A lateral flow test detecting SARS-CoV-2 neutralizing antibodies - … · 2020. 11. 5. · Eighty...
14
A lateral flow test detecting SARS-CoV-2 neutralizing antibodies Nan Zhang, Shuo Chen, Jin V. Wu, Xinhai Yang and Jianfu J. Wang Novodiax Inc. Hayward, CA 94587 Send correspondence to Jianfu J. Wang: [email protected] Abstract It is of critical importance for COVID-19 survivors, vaccine recipients, and public to know whether they have developed neutralizing antibodies or immunity. Here, we describe a 15 minutes lateral flow test for rapid detection of neutralizing antibodies against SARS-CoV-2. All other currently available neutralization tests require hours or days to complete and have to be performed in a well-equipped laboratory. This lateral flow test is the first of its kind and will serve as a convenient diagnostic tool in management of COVID-19 disease. Main Over 40 million confirmed COVID-19 cases and more than one million deaths caused by this disease have been reported as of October 2020. 1 To combat this threat, more than 300 vaccines are under development 2 , with more than 30 of them in various clinical stages. 3 The majority of these vaccines aim to target SARS-CoV-2’s spike (S) protein or the S protein’s receptor binding domain (RBD) in order to induce neutralizing antibodies (NAbs) that block the interaction of RBD with its receptor angiotensin-converting enzyme 2(ACE2) on host cells. 4 Unlike other binding antibodies (BAbs), NAbs represent a type of humoral immunity capable of neutralizing or blocking viruses from entering host cells, preventing them from reproducing and causing severe damage. However, NAbs are not equally developed among the COVID-19 convalescent patients 5,6 and IgG antibodies specific to RBD developed in patients with mild COVID-19 decay rapidly, with a half-life of approximately 36 days 7 . Multiple COVID-19 re- infection cases have been reported. 8-10 Evaluation of SARS-CoV-2 NAbs is critical for both better understanding of immunity to COVID-19 and monitoring levels of protective immunity among the recipients of COVID-19 vaccines. Various assay methods for SARS-CoV-2 NAbs are available. Conventional virus neutralization tests use live ACE2-expressing cells and live SARS-CoV-2 11 and need to be performed in a . CC-BY-NC-ND 4.0 International license It is made available under a is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review) preprint The copyright holder for this this version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596 doi: medRxiv preprint NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice.
Transcript of A lateral flow test detecting SARS-CoV-2 neutralizing antibodies - … · 2020. 11. 5. · Eighty...
-
A lateral flow test detecting SARS-CoV-2 neutralizing antibodies
Nan Zhang, Shuo Chen, Jin V. Wu, Xinhai Yang and Jianfu J. Wang
Novodiax Inc. Hayward, CA 94587
Send correspondence to Jianfu J. Wang: [email protected]
Abstract
It is of critical importance for COVID-19 survivors, vaccine recipients, and public to know
whether they have developed neutralizing antibodies or immunity. Here, we describe a 15
minutes lateral flow test for rapid detection of neutralizing antibodies against SARS-CoV-2. All
other currently available neutralization tests require hours or days to complete and have to be
performed in a well-equipped laboratory. This lateral flow test is the first of its kind and will
serve as a convenient diagnostic tool in management of COVID-19 disease.
Main
Over 40 million confirmed COVID-19 cases and more than one million deaths caused by this
disease have been reported as of October 2020.1 To combat this threat, more than 300 vaccines
are under development2, with more than 30 of them in various clinical stages.3 The majority of
these vaccines aim to target SARS-CoV-2’s spike (S) protein or the S protein’s receptor binding
domain (RBD) in order to induce neutralizing antibodies (NAbs) that block the interaction of
RBD with its receptor angiotensin-converting enzyme 2(ACE2) on host cells.4
Unlike other binding antibodies (BAbs), NAbs represent a type of humoral immunity capable of
neutralizing or blocking viruses from entering host cells, preventing them from reproducing and
causing severe damage. However, NAbs are not equally developed among the COVID-19
convalescent patients5,6 and IgG antibodies specific to RBD developed in patients with mild
COVID-19 decay rapidly, with a half-life of approximately 36 days7. Multiple COVID-19 re-
infection cases have been reported.8-10 Evaluation of SARS-CoV-2 NAbs is critical for both
better understanding of immunity to COVID-19 and monitoring levels of protective immunity
among the recipients of COVID-19 vaccines.
