
A COMPARATIVE STUDY OF THE EFFECTS OF DIFFERENT DRUGS …
17
www.wjpps.com Vol 8, Issue 7, 2019. 1595 Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences A COMPARATIVE STUDY OF THE EFFECTS OF DIFFERENT DRUGS USED TO SUPPLEMENT THE LOCAL ANESTHETIC IN INTRAVENOUS REGIONAL ANESTHESIA (BIER'S BLOCK) FOR SURGICAL PROCEDURES OF THE UPPER LIMB *Dr. Trifa Assadlah Faidlah and Ali Mohammed Kareem College of Medicine University of Sulaimani. ABSTRACT Background: block) is used for anesthesia for surgical procedures on the upper limb, it is a reliable, simple and safe method for providing anesthesia with low incidence of side effects. It is recommended as an alternative to general anesthesia for operations on the hands, forearms and arms. An intravenous cannula is inserted, the limb is exsanguinated, a tourniquet applied and the veins filled with local anesthetic. Intravenous regional anesthesia (Bier's Objective: To perform the intravenous regional anesthesia by using minimal dose of local anesthetic (lidocaine) with additive drugs (dexamethasone, atracurium) to decrease the toxicity of lidocaine and improve the quality of anesthesia, analgesia and muscle relaxation perioperatively. Study design: This study is clinical trials comparative study. Setting: This study was performed in Teaching and Emergency Hospitals in Sulimani city eriod of January 2007 to September 2007, it is approved by Suliamani Ethical mittee. uk a Laas ASA I and II status, average ages of 18-65 years of both gender were omly into three groups, thirty patients in each group, neither prepared nor me measures: ents the onset of action, time to motor and sensory recovery and gesia were measured, comparison among them is done and the epain intensity scale was evaluated. sults shows that the addition of (8 mg) dexamethasone to lidocaine 1e to sensory recovery and perioperative analgesia in group B (12.48 + is longer than in group A (plane lidocaine) (11.55 + 1.35, 52.50 ess than0.05). nonstrates that the addition of (1 mg) of atracurium to lidocaine n (complete motor and sensory block) in group C (4.40 + soup A (4.99 + 0.13) (p value is less than 0.05), while the 4 perioperative analgesia in group A (14.06 + 0.79, 52.50 5 + 1.66, 50.8 + 13.6) (p value is more0.05) Conclusions: It is concluded that the addition of (8 mg) of dexamethasone to supplement a“ intravenous WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES SJIF Impact Factor 7.421 Volume 8, Issue 7, 1595-1611 Research Article ISSN 2278 – 4357 *Corresponding Author Dr. Trifa Assadlah Faidlah College of Medicine University of Sulaimani. Article Received on 18 May 2019, Revised on 08 June 2019, Accepted on 28 June 2019 DOI: 10.20959/wjpps20197-14232
Transcript of A COMPARATIVE STUDY OF THE EFFECTS OF DIFFERENT DRUGS …

www.wjpps.com Vol 8, Issue 7, 2019.
1595
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
A COMPARATIVE STUDY OF THE EFFECTS OF DIFFERENT
DRUGS USED TO SUPPLEMENT THE LOCAL ANESTHETIC IN
INTRAVENOUS REGIONAL ANESTHESIA (BIER'S BLOCK) FOR
SURGICAL PROCEDURES OF THE UPPER LIMB
*Dr. Trifa Assadlah Faidlah and Ali Mohammed Kareem
College of Medicine University of Sulaimani.
ABSTRACT
Background: block) is used for anesthesia for surgical procedures on
the upper limb, it is a reliable, simple and safe method for providing
anesthesia with low incidence of side effects. It is recommended as an
alternative to general anesthesia for operations on the hands, forearms
and arms. An intravenous cannula is inserted, the limb is
exsanguinated, a tourniquet applied and the veins filled with local
anesthetic. Intravenous regional anesthesia (Bier's Objective: To
perform the intravenous regional anesthesia by using minimal dose of
local anesthetic (lidocaine) with additive drugs (dexamethasone, atracurium) to decrease the
toxicity of lidocaine and improve the quality of anesthesia, analgesia and muscle relaxation
perioperatively. Study design: This study is clinical trials comparative study. Setting: This
study was performed in Teaching and Emergency Hospitals in Sulimani city eriod of January
2007 to September 2007, it is approved by Suliamani Ethical mittee. uk a Laas ASA I and II
status, average ages of 18-65 years of both gender were omly into three groups, thirty patients
in each group, neither prepared nor me measures: ents the onset of action, time to motor and
sensory recovery and gesia were measured, comparison among them is done and the epain
intensity scale was evaluated. sults shows that the addition of (8 mg) dexamethasone to
lidocaine 1e to sensory recovery and perioperative analgesia in group B (12.48 + is longer
than in group A (plane lidocaine) (11.55 + 1.35, 52.50 ess than0.05). nonstrates that the
addition of (1 mg) of atracurium to lidocaine n (complete motor and sensory block) in group
C (4.40 + soup A (4.99 + 0.13) (p value is less than 0.05), while the 4 perioperative analgesia
in group A (14.06 + 0.79, 52.50 5 + 1.66, 50.8 + 13.6) (p value is more0.05) Conclusions: It
is concluded that the addition of (8 mg) of dexamethasone to supplement a“ intravenous
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.421
Volume 8, Issue 7, 1595-1611 Research Article ISSN 2278 – 4357
*Corresponding Author
Dr. Trifa Assadlah Faidlah
College of Medicine
University of Sulaimani.
Article Received on
18 May 2019,
Revised on 08 June 2019,
Accepted on 28 June 2019
DOI: 10.20959/wjpps20197-14232

