Zoë Dowling, University of Surrey Kristin Stettler, US Census Bureau

A framework for the evaluation of quality of care in
maternity services
Louise A Hulton Zoë Matthews
R William Stones
‘The question should not be why dowomen not accept the service that we
offer, but why do we not offer a servicethat women will accept?’
Mahmoud F. Fathalla 1998Professor of Obstetrics and Gynaecology, Assiut University, Egypt
Published by University of Southampton 2000HighfieldSouthamptonSO17 1BJwww.socstats.soton.ac.uk/choices/
ISBN: 085432702 9

ContentsAcknowledgements
The authors
This work was carried out as part of a researchproject on maternal health in India sponsoredby the Wellcome Trust. The authors would liketo thank the following people for their help andcomments on various drafts of the text; MargeBerer, Libby Willis, Carolina Montoro-Gurich,Shelah Bloom, Judith Fortney, Jean Robinson,Maya Unnithan and Carine Ronsmans. Thework was also made possible by support fromthe following bodies; the Parkes Foundation,the Economic and Social Research Council, theSocial Sciences Faculty at the University ofSouthampton and the Department forInternational Development. Opportunities andChoices, a knowledge programme onreproductive health in developing countriesfunded by the Department for InternationalDevelopment based at SouthamptonUniversity, has also supported the productionand distribution of this monograph. Viewsexpressed in this publication are, however,solely the responsibility of the authors.
Louise Hulton is a researcher and occasionallecturer in the Department of Social Statistics atthe University of Southampton, currentlyworking on health-seeking behaviour amongthe urban poor of Mumbai. She has previouslyworked on AIDS research in sub-Saharan Africaand maternal health care in rural India. She isalso the secretary of AIMS (Association forImprovements in Maternity Services), UK. Herwork on quality in maternal health care isdedicated to the birth of her daughter Ella.
Zoë Matthews is a researcher and lecturer inDemography in the Department in SocialStatistics at the University of Southampton. Shehas research interests in reproductive and childhealth in developing countries, with particularemphasis on maternal health in South Asia.
R.William Stones presently holds theappointment of Senior Lecturer in Obstetricsand Gynaecology, University of Southamptonand Consultant, Southampton UniversityHospitals NHS Trust. He has research interestsin interdisciplinary work on women'sreproductive health including pelvic pain,contraception and maternity services and alsoin laboratory studies of human ovarian vascularbiology.
1 Introduction .........................................................................................................................................................................................................................1
2 Background............................................................................................................................................................................................................................3
3 Quality of Care .............................................................................................................................................................................................................5
3.1 Why is Quality Important? ...........................................................................................................................................................53.2 A Reproductive Health Approach ..................................................................................................................................7
4 What is Quality? .........................................................................................................................................................................................................9
5 Quality of Care Framework .............................................................................................................................................................10
5.1 Ten Elements of Care .......................................................................................................................................................................105.2 Criteria and Standards .....................................................................................................................................................................115.3 Indicators..................................................................................................................................................................................................................125.4 Data Collection ............................................................................................................................................................................................14
6 Expanded Quality Assessment Framework .........................................................................................................18
6.1 Provision of Care.......................................................................................................................................................................................196.1.1 Human and Physical Resources6.1.2 Referral6.1.3 Maternity Information Systems6.1.4 Appropriate Technologies6.1.5 Internationally Recognised Good Practice6.1.6 Management of Emergencies
6.2 Experience of Care ...............................................................................................................................................................................386.2.1 Human and Physical Resources6.2.2 Cognition6.2.3 Respect, Dignity and Equity6.2.4 Emotional Support
7 Use of the Framework ...............................................................................................................47
8 Implementing Change ..................................................................................................................49
9 Conclusion..........................................................................................................................................50
Appendix ....................................................................................................................51
Bibliography ...............................................................................................................67

1 Introduction
1
The existence of maternal healthservices does not guarantee their useby women. Neither does the use ofmaternal health services guaranteeoptimal outcomes for women. Animportant aspect of care that has beenhighlighted to explain why womeneither do not access services at all,access them late or suffer an avoidableadverse outcome, despite timelypresentation, relates to the intangibleconcept of quality of care. Part of thereason for the intangible nature ofquality is that it is very difficult tomeasure. As long as avoidable deathsand morbidity continue to occur thatcan, at least in part, be attributed topoor quality care, there is an imperativeto overcome the difficulties ofdefinition and measurement (bothperceived and real) associated withquality.
This monograph develops a frameworkthat enables the measurement ofquality within institutional deliveryservices for use by public healthresearchers, policy makers, managersand a range of health professionals.Theframework divides the provision andexperience of care into ten elements,drawing on a wide body of researchand evidence-based good practice. Foreach element, broad standards, criteriaand selected indicators are suggested.The framework is designed to functionin two possible ways.
Firstly, as a tool by which to helpstructure a situation analysis review ofquality of care as provided at a facility,and experienced and perceived by itsclients, actual and potential.
Secondly, as a tool by which toimprove the quality of care throughthe ongoing critical examination ofactivities, compared with an agreedstandard. Where care falls short ofagreed standards it would then bepossible to instigate a process toidentify opportunities and implementchange to bring practice closer to thestandard. This framework provides aninstrument by which to guide andstructure the measurement andmonitoring of quality in this vital areaof maternal health care.
The framework weaves together anumber of distinct yet integratedcomponents of institutional deliverycare: care during normal delivery; careduring a complicated delivery; psycho-social-cultural care during labour anddelivery; hospital logistics andmanagement; and the overarchinghealth system of which the unit is part.The hospital administrator and thehead of the maternity wards areusually responsible for the first fourcomponents mentioned above whilethe district health authority isresponsible for the latter. Thecomplexity of the task of assessing

3
quality using a framework that drawson elements of care that fall under theremit of different authorities shouldnot be underestimated. However, asthe quality of each component isdependent on the quality of theothers, their inclusion conceptuallywithin one broad framework isimportant. A fully equipped operatingtheatre is of no use if it is impossible tolocate an anaesthetist. Similarly whilecare in normal delivery may beclinically exemplary, if a woman isunhappy with the psycho-socialsupport she receives, she and herfamily may prefer that she deliver athome for any future pregnancy, withthe support of traditional bir thattendants.
The framework is flexible. How it isused in practice will depend on anumber of factors such as location,resources, management structure, typeof institution, capacity for datacollection, political will, localcircumstances and the degree of staffinvolvement. Unless the process bywhich the framework is implementedis appropriate, effective change will notresult. However, it is the content of theframework that provides thefoundation for a successful qualityassessment process. The uniquecontribution of the approach taken inthis monograph is the drawingtogether of research from medical,health policy and social sciencedisciplines to produce an evidence-based model by which to assess
quality. While the process ofimplementation is briefly touched on,the primary aim is to examine thepotential content of a qualityassessment of institutional deliverycare.
It is important to note that thisframework has been designed for usein institutional facilities only, and islimited in its current form to quality ofcare to pregnant and labouringwomen and new mothers. While it isrecognised that care of the labouringwoman and the unborn fetus andnewly born infant are closely related,expanding the focus of thismonograph would have rendered itunwieldy. If services are acceptable towomen and provide appropriate,timely care, commensurate benefits tothe unborn child would be anticipated;see Johansen and Hod (1999) for adiscussion of quality development inperinatal care and Mancey-Jones andBrugha (1997) for a review of the useof perinatal audit to promote change.
2 Background
2
More than 585,000 women each yeardie of pregnancy-related causes world-wide, 99% of these occur in the lessdeveloped world (WHO, 1996a). Iftimely and appropriate obstetric carewere accessed in the event of acomplication, an estimated 75% of theabove deaths could be prevented.While in many areas services simply donot exist, where they do they are oftenunder-utilised. In addition, latepresentation by pregnant women inthe event of a complication, combinedwith poor quality of care, contributesto high levels of maternal and perinatalmortality and severe morbidity(Thaddeus and Maine, 1994). As allpregnant women are at risk ofobstetric complications, access toadequate essential obstetric care(EOC) needs to be universal (WHO1998). The existence of such care,however, guarantees neither use norimproved outcome. This will bepossible only if the care that exists is ofa high enough quality to provideadequate treatment and encourageearly utilisation. Furthermore, quality ofcare is an essential component of anyprogramme that upholds the basicprinciples of a reproductive healthapproach.
Quality is not easy to measure ordefine. However, significant progresshas been made in defining quality ofcare in relation to the family planning
element of reproductive health (Bruce,1990).The recognition that the qualityof services has an impact on the use ofservices has given suppliers of suchservices a strong incentive to improvequality of care with the goal of greateracceptance and more sustained use ofcontraceptive technologies. At thesame time, more couples are able toachieve the family size and spacing theydesire and a concomitant reduction inoverall fertility can be expected, a win-win situation.
However, while the elements of qualitycare within family planning arerelatively well defined and amenable tomeasurement, a broad approach toquality of care in maternity serviceshas received relatively little attention.Historically, the major focus inmaternity services has been to reducematernal mortality by the provision ofhospital based services. Theeffectiveness of this approach indeveloped and developing countrieshas perhaps detracted from thebroader issues of quality of care, whichaffect womens health and influence theacceptability and uptake of services.Where services exist they shouldprovide at the very least a standard ofcare that results in the best possibleoutcome given the resources availableand should not inhibit utilisation. It isclear from a review of the currentliterature that no systematic

5
3.1 Why is QualityImportant?
A maternal death is defined by the 9thand 10th revisions of the InternationalClassification of Diseases as:
‘The death of a woman while pregnant orwithin 42 days of the termination ofpregnancy, irrespective of the duration orsite of the pregnancy and which resultsfrom any cause related to or aggravated bypregnancy or its management’ (WHO,1992).
Clinical literature suggests that about75% of maternal deaths result fromdirect obstetric causes, such ashaemorrhage, obstructed labour,infection, toxaemia and unsafe abortion(WHO, 1985). This literature alsosuggests that a majority of these deathscould be prevented with timely medicaltreatment. Delay - that is an avoidabletime delay from the onset of acomplication to the accessing ofappropriate services - has emerged as apertinent and indeed central factorcontributing to maternal death anddisability (Thaddeus and Maine, 1994). Inthe past decade, growing attention hasbeen given to the vital role of essentialobstetric care in the prevention ofmaternal deaths. As all pregnant womenare at risk of obstetric complications,effective access to adequate essentialobstetric care needs to be universal andwomen should be able to access that
care promptly in the event of acomplication.
In practice, the facilities that provideessential obstetric care in an emergencyalso provide care in normal delivery. Awomans experience of care for anuncomplicated delivery is likely toinfluence her future health seekingbehaviour. It is conceivable that afterexperiencing good but disrespectfultreatment in a previous normal delivery,a woman with a complication may delayaccessing care from a facility thatprovides essential care of clinically highquality in favour of staying at home a littlelonger or travelling slightly further to aunit where the perceived, though notnecessarily actual, care is of a higherstandard.The relationships are complex.What needs to be understood is thatwhile the availability of appropriateessential obstetric care is the only way toprevent a complication becoming adeath, the quality of care provided andexperienced in normal delivery mayimpact negatively on overall outcomes ifthe timing of use is delayed as a result ofpoor perceived standards of care. Anassessment of quality must necessarilyconceptualise the various componentsof care as interdependent.
Increasing the availability of services doesnot always increase the use of services,and the reasons for this have beeninvestigated. Delays to accessing care canrange from delaying the actual decision
framework is currently available bywhich to assess quality in maternitycare. There is a need for well-definedcriteria and standards at all stages ofthe complex maternal health-carechain. As a response, this monographfocuses on quality in one specificsection of the care chain: the provisionof institutional delivery services. Aframework of meaningful andmeasurable elements of quality of careis developed, based on an extensivereview of evidence from a range ofdisciplines. The creation of thisframework provides a practical basison which the systematic improvementof care in this vital part of the maternalhealth chain may be developed.
4
3 Quality of Care

6 76
alone is not sufficient to reduce thenumber of maternal deaths. Facilitiesneed to be providing adequate services.A community-based investigation ofmaternal deaths, undertaken in bothrural and urban areas of Zimbabwe toassess their preventability, identified sub-optimal clinic and hospital managementas an avoidable factor in nearly 70% ofcases. Lack of appropriately trainedpersonnel contributed significantly tosub-optimal care (Fawcus et al., 1996).Similarly, a study conducted at auniversity hospital in Nigeria found thatdelays in obtaining appropriatetreatment were responsible for asignificant number of deaths, and thatsuch delays were more common amongwomen of lower socio-economic statusand among younger women (Okonofuaet al., 1992). Findings from this studyindicate that delays relating to healthservice failures were more significantthan postponing the initial decision toseek emergency care. Health servicefailures identified included incorrecttreatment, lack of facilities, poor staffattitude, and delays in the referralprocess. Poor co-operation betweenhealth providers, and inadequateequipment and supplies were identifiedby women themselves as constraints toessential obstetric care (Okafor andRizzuto, 1994). In a review of hospital-based studies, Sundari documentsevidence of avoidable factors and identifiesa range of failures in the health servicedelivery system that contributed tomaternal deaths in developing countries.
‘Failures ranged from the lack of minimallife-saving equipment at the first referrallevel; lack of equipment, personnel andknow-how even in referral hospitals, and,worst of all, faulty patient management’
(Sundari, 1992; p.513).
3.2 A ReproductiveHealth Approach
The concept of reproductive health,which gained currency initially in the1980s, is premised on the feministprinciple that every woman has the rightto control her own sexuality andreproduction without discrimination asto age, marital status or income.Ensuring the highest possible standardsof reproductive health-care for girls andwomen is fundamental to the exercise oftheir reproductive rights and freedoms,and to the exercise of the broad array ofother human rights to which girls andwomen are entitled (Dixon-Mueller,1993). Quality of care is an essentialcomponent of any programme thatupholds three principles of areproductive health approach:
1) A woman’s ability to regulate herfertility safely and effectively byconceiving only when desired, byterminating unwanted pregnancies,and by carrying wanted pregnanciesto term.
2) To remain free from avoidabledisease, disability or death associatedwith her sexuality and reproduction.
to seek care on the part of the individualand her family, to delays in reaching anadequate health-care facility and finally,delays in actually receiving adequate careat the facility. Factors that influence delaysin the decision to seek care include thestatus of women, illness characteristics,distance from the facility, and perceivedquality of care. Delay in actually accessingcare refers to factors such as thedistribution of facilities and the conditionof the roads, while delays in receivingadequate care include the adequacy ofreferral systems, shortages of supplies,and the competence of availablepersonnel (Thaddeus and Maine, 1994).Thus the theoretical availability ofservices does not mirror access, and anumber of socio-economic and culturalfactors combine with individual andgroup perceptions and experience ofquality of care to influence the utilisationof maternal health services.
The quality of care that a health serviceprovides is thought to influence use in anumber of ways, although little is knownabout the mechanisms by which thisrelationship functions. Studies haveshown that quality can affect thedecision to seek care (Iyun, 1983; Stock,1983; Mwabu, 1986). Where serviceusers have access to more than onefacility, it is often their perceptions ofquality of care, related to their ownexperiences or those of people theyknow, rather than proximity thatdetermines their choice of facility. It is acombination of dissatisfaction with theservice received and the effectiveness of
treatment given that shapes a patient’sand her friend’s and family’s perceptionof care, which in turn influences health-seeking behaviour (Thaddeus andMaine, 1994). Quality may also have animpact on the timing of presentation ata facility. In circumstances where thepercentage of institutional delivery ishigh (above 70%) and the option ofdelivery at home particularlyundesirable (such as within urban slums)services ideally need to discourage latepresentation by women alreadyplanning to deliver at a facility. Latepresentation (arrival within an hour ofdelivery) does not enable staff toassimilate an adequate medical andantenatal history effectively orundertake basic checks such as bloodpressure and temperature. In addition, inthe event of a complication for which nosymptoms are recognised by thewoman, sufficient time to assembleemergency staff, drugs and equipment iskey to improving outcome. Latepresentation is an example of anindication of poor quality of care inthese circumstances. It may representpoorly communicated health messages,or a desire to stay at home for as longas possible before delivery so as to avoidlabouring alone in the hostileenvironment of a hospital maternityward.
In addition, for those women who doaccess services, at whatever stage, theoutcome is partly dependent on thequality of care they receive. Theexistence and prompt use of services

98
The definition of quality of caredetermines both the content and theprocess of care. In 1966 Donabediandefined quality of care in a unique way:
‘quality of care is the extent to which actualcare is in conformity with present criteria forgood care’.
The unique feature of thisconceptualisation of quality at the timewas the introduction of evaluation into thedefinition. Evaluation became the linkbetween quality and quality assurance.Thisdefinition makes an important distinctionbetween the quality of actual care,which isestablished at the end of an evaluationprocedure, and the expected quality ofcare as it is described in terms of criteriaand clearly defined standards (Reerink,1990).A more recent definition states that:
Quality of care is the degree to which healthservices for individuals and populationsincrease the likelihood of desired outcomesand are consistent with current professionalknowledge.
(Institute of Medicine, 1990, p.94)
The above definition has been adapted toachieve a definition of quality of carerelevant in the context of maternal health.This definition incorporates the concept ofboth effective and timely access and ofreproductive rights thus:
‘Quality of care is the degree to whichmaternal health services for individuals and
populations increase the likelihood of timelyand appropriate treatment for the purpose ofachieving desired outcomes that are bothconsistent with current professionalknowledge and uphold basic reproductiverights’.
This working definition provides the basisfrom which to create a quality assessmentframework for maternal health in aninstitutional setting. The definition allowsquality in this context to be separated intotwo constituent parts:
� The quality of the provision of carewithin the institution.
� The quality of the care asexperienced by users.
For quality of care to be meaningful, it isfundamental that elements of these twocomponents of care be consistent withthe basic norms of internationally agreedreproductive rights.
The division of quality into these twocomponents recognises the fact that useof services and outcome are the result notonly of the quality of the provision of carebut of women’s experience of that care.The provision of care may be deemed ofhigh quality against all recognised standardsof good practice but unacceptable to thewoman and her family. Conversely, certainaspects of provision may be popular withwomen but objectively ineffective or evenharmful to health.
3) To bear and raise healthy children.
(Adapted from Germain and Ordway,1989, cited in Dixon-Mueller, 1993).
Where the nature of maternal care issuch that it inhibits effective utilisationand receipt of effective care, women arebeing denied the basic right to bear andraise healthy children and remain freefrom disease and disability associatedwith their reproduction. Evidencesuggests that there are proceduresspecific to childbirth in an institutionalsetting that women dislike or fear, andwhich may therefore inhibit utilisation.They may feel uncomfortable exposingtheir genitals in a hospital ward, or theymay intensely dislike positions favouredby hospitals for delivery (Thaddeus andMaine, p.1096). Not only does goodquality of care afford a woman dignity inchildbirth, it also endeavours to avoidthose aspects of care that aredisrespectful - even unnecessary - andmay impact negatively on patterns ofuse.
4 What is Quality? Definition and Measurement