Various assay methods for SARS-CoV-2 NAbs are available. Conventional virus neutralization
tests use live ACE2-expressing cells and live SARS-CoV-211 and need to be performed in a
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice.
mailto:[email protected]://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
biosafety level 3 laboratory. Several virus neutralization tests using pseudovirus12-17 have also
been developed. These tests only need a biosafety level 2 facility and usually take several days to
complete. A simpler and faster enzyme-linked immunosorbent assay (ELISA) that detects
SARS-CoV-2 NAbs based on ACE2-RBD interaction has been recently reported.18 This new test
mimics the virus-host interaction in an ELISA test which can be completed in a safety level 2
laboratory within a few hours. The lateral flow test (LFT) is the fastest and most convenient test
among the popular immunoassays, which typically takes only 15 minutes to complete. It can be
performed either in a professional laboratory or by an individual, thus if available should be a
necessary complement to all available neutralizing tests. Here we report the development of the
first COVID-19 NAb LFT, or Point of Care Test (POCT), along with several noteworthy insights
that we’ve gleaned from its development.
Eighty patients’ plasmas were purchased from a Bio-Bank company, 50 of these were PCR
positive for SARS-CoV-2 (named P1-P50) and 30 were PCR negative (N1-N30). Twenty normal
plasmas (NP1-NP20) were randomly picked from an in-house collection dated between 2014 and
2016, before the COVID-19 pandemic, to establish negative baselines. With all of this in place,
we developed an ELISA to evaluate all 100 plasmas. We then set up a pseudovirus based
neutralization test and developed a Nab LFT. The latter test, the first of its kind to our
knowledge, was compared with and evaluated against the other two popular assays.
Using the ELISA, we measured IgG and IgM BAbs specific to the spike (S) protein, envelop (E)
protein and nucleocapsid (N) protein of SARS-CoV-2 for all 100 plasmas, and measured NAbs
for the 80 patients’ plasmas. In line with previous findings, patients’ humoral immune response
to SARS-CoV-2 varied widely, from completely negative to high titer of both BAbs and NAbs
(Fig 1A-1C). Initial data analyses revealed that positive antibody response rates to N and E
proteins were far lower than the response rates to S protein, and no patient responded to N or E
protein without raising IgG or IgM against S protein. We thus focused only on S protein in the
following development. Based on the relative sensitivity of the assay (patients’ plasmas vs the 20
normal plasmas), signals above average plus 2SD of that of the 20 normal plasmas at 1:200
dilution were chosen as the positive cutoff for both IgG and IgM. In general, PCR positive
patients developed more detectable anti-S1 IgG than the PCR negative patients (78% versus
53%, p=0.0006) (Fig 1D-1F), and similar level of anti-S1 IgM (70% versus 66.7%, p=0.19) (Fig
1D-1F).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
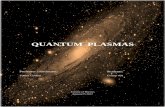
Our NAb LFT was designed to have three test lines and one control line (Fig 2A), using 60 nm
Gold Nanoparticle (GNP)-conjugated RBD or S1 protein to display signal, and using ACE2 in
strip (T1 line in Fig 2A) to capture GNP if the interaction between RBD and ACE2 was not
completely blocked by neutralizing antibodies from a plasma. Two additional test lines showing
anti-S1 protein or anti-RBD IgG (T2) and IgM (T3) were included as a positive reading
reference for positive specimen.
Using the above 4-line strip, we evaluated NAbs from all 80 patients’ plasmas. A single dilution
of 1:12 was used for the purpose to match the common practice in the field. Typical in the field,
with aid of a lancet, 10 µl of finger blood was taken and transferred into the sample pad of a LFT
device, and 50-70ul of buffer was then added to drive the blood sample through the LFT device.