www.wjpps.com Vol 8, Issue 7, 2019.
1596
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
regional anesthesia is advisable to improve the quality of anesthesia an in provide better
perioperative analgesia and the addition of a minimum dose of atracurium (1 mg) will speed
the onset of action, provide good intraoperative muscle relaxation and optimize the operative
condition with minimizing the potential toxicity of the local anesthetic.
KEYWARDS: Bier's block, simple descriptive pain intensity scale, dexamethasone and
atracurium.
1.1 INTRODUCTION
1.1.1 Intravenous regional anesthesia (Bier’s block) +
Many procedures in the upper limb can be performed on awake patients using intravenous
regional anesthesia (IVRA). This not only avoids the risks and unplea which sometimes
associated with general anest benefits such as reduced blood loss often lasts longer t! several
hours after the surgery, in addition; some patien they are awake during surgery. a Intravenous
regional anesthesia providing anesthesia for minor surgica minutes), it is suited to operations
of the dista knee), such as reduction of radial or ulna fracture, carpa wrist ganglion, foreign
body removal and palmer faciotomy. santness such as nausea and vomiting hesia but may
also provide specific han the providing pain relief for ts feel more in control when is a
reliable, simple and safe method for procedures of relatively short duration (60-90 arm or leg
(i.e. below the elbow or | tunnel syndrome, excision of (2,3)
1.1.2 Technique: Intravenous regional anesthesia (Bier‟s block) is unique regional local
anesthetic blocked via the venous system, it presumed the nerve roots by back diffusion from
the Intravenous regional anesthesia (Bier technique as it relies on the nerves being that the
local anesthetic gain access to veins. echnique involves total isolation and drainage of the
venous network in the n Esmarch bandage and tourniquet. The former empties the veins
whilst ents further influx of blood. (a specially designed double tourniquet is s cannula is
inserted in the affected arm as distally as possible Po the contra lateral one for injection of
drugs (sedatives ang d, the proximal tourniquet is inflated to a safe level (usually nd using
sterile technique. (7) ssthetic agent which is the lidocaine was used 40 ml of 0.5 % ient and
safe anesthesia. The dosage used should allow for eins are then filled with local anesthetic.
“ses in to the small veins surrounding the nerves and then id cz pillary plexus of the nerves
leading to a core to mantle in the nerves involved. Local anesthetic then diffusesn, blocking
their conduction. contributes to the analgesic action of on and motor end plate function, —
will be analgesia to pinprick he speed of onset and the (10) The tourniquet produces

www.wjpps.com Vol 8, Issue 7, 2019.
1597
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
ischemia, which the local anaestetic by blocking nerve conducti twenty minutes after
tourniquet application alone there without the injection of any local anesthetic however, t
density of anesthesia are greater with injection of local anesthetic. short time; the tourniquet
is left inflated Satisfactory anesthesia was obtained in a ion of the anesthetic agent in to the
for a minimum of 30 minutes after inject extremity, ('!? As the more proximal tourniquet
become un inflated and then the proximal tourniquet is deflated. comfortable, the distal
tourniquet is (12)
1.1.3 Advantages of intravenous regional anesthesia are
Speed of onset and rapid recovery.
Reliability (in the absence of local infection and with adequate equipment).
Muscle relaxation.
Technical simplicity. ‟13,14”
The only expertise required is ability to cannulate the vein and a vigorous technique.
Extremely high (>95%) success rate, higher than any other block. (15)
1.1.4 Disadvantages of intravenous regional anesthesia are
• Not suitable for deep operations as analgesia is not sufficiently intense.
• Tips of fingers are often missed, an additional ring block may then be necessary.
• The tourniquet may become extremely uncomfortable and thus limit the duration of surgery
(using a second tourniquet together with the judicious use of adjuvant drugs may overcome
this problem).
• Surgical time is limited to about one hour due to the tourniquet which must not be released
during the procedure. <16)
• Poor postoperative analgesia.
• The potential of systemic local anesthetic toxicity.
• Nerve damage secondary to direct compression of the tourniquet.
• Compartment syndrome and loss of the limb (very rare).(l7)
• Tourniquet paralysis may result from: (a) excessive pressure (b) insufficient pressure
resulting in passive congestion of the part with hemorrhagic infiltration of the nerve (c)
keeping the tourniquet too long (d) application of the tourniquet without considering local
anatomy. <7)
Intravenous regional anesthesia is generally a safe technique, the most important
complication to be recognized is a leaking or accidentally deflated tourniquet cuff this will