1110
The Evaluation Project Indicators forSafe Motherhood (Carolina PopulationCentre, University of North Carolina)
Guidelines for Monitoring the Availabilityand Use of Obstetric Services(WHO/UNICEF/UNFPA, 1997).
5.2 Criteria andStandards
To make the above framework apractical and analytic tool, criteria foreach constituent element need to bedeveloped and correspondingstandards defined by which quality canbe evaluated. The criteria are a set ofbroad requirements that must besatisfied before each element of qualitycan be realised. The Appendix to thismonograph contains ten tables detailingsuggested criteria, broad standards andsuggested indicators for each of theelements that make up the framework.For example, the following illustrates acriterion that can be used to assess thequality of the management informationsystem provided at a maternity unit(see Table 3 in the Appendix). Thisexample comes from the third elementof the provision of care: managementinformation systems.
Standards define the limits by which thecriteria can be assessed. In this example,sufficient and effectively are thestandards that need to be defined.Sufficient in a maternity home may nothave the same meaning as sufficient in alarge university hospital. Given theenormous variability that exists inhealth-care systems and economic andsocio-cultural conditions throughoutthe developing world, setting universalstandards is problematic. What isacceptable and achievable in one settingmay be impossible in another.
The criteria within the framework canbe applied universally amonginstitutions of similar status but localconditions should dictate the exactstandards that are appropriate in thatsetting. Given this, however, for certainaspects of maternity care it is possibleto set universal standards applicableregardless of the context; for example,the maintenance of asepsis at all times.This is what Donabedian referred to ascertain limits which should not betransgressed (1966, p.183).
It is particularly difficult to set minimumstandards for the elements of theframework relating to the experienceof care. Research conducted in thedeveloped countries indicates thatperceived quality may vary amongmembers of different socio-economicgroups (Calnan, 1988a: Roberge et al.,1996; Haddad et al., 1998). Perceptionsare influenced by the social,organisational and technologicalcontext in which the health services are
CRITERION STANDARD
Basic registers in facilities ‘sufficient’are designed to record ‘effectively’data that is sufficient to monitor and evaluate activities effectively.
5.1 Ten Elements of Care
The quality framework is presented inFigure 1. It identifies six elementsrelated to the provision of care: humanand physical resources; the referralsystem; management informationsystems; the use of appropriatetechnologies; internationally recognisedgood practice; and the management ofemergencies. Four aspects relating towomen’s experience of care are alsoidentified namely; human and physicalresources; cognition; respect, dignityand equity and emotional support.
In the process of developing theframework, a wide range of social science,health policy and medical literature wasreviewed. Prominent among these were:
The Pregnancy and Childbirth Module ofthe Cochrane Library
The UK Royal College of Obstetricians andGynaecologists Clinical Audit Unit
WHO Safe Motherhood Series (includingCare in Normal Birth and the Mother andBaby Package)
The Design and Evaluation of SafeMotherhood Programmes (Maine et al,1997)
5 A Quality of CareFramework
Quality of Care
Provision of Care Experience of Care1. Human and physical resources
2. Referral system
3. Maternity information systems
4. Use of appropriate technologies
5. Internationally recognised good practice
6. Management of emergencies
7. Human and physical resources
8. Cognition
9. Respect, dignity and equity
10. Emotional support
Figure 1: Framework for assessing quality of institutional-delivery services: Ten elements of care
Figure 1: Framework for assessing quality of institutional delivery services: Tenelements of care

1312
process of care at the institutionallevel. It would be presumptive to inferthat improved outcomes were theresult of improving the process in mostcases (De Geyndt, 1995). For example,a reduction in maternal mortality atthe facility level may be the result of animproved transportation system andhave little to do with the quality of careprovided. The cause-effect relationshipbetween process and outcome isoften tenuous. No indicator used inisolation is sufficient to provide ameaningful insight into the element ofquality being examined.
There are two important drawbacksof the input-process-output trilogy.Thefirst, as indicated above, relates to thecomplex relationship that existsbetween cause and effect. The linkbetween structural attributes and theprocess of care is inconsistent andempirically unproved (De Geyndt,1995).The simple existence of humanand physical resources necessary toprovide high quality essential care isnot enough to assure the provision ofsuch care. The second methodologicalproblem relates to the relativeimportance of the ten elements. Failingto meet standards set for certaincriteria may result in such poor qualitycare as to influence the healthoutcome directly (for example, emptyblood stores in a referral hospital),while failing to meet other standardswill have a less immediate impact (forexample, prohibiting social support inlabour). Aspiring to meet all criteria to
the highest standards would be theultimate goal, but in practice, givenlimited resources, decisions willinevitably be made about the relativeimportance of specific interventions toredress areas of poor quality identifiedin the assessment process.
Given this, however, it is not useful tohave a limitless supply of blood if thereis no one qualified to transfuse thatblood, just as the existence of aneffective communication system withreferral hospitals is practicallyredundant if transport between theunits is not available 24 hours a day.Toreduce the number of maternal deathsit is vital that the interdependence ofthe elements of care be recognised inthe assessment of care. Optimal carein one element can go hand in handwith high levels of maternal death andmorbidity if care in other areas fallsbelow an acceptable standard.
In practice, many of the problemsexperienced in the provision ofessential obstetric care, especially indeveloping countries would cost littleto address, at least in financial terms.For example, operating theatres maybe locked and the person responsiblefor the key cannot be found, thetheatre may not have been cleanedafter the previous operation,anaesthetists are usually on call duringthe night but often cannot becontacted or are unable to attendduring public holidays. Furthermorethere is evidence that an increase inthe quality of care provided and
delivered (Palmer, 1991; Ellis andWhittington, 1993). However, evenwhen staff are overwhelmed by thevolume of users, rudeness anddisrespectful behaviour, should not becondoned (Mensch, 1993). Notions ofprivacy vary culturally, as do definitionsof respect. Where the communicationof important information is inhibited,such as details of medical conditionsfrom the patient to the provider, or ofdetails of side-effects from certaindrugs, such behaviour is more thansimply rude, it can contribute toadverse outcomes. Agreeing onminimum standards for communicationand respect within institutions istherefore an important part of thequality process.
5.3 Indicators
Once appropriate standards havebeen explicitly defined, a variety ofindicators may be selected to evaluatehow closely these standards are beingmet. There already exist numerouspublications that offer a range ofindicators that can be drawn on to aidthe evaluation process (Koblinsky et al.,1995, Maine et al., 1997, Campbell etal., 1995, UNICEF/WHO/UNFPA,1997). These indicators are usuallyorganised into an input-process-outputstructure leading to outcomes.That is,indicators have been developed toevaluate the inputs to a programme,and how these are converted throughprocesses (activities) to produceresults (outputs) at the programme
level and eventually changes at thepopulation level (outcomes)(Koblinsky et al., 1995).
This is a useful way to conceptualisethe whole. However, in an assessmentof quality of care at the facility level therange of indicators so far developedfails to capture important aspects ofservice provision that contribute towomen’s experience of care. Thedetailed framework presented in theAppendix offers a number ofsuggested indicators to assess whethercriteria to assess users experience ofcare are being met. The developmentof such indicators is in its infancy andthe corresponding examples given inTables 7-10 represent workingsuggestions. In addition, the indicatorsthat are currently most commonlyused do not on the whole helpevaluate either the appropriateness ofintrapartum and postpartum care orwhether that care falls withinrecognised standards of good practice.For this reason we have paid particularattention to these aspects of thequality framework.
The degree of difficulty in measuringquality increases as one moves frominput, otherwise known as structural,variables to process measures andthen to outcomes of patient care.Certain outcomes, such as maternalmortality rates or ratios, case fatalityrates, perinatal mortality rates and soforth can reveal certain things aboutmaternal health at a general level, butalone reveal very little about the

1514
experienced could actually reduce thecost of the service by decreasingwaste, curtailing inappropriate use oflimited resources, eliminatinginefficiencies, optimising the use ofexisting inputs, and applying correctprocesses (De Geyndt, 1995).
5.4 Data Collection
Experience has shown that, dependingon the source of the information, datacan be conflicting. For example, inorder to measure the normal waitingtime between arrival at the facility andthe first examination, multiple sourcesneed to be drawn on to piecetogether the most probable timing ofevents. Provider interviews maysuggest that women are generallyexamined within half an hour of arrival.An examination of case notes, whichshould theoretically record time ofarrival and the time of firstexamination, may or may notcontradict this claim. Yet a woman’srecall of events may or may not bereliable depending on her education,progress of labour and so on. All ofthis information combined with anobservation of normal events,including an assessment of theaccuracy of time reporting in casenotes, over a period of time will enablethe investigator to define an averagenormal waiting time for bothuncomplicated and complicateddeliveries.The investigator will need tomake value judgements as to thereliability of different sources. This
enables a systematic verificationprocess that will ultimately produce amore objective assessment. While thecriteria for quality require localdiscussion and definition, theframework approach, using a variety ofindicators, has the potential to bestreflect a valid notion of quality. Thepanel opposite briefly reviews a rangeof sources and methodologies thatmay be used to calculate indicators ina quality assessment process.
Approaches to DataCollectionFacility Records
These can be divided into twogroups: information that is availablein the public domain (for example,annual reports and annual accounts)and source documents, that is,information routinely collected bythe institution (such as theadmissions register). Facility recordsinclude annual reports, accounts,staff lists, registers (admissions,delivery, discharge), hospitalguidelines (procedural/protocol,documents), blood-bank records,inventories of facility’s equipment,stocks and supplies and operatingtheatre records. The quality of thisinformation is likely to be variable,but important data can beextracted, if used with care.
Provider Interviews
Structured and semi-structuredinterviews with a full range of healthproviders can be used to obtaininformation on a range of factual,impressionistic, theoretical andsubstantive issues. An attemptshould be made to ensureinterviews are held in private andthat confidentiality is maintained.One drawback of provider
interviews is that they often elicitresponses that reflect idealisedbehaviour. In a structured interviewmany providers respond with whatthey know should be the case,rather than an accurate descriptionof existing services (Simmons andElias, 1994).
Exit Interviews
Structured and semi-structuredinterviews with women who havedelivered are best taken on the dayof discharge. They should berelatively short (30 minutesmaximum) and held in private.Theyare effective for obtaininginformation on the course of awoman’s labour ; the decision-making process; and circumstancesgoverning the timing ofpresentation, the choice of facilityand actual experience of care.Certain questions relating to herexperience of care are notappropriate in this setting and areunlikely to provide meaningful data(courtesy bias). Women may beunlikely to speak as candidly abouttheir experiences of care as theymight at their own home. However,the timing of this interview facilitatesaccurate data on, for example, the

1716
questions relating to many aspects ofquality of care, from interpersonalrelations and waiting times to theuse of specific procedures. If thesurvey covers a large enough area itcan provide information for andabout a range of institutions (public,charitable, non-governmental andprivate) as well as providinginformation about women whodelivered at home. This offers theopportunity to examine factors thatdetermine use, non-use and choiceof provider. Surveys can also be usedto obtain information indirectly thatis difficult to obtain from providersdirectly. For example, researchershave found that information relatingto operational delivery rates areoften not forthcoming from privateproviders, who fear regulation andthe potential limitation of what is avery lucrative aspect of their service(Matthews, 2000). Caesarean-section rates by provider, however,can be calculated using survey datawhere the survey covers asufficiently large number of womendelivering in a range of institutions.
It should be noted that surveys thatintend to reveal meaningfulinformation about levels ofsatisfaction need to ask questionsthat are detailed enough to revealhow women and their familiesdiscriminate among serviceattributes. Surveys from developingcountries are reported to havenoted uniformly high levels of
satisfaction despite great variability inthe quality of services (Simmons andElias,1994).
Focus Groups and In-depthInterviews
A further limitation of surveys is thatthey cannot adequately capture thecomplex feelings and perspectives ofclients or the underlying dynamics ofpower and status. Simmons and Elias(1994) draw attention to the factthat research on social services indeveloped countries has shown thatsurvey data typically reveal highlevels of client satisfaction withservices, while in-depth street-levelapproaches show extensiveevidence of dissatisfaction (Lipsky,1981). If it is possible to follow upwomen who have delivered in thefacility under assessment, theirinclusion in focus group discussionscan yield important insights intowomens experience of care in thefacility, and their reasons foraccessing care when, and where theydid. Insights into why women did notaccess care at that particular facilitycan be equally revealing. In order toidentify potential aspects of care thatmay inhibit utilisation, theorganisation of focus groups and in-depth interviews with women wholive in close proximity to the facilitybut that chose another provider ordelivered at home, would benecessary.
number of vaginal examinationsreceived - information that may beless easy to remember accuratelysome time after the delivery.Interviews should be designed toobtain some socio-economic dataand basic information about thenumber of previous pregnancies anddeliveries, place of delivery, outcome,and the nature of complicationsduring and after delivery.
Case Notes
The quantity and quality ofinformation in case notes isnotoriously variable. However, whenused in conjunction with an exitinterview they can be useful forpiecing together events. They canhelp distinguish between poormanagement and poor record-keeping. For example, case notesalone do not reveal whether bloodpressure is being routinely taken onarrival but staff are failing to recordthis in case notes, or whether bloodpressure is simply not being taken atall. They do, however, reveal if it isbeing routinely taken and recorded,and can therefore provide a usefulindicator of good quality.
Observation
General observation techniques areessential in the assessment of basicquality indicators relating tocleanliness, crowding, state ofequipment, provider-client relationsat a general level and so on.Moreover, it is an effective means of
verifying aspects of care described inprovider and client interviews.Observational approaches have theadvantage that data reflects anaction or interaction itself ratherthan someones rendering andrecollection of what happened.
Providers tend to be affected by thepresence of outsiders (best-behaviour bias), so observationtechniques require that the assessoris either internal and specificallytrained, or present for a sufficientlylong period of time to gain a fairlyaccurate insight into normal care.This will result in a more completeand accurate picture of all aspects ofcare. In reality, where quality of carenorms are not yet widely acceptedand implemented in the field,providers may not feel the need todisguise their approach to clientswhen being observed (Simmons andElias, 1994).
Community Survey
Household surveys designed to elicitclient perspectives and informationabout their experience of care arean important methodology.Undertaking a survey is often notpossible, requiring too much timeand too many resources. However, ifit is possible, survey data can providesome unique insights into health-seeking behaviour in the community.Surveys enable information to begathered about previous bir thexperiences, and can include specific

1918
6.1.1 Human andPhysical Resources
Human resources include the quantityand quality of health and non-healthpersonnel employed for providing andsupporting the delivery of patient care(De Geyndt, 1995). The term refers alsoto the configuration of staff, levels ofsupervision, management styles,population-based staffing ratios, andnature and frequency of staff training.
Physical resources are the grounds,buildings fixed and movable, medical andnon-medical equipment, vehicles,furniture, medical and office supplies,pharmaceuticals, warehousing andstorage conditions and maintenance ofphysical assets (De Geyndt, 1995, p.33).The term covers general hospitalinfrastructure, including water andelectricity supplies.
A quality assessment tool needs to beable to record in some detail theavailability, use and quality of the above.The review process would need toassess not only the clinical skills of staff,their experience, training andcommunication skills, but also theirhours and salaries. Facilities can sufferfrom staff shortages, a dysfunctional skillmix as compared with case mix, unclearjob descriptions, underskilled staff andstaff who lack confidence in their skills(Huque et al., 1999). They can alsoemploy staff who feel isolated,
unmotivated and undervalued - all ofwhich have an impact on the quality ofboth clinical and interpersonal careprovided by the institution. The SafeMotherhood Project in Nigeria drawsattention to the fact that inadequate payand benefits for health staff arefrequently mentioned as determinantsof poor quality of care. Okafor andRizzuto (1994) recommend that suchpractices should be reviewed and, ifpossible, remuneration for healthprofessionals should more closely reflectthe value of the critical service theyprovide. Simmons and Elias (1994) warnthat researchers must be aware of theprofound sense of alienation that shapesproviders behaviour in many settings.Where the threat of unemploymentand resource scarcities dictateassignments to rural work settings,rather than an intrinsic motivation toserve, providers are bound tocommunicate their sense of frustrationand lack of concern for their clients (p.4).Effective provision of maternity servicesrequires that staff are managed andsupported effectively in their roles. Delayin payment of salaries, excessive patientloads and insensitive line managementwill promote an adverse professionalenvironment. Conversely efficient andresponsive management of an institutionwill tend to enhance the quality of theworking environment and motivate staff.
Areas suitable for the application of
Opposite the ten elements of care that make up the framework are reviewed in more detail.
6 Expanded QualityAssessment Framework
6.1 Provision of Care
Quality of Care
Provision of Care Experience of Care
1. Human and physical resources
2. Referral system
3. Maternity information systems
4. Use of appropriate technologies
5. Internationally recognised good practice
6. Management of emergencies
7. Human and physical resources
8. Cognition
9. Respect, dignity and equity
10. Emotional support
Framework for assessing quality of institutional-delivery services:Ten elements of care

