Disaster through a different lens. Behind every effect, there is a

A Different LensRetooling Parenting Strategies and Relationships for Children with FASD & Trauma
Presented by Jeanne Ketola MA LPCC

Overview
• FASD Basics
• Trauma Basics
• Definition
• Hot and Cold Systems
• Impact
• Steps to Retool Child /Parent Relationships
2©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.

3©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.

4©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.

Remember…
• All behavior has a purpose
• As humans we all need to feel:
• Safe
• Belong
• Significant
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 5

What is Fetal Alcohol Spectrum Disorder (FASD)?
• Permanent brain damage caused by prenatal exposure to alcohol
• It is a disability
Spectrum Range
High IQ’s and no facial
characteristics
IQ’s below 70 with facial and other physical
deformities
Approx. 80 % have average/above average IQ’s and no facial characteristics
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 6

FASD -Who does it affect?• World Health Organization (WHO) –world-wide
epidemic - 2017 Studies estimate 1out of 67 women who consume alcohol during pregnancy will deliver a child with FAS.
• Estimate higher rate than Down Syndrome.
• Found in every socioeconomic, race, ethnic group
• Minnesota - estimates 7041 children born each year who are prenatally exposed to alcohol (MOFAS)
• High rates in children in Foster Care – up to 75% (Study by Dr. Susan Astley – Washington State University 2002)
• Top Five Countries with Highest Rates: Ireland, Belarus, Denmark, United Kingdom (Great Britain & Northern Ireland), Russian Federation. (WHO 2017)
7©Pathway Consulting, LLC ©2018 These slides may not be reproduced or used without written permission.

• FASD is an umbrella term - not a diagnosis – term to describe four categories of criteria within the spectrum:
• FAS – Fetal Alcohol Syndrome (confirmed or unconfirmed exposure)
• PFAS – Partial Fetal Alcohol Syndrome (confirmed exposure)
• ARND – Alcohol Related Neurodevelopmental Disorder (Neurodevelopmental, cognitive or behavioral issues - confirmed)
• ARBD – Alcohol Related Birth Defects (Physical defects only-
confirmed)
FASD is a Spectrum
Approx. 80 % have average/above average IQ’s and no facial characteristics
8©Pathway Consulting, LLC 2015 These slides may not be reproduced or used without written permission.

Strengths
9©Pathway Consulting, LLC 2017 These slides may not be reproduced or used without written permission.
• Artistic, drawing, pottery, music, dancing
• Technology – figures out how things are put together or how they work
• Good readers
• Likeable
• Feel badly when they make a mistake
• Good with younger children & people with disabilities
• Love of animals
• Athletic, but may not excel in team sports
• Truth tellers
• Intelligent
• Desire to be helpful
• Good arguers
• Don’t hold grudges

Challenges for Children with FASD• Appear to break rules (generalizing, processing, memory ,
Lack of cause/effect thinking – difficulty seeing the consequences, outcomes)
• Surprised when they are in trouble (impulsivity, memory issues, lack of cause and effect)
• Inconsistent performance Forgets how – one day they are masters - next day act as if it is brand new (generalizing, working memory, impulsivity – self regulation)
10©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.

Challenges for Children with FASD
• Time /Money and Organizational Skills ( difficulty with thinking future, applying abstract concepts, due to deficits in executive functioning)
• Struggles with transitions (appear anxious /dysregulated in new situations or when routine is changed)
• Sleep issues – brain keeps running (sleep issues may also be caused by unhealed trauma and abuse)
• Social cueing Difficulty reading people - doesn’t get jokes or teasing (social cues – due to frontal lobe damage) affects school, employment, answering to authority.
• Vulnerable (often mimic others to fit in; may do anything for friendships and can be taken advantage of)
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 11

