A framework for the nonantibiotic management of upper ... · A framework for the non-antibiotic...
21
ORIGINAL PAPER A framework for the non-antibiotic management of upper respiratory tract infections: towards a global change in antibiotic resistance S. Essack, 1 A. C. Pignatari 2, * SUMMARY Antibiotic resistance has become a critical health issue on a global scale, with much of the problem resulting from inappropriate use of antibiotics in primary care. To change this practice, the global respiratory infection partnership has for- mulated a pentagonal (five P) framework for the non-antibiotic management of upper respiratory tract infections (URTIs) – one of the most common conditions in primary care for which antibiotics are prescribed. The framework presents the rationale for focusing on URTIs to promote antibiotic stewardship in primary care and elaborates on five key areas to focus on to bring about change: policy, pre- vention, prescribers, pharmacy and patients. The ultimate aim is to adopt a patient-centred symptomatic management strategy using a flexible framework that can be adapted across countries to create a consistent global approach to change behaviour. What’s new • Innovative framework targeting key role players to elicit a change in behaviour to address rising resistance rates in the community What’s known • Antibiotic resistance is an escalating global health threat largely attributable to indiscriminate antibiotic use, especially in community settings Introduction Antibiotic resistance is a critical health issue on a global scale (1,2). Much of the problem results from the inappropriate use of antibiotics, in particular their overuse, in primary care. The containment of antibiotic resistance requires a consistent and coordi- nated approach towards symptomatic treatment in applicable primary care conditions where inappropri- ate antibiotic use is a problem. The most common reason for patients to seek medical attention in primary care is infection of the upper respiratory tract, such as sore throat, common cold, influenza, earache and cough (3). These infec- tions also account for a large proportion of the anti- biotics prescribed in primary care (Figure 1) (4). Depending on the country, 34–60% of patients with an upper respiratory tract infection (URTI) receive an antibiotic (5). Yet, the majority of these patients do not require an antibiotic because most URTIs are of viral origin and are self-limiting, complications are rare and an array of non-antibiotic treatment options are available to provide symptomatic relief (5). To facilitate a change towards prudent use of antibi- otics for the treatment of URTIs, members of the Glo- bal Respiratory Infection Partnership (GRIP) have developed a framework for the non-antibiotic man- agement of such infections. The framework presents the rationale for focusing on URTIs to promote anti- biotic stewardship in primary care and elaborates on five key areas to focus on to bring about change: pol- icy, prevention, prescribers, pharmacy and patients. This framework has been shared with and reviewed by healthcare professionals from Australia, Austria, Brazil, Germany, Hungary, India, Ireland, Israel, Italy, The Netherlands, Romania, Russia, Singapore, South Africa, Spain, Thailand, the United Kingdom and the United States of America. The global frame- work is strengthened through a collaborative approach by multiple primary healthcare provider specialties and is applicable across countries and conti- nents (Figure 2). It is envisaged as a prototype that can be adapted to other infections in the long term (5). Policy An environment that nurtures change enables its sus- tainability (6). In the context of appropriate, rational antibiotic use for URTIs, this means creating a policy environment where antibiotic use is not the norm. At present, there is wide variation between coun- tries in how antibiotics are used in primary care. In some countries, patients can self-treat with antibiot- ics by buying them over the counter, whereas in other countries antibiotics are only available on prescription. Treatment guidelines and essential 4 ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 4–9 doi: 10.1111/ijcp.12335 1 School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa 2 Escola Paulista de Medicina- Universidade Federal de S~ ao Paulo, Rua Leandro Dupret 188, Sao Paulo, Brazil Correspondence to: Sabiha Essack, School of Health Sciences, University of KwaZulu-Natal, Private Bag X54001, Durban 4000, South Africa Tel.: +2731 2608048 Fax: +2731 2607872 Email: [email protected] *In collaboration with the Global Respiratory Infection Partnership: Attila Altiner (Germany), John Bell (Australia), Martin Duerden (UK), Sabiha Essack (South Africa), Roman Kozlov (Russia), John Oxford (UK), Antonio Carlos Pignatari (Brazil), Aurelio Sessa (Italy), Alike van der Velden (The Netherlands). 1 1 1 1
Transcript of A framework for the nonantibiotic management of upper ... · A framework for the non-antibiotic...

ORIGINAL PAPER
A framework for the non-antibiotic management ofupper respiratory tract infections: towards a globalchange in antibiotic resistance
S. Essack,1 A. C. Pignatari2,*
SUMMARY
Antibiotic resistance has become a critical health issue on a global scale, with
much of the problem resulting from inappropriate use of antibiotics in primary
care. To change this practice, the global respiratory infection partnership has for-
mulated a pentagonal (five P) framework for the non-antibiotic management of
upper respiratory tract infections (URTIs) – one of the most common conditions in
primary care for which antibiotics are prescribed. The framework presents the
rationale for focusing on URTIs to promote antibiotic stewardship in primary care
and elaborates on five key areas to focus on to bring about change: policy, pre-
vention, prescribers, pharmacy and patients. The ultimate aim is to adopt a
patient-centred symptomatic management strategy using a flexible framework that
can be adapted across countries to create a consistent global approach to change
behaviour.
What’s new• Innovative framework targeting key role players
to elicit a change in behaviour to address rising
resistance rates in the community
What’s known• Antibiotic resistance is an escalating global
health threat largely attributable to indiscriminate
antibiotic use, especially in community settings
Introduction
Antibiotic resistance is a critical health issue on a
global scale (1,2). Much of the problem results from
the inappropriate use of antibiotics, in particular
their overuse, in primary care. The containment of
antibiotic resistance requires a consistent and coordi-
nated approach towards symptomatic treatment in
applicable primary care conditions where inappropri-
ate antibiotic use is a problem.
The most common reason for patients to seek
medical attention in primary care is infection of the
upper respiratory tract, such as sore throat, common
cold, influenza, earache and cough (3). These infec-
tions also account for a large proportion of the anti-
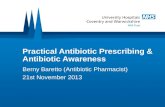
biotics prescribed in primary care (Figure 1) (4).
Depending on the country, 34–60% of patients with
an upper respiratory tract infection (URTI) receive
an antibiotic (5). Yet, the majority of these patients
do not require an antibiotic because most URTIs are
of viral origin and are self-limiting, complications
are rare and an array of non-antibiotic treatment
options are available to provide symptomatic relief (5).
To facilitate a change towards prudent use of antibi-
otics for the treatment of URTIs, members of the Glo-
bal Respiratory Infection Partnership (GRIP) have
developed a framework for the non-antibiotic man-
agement of such infections. The framework presents
the rationale for focusing on URTIs to promote anti-
biotic stewardship in primary care and elaborates on
five key areas to focus on to bring about change: pol-
icy, prevention, prescribers, pharmacy and patients.
This framework has been shared with and reviewed
by healthcare professionals from Australia, Austria,
Brazil, Germany, Hungary, India, Ireland, Israel,
Italy, The Netherlands, Romania, Russia, Singapore,
South Africa, Spain, Thailand, the United Kingdom
and the United States of America. The global frame-
work is strengthened through a collaborative
approach by multiple primary healthcare provider
specialties and is applicable across countries and conti-
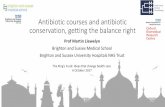
nents (Figure 2). It is envisaged as a prototype that can
be adapted to other infections in the long term (5).
Policy
An environment that nurtures change enables its sus-
tainability (6). In the context of appropriate, rational
antibiotic use for URTIs, this means creating a policy
environment where antibiotic use is not the norm.
At present, there is wide variation between coun-
tries in how antibiotics are used in primary care. In
some countries, patients can self-treat with antibiot-
ics by buying them over the counter, whereas in
other countries antibiotics are only available on
prescription. Treatment guidelines and essential
4ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 4–9
doi: 10.1111/ijcp.12335
1School of Health Sciences,
University of KwaZulu-Natal,
Durban, South Africa2Escola Paulista de Medicina-
Universidade Federal de S~ao
Paulo, Rua Leandro Dupret
188, Sao Paulo, Brazil
Correspondence to:
Sabiha Essack, School of Health
Sciences, University of
KwaZulu-Natal, Private Bag
X54001, Durban 4000, South
Africa
Tel.: +2731 2608048
Fax: +2731 2607872
Email: [email protected]
*In collaboration with the
Global Respiratory Infection
Partnership: Attila Altiner
(Germany), John Bell
(Australia), Martin Duerden
(UK), Sabiha Essack (South
Africa), Roman Kozlov (Russia),
John Oxford (UK), Antonio
Carlos Pignatari (Brazil), Aurelio
Sessa (Italy), Alike van der
Velden (The Netherlands).
1 1
1 1

drugs lists regulate access to and use of antibiotics,
particularly in the public health sectors of developing
countries, while antibiotic use in the private sector is
largely at the discretion of the prescriber in both
developed and developing countries. The recommen-
dations with regard to antibiotic therapy for specific
conditions also vary. For example, the use of antibi-
otics for the treatment of acute pharyngitis is dis-
couraged in some national guidelines and the
condition is considered to be self-limiting. National
guidelines in some other countries recommend anti-
biotics if a streptococcal infection is suspected, out
of concern for complications such as acute rheumatic
fever (7).
Reasons for these disparities in antibiotic use
include differences in interpreting clinical evidence,
influence of professional bodies/associations, charac-
teristics of the healthcare system and cultural
attitudes (7,8). Given these differences, policy
measures to advance appropriate, rational antibiotic
use need to be country-specific and tailored to local
circumstances including, but not limited to, the pre-
vailing burden of disease, taking into account under-
lying comorbidities, such as HIV and AIDS, and
existing resistance rates. Commitment from central
and local authorities, ideally national and local Min-
istries of Health, is required, as is endorsement from
professional bodies/associations, and clinical commu-
nities of practice and local experts.
Tools available to health policymakers include
national guidelines and national surveillance pro-
grammes monitoring antibiotic use and resistance
Figure 2 The pentagonal framework for change encompasses five key focus areas (the five ‘P’s)
Figure 1 Inappropriate antibiotic use for upper respiratory
tract infections (1). Reproduced, with the permission of the
publisher, from The evolving threat of antimicrobial
resistance. Options for action, 2012 (Fig. 2.1, page 18 http://
whqlibdoc.who.int/publications/2012/9789241503181_eng.
pdf, accessed 12 September 2013). ARI, Acute respiratory
infection
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 4–9
Global framework for respiratory infection management 52 2
2 2