2120
Criteria that may be used to assess thequality of the provision of care relating tohuman and physical resources include:
1) The skill mix is appropriate to copewith patient flow and the case mixof deliveries at the facility.
2)The maternity wards areadequately equipped to performtheir function effectively andconsistent with internationallyrecognised good practice.
3) The operating theatre is in goodrepair and fully equipped withdrugs and surgical equipment toperform life-saving procedureswhen required.
4)The general infrastructure of thefacility is of sufficient size and stateto cope with demand, and essentialsupport services are reliable.
5)The organisational andmanagement structure of thelabour, delivery and postpartumsuite ensures most efficient use ofresources.
6) Staff should always be adequatelyprotected from risks associatedwith their work.
7) Effective systems for maintainingthe quality of the human resourcebase should be in place at allfacilities.
8) All facilities should have a clearmanagement structure and clearlines of accountability
(also see Table 1 in the Appendix)
6.1.2 Referral
The quality of the referral system iscrucial to preventing maternal death.The hierarchy of maternity facilitiesonly becomes a functioning unit if thereferral system from the lower-orderhealth centre to the referral unit isefficient and effective. While themajority of complications areunpredictable, it is possible to identifyantenatally certain high-risk groups(such as breech presentation andmultiple pregnancies), which should bereferred to the appropriate facility wellbefore labour begins.This framework isnot concerned with referrals madeantenatally, however, but with thequality of referral procedures once awoman in labour or with acomplication presents at the facilityunder assessment.
Poor referral procedures wereidentified as a significant constraint tothe accessing of emergency care in astudy in Nigeria (Okafor andRizzuto,1994). Here, midwives inAkwa-Ibom were reportedlyfrustrated that registered maternity-centre patients were treated asunbooked cases when they went togeneral hospitals for emergencyassistance, and were therefore deniedprompt treatment. Among facilities inurban India, it has been reported thatunits providing basic emergency caremay deny care to any unbookedwoman presenting in labour, regardlessof her condition. This policy adds
quality standards related to humanresources include:
Safety at work, staff training anddevelopment and the management ofhuman resources
Staff require protection from risksassociated with their work.These includephysical violence, verbal abuse frompatients and relatives and transmissibleinfectious diseases, especially Hepatitis Band HIV.These are especially pertinent inmaternity facilities where exposure tolarge volumes of body fluids is likely.
Effective systems for staff appraisal linkedto personal and professionaldevelopment opportunities such as theavailability of courses and in-servicetraining are key to maintaining the qualityof the human resource base.
Staff operate more effectively wherethere are clear management structuresand clear lines of accountability.
Basic and Comprehensive EssentialObstetric Care
Insufficient and unqualified staff,unavailability of blood, shortages ofessential drugs and missing supplies limitaccess to life-saving procedures (Thaddeusand Maine,1994).A WHO working group(1996) identified two levels of essentialobstetric care: basic and comprehensive.Afacility at the level of a health centre isexpected to be able to provide sixessential functions: antibiotics (injectable),oxytocics (injectable), anticonvulants(injectable), manual removal of theplacenta, removal of retained products and
assisted vaginal delivery.A facility providinga comprehensive level of essential care,such as a district hospital, is expected to beable to provide not only all of the abovebut also caesarean-sections and bloodtransfusions.
The provision of these services requiresthat other aspects of the physicalinfrastructure function efficiently. In thedeveloping world there are frequentproblems with the provision of thecontinuous supply of power and water. Inaddition, the maintenance of buildings andequipment in a state of adequate repair isoften problematic in settings wherebudgets are constrained, and increaseddemand for services compromises theefficient operation of facilities.The ability ofa facility to perform effectively thefunctions expected of it is the outcomenot only of the quality of human andphysical resources but also of the otheraspects of quality identified in thisframework.
2322
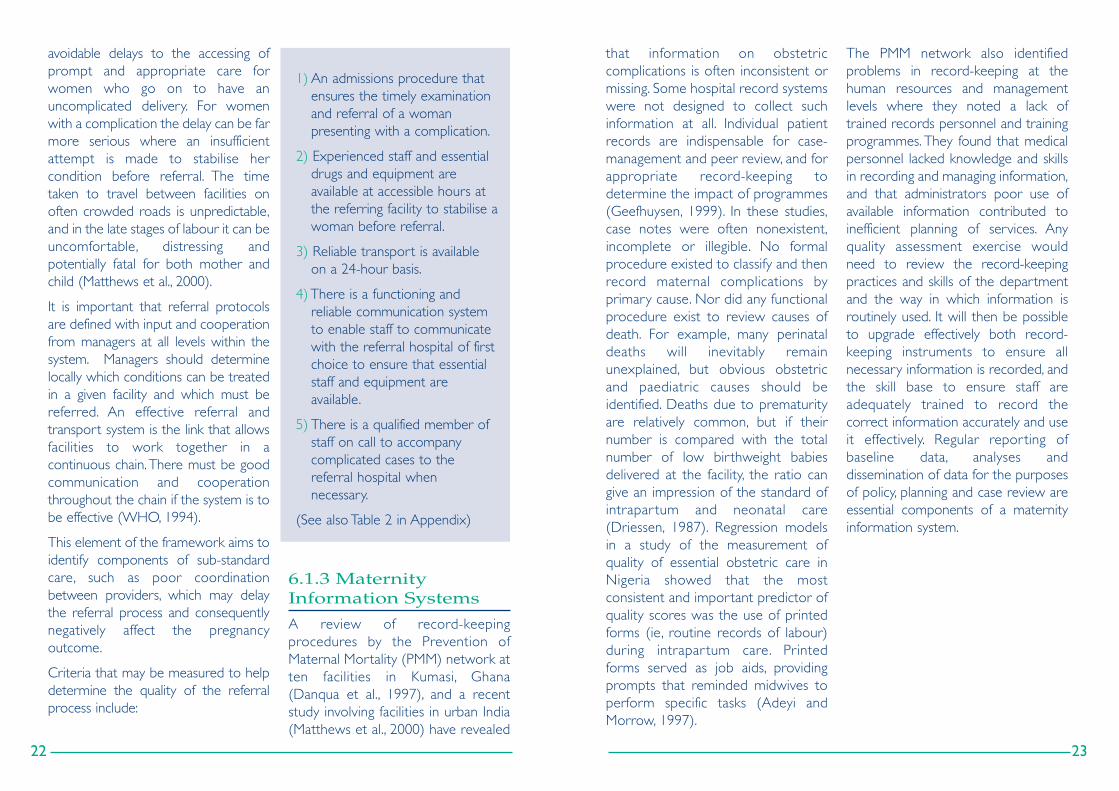
that information on obstetriccomplications is often inconsistent ormissing. Some hospital record systemswere not designed to collect suchinformation at all. Individual patientrecords are indispensable for case-management and peer review, and forappropriate record-keeping todetermine the impact of programmes(Geefhuysen, 1999). In these studies,case notes were often nonexistent,incomplete or illegible. No formalprocedure existed to classify and thenrecord maternal complications byprimary cause. Nor did any functionalprocedure exist to review causes ofdeath. For example, many perinataldeaths will inevitably remainunexplained, but obvious obstetricand paediatric causes should beidentified. Deaths due to prematurityare relatively common, but if theirnumber is compared with the totalnumber of low birthweight babiesdelivered at the facility, the ratio cangive an impression of the standard ofintrapar tum and neonatal care(Driessen, 1987). Regression modelsin a study of the measurement ofquality of essential obstetric care inNigeria showed that the mostconsistent and important predictor ofquality scores was the use of printedforms (ie, routine records of labour)during intrapar tum care. Printedforms served as job aids, providingprompts that reminded midwives toperform specific tasks (Adeyi andMorrow, 1997).
The PMM network also identifiedproblems in record-keeping at thehuman resources and managementlevels where they noted a lack oftrained records personnel and trainingprogrammes. They found that medicalpersonnel lacked knowledge and skillsin recording and managing information,and that administrators poor use ofavailable information contributed toinefficient planning of services. Anyquality assessment exercise wouldneed to review the record-keepingpractices and skills of the departmentand the way in which information isroutinely used. It will then be possibleto upgrade effectively both record-keeping instruments to ensure allnecessary information is recorded, andthe skill base to ensure staff areadequately trained to record thecorrect information accurately and useit effectively. Regular reporting ofbaseline data, analyses anddissemination of data for the purposesof policy, planning and case review areessential components of a maternityinformation system.
avoidable delays to the accessing ofprompt and appropriate care forwomen who go on to have anuncomplicated delivery. For womenwith a complication the delay can be farmore serious where an insufficientattempt is made to stabilise hercondition before referral. The timetaken to travel between facilities onoften crowded roads is unpredictable,and in the late stages of labour it can beuncomfortable, distressing andpotentially fatal for both mother andchild (Matthews et al., 2000).
It is important that referral protocolsare defined with input and cooperationfrom managers at all levels within thesystem. Managers should determinelocally which conditions can be treatedin a given facility and which must bereferred. An effective referral andtransport system is the link that allowsfacilities to work together in acontinuous chain. There must be goodcommunication and cooperationthroughout the chain if the system is tobe effective (WHO, 1994).
This element of the framework aims toidentify components of sub-standardcare, such as poor coordinationbetween providers, which may delaythe referral process and consequentlynegatively affect the pregnancyoutcome.
Criteria that may be measured to helpdetermine the quality of the referralprocess include:
1) An admissions procedure thatensures the timely examinationand referral of a woman presenting with a complication.
2) Experienced staff and essentialdrugs and equipment areavailable at accessible hours atthe referring facility to stabilise awoman before referral.
3) Reliable transport is availableon a 24-hour basis.
4) There is a functioning andreliable communication systemto enable staff to communicatewith the referral hospital of firstchoice to ensure that essentialstaff and equipment areavailable.
5) There is a qualified member ofstaff on call to accompanycomplicated cases to thereferral hospital whennecessary.
(See also Table 2 in Appendix)
6.1.3 MaternityInformation Systems
A review of record-keepingprocedures by the Prevention ofMaternal Mortality (PMM) network atten facilities in Kumasi, Ghana(Danqua et al., 1997), and a recentstudy involving facilities in urban India(Matthews et al., 2000) have revealed

2524
for this element of the framework andwill be discussed here. Those selectedare relatively easy to identify in anassessment exercise. The assessmentprocess would attempt to ascertainwhether or not these were used bythe facility being assessed, and howoften.
Routine Pubic Shaving andEnemas
Preparation for birth in a health centreor hospital often includes severalroutine procedures such as taking awoman’s blood pressure and checkingher pulse and temperature, all of whichhave implications for the birth.As a risein temperature may indicate infectionor dehydration, and a rise in bloodpressure may signal pre-eclampsia,both should normally be checked atleast every four hours. Routineprocedures such as pubic shaving andenemas before delivery, however, arecommon but have no proven benefitsand can both be uncomfortable andhumiliating. Pubic shaving waspopularly thought to reduce infectionand make suturing easier. While thereis no evidence to support this, thelikelihood is that the risk of infectionfor the woman (and indeed theprovider) will rise throughcontamination from a non-sterileblade. The transmission of HIV andhepatitis are among the more seriouspotential consequences. A studyexamining this practice as early as1922 (Johnston and Sidall, 1922) and amore recent randomised controlled
trial in 1965 were both unable todetect any lowering of puerperalmorbidity by pubic shaving. Rather,there was a tendency towardsincreased morbidity in the shavegroups (Kantor et al, 1965).
Enemas are used in the mistaken beliefthat they will help the uterus tocontract and the head to descend, andto reduce contamination at deliveryand so minimise the risk of infection tomother and baby.While some womendo ask for enemas, many find them anembarrassment. Two randomisedcontrolled trials have evaluated theeffects of routine enemas, and noeffects on the duration of labour or onneonatal infection or perineal woundinfection were detected (Romney andGordon, 1981; Drayton and Rees,1984). Routinely administering enemasto women in labour confers nobenefit. Aside from being particularlyuncomfortable during labour, theycarry some risk of bowel damage(rectal irritation, gangrene andanaphylactic shock).
Intravenous Infusion and VaginalExamination
Other routine procedures still widelyused include intravenous infusion ofglucose and fluid. Fasting in labour iscommonly observed in order tominimise the contents of the stomachshould a general anaesthetic benecessary. However, there is noguarantee that withholding food anddrink will result in a stomach volume of
Criteria for assessing the quality ofmanagement information systemsinclude:
1) Basic registers in facilities aredesigned to record data that issufficient to monitor and evaluateactivities effectively.
2) Current procedures for recordinginformation result in completeand accurate data entry.
3) A review process is in place toensure data is comprehensive andused effectively to improvepatient management and servicedelivery.
4) Each complicated case (severemorbidity or mortality, maternalor infant) is effectively reviewedand analysed, and avoidablefactors identified.
(See also Table in 3 in the Appendix)
6.1.4 AppropriateTechnologies
It is now increasingly recognised thatcertain technologies within maternitycare are not always appropriate, beingat best wasteful and at worst harmful.However, assessing the extent to whichinappropriate technologies are usedhas not yet been widely embraced asan indicator of quality of care. For thisreason this element of the frameworkis examined in some depth here.
Good care relies on the use oftechnologies that have been justifiedscientifically. Inappropriate technologiescan compromise safety, use up scarceresources unnecessarily, and in the caseof certain specific procedures be notonly uncomfortable and humiliating forthe labouring woman, but evenharmful. According to the WorldHealth Organisation a technology is:
’an association of methods, procedures,techniques and equipment whichtogether with the people using them cancontribute to solving a health problem.Anappropriate technology is one that isscientifically sound, adapted to localneeds, acceptable to those who use it orfor whom it is used, and that can bemaintained and utilized with resourcesthat the community can afford’
(WHO, 1996b).
Ideally, only interventions that supportthe process of normal birth should beused, and those that are poorlyevaluated or potentially harmfulstopped. The WHO has published areport on care in normal birth, inwhich it details aspects of normal careand identifies technologies that havebeen demonstrated by randomisedcontrolled trials to be inappropriate,unnecessary and sometimes harmful(WHO, 1996b). While there aremyriad potential interventions that canbe, and are, used by midwives andobstetricians all over the world, aselected number identified in theWHO report are included as criteria

2726
liberal use of oxytocin augmentation(active management of labour) is ofbenefit to women or infants.Additionally, the WHO (1996b)concludes that as a general ruleoxytocin should only ever be used toaugment labour in facilities wherethere is immediate access toCaesarean section should the needarise.
Intramuscular Oxytocin
In many areas of the worldintramuscular oxytocin is administeredby injection to augment labour. Use ofany intramuscular oxytocin before thebirth of the infant is generally regardedas dangerous because the dosagecannot be adapted to the level ofuterine activity. Hyperstimulation mayresult which is harmful to the fetus(WHO 1996b). An increasedincidence of ruptured uterus has alsobeen linked to this practice (Kane,1993). Recent studies of hospitals inurban India, and of assisted homedeliveries in rural Karnataka, observedthe frequent use of intramuscularoxytocin before delivery to augmentlabour (Matthews et. al. 1999,Matthews et al. 2000). This harmfulpractice should be abandoned (WHO,1996b).
Caesarean Delivery
Caesarean delivery can be life savingfor mothers and infants, but more andmore often it is being used for reasonsother than this.The appropriate use ofCaesarean delivery can lead to a
decrease in maternal mortality andmorbidity as well as decreasingperinatal mortality and morbidity. Therate of Caesarean section variesconsiderably among countries fromabout 5% to over 30% of all deliveries.Rates also vary considerably withincountries. In a resource-poor settingrates can suffer from being too low inmunicipal facilities yet too high inprivate ones. In Brazil, where deliveryin hospital is the norm, the Caesareandelivery rate for the country has beenestimated as 36.7% (DHS, 1996). Arecent study found rates in privatehospitals as high as 72% (Chacham andPerpetuo, 1998). The optimal rate ofCaesarean delivery is unknown, andwill inevitably vary by institutionaccording to its status within thereferral chain. But the national dataavailable suggest that littleimprovement in outcome appears tooccur when overall rates rise above7% (Enkin et al., 1995). The WHO(1997) suggests that rates of below 5%may indicate inadequate availability andaccess to obstetric care, while rates ofabove 15% may suggest over-utilisationfor reasons that are not essential.Excess use of Caesarean sectionexposes women to anaesthesia andmajor surgery with their concomitantrisks. It is also expensive, at a cost toeither the wider health-care resourcepool or to the woman and her family ifthey are paying for the operation andassociated costs. A study of 221consecutive Caesarean sections at a
less than 100ml. Nor can fasting berelied on to lower the acidity of thegastric contents (Crawford, 1956;Roberts and Shirley, 1976; McKay andMohan, 1988). Restricting food anddrink in labour continues in manyinstitutions. Dehydration and ketosisare possible outcomes of this type ofrestriction, the common response towhich being the use of intravenousinfusion of glucose and fluid.Dehydration can cause veins tocollapse, which would make putting ina drip, if needed, difficult. Moreover, notonly can the use of intravenousinfusion interfere with a woman’sability to move freely in labour, and sointerfere with the natural process, itmay have potentially serious unwantedeffects on the baby such as,hyperinsulinism (Lucas et al., 1980;Rutter et al., 1980;Tarnow-Mardi et al.,1981; Lawrence et al., 1982). Labourrequires enormous amounts of energy.The WHO (1996b) concludes that thecorrect approach should be not tointerfere routinely with womens wishfor food and drink during labour anddelivery (p.11).
Checking cervical dilatation is the mostcommon method used to assess theprogress of labour. This requires avaginal examination.To reduce the riskof infection, these examinations shouldbe kept to a strict minimum - onceevery four hours during the first stageaccording to the WHO (1994) andshould be carried out only by skilledattendants, with clean hands and
wearing gloves. It is important to keepinvasive techniques to a minimum.Attendants impatience often results inthe over-use of this technique.
Intravenous Infusion of Oxytocin
Impatience is sometimes a reason forthe liberal use of another technology:intravenous infusion of oxytocin.Whenthe membranes rupture early andlabour does not follow spontaneouslylabour is often augmented in order toavoid chorioamnionitis.The practice ofusing an intravenous infusion ofoxytocin, to speed up labour afterearly amniotomy if the rate of cervicaldilatation is less than 1cm per hour, hasbeen investigated in a number ofrandomised trials (Read et al., 1981;Hemminki et al., 1985; Bidgood andSteer, 1987; Cohen et al., 1987 andLopez-Zeno et al., 1992).Three of thetrials provided data on the length oflabour after oxytocin augmentationcompared with control groups only.Only one of these demonstrated ashorter mean duration with oxytocin.In one trial women in the controlgroup were encouraged to get out ofbed and move as they wanted. In thisgroup the mean length of labour wasslightly shorter than in the augmentedgroup. No difference in AGPAR scoreswere found (Hemminki et al., 1985).The majority of women in this trialdescribed the augmentation process asunpleasant, and more than 80% saidthat it increased their pain.The WHO(1996b, p. 23) concludes that it is notclear from available data that the