www.wjpps.com Vol 8, Issue 7, 2019.
1598
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
result in large volume of local anesthetic being rapidly introduced in to the circulation. The
patient may develop dizziness, nausea, vomiting, tinnitus, perioral tingling, muscle twitching,
loss of consciousness and convulsions. Avoidable deaths have occurred.[IX]
1.1.5 Intravenous regional anesthesia is contraindicated in: Severe Raynaud‟s disease
(intermittent arteriolar spasm of the distal limbs after cold or emotional stimuli).; Sickle cell
disease (IVRA is relatively contraindicated, unless meticulous exsanguinations of the limb
takes place prior to cuff inflation). e Crush injury to the limb, [VRA may provoke further
tissue damage secondary to hypoxia. e Age: young children are generally not amen
combination with sedation and additional ana e Allergy to local anesthetic. Patient refusal. „!”
able to IVRA alone, however, in Igesia it can be used successfully.
1.1.6 Relative contraindications of intravenous regional anesthesia
Severe hypertensive or peripheral vascular disease.
Local infection.
Skeletal muscle disorders or Paget's disease (loc systemic circulation via venous channels
in bone In this study, intravenous regional anesthesia is performed by using three caine,
atracurium and dexamethasone. al anesthetic may spread to the (20)
1.1.7. lidocaine (Xylocaine): hydrochloride or lignocaine, the first modern amide local
ynthesized by Lofgren and Lunquist in 1943 and was clinically n (1-3 hours). for all sorts of
regional anesthetic blocks including intravenous dental anesthesia and therapeutic blockade
in concentrations 0t intended for blocks of long duration, e.g. via intermittent bolus
oductioneae Lidocaine has a membrane — stabilizing effects on both cardiac a at tissue, it is
used to control cardiac arrhythmia and to interrupt a status epilepticus, =H a lidocaine use in
anesthesia can be explained by the fact that it alters Cee Ob neurons by blocking the fast
voltage gated sodium channels in the cell mem Pra: With sufficient blockade, the membrane
of presynaptic neuron will not, depolanze and so fail to transmit an action potential leading to
its anesthetic effects. Lidocaine is hepatically metabolized and renally excreted with only
10% unmodified. The maximum safe dose is approximately 3-5 mg iz ee epinephrine), with
epinephrine 7 mg /kg to decrease the vascular uptake. ae Systemic exposure to excessive
quantities of lidocaine mainly result in central nervous system and cardiovascular system
adverse effects, central nervous effects occur at low concentration and additional
cardiovascular effects present at higher concentration, though cardiovascular collapse may

www.wjpps.com Vol 8, Issue 7, 2019.
1599
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
also occur with low concentration. Central nervous system effects may include central
nervous system excitation (nervousness, tingling around the mouth, tinnitus, dizziness,
blurred vision, seizure) followed by depression (drowsiness, loss of consciousness,
respiratory depression and apnea), cardiovascular effects include hypotension bradycardia,
arrhythmia and/ or cardiac arrest, some of which may be due to hypoxaemia secondary to
respiratory depression. 7°
1.1.7.2 Atracurium
A benzyl isoquinolonium ester. It is an intermediate acting relaxant which is dly broken-
down by the body. s makes atracurium very predictable as wears off rapidly compared with
laxants. °” lecular weight of 1243, pH solution 3.5 stored at 4 celisus in the drug deteriorates
at room temperature, it is a highly specific ae rzing muscle relaxant, which was designed to
undergo lown, °°! ovascular system; although atracurium produces few direct e absence of
vagal blocking activity makes the patient vulnerable ng anesthesia. Histamine release may
occur if atracurium is ipitated in the syringe or vein or injected immediately after : system;
bronchospasm can occasionally occur ease. °” Pies 5. Z; A „ ns gnificant and the drug is
widely used in obstetrics. °*).
Rohavin t Distribution, metabolism and excretion
Atracurium is broken-down to inactive metabolites by minor ester hydrolysis and
Spontaneous Hoffman degradation (major pathway) to laudanosine. This metabolite has been
shown to cause seizure in animal models (>17 mcg/ml). There is little change in its effects in
patients with renal or liver failure. When used for long operation, it is very predictable. ©”).
1.1.7.2.2 Dose, administration and use
A dose of 0.3-0.6 mg/kg will provide relaxation for 20-40 minutes supplemental doses should
be 5-10 mg. Atracurium precipitates in an alkaline pH and it should never be mixed with
thiopentone, always flush the vein with saline if using the two drugs at induction.
1.1.7.2.3 Factors that altered the response to atracurium
Neuromuscular blockade can be prolonged with: electrolyte disturbances, hypothermia,
myasthenia gravis, Eaten lamberts syndrome, respiratory acidosis, furosemide, phenytoin,
theophylline, carbamazepine, sepsis, major burns and __ peripheral neuropathies. __-__It
produces more rapid recovery that the older non depolarizing agents and easily 2versed 20-25
minutes after administration of a dose of 2x ED95 (0.45 mg /kg). g does not have any direct