Viewed by others as……. • Non-compliant, lazy, doesn’t
care, lies
• Uncooperative, resistant, stubborn
• Mean, rude, mouthy, hostile
• Manipulative, demanding, unappreciative,
• Unmotivated, won’t try, won’t finish anything
• Oppositional, conduct problems (EBD)
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 12
“Act out because it is better to look tough or mean than to look dumb”

Complexities of FASDTypically layered with other issues:
• Sensory Integration
• Developmental Trauma
• Posttraumatic Stress Disorder (PTSD)
• Attachment issues including Reactive Attachment Disorder (RAD)
• Traumatic Brain Injury (TBI)
• Attention-Deficit Hyperactivity Disorder (ADHD)
• Multiple placements, foster care, adoption
• Physical and Sexual Abuse issues
• Medical Issues (seizure disorder, heart abnormalities, scoliosis, cleft palate, etc.)
• Learning disorders
13©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.

FASD – Possible Misdiagnoses
• ADHD
• Oppositional Defiant Disorder (ODD)
• Conduct Disorder
• Adolescent Depression
• Autism / Asperger’s
• Reactive Attachment Disorder (RAD)
• Traumatic Brain Injury (TBI)
• Antisocial Personality Disorder
• Borderline Personality Disorder
• Bipolar Disorder
• Bad Kid
14©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.
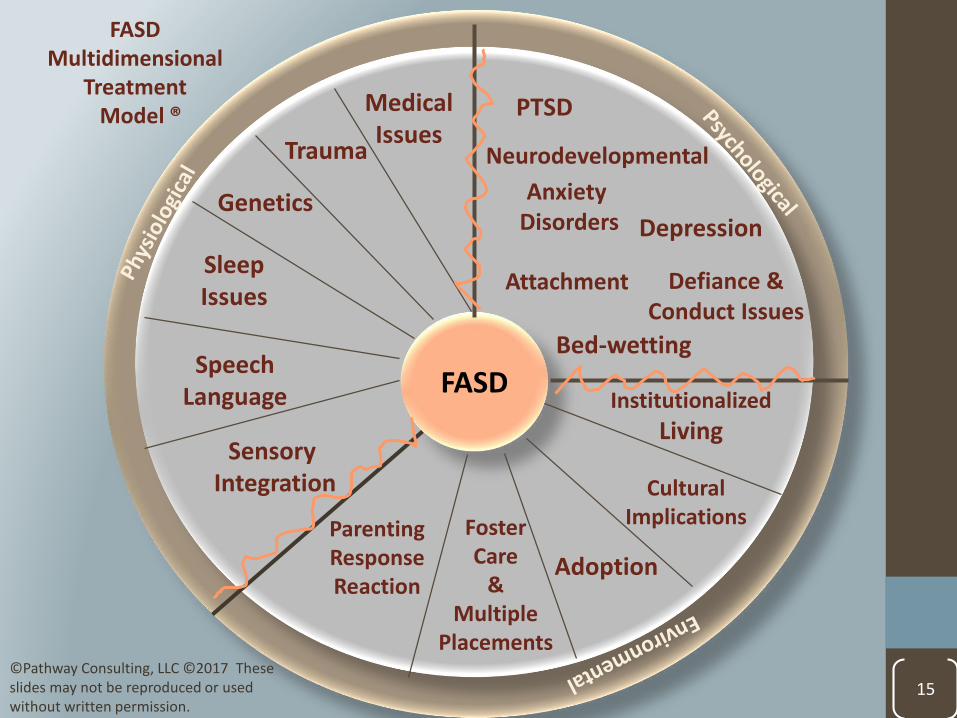
15
FASD
Trauma
Attachment
MedicalIssues
SleepIssues
SpeechLanguage
Sensory Integration
ParentingResponseReaction
Adoption
FosterCare
&Multiple
Placements
Institutionalized
Living
FASDMultidimensional
Treatment Model ®
Genetics
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.
CulturalImplications
Defiance &Conduct Issues
Depression
Anxiety Disorders
Bed-wetting
PTSD
Neurodevelopmental