Partial results are demonstrated in Figure 2B. The images of the test results on strips were
captured with a smartphone camera and analyzed with Image J software. The intensity of the test
line was computed against that of a known negative plasma and presented as inhibition
percentage (Supplementary Table 1). A good correlation was observed between the inhibition
percentage at 1:12 dilution of LFT and that of inhibition ELISA (r=0.79, 95% CI: 0.79-0.86,
p
-
contain neutralizing antibody by both inhibition ELISA and NAb LFT, thus should be considered
false PCR negatives. One (plasma # N9) of those three has been chosen to demonstrate
application of our NAb LFT (Fig. 2D). In contrast, IgG and IgM against S1 protein showed very
poor negative percent agreement with PCR and NAb data (Fig. 1F, Supplementary Table 1, 4
and 5). 53.3% of the 30 PCR negative patients showed S1 IgG and 66.7% showed S1 IgM. It is
known that the S and N proteins among all seven human infecting coronaviruses share a
significant amount of sequence homology and can induce cross reactive antibody responses.21 To
determine the contributing factor to these high negative percent disagreements, we tested 12 of
the 30 PCR negative plasmas against S and N proteins of the 4 common cold coronaviruses,
using the same ELISA protocol we used for SARS-CoV-2 proteins. Surprisingly, a higher IgG or
IgM level against S or N proteins of at least one of the 4 common cold coronaviruses was
observed, compared to that of SARS-CoV-2 among all 12 of the plasmas that were tested.
Representative expression profiles by number 1 and 2 PCR negative plasmas (N1 and N2) are
shown in Supplementary Figures 1A to 1D. Based on all of the available data, we believe that a
certain percentage of PCR negative results were true false negatives and may be improved by
testing patients’ neutralizing antibody rather than their binding antibody. Still, we cannot rule out
the possibility that some of the patients in this group actually suffered severe infection caused by
one of the 4 common cold coronaviruses rather than by SARS-CoV-2.
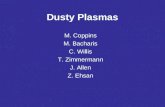
Using the strip with Positive Control and T1 lines, we demonstrated IC50 measurement of two
monoclonal NAbs and three plasmas. In this experiment, a series of dilutions of each NAb or
plasma were tested. The results were computed with Image J software and then analyzed and
graphed with GraphPad Prism (Fig 2C and 2D). We also used the same set of patients’ plasmas
to compare this procedure with inhibition ELISA and a pseudovirus neutralization test (Fig 2E).
In general, we observed quite comparable IC50 results. Among the three methods, the
pseudovirus neutralization test is the most complicated, expensive and lengthy. We used a
commercially available pseudovirus and a one-step luciferase detection system, but still needed
days of cell culture work before and after ACE2 gene transfection. Inhibition ELISA, on the
other hand, has been a routine and standard method in our laboratory, like many other
laboratories. It therefore provides a straightforward technical process. But even so, it requires
several hours of experimental work and needs to be performed in a laboratory setting. In
contrast, the NAb LFT that we’ve established works in the same way as most other lateral flow
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
tests and can be completed within 15 minutes. Besides its convenience and short turnaround
time, though, its most prominent advantage might be its nature of flexibility. In other
neutralization tests, a negative specimen has to be tested for full dilution range in duplicate or
triplicate in order to know the result. Using our LFT, we were able to eliminate all negative
specimens after testing a single concentration and then continuously testing specimens with a
higher neutralizing antibody titer until their IC50s were captured.
Theoretically, any neutralization assays using live cell and live virus simultaneously measure
neutralizing antibodies targeting three regions, N terminal domain (NTD) and RBD in S1and cell
fusion domain in S2. LFT and ELISA, without live cell involved and depending on which
protein fragment is used, can be used to evaluate NAbs specific to one or two domains in S1
protein. We compared performance of GNP labeled RBD with GNP labeled S1 and indeed found
higher NAb titer by using GNP labeled S1 (Supplementary Figure 2). However, we did not see
higher NAb titer in the pseudovirus neutralization test than the other two tests in a small but
direct comparison (Fig 2E).
To combat COVID-19 pandemic, our NAb LFT is continuously improved toward an IVD
product. Since a neutralizing antibody result has to be quantitative or semi-quantitative, we
anticipate using a smartphone and web-based solution for data capturing and processing. This not
only offers convenience, but also necessary quality control for the product.
Materials and Methods: All materials and methods are available as Supplementary information.
Acknowledgments: We acknowledge the excellent proofreading and editing by David Beglin,
PhD and Stephanie Wang, MD.