292828
position causes less discomfort anddifficulty when bearing down, lesslabour pain, less perineal trauma andfewer wound infections. In one trial ashorter second stage was observed inthe upright position. Despite this, thesupine position for delivery is generallythe position favoured by the staffattending, and is preferred not only inmost of the developing world but inmuch of the developed world as well.Much of the positive effect of thevertical position depends on the abilityof the bir th attendants and theirexperience with any position otherthan the supine. Birth attendants mayneed to be trained to help womendeliver in positions other than thesupine (WHO, 1996b, p. 27).
Episiotomy
In many parts of the world, episiotomyis used liberally, particularly for firstbirths. It is generally justified on anumber of grounds. It is thought toprevent damage to the sphincter andrectum, and permit better healing thana spontaneous tear. It is thought toprevent trauma to the fetal head, and,finally, it is thought to prevent seriousdamage to the muscles of the pelvicfloor. In practice, all of the above canbe prevented by appropriatemanagement of labour and delivery.Not only do episiotomies, like othersurgical procedures, carry a number ofrisks such as excessive blood loss andinfection, evidence has shown that theroutine use of episiotomy does notreduce the risk of perineal trauma or
improve healing, nor does it preventdamage to the fetal head or improveAPGAR scores.Also, use of episiotomyhas not been shown to reduce the riskof urinary stress incontinence afterdelivery (Sleep et al., 1991). Whererates of infectious diseases such as HIVand hepatitis are high, not only is theoveruse of episiotomy unnecessary forthe above reasons it may increase therisk of transmission for the health-careprovider responsible for the cut andsubsequent repairs. Despite this,episiotomy is the USA’s most commonsurgical operation, as most womenundergo this procedure at the birth oftheir first child for the primary purposeof avoiding a perineal tear. Routinelysubstituting a straight cut for a raggedtear, results in many thousands ofwomen having cuts when only a fewmay have suffered tearing. Episiotomycertainly has a place in safe maternalcare, but only if used appropriately.Indiscriminate routine use is notappropriate use, especially in areaswhere levels of hygiene are low, in andoutside the institution. Data fromrandomised trials do not support a‘blanket’ policy, such as those in place inmany developing world hospitals,which require all primiparous womento have an episiotomy (Carroli, 1997).The WHO (1996b) suggests that agood goal to pursue would be anepisiotomy rate of 10%, the figureattained without harm to mother orinfant in a British trial (Sleep et al.,1984).
large London teaching hospitaldemonstrated that maternal morbiditywas common after the operation.Anaesthetic problems, haemorrhage,paralytic ileus, wound problems andinfective complications were bothfrequent and often unrelated to thecondition that mandated theCaesarean section (Kelleher andCardozo, 1994).
Studies indicate that the growing useof this technology is partly the result ofthe lucrative nature of this interventionfor the providers of care. Other factorsthat have been suggested to explaindifferentials in use include the fear ofmalpractice litigation, convenience forthe clinician, the socio-economicsituation of women and patientdemand. Of women who stated thatthey would prefer to deliver byCaesarean section in the MetropolitanArea of Belo Horizonte County inBrazil, 43% gave ‘less painful’ as thereason, 22% wanted to have a tuballigation at the same time, and 16% hadhad a previous Caesarean section.Thesame study set out to establish theextent to which patient demand couldexplain the high Caesarean sectionrate in the county. Of the 400 womeninterviewed 71% said that they wanteda vaginal delivery, 21% wanted aCaesarean section delivery and 8%said they had no preference. Thesefigures suggest that patient preferenceis not a sufficient explanation for thevery high rates experienced in thisarea (Perpetuo et al 1998).
Supine Position
Many facilities move women from alabour room to a delivery room at thestart of the second stage of labour andthen require them to lie on their backsto deliver.Yet moving a woman at thisstage of labour is an added discomfort,serves no physiological purpose andcan be disruptive at this point. This istrue also of the latter procedure ofensuring women are lying on theirbacks to deliver, in some cases withtheir legs tied in stirrups or held byhospital staff. In the absence of acomplication women should be free toadopt whatever position feels mostcomfortable for them at the time ofdelivery. Generally, if given the choice,women choose positions such assquatting or standing that more closelycomplement the physiology of thelabouring woman, ensuring that gravityaids the process. Lying on her back, orsemi-reclining, effectively results in amore restricted birth passage. In thesepositions, particularly the latter, thewoman will be sitting on her coccyxand sacrum, curving the interior of herpelvis and bringing her pelvis and spinecloser together, which reduces thespace available for the babys head(Sutton and Scott, 1996). A number oftrials (Stewart and Spiby, 1989; Liddelland Fisher, 1985; Crowly et al., 1991;Bhardwaj et al., 1995) suggest that anupright position or a lateral tilt duringsecond stage labour has greateradvantages than a supine position.Findings demonstrate that the upright

fundamentally, clear evidence of theextent to which lack of drug basedpain relief in labour is associated withadverse sequelae, distress and sufferingis lacking. In contrast, studies of cancerpain in different sociocultural settingshas clearly shown comparable levels ofdistress and suffering, which has led tocurrent WHO initiatives to enhancethe availability of effective drugtreatment, especially by addressing thelegal problems surrounding themedical use of opioids in manycountries. It is not yet possible, fromthe existing literature, to identify aconsensus to inform the developmentof general criteria about the extent towhich methods of pain relief should beavailable to women in labour andprimary research in this field is urgentlyrequired. However, effective pain relieffor operative procedures is mandatoryand its availability and provision shouldform part of the evaluationframework.
In the light of the above the followingcriteria may be measured to assess thequality of the provision of care.
1) The following procedures arenot used either routinely, ormost of the time:
Pubic shavingEnemaIntravenous infusionEpisiotomy for primisparasLithotomy position for deliveryManual revision of the uterus
2) The use of vaginal examinationto assess the progress of labouris kept to the minimum necessary.
3) Intramuscular oxytocin is notused to speed up labour
4) The use of Caesarean sectionfalls within reasonable limits
5) Effective pain relief is alwaysprovided for operativeprocedures.
(see also Table 4 in the Appendix)
6.1.5 InternationallyRecognised GoodPractice
There are a number of procedures inmaternity care that have, throughcarefully designed randomised studiesbeen shown to be of benefit to themother or her baby. The UK RoyalCollege of Obstetricians andGynaecologists (RCOG) has publisheda list of effective procedures suitablefor audit (Benbow et al.,1997). Thepresent framework draws almost
31
Manual Revision of the Uterus
The delivery of the placenta is the nextpoint at which appropriate care is vital.At this point the major risks for themother are postpartum haemorrhageand retained placenta. The routinemanual revision of the uterus postdelivery is an example of anotherwidely used and yet inappropriatetechnology. Manual revision of theuterus refers to the practice ofchecking the contents of the uterus byhand for retained sections of theplacenta. The process, as well as beinguncomfortable for the newly delivered,episiotomised mother, increases therisk of postpartum infection, can causeshock or mechanical trauma and is ofno proven benefit.
Pain Relief: Behavioural andDrug Based Methods
A woman’s experience of pain inlabour may be modified by a variety ofcircumstances, including the culturalcontext, the support she receives fromcaregivers and companions, and thelabouring environment (Enkin, 1995).Anumber of factors can result inintensified feelings of pain such asabnormal labour, prolonged orcomplicated by dystocia, induced oraccelerated by oxytocics orinstrumental delivery (WHO, 1994).
The study of pain transmission and itsmodulation has provided findings thatare applied in a variety of behaviouralapproaches to relieving the pain ofchildbirth. These have been classified
by Enkin et al., 1995) as:
� Techniques that reduce painfulstimuli, such as maternalmovement and position changes,counter pressure (steady strongforce applied to an area of thelower back during labour).
� Techniques that activate peripheralsensory receptors such assuperficial hot and cold, immersionin water, during labour, touch andmassage and acupuncture andacupressure.
� Techniques that enhancedescending inhibitory pathwayssuch as attention focusing anddistraction, hypnosis, or music andaudio-analgesia.
Pharmacological control of pain inchildbirth has a long history.The use ofopiates was mentioned in earlyChinese writings. There have beenmore clinical trials of pharmacologicalpain relief during labour and childbirththen any other intervention in theperinatal field (Enkin et al., 1995).Methods have been classified as:
� Systemic agents such as narcotics,sedatives and tranquillisers.
� Inhalational analgesia (such as,nitrous oxide).
� Regional analgesia, usually epiduralor spinal analgesia.
For many in the developing world,access to drug based methods of painrelief are very limited. More
30

As trauma to the perineum andproblems with healing are a significantcomponent of maternal morbidity(Glazener et al., 1995) and can affectthe mothers ability to care for herbaby, perineal trauma should beminimised.When it occurs, polyglycolicacid suture should be used for perinealrepair (Enkin et.al. 1995; Sleep 1991).The use of polyglycolic acid materialsfor suturing causes less pain and lessuse of analgesia in the immediatepuerperium period in comparison withcatgut and non-absorbable sutures.
Whenever possible, women should beallowed to move and adopt whateverposition they choose for the birth.Upright posture in labour seems toshorten the length of the labour andreduce the need for drugs to augmentthe labour (Stewart et al., 1978;Nikodem, 1995). Exit interviews withwomen on discharge, or retrospectivesurvey questions can be used todocument position of birth and reasonfor that position. Many facilitiescontinue to insist that women assumethe supine position for delivery withno clear understanding of the reasonsfor this.
All women should have continualprofessional support in labour and thechoice of social support during labourand bir th (Hodnett and Osborn,1989a&b). Women who aresupported during labour and birth, notonly report a more enjoyableexperience but have better outcomes.The main social support giver shouldbe freely chosen (Benbow, 1997).Randomised trials on support inlabour by a single person havedemonstrated that continuousempathic and physical support duringlabour has a number of associatedbenefits.These include shorter labours,significantly less medication, fewerAPGAR scores below 7 and feweroperative deliveries (Klaus et al., 1986;Hodnett and Osborn, 1989a&b;Hemminki et al., 1990; Hofmeyr et al.,1991) The WHO (1996b) concludesthat a woman in labour should beaccompanied by people she trusts andfeels comfortable with. However, inorder to respect the privacy of otherwomen labouring in the same room,this may preclude male supporters inmany cultures. Social support can alsoreasonably be excluded fromoperative deliveries. Many hospitals inthe less developed world, as in thedeveloped world for many years,preclude all but staff from the labour
7) Women are always allowed thesocial support of their choiceduring labour and birth.
6) For a non-complicated deliverywomen are always allowed toadopt whatever position theychoose for delivery.
33
exclusively on the RCOG guidelines,but there are other sources fromwhich good-practice criteria can beobtained (see the WHO SafeMotherhood series). Table 5 in theAppendix provides a selection ofauditable procedures of good practiceidentified in the RCOG report.Number 8 is drawn from the WHOMother and Baby Package. While thecriteria selected are not in any wayexhaustive their inclusion in any qualityassessment of the type suggestedwould be relatively straightforward,and subsequent findings suggestive ofthe quality of the general level ofclinical practice.
The following criteria are suggested(see also Table 5 in the Appendix):
Eclampsia causes as many as 50,000maternal deaths a year world-wide. Itis widely recognised that magnesiumsulphate is the best treatment foreclampsia. A large multicentred,international, randomised trial (TheEclampsia Trial Collaborative Group,1995) showed that it is better attreating and preventing fur therseizures than either diazepam orphenytocin, other popularly used drugs(Royal College of Obstetricians andGynaecologists 1996).
Women who have had a Caesareansection should be actively consideredfor a subsequent vaginal delivery takinginto account the reason for theprevious section (Flamm et al., 1988;Rosen et al., 1990; Rosen et al., 1991).
The use of prophylactic antibiotics atthe time of an emergency Caesareanhas been shown to decrease theincidence of post-operative infectiousmorbidity such as pelvic abscess, septicshock and wound infection (Mungfordet al., 1989).
Evidence from randomised controlledtrials suggest that ventouse ispreferable to the use of forceps forlow-cavity operative vaginal delivery.The reason given for this is thatventouse is associated with reducedmaternal trauma, without any increasein fetal trauma (Johanson 1995, andDrife 1996).
5) When repairing perineal wounds,polyglycolic acid suture material isused.
4) Ventouse delivery is theinstrument of first choice for low-cavity operative vaginal delivery.
3) Prophylactic antibiotics are usedroutinely at the time of anemergency Caesarean section.
2) Women are actively consideredfor a vaginal delivery after oneCaesarean section.
1) Magnesium Sulphate is the drugof first choice for the treatmentof eclampsia.
32

deaths is the result of infection. Fever isthe main symptom, and antibiotictreatment is the main cure. Puerperalinfection is more likely after aCaesarean section, prolonged labour,early rupture of the membranes andfrequent vaginal examinations. Stricthygienic measures during labour areimportant for preventing puerperalsepsis (WHO, 1994). Birth attendantsshould be attentive of early signs ofpuerperal sepsis and institute adequatetreatment promptly. The choice ofantibiotics will differ from country tocountry, due to local availability,patterns of causal agents and antibioticsusceptibility (WHO, 1998)
For the management of puerperalsepsis:
� All women and birth attendantsshould be aware of the requirementsfor a clean delivery: clean hands,clean delivery surface, clean cordcutting and care.
� Health staff should be trained torecognise puerperal sepsis andmanage it appropriately or refer.
� All facilities should be able to providethe necessary treatment forpuerperal sepsis, including antibioticsand surgical procedures.
3) Eclampsia and pre-eclampsia arecommon complications of pregnancy.Pregnancy-induced hypertensionusually occurs in the second and thirdtrimester of pregnancy. If untreated,pre-eclampsia may lead to eclampsia,
with very high blood pressure,convulsions, cerebral haemorrhage ororgan failure. Once eclampsia develops,immediate treatment and rapiddelivery are needed. Eclampsia isestimated to occur in about 1 in 100 to1 in 1,700 deliveries in developingcountries (Crowther, 1985). Betweenfive to seventeen percent of womenwho develop eclampsia die.Those whosurvive may suffer paralysis, blindness,or chronic hypertension and kidneydamage.
For the management of severe pre-eclampsia and eclampsia:
� Health staff should be trained tomanage and refer women withpregnancy induced hypertension.
�The full range of services required tomanage severe pre-eclampsia andeclampsia should be available atComprehensive Essential ObstetricCare (CEOC) facilities.
4) Unsafe abortion is responsible for anestimated 13% of the 585,000maternal deaths that occur each year.
‘The prevention of abortion-relatedmaternal mortality is dependent on theemergency abortion care beingintegrated through the health-caresystem of every country, from the mostbasic rural health post to the mostsophisticated tertiary level facility, 24-hours per day. Whether it is healthinformation and education, stabilizationand referral, uterine evacuation, orspecialized care for the most severe
35
and delivery wards. This element ofgood care is also an important part ofa woman’s experience of care (se 6.2.7emotional support).
A woman’s pulse, temperature, bloodpressure, fluid intake and urine outputshould be monitored regularlythroughout her labour and delivery.
6.1.6 Management ofEmergencies
The primary direct causes of maternaldeath world-wide include:haemorrhage (25%), sepsis (15%),hypertensive disorders (12%), unsafeabortion (13%) and obstructed labour(8%) (WHO, 1994). Facilities need theessential drugs and equipment tomanage specific conditions andqualified staff who are trained torecognise, treat or refer suchconditions. This framework identifiescriteria that are indicative of thecapacity of facilities to provide highquality clinical care (see Table 6 in theAppendix). For a more completeexamination of the indications for, andapproaches to, the management of theabove emergencies, refer to the WHOMother and Baby Package (1994) andA Guide to Effective Care in Pregnancyand Childbirth (Enkin et al., 1995).
1) Postpartum haemorrhage is the
single most important cause ofmaternal death. It is estimated that150,000 women die of postpartumhaemorrhage each year. Nearly 90% ofwomen who die from postpartumhaemorrhage, die within four hours ofdelivery (Kane et al., 1992) indicatingthat they are a consequence of eventsin third stage of labour (WHO, 1998).Hospital studies suggest that about 2 to3% of women haemorrhage duringdelivery. In the majority of cases, uterineatony and retained placenta areresponsible for the haemorrhage, butvaginal or cervical lacerations and(occasionally) uterine rupture orinversion play a role (Kwast, 1991).
For the management of postpartumhaemorrhage:
� Oxytocics should be available at allfacilities and health staff should betrained to administer them byinjection as a first aid measure forpostpartum haemorrhage.
� Health workers of an appropriatelevel should be trained in clinical skillsto manage ante and postpartumhaemorrhage.
� IV fluids should be available at allfacilities and blood transfusionservices should be available atcomprehensive essential obstetriccare units on a 24-hour basis.
2) Puerperal infections such as sepsisare still major causes of maternalmortality in many developing countries.In some places, as many as one in three
8)Throughout labour a womansphysical well-being should beregularly assessed.
34

For the management of prolongedand/or obstructed labour:
� The partograph should beintroduced at hospitals and healthcentres where staff with appropriateskills and training are available.
� First level health centres should beable to effectively perform thefollowing: emptying of bladder, givingantibiotics if rupture of membranesoccurred more than 12 hourspreviously, rehydration and referral.
� In addition to the above mentionedsecond level health centres shouldbe able to rupture membranes ifrequired and perform a vacuumextractor delivery.
� Additional interventions, such asoxytocics, antibiotic and thecapacity to perform Caesareansection and other surgicalprocedures should be available atCEOC hospitals, on a 24-hourbasis.
37
complications, at least some componentsof emergency abortion care must beavailable at every service delivery site inthe health-care system’ (WHO, 1994a)
One of the most positive steps that canbe taken is to provide life-saving care atthe lowest possible level of the healthsystem, in order to maximise the chancesthat the woman will reach that carebefore it is too late (WHO 1994a).Thefirst referral level must be able to buildon the services provided at the primarylevel by providing life-saving surgical andmedical procedures for all but the mostserious abortion related-complications.
For the management of abortion relatedcomplications:
� Health workers should be trained inthe early recognition of abortionrelated complications.
� Evacuation of the uterine contents,antibiotic therapy and intravenousfluids should be available at all facilitiesand surgical treatment at CEOChospitals.
� Treatment should always be followedby counselling and contraceptioninformation and services.
5) Prolonged labour is defined as activelabour with regular uterine contractionsand progressive cervical dilatation formore than 12 hours (WHO, 1994).Obstructed labour occurs whenprogress is arrested by mechanicalfactors and delivery by Caesareansection is required. Prolonged labour isstrongly associated with several adverse
outcomes. It can lead to perinatalasphyxia, maternal exhaustion and evenmaternal death (Enkin et al., 1995).Thepurpose of monitoring progress inlabour is to recognise early problems, sothat their progression to seriousproblems can be prevented. A cervicaldilatation rate of 1 cm per hour in theactive phase of labour is often acceptedas the cut-off between normal andabnormal labour, however manywomen who show slower rates ofcervical dilatation proceed to normaldelivery. The definition of normalprogress should therefore beinterpreted with discretion in thecontext of the woman’s overall well-being (Enkin et al., 1995). Whenmonitoring the progress of labour,recording the findings makes the degreeof progress readily apparent, so thatproblems will be recognised early, andto facilitate transfer of information toother caregivers (Enkin et al.,1995).TheWHO recommends that thepartograph should be introduced athospitals and health centres where staffwith appropriate skills and training areavailable.The partograph is a structuredgraphical representation of the progressof labour that can be an effective toolfor the early recognition of obstructedlabour. Too much reliance onpartographs however, can be an agentfor regimenting labour rather thancaring for the woman in labour,especially when strict protocols ofaction related to partograph patternsare followed (Enkin et al., 1995).
36