patterns, both of which inform empiric therapy, as
well as making antibiotics contingent on a prescrip-
tion, and restricting the marketing of antibiotics
(6,8). Other options include incentivising appropriate
prescribing or penalising inappropriate prescribing of
antibiotics (6). Education of relevant healthcare pro-
viders, such as primary care physicians and phar-
macy personnel, is also a health education-related
policy consideration, as is continuing professional
development for primary care providers (8,9).
Implementation of national policies by primary
care providers will be further enhanced by incorpo-
rating the principles into clinical decision-making
and by gaining support and endorsement from local
experts. For example, leading figures in antibiotic
resistance from national societies could be actively
involved in the development of guidelines.
Prevention
Any clinical decision in terms of URTI manage-
ment needs to be driven, in part, by the aim to
prevent antibiotic resistance, in line with the call
by the Infectious Diseases Society of America for a
greater focus on antibiotic stewardship to preserve
the efficacy of current antibiotics (10). In practice,
this means that antibiotics should be used only
when necessary, with improving patient outcomes
on an individual and community level as a core
principal.
As antibiotic resistance is a function of time and
use (11), inappropriate use, overuse and misuse of
antibiotics should be explicitly avoided. When man-
aging patients with a URTI, antibiotic therapy
should, therefore, be reserved for patients with a seri-
ous infection, and those at increased risk of compli-
cations (12). The risk of serious infection can be
determined by identifying and excluding red-flag
signs and symptoms (12). Risk factors for the devel-
opment of complications include age and immune
status, with older patients and those who are immu-
nocompromised being at higher risk (13).
Confirming bacterial aetiology may be of merit in
some settings. Such diagnostic tests can guide
prescribing decisions and facilitate discussions with
the patient about the appropriate use of antibiotics
(8). However, considering that most bacterial infec-
tions are also self-limiting (5), antibiotic prescription
on the basis of a positive result in an otherwise
healthy individual should be carefully considered.
For reassurance, it is good practice to provide
patients with guidance on when to return for further
investigation, to ensure that secondary infections or
deteriorating conditions receive adequate attention
(12).
Prescribers
As part of a consultation that includes providing a
full assessment of a patient’s symptoms and expec-
tations and formulating a differential diagnosis, pre-
scribers have a key role in guiding patients with a
URTI towards seeking symptomatic relief, as
opposed to antibiotic treatment. Yet many prescrib-
ers themselves have misconceptions about the use
of antibiotics for the treatment of URTIs, believing
that antibiotics are generally warranted (12,14).
Physicians may further be inclined to prescribe an
antibiotic if the patient requests such a prescription,
in order to maintain a good relationship with the
patient (8) or for fear of litigation. Limited consul-
tation time may preclude a more detailed discus-
sion with the patient about the appropriateness of
antibiotics for a self-limiting illness, making antibi-
otic prescription an expedient option. Primary care
physicians say they often feel patient pressure to
prescribe antibiotics (15). Nonetheless, data suggest
many doctors overestimate a patient’s wish for anti-
biotics, resulting in inappropriate prescribing (14).
Research by Altiner et al. (16) indicates that the
overuse of antibiotics in many cases might not be
attributable to a lack of knowledge on behalf of the
physician but to a lack of patient-centredness (16).
The authors suggest that a substantial amount of
antibiotic prescriptions could be avoided if general
practitioners took care to identify the real expecta-
tions and concerns of their patients.
Another factor that contributes to antibiotic pre-
scribing is diagnostic uncertainty. It is notoriously
difficult to distinguish between bacterial and viral
URTIs based on clinical symptoms, and doctors may
therefore err on the side of caution and prescribe an
antibiotic (2,8,17).
Strategies to encourage appropriate prescribing in
primary care include the development of evidence-
based policies, in collaboration with local experts,
who provide practical guidance on how to rule out
serious infections and how to handle patient demand
for an antibiotic, complemented by information on
various symptomatic treatment options. Physician
awareness may also be raised by more detailed infor-
mation on the problems arising from over-prescrip-
tion of antibiotics and their lack of efficacy in
relieving patient symptoms (8).
In addition, strategies that focus on doctor–patientcommunication and patient empowerment will be
of value (14). Guidelines and procedures that outline
how to engage with patients and involve them
in treatment decisions could be implemented.
Finally, formal training in communication skills is
invaluable (18).
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 4–9
6 Global framework for respiratory infection management3 3
3 3

Pharmacy
For many patients, the pharmacy is the first port of
call when seeking advice on a common health condi-
tion. Pharmacy staff are therefore able to make a
substantial contribution towards antibiotic steward-
ship and self-management of common self-limiting
conditions, in particular URTIs, which are the most
common acute problem in primary care (3).
Pharmacists are pivotal in establishing protocols
for treatment and referral that support the aim of
symptomatic management of URTIs without the use
of antibiotics. Pharmacy staff have a fundamental
stewardship role as community educators on the
appropriate and rational use of antibiotics.
Pharmacy technicians and assistants are ideally
placed to facilitate a decision to manage a URTI
without the use of antibiotics by advising customers
on symptomatic treatment options and providing
information on the realistic duration of the illness. It
is important to advise patients that antibiotics do
not help to reduce the severity of symptoms, as they
do not offer pain relief or shorten duration of symp-
toms (19), while highlighting that with URTIs, symp-
tomatic relief is often all that is necessary (20).
It is important that any advice on medications
and formulations is tailored to the patient’s specific
symptoms and preferences. In addition, pharmacy
staff need to be able to identify red-flag symptoms
and other risk factors for a serious infection and
refer patients to physicians where necessary.
As with prescribers, guidance and training on
patient communication will be invaluable for members
of the pharmacy team, and their work can be further
supported by print leaflets for patients to take home.
Patient
To move towards a culture where non-antibiotic
management of URTIs is the norm, it is important
to mobilise the public and the patient as proponents
of non-antibiotic treatment for self-limiting condi-
tions (15). Educating the public is an important step
to nurture change (6), with potential measures
including media campaigns and educational projects
in schools and universities, to raise awareness early
in the education cycle (8). Many patients expect an
antibiotic because they erroneously believe that anti-
biotics shorten the illness. Moreover, prescription of
an antibiotic may serve to inappropriately validate
the patient’s belief that their condition is serious.
Most are unaware that most URTIs are usually
caused by viruses and that antibiotics are therefore
ineffective (Table 1) (21). The concept of a self-limit-
ing illness can also be difficult to understand and
accept, particularly if patients perceive antibiotics as
the solution to getting better and resuming normal
activities. In addition, many members of the public
do not know that the inappropriate use of antibiotics
can lead to antibiotic resistance with consequences
for the individual patient, as well as the community (4).
Previous experience of having an antibiotic pre-
scribed for a URTI reinforces any misunderstandings
and false expectations that the patient may have
(14). For example, if a patient receives an antibiotic
when presenting with a common cold, this supports
the belief that the antibiotic is necessary to clear the
cold, resulting in the expectation of the same treat-
ment approach for subsequent times when similar
symptoms occur in themselves and family members.
Such misconceptions can lead to pressure on physi-
cians to prescribe an antibiotic. There is evidence to
indicate that physicians are 10 times more likely to
prescribe an antibiotic if they believe that the patient
expects such a prescription (15), even if this goes against
their better judgement (8,22). Scott et al. (22) observed
that patients use behaviours such as directly requesting
an antibiotic, suggesting a diagnosis, portraying severity
of illness and appealing to (non-related) life circum-
stances to influence prescribing decisions (22).
However, it is also important to note that patients
do not expect an antibiotic as often as physicians
perceive they do (14). When patients describe severe
symptoms, it is important to show empathy and
reassurance that a serious illness has been ruled out
(14). Even if patients specifically ask for an antibi-
otic, they may in fact be seeking pain relief or a
medical certificate (15,23). Understanding why
patients feel an antibiotic will help their symptoms
could be an important consideration for physicians.
These issues can be addressed by taking a patient-
centred approach within consultations (14,16), which
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Knowledge about antibiotics among Europeans (21)
Knowledge item True (%) False (%) Don’t know (%)
Antibiotics kill viruses 53 36 11
Antibiotics are effective against colds and flu 47 46 7
Unnecessary use of antibiotics makes them become ineffective 83 8 9
Taking antibiotics often has side effects such as diarrhoea 68 15 17
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 4–9
Global framework for respiratory infection management 74 4
4 4

