A Multistate Study of Etiology in Infants Identified through Universal Newborn Hearing Screening...
29
A Multistate Study of Etiology in Infants Identified through Universal Newborn Hearing Screening Karin M. Dent, MS, CGC John C. Carey, MD, MPH University of Utah Division of Medical Genetics Department of Pediatrics
-
Upload
savannah-newman -
Category
Documents
-
view
212 -
download
0
Transcript of A Multistate Study of Etiology in Infants Identified through Universal Newborn Hearing Screening...

A Multistate Study of Etiology in Infants Identified
through Universal Newborn Hearing
Screening
Karin M. Dent, MS, CGCJohn C. Carey, MD, MPHUniversity of UtahDivision of Medical GeneticsDepartment of Pediatrics

Congenital Hearing Loss
Birth Prevalence:
–1 in 300 - 1 in 500 births
– includes mild to profound, unilateral and bilateral CHL
http://www.iurc.montp.inserm.fr/cric/audition/english/start2.htm

Congenital Hearing Loss
Rate per 1,000 of Permanent Congenital Hearing Loss in Published Reports of UNHS Programs
Location of Program Cohort Size Prevalence per 103
New Jersey, 1997 15,749 3.30
New York, 2000 27, 938 1.96
Colorado, 1998 41,976 2.56
Texas, 1998 54,228 2.15
Hawaii, 1997 9,605 4.15
Estimate = 2- 4 / 1000

I ≈ 1/500
Environmental ~50%
aminoglycosides infections (bacterial or viral) trauma
Genetic ~50%
Syndromic ~30%
Branchiootorenal (BOR) CHARGE Syndrome
Nonsyndromic ~70%
Autosomal Dominant 20%
Autosomal Recessive 80%
X-linked ~1%
Mitochondrial <1%
Modified from www.ACMG.net

Genetics of Hearing Loss
Nonsyndromic Human Hearing Loss Genes*Nonsyndromic Human Hearing Loss Genes*
DFNA - Autosomal Dominant– 54 Loci Mapped 54 Loci Mapped
DFNB - Autosomal Recessive– DFNB1 = DFNB1 = GJB2GJB2– 51 Loci Mapped 51 Loci Mapped
DFN - X-Linked– 7 Loci Mapped7 Loci Mapped
Syndromic Hearing Loss Genes 30 single genes known
*50% have been identified Hereditary Hearing Loss web page: www.uia.ac.be/dnalab/hhhwww.uia.ac.be/dnalab/hhh

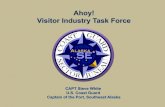
Genetic Causes of Hearing Loss:
Contribution of Cx26
DFNB1 = GJB2 (Connexin 26)
– 50% of DFNB - mutations of 50% of DFNB - mutations of GJB2GJB2 or Connexin 26 or Connexin 26
~15% of congenital hearing loss – Cx26 mutations
Genetic ~50%
Syndromic ~30%
Nonsyndromic ~70%
Dominant 20%
Recessive 80%
X-linked ~1%
Mt <1%

GJB2 / Connexin 26 gene
Mechanism
– Expressed in the cochlea– Membrane protein
forming intracellular channels =Gap Junction protein A / B
– Allows recirculation
of ions (K+)
Nature Genetics, February 2001.

Connexin 26 / GJB2
>80 mutations identified
35 del G (formerly del 30)– Carrier freq ≈ 3.5% CaucasiansCarrier freq ≈ 3.5% Caucasians
167 del T– Carrier freq ≈ 4% Ashkenazi JewishCarrier freq ≈ 4% Ashkenazi Jewish
235 del C– Seen in Asian populationsSeen in Asian populations
*M34T– Carrier freq ≈ 2-3% CaucasiansCarrier freq ≈ 2-3% Caucasians– Hypothesized as recessive alleleHypothesized as recessive allele
← GJB2
Chromosome 13Kenneson et al., Genet Med, 2002

Study Development
Universal Newborn Hearing Screening
+
Advances in Genetics of Hearing Loss
=
Prospective study of etiology of congenital hearing loss
• Utah, Hawaii, Rhode Island, and the Centers for Disease Control and Prevention

Study Objectives
To determine the etiology of congenital hearing loss based on children identified through a statewide newborn hearing screening (EHDI) program
– To evaluate all children with permanent hearing loss, unilateral or bilateral, of any degree, from a genetic perspective
– To determine the frequency of GJB2 and mitochondrial mutations in this population

Study Objectives cont…
To establish a model infrastructure linking genetic services to statewide newborn hearing screening

Hypothesis
The majority of infants identified through the newborn hearing screening program will have hearing loss due to various genetic causes including known syndromes and mutations in the GJB2 gene.