16©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.
Developmental Gaps: What is the “acts like age?”
Trauma Basics

Definition of Trauma• Central Nervous System’s reaction to arousal in the body
Trauma resides as a body memory– all senses are affected
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 18

Events to Describe Trauma• Neglect/abandonment
• Physical / emotional abuse
• Sexual abuse by adults or children
• Witnessing domestic violence of a parent
• Accidents
• Witnessing an accident or horrific event
• Medical trauma at birth or after birth
• In-vitro exposure to alchol or other substances
• Poor nutrition and prenatal care –mother didn’t want baby, mother abused during pregnancy
• Traumatic delivery
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 19

ACE Study
• Adverse Childhood Experience (ACE - 2005)• Dr. Robert Anda• Extensive Study – also has been expanded internationally• The study supported the numerous effects of childhood adverse
experiences on behavioral and physical health
Example:Area studied: Memory storage retrieval (Hippocampus)Neurobiological Defect: Hippocampal & amygdala size reduction in childhood trauma; deficits in memory function
“There are good kids who can’t learn because of stressful or neglectful experiences, which has affected their brain development.” Dr. Anda
2010
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 20
Children who survive Trauma• Impulsive, hypervigilant, hyperactive, withdrawn or
depressed, have sleep difficulties (including insomnia, restless sleep and nightmares) and anxiety.
• Show a loss of previous functioning or a slower rate of acquiring new developmental tasks including language development.
• Act in a regressed fashion.
• Persistently show physiological hyper-reactivity with fast heart rates or borderline high blood pressure.
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 21
Trauma changes the brain!
Adapted from Bruce Perry

False Perception of TraumaDefinition is often blurred by a person’s own frame of reference and can be perceived as:
• Oh – you have a little nervousness or anxiety.
• Don’t worry. Children are resilient – they will get over it.
• Just breathe.
• Just tell yourself to stop thinking about it.
• They will be fine once they settle in.
• You just need to love them and they will be fine.
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 22

Balance System (ANS -Autonomic Nervous System)
• Autonomous – occurs involuntarily
• Regulates functions of the body (i.e. connects brain, spinal cord, organs and glands)
• Full capacity when system is balanced
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 23

©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 24
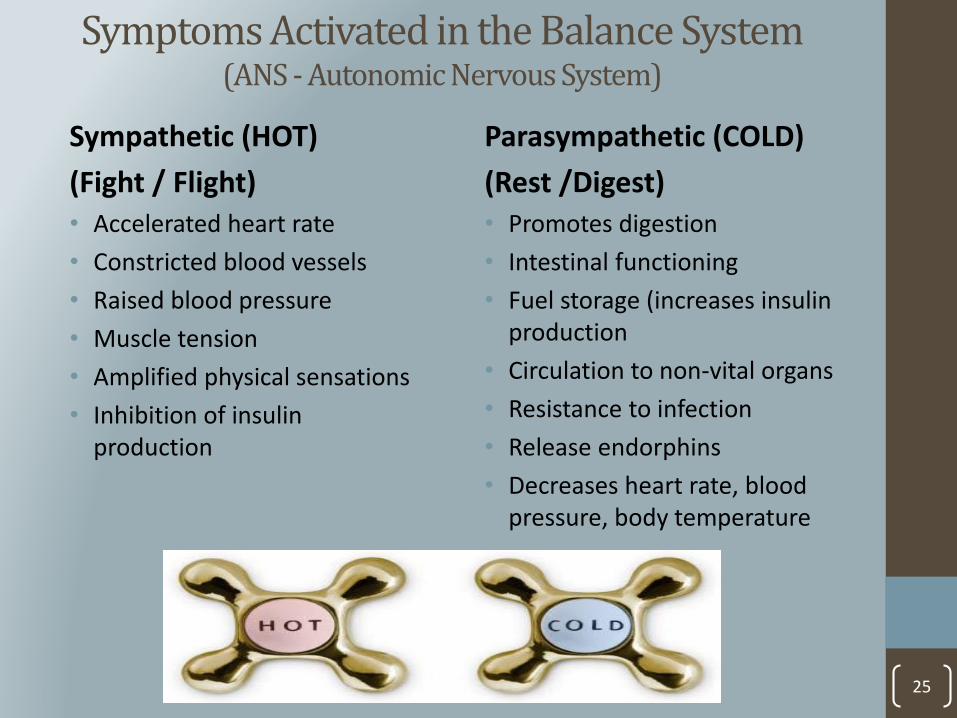
Symptoms Activated in the Balance System(ANS - Autonomic Nervous System)
Sympathetic (HOT)
(Fight / Flight)• Accelerated heart rate
• Constricted blood vessels
• Raised blood pressure
• Muscle tension
• Amplified physical sensations
• Inhibition of insulin production
Parasympathetic (COLD)
(Rest /Digest)• Promotes digestion
• Intestinal functioning
• Fuel storage (increases insulin production
• Circulation to non-vital organs
• Resistance to infection
• Release endorphins
• Decreases heart rate, blood pressure, body temperature
25