includes identifying the patient’s concerns and expec-
tations, providing education on the appropriate use of
antibiotics and the natural course of the patient’s con-
dition, reassuring patients that serious infection has
been ruled out, discussing symptomatic treatment
options and clarifying when a return visit is warranted
(23). Any advice needs to be tailored to the specific
needs and preferences of the individual patient.
Conclusions
In conclusion, a consistent and collaborative effort
that encompasses policymakers, healthcare providers
and patients is urgently required to prevent inappro-
priate antibiotic use in primary care and to contain
antibiotic resistance. URTIs are a key area for con-
cern, given their prevalence and the widespread use
of antibiotics despite the viral and self-limiting nat-
ure of most infections, together with the availability
of effective symptomatic treatments.
While guidelines exist in many countries on the use
of antibiotics for URTIs, further work is required to
elicit a change in antibiotic prescribing practice.
Policymakers are called upon to create an environment
where the use of antibiotics is not the norm, by intro-
ducing disincentives to antibiotic use and surveillance
programs, along with guidance that encourages and
promotes self-management with symptomatic medica-
tions as the treatment in the first instance.
Prescribers, pharmacists and other primary care
providers will benefit from increased knowledge in
treating respiratory tract infections, with or without
antibiotics. Such knowledge must be anchored by a
solid understanding of patient needs and evidence-
based treatments to meet these needs. Antibiotic use
should be reserved for patients with a severe infec-
tion and those with risk factors for complications.
Improved communication skills will be of great value
to healthcare providers, so that they can effectively
encourage behavioural change in patients by increas-
ing their knowledge.
It is paramount that patient concerns and needs
are taken seriously. Healthcare practitioners should
work in partnership with their patients to develop an
individualised treatment plan and empower patients
to self-manage URTIs with non-antibiotic treatment
options for symptomatic relief, with the pharmacy as
the first point of call.
Adopting these recommendations at the local level
will reinforce the recognition that antibiotic resis-
tance is a grave and growing global health issue, for
which behavioural change in the daily practice of all
roleplayers, including patients, is imperative.
Disclosures
Publication of this supplement article was supported
as part of an unrestricted educational grant by Reck-
itt Benckiser Group PLC. Editorial assistance during
the development and revision of this manuscript was
provided by Mash Health Limited and supported by
Reckitt Benckiser Group PLC.
Author contributions
The authors provided substantial contributions to
the development and revision of the manuscript and
approved the final version of the manuscript.
References
1 World Health Organization. The evolving threat of
antimicrobial resistance. Options for action, 2012.
http://whqlibdoc.who.int/publications/2012/978924
1503181_eng.pdf (accessed 12 September 2013).
2 World Economic Forum “Global Risks 2013”.
http://www.weforum.org/reports/global-risks-2013-
eighth-edition (accessed 12 September 2013).
3 Francis NA, Butler CC, Hood K, Simpson S, Wood
F, Nuttall J. Effect of using an interactive booklet
about childhood respiratory tract infections in pri-
mary care consultations on reconsulting and antibi-
otic prescribing: a cluster randomised controlled
trial. BMJ 2009; 339: b2885.
4 Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD.
Effect of antibiotic prescribing in primary care on anti-
microbial resistance in individual patients: systematic
review andmeta-analysis. BMJ 2010; 340: c2096.
5 van der Velden A, Duerden MG, Bell J et al. Pre-
scriber and patient responsibilities in treatment of
acute respiratory tract infections – essential for con-
servation of antibiotics. Antibiotics 2013; 2: 316–27.
6 Michie S, van Stralen MM, West R. The behaviour
change wheel: a new method for characterising and
designing behaviour change interventions. Imple-
ment Sci 2011; 6: 42.
7 Matthys J, De Meyere M, van Driel ML, De Sutter A.
Differences among international pharyngitis guidelines:
not just academic.Ann FamMed 2007; 5: 436–43.
8 Oxford JS, Goossens H, Schedler M, Sefton A,
Sessa A, van der Velden A. Factors influencing
inappropriate antibiotic prescription in Europe.
Educ Prim Care 2013; 24: 291–3.
9 Forsetlund L, Bradley P, Forsen L, Nordheim L,
Jamtvedt G, Bjørndal A. Randomised controlled
trial of a theoretically grounded tailored interven-
tion to diffuse evidence-based public health practice
[ISRCTN23257060]. BMC Med Educ 2003; 3: 2.
10 Boucher HW, Talbot GH, Benjamin DK et al. 10 x
‘20 Progress – development of new drugs active
against Gram-negative bacilli: an update from the
Infectious Diseases Society of America. Clin Infect
Dis 2013; 56: 1685–94.
11 Finch RG. Antibiotic resistance. J Antimicrob Che-
mother 1998; 42: 125–8.
12 National Institute for Health and Clinical Excellence
(NICE). Clinical Guideline 69. Respiratory tract
infections – antibiotic prescribing. Prescribing of
antibiotics for self-limiting respiratory tract infec-
tions and in adults and children in primary care, July
2008. http://www.nice.org.uk/cg069 (accessed 12
September 2013).
13 Borchardt RA, Rolston KV. Respiratory tract infections:
emerging viral pathogens. JAAPA 2012; 25: 19–20.
14 Altiner A, Brockmann S, Sielk M, Wilm S, Wegsche-
ider K, Abholz HH. Reducing antibiotic prescrip-
tions for acute cough by motivating GPs to change
their attitudes to communication and empowering
patients: a cluster-randomized intervention study. J
Antimicrob Chemother 2007; 60: 638–44.
15 van Driel ML, De Sutter A, Deveugele M et al. Are
sore throat patients who hope for antibiotics actually
asking for pain relief? Ann FamMed 2006; 4: 494–9.
16 Altiner A, Knauf A, Moebes J, Sielk M, Wilm S.
Acute cough: a qualitative analysis of how GPs
manage the consultation when patients explicitly or
implicitly expect antibiotic prescriptions. Fam Pract
2004; 21: 500–6.
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 4–9
8 Global framework for respiratory infection management5 5
5 5

17 Shephard A, Smith G, Aspley S, Schachtel B. Effi-
cacy of Flurbiprofen 8.75 mg Lozenges for Streptococ-
cal and Non-Streptococcal Sore Throat: Pooled
Analysis of Two Randomised, Placebo-Controlled
Studies. Berlin, Germany: ECCMID, 2013: P2085.
18 Maguire P, Pitceathly C. Key communication skills
and how to acquire them. BMJ 2002; 325:
697–700.
19 Centers for Disease Control and Prevention. Adult
appropriate antibiotic use summary. http://www.cdc.
gov/getsmart/campaign-materials/info-sheets/adult-
approp-summary.pdf (accessed 12 September 2013).
20 van Duijn HJ, Kuyvenhoven MM, Schellevis FG,
Verheij TJ. Illness behaviour and antibiotic pre-
scription in patients with respiratory tract symp-
toms. Br J Gen Pract 2007; 57: 561–8.
21 Special Eurobarometer 338. Antimicrobial resistance.
Survey carried out by TNS Opinion & Social at the
request of the Directorate-General for Health and
Consumers, 2010. http://ec.europa.eu/health/antimi
crobial_resistance/docs/ebs_338_en.pdf (accessed 12
September 2013).
22 Scott JG, Cohen D, DiCicco-Bloom B, Orzano AJ,
Jaen CR, Crabtree BF. Antibiotic use in acute respi-
ratory infections and the ways patients pressure
physicians for a prescription. J Fam Pract 2001; 50:
853–8.
23 NPS. NPS News 63: Managing expectations for anti-
biotics in respiratory tract infections, 2009. http://
www.nps.org.au/__data/assets/pdf_file/0009/71478/
news_63.pdf (accessed on 12 September 2013).
Paper received September 2013, accepted September 2013
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 4–9
Global framework for respiratory infection management 96 6
6 6

ORIGINAL PAPER
Sore throat: effective communication delivers improveddiagnosis, enhanced self-care and more rational use ofantibiotics
A. W. van der Velden,1 J. Bell,2 A. Sessa,3 M. Duerden,4 A. Altiner5*
SUMMARY
The majority of throat infections are of viral origin and resolve without antibiotic
treatment. Despite this, antibiotic use for sore throat infections remains high,
partly because it is difficult to determine when antibiotics may be useful, on the
basis of physical findings alone. Antibiotics may be beneficial in bacterial throat
infections under certain clinical and epidemiological circumstances; however, even
many of those infections in which bacteria play a role do resolve just as quickly
without antibiotics. Furthermore, non-medical factors such as patient expectations
and patient pressure are also important drivers of antibiotic use. To address these
issues, a behavioural change is required that can be facilitated by improved com-
munication between primary healthcare providers and patients. In this article, we
provide doctors, nurses and pharmacy staff, working in primary care or in the com-
munity, with a structured approach to sore throat management, with the aim of
educating and empowering patients to self-manage their condition. The first com-
ponent of this approach involves identifying and addressing patients’ expectations
and concerns with regard to their sore throat and eliciting their opinion on antibi-
otics. The second part is dedicated to a pragmatic assessment of the severity of
the condition, with attention to red-flag symptoms and risk factors for serious
complications. Rather than just focusing on the cause (bacterial or viral) of the
upper respiratory tract infections as a rationale for antibiotic use, healthcare pro-
viders should instead consider the severity of the patient’s condition and whether
they are at high risk of complications. The third part involves counselling patients
on effective self-management options and providing information on the expected
clinical course. Such a structured approach to sore throat management, using
empathetic, non-paternalistic language, combined with written patient information,
will help to drive patient confidence in self-care and encourage them to accept the
self-limiting character of the illness – important steps towards improving antibiotic
stewardship in acute throat infections.
What’s new• The Global Respiratory Infection Partnership has
developed a toolkit comprising educational
materials for primary healthcare providers and
patients.
• Toolkit materials: www.GRIP-initiative.com
• Implementation of the toolkit is expected to
enhance patients’ self-care of sore throat,
thereby limiting antibiotic use.
What’s known• Antibiotics have very limited effectiveness in
treatment of sore throat.
• Improved communication between healthcare
provider and patient could facilitate a
behavioural change towards appropriate use of
antibiotics for sore throat.
Introduction
In the first part of this supplement, the Global Respi-
ratory Infection Partnership (GRIP) proposed a glo-
bal framework for the non-antibiotic management of
upper respiratory tract infections (URTIs). Here, we
apply the outlined principles to the management of
sore throat (as an example of a common symptom
of URTIs), offering practical advice to primary care
teams on how to implement the guidance in their
daily practice.
Sore throat is one of the top 10 reasons for
patients to visit ambulatory care (1), and the use of
antibiotics for the treatment of sore throat is wide-
spread (2). However, up to 95% of infections in
adults are of viral origin (3). These infections are
usually self-limiting, with symptoms typically resolv-
ing within 1–2 weeks (4), and complications are rare
(5). For the vast majority of throat infections, antibi-
otics do not have any impact on the severity of
symptoms or the course of the disease, and do not
prevent complications (6). A recent review assessing
the effect of antibiotics in sore throat at one week,
described that 21 patients have to be treated in order
to see one patient benefitting from a course of anti-
biotics (7). Moreover, a systematic review found that
antibiotics are among the least effective treatment
options for sore throat (8). By contrast, the efficacy
10ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 10–16
doi: 10.1111/ijcp.12336
1Julius Center for Health
Sciences and Primary Care,
University Medical Center
Utrecht, Heidelberglaan 100,
Utrecht, The Netherlands2Pharmacy School, University of
Technology Sydney, Broadway,
Australia3Italian College of General
Practitioners, Florence, Italy4Office of Medical Director
BCUHB, Wrexham, UK5Institute of General Practice,
Rostock University Medical
Centre, Rostock, Germany
Correspondence to:
Alike van der Velden, Julius
Center for Health Sciences and
Primary Care, University
Medical Center Utrecht,
Heidelberglaan 100, 3584 CX,
Utrecht, The Netherlands
Tel.: +31-0-88-756-8511
Fax: +31-0-88-756-8099.
Email: a.w.vandervelden@
umcutrecht.nl
*In collaboration with the
Global Respiratory Infection
Partnership: Attila Altiner
(Germany), John Bell
(Australia), Martin Duerden
(UK), Sabiha Essack (South
Africa), Roman Kozlov (Russia),
John Oxford (UK), Antonio
Carlos Pignatari (Brazil), Aurelio
Sessa (Italy), Alike van der
Velden (The Netherlands).
7 7
7 7