STUDY DESIGN and FLOW
Decline to participate
No evidence of syndrome
Identified Case Fails screens, enters database
Send letter inviting participation in study
Genetic Evaluation: Determination of syndrome,
pedigree analysis
Acquired cause (e.g. CMV) Syndromic
(e.g. Waardenburg, CHARGE, etc.)
Offer GJB2, mitochondrial testing

Nonsyndromic hearing loss
Autosomal dominant or Autosomal recessive
inheritanceSporadic
X-linked or maternal inheritance
Offer GJB2 and mitochondrial testing
POSITIVE NEGATIVE
Summarize and classify case Refer for ophthalmology,
EKG (?), etc., through PCP
Offer additional genetic counseling and family member
referrals
GJB2 het
GJB6 testing
LVA
Pendred studies

Results
93 Probands (primarily Caucasian / N. European, Hispanic)
20 cases from RI 73 cases from UT
– 19 syndromic cases19 syndromic cases
– 1 cases acquired hearing loss1 cases acquired hearing loss CMV induced
– 73 cases non-syndromic73 cases non-syndromic

Results cont…
Syndromic cases (19)Syndromic cases (19)
- Williams syndrome- Wolf-Hirschhorn (4p-)- CHARGE syndrome- 18q deletion syndrome- Kabuki syndrome- 22q deletion syndrome- 10p trisomy syndrome- Wildervank
- Trisomy 21- Waardenburg x 2- Oculoauriculovertebral - VATER- Branchiootorenal (BOR)- Pendred- MCA x 4

Results cont…
Nonsyndromic Cases (73)
– 8 cases Conductive8 cases Conductive isolated microtia, meatal atresia
– 65 cases Sensorineural65 cases Sensorineural53 Bilateral
12 Unilateral
13 Familial
52 Sporadic• 1 adopted

DNA Testing Results
of 53 Bilateral Non-syndromic SNHL:
GJB2 Results (12) 35 del G / 35 del G homozygote (3)
L 90 P / 35 del G cmpd heterozygote
35 del G / 358 del GAG cmpd heterozygote
35 del G heterozygote (3)
L 90 P heterozygote
S 193 N heterozygote
M 34 T heterozygote (2)

DNA Testing Results
GJB6 Results no mutations found (RI, n = 20)
Mitochondrial DNA Resultsno mutations found

Summary
93 probands– 73 nonsyndromic
65 sensorineural hearing loss
– 53 bilateral, sensorineural hearing loss
12 / 53 (23%) have GJB2 variant
5 / 53 (9.4%) 35 del G homozygotes or compound heterozygotes

Risk Factors for Hearing Loss
Prematurity (<37 wks gestation), jaundice, aminoglycoside exposure, external ear defects, family history of hearing loss

Risk Factors
Utah:
4 patients with prematurity
(1 of 4 w/ aminoglycoside X)
1 pt aminoglycoside exp (full term pgcy)
8 pts microtia
11 familial pts
TOTAL = 24 (of 73 probands)
Rhode Island:
3 patients with prematurity and aminoglycoside exp
2 familial pts
Others with jaundice, aminoglycoside exposure, and non-isolated microtia
TOTAL > 5 (of 20 probands)

Conclusions
Frequency of GJB2 mutations in this population is consistent with reported estimates
Identification of the etiology of hearing loss allows for accurate genetic counseling in terms of recurrence risk, natural history, and anticipatory guidance.

Conclusions
Incorporation of genetic services into newborn screening programs for hearing loss is beneficial for families.
Majority of newborns identified through universal screening had no clinical risk factors for hearing loss.

Future Directions
Ascertainment (All)– pt evaluations in outreach clinics– website– parent brochure– Spanish literature
DNA Testing (Utah and Hawaii)– Connexin 30 testing– Pendrin testing

Contributors - Hawaii
Patricia Heu, MDPrincipal Investigator
Sylvia Au, MS, CGCState Genetics Coordinator
Genetic Counselors
Allison Taylor, MS Lianne Hasagawa, MS Kirsty McWalter, MS

Contributors – Rhode Island
Betty Vohr, MDWomen & Infant’s Hospital
Julie Jodoin, MEd, MAWomen & Infant’s Hospital
Jyllian Anterni, BSWomen & Infant’s Hospital
Jeffrey Milunsky, MD
Boston University
Dianne Abuelo, MDRhode Island Hospital
Kristilyn Zonno, MSRhode Island Hospital

Contributors - Utah
University of Utah
Janice C. Palumbos, MS, CGC
Bronte Clifford, BS
Rong Mao, PhD
Utah State University
Karl White, PhD
Utah Dept. of Health
Richard Harward, MS

Contributors
Centers for Disease Control and Prevention
John Eichwald, MA
Aileen Kenneson, PhD
Krista Biernath, MD"The information provided in this presentation was supported by Cooperative Agreement Number 01048 from the Centers for Disease Control and Prevention (CDC). The contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC."