
a cross sectional study on the prevalence, knowledge, attitude and ...
24
W 7 C. r 70 ývNIMPSý .1 'ý ". ý". " A CROSS SECTIONAL STUDY ON THE PREVALENCE, KNOWLEDGE, ATTITUDE AND PRACTICE OF HYPERCHOLESTEROLAEMIA AMONG THE SAMPLED POPULATION OF AGE 35 YEARS AND ABOVE IN KAMPUNG SADONG JAYA FROM 14th JUNE TO 20th AUGUST 2004 Report by YEAR 4 MEDICAL STUDENTS GROUP 1 COMMUNITY MEDICINE AND PUBLIC HEALTH POSTING: Yang Boon Yon Zuffazarina binti Zulkapli Thanuja a/p Mahaletchumy Shazni Izana binti Shahruddin Peter ak Jerampang Koe Hooi Ming Daphne Dewi ak Stephen Kalong Alex Lee Fook Seng Aisah Munirah binti Wahi Norizan binti R. osli Noor Suhaila binti Abu Bakar Mursyida binti Md Nujid Mariza binti Md Rasip Adeline Kueh Mei Ling
Transcript of a cross sectional study on the prevalence, knowledge, attitude and ...

W 7
C. r
70
ývNIMPSý
.1 'ý ". ý". "
A CROSS SECTIONAL STUDY ON THE PREVALENCE, KNOWLEDGE, ATTITUDE AND PRACTICE OF
HYPERCHOLESTEROLAEMIA AMONG THE SAMPLED POPULATION OF AGE 35 YEARS AND ABOVE IN KAMPUNG
SADONG JAYA FROM 14th JUNE TO 20th AUGUST 2004
Report by YEAR 4 MEDICAL STUDENTS
GROUP 1 COMMUNITY MEDICINE AND PUBLIC HEALTH POSTING:
Yang Boon Yon Zuffazarina binti Zulkapli
Thanuja a/p Mahaletchumy Shazni Izana binti Shahruddin
Peter ak Jerampang Koe Hooi Ming
Daphne Dewi ak Stephen Kalong
Alex Lee Fook Seng Aisah Munirah binti Wahi Norizan binti R. osli Noor Suhaila binti Abu Bakar Mursyida binti Md Nujid Mariza binti Md Rasip Adeline Kueh Mei Ling
Pusat lCluacnai lvtui: lur[taº Aic. ̂. cicmik UNIVERSI'll MALAYSIA SARAWAK
FACULTY OF MEDICINE AND HEALTH SCIENCES,
UNIVERSITY OF MALAYSIA SARAWAK
,0
ý; ý R`ý
A CROSS SECTIONAL STUDY ON THE PREVALENCE, KNOWLEDGE, ATTITUDE AND PRACTICE OF
HYPERCHOLESTEROLAEMIA AMONG THE SAMPLED POPULATION OF AGE 35 YEARS AND ABOVE IN
KAMPUNG SADONG JAYA FROM 14TH JUNE TO 20TH AUGUST 2004
Report by YEAR 4 MEDICAL STUDENTS
GROUP 1 COMMUNITY MEDICINE AND PUBLIC HEALTH POSTING:
Yang Boon Yon 7642 Zuffazarina binti Zulkapli 7305 Thanuja a/p Mahaletchumy 7219 Shazni Izana binti Shahruddin 7133 Peter ak Jerampang 7026 Koe Hooi Ming 6676 Daphne Dewi ak Stephen Kalong 6432 Alex Lee Fook Seng 6263 Aisah Munirah binti Wahi 6259 Norman binti Rosli 6084 Noor Suhaila binti Abu Bakar 6051 Mursyida binti Md Nujid 6029 Mariza binti Md Rasip 3258 Adeline Kueh Mei Ling 6226

DECLARATION
We, the research team members whose names appears herein below hereby declare that this
research is our own original work with the exception of quotations of the works in which we
had stated their sources.
Yang Boon Yon 7642
Zuffazarina binti Zulkapli 7305
Thanuja a/p Mahaletchumy 7219
Shazni Izana binti Shahruddin 7133
Peter ak Jerampang 7026
Koe Hooi Ming 6676
Daphne Dewi ak Stephen Kalong 6432
Alex Lee Fook Seng 6263
Aisah Munirah binti Wahi 6259
Norizan binti Rosli 6084
Noor Suhaila binti Abu Bakar 6051
Mursyida binti Md Nujid 6029
Mariza binti Md Rasip 3258
Adeline Kueh Mei Ling 6226
i

ACKNOWLEDGEMENT
Embarking upon the journey in completing this daunting task, no words could
compensate the gratitude we fell towards those that have been a big help in completing our
report. Thus, we would like to extend our most sincere thank you to those who were
involved directly or indirectly in making this research a success. First and foremost, we
would like to convey our deepest appreciation to Penghulu Tuan Haji Yaakob Matsir,
members of Jawatankuasa Kemajuan dan Keselamatan Kampung (Village Committee) and
all the residents of Kampung Sadong Jaya.
We would like to express our heartfelt appreciation to University Malaysia Sarawak
(UNIMAS) for extending her full cooperation towards the success of this project. We would
like to express our sincere gratitude to Mr Cliffton Akoi anak Pangarah, and Dr Kamaluddin
Bakar, coordinators of Community Medicine and Public Health Posting, who contributed
tremendously through time, advice and guidance towards the success of our research.
We further extend our sincere gratitude to Professor Dr. Hashami Bohari, Deputy
Dean of Medicine and Health Science Faculty; Associate Professor Dr. Mariah Ahmad,
Associate Professor Dr. Win Kyi and Puan Rasidah Abd. Wahab for their support, guidance
and encouragement.
We would also like to acknowledge Professor Dr Syed Hassan Ahmad Al-Mashoor,
Dean of Faculty of Medicine and Health Sciences UNIMAS, all lecturers and other staff
members of the faculty for their help and support in any forms, towards a success in our
research and intervention programme
11

We would like to further express our heartfelt gratitude to the Divisional Health
Office of Kota Samarahan and all the staff members of Klinik Kesihatan Sadong Jaya for
their support and cooperation during our posting in Sadong Jaya.
Our appreciation is also extended to those who were directly or indirectly involved in
our community program and all the individuals as well as companies who had given their
fullest support in the forms of finance and materials.
Last but not least, our deepest gratitude is extended to all the 14 members of the group
for their commitment and contribution of productive ideas for the successful completion of
this research.
ül
ABSTRAK
Hiperkolesterolemia ialah suatu keadaan penyakit yang semakin meningkat di seluruh dunia, terutamanya kerana perubahan pada gaya hidup dan juga amalan pemakanan. Keadaan ini adalah disebabkan oleh kandungan kolesterol yang tinggi dalam darah. Hiperkolesterolemia
merupakan salah satu risiko utama berlakunya penyakit jantung. Walaupun hiperkolesterolemia selalunya dianggap sebagai ̀penyakit penduduk bandar', tetapi disebabkan Malaysia sedang berkembang pesat sebagai sebuah negara moden pesat, kesan-kesan
urbanisasi, terutamanya dari sudut kesihatan, kawasan luar banda juga akan turut mengalami tempiasnya.
Satu kajian rentas ke atas prevalens, pengetahuan, amalan dan perlakuan terhadap hiperkolesterolemia di kalangan sample populasi yang berumur 35 tahun dan ke atas telah dijalankan di Kampung Sadong Jaya.
Melalui kaedah bancian dan EPI Info 6.04, seramai 150 responden telah dipilih secara rawak. Temuramah dan pengukuran tahap kolesterol dalam darah telah dilakukan ke atas setiap responden. Antara kriteria pengecualian yand telah diambil kira dlah mereka yang terlampau sakit dan telah menolak dari menurut serta melakukan kaji selidik selepas tiga kali
percubaan.
Melalui kajian yang dilaksanakan, hanya separuh daripada responden, iaitu sebanyak 55.0% mempunyai pengetahuan yang baik tentang hiperkolesterolemia, manakala sebanayk 45.0% lagi tidak. Tambahan lagi, terdapat 60.0% responden yang mempunyai sikap yang betul dan sebanyak 40.0% mempunyai sikap yang salah terhadap hiperolesterolemia. Sebanyak 54.0% responden mempunyai amalan yang baik terhadap hiperkolesterolemia, dan selebihnya sebanayk 46.0% tidak. Daripada kajian yang telah dilakukan juga, privalens mereka yang mempunyai tahap kolesterol keseluruhan yang optimum (kurang dari 5.20 mmol/1) adalah sebanyak 69.0%. Bagi mereka yang mempunyai tahap kolesterol keseluruhan yang atas garis garis sempadan (dari 5.21 mmol/l ke 6.20 mmol/l) pula adalah sebanyak 25.0%. Didapati,
sebanayk 6.0% responden mempunyai risiko yang tinggi terhadap hiperkolesterolemia (lebih dari 6.20 mmoVl)
ABSTRACT
Hypercholesterolaemia is a disease condition, which is on the rise worldwide, owing mainly due to the changes in lifestyle and dietary habits. It is a condition where there is excess cholesterol in the blood. It is one of the major risk factors for cardiovascular mortality. Although hypercholesterolaemia is normally thought as a `disease among the urban', but since Malaysia is progressively encroaching modernization, the effect of urbanization, especially regarding health, will leak towards it's surrounding area, including the rural parts.
A cross-sectional study on the prevalence, knowledge, attitude and practice of hypercholesterolaemia among the sampled population aged 35 years old and above was carried out in Kampung Sadong Jaya.
Through census and EPI info 6.04 a total of 150 respondents were randomly selected for questionnaire interviews, measurements of total cholesterol level and body mass index. The exclusion criteria include those who are severely ill, and those that refuses even after 3 attempts of approaching the respondent fails.
From the research that has been conducted, only about half of the respondents, which accounts towards 55.0%, had good knowledge regarding Hypercholesterolaemia while another 45.0% did not. Furthermore, there were 60.0% of respondents having good attitude and another 40.0% have unhealthy attitude regarding Hypercholesterolaemia. A percentage of 54.0% respondents have good practice while another 46.0% did not. As for the prevalence of hypercholesterolaemia among the respondents, 69.0% of the respondents had desirable total cholesterol (less than 5.20 mmol/1), 25.0% had borderline hypercholesterolaemia (from 5.21 mmol/l to 6.20 mmol/1) while 6.0 % had high risk of hypercholesterolaemia (more than 6.20 mmol/1).
V

UIVIVERSTI] MALAYSIA SARgwAK
CONTENT
TABLE OF CONTENTS
DECLARATION
ACKNOWLEDGEMENT
ABSTRACT
ABSTRAK
CONTENTS
LIST OF TABLES
LIST OF FIGURES
CHAPTER I INTRODUCTION AND BACKGROUND
1.1 Introduction
1.2 Background information
CHAPTER II RESEARCH PROBLEM AND LITERATURE
REVIEW
2.1 Research Problem
2.2 Literature Review
CHAPTER III OBJECTIVES AND HYPOTHESES
3.1 General objective
3.2 Specific objectives
3.3 Research Hypotheses
CHAPTER IV RESEARCH METHODOLOGY
4.1 Research design
Page
i
I1
iv
V
V1
ix
X
1
4
7
10
18
18
19
20
vi

4.2 Research setting
4.3 Population and sampling
4.4 Study Instrument
4.5 Data collection and data analysis
4.6 Research methodology flow chart
4.7 Operational definition
CHAPTER V RESULTS
5.1 Sociodemography
5.2 Knowledge on Hypercholesterolaemia
5.3 Attitude on Hypercholesterolaemia
5.4 Practice on Hypercholesterolaemia
5.5 Prevalence of Hypercholesterolaemia
5.6 Body Mass Index
5.7 Level of knowledge with level of attitude
5.8 Level of knowledge with level of attitude
CHAPTER VI DISCUSSION
6.1 Introduction
6.2 Knowledge on Hypercholesterolaemia
6.3 Attitude on Hypercholesterolaemia
6.4 Practice of Hypercholesterolaemia
6.5 Prevalence of hypercholesterolaemia
CHAPTER VII LIMITATION, RECOMMENDATION AND CONCLUSION
20
20
21
22
23
24
29
32
45
49
58
65
66
67
69
69
71
72
72
vii
7.1 Limitation
7.2 Recommendation
7.3 Conclusion
BIBLIOGRAPHY
APPENDICES
I. Organisational Chart of the Research Team
II. Map of Kampung Sadong Jaya
III. Questionnaire
a. Englishn version
b. Malay version
c. Bahasa Melayu Sarawak version
IV. Census card
V. Group Activity Photos
76
78
78
80
84
85
86
92
99
105
106
viii
LIST OF TABLES
NO TITLE 1 Mean and standard deviation of age with gender among the
respondents
PAGE 29
2 Answers Regarding Knowledge on the meaning of cholesterol, HDL 32
and LDL
3 Knowledge on the association between diet and hypercholesterolaemia 34
4 Respondents' knowledge about methods of cooking that increase 35 cholesterol in food.
5 The respondents' knowledge on non-dietary risk factors of 37 hypercholesterolaemia.
6 The respondents' knowledge on non-dietary risk factors of 38 hypercholesterolaem. ia.
7 Level of Knowledge of Respondents according to Gender 43
8 Mean Age and Standard Deviation of Age according of 43 Respondents with for Good and Bad Knowledge
9 Mean and Standard Deviation of Income according to Knowledge 44
10 Relationship between Knowledge and Educational Level of 44 Respondents
11 Answer of Respondents Regarding Food Preparation Methods 51
12 Percentage of Respondents according to Types of Food and Units 51-52 of food intake within a week
13 Percentage of High Fiber Food Intake among the Respondents 53
14 Percentage of Respondents according to Frequency of Weight 56 Measurement
ix

LIST OF FIGURES
NO FIGURES PAGES I Percentage of The Respondents according to Educational Level 30
2 Monthly Household Income of Respondents 31
3 Answer for the Question 36
4 Percentage of Respondents With Good Knowledge on Types of 36 Food High in Cholesterol
5 Percentage of Respondents Having Good Knowledge on Methods of 38 Cooking That Could Increases Cholesterol Level
6 Percentage of Respondents Having Good Knowledge on Non- 39 Dietary Risk Factors and the Prevention of Hypercholesterolaemia
7 Knowledge of Respondents on Complications of Hypercholesterolaemia
40
8 Percentage of Respondents Having Good Knowledge on the 41 Conditions Related to Hypercholesterolaemia
9 Percentage of Respondents with Knowledge on the Availability of 41 Pharmacotheray for the Control of Hypercholesterolaemia
10 Knowledge Regarding Hypercholesterolaemia 42
11 Percentage of Answer for each Question regarding to Attitude of 45 Food Modification among the Respondents.
12 Percentage of Respondents towards the Willingness to Exercise 46 assumed to be Normal and to have Hypercholesterolaemia
13 Willingness to Stop Smoking if have Hypercholesterolaemia 47
14 Answers towards the Willingness to Seek for Treatment 48
15 Attitude of the Respondents towards Hypercholesterolaemia 49
X
16 Food Preparation Methods 50
17 Cholesterol Level in the Diet of the Respondents 52
18 Frequency of Eating Out among Respondents 54
19 Percentage of Respondents Exercise at Least 3 Times per Week 55
20 Number of Respondents Had Screened Their Cholesterol Before. 57
21 Practice to Prevent Hypercholesterolaemia 58
22 Total Cholesterol Level of Respondents 59
23 Scattergram Showing Distribution of Total Cholesterol Level 60 according to Age
24 Level of Total Cholesterol with Gender 61
25 Level of Total Cholesterol with Race 62
26 Level of Total Cholesterol with Educational Level 63
27 Total Cholesterol Level in mmol/l with Monthly Household Income 64
28 Level of Total Cholesterol with Cholesterol Level In Diet 65
29 Body Mass Index of Respondents 66
30 Scattergram Showing Distribution of Total Cholesterol Level 67 according to Body Mass Index
31 Relationship between Level of Knowledge and Level of Attitude 68 on Hypercholesterolaemia
32 Relationship between Knowledge and Practice 69
XI
CHAPTER 1
INTRODUCTION AND BACKGROUND
1.1 Introduction
Hypercholestrolaemia is a condition in which the level of cholesterol in the blood is
high. When there is too much cholesterol, deposits of fat in the blood called plaque form inside
blood vessel walls. This causes the blood vessel walls to thicken and become narrower. This
change in the blood vessels reduces blood flow through the blood vessels, increasing the risk
of coronary heart disease (Ehnholm et al, 1982).
A period of over 20 years of sustained economic growth and political stability has
made Malaysia one of the most buoyant Southeast Asian countries. Such rapid advancements
in the socio-economic situation in the countries in Asia, resulted in significant changes in the
life-styles of communities, including food habits, and food purchasing and consumption
patterns. The shift towards to the "westernized" dietary pattern has also brought about a new
nutrition scenario in our country. These has caused some segments of the communities to
suffer from the problems of hypercholestrolaemia and associated disorders in other groups.
These disorders, frequently termed the diet-related chronic non-communicable diseases include
coronary heart disease as the major one (WHO, 1996).
Serum cholesterol concentrations vary widely throughout the world. Generally,
countries associated with low serum cholesterol concentrations (eg, Japan) have lower CHD
event rates, while countries associated with very high serum cholesterol concentrations (eg,
Finland) have very high CHD event rates. However, some populations with similar total
1
cholesterol levels have very different CHD event rates, suggesting that other factors also
influence CHD risk (Brown, 1986). Therefore, it is vital to identify all the risk factors
involved in elevation of cholesterol level.
In Malaysia, rapid and marked socioeconomic advancements for the past decades have
brought about significant changes in the lifestyle of communities. These include significant
changes in the dietary patterns of Malaysian, for example the increase in consumption of fats
and oils and refined carbohydrates and a decreased intake of complex carbohydrates (Tee, Ng
& Azriman, 1999).
Several epidemiological studies which were conducted in Malaysia on risk factors of
coronary heart disease have shown that hypercholesterolemia was a problem amongst the more
affluent segments of the population whereas the rural population have lower levels of serum
cholesterol of about 3.6 mmol/L. Urban Malaysian were found to have higher serum
cholesterol level (Tee et al, 1999). Urban Malaysians were found to have the highest serum
cholesterol levels of 4.2-4.4 mmol/L. The prevalence of hypercholesterolemia amongst this
group is almost 30% (Ministry of Health, 1997).
The mean blood cholesterol level for the aborigines in west Malaysia was found to be
low at about 3.8mmol/L and none of them were hypercholesterolaemic. The average
cholesterol level among poor rural Malay men was reported to be also low, at 3.6mmol/L
(Khor et al, 1997).
Among the main ethnic groups, Indians are reported to have the highest prevalence of
hypercholesterolaemia (43.2%), as compared to 35.2% and 24.2% among the Malays and
Chinese respectively. Earlier studies did not find a significantly higher prevalence of
hypercholesterolaemia among the Indians than the Chinese and Malays. This development is
2

of significance in light of the fact that the Indians presently show the highest mortality rate for
coronary heart disease (Ministry of Health, 1997).
World wide, due to marked geographical differences in the incidence of coronary heart
disease within the countries and early study about these interpopulation differences was done
which known as The Seven Countries Study. It was found that the median cholesterol levels
which were very high are correlated with increased coronary heart mortality (Seven Countries
studies, 1980).
All the above evidence clearly shows that hypercholestrolaemia is in the rise among
almost all societies both in Malaysia as well as in the world. It is therefore a step in the right
direction to conduct a research on this aspect. By assessing the knowledge, attitude and
practice of people regarding hypercholestrolaemia, would help to identify the problem at the
grassroot level. By assessing the prevalence of hypercholestrolaemia we aim to identify the
target group so that future strategies for nutrition education can be carried out effectively.
Another importance is so that more effective dissemination of information regarding this
health topic could be done. At the same time, we can determine how best to promote healthy
eating within the present scenario of rapid urbanization, "western" dietary pattern influence, a
whole barrage of convenience and " health" foods and nutrition misinformation.
It is hoped that this research would contribute to enriching the knowledge on
hypercholestrolemia and the ways to reduce it among the rural community of Kampung
Sadong Jaya.
3
1.2 Background
Geographical location
Kampung Sadong Jaya, an area in the district of Sadong Jaya and Kota Samarahan
division is a Malay community area, which is located in close vicinity to the South China Sea.
It is situated approximately 70 km from Kuching and can be accessed either via road or river.
Population and organization
According to the statistics of year 2004, the population of Kampung Sadong Jaya
stands at 1162 which consists 9.75% of the total population of Sadong Jaya. The largest ethnic
group here is Malay (70%) followed by Bugis (12%), Jawa (13%), Chinese (4%) and others
(1%). A census carried by us on 30th June found out that out of this, 23.1% (269 person) are
aged more than 35. The organisation of this village consists of the Penghulu, Ketua Kampung,
Jawatankuasa Kemajuan dan Keselamatan Kampung(JKKK) followed by the community.
Economy
The majority of people in Kampung Sadong Jaya are farmers. Other occupations
include labourers in construction sites, fishermen and government servants. The common
plantations include coconut, cocoa, corn, pineapple and banana. Most of the farmers sell their
products such as coconut either directly to the shops or through Pertubuhan Peladang Sarawak.
Some bring the products to be sold at pasar rani.
4

Pusat KhidmAt Maktuiuat Akadelrcil, UNiVERSITI MALAYSIA SARAWAK
Basic amenities
Kampung Sadong Jaya is well equipped with basic amenities such as treated water and
electrical supply since the early 1990's. The houses are also supplied with phone lines. The
roads in this village are tar roads. The presence of rented vans as well as own transportation
enable the villagers to commute to the surrounding areas. Other facilities in this village include
public phones, post office, police station, common hall, registration office and primary school.
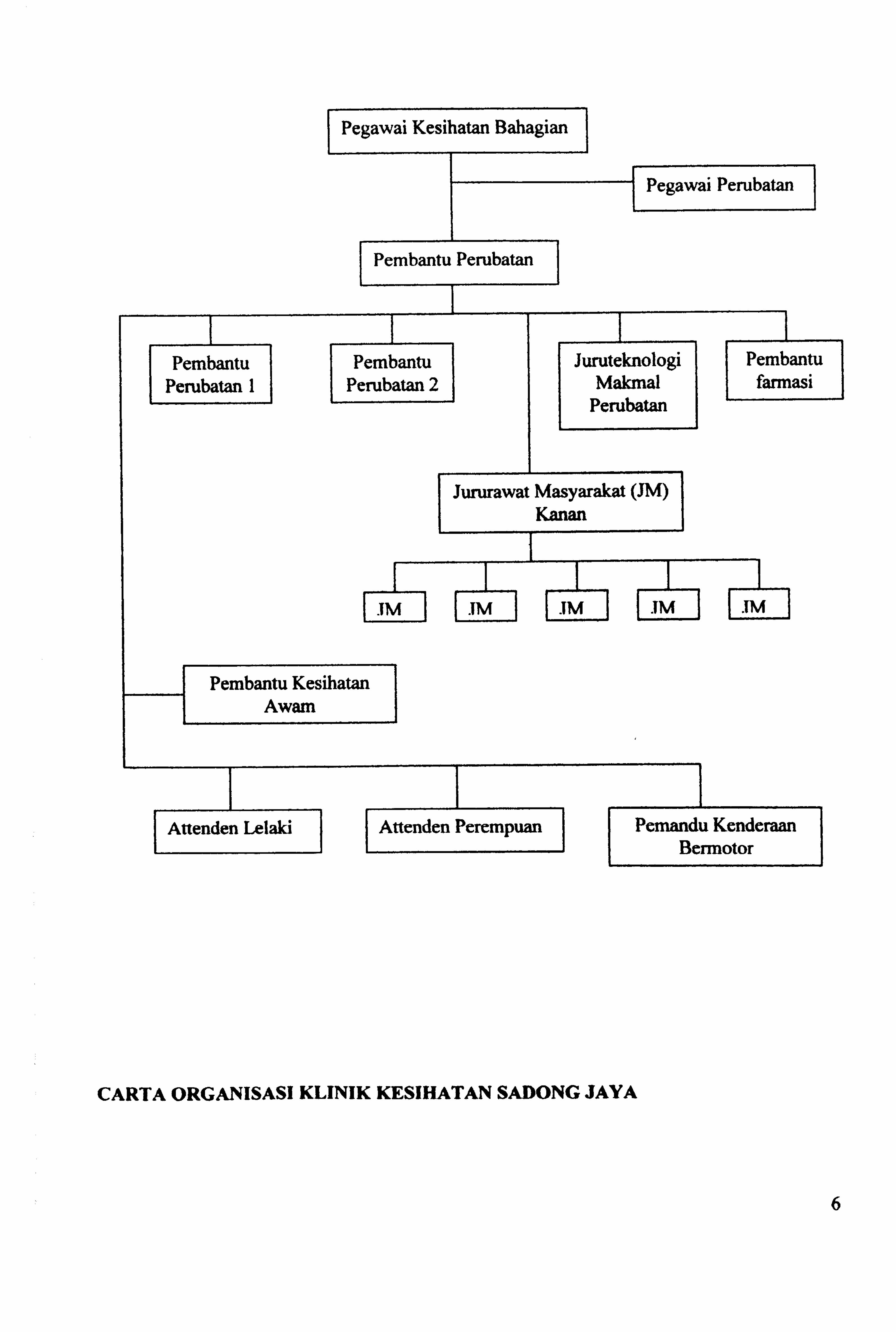
Health facilities
The health facilities in Kampung Sadong Jaya is mainly provided by the Klinik
Kesihatan Sadong Jaya which is situated 3 km away with more serious cases being referred to
the Sarawak General Hospital. The organization of this health clinic consists of a health
officer (Bahagian), a medical officer (clinic), two medical assistants, a lab technologist, six
community nurses, an assistant pharmacist, a public health assistant, two health attendants and
a driver. The services offered by this clinic include out patient care, antenatal care, post natal
care, dental care, environmental health (KAS), health education (HE), lab facilities, mental
care, village health team (VHT), tuberculosis control program (TBCP), immunization and
school health (SH). These services are offered according to a schedule.
5
Pegawai Kesihatan Bahagian
Pegawai Perubatan
Pembantu Perubatan 1
Pembantu Perubatan
Pembantu Perubatan 2
im
Juruteknologi Makmal
Perubatan
Pembantu farmasi
Jururawat Masyarakat (JM) Kanan
TM
Pembantu Kesihatan Awam
Altenden Lelaki Attenden Perempuan
im
Pemandu Kenderaan Bernrotor
CARTA ORGANISASI KLINIK KESIHATAN SADONG JAYA
6

CHAPTER II
STATEMENT OF PROBLEM AND LITERATURE REVIEW
2.1 Statement of problem
During our first visit to Kampung Sadong Jaya on 19th June 2004, the villagers did not
complaint of any health problems. However, upon direct questioning, we found out that their
diet contain significantly high cholesterol food such as rendang, nasi lemak sambal udang,
ikon bills, coconut milk containing food, eggs and beef. This pattern of diet is an important risk
factor for the development of coronary heart disease. Therefore, we proposed to do a study on
the knowledge, attitude and practice of hypercholesterolaemia as a risk factor for coronary
heart disease in the age group 35 years old and above in this village and were accepted by
them.
Even though, Kampung Sadong Jaya is situated in a rural setting, it still faces the effects
of urbanization of the surrounding area. It is therefore widely exposed to the risk factors of
diseases of the modern society of which coronary heart disease is the major one. This is mainly
due the changes in diet which leads to nutritional disorders such, as hypercholestrolaemia.
Despite such changes, the villagers still lack in knowledge regarding hypercholesterolaemia
which in turn affect their attitude and behaviour towards it.
We aim our study on the sample population aged 35 years old and above because the
major increase in hypercholestrolaemia is noted to begin at this age especially in men.
Furthermore, at this age the effects of hypercholestrolaemia as a risk factor for coronary heart
disease are widely seen. Since hypercholestrolaemia and coronary heart disease prevail as the
7
most significant cause of premature deaths in middle aged men (WHO, 1996), it is therefore a
move in the correct direction to target this age group as our study subject.
During the discussion with the villagers, they also revealed the lack of knowledge on
hypercholestrolaemia as a risk factor for coronary heart disease. Lack of knowledge affects their
attitude and practice towards this risk factor. By doing this study, we can measure the level of
awareness among the villagers regarding hypercholestrolaemia which is an important modifiable
risk factor of coronary heart disease.
Furthermore, most of the studies regarding hypercholesterolaemia are carried out in
urban areas because we generally fail to realize that these risk factors are also present in the rural
population. According to the villagers, although there is an outpatient department that deals with
problems of hypercholesterolaemia but programs involving educational and awareness-raising
intervention are seldom carried out in their village.
Hence, by carrying out this research we aim to identify the knowledge, attitude and
practice regarding hypercholesterolaemia as a risk factor of coronary heart disease so that early
health screening and health education intervention program can " be done to decrease the
morbidity and mortality due to coronary heart disease.
8
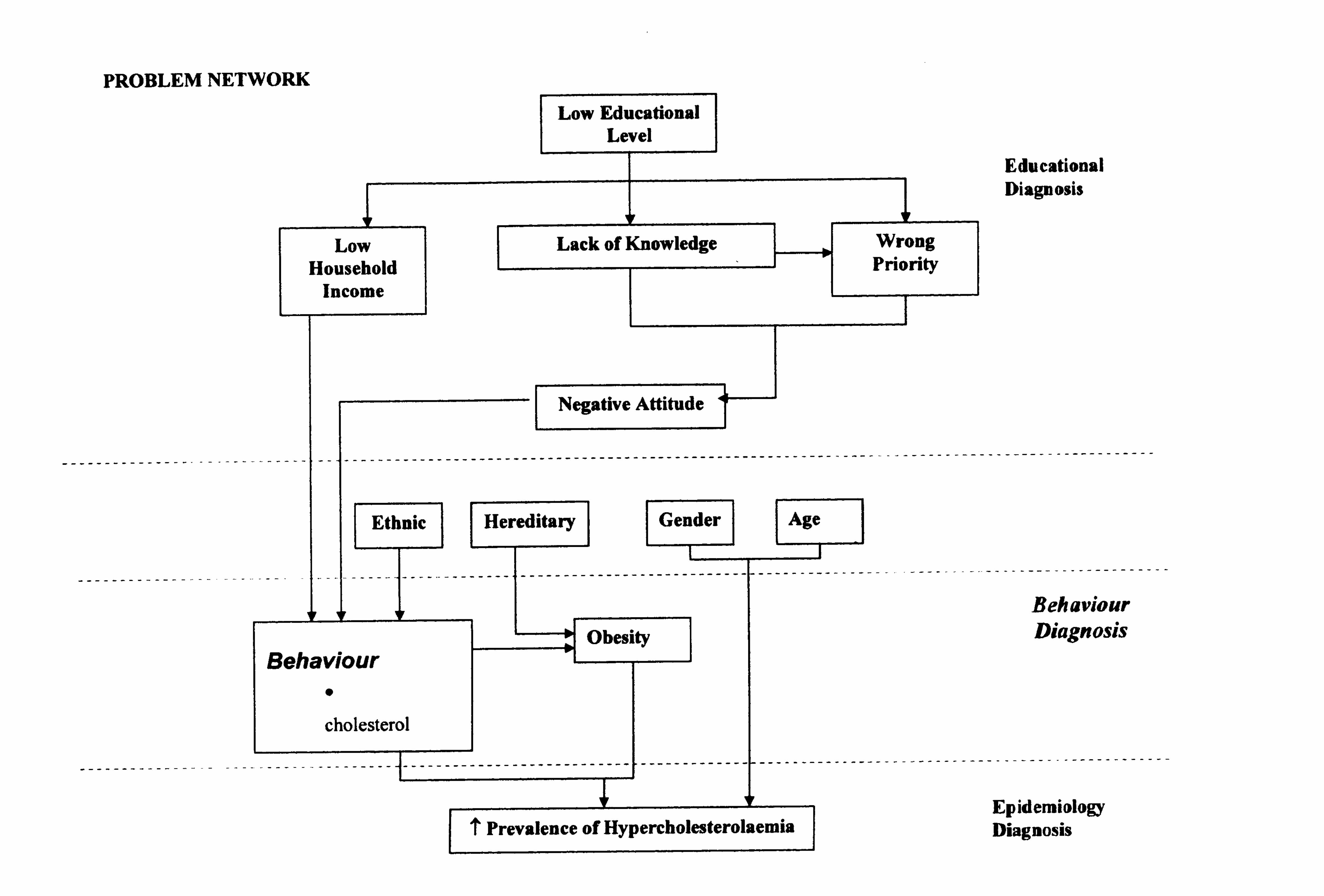
PROBLEM NETWORK
Hereditary
'I! ___ ____I__
Low Household
Income
N
-------------------------------------------------------------
Ethnic Gender
I ---------------------------
TT
Behaviour 0
cholesterol
N
Low Educational Level
Lack of Knowledge
Negative Attitude
Obesity
-I --------------------------- f------------- r-
Age
Educational Diagnosis
Behaviour Diagnosis
-----------------------------------
T Prevalence of Hypercholesterolaemia
Wrong Priority
Epidemiology Diagnosis
2.2 Literature review
Cholesterol is a substance that occurs naturally and is needed for our body to function
properly. Cholesterol is a soft, waxy substance found among the lipids in the bloodstream and in
all the body's cells. It is an important part of a healthy body because it is used to form cell
Membranes, some hormones, and other needed tissues. Cholesterol circulates in the blood stream.
it is an essential molecule for the human body. Cholesterol is a molecule from which hormones
land steroids are made. It is also used to maintain nerve cells.
Cholesterol is found in animal sources of food. It is not found in plants. Cholesterol is also
p form of fat found in egg yolks, meat, poultry, seafood and dairy products. Foods from plants