of symptomatic treatments, such as NSAIDs and par-
acetamol, was up to 93% higher than placebo. Group
A beta-haemolytic streptococcus infections are the
most common bacterial cause of sore throat, yet they
are responsible for only 10% of sore throats (3). It is
these infections where antibiotics may be beneficial
in shortening the clinical course and preventing
complications (e.g. rheumatic fever), notably in set-
tings where risk of complications may be high (9).
However, in clinical practice it is notoriously difficult
to distinguish between URTIs of viral and bacterial
origin, as physical signs and symptoms are similar in
both types of infection (9–11). Diagnostic certainty
can only be achieved with a throat culture (3,9). As
this delays treatment and does not accurately predict
benefit from antibiotics, physicians in many coun-
tries tend to base their treatment decision on other
(non-medical) factors.
Many authors therefore recommend the manage-
ment of sore throat based on the severity of the
infection, combined with how unwell the patient
appears and on the risk profile of the patient (4).
Several prediction rules have been developed that use
a combination of signs and symptoms to evaluate
the risk of bacterial infection, where antibiotic treat-
ment may be indicated. The most commonly used is
the Centor score (1,9). This score incorporates the
following symptoms: tonsillar exudate; tender ante-
rior cervical adenopathy; absence of cough and his-
tory of fever (> 38.0 °C). Patients meeting three or
four Centor criteria have a higher likelihood of strep-
tococcal infection (12); however, although the Centor
criteria predict the likelihood of streptococcal infec-
tion, they do not predict the patient’s response to
antibiotic treatment.
There are also certain patient subgroups that
should be monitored more closely, or treated,
because they have an elevated risk of severe respira-
tory disease. Factors associated with an increased risk
include advanced age, respiratory or immunocom-
promising comorbidity and long duration of symp-
toms (13,14).
Diagnostic certainty can be increased by the use of
point-of-care testing, the rapid Strep A test for sore
throat, if available. A point-of-care test may also
prove useful as a tool to reassure patients and
increase their understanding of the prescribing deci-
sion (2,15).
Finally, any prescribing decision needs to include
consideration of the risks and disadvantages associ-
ated with antibiotic therapy. These include side
effects such as diarrhoea, nausea and rash (4,16,17),
and disturbance of the microbiota. Wilton et al.
reported an increased risk of developing vaginal can-
didiasis after antibiotic therapy (17). In addition,
bacteria may become resistant to the antibiotic used
(16,18); resistant bacteria can be found for up to
one year in the individual (18). This could make
future infections more difficult to treat, not only in
this individual patient but also in the community,
because resistant bacteria can be passed on to family
members, work colleagues and friends. Antimicrobial
resistance is a major public health threat, as it makes
infections more difficult to treat or even untreatable
(18,19).
Interaction between prescriber/pharmacy team and patient
Treatment decisions are not only influenced by med-
ical factors; non-medical factors such as cultural
issues or patient expectations and pressure also affect
prescribing behaviour (20). Tackling the overuse of
antibiotics in the management of sore throat there-
fore requires a broader approach that focuses on the
relationship between healthcare provider and patient.
In this interaction it is the responsibility of the
prescriber to firstly identify the need for an
antibiotic, bearing in mind that most URTIs are of
viral origin and self-limiting (14,21). Prescribers
can help combat the overuse of antibiotics for
sore throat management by addressing any misper-
ceptions and expectations about antibiotics that
the patient may bring to the consultation (2,20,22).
In fact, antibiotic demand may not be the main
reason patients consult their healthcare provider for
sore throat. Primary reasons for patients with respi-
ratory tract infections visiting healthcare providers
include:
• To establish the cause of symptoms and disease
• To exclude serious illness (and seek reassurance)
• To obtain symptomatic relief
• To gain more information on the course and
duration of the disease (20).
Pharmacy staff tend to see patients who have
already chosen the self-management route. Their role
is important and diverse. They need to support this
approach by offering reassurance and advice on
appropriate treatment to increase the chances of
optimum symptomatic relief and patient satisfaction.
Furthermore, they need knowledge for patient-cen-
tred advice on when to consult another healthcare
provider.
Applying a structured approach to patient consul-
tations may help healthcare providers to fulfil these
roles in a time-efficient manner. Such a structured
approach could have the following components: (i)
Address patient’s concerns; (ii) Be vigilant; assess
severity; (iii) Counsel on effective self-management.
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 10–16
Sore throat: encourage self-care, reduce antibiotic use 118 8
8 8

Address patient’s concernsThe first task for prescribers and pharmacy staff is to
identify the concerns and expectations of the patient
(4). It is crucial not to trivialise patient complaints,
to listen with interest and to react to the patient with
tailored advice (23).
For prescribers, it is particularly important to
determine the primary reason for patients presenting
with sore throat and what their treatment expecta-
tions are. In practice, fewer patients want an antibi-
otic than some physicians believe (4). In a study by
van Driel et al., over 80% of patients who visited a
doctor for sore throat did so first and foremost to be
examined for the cause of their symptoms, to obtain
pain relief and/or to gain information on the course
of their condition (20). Antibiotics ranked 11th out
of 13 reasons in total. Further analysis indicated that
many patients who request an antibiotic may, in fact,
want an effective medication to relieve their pain, yet
mistakenly believe that they can achieve this quickly
with an antibiotic.
Be vigilant: assess severityAs the next step, primary care providers should eval-
uate the severity of the infection and the risk of
complications. This involves physical examination
for red-flag symptoms, asking questions about risk
factors for complications and symptom duration.
Pharmacy staff do not conduct a full consultation;
they should, however, be aware of an increased risk
for serious infection and, if necessary, refer the
patient to the primary care physician for further
evaluation, i.e. if symptoms get worse or last longer
than 2 weeks.
Medical-history taking and physical examination
by prescribers can be complemented by point-of-care
testing where this is available, to reassure both them-
selves and the patient that a non-antibiotic treatment
strategy is appropriate. A Dutch study reported that
patients with respiratory tract symptoms who were
carefully examined during a GP consultation were
more likely to be satisfied with their visit to the GP,
regardless of whether or not they had received anti-
biotics (13).
Counsel on effective self-managementAt this point of the consultation, after having
addressed patients’ concerns, history-taking and
physical examination, the key tasks for primary care
providers are to reassure patients that their condition
is self-limiting, to recommend symptomatic relief
and to advise on next steps.
Prescribers should encourage patients at low risk
to self-manage their condition without using antibi-
otics. Depending on the patient expectations identi-
fied at the beginning of the consultation, a more
detailed discussion about appropriate use of antibiot-
ics may be helpful, also highlighting the advantages
of not taking antibiotics, such as avoiding side effects
and a reduced likelihood that antibiotics will fail if
needed to treat a serious illness in future (23).
Another helpful approach is to stress the self-limiting
nature of the condition and explain that the patient’s
own immune system can deal with the infection.
Patients will also need and appreciate specific advice
on symptomatic treatment options and formulations
(Table 1) that meet their individual preferences.
Finally, patients benefit from information on the
expected course of the illness and on red-flag symp-
toms that warrant a return visit (4,23). Written
information can aid in this process by reinforcing
the GP’s face-to-face explanation.
The value of spending time with the patient and
providing information and reassurance is not to be
underestimated (23,24). In a survey by Welschen
et al., these factors were strongly linked to patient
satisfaction (25). In addition, directing patients to
effective self-care and providing information on the
expected duration of symptoms reduces re-consulta-
tion rates (23,26).
In a similar manner, pharmacy staff should reas-
sure patients that symptoms typically resolve within
one week. They should provide reassurance to
patients by offering more detailed advice on symp-
tomatic treatment options in line with the patient’s
primary concerns (fever, pain, swelling) and prefer-
ences. This will include information on suitable for-
mulations (Table 1) and on the correct use of any
purchased medication.
Patient communication
To facilitate a cultural change towards the appropri-
ate use of antibiotics for sore throat management,
healthcare providers need to communicate effectively
about self-limitedness of disease, appropriate treat-
ment and antibiotic resistance, and work towards
creating a partnership with the patient (22). Research
has shown that the way healthcare providers commu-
nicate with their patients has a strong impact on
treatment outcome and patient satisfaction. For
example, Thomas et al. report that better doctor–patient communication – with an increase in consul-
tation time from 6 to 10 minutes and improved
courtesy from the doctor – resulted in improved sore
throat management (8). In another study among
patients who visited a physician because of respira-
tory tract symptoms (24), there was no link between
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 10–16
12 Sore throat: encourage self-care, reduce antibiotic use9 9
9 9

a prescription for antibiotics and patient satisfaction;
however, satisfaction was associated with patients’
understanding their illness and the physician spend-
ing enough time with them, confirming the impor-
tance of effective communication and explanation.
Many patients lack awareness of when antibiotics
are appropriate. A useful strategy on which to focus
is the effect treatment has on symptoms, rather than
explaining bacterial or viral aspects. Nonetheless, it is
important to state that antibiotics will not clear a
viral infection, reduce symptoms or help the patient
recover more quickly – even in most cases of bacte-
rial infection; moreover, antibiotics may do more
harm than good by causing side effects (23). Many
patients are also not aware of the connection between
overuse of antibiotics and antibiotic resistance (18).
Healthcare providers need to inform patients that
antibiotic resistance can have serious consequences
both for the individual patient and for the commu-
nity, owing to the spread of resistant bacteria to fam-
ily members, work colleagues and friends (19).
In addition to providing patient education about
the appropriate use of antibiotics, healthcare provid-
ers and patients should work together to agree on a
treatment plan around patients’ individual needs and
concerns.
The use of non-paternalistic, patient-centred lan-
guage by both prescribers and pharmacy staff is a
key to the process of establishing such a partnership
approach. Communicating with empathy reassures
patients that their concerns have been taken seriously
and supports confidence in self-care. Patients will be
more likely to accept the rationale for a symptomatic
treatment approach and understand the risks of anti-
biotic use.
To be a participating partner in the management
of their sore throat symptoms, patients should be
empowered to:
• Assess their symptoms,
• Beat their symptoms and
• Care for themselves.
In practice, this means that patients should be
encouraged to assess their symptoms to be able to
give their primary care provider a good description
of their condition and any concerns.
In addition, patients should be encouraged to seek
the best medicines for their specific symptoms. To
help them in this process, primary care providers
need to help patients understand that there is a wide
range of therapeutic options available that provide
symptomatic relief and that pharmacy staff can help
in determining the medicines and formulations that
best suit their needs and preferences.
Finally, patients should be encouraged to take care
of themselves. Besides advice on effective symptom-
atic relief, rest and/or staying home from school or
work can possibly be advised.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Tailoring sore throat treatment
Formulation
Local
delivery Relieves pain
Anti-
inflammatory
effect
Demulcent
effect
Low dose,
reduced side
effect risk Note on formulation
Oral NSAIDs No Yes (28,29) Yes No No Slower action than local treatments (30)
Other analgesics No Yes (31,32) No No No Slower action than local treatments (30)
Local NSAID lozenge Yes Yes (33–36) Yes (34,35) Yes (33,34) Yes (33–36) Faster action than systemic treatments (30)
Can relieve pain in 2 min and last up to
4–6 h (35,35)
Local NSAID spray/gargle Yes Yes (37) Yes (37) No Yes (37) Faster action than systemic treatments (28)
Gargles are often swallowed and the
active ingredients do not reach the
throat (38)
Antiseptic/anaesthetic
lozenge
Yes Yes (39) No Yes (39) Yes (39) Faster action than systemic treatments (30)
Lozenges dissolve slowly to release
active ingredients (30)
Antiseptic/anaesthetic
spray/gargle
Yes Yes (30,40) No No Yes (30) Faster action than systemic treatments (30)
Antiseptic/anaesthetic
ear drops
Yes Yes (41) No No Yes (30) Acidic agent preferred for acute early stage
disease compared with topical/oral
antimicrobial agents (35)
Cough syrup Yes No No Yes (30) Yes Provides a cough suppressant (antitussive)
effect (39)
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 10–16
Sore throat: encourage self-care, reduce antibiotic use 1310 10
10 10