Author Contributions: J.J.W. designed the NAb LFT experiments; N.Z. prepared GNP and
strips; N.Z. and J.J.W. performed LFT and ELISA tests; X.Y. set-up and performed pseudovirus
neutralization assays; J.V.W., S.C., N.Z. and J.J.W. contributed to data analyses; all authors
contributed to the writing, editing, and completion of the manuscript.
Competing interests All authors are full time employee of Novodiax Inc. N.Z., S.C. J.V.W and
J.J.W. are author and inventor of a patent application that covers the NAb measurement by LFT
described in this article.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
References
1 WHO. WHO Coronavirus Disease (COVID-19) Dashboard, (2020).
2 Le, T. T., Cramer, J. P., Chen, R. & Mayhew, S. Evolution of the COVID-19 vaccine development
landscape. Nat Rev Drug Discov, doi:10.1038/d41573-020-00151-8 (2020).
3 Blueprint, W. T. R. D. DRAFT landscape of COVID-19 candidate vaccines – 9 September 2020.
(2020).
4 Yan, R. et al. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2.
Science 367, 1444-1448, doi:10.1126/science.abb2762 (2020).
5 Wu, F. et al. Evaluating the Association of Clinical Characteristics With Neutralizing Antibody
Levels in Patients Who Have Recovered From Mild COVID-19 in Shanghai, China. JAMA Internal
Medicine, doi:10.1001/jamainternmed.2020.4616 (2020).
6 Mei, Q. et al. Assessment of patients who tested positive for COVID-19 after recovery. Lancet
Infect Dis 20, 1004-1005, doi:10.1016/S1473-3099(20)30433-3 (2020).
7 Ibarrondo, F. J. et al. Rapid Decay of Anti–SARS-CoV-2 Antibodies in Persons with Mild Covid-19.
New England Journal of Medicine, doi:10.1056/NEJMc2025179 (2020).
8 To, K. K. et al. COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain
confirmed by whole genome sequencing. Clin Infect Dis, doi:10.1093/cid/ciaa1275 (2020).
9 Richard Tillett, e. a. Genomic evidence of a Case of reinfection with SARS-CoV-2. SSRN eJournals,
doi:http://dx.doi.org/10.2139/ssrn.3680955 (2020).
10 Iwasaki, A. What reinfections mean for COVID-19. The Lancet Infectious Diseases,
doi:10.1016/S1473-3099(20)30783-0.
11 Suthar, M. S. et al. Rapid Generation of Neutralizing Antibody Responses in COVID-19 Patients.
Cell Rep Med 1, 100040, doi:10.1016/j.xcrm.2020.100040 (2020).
12 Xiong, H. et al. Robust neutralization assay based on SARS-CoV-2 S-bearing vesicular stomatitis
virus (VSV) pseudovirus and ACE2-overexpressed BHK21 cells. (2020).
13 Zettl, F. et al. Rapid Quantification of SARS-CoV-2-Neutralizing Antibodies Using Propagation-
Defective Vesicular Stomatitis Virus Pseudotypes. Vaccines (Basel) 8,
doi:10.3390/vaccines8030386 (2020).
14 Schmidt, F. et al. Measuring SARS-CoV-2 neutralizing antibody activity using pseudotyped and
chimeric viruses. J Exp Med 217, doi:10.1084/jem.20201181 (2020).
15 Crawford, K. H. D. et al. Protocol and Reagents for Pseudotyping Lentiviral Particles with SARS-
CoV-2 Spike Protein for Neutralization Assays. Viruses 12, doi:10.3390/v12050513 (2020).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://covid19.who.int/http://dx.doi.org/10.2139/ssrn.3680955https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
16 Nie, J. et al. Establishment and validation of a pseudovirus neutralization assay for SARS-CoV-2.
Emerg Microbes Infect 9, 680-686, doi:10.1080/22221751.2020.1743767 (2020).
17 Xie, X. et al. A nanoluciferase SARS-CoV-2 for rapid neutralization testing and screening of anti-
infective drugs for COVID-19. bioRxiv, doi:10.1101/2020.06.22.165712 (2020).
18 Tan, C. W. et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated
blockage of ACE2-spike protein-protein interaction. Nat Biotechnol 38, 1073-1078,
doi:10.1038/s41587-020-0631-z (2020).
19 Kurane, I. in Vaccines for Biodefense and Emerging and Neglected Diseases (eds Alan D. T.
Barrett & Lawrence R. Stanberry) 527-535 (Academic Press, 2009).