www.wjpps.com Vol 8, Issue 7, 2019.
1600
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
cardiovascular effect, but may release histamine / 3 of that released by tubocurium) and
therefore produce a local wheal and 1 the injection site, especially if a small vein is used.
This may b y a slight fall in arterial pressure. ° roid similar to normal steroid hormone
produced by the adrenal -inflammatory, metabolic and immunosuppressant effects. It helps,
redness, itching and allergic reactions, so it treats severe allergies, hma, arthritis and other
conditions, decreases nausea and vomiting notherapy drugs, kills some types of cancer cells
and decreases injury or illness. °°?” bound to the plasma proteins and distributed via the
blood, it is and excreted by the kidneys.
It has many side effects: an allergic reaction, hypertension, sudden weight gain, insomnia,
nausea, vomiting, stomach upset, fatigue, dizziness, muscle weakness or joint pain, problems
with diabetes control or increased hunger or thirst, acne, increased hair growth, thinning of
the skin, cataract, glaucoma, moon face, change in behavior, hallucination and osteoporosis.
cy) A single large dose of this medication is unlikely t over dose is more likely to be caused
by a chronic over dose aperiod of time. °” o cause symptoms or death, an —large doses taken
over.
1.1.8 Tourniquets
er by the use of a tourniquet. The t that must be used with proper t is luxury, while in others
such Operations on the extremities are made easi tourniquet is a potentially dangerous
instrumen knowledge and care. In some procedures, a tourniquet as delicate operation on the
hand, it is a necessity. A pneumatic tourniquet is safer than an Esmarch tourniquet or the
Martin sheet rubber bandage. A pneumatic tourniquet with a hand pump and an accurate
pressure gauge is probably the safest, but a constantly regulated pressure tourniquet is quite
satisfactory if it is properly maintained and checked. When a sphygmomanometer cuff is
used, it should be wrapped with gauze alii bandage „According to Cren show et al., wide
tourniquet cuffs are none effective at lower sure than are narrow ones. demonstrated that
curved tourniquet on conical extremities require er arterial occlusion pressure than straight
(rectangular) tourniquet, sht tourniquet on conical thighs should be avoided specially in or
obese individuals. uets should be kept in good repair and all valves and gauges checked. The
Esmarch tourniquet is still in use some areas and it is cal of the elastic tourniquets. „”
1.2 Aim of the Study
The aim of the study is to improve the quality of the apeional aes ee a inimum toxic level of
local anesthetics by the pe pepoance Of tis by usin plain anesthesia (Bier‟s block) for surgical

www.wjpps.com Vol 8, Issue 7, 2019.
1601
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
procedures in the upper limb by) making lidocaine, lidocaine with additive
Simecicarnerigsgge, airacurium), comparison between these two groups with a group of plain
lidocaine.
PATIENTS AND METHODS
7 This study was performed at Teaching and Emergency hospitals in Sulaimani ty in period
from January 2007 to September 2007. It was approved by Sulaimani Ethical Committee.
Ninety patients of ASA I and Il, ages 18-65 years of either gender were included in this
study, All patients had been admitted for surgical procedures in the upper limb (hand, wrist
and forearm) which is lasting 60-90 minutes. e Adequately informed about the procedure and
have consented to it. e Patients with open wounds or crush injuries in the upper limb were
excluded from this study. e Patients were not premedicated and randomly allocated in to three
groups, thirty patients in each.
Forty five patients were an emergency cases, subjected to upper limb (hand ed; had full
stomach, they, forearm) trauma; they were unprepared, not premedicat were a good candidate
for intravenous regional anesthesia (Bier‟s block), after obtaining an informed consent that
includes understanding all the risks and benefits with considering the surgeon preference and
physiological and mental state of the_ patient, the procedure was performed for them.:
received 40 ml (3mg/kg) of 0.5% lidocaine solution. Surgical hand. of pain is done by simple
descriptive pain intensity scale which snts words (mild, moderate, severe) to describe their
degree of e perioperative analgesia was assessed and their need for rugs also evaluated.
2.1 The equipments required for intravenous regional anesthesia
Double tourniquet or reliable sphygmomanometer.
Esmarch bandage.
Local anesthetic solution.
Resuscitation equipment and drugs.
Before beginning to perform the block, the patient's blood pressure should be measured. en
inserted in a distal vein in the he hand), and another cannula which may require _ An
intravenous cannula or butterfly needle is th limb scheduled for surgery (e.g. in the dorsum of
t placed on the other hand for cases of any complications, occur, intravenous drug
administration.„ “After the limb is exsanguinated (blood removed) before tourniquet is