A successful intervention may then mean that the
patient will be able to self-manage sore throat symp-
toms in future.
Local education and support forprimary care providers: the 1,2,3toolkit
The campaign towards appropriate use of antibiotics
for the management of sore throat will only be effec-
tive if the outlined strategies are implemented in line
with local needs, with a consistent approach from
healthcare providers. There is a strong need for tar-
geted education of primary care providers in line
with local management, advice and prescribing prac-
tice. Secondly, patients visiting the GP or pharmacy
should be informed with written information about
non-antibiotic management of sore throat. Finally,
commitment from government and/or local health
authorities is required to support and promote the
benefits of self-management by symptomatic care
and the concept of antibiotic stewardship when man-
aging acute throat infections.
Nationwide recommendations and media cam-
paigns for appropriate use of antibiotics in URTIs
can be used as tools to communicate this issue to
patients. At the end of the 1990s, Finland demon-
strated that the campaign reduced not only the
amount of antibiotics prescribed but also decreased
the rate of erythromycin resistance (27).
It is also desirable to promote local educational
programmes where healthcare providers can share
data about prescription and consumption of thera-
pies for URTIs, and find out about the evidence and
information strategies that should be adopted.
Healthcare providers should use consistent commu-
nication with patients to promote patient confidence
in the advice they are given. Incongruent messages
among healthcare providers would likely result in
patients seeking a second opinion from another
healthcare provider, which could result in ineffective
management of the URTI and frustration.
To provide practical support in this complex pro-
cess, the GRIP team has developed a toolkit (Fig-
ure 1) with template materials for healthcare
providers and patients that can be adapted to meet
local needs. The materials include:
• A continuing professional development module
for primary care teams
• A pharmacy education tent cart (flip chart-style
booklet), which can be used by pharmacists when
training pharmacy staff, or serve as a general resource
on the management of URTIs for pharmacy teams
• Various patient-oriented materials (leaflet and pos-
ter) providing guidance on URTIs including expected
duration of symptoms and information on self-man-
agement
• A patient pressure conversation guide with picto-
grams to support the text, for prescribers when
Figure 1 GRIP Toolkit including template materials for healthcare providers and patients that can be adapted to meet
local needs
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 10–16
14 Sore throat: encourage self-care, reduce antibiotic use11 11
11 11

explaining to patients the non-prescribing of antibi-
otics
• A ‘non-prescription’ tear-off pad to be used by
prescribers to offer patients general information, as
well as individualised advice
The toolkit materials and further information on
GRIP are available on the GRIP website (www.
GRIP-initiative.com).
Conclusions
To address the problem of inappropriate antibiotic
use in primary care, many countries are now pro-
moting a self-care approach for the management of
self-limiting illnesses (4,23). Sore throat is a prime
example as the condition is caused by a virus in the
majority of patients, resolves within one week with-
out the need for antibiotics, and effective treatment
options are available to provide symptomatic relief.
As the first port of call for patients who seek med-
ical attention for sore throat, and other self-limiting
URTIs, primary care physicians and pharmacy team
members need to take an active approach to direct
patients towards self-management strategies. They
have an important role in educating patients on the
appropriate use of antibiotics; providing reassurance
that the condition is not serious, but self-limiting;
and advising that symptomatic treatment is the most
appropriate course of action. They need to work with
patients to create a personal self-management plan in
line with patient preferences. For this purpose,
patients’ expectations and concerns should be identi-
fied and addressed and serious infection must be
ruled out. A structured approach to patient consulta-
tions – (i) Address patient’s concerns; (ii) Be vigi-
lant; assess severity; (iii) Counsel on effective self-
management – will help healthcare providers to take
a consistent approach to the management of sore
throat and to put the patient at the centre of the
consultation. This approach, complemented by the
use of written patient information, will help to drive
patient confidence in self-care and, ultimately, aug-
ment efforts to reduce antibiotic prescribing in pri-
mary care for URTIs.
Disclosures
Publication of this supplement article was supported
as part of an unrestricted educational grant by Reckitt
Benckiser Group PLC. Editorial assistance during the
development and revision of this manuscript was
provided by Mash Health Limited and supported by
Reckitt Benckiser Group PLC.
Author contributions
The authors provided substantial contributions to
the development and revision of the manuscript and
approved the final version of the manuscript.
References
1 Centor RM, Samlowski R. Avoiding sore throat
morbidity and mortality: when is it not “just a sore
throat?”. Am Fam Physician 2011; 83(26): 28.
2 Oxford JS, Goossens H, Schedler M, Sefton A,
Sessa A, van der Velden A. Factors influencing
inappropriate antibiotic prescription in Europe.
Educ Prim Care 2013; 24: 291–3.
3 Worrall GJ. Acute sore throat. Can Fam Physician
2007; 53: 1961–2.
4 National Institute for Health and Clinical Excel-
lence (NICE). Clinical Guideline 69. Respiratory
tract infections – antibiotic prescribing. Prescribing
of antibiotics for self-limiting respiratory tract
infections and in adults and children in primary
care, July 2008. http://www.nice.org.uk/cg069
(accessed 12 September 2013).
5 Francis NA, Butler CC, Hood K, Simpson S, Wood
F, Nuttall J. Effect of using an interactive booklet
about childhood respiratory tract infections in pri-
mary care consultations on reconsulting and antibi-
otic prescribing: a cluster randomised controlled
trial. BMJ 2009; 339: b2885.
6 Centers for Disease Control and Prevention. Adult
appropriate antibiotic use summary. http://www.
cdc.gov/getsmart/campaign-materials/info-sheets/
adult-approp-summary.pdf (accessed September
2013).
7 Spinks A, Glasziou P, Del Mar CB. Antibiotics for
sore throat. Cochrane Database Syst Rev 2006; (4)
Art. No.: CD000023. DOI: 10.1002/14651858.
CD000023.pub3.
8 Thomas M, Del Mar C, Glasziou P. How effective
are treatments other than antibiotics for acute sore
throat? Br J Gen Pract 2000; 50: 817–20.
9 Aalbers J, O’Brien KK, Chan WS et al. Predicting
streptococcal pharyngitis in adults in primary care:
a systematic review of the diagnostic accuracy of
symptoms and signs and validation of the Centor
score. BMC Med 2011; 9: 67.
10 Shephard A, Smith G, Aspley S, Schachtel B. Effi-
cacy of Flurbiprofen 8.75 Mg Lozenges for Streptococ-
cal and Non-Streptococcal Sore Throat: Pooled
Analysis of Two Randomised, Placebo-Controlled
Studies. Berlin, Germany: ECCMID, 2013; P2085.
11 Bisno AL, Gerber MA, Gwaltney JM Jr, Kaplan EL,
Schwartz RH. Diagnosis and management of group
A streptococcal pharyngitis: a practice guideline.
Infectious Diseases Society of America. Clin Infect
Dis 1997; 25: 574–83.
12 Pelucchi C, Grigoryan L, Galeone C et al. Guideline
for the management of acute sore throat. Clin
Microbiol Infect 2012; 18(Suppl. 1): 1–28.
13 van Duijn HJ, Kuyvenhoven MM, Schellevis FG,
Verheij TJ. Illness behaviour and antibiotic pre-
scription in patients with respiratory tract symp-
toms. Br J Gen Pract 2007; 57: 561–8.
14 Borchardt RA, Rolston KV. Respiratory tract infec-
tions: emerging viral pathogens. JAAPA 2012; 25:
19–20.
15 Cals JW, Butler CC, Hopstaken RM, Hood K,
Dinant GJ. Effect of point of care testing for C
reactive protein and training in communication
skills on antibiotic use in lower respiratory tract
infections: cluster randomised trial. BMJ 2009; 338:
b1374.
16 Kenealy T, Arroll B. Antibiotics for the common
cold and acute purulent rhinitis. Cochrane Database
Syst Rev 2013; 6: CD000247.
17 Wilton L, Kollarova M, Heeley E, Shakir S. Relative
risk of vaginal candidiasis after use of antibiotics
compared with antidepressants in women: post-
marketing surveillance data in England. Drug Saf
2003; 26: 589–97.
18 Costelloe C, Metcalfe C, Lovering A, Mant D, Hay
AD. Effect of antibiotic prescribing in primary care
on antimicrobial resistance in individual patients:
systematic review and meta-analysis. BMJ 2010;
340: c2096.
19 Hildreth CJ, Burke AE, Glass RM. JAMA patient
page. Inappropriate use of antibiotics. JAMA 2009;
302: 816.
20 van Driel ML, De Sutter A, Deveugele M et al. Are
sore throat patients who hope for antibiotics actu-
ally asking for pain relief? Ann Fam Med 2006; 4:
494–9.
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 10–16
Sore throat: encourage self-care, reduce antibiotic use 1512 12
12 12

