A Clinical Guide to Orthodontics - J. Sandy (2004) WW
77
BRITISH DENTAL JOURNAL VOLUME 195 NO. 8 OCTOBER 25 2003 433 PRACTICE Orthodontics. Part 1: Who needs orthodontics? D. Roberts-Harry 1 and J. Sandy 2 There are various reasons for offering patients orthodontic treatment. Some of these include improved aesthetics, occlusal function and the long-term dental health. 1* Consultant Orthodontist, Orthodontic Department, Leeds Dental Institute, Clarendon Way, Leeds LS2 9LU; 2 Professor in Orthodontics, Division of Child Dental Health, University of Bristol Dental School, Lower Maudlin Street, Bristol BS1 2LY *Correspondence to: D. Roberts-Harry E-mail: [email protected] Refereed Paper doi:10.1038/sj.bdj.4810592 © British Dental Journal 2003; 195: 433–437 ● This series of articles is designed to aid in the orthodontic evaluation of patients ● Not every malocclusion needs orthodontic treatment ● Not every patient is suitable for treatment ● Understanding the treatment benefit for the patient is important ● GDPs have an important role to play in assessing the need for orthodontic treatment IN BRIEF Orthodontics comes from the Greek words ‘orthos’ meaning normal, correct, or straight and ‘dontos’ meaning teeth. Orthodontics is concerned with correcting or improving the position of teeth and correcting any malocclu- sion. What then do we mean by occlusion and malocclusion? Surprisingly the answer is not straightforward. There have been various attempts to describe occlusion using terms such as ideal, anatomic (based on tooth morpholo- gy), average, aesthetic, adequate, normally functioning and occlusion unlikely to impair dental health. With these different definitions of what con- stitutes malocclusion, there is, not surprisingly a degree of confusion as to what should be treated and what should not. Although some tooth posi- tions can produce tooth and soft tissue trauma, it is important to remember that malocclusion is not a disease but simply a variation in the nor- mal position of teeth. Essentially, there are three principal reasons for carrying out orthodontic treatment: 1. To improve dento facial appearance 2. To correct the occlusal function of the teeth 1 ORTHODONTICS 1. Who needs orthodontics? 2. Patient assessment and examination I 3. Patient assessment and examination II 4. Treatment planning 5. Appliance choices 6. Risks in orthodontic treatment 7. Fact and fantasy in orthodontics 8. Extractions in orthodontics 9. Anchorage control and distal movement 10. Impacted teeth 11. Orthodontic tooth movement 12. Combined orthodontic treatment Fig. 1a A child with a Class II division 1 malocclusion and very poor aesthetic appearance Fig. 1b The same child as in Fig. 1a ➠ ➠ VERIFIABLE CPD PAPER
Transcript of A Clinical Guide to Orthodontics - J. Sandy (2004) WW

BRITISH DENTAL JOURNAL VOLUME 195 NO. 8 OCTOBER 25 2003 433
PRACTICE
Orthodontics. Part 1: Who needs orthodontics?D. Roberts-Harry1 and J. Sandy2
There are various reasons for offering patients orthodontic treatment. Some of these includeimproved aesthetics, occlusal function and the long-term dental health.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professorin Orthodontics, Division of Child DentalHealth, University of Bristol Dental School,Lower Maudlin Street, Bristol BS1 2LY*Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4810592© British Dental Journal 2003; 195:433–437
● This series of articles is designed to aid in the orthodontic evaluation of patients● Not every malocclusion needs orthodontic treatment● Not every patient is suitable for treatment● Understanding the treatment benefit for the patient is important● GDPs have an important role to play in assessing the need for orthodontic treatment
I N B R I E F
Orthodontics comes from the Greek words‘orthos’ meaning normal, correct, or straightand ‘dontos’ meaning teeth. Orthodontics isconcerned with correcting or improving theposition of teeth and correcting any malocclu-sion. What then do we mean by occlusion andmalocclusion? Surprisingly the answer is notstraightforward. There have been variousattempts to describe occlusion using terms suchas ideal, anatomic (based on tooth morpholo-gy), average, aesthetic, adequate, normallyfunctioning and occlusion unlikely to impairdental health.
With these different definitions of what con-stitutes malocclusion, there is, not surprisingly adegree of confusion as to what should be treatedand what should not. Although some tooth posi-tions can produce tooth and soft tissue trauma, itis important to remember that malocclusion isnot a disease but simply a variation in the nor-mal position of teeth. Essentially, there are threeprincipal reasons for carrying out orthodontictreatment:
1. To improve dento facial appearance2. To correct the occlusal function of the teeth
1
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
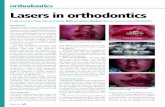
Fig. 1a A child with a Class IIdivision 1 malocclusion andvery poor aesthetic appearance
Fig. 1b The same child asin Fig. 1a
➠
➠
VERIFIABLECPD PAPER

PRACTICE
434 BRITISH DENTAL JOURNAL VOLUME 195 NO. 8 OCTOBER 25 2003
3. To eliminate occlusion that could damage thelong-term health of the teeth and periodontium
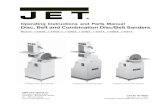
DENTO FACIAL APPEARANCEImproving the appearance of the teeth is withoutquestion the main reason why most orthodontictreatment is undertaken. Although it might betempting to dismiss this as a trivial need, there islittle doubt that a poor dental appearance canhave a profound psychosocial effect on children.Figure 1 illustrates such a case with a child whohas a substantial aesthetic need for treatment.The case is shown before (Fig. 1a, b) and after(Fig 2a, b) orthodontic treatment. Few wouldquestion that there has been an improvement inboth the dental and facial appearance of thischild. Indeed, orthodontic treatment can have abeneficial psychosocial effect. For exampleShaw et al.1 found that children were teasedmore about their teeth than anything else, suchas the clothes they wear or their weight andheight (Table 1).
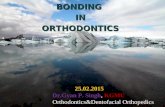
OCCLUSAL FUNCTIONTeeth, which do not occlude properly, can makeeating difficult and may predispose to temporo-mandibular joint (TMJ) dysfunction. However,the association with TMJ dysfunction and mal-occlusion is a controversial subject and will bediscussed in more detail in a later section. Indi-viduals who have poor occlusion, such as shownin Figure 3, may find it difficult and embarrass-ing to eat because they cannot bite through foodusing their incisors. They can only chew foodusing their posterior teeth.
DENTAL HEALTH Surprisingly there is no strong associationbetween dental irregularity and dental caries orperiodontal disease. It seems that dietary factorsare much more important than the alignment ofthe teeth in the aetiology of caries. Althoughstraight teeth may be easier to clean thancrooked ones, patient motivation and dental
Table 1 Features children most dislike or are teasedabout (Shaw et al.1)
Feature Disliked appearance or teased (%)
Teeth 60.7
Clothes 53.8
Ears 51.7
Weight 41.5
Brace 33.3
Nose 29.3
Height 25.3
Fig. 2a Same child as in Fig. 1 after orthodontictreatment
Fig. 2b Occlusion of the samepatient as in Fig. 2a, there hasbeen a significantimprovement in the buccalsegment relation and overjetcompared with the initialpresentation in Fig. 1b
➠
➠
Fig. 3 This patienthas a severeanterior open bitewith contact onlyon the molars
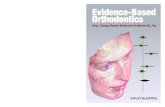
Fig. 4 Class IIDivision 1 with anincreased overjet.The anterior teethare at risk ofpotential traumawith an overjet of10 mm or greater

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 195 NO. 8 OCTOBER 25 2003 435
hygiene seems to be the overriding factor in pre-venting gingivitis and periodontitis. That said,few of the studies that have investigated the linkbetween crowding and periodontal disease havebeen longitudinal, over a long term and includedolder adults. It would appear that aligned teethconfer no benefit to those who clean their teethwell because they can keep their teeth cleanregardless of any irregularity. Similarly, align-ment will not help bad brushers. If there is poortooth brushing, periodontal diseases will devel-op no matter how straight the teeth are. Howev-er, having straight teeth may help moderatebrushers, although there is no firm evidence tosupport or refute this statement. This is an areathat requires further study.
Some malocclusions may damage both theteeth and soft tissues if they are left untreated. It iswell known that the more prominent the upperincisors are the more prone they are to trauma2,3
(Table 2). When the overjet is 9 mm or more the risk of
damaging the upper incisors increases to over40%. Reducing a large overjet is not only bene-ficial from an aesthetic point of view but min-imises the risk of trauma and long-term com-plications to the dentition. Fig. 4 shows a childwith a large overjet and it is not difficult toimagine the likely dental trauma that wouldresult if he or she fell over.
Certain other occlusal relationships are alsoliable to cause long-term problems. Figure 5aand b show a case where there is an anteriorcross-bite with an associated mandibular dis-placement in a 60-year-old man. The constantattrition of the lower incisors against the upperwhen the patient bites together, have producedsome substantial wear. If allowed to continuethen the long-term prognosis for these teeth isextremely poor. In order to preserve the teeth,the patient accepted fixed appliance treatmentthat eliminated the cross bite and helped preventfurther wear Figure 5c and d.
Another example of problems caused by ananterior cross bite is shown in Figure 6. A trau-matic anterior occlusion produced a displacingforce on the lower incisors with apical migrationof the gingival attachment as a consequence. Pro-vided this situation is remedied early (Fig. 7) thesoft tissue damage stops and as the rest of thegingivae matures the situation often resolves
Table 2 Relation between size of overjet andprevalence of traumatised anterior teeth
Overjet (mm) Incidence %
5 22
9 24
> 9 44
Fig. 5a Anterior crossbite in a 60-year-old man occludingin the intercuspal position
Fig. 5b Shows the retruded contact position of the patient.To reach full intercuspation the mandible displaces forwardand this movement is probably associated with the wear onthe incisors
Fig. 5c The patient in fixed appliances in order to correct the displacement and the position of his upperanterior teeth
Fig. 5d After correction and space reorganisation the patientis wearing a prosthesis to replace the missing lateral incisors

PRACTICE
436 BRITISH DENTAL JOURNAL VOLUME 195 NO. 8 OCTOBER 25 2003
spontaneously and no long-term problems usu-ally develop.
Deep overbites can occasionally cause strip-ping of the soft tissues as shown in Figure 8aand b. This is a case where there is little aes-thetic need for treatment but because of thedeep overbite there is substantial damage tothe soft tissues. Clearly if this is allowed tocontinue there is a risk of early loss of thelower incisors that would produce a difficultrestorative problem.
WHO SHOULD BE TREATED?Dental irregularity alone is not an indication fortreatment. Most orthodontic treatment is carriedout for aesthetic reasons and the benefit an indi-
vidual will receive from this will depend on theseverity of the presenting malocclusion as well asthe patients own perception of the problem.Some individuals can have a marked degree ofdento-facial deformity and be unconcerned withtheir appearance. Although a practitioner maysuggest treatment for such an individual,patients should not be talked into treatment andmust be left to make the final decision them-selves. Mild malocclusions should be treated withcaution. Not only will the net improvement in theappearance of the teeth be small, but also asnearly all teeth move to some degree after ortho-dontic treatment the risk of relapse in these casesis high. Whilst minor movements after the cor-rection of severe malocclusions will still producea substantial net overall improvement for thepatients, the same is not true of minor problems.Many practitioners will have encountered theparent who can spot a 5-degree rotation of anupper lateral incisor from fifty metres and is con-vinced this will be the social death of their child.Regardless of how insistent the parent or child is,the practitioner should approach such problems
Fig. 6 A traumaticanterior occlusionis displacing thelower right centralincisor labially andthere is anassociateddehiscence
Fig. 7 The samepatient as in Fig. 6,but the cross bitehas been correctedwith a removableappliance andthere has been an improvement in the gingivalcondition
Fig. 8a This malocclusion has an extremely deep bite whichcan be associated with potential periodontal problems
Fig. 8b The same patient as in Fig. 8a, but not inocclusion. The deep bite has resulted in labial strippingof the periodontium on the lower right central incisor
Table 3 Index of Treatment NeedDental health component Treatment need
1 No need
2 Little need
3 Moderate need
4 Great need
5 Very great need
Aesthetic component Treatment need
1
2 Little need
3
4
5
6 Moderate need
7
8
9 Great need
10

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 195 NO. 8 OCTOBER 25 2003 437
with care and only carry out the treatment if it is inthe best interests of the patient. It is essential thatthe patient and parent are fully aware of the limi-tations of treatment and that long term, ie perma-nent retention is currently the only way to ensurelong-term alignment of the teeth.
In order to assess the need for orthodontictreatment, various indices have been developed.The one used most commonly in the United King-dom is the Index of Orthodontic Treatment Need(IOTN).4 This index attempts to rank malocclu-sion, in order, from worst to best. It comprises twoparts, an aesthetic component and a dental healthcomponent (Table 3). The aesthetic componentconsists of a series of ten photographs rangingfrom most to least attractive. The idea is to matchthe patient’s malocclusion as closely as possiblewith one of the photographs. It is unlikely that aperfect match will be found but the practitionershould use his or her best guess to match to thenearest equivalent photograph. The dental healthcomponent consists of a series of occlusal traitsthat could affect the long-term dental health ofthe teeth. Various features are graded from 1–5(least severe — worst). The worst feature of thepresenting malocclusion is matched to the list andgiven the appropriate score.
Many hospital orthodontic services will notaccept patients in categories 1–3 of the dentalhealth component or grade 6 or less of the aes-thetic component of the IOTN unless they are suit-able for undergraduate teaching purposes.
Whilst the IOTN is a useful guide in prioritisingtreatment and determining treatment need it
takes no account of the degree of treatment diffi-culty. For example, class II division 2 malocclu-sions are notoriously difficult to treat yet theymight have a low IOTN. Figure 9 illustrates such acase. The IOTN of this patient is only 2 but it is adifficult case to manage and treatment requires a high level of expertise.
1. Shaw W C, Meek S C, Jones D S. Nicknames, teasing,harassment and the salience of dental features among schoolchildren. Br J Orthod 1980; 7: 75-80.
2. Office of Population Censuses and Surveys (1994). Children’sdental health in the United Kingdom 1993. London: HMSO0116916079.
3. Office of Population Censuses and Surveys (1985). Children’sdental health in the United Kingdom 1983. London: HMSO0116911360.
4. Brook P, Shaw W C. The development of an index oforthodontic treatment priority. Eur J Orthod 1989; 11: 309-320.
Fig. 9 The Index ofTreatment Needfor this patient is 2. Although thisis low, the level ofexpertise requiredto treat it is high
BDA Information Centre Services
Did you know?
• As a BDA member you can gainaccess to one of the best dental infor-mation services in the world
• You don’t have to be based in Londonto use the service
• You can borrow books, videos andinformation packages
• You can borrow up to eight items viathe postal systemThe only cost to you is the cost of thereturn postage. If you’re not surewhat to request then telephone us andwe can advise you.
• You are entitled to free MEDLINE searchesTelephone us with a subject and wewill send you a list of relevant refer-ences with abstracts.
• You can request photocopies of journalarticles
There is a small charge for this serviceand you need to fill in a PhotocopyRequest Form first. Telephone us ifyou would like one of these forms.
• BDA Members can view the latestCurrent Dental Titles on our web sitefree of charge.These are Medline-based lists of refer-ences on eight areas of dentistry whichare available to BDA members only onthe web site and which are updatedtwice yearly. Just use your passwordwith which you have been issued.
For further details of any of these servicesdial 020 7563 4545.
Contact us via e-mail at:[email protected]
Visit the Information Centre webpages at:
http://www.bda.org

BRITISH DENTAL JOURNAL VOLUME 195 NO. 9 NOVEMBER 8 2003 489
PRACTICE
Orthodontics. Part 2: Patient assessment andexamination ID. Roberts-Harry1 and J. Sandy2
The patient assessment forms the essential basis of orthodontic treatment. This is dividedinto an extra-oral and intra-oral examination. The extra-oral examination is carried out firstas this can fundamentally influence the treatment options. The skeletal pattern, soft tissueform and the presence or absence of habits must all be taken into account.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professorin Orthodontics, Division of Child DentalHealth, University of Bristol Dental School,Lower Maudlin Street, Bristol BS1 2LY*Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4810659© British Dental Journal 2003; 195:489–493
● Careful patient assessment is the most important part of treatment● The extra-oral examination is conducted first● The skeletal relationship must be assessed three-dimensionally● The teeth lie in a position of soft tissue balance● Habits such as thumb sucking can induce a malocclusion● There is no proven association between TMJ dysfunction and orthodontics
I N B R I E F
The most important part of orthodontic treat-ment is the patient assessment. Once a particu-lar treatment strategy is started subsequentchanges are often difficult. If it is decided thatextractions are needed and since the process isirreversible, they must be carefully consideredin the treatment planning process. Inappropri-ate orthodontic treatment can produce adverseresults and it is essential that full examinationof skeletal form, soft tissue relationships andocclusal features are performed prior to under-taking treatment. It is sensible to carry out theassessment in a logical order so that none of thesteps are missed. A simple assessment shouldinclude the following:
• Medical history• Patient’s complaint• Extra-oral examination• Intra-oral examination• Radiographs• Orthodontic indices• Justification for treatment• Treatment aims• Treatment plan
This section concentrates on the extra- andintra-oral examination of the patient.
EXTRA-ORAL EXAMINATIONIt is helpful to follow the examination sequenceoutlined:
• Skeletal pattern• Soft tissues• Temporomandibular joint examination
Skeletal patternPatients are three-dimensional and therefore theskeletal pattern must be assessed in anterior-posterior (A-P), vertical and transverse relation-ships. Although the soft tissues can tip thecrowns of the teeth the skeletal pattern funda-mentally determines their apical root position.The relative size of the mandible and maxilla toeach other will determine the skeletal pattern.The smaller the mandible or the larger the maxil-la the more the patient will be Class II. Converse-ly with a bigger mandible or smaller maxilla thepatient will be more Class III. The bigger the sizediscrepancy between the maxilla and mandible,the more difficult treatment becomes and theless likely it is that orthodontics alone will beable to correct the malocclusion. Although someorthodontic appliances have a small orthopaediceffect, treatment is generally most easily accom-plished on patients with a normal skeletal pat-tern and a normal relationship of the maxilla tothe mandible.
Anterior-posterior (AP)Although precise skeletal relationships can bedetermined using a lateral cephalostat radi-ograph, many practices do not have this facilityand it is important to be able to assess the skele-tal relationships clinically.
To assess the AP skeletal pattern the patienthas to be postured carefully with the head in aneutral horizontal position (Frankfort Plane hor-izontal to the floor). Different head postures canmask the true relationship. If the head is tippedback the chin tends to come further forward andmakes the patient appear to be more Class III.
2
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
VERIFIABLECPD PAPER

PRACTICE
490 BRITISH DENTAL JOURNAL VOLUME 195 NO. 9 NOVEMBER 8 2003
Conversely, if the head is tipped down the chinmoves back and the patient appears to be moreClass II. Sit the patient upright in the dentalchair and ask them to occlude gently on theirposterior teeth. Ask them to gaze at a distantpoint; this will usually bring them into a fairlyneutral horizontal head position. Look at thepatient in profile and identify the most con-cave points on the soft tissue profile of theupper and lower lips (Fig. 1).
The point on the upper lip is called soft tis-sue A point and on the lower lip soft tissue Bpoint. In a patient with a class I skeletal patternB point is situated approximately 1 mm behindA point. The further back B point is, the morethe pattern is skeletal II and the more anterior,the more skeletal III it becomes. Figure 2 showsa patient with a skeletal III pattern where theoutline of the hard tissues has been superim-posed on the photograph. This demonstratesthat although we are examining the soft tissueoutline this also gives an indication of the
underlying skeletal pattern. Obviously the softtissue thickness may vary and mask the A–Pskeletal pattern to some degree but generallythe thickness of the upper and lower lips is sim-ilar. The underlying skeletal pattern is thereforeoften reflected in the soft tissue pattern. Themore severe the skeletal pattern is the more dif-ficult treatment of the resulting malocclusionbecomes. Figure 3a and b, shows an adult withan obvious skeletal III pattern and a malocclu-
Fig. 3a Profile of anadult who has anobvious skeletal IIIpattern
Fig. 2 Shows a patient with a skeletal III patternwhere a tracing of the lateral cephalostatradiograph has been superimposed on thephotograph. The soft tissue masks to someextent a significant skeletal III pattern
Fig. 3b Malocclusions of the samepatient in Figure 3a. The patienthas a Class III malocclusion which is beyond the scope oforthodontics alone
➠ ➠
�A
BFig. 1 A tracing of a lateral cephalostatradiograph identifying softtissue points A and B

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 195 NO. 9 NOVEMBER 8 2003 491
sion that is clearly beyond the scope of ortho-dontic treatment alone.
Vertical dimensionThis dimension gives some indication of thedegree of overbite. The vertical dimension isusually measured in terms of facial height andthe shorter the anterior facial height the morelikely it is that the patient will have a deep over-bite. Conversely the longer the facial height themore the patient is likely to have an anterioropen bite. Deep overbites associated with a shortanterior facial height and open bites with longface heights are difficult to correct with ortho-dontics alone. The greater the skeletal differencethe more likely it is that the patient will need acombination of orthodontics and orthognathicsurgery to correct the occlusion and the underly-ing skeletal discrepancy.
There are various ways of measuring thevertical dimension, one of the most common isto measure the Frankfort Mandibular PlanesAngle. This is not a very easy clinical angle tomeasure and the problem is compounded bythe fact that not many clinicians can identifythe Frankfort Plane correctly. A more practicalway of assessing this is simply to measure thevertical dimension as indicated in Figure 4.
The lower anterior facial height is the dis-tance from the base of the chin to the base ofthe nose. The upper anterior facial height isthe distance from the base of the nose to apoint roughly between the eyebrows. Thesedimensions can be measured with a ruleralthough the index finger and thumb will doalmost as well. The lower and upper facialheights are usually equal. If the lower anteriorfacial height is reduced, as illustrated in Fig-ure 5, this can result in a deep overbite thatcan be difficult to correct (Fig. 6). Conversely,if the lower anterior facial height is greater
than 50% this can produce an anterior open-bite (Fig. 7).
Transverse dimensionTo assess this dimension, look at the patienthead-on and assess whether there is any asym-
50%
50%
Fig. 4 Assessment offacial proportions.The upper andlower anterior face heightsshould beapproximatelyequal
Fig. 5 Profile of apatient with amuch reducedlower anteriorfacial height
Fig. 6 Occlusion of the patientshown in Figure 5. The reducedlower anterior face height isoften associated with a deepbite as shown
➠ ➠
Fig. 7 Anterioropen bites areoften associatedwith an increase inlower anterior faceheight

PRACTICE
492 BRITISH DENTAL JOURNAL VOLUME 195 NO. 9 NOVEMBER 8 2003
metry in the facial mid-line. If there appears tobe any mandibular asymmetry this may bereflected in the position of the teeth as shownin Fig. 8. If there is asymmetry it is importantto distinguish between false and true asymme-try. A false asymmetry arises when occlusalinterferences force the patient to displace themandible laterally producing a cross-bite inthe anterior or buccal region. If the displace-ment is eliminated then the mandible willreturn to a centric position. A true asymmetryarises as a consequence of unequal facialgrowth on the left or right side of the jaws. Inthese cases elimination of any occlusal cross-bites (which can be very difficult) is unlikely toimprove the facial asymmetry.
SOFT TISSUE EXAMINATIONThe soft tissues comprise the lips, cheeks andtongue and these guide the crowns of the teethinto position as they erupt. Ultimately, the teethwill lie in a position of soft tissue balancebetween the tongue on one side and the lips andcheeks on the other (Fig. 9).
In patients with a Class I incisor relation-ship the soft tissues rarely play an importantpart unless there is an anterior open-bite. Theanterior open-bite may be caused by a digitsucking habit, a large lower anterior facialheight, localised failure of eruption of theteeth, proclination of the incisors or to anendogenous tongue thrust. The latter cause isvery rare and is usually identified by a largethrusting tongue that seems to permanently sitbetween the upper and lower incisors. Thistype of anterior open-bite is extremely diffi-cult to correct. It is usually possible to reduceit, but on completion of treatment the tongueinvariably pushes between the teeth and theymove apart once again.
An important aspect of lip position is seenin patients with an increased overjet. If theupper incisor prominence is reduced, stabilityusually depends on the lower lip covering theupper incisors in order to prevent the overjetincreasing post-treatment. Therefore, carefulexamination of the position of the lower lip inrelation to the upper incisors is important. Ifthe lower lip does not cover the upper incisorssufficiently after treatment, relapse of theoverjet may occur. Similarly, if the overjet isto be reduced, full reduction is very importantin order to give the lip the best possiblechance of stabilising the incisors. Figure 10illustrates the point; partial reduction of theoverjet does not allow the lip to cover theupper incisors and they are likely to return totheir pre-treatment position.
Whilst many young children have incompe-tent lips, this is often just a normal stage ofdevelopment. As they pass through puberty, thelip length increases relative to the size of the faceand the degree of lip competence graduallyimproves (Fig. 11).1
Lip incompetence can be caused by either alack of lip tissue or an adverse skeletal pattern. If
Fig. 8 A centre lineshift where thelower centre line isto the left
Fig. 9 Teeth are in soft tissue balancebetween the tongue andthe lips
Fig. 10 These diagrams show how partial reduction of the overjet does not allow thelip to cover the upper incisors. The upper incisors are then quite likely to return totheir pre-treatment position