converge to impact patterns of healthutilization, compliance with recommendedmedical interventions, and healthoutcomes. Increased sensitivity [in turn]can facilitate positive interactions withthe health-care delivery system andoptimal-health outcomes for the patientserved, resulting in increased patient andprovider satisfaction’.
(American College of Obstetrics andGynecology, Committee on Health-care for Underserved Women, 1998).
A womans experience of care can bedivided into four broad areas: hercontact with and experience of humanand physical resources; her cognition,that is, the level to which sheunderstands what is happening to herand why; the respect, dignity and equityof care she receives throughout herstay at the facility; and, finally, theemotional support she receives duringher labour and beyond.
6.2.1 Human andPhysical Resources
A womans experience of care relatesnot only to the quality andappropriateness of the obstetric careshe receives and her perception of thequality of that care, but also to herimpression of the state of theinfrastructure (the bed, sheets, food,toilets and so on). Her experience ofcare here refers also to her experienceof actual contact time with qualifiedstaff. This is distinct from herimpression of how staff treated her
during an interaction (see 6.2.3 onrespect, dignity and equity). Areproviders qualified to undertake thetasks they are responsible for, and isthe time they spend with clientssufficient? For example, criteria herewould help identify whether or notwomen are being left alone forextended periods, or whetherunqualified personnel are undertakingcertain duties that should be theresponsibility of nurses or midwives.
In a study that examined the meaning ofquality for women who receivedreproductive health services at a non-governmental family planning andmaternal and infant care clinic inSantiago, Chile the clinic’s cleanlinesswas regarded as a sign of respect forthe client and its hygienic conditionsrelieved fears of infection (Vera, 1993).Women also referred to the quality oftime and attention they received as animportant element of overall quality.They described having to wait for hoursand hours as characteristic of thegovernment health services. In the clinicin question, women felt they were giventhe time to both talk and learn: ‘theyexplain things’. For the womeninterviewed in this study a high qualityof health services meant treatment thatincluded the following elements: a clean,hygienic place, prompt service, accurateinformation, an opportunity to learn,and enough time to consult with staffand receive advice (Vera, 1993).
39
While the quality of the provision ofcare in facilities is fundamental toensuring effective care, women’s actualexperience of care is also significant. Ifwomen’s cumulative experience at afacility is such that it deters some fromreturning for a subsequent delivery, orleads to rumours to the same effect inthe wider community, the actual qualityof the provision of care for thesewomen is academic. The SafeMotherhood study in Nigeria reportedfindings from focus groups in whichparticipants cited a litany ofinadequacies that they expected toexperience at health services, includingpoor hygiene and medical treatment,and censure or abuse from healthworkers. Cost, convenience andkindness were principal factors in thechoice of health-care provider (Okaforand Rizzuto, 1994). A study in Zairethat identified qualities that womenthought should be found among healthworkers showed that they valuedinterpersonal qualities (respect,patience, courtesy, attentiveness,friendliness and straightforwardness),technical qualities and, to a lesserextent, integrity (Haddad and Fournier,1995). When they were asked aboutthe two best qualities a nurse shouldhave, the majority mentioned arelational component first and atechnical component second. Thisobservation is supported by findings
from studies conducted in a variety ofsettings (Calnan, 1988a; Bruce, 1990;Lohr et al., 1991;Vera, 1993).What thissuggests is that the provision of carecould be of the highest technicalquality yet still be unacceptable to thewomen and families for whom thecare is intended.
To help reduce the number of womenpresenting late once in labour, and toincrease overall utilisation, facilitiesneed to concern themselves with theexperience of care that womenreceive during their contact with thefacility.While effective antenatal care inthis respect is vital, this qualityassessment tool has been designed toassess only care internal to a facility.However, late presentation (within onehour of delivery) is one indication ofpoor communication of healthmessages at contact opportunitieswith women during pregnancy; forexample, at an antenatal visit orhospital admission for a complicationin pregnancy. The criteria selected toassess the woman’s experience of careincludes indicators to measure thequality of information exchange, whichcan be fundamental to, among otherthings, ensuring patient compliance andother such outcome indicators.
‘During every health-care encounter, theculture of the patient, the culture of theprovider and the culture of medicine
38
6.2 Experience of Care

not always equate to good qualitycare. There are other means ofassessing whether or not she receivedadequate information in a specificcircumstance. For example; if an infantdies within hours of birth and his/hermother is unable to give anyexplanation for the cause of deathbefore being discharged, this is a strongindication that the standard of care shereceived (information exchange) fellbelow an acceptable standard. Arecent study in urban India observedthat the quality of information exchangeappeared to be consistently lower forilliterate women (Matthews et al., 2000).Also, in the case of episiotomy, manywomen did not know this was going tohappen to them, nor did they know thattheir uterus was about to be revisedmanually, without anaesthetic, afterdelivery both providing evidence thatwomen were not being adequatelyprepared for certain particularlyuncomfortable and often inappropriateprocedures.
Women interviewed by Campero et al.(1998) in a study examining theinfluence of support in labour in a socialsecurity hospital in Mexico madeconstant reference to the lack ofinformation provided by the medicalstaff regarding their health and that oftheir babies, the hospital routines andmedical interventions. The informationthat was provided was reported ashaving been delivered in an authoritarianand vertical manner such that thewomen did not have a chance to speak,
let alone ask questions. It was reportedlytaken for granted that the womanwould accept whatever the doctor toldher: We’re going to examine you We’regoing to remove the drip’ and so on(Campero et al., 1998, p. 398). Withregard to the degree to which womenreceived information about their ownlabour and delivery, this study found thatit was often hard to know exactly whatwomen had been told about aCaesarean section, for example. Evenwhen the doctor gave the woman someinformation, almost no one in the studyunderstood it, and the information wasoften inaccurate and confusing. Somewomen consequently felt guilty andthought that the indication for aCaesarean section was theconsequence of their poor effort duringlabour (Campero et al., 1998). Likewise,with regard to episiotomies, lack ofinformation resulted in some womenperceiving it was their fault that theepisiotomy had to be performed. As inthe study in urban India, some womenwere not even aware that it had beenperformed until afterwards.
Whether or not a woman clearlyunderstands what is happening, why, andany specific instructions will determineher subsequent behaviour. In maternitycare, postpartum health is vital and it isessential that a woman returns for apostnatal check. She also needs to beaware of symptoms that may signal acomplication postnatally, such as fever orfoul-smelling discharge, and know whatto do in the case of such a development.
41
Criteria that may be selected as part ofa quality assessment of this aspect ofcare include:
1)The physical infrastructure and theoverall environment of the maternitywards are acceptable to all/mostwomen.
2) Contact time with qualified staff issufficient.
3) Male/female staff ratios areacceptable to most women.
4) Staff are competent to provideappropriate care.
(see also Table 7 in the Appendix)
6.2.2 Cognition
One aspect of care that Donabedian(1988) drew attention to in his modelwas the interpersonal care. Thisconsisted of communication betweenthe client and provider for the purposeof both diagnosis and thedetermination of preferences fortreatment. The relationship betweenthese two parties should becharacterised by ‘privacy, confidentiality,informed choice, concern, empathy,honesty, tact and sensitivity’.
Cognition relates to two specificexperiences of care:
� The extent to which a woman feelsshe understands what is going onand feels that her questions havebeen answered adequately.
� Whether she actually receives
sufficient information in a form thatshe and her family can understandand that she has the right to know.
Cognition depends on what Brucerefers to as provider-client informationexchange (Bruce, 1990). How effectivethis information exchange is dependson having adequately trained andqualified staff and a positive client-provider interaction. An analysis ofwomen’s demand for services in SouthAsia identified this aspect of care as acrucial factor explaining women’s useof medical services (Leslie and Gupta,1989). Reasons that have been givenfor under-utilisation of available healthservices include poor relationsbetween health-care providers andtheir clients (Jacobsen, 1991). Womenoften have questions that they hesitateto raise with the typical Western-trained or male provider, fearing thatproviders are too busy to attend to awomen’s real concerns, or that suchquestions would be considered stupid(Simmons and Elias, 1994; Lubis et al.,1992). The clients view that providersmight consider them stupid is oftenwell-founded (Simmons and Elias,1994).
Questions included in an exitinterview or survey questionnaireschedule can address whether thewoman was happy with theexplanations she received, whether sheunderstood what was going on,whether she was confused andignored, and so on. Positive responsesor not-negative responses, however, do
40

complaints about certain routineinterventions such as vaginalexaminations were expressed with asense of shame: ‘It’s the first time anyoneever did that to me. It made me feel verystrange [and] ashamed that everyonewas seeing it, and that they were doing itin front of other people.’ Othercomplaints about vaginal examinationsreported in this study concerned pain:‘Why are they so rough?, Why don’t theywait until the contraction is over?’(Campero et al., 1998).
Modern medical facilities have a cultureof their own that often clashes with theculture of the potential users(Finerman, 1983). An investigation in avillage in Rajasthan produced anecdotalevidence from in-depth interviews thatvillagers were generally perceived asdirty and ignorant of modern ways inthe government hospital. The womanand her attendants were found to feeluncomfortable in the hospital, and theyreported feeling insulted and ignored.In the village the common image of ahospital delivery is one in which noattendants are allowed near thelabouring woman and she is made tolie on a table all by herself: ‘Is this theway to treat a labouring woman?’ (Patel,1991).
There are cultural practices thatcurrently have no place in modernhospitals in the developing world but ifrecognised by institutions, assuming theydid not interfere with the provision ofhigh quality care, would greatly enhancewomen’s experience of care and may
even be beneficial. The squattingposition for childbirth, traditional inmany cultures, is known to promote theprogress of labour more effectively thanthe supine position typically used inhospital settings (Rohde, 1995). Theadoption of such a tradition byproviders would have multipleadvantages (with appropriate training ofbirth attendants). In addition, in manyareas the placenta is considered to haveenormous ritual significance and formspart of the celebration of the new life.In hospital settings, placentas aregenerally routinely disposed of and thefamily given no choice in what is doneto this symbolic part of the newborn.Some hospitals in Cochambamba nowprovide the placenta to families onrequest (Rohde, 1995).
If a woman and her family are treatedwith disdain and disrespect, if she isignored and subjected to unnecessary,uncomfortable and humiliatingprocedures, it would not be surprisingthat if given a choice she and her familysubsequently chose to deliver at home,or at an institution where she expectedto receive higher quality care. Beingtreated like a person was the singlemost frequent theme in Vera’s study ofwomen’s attitudes to quality ofreproductive health services in Santiago.Other elements identified as importantto quality by the women interviewed inthis study included treatment as anequal in transactions and ‘cordial,likeable, friendly staff’ (Vera, 1994).
43
High quality provider-client informationexchange is more than a nicety that maycontribute to a positive experience: it isa medical necessity. It has been arguedthat the interpersonal process is thevehicle by which technical care isimplemented and on which its successdepends (Donabedian, 1966). It is thetask of the provider to give the womanas much information and explanation asshe desires and needs (WHO, 1996b).
Criteria that may be used tomeasure this aspect of care include:
1) Necessary information isconveyed effectively in a languagethat is understandable to allwomen.
2) All women are fully prepared fortreatment and understand theiroptions. Where possible theyexperience real informed choice.
3) The reasons for a specificintervention or outcome arealways clearly explained to allwomen
4) Information about postpartumcare is effectively conveyed.
(see also Table 8 in the Appendix)
6.2.3 Respect, Dignityand Equity
Client-provider exchanges reflect andare shaped by what Simmons and Elias(1994) refer to as latent dimensions ofprogramme-client interactions, whichare relatively hidden but nonetheless
powerful components of theinteractions. Such components reflectthe fundamental differences in thestatus, power and culture ofparticipants in the encounter(Simmons and Elias, 1994). Theseinteractions are rarely characterised bysupportive relationships, more oftenexpressing dissonance, inherent conflictand social disparities (Simmons andElias, 1994; Mernissi, 1975; Nichter,1989; Scrimshaw, 1974; Misra et al.,1982).
There are numerous instances duringlabour and delivery where staff can failto treat women with the respect anddignity they have the right to expect.This includes the observance of herprivacy and dignity during physicalexaminations, late-stage labour anddelivery. All women’s privacy in thebirthing setting should be respected(WHO 1996b). Insensitive treatment,poor standards of confidentiality,tactlessness and moral judgements byhealth providers are all elements ofpoor quality care documented bynumerous studies as women’sexperience of care (Lasker, 1981;Finerman, 1983; Wedderburn andMoore, 1990). A study of public-healthunits in the Rakai district of Ugandafound that some midwives wereperceived as rude, proud, negligent andvulgar. Some young midwives were alsosaid to abuse mothers if they had neverattended antenatal care, or if they hadhad many pregnancies. Campero et al.(1998) report that in Mexico, women’s
42

labour ; explaining in clear andunderstandable terms, the medicalindications and procedures; answeringquestions; encouraging the woman toadopt the most comfortable positionspossible; suggesting how to relax, breathand push when appropriate; givingmassages; holding hands and gentlycaressing the woman; offering her thebedpan; and changing the bed clotheswhen necessary’
(Campero et al., 1998, p.397).
The findings were that those womensupported by a doula had a morepositive birth experience. It has alsobeen shown that support during labouraccelerates recovery, favours earlybonding between mother and child,decreases anxiety and depressionduring the first six weeks postpartumand reduces the time spent in labour(Klaus and Kennell, 1992; Hofmeyr andNikodem, 1991). In light of thesefindings, it has been recommended thatall women should have continualprofessional support in labour and thechoice of social support during labourand birth (Hodnett, 1997).
Women who are given support in theform of receiving adequate informationor encouragement are reported asfeeling a greater sense of control overtheir labour. Control has beenrecognised as a key component in alabour process experienced assatisfactory. In addition while a womanexpects to have some degree ofcontrol her primary satisfaction and
self-esteem depend on whether shecan achieve it (Campero et al., 1998;Butani and Hodnett, 1980; Kitzinger,1990; Hillan, 1990). In addition to awoman’s immediate experience of careand childbirth, the influence of thoughtsand feelings about her childbir thexperience on later self-perception aswomen and mothers has beenemphasised (Campero et al., 1998;Simkin, 1992; Konrad, 1987).
Emotional support in this context refersnot only to a woman’s access to herown social and emotional support butto emotional support given bymembers of staff. Professional birthattendants need to be familiar not onlywith their medical tasks but also withtheir supportive tasks, both of whichthey need to be able to perform withsensitivity and competence (WHO,1996b)
45
Criteria that may be used to assess thisaspect of care include:
1) All facilities have an individualresponsible for assessing socio-economic and cultural context ofthe catchment area and aneffective mechanism for feedingrelevant recommendations toproviders.
2) All women feel they have beentreated with appropriate respect.
3) Women do not have to undergoany unnecessary and humiliatingprocedures.
4) Cultural practices that do notinterfere with high quality careare respected.
5) All women are treated with thesame standard of care regardlessof education, class, caste and age.
6) Services are appropriately pricedfor the catchment.
(see also Table 9 in the Appendix)
6.2.4 Emotional Support
Many factors in the birth environmentcan induce stress.The setting and manyof the people in it may be strange tothe labouring woman. Fear, pain andanxiety may be increased by amechanised clinical environment andunknown attendants, with potentiallyadverse effects on the progress oflabour. A hospital environment, whereseparation of family members and rigidprotocols are enforced is one of the
factors believed to cause the highintervention rates during labour thatare seen in many industrialised societies.
There are numerous studies, thathighlight the relationship betweenpsycho-social support and thereduction of various types of medicalinterventions such as the use of forceps,analgesics and Caesarean sections (Sosaand Kennell, 1980; Klaus and Kennell,1986; Keirse and Enkin, 1989; Kennelland Klaus, 1991).
The needs of a woman in labour aredivided into three parts by Butani andHodnett (1980).The first is the need tomaintain her self-control, the secondthe need to live up to certainexpectations, and the third the need topreserve her self-esteem. In Mexicothese needs were fulfilled by doulas(birth attendants) in a recent study thatevaluated the effects of the provision ofpsycho-social support to first-timemothers during labour, childbirth andthe immediate postpartum period in asocial security hospital. Women wereoffered cognitive, emotional andphysical support by a doula who helpedthe woman maintain a positiveemotional state throughout labour andchildbirth (Campero et al.,1998).Supportive strategies identified andused in this study included the following:
‘Talking to the soon-to-be mother in anencouraging and soothing language;recognising the woman’s labour efforts;maintaining constant eye contact; givinginformation about the progress of her
44

The framework has two possiblefunctions.The first is as a tool by whichto help structure a situation analysisreview of the quality of care provided ata facility, and experienced and perceivedby its clients, actual and potential. Thesecond is as a tool by which to improvethe quality of care through the ongoingcritical examination of activities,compared with an agreed standard.Where care falls short of agreedstandards, a process can then beinstigated to identify opportunities andimplement change to bring practicecloser to the standard. The danger isthat, unless implemented appropriately,the assessment process will not result ineffective change. In a review of perinatalaudits, Mancey-Jones and Brugha.(1997) conclude that: ‘Successful changeis more likely where the audit process isadapted to suit the local culture, wherethose who need to implement change areinvolved in identifying problems anddeciding how to address them, whererecommendations are appropriate toavailable resources and build on existingpractices’ (Stocking, 1992, Atkinson andHayden, 1992; Greco and Eisenberg,1993)
The successful implementation of aquality assessment is as much aboutcontent as it is about process.Amoono-Lartsen (1985) concluded that whenperformance criteria are agreed uponas achievable and acceptable by health
centre staff, their use in evaluatingquality of care can provide an impetusfor improving care and in-servicetraining of staff. While feeding resultsback to staff is a necessary componentof the assessment process, research hasgenerally found that in the absence ofexplicit recommendations, little impacton practice is observed (Mancey-Jonesand Bruga, 1997; Mugford et al., 1991;Mooney and Ryan, 1992; Robinson1994). Mancey-Jones and Brugaconclude that the impact of activefeedback where data is disseminatedwith specific recommendations, isuncertain. While some authors indeveloping countries have reportedshort-term improvements in clinicalpractice, following a clinical audit(Mitchell and Fowkes, 1985), othershave reported that active feedbackalone has failed to change practice evenwhere the relevant practitioners haveacknowledged the need for change(Lomas, 1991). In practice,recommendations will often need to besupported by additional time andresources such as further education andtraining and supportive supervision.Where the lack of obvious signs ofimprovement resulting from anassessment process is partly the resultof inadequate resources, staff moralewill be difficult to sustain.
In their review of literature onperinatal audit in developing countries
47
Criteria that may be used to assess thequality of the experience of care in thisrespect include :
1) Except in exceptional cir-cumstances women are able tochoose freely the social supportthey receive in labour and atdelivery.
2) All women are treated withhonesty, kindness andunderstanding.
3) In the event of a death ordisability, appropriate levels ofprofessional and emotional careare made available to women andtheir families.
4) All staff are aware of theirsupportive role in the provisionof care during labour, delivery andthe immediate postpartumperiod
5) An effective process exists in allunits through which providers areable identify and respond to userexpectations.
(see also Table 10 in the Appendix)
7 Use of the Framework
46

How the assessment process is organised will vary depending on multiple factors;management style: location, political will, financial backing and so forth. However,certain features need to be in place for it to bring about measurable change.These have been explored by Cleaves (1980); Stocking (1992); Greco andEisenberg (1993) and Walt (1994) and adapted by Mancey-Jones and Bruga(1997) who divide the factors necessary to facilitate change into four groups:context, content, process and actors (see Figure 2).
Figure 2
Context The local culture is accepting of the concept of ‘constructive criticism’Environment is non-threatening, open and supporting of changeThe assessment and recommendations are appropriate to the level of resources
Content Proposed change is appropriate for the specific problem identifiedChange is recognised as likely to be effective, supported by research of consensus opinionChange is compatible with current beliefs and practicesChange represents a small incremental change from current practicesProposed change is simple, involving few individuals
Process A combination of a number of strategies are used to implement the change including:Recognition of positive behaviourPresentation of supportive evidence from researchEducation activities and supervisionFollow-up audit and feedbackFinancial incentivesAdministrative regulations
Actors Willing to participate in audit processRecognise need for change and improvementFeel involved in the decision makingPersons in position of power committed to change and improvementPersonal incentives for change
Source:Taken from Mancey-Jones and Bruga 1997
Factors facilitating implementation of change
49
Mancey-Jones and Bruga (1997) alsoreport finding no published systematicevaluations from developing countrieson the effects of perinatal audit onspecific elements of practice, nor onparticipants knowledge, attitudes ormotivation. In published work theyreport that assertions about thepositive impact of audit on staffmorale, motivation andcommunication are not substantiated.Audit does not necessarily have apositive effect on participants attitudesas it may be perceived as threatening,and the critical analysis necessary inthis type of process may lead to adeterioration of staff relationships,particularly in cultures where criticismis experienced as aggression.Preliminary findings from an ongoingstudy involving maternal near missaudits in hospitals in West and NorthAfrica suggest that while staff oftenreadily identify examples ofsubstandard care, translating therecognition of poor quality care intopositive behaviour change is a morecomplex process.The steps needed toyield such change and so improveoutcome are still not clear (Ronsmans1999). Little improvement in theprovision of quality of care can beexpected until the process ofimplementing a successful assessmentis better understood.
8 Implementing Change
48

