir J.2013;42(6):1484–94.
17. Decramer M, Anzueto A, Kerwin E, et al. Efficacyand safety of umeclidinium plus vilanterol versus
tiotropium, vilanterol, or umeclidiniummonotherapies over 24 weeks in patients withchronic obstructive pulmonary disease: results fromtwo multicentre, blinded, randomised controlledtrials. Lancet Respir Med. 2014;2(6):472–86.
18. Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M,Church A. Efficacy and safety of umeclidinium/vilanterol 62.5/25 mcg and tiotropium 18 mcg inchronic obstructive pulmonary disease: results of a24-week, randomized, controlled trial. Respir Med.2014;108(12):1752–60.
19. Tashkin DP, Ferguson GT. Combination bron-chodilator therapy in the management of chronicobstructive pulmonary disease. Respir Res.2013;14:49.
20. van der Molen T, Cazzola M. Beyond lung functionin COPD management: effectiveness of LABA/LAMA combination therapy on patient-centredoutcomes. Prim Care Respir J. 2012;21(1):101–8.
21. Novartis. Ultibro� Breezhaler� Summary of ProductCharacteristics. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002679/WC500151255.pdf. Accessed 24 Oct 2016.
22. Novartis. UTIBRONTM
NEOHALER�. Highlights ofprescribing information. Available at https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/207930s000lbl.pdf. Accessed 24 Oct 2016.
23. GlaxoSmithKline. ANOROTM ELLIPTA�. Summary ofproduct characteristics. Available at http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002751/WC500168424.pdf. Accessed 24 Oct 2016.
24. GlaxoSmithKline. ANOROTM ELLIPTA�. Highlightsof prescribing information. Available at http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/203975s000lbl.pdf. Accessed 24 Oct 2016.
25. AstraZeneca. Duaklir� Genuair�. Summary ofProduct Characteristics. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003745/WC500178413.pdf. Accessed 24 Oct 2016.
26. Boehringer Ingelheim. Spiolto� Respimat�. Sum-mary of Product Characteristics. Available athttps://www.spiolto.com/public/assets/spiolto_spc_published.pdf. Accessed 24 Oct 2016.
27. Boehringer Ingelheim. Stiolto� Respimat�. High-lights of prescribing information. Available at http://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Stiolto%20Respimat/stiolto.pdf.Accessed 24 Oct 2016.
314 Pulm Ther (2017) 3:297–316

28. HuismanEL,CockleSM, IsmailaAS,KarabisA,PunekarYS. Comparative efficacy of combination bron-chodilator therapies in COPD: a network meta-analy-sis. Int J Chron Obstr Pulm Dis. 2015;10:1863–81.
29. Higgins JPT, Green S, editors. Cochrane Handbookfor Systematic Reviews of Interventions Version5.1.0. Updated March 2011. Available at http://handbook.cochrane.org. Accessed 5 Oct 2015.
30. Institute for Quality and Efficiency in Healthcare(Institut fur Qualitat und Wirtschaftlichkeit imGesundheitswesen). Dossier zur Nutzenbewertunggemaß § 35a SGB V. 2013. Available at https://www.g-ba.de/downloads/17-98-3528/2013-04-18_Anl2_6_Modul4.pdf. Accessed 3 Oct 2016.
31. Caldwell DM, Ades AE, Higgins JP. Simultaneouscomparison of multiple treatments: combiningdirect and indirect evidence. BMJ. 2005;331(7521):897–900.
32. Jansen JP, Crawford B, Bergman G, Stam W. Baye-sian meta-analysis of multiple treatment compar-isons: an introduction to mixed treatmentcomparisons. Value Health. 2008;11(5):956–64.
33. Lu G, Ades AE. Combination of direct and indirectevidence in mixed treatment comparisons. StatMed. 2004;23(20):3105–24.
34. Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSUTechnical Support Document 2: a generalised linearmodelling framework for pairwise and networkmeta-analysis of randomised controlled trials. 2011.Available at http://www.nicedsu.org.uk/TSD2%20General%20meta%20analysis%20corrected%202Sep2016v2.pdf. Accessed 4 Oct 2015.
35. Wedzicha JA, Decramer M, Ficker JH, et al. Analysis ofchronic obstructive pulmonary disease exacerbationswith the dual bronchodilator QVA149 comparedwith glycopyrronium and tiotropium (SPARK): arandomised, double-blind, parallel-group study. Lan-cet Respir Med. 2013;1(3):199–209.
36. Wise RA, Anzueto A, Cotton D, et al. Tiotropiumrespimat inhaler and the risk of death in COPD.N Engl J Med. 2013;369(16):1491–501.
37. Cope S, Donohue JF, Jansen JP, et al. Comparativeefficacy of long-acting bronchodilators for COPD: anetwork meta-analysis. Respir Res. 2013;14:100.
38. Anzueto A, Wise R, Calverley P, et al. The Tio-tropium Safety and Performance in Respimat�
(TIOSPIR�) trial: spirometry outcomes. Respir Res.2015;16:107.
