A framework for psychopathology 1.Symptoms 2.Neural Causes (systems approach) –A. Which...
14
A framework for psychopathology 1. Symptoms 2. Neural Causes (systems approach) – A. Which neurotransmitters? – B. ‘Where’ in the brain? which methods measure it? – Other causes: Genetic, Social 3. Neural Treatment – A. Pharmacotherapy – B. Brain stimulation, lesion – Other (e.g., Cognitive behavioral therapy)
-
Upload
abigail-byrd -
Category
Documents
-
view
216 -
download
0
Transcript of A framework for psychopathology 1.Symptoms 2.Neural Causes (systems approach) –A. Which...

A framework for psychopathology
1. Symptoms
2. Neural Causes (systems approach)– A. Which neurotransmitters?– B. ‘Where’ in the brain? which methods measure it?– Other causes: Genetic, Social
3. Neural Treatment– A. Pharmacotherapy– B. Brain stimulation, lesion– Other (e.g., Cognitive behavioral therapy)

Psychopathology
Diseases with localized lesion• Fronto-temporal dementia (last class)• Orbitofrontal lesion (e.g, Traumatic brain injury)• Strokes & other lesions
– Lesion of medio-frontal structures: Akinetic mutism– Lesion of amygdala: impaired processing of fear
Diseases defined initially by their symptoms• Depression• Obsessive compulsive disorder• Huntington’s disease• Autism• Schizophrenia• ADHD• Anxiety

Depression: Symptoms Possible substrates
• Cognitive processes – Reduced concentration DLPFC– impaired memory hippocampus
• Emotion/motivation/self Mid frontal, OFC– Lack of energy– Loss of interest– Slowness of movement– Mood: Pessimism (depressive realism)
• Autonomic processes Ventral cingulate– Changes in Apetite insula– Reduced libido hypothalamus– Changes in Sleep pattern: (Shallow, Fragmented, Early REM onset)– Increased cortisol levels

Depression: Neural changes
• Change activity in– ventral frontal, – midfrontal, – dorsolateral prefrontal– amydgala

Depression: Treatment
• Cognitive behavior therapy• Pharmacotherapy
– SSRI, acts upon serotonin system– MAOi, – tricyclic antidepressants
• Electroconvulsive therapy• Repeated Transcranial Magnetic Stimulation• Deep Brain stimulation
• Sleep deprivation – Selective (REM)– Total (not feasible)

Relation between Depression and Stress
• Stress “activates” depression in susceptible individuals
• High levels of circulating cortisol in hospitalized depression cases and suicide victims

Dexamethasone suppresses waking ACTH release when given at night.

Relation between Depression & Sleep
• Complete loss of SWS• Increased REM – decreased latency to 1st REM• Decreasing REM -> improved functioning• MAOi suppress REM


Obsessive-Compulsive Disorder (OCD)
Symptoms• Recurrent behaviors (compulsive) • Recurrent thoughts (obsessive)• People repeat things until they feel that they have
“gotten it right”• Frequently related to cleanliness or territoriality
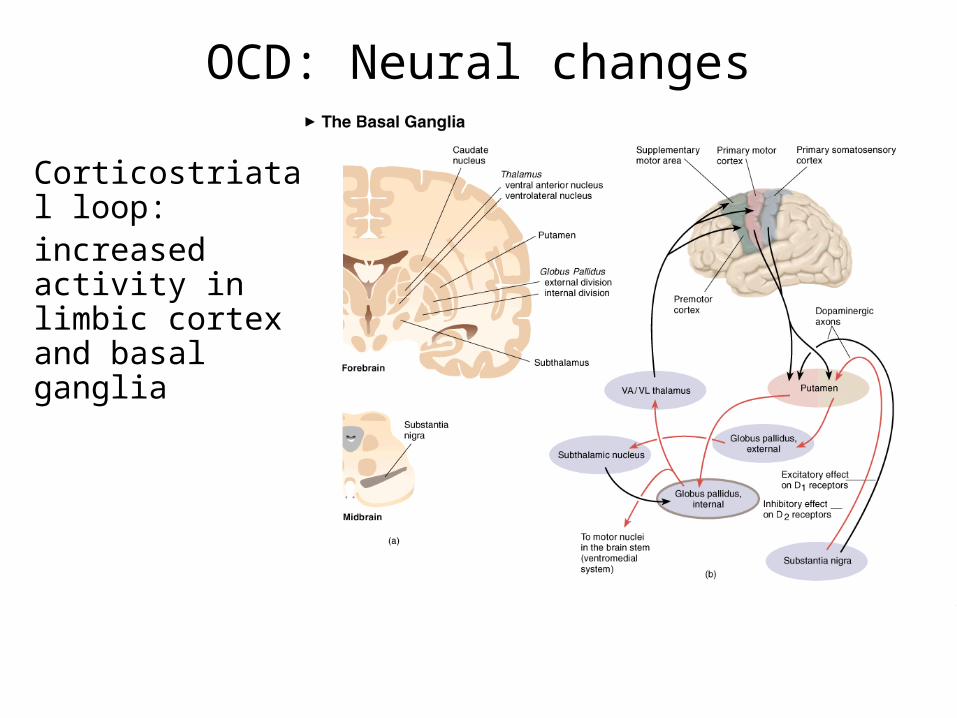
OCD: Neural changes
Corticostriatal loop:increased activity in limbic cortex and basal ganglia