51
The provision of a high quality of careat maternal health facilities is not aluxury but a necessity. There issubstantial evidence to suggest thatthere is a relationship between thequality of care that a facility provides,and patterns of utilisation. The moreintuitively obvious relationshipbetween quality of care and outcomeis better established. Less is known,however, about the mechanismsthrough which both of theserelationships function. Clearly, thequality of institutional delivery servicescan make the difference between lifeand death, but before change can beinitiated to improve quality it isimportant that we understand thesemechanisms. To analyse theserelationships effectively, instrumentsthat capture the complex nature of thediverse aspects of quality need to bedeveloped and tested within a range offacilities in a variety of contexts. Atpresent, in the field of maternal health,despite an extensive literature devotedto many different aspects of quality inmaternity care, no integrated approachto the evaluation of services has yetbeen established.
In this monograph we draw togetherexperience and evidence from theextensive medical, health policy andsocial science literature that exists onall aspects of quality in maternity careto create a flexible quality assessment
framework specifically for use at theinstitutional level in developingcountries. It divides quality into twoelements that are conceptually distinctbut closely related in practice: firstlyinto the provision of quality of care,and second into elements relating toclient’s experience of that care. Thesetwo important aspects of quality ofcare in pregnancy and childbirth areintrinsic components of a basicreproductive rights approach. Thebenefits of improving quality of care tomothers at delivery are multiple. Notonly could we expect to see anincrease in timely and effective use ofservices, and improved psycho-socialand health outcomes, improved qualityhas been shown to curtailinappropriate use of limited resources,reduce the use of ineffective andharmful technologies, eliminateinefficiencies, optimise the use ofexisting inputs and promote thefollowing of correct procedures. Withreal political will, and the allocation ofnew resources for safe motherhood,quality of care in maternal health canbecome a reality.
50
9 Conclusion Appendix

5352 Table 1: Human and Physical Resources (Provision of care)
Criteria
The skill mix is appropriateto cope with the patient flowand case mix at the facility.
The maternity wards areadequately equipped toperform their functioneffectively and consistentwith internationallyrecognised good practice.
The operating theatre is ingood repair and fullyequipped with drugs andsurgical equipment toperform life savingprocedures when required.
The general infrastructure ofthe facility is of sufficient sizeand state to cope withdemand and essentialsupport services are reliable.
Standard
‘appropriate to cope’
‘adequately’‘effectively’‘consistent withinternationallyrecognised goodpractice’
‘good repair’‘fully equipped’
‘sufficient’‘reliable’
Suggested basis for indicators
•No. of qualified staff (experience, qualifications)•Terms and conditions of staff (hours, income, conditions)•Normal level of supervision•Staff attitudes (morale, job satisfaction)•Actual day-to-day staffing levels •Staff turnover•Staff training (quantity, content and attendance)
•Number of beds, blinds, toilets, handbasins etc per delivery•Quantity of essential drugs by sell-by dates•State of essential equipment•Nature of sterilisation procedures•Layout of wards•Diagnostic and therapeutic capabilities
•Physical layout of operating theatre/location•Quantity of essential surgical equipment•State of repair of equipment•Number and availability of qualified staff•Access to blood stocks•Quantity of essential medical supplies
•Structural features of physical infrastructure•Identify essential support services (electricity, running water,transport)•Reported reliability versus observed reliability•Frequency of maintenance of physical assets, vehicles andequipment•State of furniture, medical and office supplies, warehousing andstorage conditions
Sources
Facility RecordsProvider InterviewsObservation
Provider InterviewsObservationFacility Records
Facility Records Provider InterviewsObservation
Provider InterviewsObservationFacility Records Exit Interviews
Criteria
The organisational andmanagement structure of thelabour, delivery andpostpartum suite ensuresmost efficient use ofresources
Staff should always beadequately protected fromrisks associated with theirwork.
Effective systems formaintaining the quality of thehuman resource base shouldbe in place at all facilities.
All facilities should have aclear management structureand transparent lines ofaccountability
Standard
‘most efficient use’
‘always’‘adequately’
‘effective’‘all’
‘all’‘clear’‘transparent’
Suggested basis for indicators
•Nature of management capabilities •Evidence of management plan•Reported and observed administrative red tape•Financial inputs•Spending breakdown•Use of wasteful technologies•Over prescription or inappropriate use of drugs and interventions•Financial capacity•Transparency
•A written policy on violence to staff•Provision of security personnel where required•The existence and application of policies and practices forminimising exposure to body fluids•The existence and application of policies and practices for safedisposal of sharps•The existence and application of policies for the management ofneedle-stick injuries•The provision of Hepatitis B vaccination •Availability of HIV testing and post-exposure prophylaxis
•Appropriate and fair systems of reward and promotion•Listing of available training opportunities •The provision of study leave•The uptake of training courses •Evidence of in-service training including skill certification or portfolios
•Job descriptions for all positions•The existence and use of an organisational structure chart•Timeliness of salary payments•Staff knowledge of their responsibilities and the responsibilitiesof other staff members•Managers knowledge of their job descriptions and responsibilities
Sources
Facility RecordsProvider InterviewObservation
Facility RecordsProvider InterviewObservation
Facility RecordsProvider InterviewObservation
Facility RecordsProvider InterviewObservation
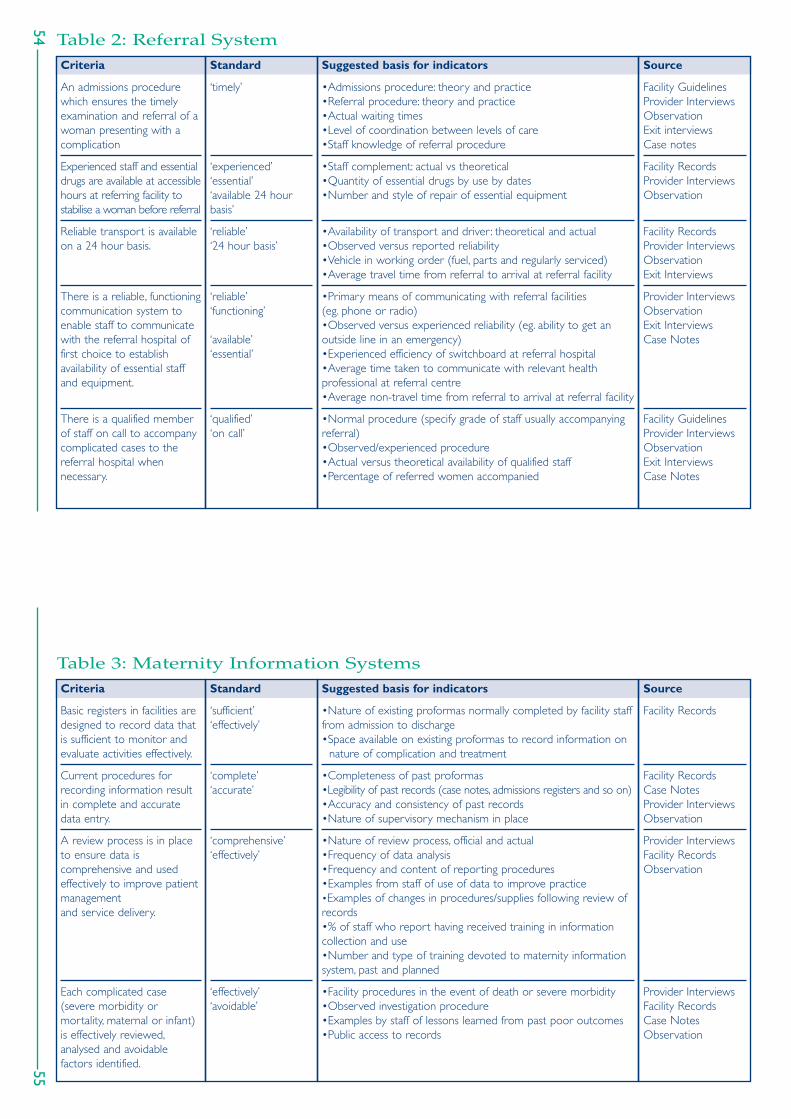
5554
Table 3: Maternity Information SystemsCriteria
Basic registers in facilities aredesigned to record data thatis sufficient to monitor andevaluate activities effectively.
Current procedures forrecording information resultin complete and accuratedata entry.
A review process is in placeto ensure data iscomprehensive and usedeffectively to improve patientmanagementand service delivery.
Each complicated case(severe morbidity ormortality, maternal or infant)is effectively reviewed,analysed and avoidablefactors identified.
Standard
‘sufficient’‘effectively’
‘complete’‘accurate’
‘comprehensive’‘effectively’
‘effectively’‘avoidable’
Suggested basis for indicators
•Nature of existing proformas normally completed by facility stafffrom admission to discharge•Space available on existing proformas to record information on
nature of complication and treatment
•Completeness of past proformas•Legibility of past records (case notes, admissions registers and so on)•Accuracy and consistency of past records•Nature of supervisory mechanism in place
•Nature of review process, official and actual•Frequency of data analysis•Frequency and content of reporting procedures•Examples from staff of use of data to improve practice •Examples of changes in procedures/supplies following review ofrecords•% of staff who report having received training in informationcollection and use•Number and type of training devoted to maternity informationsystem, past and planned
•Facility procedures in the event of death or severe morbidity•Observed investigation procedure •Examples by staff of lessons learned from past poor outcomes•Public access to records
Source
Facility Records
Facility RecordsCase NotesProvider InterviewsObservation
Provider InterviewsFacility RecordsObservation
Provider InterviewsFacility RecordsCase NotesObservation
Table 2: Referral SystemCriteria
An admissions procedurewhich ensures the timelyexamination and referral of awoman presenting with acomplication
Experienced staff and essentialdrugs are available at accessiblehours at referring facility tostabilise a woman before referral
Reliable transport is availableon a 24 hour basis.
There is a reliable, functioningcommunication system toenable staff to communicatewith the referral hospital offirst choice to establishavailability of essential staffand equipment.
There is a qualified memberof staff on call to accompanycomplicated cases to thereferral hospital whennecessary.
Standard
‘timely’
‘experienced’‘essential’‘available 24 hourbasis’
‘reliable’‘24 hour basis’
‘reliable’‘functioning’
‘available’‘essential’
‘qualified’‘on call’
Suggested basis for indicators
•Admissions procedure: theory and practice•Referral procedure: theory and practice•Actual waiting times•Level of coordination between levels of care•Staff knowledge of referral procedure
•Staff complement: actual vs theoretical •Quantity of essential drugs by use by dates•Number and style of repair of essential equipment
•Availability of transport and driver : theoretical and actual•Observed versus reported reliability•Vehicle in working order (fuel, parts and regularly serviced)•Average travel time from referral to arrival at referral facility
•Primary means of communicating with referral facilities(eg. phone or radio)•Observed versus experienced reliability (eg. ability to get anoutside line in an emergency)•Experienced efficiency of switchboard at referral hospital•Average time taken to communicate with relevant healthprofessional at referral centre•Average non-travel time from referral to arrival at referral facility
•Normal procedure (specify grade of staff usually accompanyingreferral)•Observed/experienced procedure •Actual versus theoretical availability of qualified staff•Percentage of referred women accompanied
Source
Facility GuidelinesProvider InterviewsObservationExit interviewsCase notes
Facility RecordsProvider InterviewsObservation
Facility RecordsProvider InterviewsObservationExit Interviews
Provider InterviewsObservationExit InterviewsCase Notes
Facility GuidelinesProvider InterviewsObservationExit InterviewsCase Notes
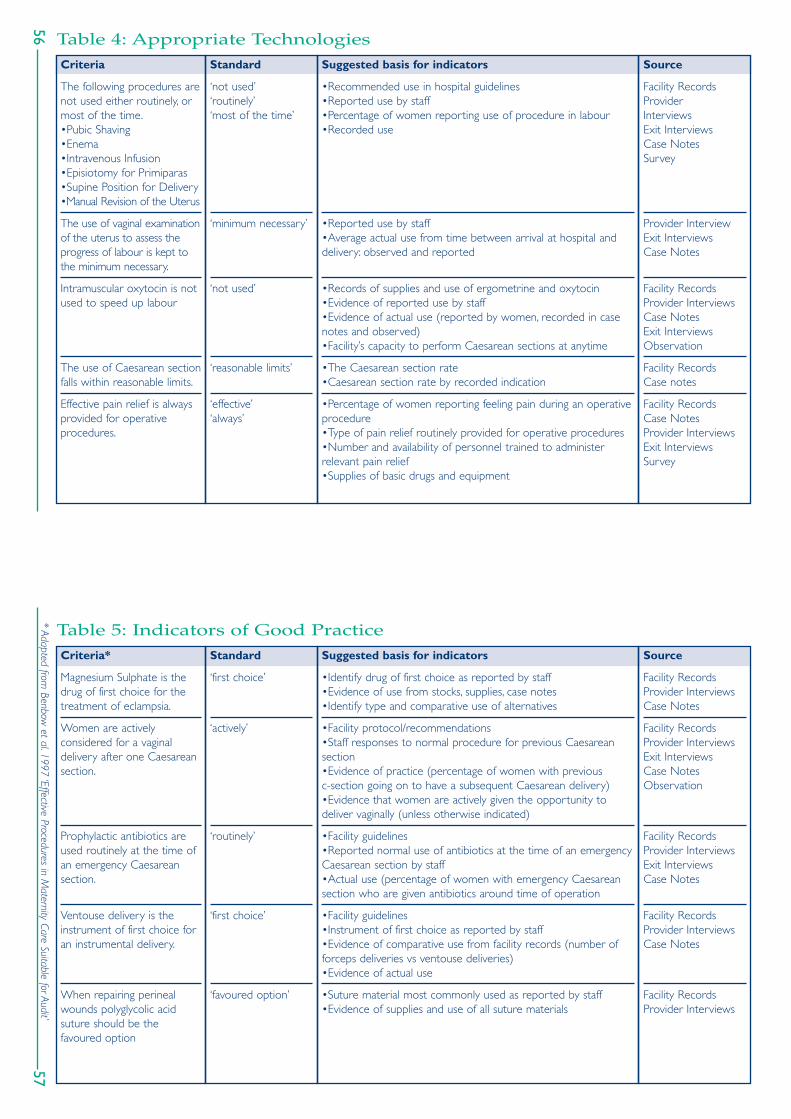
5756
* Adapted from Benbow
et al.1997 ‘Effective Procedures in Maternity Care Suitable for Audit’
Table 4: Appropriate TechnologiesCriteria
The following procedures arenot used either routinely, ormost of the time.•Pubic Shaving•Enema•Intravenous Infusion•Episiotomy for Primiparas•Supine Position for Delivery•Manual Revision of the Uterus
The use of vaginal examinationof the uterus to assess theprogress of labour is kept tothe minimum necessary.
Intramuscular oxytocin is notused to speed up labour
The use of Caesarean sectionfalls within reasonable limits.
Effective pain relief is alwaysprovided for operativeprocedures.
Standard
‘not used’‘routinely’‘most of the time’
‘minimum necessary’
‘not used’
‘reasonable limits’
‘effective’‘always’
Suggested basis for indicators
•Recommended use in hospital guidelines•Reported use by staff•Percentage of women reporting use of procedure in labour•Recorded use
•Reported use by staff•Average actual use from time between arrival at hospital anddelivery: observed and reported
•Records of supplies and use of ergometrine and oxytocin•Evidence of reported use by staff•Evidence of actual use (reported by women, recorded in casenotes and observed)•Facility’s capacity to perform Caesarean sections at anytime
•The Caesarean section rate •Caesarean section rate by recorded indication
•Percentage of women reporting feeling pain during an operativeprocedure•Type of pain relief routinely provided for operative procedures•Number and availability of personnel trained to administerrelevant pain relief•Supplies of basic drugs and equipment
Source
Facility RecordsProvider InterviewsExit InterviewsCase NotesSurvey
Provider InterviewExit InterviewsCase Notes
Facility RecordsProvider InterviewsCase NotesExit InterviewsObservation
Facility Records Case notes
Facility Records Case NotesProvider InterviewsExit InterviewsSurvey
Table 5: Indicators of Good PracticeCriteria*
Magnesium Sulphate is thedrug of first choice for thetreatment of eclampsia.
Women are activelyconsidered for a vaginaldelivery after one Caesareansection.
Prophylactic antibiotics areused routinely at the time ofan emergency Caesareansection.
Ventouse delivery is theinstrument of first choice foran instrumental delivery.
When repairing perinealwounds polyglycolic acidsuture should be thefavoured option
Standard
‘first choice’
‘actively’
‘routinely’
‘first choice’
‘favoured option’
Suggested basis for indicators
•Identify drug of first choice as reported by staff•Evidence of use from stocks, supplies, case notes•Identify type and comparative use of alternatives
•Facility protocol/recommendations•Staff responses to normal procedure for previous Caesareansection•Evidence of practice (percentage of women with previous c-section going on to have a subsequent Caesarean delivery)•Evidence that women are actively given the opportunity todeliver vaginally (unless otherwise indicated)
•Facility guidelines•Reported normal use of antibiotics at the time of an emergencyCaesarean section by staff•Actual use (percentage of women with emergency Caesareansection who are given antibiotics around time of operation
•Facility guidelines•Instrument of first choice as reported by staff•Evidence of comparative use from facility records (number offorceps deliveries vs ventouse deliveries) •Evidence of actual use
•Suture material most commonly used as reported by staff•Evidence of supplies and use of all suture materials
Source
Facility RecordsProvider InterviewsCase Notes
Facility Records Provider InterviewsExit InterviewsCase NotesObservation
Facility RecordsProvider InterviewsExit InterviewsCase Notes
Facility Records Provider InterviewsCase Notes
Facility RecordsProvider Interviews