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 195 NO. 9 NOVEMBER 8 2003 493
the skeletal pattern is unfavourable in either thevertical or anterior-posterior position then evenwith normal lip length the soft tissues are stillwidely separated.
HABITSDigit sucking is a well-known factor in pro-ducing anterior open-bite, proclined upperincisors and buccal cross-bites. If the habitceases while the child is still growing then theincisors are very likely to return to their nor-mal position. However, once the teenage yearsare passed and facial growth slows down,spontaneous resolution becomes increasinglyunlikely. If the habit persists into adult life itmay be necessary to use appliance treatment tocorrect the habit induced anterior open-bite.Buccal cross-bite possibly produced by digitsucking habits, rarely resolve spontaneouslyon cessation of the habit because of occlusalinterferences. These buccal cross-bites often
need to be corrected with active appliancetreatment.
TEMPORO-MANDIBULAR JOINT PROBLEMSA comprehensive review of the literature byLuther2,3 failed to demonstrate any conclusiveassociation between TMJ dysfunction, maloc-clusion and orthodontic treatment. However, itis important that the joints are palpated andassessed for signs and symptoms of TMJ dys-function. Patients who present with TMJ painseeking an orthodontic solution to correct theproblems should be treated with caution.
1. Vig P S, Cohen A M. Vertical growth of the lips: a serialcephalometric study. Am J Orthod 1979; 75: 405-415.
2. Luther F. Orthodontics and the tempromandibular joint:where are we now? Part 1. Orthodontic treatment andtemporomandibular disorders. Angle Orthod 1998; 68:305-318.
3. Luther F. Orthodontics and the temporomandibular joint:where are we now? Part 2. Functional occlusion,malocclusion, and TMD. Angle Orthod 1998; 68: 305-318.
5
50-5
0
10 15 20
Age (years)
Overlap (mm)
Fig. 11 Lip length is thought to increase as children pass through the pubertal growthspurt. This will aid retention of overjet reduction

BRITISH DENTAL JOURNAL VOLUME 195 NO. 10 NOVEMBER 22 2003 563
PRACTICE
Orthodontics. Part 3: Patient assessment andexamination IID. Roberts-Harry1 and J. Sandy2
The intra-oral assessment examines the oral health, individual tooth positions and inter-occlusal relationships. When this has been completed in conjunction with theextra-oral examination, a treatment plan can then be formulated.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professorin Orthodontics, Division of Child DentalHealth, University of Bristol Dental School,Lower Maudlin Street, Bristol BS1 2LY*Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4810724© British Dental Journal 2003; 195:563–565
● Careful patient assessment is the most important part of treatment● The intra-oral examination is conducted after the extra-oral assessment● The degree of occlusal discrepancy influences the treatment options● The dental health and patient motivation determine if appliance therapy can be used
I N B R I E F
INTRA-ORAL EXAMINATIONThere are various systems available to assess thisaspect but the following sequence is both practi-cal and thorough:
• Dental health• Lower arch• Upper arch• Teeth in occlusion• Radiographs
Dental healthEven individuals with severe malocclusionsshould not have active orthodontic treatment inthe presence of dental disease. Orthodonticappliances accumulate plaque and if the patienthas a poor diet and tooth brushing then irre-versible damage can result as demonstrated inFigure 1. Although the patient has straight teeththere is considerable decalcification and it couldbe argued is worse off as a consequence of treat-ment. Clearly this could have serious medico-legal complications, particularly if the clinicianfails to write in the notes that appropriate dentalhealth advice has been given
Decalcification around orthodontic appliancesis a recognised hazard and will occur in the pres-ence of poor oral hygiene and a cariogenic diet.Not only will decalcification occur around thebrackets but tooth movement in the presence ofactive gingivitis or periodontal disease willaccelerate any bone loss. Attempting to moveteeth in the presence of active dental disease canhave disastrous consequences and must beavoided.
Therefore, treatment for patients with ques-
tionable dental health should be confined toextractions and spontaneous alignment of theteeth only. Figure 2 illustrates a case where thereis an obvious need for orthodontic treatment butthis was precluded by the patient's extremelypoor oral hygiene.
Minor apical root resorption is a commonconsequence of orthodontic tooth movement.However, this resorption can occasionally besevere. Tooth movement in the presence of api-cal pathology is known to accelerate resorptionand should be dealt with prior to commencingtreatment.
Lower archThe lower arch should be examined and plannedin the first instance. Whatever treatment is car-ried out in the lower arch often determines thetreatment to be carried out in the upper. Examinethe teeth for any tipping, rotations and crowd-ing. Teeth which are tipped mesially are muchmore amenable to treatment, both with remov-able and fixed appliances than teeth which aredistally tipped. They also respond much better toextractions and spontaneous alignment thanother teeth. The presence or absence of rotationsis important because rotated teeth are most easilytreated with fixed appliances. The more crowdedthe teeth are the more likely it is that extractionswill be needed in order to correct the malocclu-sion. A method of assessing crowding is given inFigure 3. Firstly, measure the size of the teethand add these together (length A). Then measurefrom the mid-line to the distal of the canine witha pair of dividers. Measure from the distal of thecanine to the mesial of the first permanent
3
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
VERIFIABLECPD PAPER

PRACTICE
564 BRITISH DENTAL JOURNAL VOLUME 195 NO. 10 NOVEMBER 22 2003
molar. Add these together to give you theapproximate arch length (length B). Subtract Bfrom A to give you the degree of crowding. Thismust be repeated for both sides of the arch.
The degree of crowing influences the need forextractions. Although one should not be dog-matic and several other factors influence theplanning of extractions, as a general rule thegreater the crowding the more likely extractionsare necessary. Table 1 gives an outline of therelation between degree of crowding and needfor extractions.
Upper archThis is examined in a similar way to the lowerarch. Additional points to note in the mixed den-tition are the presence of a mid-line diastemaand the position of the upper canines.
A mid-line diastema is commonly seen in themixed dentition. The aetiological factors to beconsidered are:
• Normal (physiological) development• Fraenum• Small teeth• Missing teeth• Midline supernumerary
Physiologic spacing usually disappears as theocclusion matures, especially when the upperpermanent canines erupt and no treatment apartfrom observation is needed. Fraenectomies arerarely indicated and generally do not need to beremoved unless the fraenum is particularly largeand fleshy.
The upper permanent canine should be pal-pable in the buccal sulcus by 10 years of age. If not, and the deciduous canine is firm, parallaxradiography should be undertaken to determinewhere the permanent tooth is. If the tooth ispalatally positioned then the deciduous canineson both sides should be removed. This will helpguide the permanent tooth into a morefavourable path of eruption and prevent anycentre line shift caused by a unilateral deciduousextraction. It is essential that this palpation becarried out on all patients in this age group. Veryoften impacting canines are missed and thepatient not referred for treatment until 15 or 16years of age. Not only is this negligent, but thepatient may then need to undergo a lengthycourse of treatment at a socially difficult time.
Teeth in occlusionThe overjet and overbite should be measuredand the incisor classification assessed. TheBritish Standards Institute (BS EN21942 Part 1(1992) Glossary of Dental terms) defines theincisor classification as follows:
Fig. 1 Decalcificationattributable to fixedappliances and a patient withpoor oral hygiene throughouttreatment
Fig. 2 This patient has a reasonable need fororthodontic treatment, but the poor oral hygieneand gingival conditionprecludes this
Table 1 Relationship between crowding andextractionsDegree of crowding Need for extractions
< 5 mm No
5–10 mm Possibly
> 10 mm Yes
1+2+3+4+5 = A 1+2 = B
1
2
B – A = Degree of crowding
Fig. 3 Assessment ofcrowding. The widths ofall the teeth anterior tothe molars are measuredand subtracted from thesum of two measurements(mesial of the lowerincisor to the distal of thelower canine, plus distalof lower canine to themesial of the first molar)to give the degree ofcrowding

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 195 NO. 10 NOVEMBER 22 2003 565
• Class I. The lower incisor edges occlude withor lie immediately below the cingulum plateau(middle part of) the upper central incisors.
• Class II. The lower incisor edges lie posteriorto the cingulum plateau of the upper centralincisors. There are two divisions:Division 1 — there is an increase in the overjetand the upper central incisors are usually proclined.Division 2 — the upper central incisors areretroclined. The overjet is usually minimal butmay be increased.
• Class III. The lower incisor edges lie anteriorto the cingulum plateau of the upper centralincisors. The overjet is reduced or reversed.
The centre line should be measured by plac-ing a ruler down the patient's facial mid-line andmeasuring how far away from this the centrelines deviate (Fig. 4). This can then be marked inthe notes as shown in Figure 5.
The buccal occlusion is assessed next, par-ticularly the molar relationship. This is impor-tant because when assessing the treatment, ithas to be decided whether the buccal occlusionis to be accepted or whether it should be cor-rected as part of the treatment plan. The canineand molar relationships should be recorded asclass I, II or III
Finally, the presence of any anterior or pos-terior cross-bites should be assessed and ifthere is a cross-bite, the clinician should checkto see whether there is any mandibular dis-placement associated with it. This is importantbecause any displacement will mask the posi-tion of the teeth and give a misleading indica-tion of the inter-occlusal relationships. Figure 6shows a child who has an apparently severeclass III incisor relationship. However, he canget his teeth into an edge-to-edge relationshipand in this position the occlusion does notappear to be so severe. The amount of procli-nation of the upper incisors needed to correctthe incisor relationship was quite mild andeasily accomplished using a removable appli-ance (Fig. 7 and 8).
Fig. 5 Method for recording deviations in thecentre line where the lower is to the right by 1mmand the upper to the left by 2 mm
Fig. 4 Measurement of centre linedeviation using a ruler placed inthe patient's mid line
Fig. 6 Class IIImalocclusion with adisplacementanteriorly. The patientcan achieve an edge toedge incisor relation inthe retruded positionof the mandible
Fig. 8 The correctedincisor position forthe patient
Fig. 7 Upper removable appliance used to correct theanterior cross bite

BRITISH DENTAL JOURNAL VOLUME 195 NO. 12 DECEMBER 20 2003 683
PRACTICE
Orthodontics. Part 4: Treatment planningD. Roberts-Harry1 and J. Sandy2
The treatment plan is an integral part of orthodontic management. It should be divided intoboth treatment aims (what do you want to do?) and plan (how are you going to do it?). Thetreatment aims will include, for example overjet reduction. The plan will consider how tocreate space in order to accomplish this as well as the appliance system that will be used.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professorin Orthodontics, Division of Child DentalHealth, University of Bristol Dental School,Lower Maudlin Street, Bristol BS1 2LY*Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4810820© British Dental Journal 2003; 195:683–685
● Treatment planning is an essential part of orthodontic management● Consider the treatment aims first, then the treatment plan● The teeth and periodontium must be healthy before starting orthodontic treatment● To help ensure a successful treatment outcome the oral hygiene and diet must be good● Choosing the correct appliance is important
I N B R I E F
Treatment planning is the second mostimportant part of orthodontic managementfollowing the patient examination. It is help-ful to divide treatment planning into two sec-tions, treatment aims and treatment plan.Although it is possible that orthodontic treat-ment can influence the skeletal form whengrowth-modifying (functional) appliancesare used, it has little effect on soft tissues,tooth size and arch length. Remember that itis not necessary to treat every malocclusionand the benefits to the patient should becarefully assessed prior to undertaking anyorthodontic treatment.
TREATMENT AIMSThe following list is not comprehensive and hasto be tailored to the individual case. Some of theproblems that may need to be addressed duringtreatment are:
• Improve dental health• Relieve crowding• Correct the buccal occlusion• Reduce the overbite• Reduce the overjet• Align the teeth
As emphasised previously, it is essential thatthe oral health is of a high standard before treat-ment starts. Carious teeth should be restored andthe periodontal condition and oral hygieneshould be excellent before treatment starts.
Relieve crowdingThe decision to extract teeth needs to be careful-ly considered and depends on the degree ofcrowding, the difficulty of the case and thedegree of overbite correction.
Correct the buccal occlusionThe key to upper arch alignment is to get thecanines into a Class I relationship (Fig. 1).
4
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
Fig. 1 It is important to achieve a Class I canineposition in order to fully correct the overjet andthe buccal segment relations
VERIFIABLE CPD PAPER
12p683-685.qxd 13/11/2003 11:02 Page 683

PRACTICE
684 BRITISH DENTAL JOURNAL VOLUME 195 NO. 12 DECEMBER 20 2003
Providing the lower incisors are well aligned,achieving this will generally produce suffi-cient space to align the upper incisors.
In order to get the canines Class I there are, ingeneral two choices for the molar relationship atthe end of treatment; either Class I or a full unitClass II. This will be covered in more detail laterin the section on treatment plan.
Overbite and overjet reductionThe overbite should always be reduced beforeoverjet reduction is attempted. A deep overbitewill physically prevent the overjet from beingreduced because of contact between the upperand lower incisors.
RetentionOnce the overjet has been reduced and or upperincisors have been aligned a retainer should be
fitted. These are designed to reduce the risk ofrelapse post treatment by allowing remodellingand consolidation of the alveolar bone aroundthe teeth and reorganisation and maturation ofthe periodontal fibres. There are many differenttypes of retainers but they are generally remov-able or fixed. There are no hard and fast rulesregarding the length of time retention shouldcontinue. The authors recommend for removableappliance treatment that retention should con-tinue for 3 months full time and 3 months atnight-time only. For fixed appliance cases thisshould be 3 months full time and a minimum of9 months at night-time only. At the end of thisminimum year’s worth of retention, discre-tionary wear should be advised. This means thatthe patient is given the option of discarding theretainer if they are fed up with wearing it, orcontinuing on a part-time regime to give theteeth the best possible chance of stayingstraight. If they decide to stop wearing theretainer they should be warned there is no guar-antee that the teeth will remain straightthroughout life and the only way to improve thisprospect is by indefinite (ie life-long) wearing ofthe retainer.
Some cases, especially those that were spacedor where rotations were present prior to treat-ment, should be retained indefinitely, usuallywith bonded retainers.
TREATMENT PLANThe treatment plan should be considered as follows:
• Oral health• Lower arch• Upper arch• Buccal occlusion• Choose the appliance
Oral healthTooth brushing and diet advice must be givenand written in the notes. Daily fluoride rinses arealso recommended. Caries must be treated andperiodontal problems appropriately addressed.
Lower archPlan the lower arch first. The size and form ofthe lower arch should generally be accepted.Excessive expansion in the buccal regions orproclination of the lower incisors is contra-indicated in most cases because the soft tis-sues will generally return the teeth to theiroriginal position.
The need for extractions depends on thedegree of crowding. In some cases, slight procli-nation of the lower incisors and expansion inthe lower premolar region is acceptable,although this should be kept to a minimum incarefully planned cases. Generally this type oftreatment is confined to the correction of mildcrowding (less than 5 mm), cases where incisorshave been retroclined by a digit habit or trappedin the vault of the palate, or during developmentof Class II Division 2 malocclusions especially
Fig. 2 The importance ofkeeping extraction patternssymmetrical is demonstrated.The lower arch crowding hasbeen dealt with by removal oftwo lower premolars. The lossof the corresponding upperpremolars means the molarrelationship at the end oftreatment should be Class I
Fig. 3 Where upper premolarsalone are extracted (assumingno crowding in the lower arch),reduction of the overjet andspace closure means the molarrelationship must be a full unit Class II
12p683-685.qxd 13/11/2003 11:03 Page 684

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 195 NO. 12 DECEMBER 20 2003 685
where there is a deep bite. Any case where theoverbite is excessive must be very carefullyassessed before extraction decisions are made.
As the degree of crowding increases from 5–10 mm the need for extractions increases andwith more than 10 mm of crowding extractionsare nearly always required. If spontaneousalignment or removable appliances are to beused, first premolars are usually the extractionof choice because they are near to the site ofcrowding, allow the canines to upright and pro-duce the best contact point relationship. If otherteeth are to be extracted then generally fixedappliances will be required. Crowding tends toworsen with age and is thought to be related tofacial growth which continues at least until thefifth decade.
Upper archPlan the upper arch around the lower. If extrac-tions are undertaken in the lower arch theseshould generally be matched by extractions inthe upper. If no extractions are carried out in thelower arch the space for upper arch alignmentmay come from either distal movement of theupper buccal segments or extraction of upperpremolars. The choice depends on the spacerequirements and the buccal occlusion. As thedegree of crowding and overjet increase, thenthe space requirements will also increase and itis more likely that extractions as opposed to dis-tal movement will be indicated.
Determine whether the teeth are favourablypositioned for spontaneous alignment. If appli-ances are needed can removable or fixed appli-ances accomplish the tooth movements?
Plan the buccal occlusionConsider whether this needs to be corrected andif so how. If headgear is to be used, should it beused in conjunction with a removable or a fixedappliance? If the lower arch is crowded, spacemay be created by the removal of two lower pre-molars. This is then matched by upper premolarextractions and the molar relationship must beClass I at the end of treatment to allow the arch-es to fit together (Fig. 2).
However if the lower arch is well aligned,space to align the upper arch can be created byeither upper premolar extractions or by distalmovement of the upper buccal segments. Thechoice depends on how much space is requiredand what the molar relationship is at the startof treatment. Generally the more Class II themolars are the more likely one will opt for pre-molar extraction rather than distal movement.Moving molars more than 3–4 mm distally is
possible but becomes increasingly demandingon patient co-operation. In circumstanceswhere the space requirements are large, upperpremolar extraction reduces the treatmenttime and increases patient compliance. Figure3 shows the sequence of events when upperpremolar extraction alone is undertaken as anaid to overjet reduction.
The nearer to Class I the initial buccal occlu-sion is, the more likely it will be that distalmovement is appropriate. Therefore, spacerequirements that involve less than half a unitClass II correction can be accomplished by distalmovement of the molars in a relatively shorttime with more chance of good patient co-oper-ation (Fig. 4). Extracting upper premolars inthese cases produces an excess of space and mayincrease the treatment time.
Choose the applianceOnce the need for extractions has been consid-ered the appropriate appliance should be select-ed. This can involve allowing some spontaneousalignment to occur, using removable, fixed orfunctional appliances with the addition of extra-oral traction or anchorage. Appliance choicesare covered in the next section.
Fig. 4 Where a relatively smallClass II correction is required —this can be achieved throughdistal movement of the molars.The loss of upper premolars inthis case would produce anexcess of space
12p683-685.qxd 13/11/2003 11:04 Page 685

BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004 9
PRACTICE
Orthodontics. Part 5: Appliance choicesD. Roberts-Harry1 and J. Sandy2
There are bewildering array of different orthodontic appliances. However, they fall into fourmain categories of removable, fixed, functional and extra-oral devices. The appliance has tobe selected with care and used correctly as inappropriate use can make the malocclusionworse. Removable appliances are only capable of very simple movements whereas fixedappliances are sophisticated devices, which can precisely position the teeth. Functionalappliances are useful in difficult cases and are primarily used for Class II Division Imalocciusions. Extra-oral devices are used to re-enforce anchorage and can be an aid inboth opening and closing spaces.
1Orthodontic Department, Leeds DentalInstitute, Clarendon Way, Leeds LS2 9LU;2Division of Child Dental Health, Universityof Bristol Dental School, Lower MaudlinStreet, Bristol BS1 2LY
Refereed Paperdoi:10.1038/sj.bdj.4810872© British Dental Journal 2004; 196:9–18
● The correct appliance choice is essential for optimum treatment outcome● Removable appliances have an important but limited role in contemporary orthodontics● Fixed appliances are usually the appliance of choice● Functional appliances are helpful in difficult cases but may not have an effect on
facial growth● Extra-oral devices include headgear, face-masks and chin-caps
I N B R I E F
There are four main types of types of appliancethat can be used for orthodontic treatment.These are removable, fixed, functional and extraoral devices.
REMOVABLE APPLIANCES In general these are only capable of simple toothmovement, such as tipping teeth. Bodily move-ment is very difficult to achieve with any degreeof consistency and precise tooth detailing andmultiple tooth movements are rarely satisfactory.These appliances have received bad press overthe past few years because studies have shownthat the treatment outcomes achieved can oftenbe poor.1,2 In these studies as many as 50% ofcases treated with removable appliances wereeither not improved or worse than at the start oftreatment. When faced with evidence such asthis, one might be justified in discarding remov-able appliances completely. However, providedthey are used in properly selected cases they stillcan be very useful devices and the treatmentoutcome can be satisfactory.3 In general, remov-able appliances are only recommended for the following:
• Thumb deterrent• Tipping teeth• Block movements• Overbite reduction• Space maintenance• Retention
Thumb deterrentDigit sucking habits which persist into theteenage years can sometimes be hard to breakand may result in either a posterior buccal crossbite or an anterior open bite with proclination ofthe upper and retroclination of the lower inci-sors. In general, if the habit stops before facialgrowth is complete then the anterior open biteusually resolves spontaneously and the overjetreturns to normal.4
Figs. 1a–c show a case with an anterioropen bite associated with an avid digit suck-ing habit. A simple upper removable appliancewas used successfully to stop the habit. Theappliance simply makes the habit feel less of acomfort and acts as a reminder to the patientthat they should stop sucking the thumb.Complex appliances with bars or tongue cribsare rarely needed. In this patient once thehabit had stopped the open bite closed downon its own without the need for further ortho-dontic treatment.
TippingOne of the major uses of removable appliancesis to move one incisor over the bite as shown inFigs 2a–d. A simple upper removable applianceutilized a ‘T’ spring constructed from 0.5 mmwire activated 1–2 mm which delivered a forceof about 30 g to the tooth. After only a fewweeks the cross bite was corrected without theneed for complex treatment. Note the anterior
5
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
VERIFIABLE CPD PAPER
NOW AVAILABLE AS A BDJ BOOK
01p9-18.qxd 04/12/2003 14:27 Page 9

PRACTICE
10 BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004
retaining clasp that prevents the appliancefrom displacing downwards when the spring isactivated.
If teeth are to be pushed over the bite withremovable appliances, a stable result is morelikely to be achieved if the tooth is retroclined inthe first instance, the overbite is deep and there
is an anterior mandibular displacement associ-ated with a premature contact. Tipping teethtends to reduce the overbite because the tip ofthe tooth moves along the arc of a circle asshown in Figure 3a. Excessive tipping may alsomake the tooth too horizontal which can be notonly aesthetically unacceptable but may also
Fig. 1a–c A 9 year-old patient with an anterioropen bite caused by a thumb sucking habit. Notethe wear on the thumb as a result of this. Shewas fitted with a simple upper removableappliance and gently encouraged to stop thehabit. She did so successfully and the open biteclosed down spontaneously in 6 months
Fig. 2a an anterior cross bite involving the upperleft and lower left central incisors
Fig. 2c The appliance in place. The T spring isactivated 1–2 mm every 4 weeks
Fig. 2d The completed case. Active treatment took12 weeks
Fig. 2b An upper removable appliance with Adamscribs for retention made from 0.7 mm wire on thefirst permanent molars and the upper left centralincisor. A ‘T‘ spring made from 0.5 mm wire isused to push the tooth over the bite. The anteriorretention is to prevent the front of the appliancebeing displaced as the spring is activated
01p9-18.qxd 04/12/2003 14:30 Page 10

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004 11
result in excessive non-axial loading of thetooth as illustrated in Figure 3b.
Overbite reduction when teeth are over pro-clined is illustrated in Figures 4a–d. In this caseboth the upper lateral incisors were pushed overthe bite with an upper removable appliance. Thecross bite was corrected but note the reductionin overbite on the lateral incisors. Six monthsafter completion of treatment the upper rightlateral had relapsed back into cross bite.
Block movementsIf a cross bite involves a number of teeth, forexample a unilateral buccal cross bite, remov-able appliances can be used to correct this. The
sequence of events is shown in Figures 5a–f.Adams cribs are generally placed on the firstpremolars and the first permanent molars and amidline expansion screw is incorporated intothe base plate. This midline screw is opened0.25 mm (one quarter turn) twice a week untilthe cross bite is slightly overcorrected. Posteri-or buccal capping can also be used to disen-gage the bite and prevent concomitant expan-sion of the lower arch. Once the cross bite iscorrected the buccal capping can be removedand the appliance used as a retainer to allowthe buccal occlusion to settle in. Occasionallytwo appliances will be needed if a considerableamount of expansion is needed.
Fig. 3a The effect of tipping anteriorteeth on the overbite. As the teethmove around a centre of rotation theincisal tip moves along the arc of acircle. By the laws of geometry, asthe tooth is proclined the overbitereduces once it moves past thevertical
Fig. 3b Excessive tipping not onlyreduces the overbite but also makesthe axial inclination of the teeth too horizontal. In thesesituations stability is reduced, theappearance is poor and the tooth maysuffer from unwanted non-axial loading ➠
➠
Fig. 4a Both the upper lateral incisors are in crossbite
Fig. 4c The cross bites have been corrected. Notethe reduction in the overbite
Fig. 4d 6 months later the upper right lateral hasrelapsed into cross bite due to the reducedoverbite
Fig. 4b An upper removable appliance was used totip the laterals over the bite
01p9-18.qxd 04/12/2003 14:31 Page 11

PRACTICE
12 BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004
Fig. 5a Narrowness of the upper arch can produce a traumatic bite
Fig. 5c An upper removable appliance with a mid line expansionscrew can be used to correct the cross bite. The screw is opened one-quarter turn twice a week by the patient
Fig. 5d The corrected cross bite. The treatment time varies with theamount of expansion needed but usually takes about twelve weeks
Fig. 5b To avoid painful cuspal contact the patient may move themandible to one side producing a mandibular deviation and a crossbite
Fig. 5e Once active treatment is completed the appliance can beworn as a retainer. The posterior capping can be reduced to allowinterdigitation of the buccal teeth thus helping to prevent anyrelapse
Fig. 5f The completed case
01p9-18.qxd 04/12/2003 14:31 Page 12