OCD: Treatment
• Tricyclic antidepressants alleviate symptoms (particularly 5-HT)
• Brain lesion

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Tourette’s syndrome• Dysfunction of cortico-striatal loop • number of D2 receptors in basal ganglia is increased as revelead by PET• tics reduced by D2 antagonists (neuroleptics)
• abnormal cortico-striatal loop may explain aspects of repetitive behavior in OCD, FTD, autism
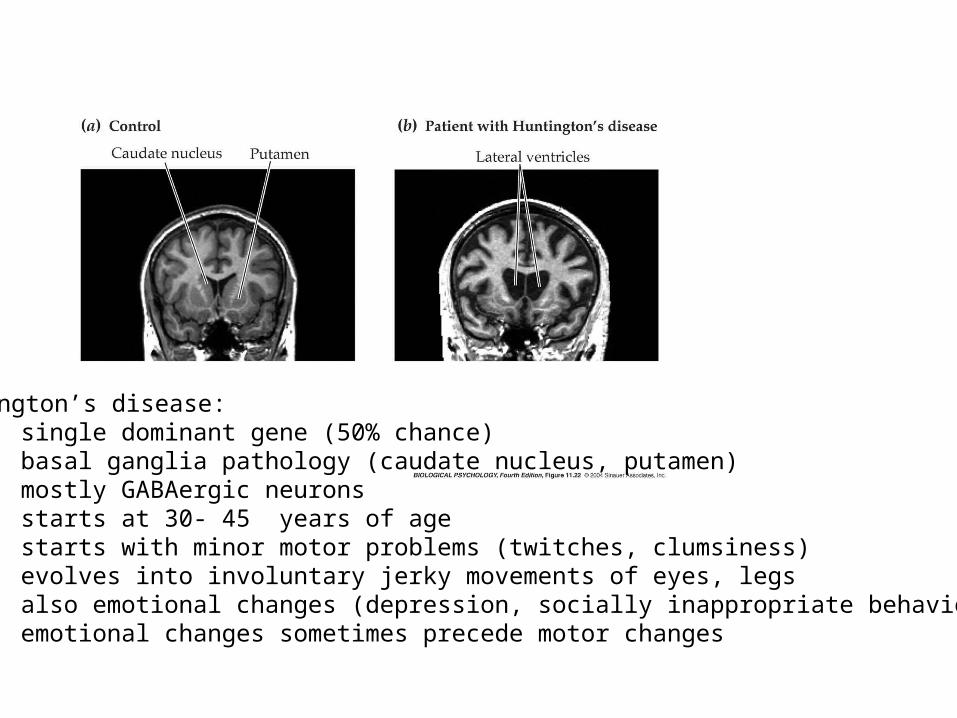
Huntington’s disease:single dominant gene (50% chance)basal ganglia pathology (caudate nucleus, putamen)mostly GABAergic neuronsstarts at 30- 45 years of agestarts with minor motor problems (twitches, clumsiness)evolves into involuntary jerky movements of eyes, legs also emotional changes (depression, socially inappropriate behavior)emotional changes sometimes precede motor changes