21 van Gageldonk-Lafeber AB, Heijnen ML, Bartelds
AI, Peters MF, van der Plas SM, Wilbrink B. A
case-control study of acute respiratory tract infec-
tion in general practice patients in The Nether-
lands. Clin Infect Dis 2005; 41: 490–7.
22 van der Velden A, Duerden MG, Bell J et al. Pre-
scriber and patient responsibilities in treatment of
acute respiratory tract infections – essential for con-
servation of antibiotics. Antibiotics 2013; 2: 316–27.
23 NPS. NPS News 63: Managing expectations for anti-
biotics in respiratory tract infections. June 2009.
http://www.nps.org.au/__data/assets/pdf_file/0009/
71478/news_63.pdf (accessed 12 September 2013).
24 Hamm RM, Hicks RJ, Bemben DA. Antibiotics and
respiratory infections: are patients more satisfied
when expectations are met? J Fam Pract 1996; 43:
56–62.
25 Welschen I, Kuyvenhoven M, Hoes A, Verheij T.
Antibiotics for acute respiratory tract symptoms:
patients’ expectations, GPs’ management and
patient satisfaction. Fam Pract 2004; 21: 234–7.
26 Little P, Gould C, Williamson I, Warner G, Gantley
M, Kinmonth AL. Reattendance and complications
in a randomised trial of prescribing strategies for
sore throat: the medicalising effect of prescribing
antibiotics. BMJ 1997; 315: 350–2.
27 Sepp€al€a H, Klaukka T, Vuopio-Varkila J et al. The
effect of changes in the consumption of macrolide
antibiotics on erythromycin resistance in group A
streptococci in Finland. Finnish Study Group for
Antimicrobial Resistance. N Engl J Med 1997; 337:
441–6.
28 Burian M, Geisslinger G. COX-dependent mecha-
nisms involved in the antinociceptive action of
NSAIDs at central and peripheral sites. Pharmacol
Ther 2005; 107: 139–54.
29 Rainsford KD. Ibuprofen: from invention to an
OTC therapeutic mainstay. Int J Clin Pract Suppl
2013; 178: 9–20.
30 Oxford JS, Leuwer M. Acute sore throat revisited:
clinical and experimental evidence for the efficacy
of over-the-counter AMC/DCBA throat lozenges.
Int J Clin Pract 2011; 65: 524–30.
31 Graham GG, Scott KF. Mechanism of action of
paracetamol. Am J Ther 2005; 12: 46–55.
32 Derry S, Moore RA, McQuay HJ. Single dose oral
codeine, as a single agent, for acute postoperative
pain in adults. Cochrane Database Syst Rev 2010;
(4). Art. No.: CD008099. DOI: 10.1002/146518
58.CD008099.pub2.
33 Blagden M, Christian J, Miller K, Charlesworth A.
Multidose flurbiprofen 8.75 mg lozenges in the
treatment of sore throat: a randomised, dou-
ble-blind, placebo-controlled study in UK general
practice centres. Int J Clin Pract 2002; 56: 95–100.
34 Watson N, Nimmo WS, Christian J, Charlesworth
A, Speight J, Miller K. Relief of sore throat with
the anti-inflammatory throat lozenge flurbiprofen
8.75 mg: a randomised, double-blind, placebo-con-
trolled study of efficacy and safety. Int J Clin Pract
2000; 54: 490–6.
35 Benrimoj SI, Langford FH, Christian F, Charles-
worth A, Steans A. Efficacy and tolerability of the
anti-inflammatory throat lozenges Flurbiprofen
8.75mg in the treatment of sore throat. A rando-
mised, double-blind, placebo-controlled study. Clin
Drug Invest 2001; 21: 183–93.
36 Schachtel BP, Aspley S, Sternberg M et al. Onset of
demulcent and analgesic activity of flurbiprofen
lozenge. Int J Clin Pharm 2012; 34: 143–258.
37 Pass�ali D, Volont�e M, Pass�ali GC, Damiani V, Bell-
ussi L, Group MIS. Efficacy and safety of ketopro-
fen lysine salt mouthwash versus benzydamine
hydrochloride mouthwash in acute pharyngeal
inflammation: a randomized, single-blind study.
Clin Ther 2001; 23: 1508–18.
38 Limb M, Connor A, Pickford M et al. Scintigraphy
can be used to compare delivery of sore throat for-
mulations. Int J Clin Pract 2009; 63: 606–12.
39 Wade AG, Morris C, Shephard A, Crawford GM,
Goulder MA. A multicentre, randomised, dou-
ble-blind, single-dose study assessing the efficacy of
AMC/DCBA Warm lozenge or AMC/DCBA Cool
lozenge in the relief of acute sore throat. BMC Fam
Pract 2011; 12: 6.
40 Buchholz V, Leuwer M, Ahrens J, Foadi N,
Krampfl K, Haeseler G. Topical antiseptics for the
treatment of sore throat block voltage-gated neuro-
nal sodium channels in a local anaesthetic-like
manner. Naunyn Schmiedebergs Arch Pharmacol
2009; 380: 161–8.
41 Prasad S, Ewigman B. Use anesthetic drops to relieve
acute otitis media pain. J Fam Pract 2008; 57: 370–3.
Paper received September 2013, accepted September 2013
ª 2013 John Wiley & Sons Ltd Int J Clin Pract, November 2013, 67 (Suppl. 180), 10–16
16 Sore throat: encourage self-care, reduce antibiotic use13 13
13 13

More action, less resistance: report of the 2014 summit ofthe Global Respiratory Infection PartnershipAttila Altinera, John Bellb, Martin Duerdenc, Sabiha Essackd, Roman Kozlove, Laura Noonanf,John Oxfordg, Antonio Carlos Pignatarih, Aurelio Sessai and Alike van der Veldenj
aInstitute of General Practice, University of Rostock, Rostock, Germany, bGraduate School of Health, University of Technology, Sydney, NSW, Australia,cSchool of Medical Sciences, Bangor University, Bangor, gQueen Mary’s School of Medicine and Dentistry, Barts and The London School of Medicineand Dentistry, St Bartholomew’s and the Royal London Hospital, Queen Mary’s School of Medicine and Dentistry, London, UK, dSchool of HealthSciences, University of KwaZulu-Natal, Durban, South Africa, eInstitute of Antimicrobial Chemotherapy, Smolensk State Medical Academy, Smolensk,Russian Federation, fSchool of Medicine, National University of Ireland, Galway, Ireland, hDepartment of Medicine, Division of Infectious Diseases,Federal University of Sao Paulo, Sao Paulo, Brazil, iSocietà Italiana di Medicina Generale, Arcisate, Italy and jUniversity Medical Center, UtrechtUniversity, Utrecht, The Netherlands
Keywordsantibiotics; community pharmacy; delivery ofcare; inappropriate prescribing; OTC medicines
CorrespondenceProfessor Sabiha Essack, B. Pharm., M. Pharm.,PhD, Dean: Teaching & Learning, College ofHealth Sciences, Professor: PharmaceuticalSciences, School of Health Sciences, Universityof KwaZulu-Natal, Private Bag X54001,Durban, 4000, South Africa.E-mail: [email protected]
Received November 12, 2014Accepted December 4, 2014
doi: 10.1111/ijpp.12177
Abstract‘Antimicrobial resistance is a global health security threat that requires concertedcross-sectional action by governments and society as a whole,’ according to a reportpublished by the WHO in April 2014[1]. On 24–25 June 2014, the Global RespiratoryInfection Partnership (GRIP) met in London, UK, together with delegates from 18different countries to discuss practical steps that can be taken at a local level toaddress this global problem in an aligned approach.
This was the second annual summit of GRIP. The group, formed in 2012, includesprimary care and hospital physicians, microbiologists, researchers, and pharmacistsfrom nine core countries. GRIP aims to unite healthcare professionals (HCPs)around the world to take action against inappropriate antibiotic use, focussing onone of the most prevalent therapy areas where antibiotics are inappropriatelyprescribed – upper respiratory tract infections (URTIs).
Chaired by GRIP member, Professor John Oxford (UK), the 2014 summitincluded engaging presentations by guest speakers examining the latest scienceregarding the impact of inappropriate antibiotic use.
Guest Speaker Presentations
Antibiotic stewardship: more action,less resistance
Opening the meeting, guest speaker Professor Stuart Levy,Professor of Molecular Biology and Microbiology and ofMedicine, and Director of the Centre for AdaptationGenetics and Drug Resistance at Tufts University Schoolof Medicine, made a strong case for antibiotic resistancebeing an environmental and societal problem, as well as amedical one.
Professor Levy reinforced the fact that resistance to multi-ple antibiotics is now not just a problem in the hospital butcommon in the community, making it difficult to control itsspread. The consequences of this spread are alarming. Resist-ance leading to treatment failure and/or deaths affects a vast
array of medical conditions and procedures including cancer,pneumonia, infant bloodstream infections and organ trans-plantations. Use of a single antibiotic can result in multidrugresistance, as bacteria tend to accumulate resistances. Onceselected, a drug resistance will not disappear again, heemphasised, although it may drop in frequency.
Antibiotic resistance develops wherever antibiotics areused – in agriculture as much as in healthcare. A major con-tributor is the use of antibiotics at subtherapeutic doses topromote growth in food animals. ‘Given enough antibioticand time, resistance will appear,’ said Professor Levy.
The effect of antibiotic resistance on both humans andagriculture – and their interaction – makes this an environ-mental problem. Resistant bacteria are transmitted fromhumans to animals and vice versa; they also enter water andsoil; are dispersed to fruit, vegetables and wildlife; and aretransferred back to humans and food animals (Figure 1).
bs_bs_banner
International Journal of
Pharmacy PracticeInternational Journal of Pharmacy Practice 2015, ••, pp. ••–••
Conference Report
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
14 14
14 14