such as fiuits, vegetables, vegetable oils, grains, cereals, nuts and seeds may contain fat but not
cholesterol. Approximately 80 per cent of the cholesterol in the blood is manufactured by the liver.
The remaining 20 per cent comes from the foods we eat. Although many foods may be labelled
cholesterol free" or "cholesterol reduced", the liver manufactures lipoproteins from all fats we
consumed, therefore it is important to concentrate more on reducing the total fat consumption, than
on merely limited cholesterol consumption.
Cholesterol and other fats are not able to dissolve in the blood, and so are transported to
, and from the cells in the form of lipoproteins. Lipoproteins are a combination of fat (lipids) and
; proteins. There are several kinds of lipoproteins. But the ones to be most concerned about are low-
density lipoprotein (LDL) and high-density lipoprotein (HDL). Low-density lipoprotein (LDL) is
the major cholesterol carrier in the blood. Normal levels of LDL are essential for cell repair and
growth, however high levels of LDL in the blood are associated with the development of
atherosclerosis, and therefore coronary artery disease, heart attacks and strokes. This is why LDL
10
cholesterol is often referred to as the "bad" cholesterol. " Lower levels of LDL cholesterol reflect a
lower risk of heart disease. High-density lipoprotein or HDL has a higher protein-to-fat ratio than
. DL and it makes up about one-third to one-fourth of the blood cholesterol. HDL is commonly
referred to as the "good cholesterol" because it helps to carry excess LDL away from the walls of
, the blood vessels and back to the liver for excretion (Johnson et al, 1993). Research suggests that
high levels of HDL may protect the heart against atherosclerosis, and may even remove cholesterol
from atherosclerotic plaques and slow down their growth.
The desirable total cholesterol level is below 5.2 mmol/L. Borderline high is when the
(cholesterol level is between 5.2 to 6.2 mmol/L and it is considered high when more than
6.2mmol/L. The desired HDL cholesterol level is more than 0.9mmol/L. Ideal LDL cholesterol
! level is less than 3.5 mmol/L, borderline high is in between 3.5 to 3.9 mmol/L and high is more
than 4.0 mmol/L. Ideal triglycerides level is less than 2.0 mmol/L, borderline high is between 2.0
, to 3.0 mmol/L and high is more than 3.0 mmol/L (WHO Expert Committee, 1996).
Hypercholesterolaemia is very much influenced by lifestyle factors such as diet, exercise
and stress levels. On the other hand, it is also influenced by patients' knowledge, attitude, practice
and the intercorrelation between these factors.
Obesity, which generally results from eating a diet high in fat, can also lead to elevated
I cholesterol levels in the blood. This is because obesity itself leads the body to produce excessive
amounts of cholesterol. Being overweight is a risk factor for heart disease. It also tends to increase
the cholesterol. Losing weight can help lower LDL and total cholesterol levels, as well as raise
HDL and lower triglyceride levels (Neaton, 1992).
11


