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004 13
Overbite reductionRemovable appliances are very effective in cor-recting a deep overbite, especially in a growingpatient. An upper removable appliance with ananterior bite plane is used which disengages themolars by 2–3 mm whilst at the same timeestablishing lower incisor contact with the biteplane (Fig. 6). Eruption of the posterior teethproduces a reduction in the overbite. It is essen-tial that the inter-incisor angle is corrected atthe completion of treatment so that an occlusalstop between the upper and lower incisors isproduced preventing re-eruption of the incisorsand a relapse of the overbite. Bite planes areusually used in conjunction with fixed appli-ances to help the overbite reduction (Figures7a–d) or can be used as an aid to restoration of the anterior teeth. Figures 8a–d show a patient with a deep bite who had marked enamelerosion. Porcelain crowns were to be placed onthe anterior teeth to restore them, but the deepbite made this technically difficult. The overbite
was therefore reduced with a bite plane to makeroom for the crowns.
Space maintenance Space maintainers are rarely indicated in ortho-dontic treatment but occasionally can be used,particularly if the upper canine is buccally crowd-ed. Whilst the extraction of the first premolarswill often create space for the canines, there is a danger that the space will close before thecanine erupts as the buccal teeth drift mesially.Figures 9a–e illustrate such a case where the fit-
ting of a space maintainer proved useful. Theappliance was fitted just prior to the emergenceof the permanent canines. The four first premo-lars were then extracted and the appliance left inposition until the canines erupted. This tookabout 6 months and saved a considerableamount of extra treatment for the patient byallowing spontaneous alignment of the canines.
RetentionMany orthodontists use various types of remov-able appliances to act as retainers, usually at the
2-3mm
Fig. 6 Overbite correction with a removable appliance. The posterior teethshould be separated by about 2–3 mm
Fig. 7a A case with a deep bite and retroclinedupper incisors
Fig. 7c Once the overbite is fully reduced theupper fixed appliance can be placed
Fig. 7d The completed case with good overbitereduction
Fig. 7b An upper removable appliance is used tohelp the overbite reduction whilst palatal springssimultaneously move the first permanent molars distally
01p9-18.qxd 04/12/2003 14:33 Page 13

PRACTICE
14 BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004
Fig. 8a, b A patient with severe erosion of theteeth
Fig. 8c A bite plane was used to reduce theoverbite
Fig. 8d Strip crowns were placed on the incisorsonce the overbite was reduced
Fig. 9a, b A case with severe upper arch crowding. The upperpermanent canines were unerupted, buccally positioned andvery short of space
Fig. 9c An upper removable space maintainer. Adam cribs havebeen placed on the first permanent molars and a Southend claspon the upper central incisors
Fig. 9d,e The first premolars have been extracted and the upper caninesare erupting into a good position
➠
➠
➠ ➠
01p9-18.qxd 04/12/2003 14:34 Page 14

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004 15
completion of fixed appliance treatment.Removable retainers are usually held in positionwith Adams Cribs on the first permanent molarswith a labial bow and possible acrylic coverageof the anterior teeth (Fig. 10).
FIXED APPLIANCESThese appliances are attached to the crowns ofteeth and allow correction of rotations, bodilymovements of teeth and alignment of ectopicteeth. They have increased in sophisticationenormously over the past 10–15 years andtogether with advancements in arch wire tech-nology are capable of producing a very highlevel of treatment result. Simultaneous multiple
tooth movements can be achieved, invariablycreating a better treatment outcome than can beachieved with removable appliances. Althoughthere are a variety of fixed appliances availablethey all operate in a similar way producing afixed point of attachment to control the positionof the teeth. Brackets are attached to the teethand wires (arch wires) are placed in the bracketslots to move the teeth. The closer the fit of rec-tangular arch wires in a rectangular slot on thebracket the greater the control of the teeth(Fig 11). As treatment progresses, thicker rectan-gular wires are used to fully control the teeth inthree dimensions. Fixed appliances are theappliances of choice for most orthodontic treat-
ment because the results are far more predictableand of a higher standard achieved than by othermeans. However, they are relatively complexappliances to use and further training in thesedevices is essential. An example of a case treatedwith fixed appliances is shown in Figure 12a–j.The anchorage requirements for the bodilymovement of teeth are considerably greater thanfor tipping movements (Fig. 13).
FUNCTIONAL APPLIANCESThese are powerful appliances capable of impres-sive changes in the position of the teeth. Theyare generally used for Class II Division I maloc-clusions although they can be used for the
Fig. 10 One exampleof the manydifferent types ofremovable retainers
Fig. 11 Rectangular arch wire in rectangular bracketslots allows three-dimensional control of the teeth. The tighter the fit of the wire in the slotthe greater the control of the teeth
01p9-18.qxd 04/12/2003 14:37 Page 15

PRACTICE
16 BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004
Fig. 12a, b Pre treatment photographs of a patient with palatallyimpacted canine, a buccal cross bite, an increased overjet andcrowding in both arches
Fig. 12c Upper first and lower secondpremolars were extracted and the caninessurgically exposed
Fig. 12d A tri-helix was used to expand the upperarch and a sectional fixed appliance used to pullthe canine into the line of the arch
Fig. 12e Full fixed appliances were then used to reduce the over biteand overjet, move the apex of the canine into the line of the arch andcorrect all the other features of the malocclusion. The initial archwire was a very thin flexible wire. If a thick wire is used at this stageexcess force will be applied to the teeth that can produce rootdamage and be very painful for the patient
Figs 12f,g Once initial alignment of the teeth is producedprogressively thicker, stiffer wires are employed. Because these fitthe bracket slot more closely they control tooth position moreprecisely than the thinner aligning wires
Fig. 12h,i Thecompleted case.The canine is fullyaligned and theoverjet reducedwithout anyunwanted tippingof the teeth
Fig. 12j Appropriate extractionsand treatment mechanics havenot been detrimental to the facialappearance
➠➠
01p9-18.qxd 04/12/2003 14:39 Page 16

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004 17
correction of Class II Division II and Class IIImalocclusions on occasion. They are eitherremovable from the mouth or fixed to the teeth,and work by stimulating the muscles of mastica-tion and soft tissues of the face. This produces adistalising force on the upper dentition and ananterior force on the lower. Whilst they are capa-ble of substantial tooth movement, like allremovable appliances they are not capable ofprecise tooth positioning and cannot deal effec-tively with rotations or bodily tooth movement.
There is some controversy as to the precisemode of action of functional appliances. Someclinicians feel they have an effect on this facialskeleton, promoting growth of the mandibleand/or maxilla. Others feel that the effects aremainly dento-alveolar and that the resultsachieved are accomplished by tipping the upperand lower teeth. Unfortunately many of the stud-ies relating to functional appliance treatmenthave been poorly constructed and their conclu-sions should be treated with caution. A large-scale, prospective, randomized clinical trialcurrently being undertaken in United Kingdomstrongly suggests that 98% of the occlusal
Fig. 13 Bodily movement of the teeth requires a greater degree offorce than tipping movements
Fig. 14c A functionalappliance was used tocorrect the saggitalrelationship
Fig. 14d The final resultafter detailing of theocclusion with fixedappliances
Fig. 14e,f Thefacial appearancefollowingtreatment
Fig. 14a,b Pre-treatmentphotographs of a 12-year-old girl with an increasedoverjet and a class II skeletalpattern associated with aretrognathic mandible
➠
➠
➠
➠
➠
➠
01p9-18.qxd 04/12/2003 14:41 Page 17

PRACTICE
18 BRITISH DENTAL JOURNAL VOLUME 196 NO. 1 JANUARY 10 2004
correction is by tipping of the teeth with analmost negligible effect on the skeletal pattern.5
Nevertheless, dramatic occlusal changes are pos-sible with these appliances and they can aid thecorrection of some quite severe malocclusions.Figures14a–f show a case treated with a function-al appliance that had a marked effect not only on the occlusion but also on the patient's facialappearance.
EXTRA-ORAL DEVICESThese are headgear devices, chin caps and facemasks, which are used to provide an externalsource of anchorage or traction for teeth in one orboth arches. The commonest type is headgear forthe distal movement of the buccal teeth. A metalface bow is attached to either a removable or afixed appliance inside the mouth and elastic trac-tion applied to it. As well as force being applieddistally to either the maxilla or the mandible itcan be applied mesially via a facemask. This istypically used in Class III cases to correct an ante-
rior cross bite or in cases where the buccal seg-ments are being moved forward to close spaces inthe arches. Examples of extra oral tractiondevices are shown in Figures 15, 16a and b. Chincaps have been used to try and restrain mandibu-lar growth in Class III malocclusions. However,the evidence from the literature suggests that theyare not terribly effective and their use hasdeclined in recent years.
1. Richmond S, Shaw W C, O'Brien K D et al. The development ofthe PAR index (Peer Assessment Rating): reliability and validity.Eur J Orthod 1992; 14: 125-139.
2. Richmond S, Shaw W C, Roberts C T, Andrews M. The PAR index(Peer Assessment rating): methods to determine the outcomeof orthodontic treatment in terms of improvements andstandards. Eur J Orthod 1992; 14: 180-187.
3. Kerr W J S, Buchanan I B, McColl J H. The use of the PAR index inassessing the effectiveness of removable orthodonticappliances. Br J Orthod 1993; 20: 351-357.
4. Leighton B C. The early signs of malocclusion. Trans EuropOrthod Soc 1969; 353-368.
5. O'Brien K, Wright J, Conboy F et al. Effectiveness of treatmentfor Class II malocclusion with the Herbst or twin-blockappliances: a randomized, controlled trial. Am J OrthodDentofacial Orthop 2003; 124: 128-137.
Fig. 16a,b A facemask or reverse headgearFig. 15 Extra-oral tractionapplied via an Interlandiiheadgear
A letter to the BDJ highlighting the concerns of one of its members.
Sir, - There is a movement on foot to establish a “Section” of Dental Surgery in theBritish Medical Association, of which membership is only possible to those members ofthe British Dental Association who are on the Medical register.
I beg you most emphatically to protest against any new section, or society of dentalsurgeons being formed to which every member of the British Dental Association is noteligible. I am strongly in favour of every dentist being a surgeon as well (if possible), butI protest against a revival of the “Association of Surgeons practising Dental Surgery” inthis insidious form.
Yours trulyS. J. Hutchinson, M. R. C. S., LDS.Eng
BR Dent J, 1903; 24: 828
One Hundred Years Ago
01p9-18.qxd 04/12/2003 14:42 Page 18
usha
Rectangle

BRITISH DENTAL JOURNAL VOLUME 196 NO. 2 JANUARY 24 2004 71
PRACTICE
Orthodontics. Part 6: Risks in orthodontic treatmentH. Travess1, D. Roberts-Harry2 and J. Sandy3
Orthodontics has the potential to cause significant damage to hard and soft tissues. The most important aspect oforthodontic care is to have an extremely high standard of oral hygiene before and during orthodontic treatment. It isalso essential that any carious lesions are dealt with before any active treatment starts. Root resorption is a commoncomplication during orthodontic treatment but there is some evidence that once appliances are removed this resorptionstops. Some of the risk pointers for root resorption are summarised. Soft tissue damage includes that caused byarchwires but also the more harrowing potential for headgears to cause damage to eyes. It is essential that adequatesafety measures are included with this type of treatment.
1Senior Specialist Registrar, 2 ConsultantOrthodontist, Orthodontic Department,Leeds Dental Institute, Clarendon Way,Leeds LS2 9LU; 3Professor of Orthodontics,Division of Child Dental Health, Universityof Bristol Dental School, Lower MaudlinStreet, Bristol BS1 2LY
Refereed Paperdoi:10.1038/sj.bdj.4810891© British Dental Journal 2004; 196:71–77
● Before any active orthodontic treatment is considered it is essential that the oral hygiene isof a high standard and that all carious leions have been dealt with
● Arch wires, headgears and brackets themselves may cause significant damage either duringan active phase of treatment or during debonding. Much care needs to be taken wheninstructing patients about their role in orthodontic treatment
● The aim of this section is to outline potential risks in orthodontic treatment and to giveexamples. There are also a number of illustrations to help highlight these points
I N B R I E F
If orthodontic treatment is to be of benefit to apatient, the advantages it offers should outweighany possible damage it may cause.1 It is impor-tant to assess the risks of treatment as well as thepotential gain and balance these aspects of treat-ment before deciding to treat a malocclusion.The psychological trauma of having orthodontictreatment, or indeed not having treatmentshould not be overlooked and is an importantconsideration in treatment planning. Patientselection plays a vital role in minimising risks oftreatment and the clinician should be vigilant inassessing every aspect of the patient and theirmalocclusion. However, clinically there are anumber of areas of concern for risk manage-ment. These are discussed in detail under thebroad categories of intra-oral, extra-oral and systemic risks.
INTRA-ORAL RISKS
Enamel demineralisation/cariesEnamel demineralisation, usually on smooth sur-faces, is unfortunately a common complicationin orthodontics; figures range from 2–96% oforthodontic patients (Fig.1).2 This large variationprobably arises as a result of the variety of meth-ods used to assess and score the presence ofdecalcification. There is also inconsistency onwhether idiopathic lucencies are included orexcluded in the study design.3 The teeth mostcommonly affected are maxillary lateral incisors,maxillary canines and mandibular premolars.4
However, any tooth in the mouth can be affected,and often a number of anterior teeth show decal-
cification. Whilst the demineralised surfaceremains intact, there is a possibility of remineral-isation and reversal of the lesion. In severe cases,frank cavitation is seen which requires restora-tive intervention (Figs. 2 and 3).
Gorelick et al.5 in a study on white spot for-mation in children treated with fixed appliances,found that half of their patients had at least onewhite spot after treatment, most commonly onmaxillary lateral incisors. The length of treat-ment did not affect the incidence or number ofwhite spot formations, although O'Reilly andFeatherstone6 and Oggard et al.7 found thatdemineralisation can occur rapidly, within thefirst month of fixed appliance treatment. Thishas obvious aesthetic implications and high-lights the need for caries rate assessment at thebeginning of treatment. Interestingly, Gorelick et al.5 found no incidence of white spot forma-tion associated with lingual bonded retainers,which would suggest salivary buffering capaci-ty, and flow rate have a role in protection againstacid attack.
6
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
Fig. 1 Decalcification on labial surfaces ofnumerous teeth
VERIFIABLE CPD PAPER
02p71-77.qxd 12/12/2003 11:58 Page 71

PRACTICE
72 BRITISH DENTAL JOURNAL VOLUME 196 NO. 2 JANUARY 24 2004
The dominant hand may also influence thearea of decalcification as brushing is more diffi-cult on the side of the dominant hand. Whilstgood oral hygiene is vital, dietary control ofsugar intake is also needed in order to minimisethe risk of decalcification. Fluoride mouthwash-es used throughout treatment can prevent whitespot formation8 surprisingly, compliance withthis is low (13%). Other fluoride release mecha-nisms include fluoride releasing bonding agents,elastic ligatures containing fluoride, and depotdevices on upper molar bands.9
Preventive measures to minimise damageinclude patient selection, vigorous oral hygienemeasures and dietary education. Reinforcementof oral hygiene and dietary education should beperformed at each visit. Positive reinforcementeven where oral hygiene is satisfactory willencourage the patient further. Inspection of thelabial surfaces of the teeth at each adjustmentappointment will identify cases that require moreintervention and advice. It is important whenexamining the teeth that they are plaque-freeotherwise early demineralisation may be missed.This can be done by instructing the patient toclean their teeth in the surgery with or without thewires in place, or by professional prophylaxis. Theuse of auxillaries such as dental health educatorsand hygienists is highly desirable. Removal of theappliance in cases with extreme demineralisationor poor hygiene is the last resort, but should notbe discounted by the clinician.
Where demineralisation is present post treat-ment, fluoride application either via toothpaste,
or by adjunct fluoride mouthwash (0.05% sodi-um fluoride daily rinse or 0.2% sodium fluorideweekly rinse), can be helpful in remineralisingthe lesion and reducing the unsightliness of thedecalcification.10 Acid/pumice micro abrasionhas also been advocated to improve the aesthet-ics of stabilised lesions.11,12 This procedureshould be delayed at least 3 months followingdebond to allow for spontaneous improvementof the lesions and remineralisation with fluorideapplications.13 Persistent lucencies should beabraded with 18% hydrochloric acid in finepumice under rubber dam in bursts of 30 sec-onds for a maximum of 10 times. After the lastapplication the tooth is washed well and a fluo-ride varnish applied.11
Enamel traumaWhen placing appliances careless use of a bandseater can result in enamel fracture. Care isrequired when large restorations are presentsince these can result in fracture of unsupportedcusps.14 Debonding can also result in enamelfracture, both with metal and ceramic brackets(Fig. 4).15,16 Care must always be taken toremove brackets and residual bonding agentsappropriately to minimise the risk of enamelfracture. The use of debonding burs has thepotential to remove enamel, especially in air tur-bine fast handpieces. Care and attention is need-ed when adhesives are removed.
Enamel wearWear of enamel against both metal and ceramicbrackets (abrasion) may occur. It is common onupper canine tips during retraction as the cusptip hits the lower canine brackets (Fig. 5). It mayalso be seen on the incisal edges of upper ante-rior teeth where ceramic brackets are placed onlower incisors.17 Ceramic brackets are veryabrasive and therefore contraindicated for thelower anterior teeth where there is any possibil-ity of the brackets occluding with the upperteeth, bearing in mind that the overbite may
• Good oral hygieneis essential for successful orthodontic treatment
• Daily fluoride rinses may prevent and reduce decalcifications
• Care is neededwhen debracketingas there is thepotential for enamel damageespecially withceramic brackets
Fig. 3 Obvious caries in the disto-occlusalaspect of a lower molar
Fig. 4 Enamel fracture at debond
Fig. 2 Cavitation at the gingival margin ofthe lower right canine and first premolarrequiring restoration
02p71-77.qxd 12/12/2003 11:59 Page 72

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 2 JANUARY 24 2004 73
increase in the early stages of treatment. Anyenamel erosion must be recorded prior to treat-ment commencing and appropriate dietaryadvice given to minimise further tooth sub-stance loss. Carbonated drinks and pure juicesare the commonest causes of erosion and shouldbe avoided in patients with fixed appliances.
Pulpal reactionsSome degree of pulpitis is expected withorthodontic tooth movement which is usuallyreversible or transient. Rarely it leads to lossof vitality, but there may be an increase inpulpitis in previously traumatised teeth withfixed appliances. Light forces are advocatedwith traumatised teeth as well as baselinemonitoring of vitality which should be repeat-ed three monthly.18 Transient pulpitis mayalso be seen with electrothermal debonding ofceramic brackets19 and composite removal atdebond.20
Root resorptionSome degree of external root resorption isinevitably associated with fixed appliancetreatment, although the extent is unpre-dictable.21 Resorption may occur on the apicaland lateral surface of the roots, but radiographsonly show apical resorption to a certain degree.Many cases will not show any clinically signif-icant resorption but, microscopic changes arelikely to have occurred on surfaces which arenot visualised with routine radiographs.Resorption however rarely compromises thelongevity of the teeth.22 Vertical loss of bonethrough periodontal disease creates a fargreater loss of attachment and support than itsequivalent loss around the apex of a tooth.
The mechanism of tooth resorption is unclear.Theories include excessive force and hyalinisa-tion of the periodontal ligament resulting inexcessive cementoclast and osteoclast activity.What is clear are the risk factors which are asso-ciated with cases with severe resorption. Thesecan be summarised as:
• Blunt and pipette shaped roots show a greateramount of resorption than other root forms.
• Short roots are more at risk of resorption thanaverage length roots.
• Teeth previously traumatised, have anincreased risk of further resorption.
• Non vital teeth and root treated teeth have anincreased risk of resorption.
• Heavy forces are associated with resorption,as well as the use of rectangular wires, Class IItraction, the distance a tooth is moved and thetype of tooth movement undertaken.
• Combined orthodontic and orthognathic pro-cedures.
Treatment of ectopic canines may induceresorption of the adjacent teeth because of thelength of treatment time and the distance thecanine is moved. Tooth intrusion is also associ-ated with increased risk as well as movement ofroot apices against cortical bone. Above the ageof 11 years the risk of resorption with treatmentseems to increase. Adults have shorter roots atthe outset and the potential for resorption isincreased.
Opinion is divided on whether treatmentlength is associated with increased resorp-tion. Some find no correlation with treatmenttime, whereas others find that there isincreased resorption with increased treatmenttime. In a few patients systemic causes maycontribute, for example hyperthyroidism, butfor the most part no underlying cause is iso-lated other than individual susceptibility.Familial risk is also known.
A wide range in the degree of resorption isseen, highlighting the role of individual sus-ceptibility over and above the risk factorsidentified. Research is still required in this areato identify the mechanisms of resportion, trig-ger factors and reparative mechanisms if treat-ment modalities are to be modified in thefuture to minimise root damage. Currently, nocase is immune from the risk of root resorp-tion, to some degree, and patients should bewarned at the outset of treatment that such arisk exists. Recognition of specific risk factors,accurate radiographs and interpretation ofradiographs at the outset of treatment areimportant if root resorption is to be minimised.Once resorption is recognised clinically duringtreatment, light forces must be used, rootlength monitored six monthly with radi-ographs and treatment aims reconsidered tomaximise the longevity of the dentition. Theuse of thyroxine to minimise root resorptionhas been advocated by some authors, but thisis not routinely used.23, 24
Periodontal tissuesFixed appliances make oral hygiene difficulteven for the most motivated patients, andalmost all patients experience some gingivalinflammation (Fig. 6). Resolution of inflamma-tion usually occurs a few weeks after debond,bands cause more gingival inflammation thanbonds, which is not surprising since the mar-gins of bands are often seated subgingivally.
• Root resorption isinevitable withfixed appliancetreatment
• On average 1-2 mmof apical root is lostduring a course of orthodontictreatment
• Previously traumatised teethhave an increasedrisk of root resorption
Fig. 5 Upper canine tip showing abrasion from thelower canine metal bracket
02p71-77.qxd 12/12/2003 12:00 Page 73

PRACTICE
74 BRITISH DENTAL JOURNAL VOLUME 196 NO. 2 JANUARY 24 2004
For the most part, the literature suggeststhat orthodontic treatment does not affect theperiodontal status of patients over the longterm. Patients with pre-existing periodontaldisease require special attention, but bone lossduring treatment does not seem to be relatedto previous bone loss. The need for excellentoral hygiene during treatment must beemphasised in patients with existing peri-odontal disease. The use of bonds rather thanbands on molars and premolars may be moreappropriate to eliminate unwanted stagnationareas. Plaque retention is increased with fixedappliances and plaque composition may alsobe altered. There is an increase in anaerobicorganisms and a reduction in facultativeanaerobes around bands, which are thereforeperiopathogenic.25
Oral hygiene instruction is essential in allcases of orthodontic treatment, and the use ofadjuncts such as electric toothbrushes, inter-proximal brushes, chlorhexidine mouthwash-es, fluoride mouthwashes and regular profes-sional cleaning must be emphasised. However,patient motivation and dexterity are para-mount in the success of hygiene, and there willalways be cases where oral hygiene is unsatis-factory from the outset. This should be careful-ly considered when advising a patient to havetreatment. Experience shows those patientswho are unable to maintain a healthy oralenvironment in the absence of fixed orthodon-tics will fail spectacularly with braces in place.Benefit must therefore significantly outweighthe risk of carrying out treatment in suchpatients (Figs. 7 and 8).
AllergyAllergy to orthodontic components intra-orally is exceedingly rare, however, there havebeen studies on the nickel release and corro-sion of metals with fixed appliances. Gjerdetet al.26 found a significant release of nickeland iron into the saliva of patients just afterplacement of fixed appliances. However, nosignificant difference was found in nickel oriron concentrations between controls andsubjects where the appliances had been inplace for a number of weeks. The clinical sig-nificance of nickel release is as yet unclear,but should be considered in nickel sensitivepatients. There are a few cases with severelatex allergies who may be affected by elas-tomerics or operators gloves.
TraumaLaceration to the gingivae, and mucosa seenas areas of ulceration or hyperplasia, oftenoccur during treatment or between treatmentsessions from the archwire (Fig. 9) andbonds, especially where long unsupportedstretches of wire rest against the lips. Theuse of dental wax over the bracket may helpto reduce trauma and discomfort, (Fig. 10) asmay rubber bumper sleeving on the unsup-ported archwire (Fig. 11).
Fig. 6 Severe gingival inflammation duringfixed appliance treatment. Note theinflammation covers the headgear tubeand hook on the upper molar band
Fig. 9 Trauma to the cheek from anunusally long distal length of archwireresulting in an ulcer
Fig. 8 Chronic lack of oral hygiene showing accumulation of plaque gingivally andaround the brackets
Fig. 7 Disclosing solution highlighting the areasof poor oral hygiene in a patient
02p71-77.qxd 12/12/2003 12:02 Page 74

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 2 JANUARY 24 2004 75
EXTRA-ORAL RISKS
AllergyAllergy to nickel is more common in extra-oralsettings, most usually the headgear face bow orhead strap. Over 1% of patients have some formof contact dermatitis to zips and buttons/studson clothing. Of these patients, 3% claim to haveexperienced a similar rash with orthodonticappliances (Fig. 12). The use of sticking plasterover the area in contact with the skin is suffi-cient to relieve symptoms. Allergy to latex27 andbonding materials has been reported althoughthese are rare.
TraumaFollowing a well publicised case of eye traumain a patient wearing headgear28 a number ofsafety headgear products have been designedand explicit guidelines are now available. Thesemeasures include safety bows (Figs 13 and 14),rigid neck straps (Fig. 15) and snap release prod-ucts (Fig. 16) to prevent the bow from disengag-ing from the molar tubes or acting as a projec-tile. A survey among British orthodontists founda 4% incidence of facial injury with headgear. Ofthese injuries, 40% were extra-oral and 50% ofthese were in the mid face. Two patients wereblind as a result of headgear trauma. Eye injuryis uncommon, but a serious risk and all availablemethods of reducing the risk of penetrating eyeinjury must be used. Every headgear and Kloehn
bow must incorporate a safety feature. Failure toobserve safety guidelines on the use of headgearis medico-legally indefensible.
BurnsBurns, either thermal or chemical are possibleboth intra- and extra-orally with inadvertentuse of chemicals or instruments. Acid etch, elec-trothermal debonding instruments and sterilisedinstruments which have not cooled down allhave the potential to burn and care should betaken in their use.
Tempromandibular dysfunction (TMD)Much attention in the literature has beenfocused on the relationship between TMD andorthodontic treatment. Whilst TMD is com-mon in the orthodontic aged populationwhether orthodontic treatment is carried outor not, there is no evidence to support the theory that orthodontic treatment causes TMDor cures it.29 Pre-existence of TMD should berecorded, and the patient advised that treat-ment will not predictably improve their condi-tion. Some patients may suffer with increasedsymptoms during treatment which must alsobe discussed at the beginning of treatment.Where patients experience symptoms duringtreatment, treatment should be directed ateliminating occlusal disharmony and jointnoises whilst reassuring the patient. Standard
Fig. 12 Nickel allergy (contactdermatitis) in a headgear wearer
Fig. 11 Ulcer in a patient’slower lip from a longstretch of unsupportedwire. Bumper sleeve hasbeen placed along the wireto prevent further trauma
Fig. 10 Dental wax placed over a bracket canease the pain of ulceration in the lip and mucosa
Fig. 13 Safety Kloehn bow showing recurvedloops for smooth distal ends to prevent injury if the bow becomes disengaged
Fig. 14 Safety Kloehn bow with Nitom lockingmechanism to prevent disengagement fromthe molar tube
02p71-77.qxd 12/12/2003 12:28 Page 75