20 Rubin, S. A. & Plotkin, S. A. in Vaccines (Sixth Edition) (eds Stanley A. Plotkin, Walter A.
Orenstein, & Paul A. Offit) 419-446 (W.B. Saunders, 2013).
21 Huang, A. T. et al. A systematic review of antibody mediated immunity to coronaviruses:
kinetics, correlates of protection, and association with severity. Nature Communications 11,
4704, doi:10.1038/s41467-020-18450-4 (2020).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
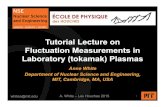
Figure 1. Serological evaluation of 80 plasmas from COVID-19 patients by ELISA.
A. Antibody expression profile of PCR negative patient plasma N6 shows no SARS-Cov-2
specific binding antibody and neutralizing antibody developed; B. Antibody expression profile of
PCR positive patient plasma P42 represents specimens with moderate level of SARS-Cov-2
antibodies; C. Plasma P7 profile represents a group of specimens with high level of antibody
expression against S, N and E proteins and with strong neutralizing activity; D. Distribution of
IgG and IgM against S1 protein among different specimen groups, IgG is significantly higher in
PCR positive plasmas than in PCR negative plasmas but no difference was seen for IgM. E.
Distributions of S1 IgG and S1 IgM of the 50 PCR positive patients sorted first by IgG and then
IgM expression level, only displayed are the those signals above the average plus 2SD of the 20
normal plasmas; F. The same distributions as in Fig. 1E but for PCR negative group, the scale
has been adjusted to be the same as Fig. 1E. A few representative specimens were indicated with
label and arrow.
Figure 2. A Lateral Flow Test based on ACE2-RBD interaction
A. Schematic structure of the LFT strip constructed in this report and projected results. One
representing format used a 60nm GNP labeled RBD with a rabbit Fc tag and accordingly an anti-
rabbit IgG gamma chain antibody in control line. The strip contains three test lines, one for
neutralization activity (T1) and the other two for measurement of RBD-specific IgG and IgM
respectively (T2 and T3). Another 60nm GNP labeled with S1 protein was also used through the
project. B. A manually prepared strip (using adjustable pipette to dispense/coat) demonstrating
various levels of inhibition effect by different patient’s plasmas. C. Measurement of inhibition
concentration of two neutralizing antibodies using 60nm GNP labeled RBD with a rabbit Fc tag
and a workflow from 15 min test to IC50 calculation. D. Half-Strip demonstration of 3 plasma
samples and the workflow to obtain their IC50. A GNP labeled S1 protein was used in this test.
Inhibitory effects on some control lines were caused by the use of a neutralizing antibody in the
control line. E. A comparison of three different inhibition tests, LFT, ELISA and pseudovirus
based neutralization test, using one moderate and two strong inhibitory plasma specimens.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
1A
0 2 4 60
20000
40000
60000
80000
100000
0
20
40
60
80
100
PCR positive patient P7
Titer (LogX)
Bind
ing
antib
ody
(RFU
)
Anti-S IgG
Anti-S IgM
Anti-E IgG
Anti-E IgM
Anti-N IgG
Anti-N IgM
Neutralizing Antibody
1:5
1:20
1:20
0
1:2,
000
1:20
,000
1:20
0,00
0
1:2,
000,
000
Dilution of Plasma
NA
bs (Inhibition %)
0 2 4 60
20000
40000
60000
80000
100000
0
20
40
60
80
100