‘Antibiotics are societal drugs’, said Professor Levy. Peoplein close contact with a person using antibiotics have beenfound to carry bacterial strains resistant to both single andmultiple antibiotics, he explained.[2] This implies that indi-vidual use of antibiotics affects family, the community andsociety as a whole.
Professor Levy called for greater antimicrobial stewardshipby preventing infections, tracking resistance patterns, devel-oping rapid diagnostic methods, and improving the use ofantibiotics. Conversely, regarding the frequent use of the term‘war on antibiotics’, Professor Levy suggested an alternativeview of the challenge: ‘We have to make peace with bacteria.They are the ones that have survived and that will survive.’
The human microbiome and antibiotics
Professor Thomas MacDonald, Professor of Immunologyand Dean for Research at Barts and The London School ofMedicine and Dentistry, gave a presentation on the effectsof antibiotics on the highly balanced ecosystem of thecommensal bacteria in the gut.
The huge surface area of the gut is populated by some 500species of bacteria, with the whole microbiome having apopulation of approximately 1014 organisms. The specificcomposition of the microbiota community differs fromindividual to individual and is imprinted early in life.
The commensal bacteria in the gut have a variety of struc-tural, metabolic and protective functions including barrierfortification, vitamin synthesis, salvage of energy from food
and pathogen displacement.[3] They are also essential for ahealthy immune system, with gut-associated lymphoid tissuecomprising 70% of the entire human immune system.Evidence from germ-free mice shows that bacterial colonisa-tion of the gut is prerequisite for the development ofthe immune system, in particular the early induction ofimmunoglobulin A in neonates.[3] ‘There is absolutely nodoubt that the activation and development of systemic andmucosal immunity and the tissues involved in it are driven bythe presence of the microbiota’, said Professor MacDonald.
What does this mean for treatment with antibiotics? Pro-fessor MacDonald presented research showing that the use ofantibiotics leads to a loss of diversity and a shift in communitycomposition of the gut microbiota.[4] The microbiota stabi-lise again once the antibiotics have stopped, but it neverreturns to its original state.
The exact consequences of this shift are unknown, butthere is mounting evidence that the composition of the gutmicroflora has a direct impact on the body’s ability to fightinfections, said Professor MacDonald. For example, signalsfrom the microbiota promote the differentiation of T cellsresiding in the intestinal epithelia – in particular the popula-tion of Th17 cells.[5] Ironically, this subset of T helper cells isresponsible for protecting the body against bacteria andfungi.
This implies the paradox that taking antibiotics to clear aninfection will simultaneously destroy the body’s naturaldefence mechanisms against infection, and in some individ-uals, this damage may be permanent. It is therefore crucial to
Figure 1 Ecological impact of antibiotics in agriculture (Alliance for the Prudent Use of Antibiotics [APUA]).
2 Meeting report
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
15 15
15 15

avoid the use of antibiotics unless this is clearly indicated bythe nature and severity of the infection.
Sessions Led by GRIP Members
Global guidance in URTI management
GRIP’s approach to tackling antibiotic resistance is based onthe premise that inappropriate use of antibiotics for URTIs, inparticular sore throat, is a key driver for increasing antibioticresistance rates in the community and that effective actionrequires a consistent approach across healthcare professionsand countries.[6,7] GRIP members, Dr Alike van der Velden(the Netherlands) and Professor Roman Kozlov (Russia),addressed the challenges that make it necessary to establish aunified approach.
The challenges to a unified approach
National guidelines on the management of sore throat varyenormously between countries to the extent that differentstrategies are recommended for the symptoms around theworld. For example, the American Association of FamilyPractitioner guidelines[8] recommend that patients with posi-tive throat cultures should be treated with antibiotics regard-less of severity of infection or ability of the patient to fight offthe infection, whereas guidelines in the Netherlands (NHGguideline) focus on the distinction between mild and severethroat infections.
A second challenge is the variation in antibiotic resistancerates between countries, highlighting the influence of socialand cultural factors on attitudes towards antibiotic use.
Thirdly, there is a gap between the knowledge and skillsrequired by HCPs and the education they receive on prudentantimicrobial prescribing.‘Topics such as bacterial resistance;diagnosis, treatment and prevention of infection; antimicro-bial stewardship and communication skills receive insuffi-cient attention in the curricula of HCPs’, said ProfessorKozlov.
Additional challenges include differences between coun-tries in time allocated for patient consultations and variationsin knowledge level regarding antibiotics and the naturalcourse of URTIs among the general public.
5P framework – a globalcollaborative approach
To address the variation in global antibiotic use guidelines,GRIP has developed a framework for the management ofURTIs in primary care that can be adapted across countries.The framework involves a collaborative approach by multiplestakeholders and focuses on five key areas: policy, prevention,prescribers, pharmacy teams, and patients (Figure 2).[9]
GRIP believes that much can be achieved by addressing theinteraction between HCPs and their patients. The group hasdeveloped the 1, 2, 3 approach in order to provide a struc-tured approach for the consultations, and to help the HCPeffectively treat and communicate with their patients(Table 1).
Briefly, step 1 involves identifying and addressing patientconcerns and expectations. During step 2, the severity of thecondition is assessed, with attention being paid to risk factorsfor complications. In step 3, the HCP provides counselling oneffective self-management options.
Dr van der Velden emphasised that this universal approachcan be adapted for use in any local environment, regardless ofguideline variations between countries, resistance patterns ormedical curricula. She presented to the delegates a consulta-tion algorithm designed to assist prescribers and pharmacistsin applying the 1, 2, 3 approach when engaging with sorethroat patients. The algorithm includes questions andprompts for each step of the approach and is developed in linewith the structured 1, 2, 3 approach. The algorithm – alongwith other GRIP materials – is available on the GRIP websiteat www.grip-initiative.org.
More action – the latest support from GRIP
Throughout the past 3 years, GRIP has developed a series ofresources for HCPs and patients to support their initiative.GRIP members Dr Martin Duerden (UK) and ProfessorSabiha Essack (South Africa) provided an overview of thesematerials and how they can help support HCPs in managingpatients with URTIs (Figure 3).
Figure 2 Global Respiratory Infection Partnership (GRIP)’s pentagonalframework for change in antibiotic use.
Attila Altiner et al. 3
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
16 16
16 16

GRIP’s 1, 2, 3 toolkit resources – launched last year –provide a plethora of useful materials that help educate theHCP on the need to change behaviour, the value of managingsymptoms and guidance on communicating with patients inline with the GRIP 1, 2, 3 approach. The resources alsoincluded patient materials, which help provide guidance onthe realistic duration of URTI symptoms, reassurance thatappropriate symptomatic relief can meet their needs andguidance on when to seek further advice. The resources aredesigned to be adaptable for local use while maintaining theconsistency of GRIP’s approach.
Dr Duerden and Professor Essack launched new GRIP2014 materials, which aim to complement the existing 2013materials. The new 2014 materials included continuing pro-fessional development (CPD) modules, covering antibioticresistance, URTI management in primary care and commu-nication skills – the activities of which can be logged as part ofhealthcare provider personal development points. Patientmaterials were also launched, further helping to shape shareddecision-making during the consultation. Much of these
patient materials not only helped provide the relevantreassurance and reasoning for why antibiotics do not helpmanage symptoms in the majority of cases, but also em-powered the patients in providing the right tools tohelp HCPs choose the most appropriate treatment for theircondition.
Consultation skills
An interactive session run by GRIP members Dr Duerdenand Mr John Bell (Australia) looked into consultation skills.Dr Duerden emphasised that effective communicationbetween the HCP and the patient is a skill that can be learnt,just as much as other medical skills. He recommended givinga structure to the consultation, for example using theCalgary–Cambridge model: (1) initiating the session; (2)gathering information; (3) building the relationship; (4)explaining and planning; and (5) closing the session.[10,11]
Mr Bell discussed the role of pharmacy engagement intreating patients with URTIs, emphasising the need for phar-macy teams to move away from a paternalistic approach to acollaborative partnership that endeavours to place the patientat the centre of the decision-making process. He re-enforcedthe importance of explaining symptom duration – along withreasoning as to why a visit to the doctor was not important–and how it is vital to advise the patient on the most effectivesymptomatic relief options in order to cater for specificsymptoms and preferences. Mr Bell touched on theimportance of medicine optimisation when antibiotics areneeded, re-enforcing messaging on antibiotic resistance withreasoning for appropriate course fulfilment.
Observation of certain ground rules can also help tomake the interaction more effective by helping elicit thepatient’s problems and concerns. Tips included sitting at aright angle from the patient, maintaining a comfortablelevel of eye contact and using verbal signposting to separatelistening from note reading. A particularly powerful skill isto allow the patient to complete the opening statementwithout interruption – this can lead to a significant reduc-
Table 1 Using the 1, 2, 3 step approach for sore throat
1. Address the patient’s concerns• Identify the patient’s main symptom or concern and ascertain how unwell they are• Doctors should perform a clinical assessment of the head and neck. Check glands and tonsils
2. Be vigilant – assess severity• For doctors: use the Centor criteria to identify risk of group A beta-haemolytic streptococci (GABHA) and identify potential risk factors• For pharmacy: identify risk factors, co-morbidities and/or red flag symptoms and refer when needed
3. Counsel on effective self-management• Provide reassurance for the patient with information on the duration of symptoms, recommend symptomatic relief and, if required, advise the
patient when they should see a doctor or return for a reconsultation• Explain why antibiotics are not needed together with the benefits that symptomatic relief can provide• The pharmacy can help explain to patients the range of symptomatic relief products available
Figure 3 Global Respiratory Infection Partnership (GRIP)’s 1, 2, 3 toolkitmaterials, available on the GRIP website: www.grip-initiative.org.
4 Meeting report
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
17 17
17 17