Trauma OccurrenceBody Reaction –Hot System Dominance
• Chemical Dump
• 30 chemicals including cortisol
• 12-30 hours to metabolize until return to a full balanced state
• Multiple dumps may occur in as little as 2 minutes
• Rewires the whole system
• Multiple small events happening over time activates small doses that has same effect as a big event
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 26
Body Reaction - Hot System DominanceDysregulation of the ANS Produces Survival Strategies
When brain is swimming in a chemical dump – noability for:
• Self awareness
• Self regulation
• Goal setting
• Positive self image
• Demonstration of empathy (self centered, narcissistic)
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 27
Survival Response !

Body Reaction - Hot System DominanceNot Bad Behaviors –Changes in Nervous System
• Fight, Freeze, Flight
• Aggression
• Hyperactivity
• Tantrums
• Name calling
• Anxiety
• Sadness /Withdrawal
• Inattention
• Impulsivity / reactionary
• Logic and reasoning shift
• Moral reasoning lessens
• Language ability reduces
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 28
Normal Response – Correct Behavior!

Environmental Impact on Hot System Dominance
• Provocative, stress filled environments on a repeated basis activates the hot system
• All environments need to be managed to prevent reaction• Home• School• Community
• Takes less than15 milliseconds for a person who has a danger focused radar system to react
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 29
Actual event doesn’t need to happen…just the perception of threat or stress!

When FASD, Trauma Meet…
FASD behaviors are pronounced
• More impulsive, hyperactive, forgetful
• Additional issues may occur
• Bedwetting, aggression, reactionary behaviors, rages, lying, stealing
• Hypervigilence may appear like extreme anxiety
• Trauma may be overlooked as the symptoms will appear like exaggerated ADHD, conduct disorder, anxiety and major depressive disorders resulting in misdiagnosis
• Overlooked as the professional may not be well-versed on the complexity of FASD and Trauma
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 30
Challenges for Caregivers
Child’s behaviors may rekindle painful feelings in caregivers who have attachment or trauma issues of their own
• Parent will avoid experiencing own emotions and will not respond appropriately
• Caregiver may see behaviors as a personal threat
• Behaviors trigger parent’s own memories of loss, rejection, abuse – results in diminished parenting
• When caregiver distress overrides the child’s distress the child may suppress or avoid their own feelings, as well as avoid the caregiver
• Behaviors can induce secondary trauma which can impact other family members – especially parents
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 31
Caring for children with Trauma Histories
Main Elements to Implement• Believe and validate the child’s experience
• Tolerate your child’s emotions
• Manage your own emotional response
• Reduce exposure to environmental chaos
Denying the child’s experience forces them to act as if it didn’t occur• Child learns to not trust the primary caregiver
• Child does not learn the language to deal with the experience
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 32