www.wjpps.com Vol 8, Issue 7, 2019.
1602
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
inflated, this is done by tightly wrapping the distal part of the limb with Esmarch rubber
bandage, before inflating the tourniquet, or elevation of the arm for 20-30 seconds whilst
applying firm digital pressure on the brachial artery, this will allows venous blood to drain
from the limb whilst preventing further arterial blood entering.*”
The tourniquet (cuff of the sphygmomanometer) is then inflated to a pressure 50 _mmHg or
more above the patient's systolic pressure. The local anesthetic solution is then injected
slowly into the cannula of the surgical hand and the patient warned that e limb may start to
feel hot and that the skin will take on a mottled appearance, Igesia rred within 3-4 minutes
and after that the surgery commenced. Even if mpleted within a few minutes, on no account
the tourniquet deflated) minutes has passed since the injection of the local anesthetic or ffects
may occur, the pressure in the tourniquet was constantly ained at least 50 mmHg above the
patient's systolic blood 1 expected to be prolong, that will lead to pain due to pressure cuff of
sphygmomanometer) this reduced by the use of a double 1e two tourniquets are placed on the
patient's arm, initially, the ne is applied and the local anesthetic agent injected when the the
distal (lower) tourniquet is placed and then the proximal d or loosed and normal ee sca a ae
procedure, the tourniquet is deflate Be of ured; es, the tourniquets is reinflated or tighten
again 20-30 seconds, ee of local anesthetic from the limb and hence the incidence of side
ased. In any event, the patient warned that they may experience tinnitus, flation of the
tourniquet.„*dizziness or transient drowsiness following de ES Monitoring of the patient is
done for the vital signs (heart rate, blood pressure _Tespiratory rate) and sings of
complications of drugs on cardiovascular, respiratory and central nervous systems. tients to
flex and extend the wrist Motor function was assessed by asking the pa‟ en no voluntary
movement was and fingers; complete motor block was noted wh possible. Sensory block was
assessed by a pinprick test performed with a needle every 30 seconds. e was evaluated in the
dermatomal sensory distribution of the and radial nerves. median, ction of the study drug
until Patient respons e was the time elapsed medial and lateral ante brachial coetaneous,
ulnar, Sensory block onset time was noted as the time from inje sensory block in all
dermatomes, and motor block onset tim: injection of the study drug to complete motor
block.°” aa1yuL 19}deyD
www.wjpps.com Vol 8, Issue 7, 2019.
1603
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
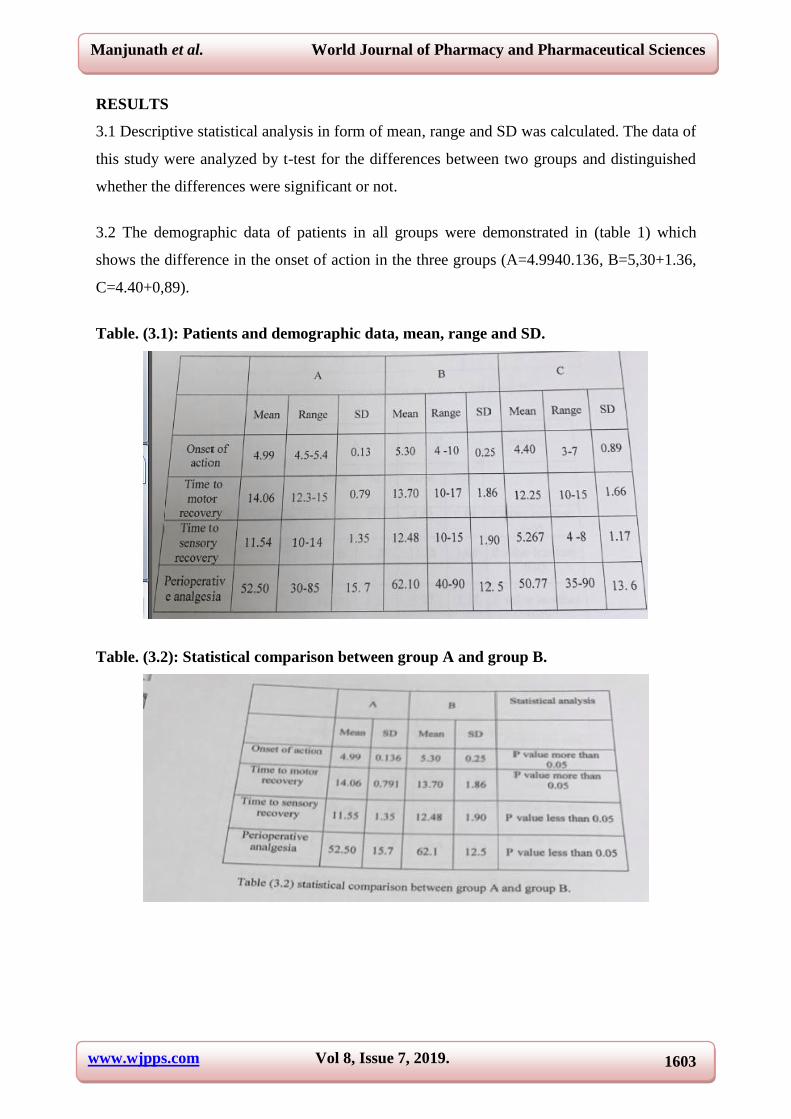
RESULTS
3.1 Descriptive statistical analysis in form of mean, range and SD was calculated. The data of
this study were analyzed by t-test for the differences between two groups and distinguished
whether the differences were significant or not.
3.2 The demographic data of patients in all groups were demonstrated in (table 1) which
shows the difference in the onset of action in the three groups (A=4.9940.136, B=5,30+1.36,
C=4.40+0,89).
Table. (3.1): Patients and demographic data, mean, range and SD.
Table. (3.2): Statistical comparison between group A and group B.