59
Table 6: Management of EmergenciesCriteria
Sufficient stocks of oxytocicsshould be available at allfacilities and relevant healthstaff should be effectivelytrained to administer themby injection as a first aidmeasure for postpartumhaemorrhage
Health workers of anappropriate level areeffectively trained in clinicalskills to manage ante andpost partum haemorrhage
Intravenous fluids areavailable at all facilities andblood transfusion servicesshould be available atcomprehensive essentialobstetric care facilities on a24 hour basis
The partograph is usedeffectively to assess progressof labour where staff withappropriate skills are available
Standard
‘sufficient’‘all’‘relevant’‘effectively trained’
‘appropriate level’‘effectively’
‘all available’’24 hour’
‘effectively’‘appropriate’
Suggested basis for indicators
•Number of units of oxytocics in store within expiry date•Number and timing of specialist training courses inadministration of oxytocics per individual staff post in past twoyears/five years•Percentage of deliveries in which oxytocics were administered•Refrigerator working and system for dealing with power cuts inplace•Case fatality rate for haemorrhage over time
•Number and timing of staff training courses dedicated tomanagement of haemorrhage per individual staff post in pasttwo/five years•Recall by staff of key procedures•Evidence of major haemorrhage protocol in the unit•Case fatality rate for haemorrhage over time
•Number of units of intravenous fluids in store within expiry date•Availability of blood supplies (by time of day, type, cost, distance) •Availability of staff trained to administer blood transfusion (bytime of day)
•Number of labours whose progress was assessed by partograph•Number of staff trained to use partograph•Number of labours assessed by partograph as prolonged bysubsequent interventions
Source
Facility Records Provider InterviewsLabour NotesObservation
Facility Records Provider InterviewsLabour NotesObservation
Facility Records Provider InterviewsObservation
Facility Records Labour NotesProvider InterviewsObservation
58
Criteria
For a non complicateddelivery women are alwaysallowed to adopt whateverposition they choose fordelivery.
Women are always allowedsocial support of her choiceduring labour and birth.
Throughout labour awoman’s physical well beingshould be regularly assessed.
Standard
‘always’
‘always’
‘regularly’
Suggested basis for indicators
•Normal practice as reported by staff•Evidence of actual delivery positions (percentage delivered insupine position, percentage standing, squatting, other)•Percentage of women reporting choosing of delivery position ofher choice
•Facility guidelines•Normal practice as reported by staff•Percentage of women who report being accompanied in labourand delivery by person of her choice•Observed practice
•Number and timing of blood pressure measures•Number and timing of temperature and pulse measurements•Quantity of fluid intake vs urine output noted
Source
Provider InterviewsExit InterviewsSurvey
Facility GuidelinesObservationStaff InterviewsExit InterviewsSurvey
Labour NotesProvider InterviewsExit InterviewsObservationSurvey
Table 5: Indicators of Good Practice - continued

6160
Criteria
The appropriate range ofservices required to manageprolonged or obstructedlabour are available atreasonable hours at eachstage of the referral chain
All birth attendants areaware of the requirementsfor a clean delivery andfollow them effectively.
Health staff are effectivelytrained to recognisepuerperal sepsis and manageit appropriately or refer.
All facilities should be able toprovide the necessarytreatment for puerperal sepsis
Standard
‘appropriate’‘available’‘reasonable’
‘all’‘aware’‘effectively’
‘effectively trained’‘appropriately’
‘All’‘necessary’
Suggested basis for indicators
•Evidence that first level health centres have facilities and trainedstaff to: empty bladders; give antibiotics; rehydrate and refer women•Evidence that second level health centres have facilities andtrained staff to rupture membranes if required and perform avacuum extractor delivery•Evidence that CEOC hospitals have trained staff, essential drugsand equipment to perform additional interventions, such asoxytocics, antibiotic and the capacity to perform Caesareansection on a 24-hour basis•Percentage of women referred from first level health centrewho go on to have instrumental delivery or caesarean section•Case fatality rates for obstructed labour over time•Perinatal death rates attributed to birth asphyxia over time
•Observance of asepsis at all times•Hands always cleaned before and after any contact with woman•Delivery surface sterilisation procedure•Sterilisation procedure for instruments
•Percentage of staff who have attended specialist training inpuerperal sepsis•Percentage of staff who can accurately describe the signs,symptoms and treatment of puerperal sepsis•Case fatality rate for puerperal sepsis
•Availability of thermometers and antibiotics per facility
Source
Facility Records Case NotesExit InterviewsProvider InterviewsObservation
Facility Records Provider InterviewsExit InterviewsObservation
Facility Records Provider InterviewsObservation
Facility Records Provider InterviewsObservation
Criteria
Health staff are effectivelytrained to manage and torefer women with pregnancyinduced hypertension
The full range of servicesrequired to manage severepreeclampsia and eclampsia isavailable at CEOC facilities.
Health workers are effectivelytrained in the early recognitionand treatment of abortion-related complications
Evacuation of the uterinecontents, antibiotic therapy andintravenous fluids are available atall facilities and surgicaltreatments at all CEOC hospitals
Treatment is always followedby appropriate counsellingand contraceptioninformation and services
Standards
‘effectively trained’
‘full range required tomanage’
‘effectively trained’
‘available at allfacilites’‘all’
‘always appropriate’
Suggested basis for indicators
•Percentage of staff who have attended specific training inrecognition and management of pregnancy induced hypertensionwithin past two or five years•Percentage of staff able to accurately recount signs, symptomsand course of action•Case fatality rate for pre-eclampsia and eclampsia
•Sphygmomanometers, stethoscopes and urine testing reagentsreadily available•Magnesium sulphate, intravenous and oral anti-hypertensiveagents available in store within expiry date•Capacity to undertake emergency Caesarean section (availabilityof staff and equipment)
•Access to laboratory services for haematology and biochemistry
•Percentage of staff who have attended specific training inrecognition and treatment of abortion-related complicationswithin past two/five years•Percentage of staff who can recount signs and symptoms ofabortion-related complications and appropriate course of action•Availability of antibiotic therapy, intravenous fluids and skills andequipment to evacuate uterine contents
•Percentage of women who received counselling after anabortion•Percentage of women who received contraceptive informationand services after an abortion•Percentage of staff trained in counselling
Source
Facility Records Provider InterviewsObservationLabour Notes
Facility Records Provider InterviewsObservation
Facility Records Provider InterviewsObservation
Facility Records Provider InterviewsObservation
Facility Records Provider InterviewsExit InterviewsObservationSurvey
Table 6: Management of Emergencies - continued

6362
Table 8: CognitionCriteria
Necessary information isconveyed effectively in alanguage that isunderstandable to all women.
All women are fully preparedfor treatment andunderstand their options.Where possible theyexperience real informedchoice
The reasons for a specificintervention or outcome arealways clearly explained to allwomen
Information about post-partum care effectivelyconveyed.
Standard
‘necessary’‘effectively’‘understandable toall’
‘fully prepared’‘where possible’‘real informed choice’
‘always’‘clearly’‘all’
‘effectively’
Suggested basis for indicators
•Percentage of women who had full medical and birth history taken•Percentage of women who are explained and understand a diagnosis•Percentage of staff speaking local dialects•Percentage of women able to give accurate information aboutcontraindications or side effects of certain interventions or procedures•Percentage of women who report that their questions wereanswered in a language they were able to understand
•Percentage of women who knew they were going to have anepisiotomy before the procedure was carried out•Percentage of women who have had a Caesarean section andwho report being having the reason for their operation explainedand what the operation would involve•Percentage of women who report delivering in a position of her choice•Percentage of women who report the presence of at least onebirth supporter of her choice
•Percentage of women who are able to explain why they had aspecific procedure or intervention •Percentage of women who report having been explainedreasons for a poor outcome•Percentage of women who understand probable reason forpoor outcome
•Percentage of women complying with treatment and returningfor post natal appointments•Percentage of women who know how to care for perinealwounds correctly•Percentage of women at time of discharge who can namesymptoms that may indicate a post-natal complication
Source
ObservationExit InterviewsFacility RecordsCase NotesSurvey
Exit InterviewsObservationFocus GroupsIn-depth interviewsSurvey
Exit InterviewsProvider InterviewsObservationIn-depth InterviewSurvey
Facility RecordsExit InterviewsSurvey
Table 7: Human and Physical Resources (Experience of care)Criteria
The physical infrastructureand the overall environmentof the maternity wards areacceptable to all or mostwomen.
Contact time with qualifiedstaff is sufficient.
Male/female staff ratios areacceptable to most women.
Staff are competent toprovide appropriate care
Standard
‘acceptable to all ormost’
‘qualified’‘sufficient’
‘acceptable’‘most’
‘competent’
Suggested basis for indicators
•Percentage of women who report they are satisfied with thestate of infrastructure and wards (buildings, bed, sheets)•Percentage of women who perceive toilets and washing facilitiesto be accessible and clean•Perceived quality and acceptability of food and drink•Reported reliability of running water and electricity
•Percentage of women who report contact time with staff assufficient (per contact)•Percentage of women reporting being alone at a time when itworried her to be alone•Percentage of specific procedures reported as being carried outby grade of staff•Average number of staff of all grades per delivery and percomplication
•Percentage of female doctors•Percentage of women reporting feeling embarrassed, shy oruncomfortable with staff of opposite sex
•Level of staff knowledge about a specific diseases andcomplications and their appropriate treatment•Effective supervision•Qualifications and experience of staff as per responsibilities•Performance review, training and staff development in place•Training record
Source
Exit InterviewsFocus GroupsIn-depth InterviewSurvey
Facility Records ObservationExit InterviewsCase NotesFocus GroupsIn-depth InterviewsSurvey
Facility RecordsExit InterviewsFocus GroupsIn-depth InterviewCommunity Survey
Facility RecordsProvider InterviewsObservationCase NotesExit Interviews

6564
Table 10: Emotional SupportCriteria
Except in exceptionalcircumstances women areable to choose freely thesocial support they receive inlabour and at delivery
All women are treated withhonesty, kindness andunderstanding.
In the event of a death ordisability appropriate levels ofprofessional and emotionalcare are made available towomen and their families.
All staff are aware of theirsupportive role in theprovision of care duringlabour, delivery andimmediate post-partum period
An effective process exists inall units through whichproviders are able to identifyand respond to userexpectations
Standard
‘exceptionalcircumstances’‘freely’
‘all’‘honesty, kindness,understanding’
‘appropriate levels’
‘all’
‘effective’
Suggested basis for indicators
•Percentage of women reporting companionship of her choice inlabour and delivery•Hospital policy on social support in labour•Observed practice
•% of women reporting unauthorised payments to staff for services•% of women reporting being satisfied with interpersonal care•Document examples of poor interpersonal care reported bywomen/families
•Percentage of staff trained in bereavement counselling•Percentage of women satisfied with post-natal care in event ofdeath or disability•Percentage of women and their families who feel that theyunderstand the reasons for a death or disability before dischargecompared with recorded causes of death
•Percentage of staff who include supportive role in description ofresponsibilities•Percentage of women who describe examples of supportivebehaviour of staff during labour, delivery and immediate post-partum period
•Number and grade of staff responsible for investigating users-views•Examples of changes made following process to obtain usersviews•Evidence of a complaints procedure (theoretical vs observed)
Source
Facility Records Exit InterviewsProvider InterviewObservationSurvey
Exit interviewsObservationFocus GroupsIn-depth interviewsSurvey
Facility RecordsCase NotesExit InterviewsProvider InterviewsObservationSurvey
Facility RecordsProvider InterviewsExit InterviewsIn-depth interviews
Facility RecordsProvider InterviewsObservation In-depth Interviews
Table 9: Respect, Dignity and EquityCriteria
All facilities have an individualresponsible for assessing socio-economic and cultural context ofthe catchment area and an effectivemechanism for feeding relevantrecommendations to providers
All women feel they havebeen treated withappropriate respect
Women do not have toundergo any unnecessaryand humiliating procedures
Cultural practices that do notinterfere with high qualitycare are respected.
All women are treated withthe same standard of careregardless of education, class,caste, age etc
Services are appropriatelypriced for the catchment
Standard
‘all’‘effective mechanism’‘relevant’
‘appropriate’
‘do not’
‘do not’‘respected’
‘all’‘same standard’
‘appropriately’
Suggested basis for indicators
•Appointment of staff member responsible for research•Evidence of remit, resources and methods of staff responsible•Evidence of change in practice following recommendations (eg.examples of this)
•Percentage of women who report respectful or notdisrespectful treatment•Nature of observed interactions
•Percentage of women undergoing unnecessary procedures•Percentage of women who report undergoing procedures thatthey felt were uncomfortable and/or humiliating)
•Reported use or non use of practices identified as culturallyoffensive to women and their families or practices that theywould have wanted to happen and were denied
•Comparison of responses to other quality indicators by socio-economic/religious/caste status
•Cost of specific services as a percentage of monthly income•% of women reporting financial constraints as limiting access toservices
Source
Facility RecordsProvider InterviewsObservation
Exit InterviewsObservationFocus Groups
Case NotesExit InterviewsObservationFocus GroupIn-depth InterviewsSurvey
ObservationExit InterviewsFocus GroupsIn-depth Interviews
Case NotesExit InterviewsSurvey
Exit interviewsSurveyFocus GroupsIn-depth Interviews

67
American College of Obstetricians andGynecologists (1998),ACOG CommitteeOpinion: Cultural competency in health care,Committee on Health Care for UnderservedWomen, International Journal of Gynecology andObstetrics 62, pp. 96-99.
Amooti-Kaguna, B. and Nuwaha, F. (2000),Factors influencing choice of delivery sites inRakai district of Uganda, Social Science andMedicine 50, 1, pp. 203-213.
Adeyi, O. and Morrow, R. (1997), Essentialobstetric care:Assessment and determinants ofquality, Social Science and Medicine 45, 11, pp.1631-1639.
Aitken, I. and Reichenbach, L. (1994),Reproductive and sexual health services:Expanding access and enhancing quality, in Chen,L.C. (ed) Population Policies Reconsidered,Harvard University Press, Boston, pp. 177-192.
Atkinson, C. and Hayden, J. (1992), Managingchange in primary care: Strategies for success,British Medical Journal 304, pp. 1488-1490.
Benbow,A., Semple, D. and Maresh, M. (1997),Effective procedures in maternity care suitable foraudit, Clinical Audit Unit, Royal College ofObstetricians and Gynaecologists, London.
Bertrand, J.T., Hardee, K., Magnani, R.J. and Angle,M.A. (1995),Access, quality of care and medicalbarriers in family planning programs, InternationalFamily Planning Perspectives 21, 2, pp. 64-69.
Bidgood, K.A. and Steer, P.J. (1987),A randomisedcontrolled study of oxytocin augmentation oflabour, British Journal of Obstetrics andGynaecology 94, pp. 512-517.
Bhardwaj, N., Kukade, J.A., Patil, S. and Bhardwaj, S.(1995), Randomized controlled trial on modifiedsquatting position of delivery, Indian Journal ofMaternal and Child Health 6, 2, pp. 33-39.
Bruce, J. (1990), Fundamental elements of thequality of care: A simple framework, Studies inFamily Planning, 21, pp. 61-91.
Butani, P. and Hodnett, E. (1980), Mother’sperceptions of their labour experiences,Maternal Nursing Journal 9, pp. 73-82.
Calnan, M (1988) Lay evaluation of medicineand medical practice: Report of a pilot study,International Journal of Health Services 18, 2, pp.311-322.
Campero, L., Garcia, C., Diaz, C., Ortiz, O.,Reynoso, S. and Langer, A. (1998), "Alone Iwouldn’t have known what to do": Aqualitative study on social support duringlabour and delivery in Mexico, Social Scienceand Medicine 47, 3, pp. 395-403.
Campbell, O., Koblinsky, M. and Taylor,P. (1995),Off to a rapid start: Appraising maternalmortality and services, International Journal ofGynecology and Obstetrics, 48, Supplement, pp.S33-S52.
Carroli, G., Belizan, J. and Stamp,J. (1997)Episiotomy policies for vaginal birth, inNeilson, J.P., Crowther, C.A., Hodnett, E.D.,Hofmeyr, G.J. and Keirse, M.J. (eds) Pregnancyand Childbirth Module of the CochraneDatabase of Systematic Reviews, UpdateSoftware,The Cochrane Collaboration,Oxford.
Chacahm, A.S. and Perpetuo, I.H.O. (1998),Theincidence of Caesarean deliveries in BeloHorizonte, Brazil: Social and economicdeterminants, Reproductive Health Matters 6,pp. 115-121.
Cleaves, P. (1980), Implementation amidstscarcity and apathy: Political power and policydesign, in Grindle, M. (ed) Politics and PolicyImplementation in the Third World, PrincetonUniversity Press, New Jersey.
Bibliography
66