tion in late-arising problems. After a review of the phrasesthat HCPs can use to explore patient’s ideas, concerns andexpectations (the ICE approach), the speakers demonstratedin two role play scenarios how physicians and pharmacistscan apply GRIP’s 1, 2, 3 approach during a patientconsultation for sore throat.
Interventions in practice
In another interactive session, GRIP members Dr LauraNoonan (Ireland) and Dr Aurelio Sessa (Italy) encourageddelegates to implement and evaluate interventions to reduceantibiotic prescribing in their local community practices.
Dr Noonan described her experience of testing the effec-tiveness of a take-home patient information leaflet thatcontained information on viral illnesses, antibiotics andantibiotic resistance, the likely duration of symptoms, andinformation on when to reconsult; the leaflet could bepersonalised and signed by the general practitioner (GP).
What were the results of the study?
Use of the leaflet resulted in a reduction of immediate anti-biotic prescriptions from 47.5% to 13.3%; it also reduced themean duration of consultations from 11 min to 10 min, andreconsultation rates dropped from 7.5% to 6.6%. These arethe results of a study Dr Noonan conducted at two rural GPpractices in Ireland, involving a 1-week control period duringwhich consultations for URTIs proceeded as usual, and a1-week intervention period during which the informationleaflet was used. The findings confirmed the value of givingpatients something tangible to take home to support anonantibiotic management approach.
Dr Sessa reported on the impact of introducing the use ofthe GRIP toolkit materials in his GP group practice in north-ern Italy. He conducted a study in which GPs could choose touse materials from the GRIP toolkit or to conduct the consul-tation without such materials. The results found that the useof the toolkit materials halved the number of antibioticprescriptions, as shown in Table 2.
The study protocol used by Dr Sessa, together with tem-plate data collection forms, is available from the GRIP website(www.grip-initiative.org). The group are keen for other prac-
titioners to use it to gather further data on the differences thatthe materials can make in actual practice. The study resultscan also help GP practices to evaluate whether their currentlevel of antibiotic use is appropriate.
Local Activation
In this session, practitioners from three different countriesshared their efforts to promote the principles of antibioticstewardship at a local level. These talks gave insight into howstrategies can be tailored to local needs and opportunities,and how successful implementation can result in substantialsuccess within localities.
Brazil
In Brazil, a new regulation was introduced in 2010 to stop thewidespread sale of antibiotics without prescription. Giventhis relatively recent change in policy, GRIP member Profes-sor Antonio Pignatari and ENT specialist Professor MônicaMenon decided to target opinion makers and prescribers byholding interactive symposia at key congresses in the country.The first symposium took place at a national congress forENT specialists in November 2013 and the second at aregional congress for GPs in April 2014. Delegates receivedinformation about appropriate antibiotic prescribing and theGRIP initiative (Table 3).
Both symposia were well received, and Professor Menonand Professor Pignatari are planning further talks at con-gresses and other relevant meetings, in addition to introduc-ing the concept of antibiotic stewardship in trainingprogrammes for hospital staff. There are also plans to reach
Table 2 Impact of GRIP toolkit use on antibiotic prescribing at a GPgroup practice in Italy
Toolkit use
Antibioticprescription,n = 70
No antibioticprescription,n = 115
P value (χ2)(%) (%)
Yes 22 (31.4) 53 (46.1) 0.056 (3.55)No 48 (68.6) 62 (53.9)
GP, general practitioner; GRIP, Global Respiratory Infection Partnership.
Table 3 Feedback of the GRIP message in Brazil
• ABORL Symposium• National ENT congress – 19–22/11/2014*
• 100% of the audience rated the GRIP idea as a very good idea• 49.9% like GRIP as every step helps to combat the inappropriate
use of antibiotics• 50.1% think it is crucial for GRIP to develop good material• 94.6% would like to receive more information for their patients
to help them use antibiotics correctly for the treatment of URTI• Clinica Medica Symposium, São Paulo
• Regional Congress for GPs in São Paulo – 4–5/4/2014†
• 78% rated the presentations as excellent to very good• 85% stated that antibiotic resistance is a problem in their daily
practice• There was a 100% agreement towards the statement that it is
not always necessary to prescribe an antibiotic for an URTI
*Sixty participants filled in a questionnaire. †A total of 107 participantsfilled in a questionnaire.GRIP, Global Respiratory Infection Partnership; ABORL, AssociaçãoBrasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial; ENT, Ear,Nose and Throat; GP, General Practitioner; URTI, Upper Respiratory TractInfection.
Attila Altiner et al. 5
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
18 18
18 18

wider audiences by publishing short articles in professionaljournals and hospital magazines.
United Kingdom
Dr Terry Maguire, a community pharmacist and health com-missioner from Northern Ireland, spoke about the promotionof antibiotic stewardship collaborating with existing publichealth initiatives. Examples for Northern Ireland include theMinor Ailments Scheme (promoting self-management ofminor ailments) and the Choose Well campaign (promotingbetter use of medicines, including antibiotics).
In addition, the Primary Care Intranet and other healthauthority websites in Northern Ireland are being used to giveGPs access to relevant patient information leaflets. GPs canalso download an audit template that has been adapted forthe audit of antibiotic prescribing.
Finally, Antibiotics Awareness Day 2013 offered the oppor-tunity to launch a CPD module for pharmacists and to sendantibiotic awareness resources to GP surgeries across the UK;the materials had been adapted from the GRIP 1, 2, 3 toolkitand were rated as good or excellent by 98% of responders.
5P Debate
The meeting ended with a stimulating debate that focussedon the question ‘which of the five Ps in GRIP’s pentagonalframework for change will have the biggest impact on coun-tering inappropriate antibiotic use in management of URTIsin primary care’. In an election panel style, each P was repre-sented by two GRIP members seeking to show the merits oftheir P over the other Ps.
In an audience vote before the debate, there was a clearwinner, with 33% of the audience feeling that the ‘prescriber’has the most influence on inappropriate antibiotic use, aheadof ‘patients’ (27%), ‘policy’ (23%), ‘prevention’ (10%) and,finally, ‘pharmacy’ (6%) (Figure 4).
Subsequently, the discussion began with a short openingpresentation for each P, followed by a debate in which eachteam defended its P.• Policy: The policy team argued that it is not possible to sub-
stantially affect antibiotic prescribing and purchasingbehaviours without national guidelines supported byregulation and antibiotic surveillance systems.
• Prevention: Those campaigning for prevention called for agreater ‘use of prevention strategies (so that) you won’tneed to treat the patient’.
• Prescriber: The prescriber team said that ‘[d]octors holdthe key’, and that ‘[t]hey are the ones who stand between thepatient and the antibiotic’.
• Pharmacy: The defenders of pharmacy asserted that phar-macists are more accessible than any other health profes-sionals and are most suited to provide individualised andtailored treatment advice.
• Patients: Arguments in favour of the P for patients includedthe fact that patients are often driving prescribing, and ulti-mately, they make the decision of whether to take the anti-biotic. ‘If we teach [a patient] to treat one sore throatinfection symptomatically, a large number of subsequentinfections will also be treated without antibiotics.’The debate ended with another vote by the audience, which
resulted in a tie between prescribers and patients (26% each),followed closely by pharmacy (23%) and policy (19%), andfinally prevention (6%) (Figure 5).
0%
5%
10%
15%
20%
25%
30%
35%
Policy Preven�on Prescriber Pharmacy Pa�ents
23%
10%
33%
6%
27%
Figure 4 The results from the initial vote on which ‘P’ was considered the strongest driver.
6 Meeting report
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
19 19
19 19

‘We have seen an equalisation and that’s a very good result,’said GRIP member Professor Attila Altiner (Germany). Heemphasised that all Ps are important, confirming the need forpartnership – a topic that came up repeatedly during thedebate and in audience contributions. ‘We have to work handin hand,’ concluded Professor Altiner.
You can access the edited recordings of the debate from theGRIP Summit at www.grip-initiative.org.
Localisation of Approach
The GRIP 2014 materials were reviewed by the assembledaudience of international HCPs. The attendees were brokendown into regions and discussed in detail how these materialscould be utilised and implemented in order to engage anddeliver a sustainable message to enact change. Feedback fromall the materials was positive, with many countries discussinghow to adapt and evolve the existing materials in order tocater for their region’s specific barriers to change.
The GRIP patient leaflet, URTI guide for patients andGRIP video brought significant praise from the audience. Itwas felt that the GRIP patient leaflet and URTI guide forpatients (a guide which the patient fills out prior to the con-sultation and allows them to detail their symptoms, durationsand reasons for visiting the HCP) were excellent tools to helpdrive the joint decision-making process. It was felt that theGRIP video – which follows the character of Bob who is suf-fering from an URTI – resonates with the apprehension felt bymany patients and greatly explains the importance of
effective symptomatic relief in a clear, concise and humorousformat.
The GRIP resources are available for download by all HCPson the GRIP website: www.grip-initiative.org. There areadditional resources on the website including the 2013 GRIPmaterials, podcasts (Table 4) and the debate footage. Abespoke GRIP YouTube channel page has also been launched,which includes interactive footage on the GRIP members’thoughts on the 5P framework and the 1, 2, 3 approach, thethreat of antibiotic resistance, and the challenges facingeffective and appropriate URTI management (Table 4).
Declarations
Conflict of interest
The Author(s) declare(s) that they have no conflicts ofinterest to disclose.
0%
5%
10%
15%
20%
25%
30%
Policy Preven�on Prescriber Pharmacy Pa�ents
19%
6%
26%
23%
26%
Figure 5 The results of the second vote regarding the most pertinent ‘P’, following the debate.
Table 4 The podcasts – involving members of GRIP – explore the diversechallenges that affect antibiotic prescription within the community. Thetone is personal and educational and delves into the speakers’ personalexperiences in dealing with such situations
• Antibiotic prescription for children – challenges and communication –Dr Alike van der Velden and Professor Attila Altiner
• Effective treatment of URTI’s – Dr Laura Noonan and Mr John Bell• Antibiotic prescription for adults – challenges and communication –
Dr Laura Noonan and Professor Attila Altiner
Attila Altiner et al. 7
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
20 20
20 20

Funding
The Global Respiratory Infection Partnership was convenedby RB. All materials were sponsored by and developed inpartnership with RB Healthcare. The views expressed inthe materials are those of the Partnership.
Authors’ contributions
All Authors state that they had complete access to the studydata that support the publication. All listed individuals wereattendees at the meeting and members of the Global Respira-tory Infection Partnership.
References
1. World Health Organization. Antimicro-bial Resistance. Global Report on Sur-veillance. Geneva, Switzerland: WHO,2014.
2. Miller YW et al. Sequential antibiotictherapy for acne promotes the carriageof resistant staphylococci on the skin ofcontacts. J Antimicrob Chemother 1996;38: 829–837.
3. Grenham S et al. Brain–gut–microbecommunication in health and disease.Front Physiol 2011; 2: 94. doi: 10.3389/fphys.2011.00094
4. Dethlefsen L, Relman DA. Incompleterecovery and individualized responsesof the human distal gut microbiota to
repeated antibiotic perturbation. ProcNatl Acad Sci U S A 2011; 108(Suppl. 1):4554–4561.
5. Ivanov II et al. Specific microbiotadirect the differentiation of IL-17-producing T-helper cells in the mucosaof the small intestine. Cell Host Microbe2008; 4: 337–349.
6. van der Velden AW et al. Prescriber andpatient responsibilities in treatment ofacute respiratory tract infections –essential for conservation of antibiot-ics. Antibiotics 2013; 2: 316–327.
7. van der Velden AW et al. Sore throat:effective communication deliversimproved diagnosis, enhanced self-careand more rational use of antibiotics. IntJ Clin Pract Suppl 2013; 180: 10–16.
8. American Academy of Family Physi-cians. Diagnosis and treatment ofstreptococcal pharyngitis. Am FamPhysician 2009; 79: 383–390.
9. Essack S, Pignatari AC. A frameworkfor the non-antibiotic management ofupper respiratory tract infections:towards a global change in antibioticresistance. Int J Clin Pract Suppl 2013;180: 4–9.
10. Kurtz S et al. Teaching and LearningCommunication Skills in Medicine.Oxford: Radcliffe Medical Press, 1998.
11. Silverman J et al. Skills for Communica-tion with Patients, 2nd edn. Oxford:Radcliffe Publishing, 2005.
8 Meeting report
© 2015 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2015, ••, pp. ••–••
21 21
21 21