PRACTICE
76 BRITISH DENTAL JOURNAL VOLUME 196 NO. 2 JANUARY 24 2004
treatment regimes may also be indicated egsoft diet, jaw exercises. We have not reviewedthis area in detail in this section as it is dealtwith under facts and fantasy in the next, butan excellent overview of the relation betweenorthodontics and occlusal relation has recentlybeen published.30
Profile damageExtraction of premolars has been condemnedby some with very little evidence, as alteringthe facial profile of the patient.31 A large num-ber of studies have shown that there is no sig-nificant difference in profiles treated by extrac-tion or non extraction means. Boley et al.32
found that neither orthodontists nor generaldentists could distinguish between extractionand non extraction treatment by looking atprofile alone. A recent review examined theeffects of orthodontics on facial profie andconcluded that it does not, although it high-lights areas where planning is crucial.33 Itshould be remembered that soft tissue changesoccur naturally with age, regardless of ortho-dontic intervention. Proper diagnosis shouldtake into account skeletal form, tooth positionand soft tissue form to negate the possibility ofany detrimental effect on profile by treatmentmechanics.34
SYSTEMIC RISKS
Cross infectionSpread of infection between patients, betweenoperator and patient and by a third party shouldbe prevented by cross infection proceduresthroughout the surgery. Use of gloves, masks,sterilised instruments and 'clean' working areasare paramount. A medical history must be takenfor every patient to determine risk factors,
although cross infection control should be of astandard to prevent cross contaminationregardless of medical status.
Infective endocarditisPatients at risk of endocarditis should be treatedin consultation with their cardiologist and withinthe appropriate guidelines.35,36 The patient mustexhibit immaculate oral hygiene, antibiotic coverwill be required for invasive procedures such asextractions, separation, band placement andband removal. It is recommended that bondedattachments are used on all teeth to negate theneed for antibiotic cover for both separator andband placement, as well as removal. This alsoreduces the risk of unwanted plaque stagnationareas. Chlorhexidine mouthwash has been advo-cated prior to any treatment and in some casesdaily to minimise bacterial loading.36
CONCLUSIONSClearly there are a number of sources of poten-tial iatrogenic damage to the patient duringorthodontic treatment. However, severe dam-age is rare. Severe malocclusions have more tobenefit from treatment than less severe maloc-clusions, and motivation between such groupsmay vary. Individuals should be assessed forrisk factors for all aspects of care. Lack oftreatment can result in damage, physical orpsychosocial. Discontinuation of treatmentwithout full correction of the malocclusion,although a last resort, can leave the patientworse off than before treatment. Good clinicalpractice, careful patient selection and informa-tion on a patient’s responsibility are essentialto minimise tissue damage.
The authors are grateful to Francis Scriven , ThomasHartridge and Ingrid Hosein for some of the figures andJane Western who cheerfully typed this manuscript.
Fig. 15 Interlandi headgear with a rigidMasel safety strap to hold the Kloehnbow and prevent disengagement for the buccal tubes
Fig. 16 Quick release headgearattachment. The breakaway design allowsthe bow to come out of the headgeartube, but is no longer under tension andtherefore unable to act as a projectile
02p71-77.qxd 12/12/2003 12:04 Page 76

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 2 JANUARY 24 2004 77
1. Shaw W C, O'Brien K D, Richmond S, Brook P. Quality control inorthodontics: risk/benefit considerations. Br Dent J 1991; 170:33-37.
2. Chang H S, Walsh L J, Freer T J. Enamel demineralisationduring orthodontic treatment. Aetiology and prevention. AusDent J 1997; 42: 322-327.
3. Mitchell L. Decalcification during orthodontic treatment withfixed appliances — An overview. Br J Orthod 1992 ; 19: 199-205.
4. Geiger A M, Gorelick L, Gwinnett A J, Griswold P G. The effectof a fluoride program on white spot formation duringorthodontic treatment. Am J Orthod Dento Orthop 1988; 93:29-37.
5. Gorelick L, Geiger A M, Gwinnett A J. Incidence of white spotformation after bonding and banding. Am J Orthod 1982;81: 93-98.
6. O'Reilly M, Featherstone J. Demineralisation andremineralisation around orthodontic appliances — an in vivostudy. Am J Orthod Dento Orthop 1987; 92: 33-40.
7. Öggard B, Rølla G, Arends J. Orthodontic appliances andenamel demineralisation. Part 1. Lesion development. Am JOrthod Dento Orthop 1988; 94: 68-73.
8. Geiger A M, Gorelick L, Gwinnett A J. Griswold P G. Effect of afluoride program on white spot formation duringorthodontic treatment. Am J Orthod Dento Orthop 1988; 93:29-37.
9. Marini I, Pelliccioni G A, Vecchiet F, Alessandri Bonetti G,Checchi L. A retentive system for intra-oral fluoride releaseduring orthodontic treatment. Eur J Orthod 1999; 21:695-701.
10. Featherstone J D B, Rodgers B E, Smith M W. Physiochemicalrequirements for rapid remineralisation of early cariouslesions. Caries Res 1981; 15: 221-235.
11. Welbury R R, Carter N E. The hydrochloric acid-pumicemicroabrasion technique in the treatment of postorthodontic decalcification. Br J Orthod 1993; 108: 181-185.
12. Elkhazindar M M, Welbury R R. Enamel Microabrasion. DentUpdate 2000; 27: 194-196.
13. Artun J, Thylstrup A. Clinical and scanning electronmicroscopic study of surface changes of incipient carieslesions after debonding. Scand J Dent Res 1986; 94: 193-201.
14. McGuinness N. Prevention in orthodontics — a review. DentUpdate 1992; 19: 168-175.
15. Meister R E. Comparison of enamel detachments afterdebonding between uniteck's dynalok bracket and a foilmesh bracket: a scanning electron microscope study. Am JOrthod 1985; 88: 266 (abstract).
16. Jones M. Enamel loss on bond removal. Br J Orthod 1980; 7: 39.
17. Swartz M L. Ceramic brackets. J Clin Orthod 1988; 22: 82-88.18. Atack N E. The orthodontic implications of traumatised upper
anterior teeth. Dent Update 1999; 26: 432-437.
19. Takla P M, Shivapuja P K. Pulpal response in electrothermaldebonding. Am J Orthod Dento Orthop 1995; 108: 623-629.
20. Zachrisson B U. Cause and prevention of injuries to teeth andsupporting structures during orthodontic treatment. Am JOrthod 1976; 69: 285-300.
21. Brezniak N, Wasserstein A. Root resorption after orthodontictreatment Part I Literature review. Am J Orthod 1993; 103:62-66.
22. Hendrix I, Carels C, Kuijpers-Jagtman A M, Van 'T Hof M. A radiographic study of posterior apical root resorption inorthodontic patients. Am J Orthod Dento Orthop 1994; 105:345-349.
23. Shirazi M, De Hpour A R, Jafari F. The effect of thyroidhormone on orthodontic tooth movement in rats. J Clin PaedDent 1999; 23: 259-264.
24. Loberg E L, Engstrom C. Thyroid administration to reduceroot resorption. Angle Orthod 1994; 64: 395-399.
25. Diamanti-Kipioti A, Gusberti F A, Lang N P. Clinicalmicrobiological effects of fixed orthodontic appliances. J Clin Perio 1987; 14: 326-333.
26. Gjerdet N, Erichsen E S, Remlo H E, Evjen G. Nickel and iron insaliva of patients with fixed orthodontic appliances. ActaOdont Scand 1991; 49: 73-78.
27. Natrass C, Ireland A J, Lovell C R. Latex allergy in anorthodontic patient and implications for clinicalmanagement. Br J Oral Maxillofac Surg 1999; 37: 11-13.
28. Booth-Mason S, Birnie D. Penetrating eye injury fromorthodontic headgear: a case report. Eur J Orthod 1988; 10:111-114.
29. Luther F. Orthodontics and the temperomandibular joint:where are we now? Part 1 Orthodontic treatment andtemperomandibular disorders. Angle Orthod 1998; 68:295-304.
30. Davies S J, Gray R M J, Sandler P J, O'Brien K D. Orthodonticsand occlusion. Br Dent J 2001; 191: 539-549.
31. Rushing S E, Silberman S L, Meydrech E F, Tuncay O C. Howdentists perceive the effect of orthodontic extraction onfacial appearance. J Am Dent Assoc 1995; 126: 769-772.
32. Boley J C, Pontier J P, Smith S, Fulbright M. Facial changes inextraction and non extraction patients. Angle Orthod 1998;68: 539-546.
33. DiBiase A T, Sandler P J. Does Orthodontics damage faces?Dent Update 2001; 28: 98-104.
34. Ackerman J L, Proffit W R. Soft tissue limitations inorthodontics: treatment planning guidelines. Angle Orthod1997; 67: 327-336
35 Khurana M, Martin M V. Orthodontics and infectiveendocarditis. Br J Orthod 1999; 26: 295-298.
36. Hobson R S, Clark J D. Management of the orthodonticpatient at risk from infective endocarditis. Br Dent J 1995;178: 289-295.
Guest leaders
Guest leaders in the BDJ are there to provide an opportunity for anyone involved indentistry (including patients) to write an appropriate comment for publication.These are published to accompany the usual Leader from the Editor
Submissions must be between 200 and 500 words, typed and double-spaced.Name, address and telephone number should be supplied, as well as your positionin the dental world.
For further help and guidance, please contact:
The Editor, British Dental Journal, 64 Wimpole Street, London W1G 8YS or
E-mail: [email protected]
02p71-77.qxd 18/12/2003 15:37 Page 77
usha
Rectangle

BRITISH DENTAL JOURNAL VOLUME 196 NO. 3 FEBRUARY 14 2004 143
PRACTICE
Orthodontics. Part 7: Fact and fantasy in orthodonticsP. Williams1, D. Roberts-Harry2 and J. Sandy3
Clinical research has previously lacked good methodology and much opinion was based onanecdote which is widely regarded as the weakest form of clinical evidence. There are fewrandomised control trials in orthodontics which support or refute areas of dogma. Thenumber of randomised control trials is increasing significantly. There is currently howeverno good evidence that orthodontics causes or cures temporomandibular joint dysfunction,that appropriate extractions in orthodontics ruin patients' profiles, or that the orthodontistis able to significantly influence facial growth with appliances.
1Specialist Registrar in Orthodontics,3Professor of Orthodontics, Division ofChild Dental Health, University of BristolDental School, Lower Maudlin Street,Bristol BS1 2LY; 2*Consultant Orthodontist,Orthodontic Department, Leeds DentalInstitute, Clarendon Way, Leeds LS2 9LU *Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4810935© British Dental Journal 2004; 196:143–148
● There is no good evidence that orthodontics cures or causes temporomandibular jointdysfunction
● Extracting teeth does not inevitably result in an altered profile● There is a need for better quality research in many of the controversial areas in orthodontics
I N B R I E F
Orthodontics, like other fields of medicine anddentistry has its fair share of controversies.Some of these controversies have haunted theprofession since its inception and some indi-viduals may be reluctant to change their treat-ment philosophies in the light of new clinicalevidence.
Orthodontics has evolved from many years ofclinical experience, in which the opinions ofrespected individuals during the birth of the spe-ciality have determined how orthodonticsshould be practised. A problem with this form ofteaching is that it is based on anecdotal experi-ence rather than sound scientific evidence. Newresearch often highlights inadequacies in thesefundamental teachings, eventually leading to achange in clinical practice. A trend is emergingtowards evidence-based rather than opinion-based decisions as more and more structuredresearch is published.
EVIDENCE-BASED DECISIONSEvidence-based dentistry can be defined as: ‘theconscientious, explicit, and judicious use of cur-rent best evidence in making decisions about thecare of individual patients’.1 The ‘gold standard’is strong evidence from at least one publishedsystematic review of multiple well-designed ran-domised controlled trials. Meta-analysis is aform of systematic review looking at all the rele-vant literature whether good, bad or indifferentand producing a single estimate of the clinicaleffectiveness. The advantage of meta-analysis isthat it summarises the available evidence andbecause of its systematic nature it can beappraised rapidly and applied to patient care.2
There are various levels of evidence beneaththe ‘gold standard’, of which the weakest is anec-dotal evidence. In the field of orthodontics thereare few well-designed randomised controlled tri-als which lend themselves to a systematicreview. Currently there are two such reviews,namely the change of intercanine width follow-ing orthodontic treatment and the treatment ofposterior crossbites.3,4
Recently, media attention has focused onviews made by a small number of orthodontistsand general dental practitioners on the adverseeffects of conventional orthodontic treatment.Much of this has centred on the role of extract-ing teeth as part of orthodontic therapy to alignteeth, retract protrusive incisors and to camou-flage dentally any skeletal disharmoniesbetween the mandible and the maxillae.
ORTHODONTICS AND TEMPOROMANDIBULARDYSFUNCTIONRelatively recently, orthodontists have beenconcerned about the possibility of a link betweenthe orthodontic treatment they provide and tem-poromandibular dysfunction (TMD) which is a
7
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
Summary of evidence-based dentistry• Anecdotal evidence is the weakest
form of evidence • ‘Gold standard’ is a randomised
controlled trial • Orthodontics has little ‘gold standard’
evidence
VERIFIABLE CPD PAPER
NOW AVAILABLE AS A BDJ BOOK
03p143-148.qxd 12/01/2004 11:24 Page 143

PRACTICE
144 BRITISH DENTAL JOURNAL VOLUME 196 NO. 3 FEBRUARY 14 2004
common finding in the population. Longitudinalstudies show that the prevalence of signs andsymptoms of TMD increases with age and thatthe prevalence of signs is greater than the preva-lence of symptoms. It has a variable incidence inan adolescent population between 5–35%.5
Most of the attempts at relating TMD toorthodontic treatment have been based on anec-dotal evidence or retrospective studies,approaches that cannot demonstrate a cause andeffect relationship between treatment and dis-ease. An opinion held by a few was that occlusalinterferences induced by orthodontic treatmentwould lead to TMD. This extended to the sugges-tion that orthodontic treatment is needed forthose whose occlusion is not functionally opti-mal to prevent the development of TMD. A func-tional occlusion was defined as one in whichintercuspal position should coincide withretruded contact position, there should not beany balancing side interferences and thereshould be anterior and canine guidance. Guide-lines such as these are often referred to as treat-ing to a ‘functionally optimal occlusion’ andwere advocated by a group of ‘functional ortho-dontists’. One viewpoint from a group of ‘func-tional orthodontists’ is that when premolar teethare extracted for orthodontic treatment thisleads to TMD because of over retracting theupper incisors during space closure, forcing thecondyle into a posterior position. It is this poste-rior position of the condyle within the fossa,which is presumed to cause an anteriorly dis-placed disc and therefore TMD.6 It was alsobelieved that occlusal interferences would leadto TMD, as well as tooth wear, periodontal dis-ease and instability of tooth position after ortho-dontic treatment if the position of the condylewas not ‘rear most, mid most and upper most’.Roth demonstrated that the symptoms of TMDcould be resolved once they were equilibratedwith occlusal positioning splints.7 However,these conclusions were reached after Roth hadevaluated only nine patients post treatment andtwo of these acted as controls.
The debate concerning a relationshipbetween orthodontic treatment and TMD cameto a head in 1987 following a lawsuit, Brimm vsMalloy, in which it was claimed that orthodontictreatment had caused TMD in a patient. Duringthe trial, the lack of good scientific evidenceinvestigating the effects of orthodontic treat-ment and TMD was highlighted and promptedthe formation of the American Association ofOrthodontics Temporo Mandibular JointResearch Programme. This is perhaps the firsttime that orthodontists realised the lack ofobjective, scientific research into the effects oforthodontic treatment. Only recently hasstronger evidence been forthcoming in assessingthe role of orthodontic treatment with respect toTMD.
A number of studies have examined the posi-tion of the condyle and its relationship withTMD. They found that individuals with ‘normal’joints (ie none have reported any signs or symp-
toms of TMD) had condyles that could beobserved, randomly distributed, in anterior, cen-tric and posterior positions in the glenoid fossa.8
A posterior position of the condyle within theglenoid fossa cannot therefore be taken as proofof TMD.
When orthodontic treatment involves theextraction of upper first premolar teeth and theretraction of the upper incisors some have sug-gested that this predisposes the patient to TMDby posteriorly positioning the condyle. Somelight has been shed on this position in a study of42 patients with a Class II Division 1 malocclu-sion treated by the extraction of both upper firstpremolars and fixed appliances. Seventy per centshowed a forward movement of mandibularbasal bone and the changes in condylar positiondid not correlate with incisor retraction (ie ortho-dontic treatment caused a transitory forwardposition of the condyle in the intercuspal posi-tion with a return to the pretreatment positionafter treatment). It was therefore concluded thatorthodontic treatment involving the loss of pre-molar teeth did not cause TMD and this has beensupported by the finding of other workers.9,10
The suggestion that orthodontic treatmentcauses a posteriorly positioned condyle, whichin turn leads to TMD, appears to be ill founded.The clinical studies published so far concludethat orthodontic treatment has no role in wors-ening or causing TMD when treated patients arecompared with untreated patients with or with-out a malocclusion.11
The final question that should be addressed isthe need to treat our orthodontic cases to a‘functionally optimal occlusion’. There is littleclinical evidence to suggest that such an occlu-sion has any benefits in terms of reducing thefollowing:• Tooth wear• TMD• Periodontal disease• Instability of tooth position
Indeed intercuspal position rarely coincideswith retruded contact position in a good occlu-sion and it has yet to be shown that canine guid-ance has an effect of preventing or curing TMD.A natural dentition with canine guidance willtend to become group functioning with time asthe canines wear. Furthermore canine guidancedoes not seem to offer any protection againstTMD.12
Although canine guidance is often advocatedas the functioning mode of choice, it is often anunobtainable aim for a substantial proportion oforthodontic patients. A study investigating thefrequency of group function and canine guid-ance patterns of occlusion as related to theFrankfort-mandibular plane angle found thefollowing. It showed a positive relationshipbetween canine guidance and low Frankfort-mandibular plane angles and of group functionto high Frankfort-mandibular plane angles.13
This would suggest that facial morphology mayindicate which functional goal to aim for.
Temporomandibularjoint problems arenot caused or curedby orthodontic treatment
Litigation forcedorthodontists intogenerating objectivescientific researchinto the effects oforthodontic treatment
03p143-148.qxd 12/01/2004 10:25 Page 144

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 3 FEBRUARY 14 2004 145
There are no clear occlusal objectives fororthodontic treatment although there are manyocclusal goals which have been suggested.Occlusal goals are those directed at the relation-ship of the teeth both in static intercuspal posi-tion and during function. Andrews introducedhis six keys to a normal occlusion as a means ofobtaining a static intercuspal position that isseen as ideal.14 A summary of these six keys isgiven below:• Class I molar relationship• Correct crown angulation• Correct crown inclination• No rotated teeth• No interdental spaces• Flat occlusal plane
In practice, orthodontically treated occlu-sions seldom achieve all occlusal keys becauseof differences in skeletal pattern and tooth sizediscrepancies.15 It has however been shown thatwell intercuspated teeth may be more stable andless likely to relapse.16
There is a general agreement that intercuspalposition should coincide with retruded contactposition although there is a disagreement as tohow closely they should coincide. The majorityof the population have been shown to exhibit adiscrepancy between the two positions with noill effects. It seems sensible therefore to acceptsmall discrepancies of approximately 1 mm orso of each other.
THE EXTRACTION VERSUS NON-EXTRACTIONDEBATEThe extraction of teeth as part of orthodontictreatment continually causes controversy. Teethare extracted for several reasons in orthodontics.The most common reason for extraction is therelief of crowding and the need to create space togain good alignment of the teeth. The reductionof overbite and the correction of an increasedoverjet to obtain a Class I incisor relationship arealso important issues to consider where extrac-tions will be required.
Edward Angle was very influential during the1890s in developing orthodontics as a speciality,with himself as the ‘father of modern orthodon-tics’. He is credited with much of the develop-ment in the concept of occlusion in the naturaldentition and a classification of malocclusion.
Angle believed in non-extraction orthodontictreatment and that every person had the poten-tial for an ideal relationship of all 32 teeth. Hewas also concerned with the ideal facial aesthet-ics which he felt could be achieved when thedental arches had been expanded so that all theteeth were in ideal occlusion. Angle did notcome to this expansion philosophy through clin-
ical research but was convinced by the ideas ofinfluential people of his time, namely Rousseauand Wolff. It was felt by Rousseau, a philoso-pher, that many of the ills of modern man weredue to the environment we now live in andemphasised the ‘perfectibility of man’. Thereforefrom an orthodontic perspective, a perfectocclusion could never be achieved by the extrac-tion of teeth. In the early 1900s Wolff, a physiol-ogist, demonstrated that remodelling of bonecould occur in response to functional loading.Angle therefore reasoned that if teeth wereplaced in a proper occlusion, forces transmittedto the teeth would cause bone to grow aroundthem. He went as far as describing his edgewiseappliance as the ‘bone growing appliance’. Anyrelapse seen in any of his treated cases wasattributed to an inadequate occlusion.
It was not until the 1930s and the 1940s thatthis non-extraction rule advocated by Anglewas challenged by Tweed and Begg. They bothfelt that a malocclusion was an inherited condi-tion and dismissed the notion about the ‘per-fectibility of man’. Tweed argued about the poorlong term stability of expanded dental archesand decided to retreat many of Angles cases byextracting four first premolars. He publiclydemonstrated 100 consecutively treated patientsclaiming a more stable occlusion after extrac-tion based treatment. An appliance system wascreated by Begg, which was designed to be usedon extraction based treatments, which popu-larised this treatment approach.
The extraction debate has reopened recently,especially in North America, because of con-cerns of litigation if extraction based treatmentphilosophies are used. In recent years there hasbeen a trend towards non-extraction treatmentas studies have shown that even cases treatedwith the extraction of first premolars are notguaranteed a stable result.17
DOES EXTRACTING TEETH DAMAGE FACES?Some practitioners in recent years have shownanecdotal evidence that extracting teeth fororthodontic purposes ruins a patient’s profileand compromises their facial aesthetics. It hasbeen claimed that the orthodontic extraction ofteeth may cause less attractive smiles with darkbuccal spaces lateral to the buccal segments,known as the ‘dark buccal corridor’, and also bythe retraction of the upper incisors when closing
Orthodontic treatment on an extraction or non-extraction basiswill still show somerelapse in most cases
Summary of orthodontics and TMD• Extracting teeth does not cause
a posteriorly positioned condyle• Orthodontics does not cause TMD
Summary of the extraction versus non-extraction debate• Changing trends over the years in
extraction/ non-extraction based treatment
• Arch expansion shows worst levels ofrelapse
• Extracting teeth does not guaranteefuture stability
• Each case should be properly treatmentplanned to give greatest future stability
03p143-148.qxd 12/01/2004 10:26 Page 145

PRACTICE
146 BRITISH DENTAL JOURNAL VOLUME 196 NO. 3 FEBRUARY 14 2004
the remaining extraction spaces giving a ‘dishedin’ aged appearance.
These practitioners advocate a non-extrac-tion approach to treatment on the basis that itwill produce a more youthful, protrusive facialprofile — a view held by Angle some one hun-dred years ago. The opinion that non-extractiontreatment is better than extraction treatmentwhen assessing facial attractiveness is clearlymisinformed given the studies that have nowbeen carried out.
There is a relationship between retraction ofthe upper incisors and the posterior movementof the upper lip but for any given individual thisis unpredictable. Indeed, when the upper incisorsare retracted by 5 mm it has been shown there ison average 1.4 mm posterior movement of theupper lip.9 Those patients treated on an extrac-tion basis have been found to have slightly moreprominent lips compared with those treated on anon-extraction basis at the end of treatment.18,19
It is of note to mention that in the extractiongroup they tended to have more prominent lipsbefore commencing treatment because of anincreased overjet, an important considerationwhen treatment planning these patients. Thereare many patients who have been treated on anon-extraction basis with a ‘dished in’ appear-ance and many other patients with fuller profileswho have had four teeth extracted as part oftheir orthodontic treatment. An important con-sideration before deciding on whether treatmentis going to proceed on an extraction or non-extraction basis is the profile of the patientbefore treatment. It is important at this initialstage of assessment and planning to identifywhich patients are vulnerable to worsening analready flat or ‘dished in’ profile as they maynot be amenable to orthodontic treatment aloneand may require a combined surgical andorthodontic approach.
A question frequently raised is that of the dif-ferences in facial appearance if the same mildlycrowded case was treated on an extraction ornon-extraction basis. What would we expect tosee at the end of treatment? One such retrospec-tive study has addressed these issues byanalysing the impact of extractions on the lipmorphology in borderline Class II Division 1malocclusions. In the extraction group wherefour first premolars were removed the lowerincisors were on average 2 mm posterior and thelower lip 1.2 mm posterior when compared witha non-extraction group. It was seen that thenon-extraction group had 2 mm fuller profile,although both groups were happy with their aesthetic appearance.19
Clinicians tend to be very critical about thechanges, both in terms of the hard and soft tis-sues, which are brought about as a result oforthodontic treatment whether or not extrac-tions have been carried out. Therefore the gener-al public's perception about the profile of ourpatients after treatment should be given somethought. A timely and relevant study of the public's perception of the changes in profile of
patients treated for a Class II Division 1 maloc-clusion concluded that they preferred the profilechanges more in the extraction group comparedwith the non-extraction group. There was nopreference for the profiles for either group twoyears after treatment.20 It would seem then thatthere is no evidence to suggest that extractionbased treatment when prescribed correctly‘damages faces’.
SHOULD WE EXTRACT SECOND MOLARS ASPART OF ORTHODONTIC TREATMENT?There are said to be many advantages in extract-ing second molars as part of orthodontic treat-ment. These advantages include the following:
• Less detrimental to facial profile• Facilitates the eruption of third molars• Spontaneous relief of crowding in the premo-
lar region• Prevents crowding in a well aligned lower
arch• Aids distal movement of the buccal segments
with extra oral traction• Shorter treatment time • Functional occlusion is better
It can be seen that it is an impressive list ofadvantages! There are however several consider-ations that need to be taken into account beforeextracting second molar teeth with radiologicalevaluation of third molar development essential.All third molars should be present, and havegood size, shape and position.
The idea that extracting second molars is lessdetrimental to the facial profile is an interestingconcept, given that the tooth to be extracted is ina more posterior position in the mouth com-pared with premolar teeth and is thereforethought less likely to adversely affect soft tissueprofile. One study investigated this claim bycomparing the effects of different extractionpatterns on the facial profile between twogroups, those treated by first premolar extrac-tion and those by second molar extraction. Theyfound the average decrease in the soft tissueangle of facial convexity of 1.7° for the secondmolar extraction group and 2.2° for the first pre-molar group. However, these reductions werenot statistically significant and it must beremembered that these patients were not derivedfrom the same population, as they were not ran-domised to one of the extraction patterns.21
The ideal time for extracting second molarsis controversial, some studies have suggestedthe best time to extract them is when the third
Summary of extracting teeth anddamaged faces• No evidence to suggest that extracting
teeth in appropriate cases causes a‘dished in’ appearance
• Lay opinion finds both extraction andnon-extraction treatment equally pleasing
Lay populations andpatients cannot perceive significantprofile changes after appropriate orthodontic treatment which mayor may not involveorthodontic extractions
03p143-148.qxd 12/01/2004 10:27 Page 146