Greco, P.J. and Eisenberg, J.M. (1993) Changingphysicians’ practices, New England Journal ofMedicine. 329, pp. 1271-73.
Haddad, S. and Fournier, P. (1995), Quality, costand utilisation of services in developingcountries. A longitudinal study in Zaire, SocialScience and Medicine 40, 6, pp. 743-753.
Haddad, S., Fournier, P., Machouf, N. and Yatara,F. (1998),What does quality mean to laypeople? Community perceptions of primaryhealth care services in Guinea, Social Scienceand Medicine 47, 3, pp. 381-394.
Hillan, E. (1990), Research and audit:Women’sviews of caesarean sections, in Roberts, H.(ed), Women’s Health Matters, Routledge Press,London, pp. 157-175.
Hemminki, E. and Saarikoski, S. (1983),Ambulation and delayed amniotomy in thefirst stage of labour, European Journal ofObstetrics, Gynaecology and Reproductive Biology15, pp. 129-139.
Hemminki, E., Lenck, M., Saarikoski, S. andHenriksson, L. (1985), Ambulation versusoxytocin in protracted labour: A pilot study,European Journal of Obstetrics, Gynaecology andReproductive Biology 20, pp. 199-208.
Hemminki, E.,Virta, A.L., Kopnen, P., Malin, M.,Kojo-Austin, H. and Tuimala, R. (1990), A trialon continuous human support during labour:Feasibility, interventions and motherssatisfaction, Journal of Psychosomatic Obstetricsand Gynaecology 11, pp. 239-250.
Hodnett, E.D. and Osborn, R.W. (1989a), Arandomized trial of the effect of montricesupport during labour: Mothers’ views two tofour weeks postpartum, Birth 16, pp. 177-183.
Hodnett, E.D. and Osborn, R.W. (1989b),Effects of intra-partum professional supporton childbirth outcomes, Research on Nursingand Health 12, pp. 289-297.
Hofmeyr, G.J., Nikodem,V.C.,Wolman,W.L.,Chalmers, B.E. and Kramer,T. (1991),Companionship to modify the clinical birthenvironment: Effects on progress andperceptions of labour and breastfeeding,British Journal of Obstetrics and Gynaecology 98,pp. 756-764.
Huque, Z. A., Mavalankar, D., Akhter, H.H. andChowdhury,T.A. (1999), Safe motherhoodprogrammes in Bangladesh, in ,Berer, M.andSundari Ravindran,T.K. (eds), Safe MotherhoodInitiatives: Critical Issues, Reproductive HealthMatters, Blackwell Science.
Institute of Medicine (1990), Medicare – Astrategy for quality assurance,Volume I, NationalAcademy Press,Washington, D.C.
Iyun, F. (1983), Hospital service areas in Ibadancity, Social Science and Medicine 17, pp. 601-610.
Jacobson, J. L. (1991),Women’s reproductivehealth:The silent emergency, Worldwatch Paper102,The Worldwatch Institute,WashingtonD.C.
Johansen, K.S. and Hod, M. (1999), Qualitydevelopment in perinatal care – the OBSQIDproject: Special Communication, InternationalJournal of Gynaecology and Obstetrics 64, pp.167-172.
Johanson, R.B. (1995),Vacuum extractionversus forceps delivery, in Enkin, M.W, Keirse,M.J, Renfrew, M.J. and Neilson, J.P. (eds)Pregnancy and Childbirth Module of theCochrane Database of Systematic Reviews,Update Software,The CochraneCollaboration, Oxford.
Johnston, R.A. and Sidall, R.S. (1922), Is theusual method of preparing patients fordelivery beneficial or necessary?, AmericanJournal of Obstetrics and Gynecology 4, pp. 645-650.
Kane,T.T., El-Kadi,A.A., Saleh, S., Aje, M., Stanback,J. and Potter, L. (1992), Maternal mortality inGiza, Egypt: Magnitude, causes and prevention,Studies in Family Planning, 23, pp. 45-57.
69
Cohen, G.R., O’Brian,W.F., Lewis, L. andKnuppel, R.A. (1987), A prospectiverandomized study of the aggressivemanagement of early labor, American Journal ofObstetrics and Gynecology, 157, pp. 1174-1177.
Crawford, J.S. (1956), Some aspects ofobstetric anaesthesia, British Journal ofAnaesthesia 28, pp. 146-208.
Crowley, P., Elbourne, D.R., Ashhurst, H., Garcia,J., Murphy, D. and Duinan, N. (1991), Deliveryin an obstetric birth chair : A randomizedcontrolled trial, British Journal of Obstetrics andGynaecology 98, pp. 667-674.
Crowther, C. (1985), Eclampsia at Hararematernity hospital: An epidemiological study,South African Medical Journal, 68, pp. 927-929.
Danquah, J.B., Appah, E.K., Djan, J.O., Ofori, M.,Essegbey, I.T. and Opoku, S. (1997), Improvingrecordkeeping for maternal mortalityprograms, Kumasi, Ghana, International Journalof Gynecology and Obstetrics 59, Supplement 2,pp. S149-S155.
Demographic and Health Survey (1996),Brazil, Macro International, Maryland.
De Geyndt,W. (1995), Managing the Quality ofHealth Care in Developing Countries,WorldBank Technical Paper 258,The World Bank,Washington D.C.
Dixon-Mueller, R. (1993),The sexualityconnection in reproductive health, Studies inFamily Planning 24, 5, pp. 269-282.
Donabedian, A. (1966), Evaluating the qualityof medical care, Millbank Memorial FundQuarterly 44, pp. 166-203.
Donabedian, A. (1988),The quality of care:How can it be assessed? The Journal of theAmerican Medical Association 260, 12, pp. 1743-1748.
Drayton, S. and Rees, C. (1984),They knowwhat they are doing: Do nurses know whythey give pregnant women enemas?, NursingMirror 5, pp. 4-8.
Driessen, F. (1987), Labour ward management,Tropical Doctor 17, pp. 174-178.
Drife, J.O. (1996), Choice and instrumentaldelivery, British Journal of Obstetrics andGynaecology 103, pp. 608-611.
Ellis, R. and Whittington, R.E.D. (1993), Qualityassurance in health care, in Whittington, R.E.D.(ed) Quality Assurance Handbook, EdwardArnold, London, pp. 1-8.
Enkin, M., Keirse, M.J., Renfrew, M. and Neilson, J.(eds) (1995), A Guide to Effective Care inPregnancy and Childbirth, 2nd Edition, OxfordUniversity Press, Oxford.
Fawcus, S., Mbizvo, M., Lindmark, G. andNyström (1996), A community-basedinvestigation of avoidable factors for maternalmortality in Zimbabwe, Studies in FamilyPlanning 27, 6, pp. 319-327.
Finerman, R.D. (1983), Experience andexpectation: Conflict and change in traditionalfamily health care among the Quichua ofSaraguro, Social Science and Medicine 17, pp.1291-1299.
Flamm, B.L., Lim, O.W., Jones, C., Fallon, D.,Newman, L.A. and Mantis, J.K. (1988),Vaginalbirth after cesarean section: Results of amulticenter study, American Journal of Obstetricsand Gynecology 158, pp. 1079-1084.
Geefhuysen, C.J. (1999), Safe motherhood inIndonesia: A task for the next century, in Berer,M and Sundari Ravindran,T.K. Safe MotherhoodInitiatives: Critical Issues, Reproductive HealthMatters, Blackwell Science Ltd.
Germain, A. and Ordway, J. (1989), PopulationControl and Women’s Health: Balancing theScales, International Women’s Health Coalition,New York.
Glazener, C.M.A., Abdalla, M. and Stroud, E.(1995), Postnatal maternal morbidity: Extent,causes, prevention and treatment, BritishJournal of Obstetrics and Gynaecology 102, pp.282-287.
68

Lucas, A., Adrian,T.E., Aynsley-Green, A. andBloom, S.R. (1980), Iatrogenic hyperinsulinismat birth, Lancet 1, pp. 144-145.
Maine, D., Murat, Z., Akalin,V. and Ward, A.(1997) The Design and Evaluation of MaternalMortality Programs, Centre for Population andFamily Health, School of Public HealthColombia University.
Mancey-Jones, M. and Brugha, R.F. (1997),Using perinatal audit to promote change: Areview, Health Policy and Planning 12, 3, pp.183-192.
Matthews, Z., Stones, R.W., Ramasubban, R.,Singh, B. and Hulton, L.A. , Maternal Health-care Seeking among the Urban Poor:Morbidity, Access and Uptake in the IndianContext, Study funded by the Wellcome Trust,report forthcoming.
Matthews, Z., Ganapathy, S., Ramakrishnan, J.,Kilaru, A. and Mahendra, S. (1999), Birth-rightsand rituals in rural Karnataka: Care seeking inthe intra-partum period, Department of SocialStatistics Working Paper No. 99-14, Universityof Southampton, UK.
McKay, S. and Mohan, C. (1988), Modifying thestomach contents of labouring women:Why,how, with what success, and at what risks?How can aspiration of vomitus in obstetricsbest be prevented?, Birth 15, 4, pp. 213-221.
Mensch, B. (1993), Quality of care: A neglecteddimension, in Koblinsky, M.Timyan, J. and Gay, J.(eds) The Health of Women: A GlobalPerspective,Westview Press, Oxford.
Mernissi, F. (1975), Obstacles to family planningpractice in urban Morocco, Studies in FamilyPlanning 6, 12, pp. 418-425.
Misra, B.D., Ashraf, A., Simmons, R. andSimmons, G. (1982), Organisation for Change –Systems Analysis of Family Planning in RuralIndia,The University of Michigan Center forSouth and Southeast Asian Studies, Ann Arbor.
Mitchell, M.W. and Fowkes, F.G.R. (1985), Auditreviewed: Does feedback of performancechange clinical behaviour?, Journal of the RoyalCollege of Physicians of London 19, pp 251-53.
Mooney, G. and Ryan, M. (1992), Rethinkingmedical audit:The goal is efficiency, Journal ofEpidemiology and Community Medicine 46, pp.180-183.
Mungford, M., Kingston, J. and Chalmers, I.(1989), Reducing the incidence of infectionafter Caesarean section: Implications ofprophylaxis with antibiotics for hospitalresources, British Medical Journal 299, pp. 1003-1006.
Mwabu, G. M. (1986), Health-care decisions atthe household level: Results of a rural healthsurvey in Kenya, Social Science and Medicine 2,pp. 315-319.
Nichter, M. (1989), Modern methods offertility regulation:When and for whom arethey appropriate?, in Nichter, M. (ed)Anthropology and International Health, KluwerAcademic Publishers, Dordrecht, pp. 57-83.
Nikodem,V. (1995), Upright versus recumbentposition during the first and second stages oflabour, in Enkin, M.W., Keirse, M.J., Renfrew, M.J.,and Neilson, J.P. (eds), Pregnancy and ChildbirthModule of the Cochrane Database of SystematicReviews, Update Software,The CochraneCollaboration, Oxford.
Okafor, C.B. and Rizzuto, R.R. (1994),Women’sand health-care providers’ views of maternalpractices in rural Nigeria, Studies in FamilyPlanning 25, 6, pp. 353-361.
Okonofua, F.E., Abejide, A. and Makanjuola, R.A.(1992), Ile-Ife, Nigeria: A study of risk factors,Studies in Family Planning 25, 5, pp. 279-291.
Palmer, R.H. (1991), Considerations in definingquality of care, Striving for Quality in Health Care:An Inquiry into Policy and Practice, HealthAdministration Press, Ann Arbor, pp. 1-59.
71
Kantor, H.I., Rember, R.,Tabio, P. and Buchanon,R. (1965),Value of shaving the pudendal-perineal area in delivery preparation, Obstetricsand Gynecology 25, pp. 509-512.
Keirse, M.J. and Enkin, M. (1989), Social andprofessional support during labour, inChalmers E.R. (ed) Effective Care in Pregnancyand Childbirth, Oxford Medical Publications,Oxford, pp. 805-819.
Kelleher, C.J. and Cardozo, L.D. (1994),Caesarean section: A safe operation? BritishJournal of Obstetrics and Gynaecology, 14, pp.86-90.
Kennell, J.H. and Klaus, M. (1991), Continuousemotional support during labour in a U.S.hospital. A randomised controlled trial, Journalof the American Medical Association 265, pp.2197-2201.
Kitzinger, S. (1990), Birth and violence againstwomen: Generating hypotheses form women’saccounts of unhappiness after childbirth, inRoberts, H. (ed) Women’s Health Matters,Routledge, London, pp. 63-80.
Klaus, M.H., Kennell, J.H., Robertson, S.S. andSosa, R. (1986), Effects of social support duringparturition on maternal and infant morbidity,British Medical Journal 293, pp. 585-587.
Klaus, M. H. and Kennell, J.H. (1992), Maternalassistance and support in labor: Father, nurse,midwife or doula?, Clinical Consultations inObstetrics and Gynaecology 4, pp. 211-217.
Koblinsky, M., McLaurin, K., Russell-Brown, P.and Gorbach, P (eds) (1995), Indicators forreproductive health programme evaluation:Final report of the subcommitttee on safepregnancy, The Evaluation Project, CarolinaPopulation Centre, Chapel Hill.
Konrad, C. (1987), Helping mothers integratethe birth experience, MCN 12, pp. 268-69.
Kwast, B.E. (1991), Postpartum haemorrhage;Its contribution to maternal mortality,Midwifery 7, pp. 64-70
Lasker, J.N. (1981), Choosing among therapies:Illness behaviour on the Ivory Coast, SocialScience and Medicine 25, pp. 1003-1011.
Lawrence, G.F., Brown,V.A., Parsons, R.J. andCooke, I.D. (1982), Feto-maternalconsequences of high-dose glucose infusionduring labour, British Journal of Obstetrics andGynaecology 89, pp. 27-32.
Leslie, J. and Gupta, G.R. (1989), Utilisation ofFormal Services for Maternal Nutrition andHeath Care in the Third World, InternationalCenter for Research on Women,WashingtonD.C.
Liddell, H.S. and Fisher, P.R. (1985),The birthingchair in the second stage of labour, Australianand New Zealand Journal of Obstetrics andGynaecology 25, pp. 65-68.
Lipsky, M. (1981), Advocacy and alienation instreet-level work, in C.T.Goodsell (ed) ThePublic Encounter, Indiana University Press,Bloomington, pp. 69-80.
Lohr, K.N., Donaldson, M.S. and Walker, A J.(1991), Medicare, a strategy for qualityassurance III: Beneficiary and physician focusgroups, Quality Review Bulletin 17, pp. 242-253.
Lomas, J., Enkin, M. and Anderson, G.M. (1991),Opinion leaders versus audit and feedback toimplement practice guidelines, Journal of theAmerican Medical Association 265, 17, pp. 2202-2207.
Lopez-Zeno, J.A., Peaceman, A.M., Adashek, J.A.and Socol, M.L. (1992), A controlled trial of aprogramme for the active management oflabor, New England Journal of Medicine 326, pp.450-454.
Lubis, F., Frajans, P., Sulistomo, A., Indrawati, S.and Simmons, R. (1992), Service DeliveryImplications of Introducing Cyclofem in Indonesia:Final Report of a Project Funded by the WHOTask Force on Research into the Introduction andTransfer of Technologies for Fertility Regulation,World Health Organization, Geneva.
70

Stock, R. (1983), Distance and the utilization ofhealth facilities in rural Nigeria, Social Scienceand Medicine 15, pp. 563-569.
Stocking, B. (1992), Promoting change inclinical care, Quality in Health Care, 1, pp. 56-60.
Sundari,T.K. (1992),The untold story: How thehealth care systems in developing countriescontribute to maternal mortality, InternationalJournal of Health Services 22, 3, pp. 513-528.
Sutton, J. and Scott, P. (1996), Understandingand teaching optimal fetal positioning, BirthConcepts, New Zealand.
Tarnow-Mardi,W.O., Shaw, J.C.L., Liu, D.,Gardener, D.A. and Flynn, F.V. (1981)Iatrogenic hyponataemia of the newborn dueto maternal fluid overload; A prospectivestudy, British Medical Journal 283, pp. 639-642.
Thaddeus, S. and Maine, D. (1994),Too far towalk: Maternal mortality in context, SocialScience and Medicine 38, 8 pp. 1091-1110.
The Eclampsia Trial Collaborative Group(1995),Which anticonvulsant for women witheclampsia? Evidence from the collaborativeeclampsia trial, The Lancet 345, pp. 1455-1463.
UNICEF/WHO/UNFPA (1997), Guidelines forMonitoring the Availability and Use ofObstetric Services, World Health Organization,Geneva.
Vera, H. (1993),The client’s view of high-quality care in Santiago, Chile, Studies in FamilyPlanning 24, 1, pp. 40-49.
Walt, G. (1994), Health policy: An Introductionto Process and Power, Zed Books, London.
Wedderburn, M. and Moore, M. (1990),Qualitative Assessment of Attitudes AffectingChildbirth Choices of Jamaican Women,MotherCare Project Working Paper 5.
World Health Organization (1992) The WHOInternational Classification of Diseases, 10thRevision,WHO, Geneva.
World Health Organization (1994a) ClinicalManagement of abortion complications: apractical guide,WHO, Geneva.
World Health Organization (1994), Motherand Baby Package: Implementing SafeMotherhood in Countries,WHO, Geneva.
World Health Organization (1996a), Revised1990 Estimates of Maternal Mortality: A NewApproach by WHO and UNICEF,WHO,Geneva.
World Health Organization (1996b), Care inNormal Birth: A Practical Guide,WHO,Geneva.
World Health Organization (1998), PostpartumCare of the Mother and Newborn: A PracticalGuide,WHO, Geneva.
73
Patel,T. (1991), Fertility Behaviour: Population andSociety in a Rajasthan Village, Oxford UniversityPress, Delhi.
Perpetuos, I.H. O., Bessa, G.H. and Fonseca, M.C.(1998), Caesarean delivery: An analysis ofwomen’s perspectives in Belo Horizonte, inAnais do XI Encontro de Estudos Populacionais,Associacao Brasiliera de Estudos Populacionais,Caxambu, pp. 95-120.
Read, J.A., Miller, F.C., Paul, R.H. (1981),Randomized trial of ambulation versus oxytocinfor labour enhancement: A preliminary report,American Journal of Obstetrics and Gynecology139, pp. 669-672.
Reerink, E., (1990), Defining quality of care:Mission impossible?, Quality Assurance of HealthCare, 2, 3/4, pp. 197-202.
Roberge, D., Loiselle, J.H., Mongrain, J. Lebel, P.Ducharme, F. and Pineault, R. (1996) Qualite desService Geriatriques: La Perspective des Clienteles,Paper presented at the 7eme ConferenceAnnuelle de l’Association Latine d’Analyse desSysteme de Sante, Geneva.
Roberts, R.B. and Shirley, M.A. (1976),Theobstetrician’s role in reducing the risk ofaspiration of pneumonitis with particularreference to the use of oral antacids, AmericanJournal of Obstetrics and Gynecology 124, pp.611-617.
Robinson, M.B. (1994), Evaluation of medicalaudit, Journal of Epidemiology and CommunityHealth 48, pp. 435-440.
Rohde, J.E. (1995), Removing risk from safemotherhood, International Journal of Gynecologyand Obstetrics 50, Supplement 2, pp. S3-S10.
Romney, M.L. and Gordon, H. (1981), Is yourenema really necessary? British Medical Journal282, pp. 1269-1271.
Ronsmans, C. (1999) Personal communication.
Rosen, G.M. and Dickinson, J.C. (1990),Vaginalbirth after Cesarean:A meta-analysis ofindicators for success, Obstetrics and Gynecology76, pp. 865-869.
Rosen, G.M., Dickinson, J.C. and Westhoff, C.L.(1991),Vaginal birth after Cesarean:A meta-analysis of morbidity and mortality, Obstetrics andGynecology 77, pp. 465-470.
Royal College of Obstetricians andGynaecologists (1996), Management ofEclampsia: Guideline No.10,The Royal College ofObstetricians and Gynaecologists, London.
Rutter, N., Spencer,A., Mann, N., Smith, M. (1980),Glucose during labour, The Lancet 2, pp. 155-156.
Scrimshaw, S. C. (1974), Modesty and familyplanning, People, 1, 2, International PlannedParenthood Federation, pp. 20-22.
Simkin, P. (1992),A day you’ll never forget, theday you gave birth to your first child, Birth, Issuesin Perinatal Care.
Simmons, R. and Elias, C. (1994),The study ofclient-provider interactions:A review ofmethodological issues, Studies in Family Planning25, 1, pp. 1-17.
Sleep, J., Grant,A.M., Garcia, J., Elbourne, D.R.,Spencer, J.A.D. and Chalmers, I. (1984),WestBerkshire perineal management trial, BritishMedical Journal 289, pp. 587-590.
Sleep, J. (1991), Perineal care:A series of fiverandomised controlled trials, in Robinson, S. andThomson,A. (eds) Midwives, Research andChildbirth,Volume 2, Chapman and Hall, London.
Sosa, R. and Kennell, J.H. (1980),The effect of asupportive companion on perinatal problems,length of labour, and mother-infant interaction,New England Journal of Medicine 303, pp. 597-600.
Stewart P., Hillan, E. and Calder,A.A. (1978),Upright position and the efficiency of labour, TheLancet 1, pp. 72-74.
Stewart, P. and Spiby, H. (1989), A randomisedstudy of the sitting position for delivery using anewly designed obstetric chair, British Journal ofObstetrics and Gynaecology, 96, pp. 327-333.
72

Louise A Hulton, Zoë Matthews andR William Stones can be contacted at:
Opportunities and ChoicesDepartment of Social StatisticsUniversity of SouthamptonHighfieldSouthampton SO17 1BJ
Telephone 023 8059 5763Fax 023 8059 3846Email [email protected]
Additional copies of this publication canalso be obtained at this address.
Please mark requests for additionalcopies for the attention of RosemaryLawrence.
74