www.wjpps.com Vol 8, Issue 7, 2019.
1604
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table. (3.3): Statistical comparison between group A and group C.
Table (3.4): Statistical comparison between group B and group C.
The onset of action in group C (4.40+0.89) was faster than in group A id group B (5.30
+1.37), (p value less than 0.05).
Overy in group A showed no significant differences with (p value more than 0.05).
perioperative analgesia in group B is significantly 2.49) as compared with that of group A
(11.54+1.34, 05). The time of perioperative analgesia in group A and C was statistically not
The time taken for motor and sensory recovery with perioperative analgesia was ignific: antly
longer in group B (13.70+1.89, 12.48+1.90, 62.10+12.49) than in group 22: (12.25+1.66,
5.26+1.17, 50.77£13.59),(p value was less than 0.05).

www.wjpps.com Vol 8, Issue 7, 2019.
1605
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. (3.1): Onset of action.
Onset of action: time of complete motor and sensory block in minutes.
A: Plane lidocaine Group.
B: Lidocaine+dexamethasone group.
C: Lidocaine+atracurium group.
Fig. (3.4): Time to motor recovery.
Time to sensory recovery: the time from the release of tourniquet till the return of sensation
(duration of sensory block after the release of tourniquet) in minutes.
Fig. (3.3): Time to sensory recovery.

www.wjpps.com Vol 8, Issue 7, 2019.
1606
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. (3.4): Perioperative Analgesia.
Perioperative analgesia the block (the time from the injection of the drugs till the return of
sensatior) in minutes.
DISCUSSION
To avoid some of $ anesthesia. such as known impossible intubation, severe sephreig de ne
problems are expected. patients who specifically request regional anesthesia, situations where
general anesthesia is} not available (rare); to provide high quality postoperative pain relief; as
part of 7 postoperative multimodal rehabilitation programme to enable carly return to
function; intravenous regional anesthesia (Bier's block) is most commonly performed on the
upper extremity for forearm and hand surgery of up to 90 minutes in duration it is reliable
and safe and has a high degree of patient satisfaction “”
The potential complications of a Bier block include the risk of excessive, toxic doses of local
anesthetic reaching the systemic circulation with accidental deflation of the tourniquet “, this
risk ean be minimized by the following: The tourniquet should not be released until at least
20 minutes after injection: even if the surgery is completed, this delay allows for diffusion of
drug into the tissues, so that plasma concentrations do not reach toxic levels after release of
the tourniquet; slow deflation may also provide a safety margin, as the local anesthetic drug is
released into the circulation in a biphasic manner. there is initial fast release of 30%, but 50%
may still be present in the limb 30 minutes later. “'°** Using adjunct drugs to supplement the
local anesthetic to decrease the need of the top-up dose, so, minimizing the potential toxicity
improving the quality of analgesia and muscle relaxation perioperatively; also decrease the
need of intraoperatively sedation thus allow a constant communication with the patient is
essential to detect early symptoms of toxicity. he patients simple descriptive pain intensity
scale score was 1 discomfort despite the use of double tourniquet especially ich last more

www.wjpps.com Vol 8, Issue 7, 2019.
1607
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
than 40 minutes; 19 patients of them received am Smeg intravenously with monitoring of
their vital signs‟ complications noted in this group. d 40m lidocaine(0.5%) plus 8mg
dexamethasone I (side effects of this drug occur after a long- term doses are harmless while
short courses are well d with toxicity, “°*7) nsory recovery and perioperative analgesi 2 lan
0.05). i ™.
DISCUSSION
There was one case who developed hypotension after the release of tourniquet, and treated by
intravenous fluids then returned to normal level blood pressure after 10 minutes.; This study
make a comparison between the supplement of dexamethasone to lidocaine and the addition
of atracurium to lidocaine; with plane lidocaine. This study demonstrates that the addition of
(8 mg) dexamethasone to lidocaine makes the time to sensory recovery and perioperative
analgesia in group B (12.48 + 1,90, 62.1 + 12.5) is longer than in group A (plane lidocaine)
(11.55 + 1.35, 52.50 £15.7), (p value less than 0.05).
This study also demonstrates that the addition of (1 mg) of atracurium to lidocaine makes the
onset of action (complete motor and sensory block) in group C (4.40 + 0.89) is faster than in
group A (4.99 + 0.13) (p value is less than 0.05), while the time to motor recovery and
perioperative analgesia in group A (14.06 + 0.79, 52.50 + 15.7) is longer than in group C
(12.25 + 1.66, 50.8 + 13.6), (p value more than 0.05). tween group B and group C
(comparison between the that of atracurium on lidocaine in intravenous regional the onset of
action in group C (4.40 + 0.89) is). (p value is less than 0.05), while the time to memeroup C
(12.25 + 1.66, 5.27+ 1.17, 50.8.
CONCLUSIONS AND RECOMMENDATIONS
5.1 CONCLUSIONS
Th ae poe ae mg) dexamethasone to supplement the local anesthesia for will improve the
perioperative analgesia, prolong the sensory and motor i: mee 3 recovery time and reducing
the simple descriptive pain scale scoring. Thea ate Riceieeigne e a minimum dose of
atracurium (1 mg) to supplement the local or Bier's block speed the onset of complete motor
and sensory block and improve the muscle relaxation intraoperatively.
5. 2 RECOMMENDATIONS
• Itis advisable to perform the intravenous regional anesthesia Oe oer surgical procedures
of the upper limb to avoid some risks of genera fee ee Further studies are recommended