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 3 FEBRUARY 14 2004 147
molar crown is fully formed and others claimthey should be extracted as soon as they eruptinto the mouth. The evidence suggests that theimportance of timing second molar extractionsis not yet known. One disadvantage of extract-ing second molars is the ‘predictably unpre-dictable’ nature of third molar developmentand eruption. A number of studies have shownthat third molar eruption is often unsatisfactory,including improper angulation and contactrelationship with the first molar. This is seenranging from 4–25% of cases22 and raisesdoubts on the length of treatment time for sec-ond molar extraction cases compared with otherextraction strategies. The loss of second molarteeth obviates the need for space closingmechanics but a second course of treatmentmay be required to orthodontically uprightthird molars at a stage in late adolescence whenco-operation may not be at its best.
An important reason for elective extractionsin orthodontics is the relief of crowding. Firstpremolar teeth are ideally located as they pro-vide up to 14 mm of space for the relief ofcrowding both anteriorly and posteriorly to theextraction site. Second molar teeth can providesome 18–22 mm of space, of which little is madeavailable to the relief of crowding in the lowerlabial segment where crowding most oftenoccurs. Given that arch length deficienciesrarely exceed 10 mm the removal of a secondmolar tooth and the space it provides seems a lit-tle excessive. However, if the premolar region iscrowded by 4–5 mm then the removal of secondmolar teeth may provide sufficient space forspontaneous relief of premolar crowding. Therelief of molar crowding in the early permanentdentition is an indication to extract secondmolars and it may also prevent late lower archcrowding.23
Many of the advantageous claims made forthe extraction of second molar teeth are unsub-stantiated. There is no evidence to suggest thattreatment times are shorter, that distal move-ment of the first maxillary molar is enhancedand that there is less effect on the soft tissueprofile. The benefits of extracting secondmolars appear to be relief of mild premolarcrowding in the early permanent dentition buteruption of the third molar needs carefulreview and the possibility of a later additionalcourse of orthodontic treatment needs to bemade clear to the patient.
THE ‘ORTHOPAEDIC EFFECT’ —CAN WE INFLUENCE GROWTH?The potential to influence growth, whether it ispromoting growth in a Class II malocclusion orrestricting growth in a Class III malocclusion,remains an area of significant controversy. A number of studies have looked into the possi-bility of modifying growth with orthopaedicappliances and the results are liberally interpret-ed to suit the position of the challenger. An‘orthopaedic effect’ is taken to mean a change inthe position of the cranio-facial skeleton in rela-tion to each other as the result of orthodontictreatment. This change should be permanent inits amount and direction.
Functional appliances have been used formany years for the correction of Class II maloc-clusions. Despite this long history there contin-ues to be much debate relating to their use, modeof action and effectiveness. Undoubtedly, nor-mal dentofacial growth has a genetic drive butmay be influenced by environmental factors.There is no doubt that functional appliances canrapidly correct Class II malocclusion but thisdoes not indicate or prove an ‘orthopaediceffect’.
Some practitioners like to claim they can‘grow mandibles’, but what is the evidence?Many studies find an increase in mandibularlength of 1—2 mm per annum during activetreatment.24 Much of the work demonstratingthe ability of functional appliances to stimulatemandibular growth is based on animal experi-mentation. A maximum of 5—15% increase inmandibular length by stimulating condylargrowth can be expected in experimental animalsunder controlled conditions and during periodsof active growth.25 Animal experimentalresearch is often cited as evidence but cautiousinterpretation of the results is required before itis applied to patients.
There is evidence from prospective ran-domised controlled trials that the effects of func-tional appliances may be transient, with rever-sion to pretreatment growth patterns over theshort or long term.26 Therefore this short-termgrowth enhancement is useful to correct incisorand molar relationships but does not result in alonger mandible. They produce their effectsmainly by dentoalveolar changes such as retro-clination of upper incisors and proclination ofthe lower incisors.27
An orthopaedic change has also beenattempted in Class III malocclusions where it islargely assumed that the fault lies with a prog-nathic mandible. Hence chin cup treatment,once popular, was directed at restraining furthermandibular growth and allowing maxillarygrowth to ‘catch up’ and therefore correct theanterioposterior component of a Class III maloc-clusion. A long-term study looking at the effect ofchin cup therapy found that it was effective inreducing mandibular prognathism before pubertybut this was then lost after puberty ie a short-term gain similar to that seen with functionalappliances. Indeed, there was no difference in
Summary on the extraction of secondmolars• Many of the claimed advantages are
unsubstantiated• Evidence suggests relief of molar and
premolar crowding is an indication• Third molar development is ‘predictably
unpredictable’ and may need furthertreatment to orthodontically uprightthem
The orthodontist'sability to influencefacial growth is limited and much ofthe change that isseen relates to dentoalveolar changes
03p143-148.qxd 12/01/2004 10:27 Page 147

PRACTICE
148 BRITISH DENTAL JOURNAL VOLUME 196 NO. 3 FEBRUARY 14 2004
the final skeletal profile of the mandible betweentreatment groups and control groups who didnot receive treatment.28
However, there appears to be a promisingmethod of achieving an ‘orthopaedic effect’ withthe use of protraction headgear. Several workershave shown that a small but significant anteriormovement of the maxillae using protractionheadgear during the mixed dentition is possiblewhich has remained stable some 2 years aftertreatment.29
In summary, orthodontic appliances thatdeliver an orthopaedic effect may induce a tem-porary improvement in the skeletal relationship.There is no evidence at present to show thatorthodontic treatment can effectively restrain orenhance cranio-facial growth that is otherwiseinherited by the individual.30
We have chosen four areas of smoulderingcontroversy, not to rekindle historic argumentsor generate a new turf war but to illustrate thesomewhat flimsy evidence both sides of an argu-ment can use. Forceful opinion currently domi-nates any cautious interpretation of the existingliterature. Given time, the quality of the data andresearch will improve and as a consequencemore definitive statements on true effects oftreatment will be possible.
1. Haynes R B, Richardson W S. Evidence based medicine: whatit is and what it isn't. Br Med J 1996; 312: 71-72.
2. Richards D, Lawrence A. Evidence based dentistry. Br Dent J1995; 179: 270-273.
3. Harrison J E. Ashby D. Orthodontic treatment for posteriorcrossbites (Cochrane Review). Cochrane Database Syst Rev2001; 1: CD000979.
4. Burke S P, Silveira A M, Goldsmith L J, Yancey J M, VanStewart A, Scarfe W C. A meta-analysis of mandibularintercanine width in treatment and postretention. AngleOrthod 1998; 68: 53-60.
5. Proffit W. Contemporary Orthodontics. 3rd ed. St Lewis:Mosby-Year book, 1999.
6. Witzig J W, Spahl T J. The clinical management of basicmaxillofacial orthopaedic appliances. Vol 2 Diagnosis.pp221-224. Boston: PSG Publishing, 1987.
7. Roth R. Temporomandibular pain-dysfunction and occlusalrelationships. Angle Orthod 1973; 43: 136-153.
8. Ren Y F. et al. Condyle position in the temporomandibular
joint. Comparison between asymptomatic volunteers withnormal disk position and patients with disk displacement.Oral Surg, Oral Med, Oral Path, Oral Radiol, Endo 1995; 80:101-107.
9. Lueke P E, Johnston L E. The effect of first premolarextraction and incisor retraction on mandibular positions:testing the central dogma of ‘functional orthodontics’. Am JOrthod Dentofac Orthop 1992; 101: 4-12.
10. Gianelly A A. et al. Condylar position and maxillary firstpremolar extraction. Am J Orthod Dentofac Orthop 1991; 99:473-476.
11. Luther F. Orthodontics and the temporomandibular joint:Where are we now? Angle Orthod 1998; 68: 295-317.
12. Bush F M. Malocclusion, masticatory muscle andtemporomandibular joint tenderness. J Dent Res 1985; 64:129-133.
13. DiPetro G J. A study of occlusion as related to the Frankfort-mandibular plane angle. J Prosthetic Dent 1977; 38: 452-458.
14. Andrews L F. The six keys to normal occlusion. Am J Orthod1972; 62: 296-309.
15. Kattner P F, Schneider B J. Comparision of Roth applianceand standard edgewise appliance treatment results. Am JOrthod Dentofac Orthop 1993; 103: 24-32.
16. Lloyd T G, Stephens C D. Changes in molar occlusion afterextraction of all first premolars: A follow up study of Class IIdivision 1 cases treated wth removable appliances. Br J Ortho1990; 6: 91-94.
17. Little R M. An evaluation of changes in mandibular anterioralignment from 10 to 20 years postretention. Am J Orthod1988; 93: 423-428.
18. James R D. A comparative study of facial profiles inextraction and nonextraction treatment. Am J OrthodDentofac Orthop 1998; 114: 265-276.
19. Paquette D E et al. A long term comparison of nonextractionand premolar extraction edgewise therapy in ‘borderline’Class II patients. Am J Orthod Dentofac Orthop 1992; 102: 1-14
20. Bishara S E., Jakobsen J R. Profile changes in patients treatedwith and without extractions: Assessments by lay people. AmJ Orthod Dentofac Orthop 1997; 112: 639-644.
21. Staggers J A. A comparison of second molar and firstpremolar extraction treatment. Am J Orthod Dentofac Orthop1990; 98: 430-436.
22. Gooris C G M. et al. Eruption of third molars after secondmolar extractions: A radiographic study. Am J OrthodDentofac Orthop 1990; 98: 161-167.
23. Richardson M E. Lower molar crowding in the earlypermanent dentition. Angle Orthod 1985; 55: 51-57.
24. Lagerstrom L. Dental and skeletal contributions to occlusalcorrection in patients treated with high pull headgear-activator combination. Am J Orthod Dentofac Orthop 1990;97: 495-504.
25. McNamara J A. Skeletal and dental changes followingfunctional regulator therapy on class II patients. Am J Orthod1985; 88: 91-110.
26. De Vincenzo J P. Changes in mandibular length before,during and after successful orthopaedic correction of Class IImalocclusion using a functional appliance. Am J OrthodDentofac Orthop 1991; 99: 214-257.
27. Bishara S E. Functional Appliances: A review. Am J OrthodDentofac Orthop 1989; 95: 250-258.
28. Suagawara J. Long term effects of chincap therapy onskeletal profile in mandibular prognathism. Am J OrthodDentofac Orthop 1990; 98: 127-133.
29. Ngan P. Cephalometric and occlusal changes followingmaxillary protraction and expansion. Eur J Orthod 1998; 20:237-254.
30. Chate R A. The burden of proof: a critical review oforthodontic claims made by some general practitioners. Am JOrthod Dentofac Orthop 1994; 106: 96-105.
Summary of the current evidence on the‘orthopaedic effect’• Orthodontic treatment cannot influence
growth in the long term• Any gain is small but is often lost in the
long term• Majority of the ‘orthopaedic effect’ is
dentoalveolar tipping of the teeth
03p143-148.qxd 12/01/2004 10:28 Page 148

BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004 195
PRACTICE
Orthodontics. Part 8: Extractions in orthodonticsH. Travess1, D. Roberts-Harry2 and J. Sandy3
Extractions in orthodontics remains a relatively controversial area. It is not possible to treat allmalocclusions without taking out any teeth. The factors which affect the decision to extractinclude the patient's medical history, the attitude to treatment, oral hygiene, caries rates andthe quality of teeth. Extractions of specific teeth are required in the various presentations ofmalocclusion. In some situations careful timing of extractions may result in spontaneouscorrection of the malocclusion.
1Senior Specialist Registrar in Orthodontics;3Professor of Orthodontics, Division ofChild Dental Health, University of BristolDental School, Lower Maudlin Street, BristolBS1 2LY; 2*Consultant Orthodontist,Orthodontic Department, Leeds DentalInstitute, Clarendon Way, Leeds LS2 9LU*Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4810979© British Dental Journal 2004; 196:195–203
● The extraction of teeth for orthodontic purposes has always been a controversial area. It isnot possible to treat all malocclusions without taking out teeth
● Where extractions are indicated, first premolars are most commonly extracted but there arereasons for extracting elsewhere in the arch and this will involve other teeth
● The use of fixed appliances has considerably changed extraction viewpoints
I N B R I E F
The role of extractions in orthodontic treatmenthas been a controversial subject for over a cen-tury. It is fair to say that even today, opinion isdivided on whether extractions are used too fre-quently in the correction of malocclusion.
Angle1 believed that all 32 teeth could beaccommodated in the jaws, in an ideal occlusionwith the first molars in a Class I occlusion, iewith the mesiobuccal cusp of the upper firstmolar occluding in the buccal groove of thelower first molar. Extraction was anathema tohis ideals, as he believed bone would formaround the teeth in their new position, accordingto Wolff's law.2 This was criticised in 1911 byCase who believed extractions were necessary inorder to relieve crowding and aid stability oftreatment.3
Two of Angle's students at around the sametime but in different countries considered theneed for extractions in achieving stable results.Tweed became disappointed in the results he wasachieving and decided to re-treat a number ofpatients who had suffered relapse followingorthodontic treatment (at no further cost) usingextraction of four premolar units.4
The demonstration of his results to the profes-sion in America resulted in a change of philoso-phy in the 1940s to extraction-based techniques.Begg, in Australia, studied Aboriginal skulls andnoted a large amount of occlusal and moreimportantly interproximal wear.5 He argued thatpremolar extractions were required in order tocompensate for the lack of interproximal wearseen in the modern Australian dentition,through lack of a coarse diet. He also developeda technique that relied on extractions to createmuch of the anchorage needed for treatment.
Recently, the extraction debate has reopened,with some individuals believing that expansionof the jaws and retraining of posture can obviatethe need for extractions and produce stableresults. These claims are for the most part unsub-stantiated. If teeth are genuinely crowded asopposed to being irregular then arch alignmentcan be achieved by one of the following:
• Enlargement of the archform • Reduction in tooth size• Reduction in tooth number
Arch expansion can be achieved by movingteeth buccally and labially (ie lateral and anterioposterior expansion) but the long-term stabilityand whether bone grows as teeth are movedthrough cortical plates remain contentiousissues. In the maxilla there is a suture whichremains patent in some patients into the seconddecade. This can also be used in expansion inthat it can be ‘split’ with rapid maxillary expan-sion. The split suture fills in with bone and thusa wider arch to accommodate teeth is created.There is no good evidence that this method ofexpansion produces a more stable result thanany other method. Longitudinal studies provideuseful guidance on whether arch expansionproduces stability. These are difficult studies toconduct but increasing mandibular length toaccommodate teeth relapses in nearly 90% ofcases with resulting unsatisfactory anteriortooth alignment.6
Reduction in tooth size, particularly in thelabial segments with interdental stripping, isanother potential mechanism to relieve crowd-ing. Variable relapse has been reported but onestudy noted relapse of some degree in all cases.7
8
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
VERIFIABLE CPD PAPER
NOW AVAILABLE AS A BDJ BOOK
04p195-203.qxd 27/01/2004 10:06 Page 195

PRACTICE
196 BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004
This work was done over 25 years ago and doesnot reflect contemporary use of inter-dentalenamel reduction or current retention regimes.
The reduction in tooth number is usuallyachieved with extractions and these cases ideallyneed to be compared with treated non extractioncases with spacing, cases treated by arch expan-sion to accommodate crowding and untreatednormal occlusions. In a review of these issues itwas concluded that arch length reduces in mostcases, including untreated normal occlusion.Any lateral expansion across the mandibularcanines decreases after treatment but this is alsoseen in those cases which have no orthodontictreatment. It was further recognised thatmandibular anterior crowding is a continuingphenomenon seen in patients into the fourthdecade and likely beyond.8 The degree of anteri-or crowding seen at the end of retention is vari-able and unpredictable.
Proffit9 in a 40-year review of extraction pat-terns showed 30% of cases were treated withextractions in 1953, 76% in 1968 and 28% in1993. He suggested the decline in extractionssince 1968 was because of concern over facialprofile, tempromandibular joint dysfunction(TMD) and stability; the change from the Beggappliance, largely an extraction-based techniqueto the straight wire technique, which seems torequire fewer extractions. The latter may alsoresult with a change in mindset and the use ofheadgear and prolonged retention.
A dogmatic approach is inadvisable andeach case must be assessed on its merits. Somecases, especially where the crowding is mildmay not need tooth removal, and a more sensi-ble approach based on the requirements of theindividual case rather that the two extremesseen in the past century is advised. Interesting-ly, in a follow up study over a 15 year period in
Scotland, orthodontics replaced caries as thecommonest reason for extraction in patientsunder 20 years of age.10 All extractions aretraumatic as far as the patient is concerned andclinicians will seek non-extraction solutionswhere possible. In the late mixed dentition,between 3 mm and 4 mm of space can be pre-served in the lower arch by simply fitting a lin-gual arch. If this is coupled with molar and pre-molar expansion of just 2 mm (with no lowercanine exapansion) and interdental enamelreduction between anterior contact points thena large proportion of otherwise ‘crowded’ casescan be treated without the loss of permanentteeth. The decision on whether or not to extractteeth is based on an assessment of many factorsincluding crowding, increase in overjet, changein arch width, curve of Spee, anchoragerequirements and other more esoteric factorsuch as adjusting the torque of the anteriorteeth. It is also worth mentioning that the con-cept of space analysis is probably underused inthe United Kingdom, but this is routinelyapplied elsewhere. This analysis enables arationale and methodical approach to treatmentplanning before extractions are recommend-ed.11 It is important then to realise that there area variety of options as far as mild to moderatecrowding cases are concerned.
FACTORS AFFECTING THE DECISION TO EXTRACTIt is important to consider the patient as a wholein treatment planning. Medical history, attitudeto treatment, oral hygiene, caries rate and thequality of the teeth are important. Patients withcardiac anomalies are at risk of complicationsduring orthodontic treatment and consultationwith a cardiologist is important. If necessary,extractions should be covered with appropriateantibiotics and impacted teeth may be bestremoved rather than aligned as traction tounerupted teeth may pose an increased risk tothese patients.12
The quality and prognosis of the teeth shouldbe carefully considered, as this may overrideother factors. Hypoplastic, heavily restored orcarious teeth should generally be removed inpreference to healthy teeth. This is especially truein the labial segments where aesthetics are diffi-cult to maintain with loss of an incisor or canine.
Teeth of abnormal form or size may be con-sidered for removal as they can look unsightlyand be difficult to align. For example, a dens-in-dente may compromise the long-term prognosisof a tooth, or a talon cusp may hinder arch co-ordination during treatment. Dilaceratedteeth should be carefully assessed to see if crownalignment is achievable. Often extraction ofthese teeth is the only option. Macrodont teeth,geminated or fused, need careful consideration(Fig. 1). The aesthetics are often poor but extrac-tion can result in an excess amount of space,which may prolong orthodontic treatment.Where supplemental teeth are present, extrac-tion may result in spontaneous correction of anycrowding (Fig. 2).
Fig. 1 Illustration of a macrodont tooth in the lower labial segment, which also exhibitsa talon cusp. Alignment and arch co-ordination is hindered by the size of the tooth andthe talon cusp. Some enamel reduction can be undertaken to reduce the width of thetooth but care must be taken not to breach the enamel. In the upper arch, reduction ofa talon cusp can help correct an increased overjet, although radiographic examinationof pulp chambers in the talon cusp is essential
04p195-203.qxd 27/01/2004 10:08 Page 196

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004 197
EASE OF EXTRACTION, AND THE PRESENCE OFIMPACTED TEETHThe extraction of teeth is a potentially traumaticexperience. The decision to extract should bemade with an awareness of the risks of treat-ment, including the psychological impact of theprocedure. The General Dental Council in itsguidance to dentists of professional and personalconduct makes it clear that dentists who referpatients for general anaesthesia must make itclear what justification there is for the proce-dure. The duties of the treating dentist include athorough and clear explanation of the risksinvolved as well as the alternative methods ofpain control available. The use of general anaes-thesia is usually considered in dealing withunerupted teeth, first molars, multiple extrac-tions in four quadrants and specific phobias.
If teeth are impacted or ectopically posi-tioned, extraction of an erupted tooth can guidethe path of eruption of the impacted tooth andobviate the need for minor oral surgery. Forexample, the impaction of a lower second pre-molar may be relieved by the removal of the firstpremolar or first molar, which only requireslocal analgesia and is less traumatic than theremoval of the impacted tooth (Fig. 3). InFigure 4, eruption of the upper second premolarsresulted in severe resorption of the roots of theupper first molars. Extracting these molarswould be fairly atraumatic and allow the secondpremolars to erupt into the mouth. Similarly, ifunerupted permanent canines are palatally posi-tioned judicious removal of the deciduouscanines can improve the path of eruption of thepermanent teeth and may help to avoid lengthyorthodontic treatment.13
CORRECTION OF OVERBITESpace closure with fixed appliances tends toincrease the overbite and therefore extractionsin the lower arch in deep bite cases should beundertaken with caution. In some malocclu-sions, where the anterior face height is reduced,extractions can make space closure difficult andgreat care must be taken in diagnosis before thisdecision is made. It is important to recognisewhether a case is genuinely crowded or whetherthe teeth are displaced lingually as in a Class IIDivision 2 case. Lingually displaced lower labialsegments are frequently not crowded, eventhough they may appear to be so.
Proclination of the lower labial segment alsoreduces the overbite, as well as overjet, and mayobviate the need for extractions. However, thistreatment approach should be undertaken cau-tiously as uncontrolled and excessive proclina-tion of the lower incisors can be unstable andshould only be undertaken in selected cases byexperienced clinicians. Flattening of an accen-tuated curve of Spee in order to reduce an over-bite, where proclination is contraindicated, doesrequire space, for which the extraction of lowerteeth can sometimes be considered. The spacerequired to flatten a curve of Spee has historicallybeen over rated, the amount of space required is
Fig. 2 A supplemental lower incisor (a) was removed,resulting in spontaneous correction of crowding in the lower labial segment (b)
Fig. 3 This case presented with missing upper first premolars and lower rightthird molar, with vertically impacted lower second premolars. (a) Both lowerfirst molars are heavily filled and would be ideal for extraction to alloweruption of the second premolars. However the missing third molar on theright resulted in extraction of the lower right first premolar and the lowerleft first molar. Spontaneous alignment occurred (b) with both impactedpremolars erupting successfully into the occlusion with no active treatment
a
a
b
b
04p195-203.qxd 27/01/2004 10:09 Page 197

PRACTICE
198 BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004
1–2 mm when the curve is severe and there is nocrowding. It is difficult then to justify extractingteeth purely for the sake of creating space toflatten an occlusal curve. The greatest challengeis the mechanical control of the teeth to preventexcessive proclination of the lower incisors. Thisusually occurs because the intrusion force is atsome distance labial to the centre of resistanceof the incisors and lingual crown torque is need-ed to prevent the labial movement of the inci-sors.
EXTRACTION OF SPECIFIC TEETHDespite the factors discussed above, certain teethare extracted preferentially for orthodontic rea-sons. A survey of extraction patterns in the hos-pital orthodontic service (Table 1) showed thatfirst premolars were most commonly extracted(59%) followed by second premolars (13%). Per-manent molars accounted for 19% of extractions(12% for first molars and 7% for second molars).Only 1% of patients had incisor extractions.14
The high percentage of premolar extractionsis related to their position in the arch and the
timing of their eruption. They are often ideal forthe relief of anterior and posterior crowding.However, each patient should be seen as an indi-vidual and their treatment planned according tothe merits of the malocclusion,
Lower incisorsIn general, removal of a lower incisor should beavoided, as the inter-canine width tends todecrease which can result in crowding develop-ing in the upper labial segment or the overjetincreasing. However, a number of situations doexist in which a lower incisor may be consideredas part of an orthodontic treatment plan andfixed appliances are generally required in thesecases. These include situations where a lowerincisor is grossly displaced from the arch form or'ectopic' and space is required to align the teeth.This is best considered in adults and especiallythose who have had previous loss of premolarunits in each quadrant and present with latelower labial segment crowding (Fig. 5). Class IIIcases at the limit of their growth can be camou-flaged with loss of a lower incisor, to allow thelower labial segment to be tipped lingually, cor-recting the incisor relationship. This also tendsto increase the overbite, which is helpful in thesecases.15 Treatment of Class I cases with moderatelower labial segment crowding of up to 5 mm (iethe size of a lower incisor) may be treated withloss of a lower incisor. An increase in overjet or aslightly Class III buccal segment relation may bean undesirable side effect.16 Cases where a toothsize discrepancy exists, for example with upperpeg shaped laterals or missing upper lateral inci-sors may also benefit from the loss of a lowerincisor. A Bolton analysis (a measure of tooth
Fig. 4 In this case, the erupting uppersecond premolars showed some resorptionof the mesial roots of the upper firstmolars. (a) Progressive resorption of themesial roots of the molars was seen onsubsequent radiographs (b), whichprogressed to such an extent (c) that bothupper first molars required extraction,allowing eruption of the second premolars
Table 1 Table of percentage extractions according totooth typeTooth % removed
Central incisor 1
Lateral incisor 3
Canine 4
First premolar 59
Second premolar 13
First molar 12
Second molar 7
a b
c
04p195-203.qxd 27/01/2004 10:10 Page 198