Nine Steps Retooling the Child /Parent Relationship
1. Be intentional about self-care• Write down one thing
you are willing to commit to once per week that fills you up –put it on the calendar
2. Identify why and what triggers your hot system. Identify supports needed to resolve.
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 33
3. Explore Parenting Framework• Bring our family of origin into our
parenting styles
• Values, expectations, beliefs, trauma backgrounds, attachment with own parents, culture
• Ask: What is currently going on in my life?
• What expectation can I get rid of?
4. Congratulate• What are the successful strategies
you currently use?
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 34
Nine Steps for Retooling cont’d.

Nine Steps for Retooling cont’d.
5. Observe your child “as if” this is the first time you met them. “Present moment focused”
• Listen – no cell phones
• No Analyzing or fixing
• No multi-tasking
• Limited talking
6. Be honestAsk what percent of the time are you correcting or consequencing your child?
• Increase noticing statements –focus on the behaviors you want instead of what you don’t want.
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 35

Nine Steps for Retooling Cont’d.
7. Explore the purpose of behavior
What sets up the behaviors and what triggers the behavior?• Are they striving for safety?
• Attention seeking or comfort seeking
• Avoiding task, avoiding connection
• Do they feel like they belong?
• Do they feel its impossible to please you?
• Evaluate the environment at home, school, community
• When do behaviors occur? Is there a common trigger i.e. sleep?
• Anniversary dates – what is the pattern
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 36

37
CHILD’S Behavior
PARENTRESPONSE
Cause of Behavior Could Be….. Child’s Needs Could Be….
Lying Memory issue Could be trauma response
Avoids looking “dumb by filling in the blanks with own story. Slow down, simplify steps. May feel threatened – trying to survive.
Doesn’t listen
Memory issue Sensory issue –auditory filteringToo many stepsAttention problems
Covers up with defiance, frustration, may shut down. Slow down requests and information. Give frequent breaks if child has attention issues. Provide quite space without background noise.
Hoardingfood in their room
Previous neglect –fear – trauma response
Safety/SurvivalNeeds assurance that she/he is safe.Child may need to have access to food at all times.
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission.

Nine Steps for Retooling cont’d.
8. Discover a common link
• Crafts, TV program, Coloring, Sports, Collections –Make it about the child – mastery is everything!
9. Reflect at the end of the day
• What do you love about your child?• What was funny? What was curious?
• What can you do tomorrow to strengthen your relationship?
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 38

Achieving Parenting Success
©Pathway Consulting, LLC ©2017 These slides may not be reproduced or used without written permission. 39
Do the best you can until you know better. Then when you know better, do better.
Maya Angelou
©Pathway Consulting, LLC. 40
Jeanne Ketola, MA, LPCC, holds a Master’s degree in clinical counseling and psychotherapy. She works with adoptive, birth and foster families specializing in working with families and children affected by Fetal Alcohol Spectrum Disorder (FASD) and trauma. She is a parent of three adopted children and has navigated the world of FASD and trauma for over 15 years as a parent, professional and national advocate. Jeanne has experienced the frustration and ineffectiveness of a one-sided approach to FASD and trauma in all areas including therapeutic settings, schools, social and criminal justice systems. Jeanne has met with Congressional offices in Washington D.C. to advocate for national bills relating to Fetal Alcohol Syndrome and played a key role in changing state legislation to include FASD in the Related Conditions Definition for Developmental Disabilities Criteria. She is certified in Families Moving Forward which is a scientifically researched program for parents of children with an FASD; she received the Permanency and Adoption Competency Certification from the University of Minnesota, and recently completed a short study on the improvement of adaptive functioning in children with an FASD who receive a multidimensional therapeutic approach. She is currently receiving training as a certified clinical trauma professional for individuals and families.
Contact Jeanne 612-810-7592