www.wjpps.com Vol 8, Issue 7, 2019.
1608
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
with other adjuvant to the local anesthe minimize the potential toxicity. ¢ More and
careful study is essential to evaluate the effects of gns petee a dexamethasone and
atracurium concurrently in the surgical hand to imp the quality of intravenous regional
anesthesia.
REFERENCES
1. Wallace A, Guardini R, Ellis S. Standard intravenous regional anesthesia, BMJ, 1982;
285: 654-6.
2. Colleen Ec. The Bier block for intravenous regional anesthesia, technical and literature
review. Anesthesia and analgesia, 1970; 49: 645-40.
3. Johnson CN. Intravenous regional, new approach to an.
4. W.F. Casey, consultant anesthetist, Gloncester Shine, World Federation Of Sociaties of
Anesthesiologist. Intravenous regional anethsia (Bier‟s block), 1992; 1: 1-2.
5. Gentili M Bonnet F, Bernard JM. Adding clonidine to lidocaine for intravenous regional
anesthesia prevent tourniquet pain. Anesthesia and analgesia, medline, 1999; 88: 1327-30.
6. F.Rodola, S.Vagnoni, S.Inglelti. An update on intravenous regional anesthesia of the arm.
European Review for medical and pharmacological sciences, 2003; 7: 131-138.
7. Glic Kman Lt, Mackinnon SE, Rao TV, Me Cabe SJ: J hand surgery 17-A: 83, 1992.
Campbell‟s Operative Orthopaedics, Wysiwyg://frame5.frame
0.2/http://,27.0.0.1:1080/ram:2002.
8. Haasio J, Hippala S, Rosenberg PH. Intravenous regional anesthesia of the arm.
Anesthesia, 1989; 44: 19-21.
9. Gordh T. Xylocaine-a new local anesthetic. Anesthesia, 1949; 4: 4-10.
10. Prithri Pr et al. The site of action of intravenous regional anesthesia. Anesthesia and
analgesia, current researches, vol.51, No5, Sept.-Oct. 1972-776-7786.
11. Esteb Jp, Le Naunre A, Chemaly L, Eccffey C.Tourniquet pain in a volunteer study.
Anesthesia, 2000; 55: 21-6.
12. Tuncal B, Karc A, Bacakoglu AK, et al. Controlled hypotension and minimal inflation
pressure, a new approach for pneumatic tourniquet application in upper limb surgery.
Anesthesia and analgesia, 2003; 97: 1529-32.
13. Cobb AG, Houghton GR. Local anesthetic infilteration versus Bier‟s block for colles
fractures. BMJ., 1985; 291: 1683-4.
14. Healy, E.J Cohen, P.J. Wylia and Churchill-Davidson‟s practice of anesthesia 6 ed. 1995
(160, 156, 157, 167).