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004 199
size discrepancies) may be used to analyse theextent of the disproportion. A Kesling set up17
(where the anterior teeth are sectioned from aplaster model and re-positioned in wax as a trialset up, having left out a lower incisor) may behelpful in predicting the final outcome (Fig. 6).
Upper IncisorsUpper incisors are rarely the extraction of choiceto treat a malocclusion. However, the upper labialsegment is particularly at risk from trauma,especially in Class II Division 1 cases with largeoverjets. In situations where the long-term prog-nosis of an incisor is poor, for example, the inci-sor is non vital, root filled, dilacerated or ofabnormal form, the tooth should be consideredfor extraction as part of the orthodontic treat-ment plan. Full consideration should be given tothe resulting occlusion and aesthetics. Placing alateral incisor in a central incisor position rarelygives a good result because the root of the toothis narrow and the emergence angle of the builtup crown is poor. In some cases transplantationof a premolar with a developing root into theincisor socket can relieve crowding in the lowerarch and provide a useful replacement in theupper labial segment (Fig. 7).
Where lateral incisors are diminutive ormissing, space closure or space maintenancecan be considered more equally. Attentionmust be paid to the shape, size, gingival heightand colour of the canine if a good aestheticresult is to be achieved. In many cases thecanines can be disguised as lateral incisors byselective grinding, and where appropriate, aes-thetic build-ups.
CaninesThese teeth are rarely considered for extractionunless very ectopic (Fig. 8). The loss of a caninemakes canine guidance impossible and maycompromise a good functional occlusal result.Contact between a premolar and lateral incisor isoften poor and canines can act as ideal abutmentteeth because of their long root length and resist-ance to periodontal problems. Palatally ectopiccanines can sometimes be in unfavourable posi-tions for alignment, and lower ectopic caninesoften require extraction rather than alignment.In many of the former cases the first premolarcan be aligned with a mesial inclination androtated mesio-palatally to hide the palatal cuspand provide a better aesthetic result.
PremolarsPremolars are often ideal for the relief of bothanterior and posterior crowding, the first andsecond premolars have similar crown forms,which means that an acceptable contact pointcan be achieved between the remaining premo-lar and the adjacent molar and canine. Thechoice between first or second premolar dependson a number of factors: for example, the degreeof crowding, the anchorage requirements, theoverjet and overbite.
In Class I cases where crowding exists and the
Fig. 5 Premolars hadpreviously been extracted aspart of orthodontictreatment in adolescence.Crowding returned in thelower labial segment (a),which was relieved byremoval of a lower incisorand fixed appliancetreatment. A bonded retainerwas fitted at the completionof treatment (b)
Fig. 6 A Kesling set up of thecase in Figure 5, removing thelower left central incisor andreplacing the remaining incisorsand canines. This showed the anticipatedtooth positions and occlusionwith the upper arch
Fig. 7 A lower premolarhas been transplantedto replace the upperleft central incisorwhich had a poorprognosis
a
b
04p195-203.qxd 27/01/2004 10:15 Page 199

PRACTICE
200 BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004
canines are mesially angulated, loss of first pre-molars may produce spontaneous improvementin the alignment of the canines (Fig. 9). Anyexcess extraction spaces may close with time,although a study by Berg et al., showed spaceclosure to be greatest in the first 6 months fol-lowing extraction.18 In carefully selected casesreasonable alignment can sometimes beachieved. However cases amenable to this typeof treatment are rare and fixed appliances espe-cially when second premolars have beenextracted invariably produce better results.
Second premolars are the third most com-monly developmentally absent teeth after thirdmolars and upper lateral incisors.19 Wheredeciduous molars are retained beyond their nor-mal exfoliation dates, a radiograph should betaken to confirm the presence and position ofthe permanent successor. In uncrowded archesdeciduous molars with good roots are oftenretained, as space closure in these cases can bedifficult (Fig. 10).
Second premolars can become impactedeither due to early loss of deciduous molars orsevere crowding. Ectopic second premolars usu-
ally erupt lingually or palatally and should beconsidered for extraction if they are completelyexcluded from the arch (Fig. 11).
First molarsFirst permanent molars are often the first perma-nent teeth to erupt into the mouth. Their deepfissure morphology predisposes them to cariesand poor tooth brushing combined with a highsugar intake, may result in gross caries. Heavilyrestored or decayed first molars should be con-sidered for removal over other non-carious teeth(Fig. 12). First molars extraction requires carefulplanning. Their position in the arch means thatwhilst relief of premolar crowding is achievedthe space created is far from the site of any inci-sor crowding or overjet reduction. The timing ofthe loss of first molars is also an important con-sideration.
Maxillary second molars have a curvilineareruptive path with mesial and vertical compo-nents. The lower second molar has a more verti-cal path, but it has to move more horizontally infavourable spontaneous molar correction. This isone of the reasons why the spontaneous tooth
Fig. 8 A severelycrowded case, whereunusually, four canineswere extracted. Theresulting occlusiongave acceptablecontacts between firstpremolar and lateralincisors and improvedthe arch form. (a-c) Pre treatment,(d-f) Post treatment
a b
c
d
e f
04p195-203.qxd 27/01/2004 10:16 Page 200

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004 201
movement is less favourable in the lower arch.Three periods of development can be consideredwhen looking at the effects of loss of firstmolars.
Maximal space closure by mesial migrationof the second molar occurs in the mixed denti-tion. At this stage the second molars areunerupted and their root furcation is just calci-fying. The best results occur in the upper archwhere the second molar will usually eruptmesially and make contact with the upper
second premolar. Spontaneous relief of mildcrowding in the labial segments may be seen. Inthe lower arch, spontaneous closure is less likely,but mesial migration of the second molar is alsooptimal at this stage and may resulting in mini-mal space between the second molar and secondpremolar (Fig. 12).
In the permanent dentition the effect of lossof a first molar can be difficult to predict afterthe second molar has erupted. Fixed appliancesare invariably needed at this stage to align theteeth and achieve space closure with parallelroots.20 The effects are more of a problem in thelower arch, where the second molar tips mesial-ly and rolls lingually forming a very poor con-tact with the second premolar or may leaveexcess space. Little spontaneous relief of ante-rior crowding is seen. The upper first molar ifretained can over-erupt, further increasing thetipping and rolling of the lower second molar.In addition mesial movement of the lower
Fig. 9 A Class I casewith mild lower labialsegment crowding inthe late mixeddentition (a) & (b). Allfour first premolarswere extracted and theocclusion allowed toalign spontaneously. (c) & (d)
Fig. 11 Localised crowding often manifests in the lower buccal segments by lingual eruption of the second premolar
Fig. 10 A hypodontia case pre-treatment showinggood quality deciduous molars which wereretained as part of the treatment plan. Mesio-distal reduction or 'slenderising' can be used tomaximise arch co-ordination, especially wheredeciduous molars are only retained in one arch
a b
dc
04p195-203.qxd 27/01/2004 10:18 Page 201

PRACTICE
202 BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004
molar may be prevented. The upper secondmolar shows less tipping and rolling than itslower counterpart, but does not align to theextent seen in the mixed dentition. In adultpatients the drifting of both upper and lowersecond molars is less marked, and the relief ofcrowding less reliable. In young patients, radi-ographs should be checked to ensure that thedeveloping lower second premolar is containedby the roots of the primary molar. If not, thensubstantial drifting of the second premolar cantake place including impaction into the mesialsurface of the second molar.
In general terms if a lower first molar is tobe extracted, the upper molar on the sameside should also be extracted (compensatingextraction). This prevents unwanted over-eruption of the upper first molar and theupper second molar will usually erupt into agood position. However, if an upper firstmolar is to be extracted, the lower counter-part is usually left in situ. This is because thelower second molar behaves unpredictablyand rarely achieves good spontaneous align-ment. An additional factor is that lowermolars over erupt less than upper molars andwill not interfere with the generally goodprogress made by upper second molars. If thecase has no crowding, then balancing extrac-tions should not be considered (removal of atooth on the opposite side of the same arch).Children presenting with carious first molarsoften show signs of disease in all of them. Ifthe timing is correct and the malocclusionjustifies treatment, all four first molars
Fig. 12 Four first molars were extracted just after theoptimal time, prior to fixed appliance treatment. Theorthopantomogram (a) shows gross caries in the left firstmolars and heavy restorations in the right first molars.Notice the discrepancy in space available in the two arches.In the upper arch the second molars have erupted in closeproximity to the second premolars due to their mesialeruptive path (b). In the lower arch there is considerablymore space remaining from the vertical eruptive path of thesecond molars (c)
Fig. 13 Extraction of second molars allowedspontaneous relief of anterior crowding, with earlyeruption of the third molars
a
b c
04p195-203.qxd 27/01/2004 10:20 Page 202

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 4 FEBRUARY 28 2004 203
should be removed to allow second molars toerupt efficiently and reduce subsequenttreatment times.
Second molarsThomas et al.21 provided a succinct summary onthe role of loss of second molars in orthodontictreatment. They state that all other teeth shouldbe present with the third molars of normal size,shape and in a good position to erupt. Mildlower labial segment crowding may be effective-ly treated by loss of second molars, howeverthey should not be considered in the treatmentof moderate or severe crowding. Second molarloss may be undertaken under the following cir-cumstances:
• To facilitate the eruption of the third molarsobviating the need for surgical removal at alater stage.
• To allow relief of premolar crowding (espe-cially where second premolars are impacted)
• May prevent crowding in a well-aligned lowerarch (Fig. 13).
• Distal movement in the upper arch is morereliable and more stable.
However, the potential disadvantages of second molar extraction are:
• Eruption of third molars especially in thelower arch is unpredictable. About 30% ofthese teeth require uprighting.
• The teeth are remote from the site of crowdingmaking alignment unpredictable.
Where second molars are considered forextraction, the timing is important. Satisfactorythird molar alignment is less likely if the secondmolars are extracted after the third molar rootsare more than one third formed.
Third molarsWhilst extraction of wisdom teeth for orthodon-tic purposes is rare, these teeth should be includ-ed in the treatment planning. The incidence ofimpaction of third molars varies widely in theliterature.22 Posterior crowding, especially in thelower arch, may increase the risk of developingimpaction. Extraction of teeth towards the frontof the mouth has little effect on posterior crowd-ing, whilst extractions towards the back improvethe chances of acceptable third molars eruption.The greatest benefit occurs when second molarsare removed, although eruption patterns areunpredictable. Richardson et al.23 suggest thatup to 90% of third molars erupt into satisfactorypositions following second molar removal, butthis depends on the degree of posterior crowdingand stage of root development of third molars attime of extraction. It also assumes a fairly broadminded view of what is a ‘satisfactory’ position.
Third molars have in the past been implicatedin the aetiology of late lower incisor crowding.23
However, more recent research shows that theirpresence is only one of the factors involved and
their influence appears to be negligible. There-fore, third molars should not be removed torelieve or prevent late lower incisor crowding.24
This forms part of the National Clinical Guide-lines on the management of patients withimpacted third molars.22
CONCLUSIONSMany factors influence the choice of teeth forextraction and careful treatment planning inconjunction with good patient co-operation,appliance selection and management of thetreatment are essential if an acceptable, aesthet-ic and functional occlusion is to be achieved.
1. Angle E H. Treatment of malocclusion of the teeth andfractures of the maxillae, Angle's system. Ed 6, 1900 S.S.Philadelphia: White Dental Manufacturing Co.
2. Wolff J. Das Gesetz der Transformation der Knochen. Berlin:Hirschwald, 1892.
3. Case C S. The question of extraction in orthdontia. Am JOrthod 1964; 50: 658-691.
4. Tweed C. Clinical Orthodontics. 1966, St Louis: Mosby.5. Begg P R. Stone age man's dentition. Am J Orthod 1954; 40:
298-312.6. Little R M, Riedel R A, Stein A. Mandibular arch length
increase during the mixed dentition: postretentionevaluation of stability and relapse. Am J Orthod DentofacOrthop 1990; 97: 393-404.
7. Betteridge M A. The effects of interdental stripping on thelabial segments evaluated one year out of retention. Br JOrthod 1981; 8: 193-197.
8. Little R M. Stability and relapse of dental arch alignment. Br JOrthod 1990; 17: 235-241.
9. Proffit W E. Forty-year review of extraction frequency at auniversity orthodontic clinic. Angle Orthod 1994; 64: 407-414.
10. McCaul L K, Jenkins W M, Kay E J. The reasons for extractionof permanent teeth in Scotland: a 15-year follow-up study.Br Dent J 2001; 190: 658-662.
11. Kirschen R H, O'Higgins E A, Lee R T. The Royal London SpacePlanning: an integration of space analysis and treatmentplanning: Part II: The effect of other treatment procedures onspace. Am J Orthod Dentofacial Orthop 2000; 118: 448-461.
12. Khurana M, Martin M V. Orthodontics and infectiveendocarditis. Br J Orthod 1999; 26: 295-298.
13. Ericson S, Kurol J. Early treatment of palatally eruptingmaxillary canines by extraction of the primary canines. Eur JOrthod 1988; 10: 283-295.
14. Bradbury A J. The influence of orthodontic extractions on thecaries indices in schoolchildren in the United Kingdom.Comm Dent Health 1985; 2: 75-82.
15. Canut J A. Mandibular incisor extraction: indications andlong-term evaluation. Eur J Orthod 1986; 18: 485-489.
16. Graber T M. New horizons in case analysis: clinicalcephalometrics. Am J Orthod 1956; 53: 439-454.
17. Tuverson D L. Anterior interocclusal relations. Part II. Am JOrthod 1980; 78: 371-393.
18. Berg R, Gebauer U. Spontaneous changes in the mandibulararch following first premolar extractions. Eur J Orthod 1982;4: 93-98.
19. Vastardis H. The genetics of human tooth agenesis: newdiscoveries for understanding dental anomalies. Am J OrthodDentofac Orthop 2000; 117: 650-656.
20. Sandler P J, Atkinson R, Murray A M. For four sixes. Am JOrthod Dentofac Orthop 2000; 117: 418-434.
21. Thomas P, Sandy J R. Should second molars be extracted?Dent Update 1995; 22: 150-156.
22. National Clinical Guidelines. The management of patientswith impacted third molar (syn. Wisdom) teeth. Royal Collegeof Surgeons of England 1997.
23. Richardson M E, Richardson A. The effect of extraction offour second permanent molars on the incisor overbite. Eur JOrthod 1993; 15: 291-296.
24. Schwarze C W. The influence of third molar germectomy - acomparative long term study. Abstract of Third InternationalCongress, London 1973; 551-562.
04p195-203.qxd 27/01/2004 10:20 Page 203

BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004 255
PRACTICE
Orthodontics. Part 9: Anchorage control and distal movementD. Roberts-Harry1 and J. Sandy2
Anchorage is an important consideration when planning orthodontic tooth movement.Unwanted tooth movement known as loss of anchorage can have a detrimental effect onthe treatment outcome. Anchorage can be sourced from the teeth, the oral mucosa andunderlying bone, implants and extra orally. If extra-oral anchorage is used, particularly witha facebow then the use of at least two safety devices is mandatory.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professor of Orthodontics, Division ofChild Dental Health, University of BristolDental School, Lower Maudlin Street,Bristol BS1 2LY; *Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4811031© British Dental Journal 2004; 196:255–263
● Anchorage is the resistance to unwanted tooth movement● It can be obtained from a number of different sources● Loss of anchorage can have a detrimental effect on treatment● Safety is of prime importance when using extra-oral devices
I N B R I E F
Anchorage is defined as the resistance tounwanted tooth movement. Newton's third lawstates that every action has an equal and oppositereaction. This principle also applies to movingteeth. For example, if an upper canine is beingretracted, the force applied to the tooth must beresisted by an equal and opposite force in theother direction. This equal and opposite force isknown as anchorage.
Anchorage may be considered similar to a tugof war. Two equal sized people will pull eachother together by an equal amount. Conversely abig person will generally pull a small one withoutbeing moved. However, if two or more smallerpeople combine then their chances of pulling abig person will increase. Similarly, the moreteeth that are incorporated into an anchorageblock, the more likely it is that desirable asopposed to undesirable tooth movements willoccur. Undesirable movement of the anchorteeth is called loss of anchorage.
If an upper canine is to be retracted, with bod-ily movement using a fixed appliance, the forceapplied to the tooth will be approximately 100 g(Fig. 1a). Forces in the opposite direction varyingfrom 67 g on the first permanent molar to 33 gon the upper second premolar resist this. Lowlevels will produce negligible tooth movementand the effect of a light force of 100 g would beto retract the canine with minimal anteriorunwanted movement of the anchored teeth.However, if the force level is increased to say300 g (Fig. 1b), the force levels on the anchorteeth increase dramatically to the level whereunwanted tooth movements will occur.Although the canine may move a little distally,
the buccal teeth will also move mesially. Spacefor the canine retraction may be eliminated withinsufficient space left for alignment of the ante-rior teeth. Figure 1c compares the root area ofsome of the upper teeth. The combined root areaof the upper incisors and upper canines isaround the same as that of the first molar andpremolars. Therefore, if the upper labial segmentincluding the upper canines is retracted in ablock, there will be an equivalent mesial move-ment of the upper molar and upper premolar.These factors need to be very carefully consid-ered in planning anchorage requirements andtooth movement.
Anchorage may be derived from four sources:
• Teeth• Oral mucosa and underlying bone• Implants• Extra oral
TEETHThe anchorage supplied by the teeth can comefrom within the same arch as the teeth that arebeing moved (intra maxillary) or from theopposing arch (inter maxillary).
Intra maxillary anchorageThe anchorage provided by teeth depends on thesize of the teeth, ie the root area of the teeth. Fig.1c shows the root surface area of each of theteeth in the upper arch. The more teeth that areincorporated into an anchorage block the lesslikely unwanted tooth movement will occur. If a removable appliance is used, the base plateand retaining cribs should contact as many of
9
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
05p255-263.qxd 09/02/2004 12:42 Page 255

PRACTICE
256 BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004
the teeth as possible. Figure 2 illustrates thepoint. If upper canines are to be retracted with aremovable appliance, cribs on the first perma-nent molars and upper incisors will not onlyhelp with retention but also increase theanchorage considerably. In addition, the baseplate must contact the mesial surface of theupper second premolars and palatal to theupper incisors. If fixed appliances are to beused, the more teeth that are bracketed orbanded, the greater will be the anchorageresistance (Fig. 3).
Inter maxillary anchorageTeeth in the opposite arch can provide very use-ful and important sites of anchorage control asFigs 4a,b illustrate. Good inter-digitation of thebuccal teeth can help prevent mesial movementof the buccal segment. Although there is onlyanecdotal evidence to support this view, manyclinicians feel this can be a useful source ofanchorage.
The second way that opposing teeth can beused is by means of elastics or springs runningfrom one arch to the other. Class II elastics(Fig. 4c) run from the lower molars to theupper incisor region, whereas Class III elastics(Fig. 4d) run from the upper molars to thelower incisor region.
Inter-maxillary elastic are invaluable inmany cases but do rely very heavily on goodpatient co-operation. The elastics need to bechanged every day and if they break (whichthey frequently do) they must be replacedimmediately. Class II elastics will also tend tohave unwanted effects on the occlusion. Theytend to tip the lower molars mesially and rollthem lingually. In addition, they can produceextrusion of the upper labial segment and thelower molars. Whilst extrusion of the lowermolars can help with overbite reduction,extrusion of the upper incisors is usually anunwanted side effect and has to be counter-acted by adding an upward curve to the upperarch-wire known as an increased curve ofSpee. Extrusion of the buccal teeth is undesir-able in patients with increased lower faceheight and therefore Class II elastics should beused sparingly in these cases. Similarly ClassIII elastics can extrude the upper molars, tipthem mesially and roll them palatally. Molarextrusion will decrease the overbite, which isusually undesirable in Class III cases. Elasticsalso tend to cant the occlusal plane and havebeen implicated in root resorption in the upperlabial segment, particularly if they are usedfor prolonged periods.
Functional appliances are another source ofintermaxillary anchorage. Whilst some clini-cians may believe these devices simply make themandible grow, this is not the case and whatevermandibular growth does take place, is accompa-nied by quite substantial movement of the denti-tion over the apical base. This means that mesialtipping of the lower and distal tipping of theupper teeth occurs.
67g67g
33g33g
100g100g
Fig. 1a A distalising force on the upper canine will produce a reciprocal force in theopposite direction on the anchor teeth. Provided the force level for bodily movement iskept low at about 100g then there will be minimal mesial movement of the anchor teeth
200g200g
100g100g
300g300g
Fig. 1b As the distalising force level increases the reciprocal forces also increase witha greater risk of loss of anchorage
2.22.21.81.8
2.72.7
2.32.3
4.64.6
6.76.7
6.96.9
Fig. 1c The combined root surface area of the anterior teeth is almost the same asthe molar and premolar. Attempting to move all the anterior teeth distallysimultaneously will result in an equal mesial movement of the posterior teeth
05p255-263.qxd 09/02/2004 12:34 Page 256

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004 257
ORAL MUCOSA AND UNDERLYING BONEContact between the appliance and the labialor lingual mucosa can increase anchorageconsiderably for either fixed or removableappliances. Contact between an orthodonticappliance and the vault of the palate providesresistance to mesial movement of the posteriorteeth. The anchorage provided by this meansis considerably greater if there is a high vault-ed palate as shown in Figure 5a, which willproduce a greater buttressing effect. A shallowvaulted palate (Fig. 5b) will provide much lessanchorage control because the appliance willsimply tend to slide down the inclined planeof the palate.
The mucosa and underlying bone can alsobe used when fixed appliances are used, forexample a Nance palatal arch (Fig. 5c). This isan acrylic button that lies on the most verticalpart of the palate behind the upper incisors andis added to a trans-palatal arch. These buttonsare again of more limited use if the palatalvault is shallow.
IMPLANTSOsseo-integrated implants can be used as avery secure source of anchorage. Implantsintegrate with bone and do not have a peri-odontal membrane. Because of this they donot move when a force is applied to them andin some cases they can provide an ideal sourceof anchorage. Recently small implants fororthodontic use have been specificallydesigned and can be used in the retro-molarregion to move teeth distally or anteriorly formesial movement. Short 4mm implants can be
Fig. 2 Incorporatingas many teeth aspossible in theappliance design andcovering the anteriorpalatal vault willincrease theanchorage
Fig. 3 When fixedappliances are used, as many teeth aspossible are banded toincrease the anchorage
Fig. 4a,b Inter-digitation of the buccal occlusion can helpincrease anchorage
Fig. 4c Intermaxillary elastics use teeth in the opposite arch as asource of anchorage. Class II traction is shown here
Fig. 4d Class III elastics
➠ ➠
05p255-263.qxd 09/02/2004 12:35 Page 257

PRACTICE
258 BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004
paced in the anterior mid-line of the palate inthe thickest part of the nasal crest and a trans-palatal bar then connects the implants to theteeth (Fig. 6).
EXTRA-ORAL ANCHORAGEThis can be applied via a number of devicesand can be used in conjunction with eitherremovable or fixed appliances. Headgear isnot a recent invention and has been in use forover a century. Figure 7a is a picture of aKingsley headgear, which was in use as earlyas 1861.
The force from the headgear is usuallyapplied to the teeth via a face-bow (Klöen bow)as shown in Fig. 7b. This is fitted either to tubesattached to the appliance or integral with it asin the en masse appliance. The direction bywhich the force is applied can be varieddepending on the type of headgear that is fitted. Headgear can be applied to both themaxillary and mandibular dentition, and thereare a number of variations:
• Cervical• Occipital• Variable• Reverse
Cervical HeadgearThis is applied via an elastic strap or spring,which runs around the neck (Fig. 8a). It has theadvantage of being relatively unobtrusive andeasy to fit. However, it does tend to extrude theupper molars and tip them distally because ofthe downward and backward direction of force.This later effect can be counteracted to somedegree by adjusting the height and length of theouter bow. Cervical headgear should not beattached to removable appliances because it isprone to dislodge the appliance and propel it tothe back of the mouth.
OccipitalThis is also known as high pull headgear andis applied via an occipitally placed head-cap(Fig. 8b). It is easy to fit but is more obviousthan the neck strap and tends to roll off thehead unless carefully adjusted. Because theforce is in a more upward direction, there isgenerally less distal tipping of the upper molarand less extrusion, but also less distal move-ment than with cervical headgear. The tippingand extrusion effect again depend on thelength and height of the outer bow.
Variable This applies a force part way between cervicaland occipital (Fig. 8c) and is our preferredchoice. It takes slightly longer to fit thaneither cervical or occipital and is more obtru-sive. However it is secure and comfortable andthe vector of the force can be varied to pro-duce relatively less tipping and/or extrusion.
Whilst headgear is a very useful source ofanchorage, it has a number of disadvantages.These are as follows:
• Safety• Clinical time• Compliance• Operator preference
The most important of these problems is thefact that headgear can be dangerous and anumber of facial and serious eye injuries havebeen reported in the literature.1–3 The Stan-dards and Safety Committee of the BritishOrthodontic Society (BOS) have addressedthese concerns. An advice sheet produced bythe BOS is essential reading for anyone whowishes to use headgear.4
The main problems with headgear safetyrelate to the prongs at the end of the face-bowthat fit into the headgear tubes on the intra-oralappliance. It is possible for the bow to becomedislodged, either because it is pulled out of themouth or when the patient rolls over when theyare asleep. The recoil effect from the elastics candamage the teeth, oral mucosa, soft tissues of theface and most seriously, the eyes. In order tominimise these problem various safety deviceshave been suggested. These involve re-curvingthe distal end of the wire, using plastic coatedface bows and various locking springs.5,6 Inaddition a variety of snap-away face bows havebeen produced. If these are pulled beyond a preset distance, the neck strap comes apart and pre-vents any recoil injury. Another popular methodof preventing recoil is to fit a rigid safety strap,which prevents the bow from coming out of themouth if it disengages from the tubes. Someexamples of these safety devices are shown inFigures 8a-i.
The importance of headgear safety cannot beover emphasized and it is recommended that twosafety mechanisms are simultaneously used, forexample a locking spring and a snap away head-gear or a safety face-bow and rigid safety strap.
ReverseReverse or protraction headgear is useful formesial movement of the teeth, either to closespaces or help to correct a reverse overjet. It doesnot employ a face-bow, which is an advantagebut instead employs intra-oral hooks to whichelastics are applied (Fig. 9a,b).
LOSS OF ANCHORAGEThis is defined as the unplanned and unexpectedmovement of the anchor teeth during orthodon-tic treatment.
There are several causes of loss of anchorage.Some examples of these are:
• Poor appliance design• Poor appliance adjustment• Poor patient wear
Poor appliance designFailure to adequately retain the appliance, orincorporate as many teeth into the anchor blockas possible are common causes of anchorageloss. If fixed appliances are used, as many
05p255-263.qxd 09/02/2004 12:36 Page 258