PCR positive patient P42
Titer (LogX)
Bind
ing
antib
ody
(RFU
) NA
bs (Inhibition %)
1:5
1:20
1:20
0
1:2,
000
1:20
,000
1:20
0,00
0
1:2,
000,
000
Dilution of Plasma
1B 1C
0 2 4 60
20000
40000
60000
80000
100000
0
20
40
60
80
100
PCR negative patient N6
Titer (LogX)
Bind
ing
antib
ody
(RFU
) NA
bs (Inhibition %)
1:5
1:20
1:20
0
1:2,
000
1:20
,000
1:20
0,00
0
1:2,
000,
000
Dilution of Plasma
1D 1F1E
20 no
rmal
plasm
a IgG
50 PC
R+ pl
asma
IgG
30 PC
R- pl
asma
s IgG
20 no
rmal
plasm
a IgM
50 PC
R+ pl
asma
IgM
30 PC
R- pl
asma
IgM
0
20000
40000
60000
80000
100000
120000
Fluo
resc
ent U
nits
Antibodies against S1 proteinS1-specific IgG and IgM among 30 PCR negative patients
N9 →P7 →
P1 → N18 →
N28 →
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
FIG. 2A
SARS-CoV-2 NAbs in sample 1st test line (T1) 2nd test line (T2) 3rd test line (T3) Control line (C)
NAbs+ Vary Vary Vary +
NAbs- + Vary Vary +
Nitrocellulosemembrane
T1
Backing card
T2Samplepad
Conjugate pad
Absorptionpad
60nm gold-bead labeled S1 or RBD-tag
ACE2
Anti-hIgG
C
Anti-tag
T3
Anti-hIgM
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
FIG. 2B
Control
T3
T2
T1
Cont
rol
PCR+
P1
PCR+
P2
PCR+
P3
PCR+
P4
PCR+
P5
PCR+
P6
PCR+
P7
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
Smartphonecamera
Image J
NAb Conc µg/ml
Inhibition % vs “0” conc
Mouse NAb Rabbit NAb
0 0.00% 0.00%0.033 10.97%
0.1 2.93% 77.35%0.33 20.87% 98.62%
1 52.10% 96.80%3.3 54.20%10 93.76%33 98.50%
Excel
GraphPad
FIG. 2C
Rabbit NAb (µg/ml)
0 0.03
3
0.1
0.33
1
0 0.1
0.33
1 3.3
10 33
Mouse NAb (µg/ml)
1 2 3 4 50
20
40
60
80
100
rNAb & mNAb inhibition %
Log10 Antibody Conc. (ng/ml)
Inhi
bitio
n %
Mouse NAb IC50: 1,402 ng/ml
Rabbit NAb IC50: 66 ng/ml
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
Smartphonecamera
Image J
Plasma dilution
Inhibition vs normal plasma NP1
P1 P7 N9
12,288 -0.2565 -0.0531 0.2668
3,072 -0.2515 0.3475 0.2391
768 -0.0768 0.5439 0.4839
192 0.0321 0.9147 0.7464
48 0.5426 0.9788 0.9349
12 0.8605 1.0019 0.9999
Excel
GraphPad
FIG. 2D
1 2 3 40
20
40
60
80
100
Nonlinear regression curve fit
Log10 Dilution
Inhi
bitio
n %
P1(S1-GNP) IC50: 49
P7 (S1-GNP) IC50: 1,138N9 (S1-GNP) IC50: 897
P1
P7
N9
C
T1
1:12
1:12
Plasma dilution
1:12
1:48
1:19
21:
768
1:3,
072
1:12
,288
NP1
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
-
1 2 3 40
20
40
60
80
100
Comparison of Inhibition effect among different methods
Log10 Dilution
Inhi
bitio
n %
P1 LFT (S1-GNP) IC50: 49
P7 LFT (S1-GNP) IC50: 1,138
N9 LFT (S1-GNP) IC50: 897
N9 Pseudovirus IC50: 467
N9 ELISA IC50: 1,165
P7 Pseudovirus IC50: 1,400
P7 ELISA IC50: 1,324
P1 Pseudovirus IC50: 185
P1 ELISA IC50: 658
FIG. 2E
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.(which was not certified by peer review)preprint The copyright holder for thisthis version posted November 10, 2020. ; https://doi.org/10.1101/2020.11.05.20222596doi: medRxiv preprint
https://doi.org/10.1101/2020.11.05.20222596http://creativecommons.org/licenses/by-nc-nd/4.0/
A lateral flow test detecting SARS-CoV-2 neutralizing antibodiesDRAFT FIGURES - Lateral flow 10-25-2020-Jin 2DRAFT FIGURES - Lateral flow 10-25-2020-Jin 3DRAFT FIGURES - Lateral flow 10-25-2020-Jin 4DRAFT FIGURES - Lateral flow 10-25-2020-Jin 5DRAFT FIGURES - Lateral flow 10-25-2020-Jin 6DRAFT FIGURES - Lateral flow 10-25-2020-Jin 7