www.wjpps.com Vol 8, Issue 7, 2019.
1609
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
15. Abdulla Wy, Fadhil NM. Anew approach to intravenous regional anesthesia, 1992; 75:
597-601.
16. B Nicolls J, Berrington and sonosite.Anesthesia and analgesia, 2005; 401: 297.
17. A Lan R.Aitkenhead. Text book of anesthesia 4th
ed., 2001; 229.
18. Valli H, Rosen berg pH, KyHa, Numinen M. Arterial hypertension associated with the
use of a tourniquet with either general or regional anesthesia. Acta Anesthesia Scand,
1987; 31: 299-83.
19. Heath ML. Death after intravenous regional anesthesia. BMJ., 1982; 285: 913-4.
20. John Oyston. Intravenous regional anesthesia. Anesthesia and analgesia, 2001; 7184-395.
21. Terry Dvolka. Intravenous regional anesthesia, New York School of anesthesia.
Anesthesia and analgesia, 2006; 102: 605-609.
22. Kari Harrison. What is lidocaine. Molecule of the month for June 2007.
23. Robert K. Stoelling. Pharmacology and physiology in anesthetic practice 2nd
ed. 1991:
208.
24. Corino B, Vasallo H. Local anesthetics mechanismof action and clinical use. Grunns and
Stralton. New York, 1976; 4-5.
25. Thomson PD, Melmon KL, Richardson JA et al. Lidocaine pharmacokinetics in advance
heart failure, liver diease and renal failure in human. Ann Inten Med., 1973; 78(4):
499-508, PMID.
26. Memis D, Turan A. Karamanhoglu et al. Adding dexmedetomidine to lidocaine for
intravenous regional anesthesia. Anesthesia and analgesia, 2004; 98: 835-40.
27. Faccenda KA, Finucaue BT. Complicatios of regional anesthesia, incidence and
prevention. Drug safety, 2001; 24: 413-42.
28. Tsui BCH, Wagner, Finucane B. Regional anesthesia in the Elderly. A clinical guide.
Drugs Aging, 2004; 21: 895-910.
29. Patrick Neligan. Local anesthetics. Source Mather Drugs, 1979; 18: 185-205.
30. McGlone R, Heyes, Harris P. Anesthesia and analgesia, 1988; 5(2): 79-85.
31. Elhakim M, Sadek RA. Addition of atracurium to lidocaine for intravenous regional
anesthesia. Acta Anesthesiol. Scand, 1994; 38: 54-4.
32. Vicker M.D, Morgan M, Spencer, P.S.J and Read M.S. Drugs in anesthetic and intensive
care practice 8th
ed. 1999-275.
33. Edward G, Morgan and Magid S., Mikali. Muscle relaxant in clinical anesthesia 2nd
1996:
160-164.

www.wjpps.com Vol 8, Issue 7, 2019.
1610
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
34. Playfor, S.D. Thomas A.D., Choonel. Duration of action of atracurium when given by
infusion to critically ill children, pediatric anesthesia, 2000 Jan; 10(1): 77-81.
35. Grallenstien, J.S. Paulus, DA. Neuromuscular function, clinical monitoring 2nd
ed.
Philadeliphia: Lippencott, 1987; 213-27.
36. Stenlake, J.B Waigh, R.B, Urwin J et al. Atracurium: conception and inception BJ.
Anesthesia, 1983; 55: 35-105.
37. Holtle K, Werner MU, lacouture PG, Kehlet H. Dexamethasone prolongs local analgesia
after subcutaneous infiteration of bupivacaine microcapsules in human volunteers.
Anesthesiology, 2002; 96: 1331-5.
38. Kopacz Dj, Lacouture PG, WuD et al. The dose response and effects of dexamethasone
on bupivacaine microcapsules for intercostal blockade (T9 to Til) in healthy volunteer.
Anesthesia and analgesia, 2003; 96: 576-82.
39. Castillo J, Curely J, Hotz J et al. Glucocorticoides, steroids prolongs rat sciatic nerve
blockade in vivo from bupivacainemicrospheres. Anesthesiol, 1996; 85: 1157-66.
40. Lee‟s synopsis of anesthesia, 13th
ed. Edited by N.J.H. Davis, N.J. Cashman, 2005; 4:
401-429.
41. A.R. Aitkenhead, G.Smith, text book of anesthesia 4th
ed. 2001; 43: 559.
42. Lorraine M. Sdrales, Ronald D.Miller, anesthesia review, 2001; 13: 194.
43. G.Edward Morgan, J., M.D., Maged S. Mikhail, M.D. Appleton and Lange, clinical
anesthesiology 2nd
ed. 2006; 17: 342.
44. James Duke, M.D., anesthesia secrets, 3rd
ed., 2006; 71: 451.
45. Lippincott‟s Illustrated reviews, 3rd
ed., 2006; 17: 342.
46. Padmaja Udaykumar, text book of medical pharmacology, 2004; 64: 406.
47. Johansson A, Hao J, Sjolund B. Local corticosteroid application blocks transmission in
normal nociceptive C-fibers. Acta Anesiol. Scand, 1990; 34: 335-8 PM1D.
48. Zekiye Bigat, Neval Boztug, Necmiye Hadimioglu, Nihan Cete, Nesil coskunfirat and
Ertugrul Ertok. Dose dexamethasone improve the quality of intravenous regional
anesthesia and analgesia. Anesth. and analgesia, 2006; 102(2): 605-9.
49. Movafeqh A, Razazia M, Hajimao hamadi F and Mey Sarnie A.Anesthesia and analgesia,
2006 Jan; 102(l): 263-7.
50. Kurt N, Kurt I, Aygunes B, oral H Tulunay M, Eur J. Anesthesiol, 2002 Jun; 19(7):
522-5.

www.wjpps.com Vol 8, Issue 7, 2019.
1611
Manjunath et al. World Journal of Pharmacy and Pharmaceutical Sciences
51. Turan A, Karaman Lyoglu B, Memis D, Kaya, Pamukcu Z. Intravenous regional
anesthesia using prilocaine and neostigmine. Anesthesia and analgesia, 2002; 95:
1419-1422.


