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004 259
Fig. 5a A steep anterior palatal vault is a useful source ofanchorage due to the buttressing effect
Fig. 5b A shallow palatal vault provides less anchorage
Fig. 5c The palatal vault can be used for removable or fixedappliances. An example of a Nance button is shown here Fig. 6 An osseo-integrated implant with a bonded
palatal arch is being used to help close space in theupper arch without retroclining the upper incisors
Fig. 7a An early Kingsleyheadgear circa 1860
Fig. 7b,c A facebow(Klöen bow) is attachedto tubes welded tobands on the molars
05p255-263.qxd 09/02/2004 12:37 Page 259

PRACTICE
260 BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004
Fig. 8a A neck strap. Note the snapaway safety mechanism
Fig. 8b An occipital (high pull)headgear again with a snap away safetysystem
Fig. 8c A variable pull Interlandiiheadgear. A rigid plastic strip isemployed as a safety mechanism toprevent the facebow disengaging fromthe molar bands and coming out of the mouth
Fig. 8d,e The end of thefacebow can be re-curvedto improve safety
Fig. 8f,g A plastic coatedfacebow together with asafety neck-strap
Fig. 8h,i A Samuels lockingspring. This secures the facebow to the tube preventingaccidental disengagement.This should be used inconjunction with a safetyneck strap or snap awayheadgear
05p255-263.qxd 09/02/2004 12:39 Page 260

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004 261
anchor teeth as possible should be banded inorder to produce optimum anchorage. Remov-able appliances should have adequate retentionusing appropriate well-adjusted cribs or claspswith as much contact with the teeth and oralmucosa as possible.
Poor appliance adjustmentThe use of excessive force or trying to move toomany teeth at the same time may result inunwanted movement of the anchor teeth. Toavoid loss of anchorage, simultaneous multipleteeth movement should be avoided. If theappliance is poorly adjusted so that it doesn'tfit very well, or the force levels applied to theteeth are too high, then undesired tooth move-ment may occur. High force levels produced byover activation are one of the key reasons foranchorage loss.
The optimal force for movement of a singlerooted tooth is about 25–40 g for tipping andabout 75 g for bodily movement. If the force istoo low there will be very little movement,whereas too much force may result in loss ofanchorage. Excess force does not increase therate of tooth retraction as illustrated in Fig. 10.7
As the force levels rise the rate of tooth tippingalso increases up to about 40 g. Beyond this verylittle extra tooth movement occurs. Thusincreasing the force levels above about 40 g willnot increase the rate of tooth tipping.
The force levels that wires from fixed orremovable appliances exert on teeth usuallydepends on the following:
• The material the wire is made from• The amount it is deflected• The length of the wire• The thickness of the wire
Steel wire will exert a force that is directlyproportional to the amount the wire is deflectedup to its elastic limit. Figure 11 demonstrateshow decreasing the wire thickness and increas-ing the length (sometimes by adding loops) con-trols the force produced.
Modern alloys such as super elastic nickel tita-nium wires do not act in the same way as steel.These remarkable wires are capable of producing
Fig. 9a, b A reverse, or protraction headgear
Rate of canine retraction
0
0.5
1
1.5
0 10 20 30 40 50 60gm
(mm per month)
Fig. 10 The graph shows how increase force levels do not necessarily increase therate of tooth movement. The y axis shows the rate of movement in mm. The x axisis the amount of tipping force applied to the tooth. As the force level initially risesthe rate of tooth movement also increases. Above about 40 g the rate slows downand very little additional tooth movement occurs. There will however be a greaterrisk of loss of anchorage with increased force levels
0.5 mm0.5 mm
0.5 mm0.5 mm
0.6 mm0.6 mm
Fig. 11 A 0.5 mm diameter wire can bedeflected more than a 0.6 mm wirewithout increasing the force level. Thus agreater degree of activation is possibleand the appliance will require lessfrequent adjustments. Similarlyincreasing the length of the wire, forexample by incorporating loops allows agreater degree of wire deflection. Theforce characteristics may also be changed by altering the material the wire is made from
05p255-263.qxd 09/02/2004 12:40 Page 261

PRACTICE
262 BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004
a continuous level of force almost independent ofthe amount of deflection and have transformedthe use of fixed appliances in recent years. Heatactivated wire is now available that will increaseits force level as the temperature changes. Thesewires exhibit a so-called shape memory effect. Ifthe wire is cooled and tied into the teeth it deflectseasily into position. As the wire warms in themouth it gradually returns to its original shapemoving the teeth with it (Figs12a–c).
For optimal tooth movement it is importantthat continuous gentle forces are applied to theteeth. Fixed appliances are ideal for doing this.When removable appliances are worn, thepatient should wear them full-time except forcleaning and playing contact sports. Part-timewear produces intermittent forces on the teethand is likely to reduce the rate of movement.
When a force is applied to a tooth, there is aninitial period of movement as the periodontal
membrane is compressed (Fig. 13). No toothmovement occurs for a few days after this, ascells are recruited in order to remodel the socketas well as the periodontal membrane. This cellrecruitment takes a few days and is known as thelag effect. Part-time wear of appliances will notallow efficient cell recruitment and the lag phasewill not be passed which may result in poortooth movement. This is another reason whyfixed appliances, which cannot be left out of themouth by patients, are much more effective thanremovable appliances at achieving a satisfactorytreatment outcome.
RETRIEVAL AND PRESERVATION OFANCHORAGEExtra-oral devices can be used for distal move-ment as well as anchorage reinforcement. Foranchorage control wearing the headgear atnight-time only is usually enough. In order toproduce distal movement, the patient shouldwear the appliance in excess of 12 hours usu-ally for the evenings as well as at nighttime.While some practitioners increase the forcelevels for distal movement purposes, it is ourexperience that this is not necessary and aforce of approximately 250–300 g per side isadequate for both distal movement andanchorage control.
Many devices have been described to reduceor eliminate the need for headgear. These arehowever of limited use and can only produce avery small amount of extra space. If these gadg-ets are used without anchorage re-enforcementunwanted mesial movement of the anchor teethcould occur. Figures 14a–c shows one exampleknown as a Jones jig. To produce distal move-ment of the molars the anchorage is reinforcedwith an anterior trans-palatal arch. A jig incor-
Fig. 12a-c Super elastic heatactivated wires produce a lightcontinuous force almost regardlessof the amount of deflection. Whencooled they become very flexible(12a) but return to their originalshape as they warm in the mouth(12b,c)
a
b c
Lag period
0
0.5
1.0
1.5
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
Days
mmFig. 13 Tooth movementrequires light continuousforces. In this graph toothmovement in mm is shownon the y-axis and time indays on the x-axis. If aforce is applied to a tooththe periodontal membraneis compressed and there isa small amount of initialmovement. Movementthen stops as bone cells arerecruited and the socketstarts to be remodeled.After about 14 dayssufficient recruitment andremodeling has occurred toallow the tooth to move
05p255-263.qxd 09/02/2004 12:41 Page 262

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 5 MARCH 13 2004 263
porating a nickel-titanium coil spring is insertedinto molar tubes and tied into the premolarbands. The molars are distalised using the ante-rior teeth from premolar to premolar as theanchorage block. It is important to note the lossof anchorage that is occurring as demonstratedby the simultaneous mesial movement of thefirst premolars. Once distal movement of themolars has been achieved the anchorage rein-forcement can be transferred to the molars(palatal arch or Nance button) and the premo-lars, canines and incisors retracted. True anchor-age re-enforcement with these devices is diffi-cult to achieve and headgear, or implants muststill be considered the mainstay of producingeffective distal movement.
Thanks to Mr. R Cousley for figure 6 and Mr. J Kinelan forfigures 14a-c
1. Booth-Mason S, Birnie D. Penetrating eye injury fromorthodontic headgear. Eur J Orthod 1998; 10: 111-114.
2. Samuels R H A, M Willner F, Knox J, Jones M L. A nationalsurvey of orthodontic face bow injuries in the UK and Eire. Br J Orthod 1996; 23: 11-20.
3. Samuels R H A, Jones M L. Orthodontic face bow injuries andsafety equipment. Eur J Orthod 1994; 16: 385-394.
4. British Orthodontic Society, 291 Grays Inn Road, LondonWC1X 8QJ.
5. Postlethwaite K. The range and effectiveness of safetyheadgear products. Eur J Orthod I988; 11: 228-234.
6. Samuels R H A, Evans S M, Wigglesworth S W. Safety catchfor Kloen face bow. J Clin Orthod 1993; 27: 138-141.
7. Crabb J J, Wilson H J. The relation between orthodonticspring force and space closure. Dent Pract Dent Res 1972;22: 233-240.
Fig. 14a-c A Jones jig for distal movement of the molars (14a).A palatal arch is fitted to the first premolars to increase theanterior anchorage. A jig is then inserted into the buccal archwire and headgear tubes. An open nickel titanium coil spring isthen slid over the shaft of the jig and compressed by sliding acollar onto the shaft and tying it to the premolar (14b). Thisthen uses the upper premolars and palatal vault to distalise the molars (14c). Note the simultaneous mesial movement of the first premolars which is a sign of anchorage loss
a
b c
BDA Information Centre Services
Did you know?• As a BDA member you can gain access to one of the
best dental information services in the world• You don’t have to be based in London to use the
service• You can borrow books, videos and information pack-
ages • You can borrow up to eight items via the postal system
The only cost to you is the cost of the return postage. Ifyou’re not sure what to request then telephone us andwe can advise you.
• You are entitled to free MEDLINE searchesTelephone us with a subject and we will send you a list ofrelevant references with abstracts.
• You can request photocopies of journal articles.There is a small charge for this service and you need tofill in a Photocopy Request Form first. Telephone us ifyou would like one of these forms.
• BDA Members can view the latest Current DentalTitles on our web site free of charge.
For further details of any of these services dial 020 7563 4545.
Contact us via e-mail at:[email protected]
Visit the Information Centre web pages at: http://www.bda.org
05p255-263.qxd 11/02/2004 11:23 Page 263
shilpa
Rectangle

BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004 319
PRACTICE
Orthodontics. Part 10: Impacted teethD. Roberts-Harry1 and J. Sandy2
This section deals with the important issue of impacted teeth. Impacted canines in Class I uncrowded cases can be improved byremoval of the deciduous canines. There is some evidence that this is true for both buccal and palatal impactions. Treatment ofimpacted canines is lengthy and potentially hazardous. Interceptive measures are effective and preferred to active treatment.Supernumerary teeth may also cause impaction of permanent incisors, their early diagnosis and appropriate treatment isessential to optimise final outcomes. If there are any doubts about impacted teeth it is better to refer too early than too late, thislatter option may unnecessarily extend the length of treatment as well as the treatment required.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professor of Orthodontics, Division ofChild Dental Health, University of BristolDental School, Lower Maudlin Street,Bristol BS1 2LY; *Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4811074© British Dental Journal 2004; 196:319–327
● Check all 10-year-olds for the position of their permanent canines by initial clinicalexamination and palpation, if necessary with further radiographs to locate possibleimpactions
● Check for late eruption of permanent incisors, if one incisor has erupted, the others shouldnot be far behind. If the permanent lateral incisors have erupted but not the permanentcentral incisors then suspicion of impaction should be heightened
● Refer too early rather than too late
I N B R I E F
This section brings together the informationgeneral dental practitioners need in order todiagnose and deal effectively with impactedteeth.
IMPACTED CANINESA canine that is prevented from erupting into anormal position, either by bone, tooth orfibrous tissue, can be described as impacted.Impacted maxillary canines are seen in about3% of the population. The majority of impactedcanines are palatal (85%), the remaining 15%are usually buccal. There is sex bias, 70% occurin females. One of the biggest dangers is thatthey can cause resorption of the roots of the lateral or central incisors and this is seen inabout 12% of the cases.
The cause of impaction is not known, butthese teeth develop at the orbital rims and havea long path of eruption before they find theirway into the line of the arch. Consequently incrowded cases there may be insufficient roomfor them in the arch and they may be deflected.It seems that the root of the lateral incisor isimportant in the guidance of upper permanentcanines to their final position. There is alsosome evidence that there may be genetic inputinto the aetiology of the impaction.
Late referral or misdiagnosis of impactedcanines places a significant burden on thepatient in relation to how much treatment theywill subsequently need. If the canines are in poorpositions it will require a considerable amount oftreatment and effort in order to get them into theline of the arch and a judgement must be madeas to whether it is worth it. Sacrificing the canineis unsatisfactory since this presents a challenge
to the restorative dentist, an aesthetic problemand by definition, cannot be used to guide theocclusion. There are times when it might be sen-sible to consider its loss, but early diagnosis canmake a significant difference to how much treat-ment is needed by the patient.
DIAGNOSIS It is easy to miss non-eruption of the permanentcanines, but there are some markers whichshould increase suspicion of possible impaction.Any case with a deep bite, missing lateral inci-sors or peg-shaped upper lateral incisors needs adetailed examination. Figure 1 shows such acase and in this instance both canines were sig-nificantly impacted on the palatal aspect. Theretained deciduous canine is self evident. Otherclues include root and crown positions. Figure 2shows a lateral incisor which is proclined. There
10
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
Fig. 1 Typical features which should arousesuspicion of impacted canines. There is a deepbite and a small peg-shaped lateral incisor. Theretained deciduous canine is obvious. In thispatient both upper permanent canines werepalatally positioned
VERIFIABLE CPD PAPER
NOW AVAILABLE AS A BDJ BOOK
6p319-327.qxd 23/02/2004 10:25 Page 319

PRACTICE
320 BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004
is a retained deciduous canine and the perma-nent canine lies buccal which moves the rootof the lateral incisor palatally and the crownlabially.
Any general dental examination of a patientfrom the age of 10 years should include palpa-tion for the permanent canine on the buccalaspect. It is possible to locate the canines withpalpation, but this will lead to some false observa-tions. For instance, the buccal root of a decidouscanine, if it is not resorbing, can feel like thecrown of the permanent tooth. It is thereforeimportant to back up clinical examination withradiographs. Failure to make these observationswill eventually result in patients complaining ofloose incisors; inevitably some permanentcanines will resorb adjacent teeth with devastat-ing efficiency as shown in Figures 3 and 4.
WHAT ARE THE BEST RADIOGRAPHIC VIEWSTO LOCATE CANINES? Most patients undergoing routine orthodonticscreening will have a dental pantomogram.Location of tooth position requires two radi-ographs in different positions. In the interests ofradiation hygiene it is sensible to use this as a base x-ray and to take further location radi-ographs in relation to the dental pantomogram.An anterior occlusal radiograph allows this andthe principle of vertical parallax can be used tolocate the position of the canine. The tube has toshift in order to take an anterior occlusal and itmoves in a vertical direction. If the tooth crownappears to move in the direction of the tube shift(ie vertically) then the tooth will be positionedon the palatal aspect. If the crown appears tomove in the opposite direction it is buccal and ifit shows no movement at all it is in the line ofthe arch (Figures 5 to 7). This also provides a rea-sonably detailed intra-oral view in cases of rootresorption.
Although there are other radiographic tech-niques which can be used to locate canines, thismethod works well. If there are difficulties inbeing sure of the exact location then two peri-apicals taken of the region with a horizontalshift of the tube may give slightly better preci-sion. The periapical radiographs will also givegood detail of the roots of adjacent teeth, partic-ularly the lateral incisors. The proximity of thecanine crown to incisor roots does make themvulnerable to root resorption. The percentage ofteeth adjacent to the crown of the canine whichundergo some form of resorption is probablyquite high at the microscopic level. No extrac-tions should be contemplated until the canineshave been located. Figure 8 shows a dental pan-tomogram of a patient who had both upper andlower first premolars removed as part of a treat-ment plan, but where the canines had not beenlocated beforehand. The dental pantomogramclearly shows the poor position of the caninesand subsequent treatment involved the removalof the permanent canines since their positionwas deemed hopeless and movement of thecanines may well have resulted in root resorp-
Fig. 2 There are clues as to the whereabouts of the upper rightpermanent canine in this patient. The upper right lateral crownis proclined because the upper right permanent canine isbuccally positioned and therefore places pressure on the rootmoving the crown of the lateral incisor labially and the root ofthe lateral incisor palatally
Fig. 3 Consequences of failure to diagnose impacted canines. Thisradiograph shows the roots of the upper lateral incisor to be resorbing
Fig. 4 The patient shown in Figure 3 had both lateral incisorsremoved because of the severe root resorption caused by theunerupted permanent canines
6p319-327.qxd 23/02/2004 10:06 Page 320

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004 321
tion of the incisors. The canines had to bereplaced prosthetically and it would be difficultto see how a legal defence of this situation couldbe raised.
INTERCEPTIVE MEASURES FOR CANINESOne of the most significant publications in theorthodontic literature came from Ericson &Kurol (1988)1 who demonstrated that extrac-tion of upper deciduous canines where theupper permanent canines were developing onthe palatal aspect, resulted in nearly an 80%chance of correcting the impaction. The paperwas very specific about what types of maloc-clusions this could be applied to. Nearly all thecases were Class I with no incisor crowding.This is important to emphasise, a subsequentfollow-up paper2 confirmed their originalobservation and also indicated that the tech-nique could not be applied easily to crowdedcases and in some cases this would result in aworsening of the situation rather than animprovement. The dental pantomogram of apatient is shown in Figure 9. The canines arepalatally positioned. Since this was anuncrowded case, the deciduous canines wereextracted and Figure 10 shows that both the
Fig. 5 Orthopantomograph of patient where the two canines are clearly impacted Fig. 6 Anterior occlusal radiograph of the samepatient shown in Figure 5. Both canines are nowmore apically positioned and therefore theseteeth have moved with the tube shift and arepalatally positioned
Fig. 7 Same patient as in Figures 5 and 6 withboth permanent canines exposed surgically andon the palatal aspect
Fig. 8 Dental pantomogram of a patient who had had all four first premolarsremoved without sufficient diagnostic information. The upper permanent canines arein a very poor position and with the distinct possibility of some root resorption it wasfelt that the upper permanent canines should be removed and replaced prosthetically
Fig. 9 Dental pantomogram of a patient with palatally impacted canines
6p319-327.qxd 23/02/2004 10:08 Page 321

PRACTICE
322 BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004
permanent canines erupted with no orthodon-tic assistance. Clearly this saved the patient aconsiderable amount of treatment and earlyappropriate referral would be wise if a generaldental practitioner is unsure. The interceptivemeasure of extracting deciduous caninesworks well if carried out between the ages of11–13 years. The closer the crowns are to themid-line the worse the prognosis. It is worthre-emphasising that this works best in Class Iuncrowded cases.
TREATMENT OF CANINES The treatment of buccally or palatally impact-ed canines involves exposure and then a formof traction to pull the tooth into the correctposition in the arch. Palatally impacted teethcan be exposed and allowed to erupt. Thistends to form a better gingival attachmentsince the tooth is erupting into attachedmucosa. This cuff may be lost on the palatalaspect as the tooth is brought into line. Someoperators prefer to raise a flap, attach a bracketpad with a gold chain to the tooth in theatreand then replace the flap. Traction is subse-quently applied to the chain and the toothpulled through the mucosa (Fig. 11). There issome evidence that this procedure is less suc-cessful than a straight forward exposure. Italso has a disadvantage that if the bondedattachment fails then a further operation,either to expose or reattach, is needed. Theadvantage with this technique is that the rootusually needs less buccal torque once thecrown is in position.
If the canine is moderately high and buccal, it will not be possible to expose the tooth since itwill then erupt through unattached mucosa andan apically repositioned flap should be consid-ered. If it is very high, it is not possible to apical-ly reposition the flap and therefore it is better inthis situation to raise a flap and bond an attach-ment with a gold chain. It is critical that thechain passes underneath the attached mucosaand exits in the space where the permanentcanine will eventually be placed as in Figure 11.If it is not placed in this situation and exits out ofnon-keratinised mucosa the final gingivalattachment will be poor (Fig. 12).
Other options include:
Accept and observeLeaving the deciduous canine in place and eitherobserving the impacted canine or removing it.Long term, the deciduous canine will need pros-thetic replacement.
Extract the impacted canineIf there is a good contact between the lateralincisor and the first premolar then it has to becarefully considered whether this should beaccepted. The purists of occlusion will argue thatthe premolar is not capable of providing goodcanine guidance. Aesthetically there are prob-lems since the palatal cusp hangs down. This canbe disguised by grinding or rotating the tooth
Fig. 10 The same patient as in Figure 9. The dental pantomogram clearly shows thatboth canines have disimpacted and are now erupting in the line of the arch. The onlyactive treatment was extraction of both upper deciduous canines
Fig. 12 A bucally positioned canine has had a gold chain attachedbut in an incorrect position. The chain should exit mid alveolus andfrom keratinised mucosa
Fig. 11 Palatally impacted canines which have had a flap raised andgold chain bonded to the crowns of the permanent canines
6p319-327.qxd 23/02/2004 10:09 Page 322

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004 323
orthodontically so that the palatal cusp is posi-tioned more distally. The placement of a veneeron the premolar is another way of improving theappearance.
TransplantationCanine transplantation has received poor pressin the past. Many of the problems arose becausethe canines were transplanted with a closedapex. These teeth were seldom followed up withroot fillings on the basis that they would revas-cularise. This is unlikely through a closed apexand it is preferable to treat them as if they werenon-vital. Transplantation is an option whichshould only be reserved for teeth that are inalmost an impossible position and where there isextensive hypodontia or other tooth loss.
Implants Implants are also an option and as single toothimplants improve, this may become morefavoured in future. It is important to rememberthat implants in a growing child will ankyloseand appear to submerge as the alveolus contin-ues to develop. These are not therefore an optionuntil the patient is at least 20 years of age.
Correction of canine positionFavourable indications for correction ofimpacted canines.Canines are moved most easily into their correctposition if the root apex is in a favourable posi-tion. If the tooth lies horizontally it is extremelydifficult to correct this and generally the closerthe tooth to the midline the more difficult thecorrection will be. Treatment is nearly alwayslengthy and can damage adjacent teeth. Figure13 shows a lateral incisor adjacent to a palatallyimpacted canine where the opposite reaction to
pulling the palatal canine out is the labial posi-tioning of the lateral incisor root. Obviously thisis not favourable and the gingival recession willworsen. The force to move the canines can beobtained from elastomeric chain or thread. Figure 14 shows elastomeric chain being used topull the canine labially. An attachment has beenbonded to the tooth, but as the tooth moves to itscorrect position it will be necessary to rebond it.Moving the tooth over the bite sometimesrequires the occlusion to be disengaged with abite plane or glass ionomer cement build ups onposterior teeth, for a few weeks.
An alternative is to use a smaller diameternickel titanium ‘piggy back’ wire with a stiffbase wire to align the tooth (Fig. 15). The thickerbase wire maintains the archform by resistinglocal distortion caused by the traction on thecanine. The nickel titanium piggy back wire pro-duces flexibility and a constant low force, unlikeelastomeric chain or thread which have a highinitial force and then a rapid decay of this force.It is better not to tie the piggy back in fully as thewire needs to be able to slide distally as thecanine moves labially. If tied in fully the frictiondoes not allow this function. It also helps if the
Fig. 13 A lateral incisor adjacent to a palatallyimpacted canine. When the canine is pulledlabially the reaction will be for the lateral rootto move labially. It is essential therefore to usethick rectangular wires during the movement ofpalatally positioned canines. Further labialmovement of the lateral root would bepotentially damaging to the periodontalattachment
Fig. 15 A ‘piggy back’ flexible wire has beendeflected in order to apply traction to the goldchain which has been attached to a palatallypositioned canine. There is a stiff base wirewhich prevents unwanted reactions to thistraction
Fig. 14 Palatally positioned canine being movedwith power chain into the correct position
6p319-327.qxd 23/02/2004 10:11 Page 323