39. Donohue JF. Minimal clinically important differencesin COPD lung function. COPD. 2005;2(1):111–24.
40. Jones PW. St. George’s respiratory questionnaire:MCID. COPD. 2005;2(1):75–9.
41. Singh D, Jones PW, Bateman ED, et al. Efficacy andsafety of aclidinium bromide/formoterol fumaratefixed-dose combinations compared with individualcomponents and placebo in patients with COPD(ACLIFORM-COPD): a multicentre, randomisedstudy. BMC Pulm Med. 2014;14:178.
42. D’Urzo AD, Rennard SI, Kerwin EM, et al. Efficacyand safety of fixed-dose combinations of aclidiniumbromide/formoterol fumarate: the 24-week, ran-domized, placebo-controlled AUGMENT COPDstudy. Respir Res. 2014;15:123.
43. Mahler DA, Witek TJ Jr. The MCID of the transitiondyspnea index is a total score of one unit. COPD.2005;2(1):99–103.
44. Kalberg C, O’Dell D, Galkin D, Newlands A, FahyWA. Dual bronchodilator therapy with umecli-dinium/vilanterol versus tiotropium plus inda-caterol in chronic obstructive pulmonary disease: arandomized controlled trial. Drugs R&D.2016;16(2):217–27.
45. U.S. Food and Drug Administration. Chronicobstructive pulmonary disease: developing drugsfor treatment-guidance for industry. 2016. Avail-able at https://www.fda.gov/downloads/drugs/guidances/ucm071575.pdf. Accessed 24 May 2017.
46. Buhl R, Gessner C, Schuermann W, et al. Efficacyand safety of once-daily QVA149 compared withthe free combination of once-daily tiotropium plustwice-daily formoterol in patients with moder-ate-to-severe COPD (QUANTIFY): a randomised,non-inferiority study. Thorax. 2015;70(4):311–9.
47. Oba Y, Sarva ST, Dias S. Efficacy and safety oflong-acting beta-agonist/long-acting muscarinicantagonist combinations in COPD: a networkmeta-analysis. Thorax. 2016;71(1):15–25.
48. Calzetta L, Rogliani P, Matera MG, Cazzola M. Asystematic review with meta-analysis of dual bron-chodilation with LAMA/LABA for the treatment ofstable COPD. Chest. 2016;149(5):1181–96.
49. Glaab T, Vogelmeier C, Buhl R. Outcome measuresin chronic obstructive pulmonary disease (COPD):strengths and limitations. Respir Res. 2010;11:79.
50. Bonini M, Usmani OS. The importance of inhalerdevices in the treatment of COPD. COPD Res Pract.2015;1:9.
51. Dal Negro RW. Dry powder inhalers and the rightthings to remember: a concept review. MultidiscipRespir Med. 2015;10(1):13.
Pulm Ther (2017) 3:297–316 315

52. Anderson P. Use of respimat soft mist inhaler inCOPD patients. Int J Chron Obstr Pulm Dis.2006;1(3):251–9.
53. Dal Negro RW, Povero M. Acceptability and pref-erence of three inhalation devices assessed by thehandling questionnaire in asthma and COPDpatients. Multidiscip Respir Med. 2016;11:7.
54. Komase Y, Asako A, Kobayashi A, Sharma R.Ease-of-use preference for the ELLIPTA� drypowder inhaler over a commonly used single-dosecapsule dry powder inhaler by inhalation devi-ce-naive Japanese volunteers aged 40 years orolder. Int J Chron Obstruct Pulmon Dis.2014;9:1365–75.
55. Pascual S, Feimer J, De Soyza A, et al. Preference,satisfaction and critical errors with Genuair andBreezhaler inhalers in patients with COPD: a ran-domised, cross-over, multicentre study. NPJ PrimCare Respir Med. 2015;25:15018.
56. Chrystyn H, van der Palen J, Sharma R, et al. Deviceerrors in asthma and COPD: systematic literaturereview and meta-analysis. NPJ Prim Care RespirMed. 2017;27(1):22.
57. Ninane V, Vandevoorde J, Cataldo D, et al. Newdevelopments in inhaler devices within pharma-ceutical companies: a systematic review of theimpact on clinical outcomes and patient prefer-ences. Respir Med. 2015;109(11):1430–8.
58. Chapman KR, Beeh KM, Beier J, et al. A blindedevaluation of the efficacy and safety of glycopyrro-nium, a once-daily long-acting muscarinic antago-nist, versus tiotropium, in patients with COPD: theGLOW5 study. BMC Pulm Med. 2014;14:4.
59. Schlueter M, Gonzalez-Rojas N, Baldwin M,Groenke L, Voss F, Reason T. Comparative efficacyof fixed-dose combinations of long-acting mus-carinic antagonists and long-acting beta2-agonists:a systematic review and network meta-analysis.Ther Adv Respir Dis. 2016;10(2):89–104.
60. Nuesch E, Trelle S, Reichenbach S, et al. Small studyeffects in meta-analyses of osteoarthritis trials:meta-epidemiological study. BMJ. 2010;341:c3515.
61. Sterne JA, Gavaghan D, Egger M. Publication andrelated bias in meta-analysis: power of statisticaltests and prevalence in the literature. J Clin Epi-demiol. 2000;53(11):1119–29.
316 Pulm Ther (2017) 3:297–316