PRACTICE
324 BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004
piggy back wires run through auxiliary tubes onthe first molar bands. One further method whichhas gained some popularity is the use of a sec-tional archwire made of beta-titanium alloy.This wire is formable and flexible, it can bedeflected as a sectional arm and pulls the caninelabially. It is important to use a palatal archwhich cross braces the molars to prevent themmoving into crossbite as an opposite force reac-tion to the buccal movement of the canines(Fig. 16).
The use of heat activated nickel titaniumalloys has also done much to improve the effi-ciency of moving impacted canines into thecorrect position. Figures 17 and 18 show asequence of tooth movements where a nickeltitanium alloy has been deflected, after coolingwith a refrigerant, into the bracket. The lengthof time between the two slides was 8 weeks and
it can be seen how much tooth movement hasoccurred. The transpalatal arch is also usefulanchorage for vertical and antero-posteriortooth movements.
WHAT CAN GO WRONG?There are a number of problems with movingpermanent canines from either a buccal or apalatal position. By and large, the older thepatient the less chance there is of succeeding,and certainly moving canines in adultsrequires caution. If the canines have to bemoved a considerable distance then ankylosisis a distinct possibility as well as loss of vascu-lar supply and therefore pulp death. Treatmentoften takes in excess of 2 years and it is impor-tant to maintain a motivated and co-operativepatient. It is necessary to create sufficientspace for the canine to be aligned and this isusually around 9 mm.
The periodontal condition of canines thathave been moved into the correct position in thearch can deteriorate, this is particularly true ifcare has not been taken to ensure that the canineeither erupts or is positioned into keratinisedmucosa. There may also be damage to adjacentteeth during surgery, or indeed the surgeons candamage the canine itself with burs or otherinstruments. Figure 19 shows the crown of acanine which has clearly been grooved by a burwhich was used for bone removal when thecanine was exposed. It is quite easy to induceroot resorption of adjacent teeth (either the lat-eral incisor or the first premolar), particularly ifcare is not taken in the direction of tractionapplied to the impacted canine. Loss of bloodsupply of adjacent teeth can also occur. It isquite common at the end of treatment to see aslightly darker crown of the permanent canine,this probably results from either a change invascularity and vitality of the canines, or poten-tially haemoglobin products can be producedand seep into the dentine thus changing thecolour of the overlying enamel. The worst sce-nario of all is that the canine ankyloses and willnot move. The protracted length of treatmentalso results in patients abandoning treatment.
Despite all of our improvements in treatmentmechanics and diagnosis for impacted canines,the eruption path is often unpredictable.Canines which have a seemingly hopeless prog-
Fig. 16 Beta titanium sectional arch which is bothformable and flexible can be deflected to applytraction to move the impacted canine buccally
Fig. 17 The impacted canine has had a heatactivated nickel titanium wire deflected intothe bracket
Fig. 18 Same patient as shown in Figure 17nearly 8 weeks later where significant toothmovement has taken place
Fig. 19 The crown of this canine was grooved bya bur used during bone removal when the caninewas exposed
6p319-327.qxd 23/02/2004 10:12 Page 324

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004 325
nosis can sometimes correct their position anderupt. Nevertheless, to sit and observe a patientwhere the canines are clearly in difficulty with-out referral to a specialist would be difficult todefend legally. Hopefully the days of patientsarriving in orthodontic departments withretained deciduous teeth at the age of 16 willdiminish as the profession takes on the chal-lenge of life long learning.
OTHER IMPACTED TEETHThe most common cause of unerupted maxillaryincisors is the presence of a supernumerarytooth. These are often typed as follows:
• Conical• Tuberculate• Odontomes (complex or compound)• Supplemental teeth
There are some conditions which have agenetic basis where impacted teeth are seenmore frequently and this includes cleidocranialdysplasia, cleft lip and palate, gingival fibro-matosis and Down's Syndrome.
It is worth remembering that most centralincisors should have erupted by the age of 7 andlateral incisors by the age of 8. Surprisingly, mostreferrals for impacted maxillary incisors arewhen the patient is 9 years of age. This delay indiagnosis could potentially influence the out-come and it is important that when the contralat-eral incisor has erupted 6 months previouslythere is likely to be a problem. Similarly, if thelateral incisors erupt well before the central inci-sor then consideration should be given to inves-tigating further (Fig. 20).
It is perfectly possible that a supernumerarytooth may be present and not affect the erup-tion of the incisors (Fig. 21). Indeed one of theclinical signs that a supernumerary may bepresent is the evidence of spacing where a supernumerary is in the midline and causinga diastema between the upper incisors. The dif-ferent types of supernumerary teeth seem tohave different implications for treatment.
Conical supernumerary teeth are small andpeg-shaped, they usually have a root and theydo not often affect incisor eruption (Fig. 21), butif they are in the midline they can cause a medi-an diastema. They should only be removed ifthey are adjacent to incisors which need toundergo root movement. Potentially the move-ment of the root against the supernumerarytooth could cause resorption of an incisor root.
Where the supernumerary teeth are tubercu-late these usually have no roots and developpalatally. They often prevent the eruption ofcentral incisors and if they do, they need to beremoved (Fig. 22). Complex and compoundodontomes are rare, but can similarly preventeruption of the permanent incisors and alsoneed to be removed. Obviously, radiographs areneeded to confirm any clinical observationsabout impacted teeth and parallax used in thesame way as for canines in order to locate theposition of the supernumerary teeth. Eighty per
Fig. 20 This patient has both her lateral incisors fairly well eruptedbut retained deciduous teeth. This could easily have been diagnosedsooner and may influence the outcome of final tooth position
Fig. 21 Conical supernumerary which hasnot inhibited the eruption of thepermanent incisors. The supernumerary is in the midline
Fig. 22 Anterior occlusal radiograph which shows both upperlateral incisors to have erupted, both upper deciduous centralincisors are retained and the upper permanent central incisors areunerupted. There are two tuberculate supernumeraries presentwhich are associated with the non-eruption of these upperpermanent central incisors
6p319-327.qxd 23/02/2004 10:13 Page 325

PRACTICE
326 BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004
cent of supernumerary teeth occur in the anteri-or part of the maxilla and there is a male tofemale ratio of 2:1. The incidence in the popula-tion as a whole varies, but is somewhere in theregion of 1–2%.
Treatment of impacted supernumerariesAlthough guidelines have been published fromthe Royal College of Surgeons,3 these reviewwhat the options are rather than defining whatthe best treatment is. In part this is due to alack of good research to show what the bestmethods are.
Obviously if there is an obstruction the soonerit is removed the better. Some suggest exposingthe incisor at the same time or attachment of agold chain in order to prevent re-operation if thetooth fails to erupt. However, this is potentiallydamaging, particularly if bone has to beremoved in order to expose or bond an attach-ment to the tooth with a gold chain brought outthrough the mucosa in order to place tractionand move the impacted incisor.
If diagnosed early and the supernumerary isremoved when the apex of the incisor is openthen eruption of the tooth can be anticipated.Even if there is a need to re-operate at a laterdate, if the tooth has come further down it ismuch easier to either expose the tooth or raise aflap and place an attachment on an incisal edgethat is now much closer to its correct position.Often incisors will erupt quite a long way andthen become impacted in fibrous tissue (Fig. 23).In this situation it only requires a small exposureusually on the palatal aspect to allow the toothto come down. Apically repositioned flaps areoften disastrous and produce poor mucosalattachment. In the main they should be avoided.
Fixed appliances are usually needed in orderto regain lost space where adjacent teeth havedrifted and these appliances are also useful iftraction does need to be applied to the impactedteeth. Removable appliances in this situation areoften cumbersome, although they have beenused with a magnet bonded to the uneruptedtooth and a further magnet embedded into theremovable appliance in order to bring the toothdown. The use of fixed appliances in this situa-tion allows alignment, space management andoverbite correction. Ultimately the early diagno-sis of unerupted teeth is the biggest contributiona practitioner can make to the management ofimpacted teeth.
IMPACTED PREMOLARSWhere crowding exists or where there has beenearly loss of deciduous molars, premolars aresometimes unable to erupt. Often relief ofcrowding (usually extraction of first premolars)allows impacted second premolars to erupt. Sec-ond premolars do seem to have enormous poten-tial to erupt and given time these teeth often findtheir way into the arch (Figs 24 and 25). Often inthe upper arch they displace palatally. There mayalso be clues from the deciduous teeth. If thedeciduous teeth become ankylosed they often
Fig. 24 Dental pantomogram of a patient who appears to havesevere impaction of her lower left second premolar
Fig. 25 The same patient as in Figure 24, 9 months later wherethere has been good eruption of the lower left second premolar.Eventually this tooth made its way fully into the line of the archand it was possible to upright the lower left first molar
Fig. 23 Typical fibrous tissue impaction of the permanent incisor. In this patient asupernumerary had been removed 9 months earlier. The tooth will only require asmall exposure on the palatal aspect to enable it to erupt. The bulge in the labialmucosa is clearly evident and this is where the crown will sit
6p319-327.qxd 23/02/2004 10:14 Page 326

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 6 MARCH 27 2004 327
appear to submerge as alveolar bone growthcontinues. This may indicate the absence of asecond premolar, but sometimes this submer-gence can be seen when permanent successorsare present. Most of these situations will resolve,but it is thought wise to consider removing thesecond deciduous molar if it slips below the con-tact points and there is then space loss as themolar tips forward. Where first molar mesialmigration compromises the contact point rela-tionship, space maintenance might be consid-ered. Figure 26 shows a radiograph of a patientwho appears to have generalised submergencesince all second deciduous molars are seen to besubmerging in all four quadrants. In this situa-tion continued observation of the developmentof the occlusion with appropriate loss of decidu-ous molars is essential. With the extensiverestorations and caries, an argument could bemade for loss of all four first molars in this case.
OTHER IMPACTIONSThe only other impactions to be considered in ageneral form are first molars. These may impactin soft tissue and it is sometimes worth consider-ing occlusal exposure where a first molar has noterupted. This usually occurs in the upper archand can be accepted if the oral hygiene is goodwith minimal caries experience. Impacted molarsof this type quite frequently self correct before orduring eruption of the second premolar. Theremay also be primary failure of eruption and if thetooth fails to move with orthodontic traction thisis usually a good indication that the tooth willnot move. First molars may also impact into sec-ond deciduous molars as they erupt and theoptions then are to try and move the molar dis-tally with a headgear or removable appliance, toconsider using separators (brass wire) to relieve
the impaction or ultimately to remove the seconddeciduous molar if any of these methods fail torelieve the impaction.
It is clear that the biggest single contributionthat can be made to the treatment of impactedteeth is to improve diagnostic skills and definecare pathways with clinical protocols. Earlyreferral does not harm, a late referral willincrease the burden of care for patients andpractitioners.
1. Ericson S, Kurol J. Early treatment of palatally eruptingmaxillary canines by extraction of the primary canine. Eur JOrthod 1988; 10: 283-295.
2. Power S, Short M B E. An investigation into the response ofpalatally displaced canines to the removal of deciduouscanines and an assessment of factors contributing tofavourable eruption. Br J Orthod 1993; 20: 215-223.
3. National Clinical Guidelines. Faculty of Dental Surgery, RoyalCollege of Surgeons of England, 1997.
Fig. 26 Dental pantomogram of a patient with all four seconddeciduous molars submerging. Those which are below the contactpoint (upper right second deciduous molar) should probably beremoved in order to aid eruption. The others should be observed
BDA Information Centre Services
Did you know?• As a BDA member you can gain access to one of
the best dental information services in the world• You don’t have to be based in London to use
the service• You can borrow books, videos and information
packages • You can borrow up to eight items via the postal system
The only cost to you is the cost of the return postage.If you’re not sure what to request then telephone usand we can advise you.
• You are entitled to free MEDLINE searchesTelephone us with a subject and we will send you a list of relevant references with abstracts.
• You can request photocopies of journal articles.There is a small charge for this service and you need tofill in a Photocopy Request Form first. Telephone us ifyou would like one of these forms.
• BDA Members can view the latest Current DentalTitles on our web site free of charge.
For further details of any of these services dial 020 7563 4545.
Contact us via e-mail at:[email protected]
Visit the Information Centre web pages at: http://www.bda.org
Please note: The Information Centre is temporarily relocated in the basement Lecture Theatreduring its major refurbishment — please ring first if you plan to visit
6p319-327.qxd 26/02/2004 15:16 Page 327
chandhu
Rectangle

BRITISH DENTAL JOURNAL VOLUME 196 NO. 7 APRIL 10 2004 391
PRACTICE
Orthodontics. Part 11: Orthodontic tooth movementD. Roberts-Harry1 and J. Sandy2
Orthodontic tooth movement is dependent on efficient remodelling of bone. The cell-cell interactions are now more fully understoodand the links between osteoblasts and osteoclasts appear to be governed by the production and responses of osteoprotegerin ligand.The theories of orthodontic tooth movement remain speculative but the histological documentation is unequivocal. A periodontal ligament placed under pressure will result in bone resorption whereas a periodontal ligament under tension results inbone formation. This phenomenon may be applicable to the generation of new bone in relation to limb lengthening and cranial-suture distraction. It must be remembered that orthodontic tooth movement will result in root resorption at the microscopic level inevery case. Usually this repairs but some root characteristics apparent on radiographs before treatment begins may be indicative oflikely root resorption. Some orthodontic procedures (such as fixed appliances) are also known to cause root resorption.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professor of Orthodontics, Division ofChild Dental Health, University of BristolDental School, Lower Maudlin Street,Bristol BS1 2LY; *Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4811129© British Dental Journal 2004; 196:391–394
● The osteoblast is the pivotal cell in bone remodelling and the link between the osteoblast andosteoclast recruitment and activation is now established
● Excessive orthodontic forces cause inefficient tooth movement and adverse tissue reactions● The mechanisms which prevent root resorption are not fully understood but it remains a
consequence of any orthodontic treatment. The extent and degree of root resorption cannotbe predicted but some indicators are available
I N B R I E F
The histological changes which occur whenforces are applied to teeth are well documented(Figs 1 and 2). Teeth appear to lie in a position ofbalance between the tongue and lips or cheeks.This zone is not completely neutral since tongueforces are usually slightly greater than the lips orcheeks. The periodontal ligament is thought tohave an intrinsic force which has to be overcomebefore teeth move. A notable feature of peri-odontal disease, where this intrinsic force is lost,is splaying, drifting and spacing of teeth. Simi-larly, if there is excessive tongue activity ordestruction of the lips or cheeks (as in cancrumoris) then the teeth will drift.
Very low forces are capable of moving teeth.Classically, ideal forces in orthodontic toothmovement are those which just overcome capil-lary blood pressure. In this situation boneresorption is seen on the pressure side and bonedeposition on the tension side. Teeth rarelymove in this ideal way. Usually force is notapplied evenly and teeth move by a series of tip-ping and uprighting movements. In some areasexcessive pressure results in hyalanizationwhere the cellular component of the periodontalligament disappears. The hyalanized zoneassumes a ground glass appearance but thisreturns to normal once the pressure is reducedand the periodontal ligament repopulated withnormal cells. In this situation a different type ofresorption is seen whereby osteoclasts appear to‘undermine’ bone rather than resorbing at the‘frontal’ edge (Fig. 3).
Mechanically induced remodelling is notfully understood. The role of the periodontalligament has been questioned since toothmovement can still occur even where the peri-
odontal ligament is not functioning normally.The ligament itself undergoes remodelling andthe role of matrix metalloproteinases (MMPs)together with their natural inhibitors, tissueinhibitors of metalloproteinases (TIMPs) areclearly of importance.1
Osteocytes (osteoblasts incorporated intomineralized bone matrix) are situated in a rigidmatrix and are thus ideally positioned to detectchanges in mechanical stresses. They could signal to surface lining osteoblasts and thusbone formation and indeed bone resorptionmay result. There is now good understanding ofkey mechanisms in bone resorption and forma-tion. Bone is formed by osteoblasts which alsohave a role in bone resorption. It is theosteoblast which has receptors for many of thehormones and growth factors which stimulatebone turnover.
By contrast, the osteoclast which resorbsmineralised tissue, responds to very few directhormone actions. Most of the classic agentswhich have direct effects on osteoclasts haveinhibitory actions. For example, Calcitonin andprostaglandin E2 will inhibit osteoclasts fromresorbing calcified matrices.
The recruitment and activation of osteo-clasts to sites of resorption comes from theosteoblast when the latter cell is stimulatedby various hormones. The signal link fromosteoblasts has recently been identified asosteoprotegerin (OPG) and the ligand (OPGL).They both potently inhibit and stimulaterespectively, osteoclast differentiation. Fur-thermore, OPGL appears to have direct effectson stimulating mature osteoclasts into activi-ty. If OPGL is injected into mice there is an
11
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
VERIFIABLE CPD PAPER
NOW AVAILABLE AS A BDJ BOOK
07p391-394.qxd 09/03/2004 16:55 Page 391

PRACTICE
392 BRITISH DENTAL JOURNAL VOLUME 196 NO. 7 APRIL 10 2004
increase in ionised blood calcium within 1 hour. These finding have done much tounravel the final links between bone forma-tion and resorption.
One other role that osteoblasts have in boneresorption is removal of the non-mineralisedosteoid layer. In response to bone resorbing hor-mones, the osteoblast secretes MMPs which areresponsible for removal of osteoid. This exposesthe mineral layer to osteoclasts for resorption. Ithas been suggested that the mineral is alsochemotactic for osteoclast recruitment andfunction.
How mechanical forces stimulate boneremodelling remains a mystery but some keyfacts are known. First, intermittent forcesstimulate more bone remodelling than contin-uous forces. It is likely that during orthodontictooth movement intermittent forces are gener-ated because of ‘jiggling’ effects as teeth comeinto occlusal contact. Second, the key regula-tory cell in bone metabolism is the osteoblast.It is therefore relevant to examine what effectsmechanical forces have on these cells. Theapplication of a force to a cell membrane trig-gers off a number of responses inside the celland this is usually mediated by second mes-sengers. It is known that cyclic AMP, inositolphosphates and intracellular calcium are allelevated by mechanical forces. Indeed theentry of calcium to the cell may come from G-protein controlled ion channels or releaseof calcium from internal cellular stores. Thesemessengers will evoke a nuclear responsewhich will either result in production of fac-tors responsible for osteoclast recruitment andactivation, or bone forming growth factors.An indirect pathway of activation also existswhereby membrane enzymes (phospholipaseA2) make substrate (arachidonic acid) avail-able for the generation of prostaglandins andleukotrienes. These compounds have bothbeen implicated in tooth movement.
The main theories of tooth movement arenow summarised:
BIOMECHANCIAL ORTHODONTIC TOOTHMOVEMENTThis theory simply states that mechanically dis-torting a cell membrane activates PLA2 makingarachidonic acid available for the action of cycloand lipoxygenase enzymes. This producesprostaglandins which feed back onto the cellmembrane binding to receptors which thenstimulate second messengers and elicit a cellresponse. Ultimately, these responses willinclude bone being laid down in tension sitesand bone being resorbed at pressure sites. It isnot clear how tissues discriminate between ten-sion and pressure. It is worth remembering thatcells which are rounded up show catabolicchanges whereas flattened cells (? under tension)have anabolic effects.
BONE BENDING, PIEZOELECTRIC ANDMAGNETIC FORCESThere was considerable interest in piezoelectricityas a stimulus for bone remodelling during the1960s. This arose because it was noted that distor-tion of crystalline structures generated small elec-trical charges, which potentially may have beenresponsible for signalling bone changes associat-ed with mechanical forces. The interest thereforein ‘electricity’ and bone was considerable.
Magnets have been used to provide the forceneeded for orthodontic tooth movement. Classi-cally an unerupted tooth has a magnet attachedto it and a second magnet is placed on an ortho-dontic appliance with the poles orientated toprovide an attractive force. It is unlikely that themagnetic forces alone have any actions on tis-sues. If magnetic fields are broken (as in pulsedelectromagnetic fields) then there is some evi-dence that tissues will respond. It is worth mak-ing the following points about the effects ofmagnetic and electric fields on tooth movement:
• The periodontal ligament is unlikely to trans-fer forces to bone. If the periodontal ligamentis disrupted, orthodontic tooth movement stilloccurs
Intermittent forcesappear to move teethand stimulate boneremodelling moreefficiently than continuous forces
Fig. 1 Pressure side of a tooth being moved. The very vascularperiodontal ligament has cementum on one side and bone on theother where frontal resorption is occurring. Osteoclasts can be seenin their lacunae resorbing bone on it's ‘frontal edge’
Fig. 2 This is a tension site where the bone adjacent to theperiodontal ligament has surface lining osteoblasts and no sign ofany osteoclasts. New bone is laid down as the tooth moves
07p391-394.qxd 09/03/2004 16:56 Page 392

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 7 APRIL 10 2004 393
• Magnetic fields alone have little, if any, effecton tissues
• Pulsed magnetic fields (which induce electricfields) can increase the rate and amount oftooth movement
• When an orthodontic force is applied, thetooth is displaced many times more than theperiodontal ligament width. Bone bendingmust therefore occur in order to account forthe tooth movement over and above the widthof the periodontal ligament
• Physically distorting dry bone producespiezoelectric forces which have been implicat-ed in tooth movement. Piezoelectric forces arethose charges which develop as a consequenceof distorting any crystalline structure. Themagnitude of the charges is very small andthere is some doubt whether they are suffi-cient to induce cellular change.
• It must also be remembered that in hydratedtissues, streaming potential and nerve impuls-es produce larger electrical fields and thus it isunlikely that piezoelectric forces alone areresponsible for tooth movement.2
A wider application of the phenomenon ofmechanically induced bone remodelling isseen where sutures are stretched. In youngorthodontic patients the midline palatalsuture can be split using rapid maxillaryexpansion techniques. The resulting tensiongenerates new bone which fills in between thedistracted maxillary shelves. A similar tech-nique is also used to lengthen limbs. This
method, known as distraction osteogenesis,can be used in any situation where it is hopedthat new bone will be generated. Originallythis was described in Russia where many sol-diers returning from war faced the problem ofnon-union limb fractures. Initially attemptswere made to induce new bone formation bycompressing bone ends. It was only when apatient inadvertently turned the screw forcompression of bone ends in the wrong direc-tion that it was noted excessive new bone for-mation was seen where bone ends were dis-tracted rather than compressed.
This may also have application in patientswhose sutures fuse prematurely (craniosynos-toses such as Crouzon's or Aperts Syndrome).In this situation continued growth of the brainresults in a characteristic appearance of thecranium but more importantly the eyesbecome protuberant with possible damage tothe optic nerve. Treatment involves surgicallyopening the prematurely fused sutures andburring out to enable normal brain growth. Ifdistraction forces are applied prior to this earlyfusion then bony infill could occur at a con-trolled rate. The phenomenon of pressureresulting in bone loss is also seen in pathologi-cal lesions. Much work was done to examinepressures within cystic lesions and to equatethis with the rate of bone destruction. It is nowrecognised that cytokines and bone resorbingfactors produced by cystic and malignantlesions are more likely to be responsible for theassociated bone resorption.
Tension results inbone formation, thiscan be used to generate new bonefor digit lengtheningor suture distraction
Fig. 3 This is an area of excessive pressurewhere the periodontal ligament has beencrushed or ‘hylanized’ and the periodontalligament has lost its structure. There is a largecell lying in a lacunae behind the frontal edgewhich is probably an area of underminingresorption
Fig. 4 Area of root resorption associated withorthodontic tooth movement. The apex ofthe tooth has a large excavation of the rootsurface and this is typical of excessivetipping forces that are placed on the apicesof the teeth
07p391-394.qxd 09/03/2004 16:58 Page 393

PRACTICE
394 BRITISH DENTAL JOURNAL VOLUME 196 NO. 7 APRIL 10 2004
ROOT RESORPTIONThe ability to move teeth through bone isdependent on bone being resorbed and toothroots remaining intact. It is highly probable thatall teeth which have undergone orthodontictooth movement exhibit some degree of micro-scopic root resorption (Fig. 4). Excessive rootresorption is found in 3–5% of orthodonticpatients. Some teeth are more susceptible thanothers, upper lateral incisors can, on average,lose 2 mm of root length during a course of fixedorthodontic treatment. There are specific fea-tures of appliances which can increase the risk ofroot resorption. The following are consideredrisk factors:
• Fixed appliances • Class II elastics• Rectangular wires• Orthognathic surgery
There is also some evidence that the use offunctional appliances appears to cause lessresorption than fixed appliances and may beused to reduce increased overjet where there arerecognised risks of root resorption which includepre-existing features such as:
• Short roots• Blunt root apices• Thin conical roots• Root filled teeth• Teeth which have been previously traumatised
What prevents roots from resorbing is notknown but the following have been suggested:
• Cementum has anti-angiogenic properties.This means blood vessels are inhibited fromforming adjacent to cementum and osteo-clasts have less access for resorption.
• Periodontal ligament fibres are inserted moredensely in cementum than alveolar bone andthus osteoclasts have less access to the cemen-tal layer.
• Cementum is harder than bone and moredensely mineralised.
• Cemental repair may be by a material which isintermediate between bone and cementum.These semi-bone like cells may be moreresponsive to systemic factors such as parathy-roid hormone and thus where roots are alreadyshort (and repaired with a bone/cementum likematerial) the teeth are more susceptible to fur-ther root resorption.
The exact reason why roots generally do notresorb is not known but without this property itwould not be possible to move teeth orthodonti-cally. A number of reviews are available whichcover bone remodelling and tooth movement ingreater depth.3,4
1. Waddington R J, Embery G, Samuels R H. Characterization ofproteoglycan metabolites in human gingival fluid duringorthodontic tooth movement. Arch Oral Biol 1994; 39: 361-368.
2. McDonald F. Electrical effects at the bone surface. Eur JOrthod 1993; 15: 175-183.
3. Hill P A. Bone remodelling. Br J Orthod 1998; 25: 101-107.4. Sandy J R, Farndale R W, Meikle M C. Recent advances in
understanding mechanically-induced bone remodelling andtheir relevance to orthodontic theory and practice. Am JOrthod Dento-fac Orthop 1993; 103: 212-222.
The British Dental Association Research Foundationinvites applications for awards from the Shirley GlasstoneHughes Memorial Prize Fund.
The Prize may be awarded as a single three year projectgrant commencing in 2004, to a maximum of £16,000including all salary ‘on costs' and running expenses.Alternatively, smaller grants may be made to more projects, to the same total. Applications will be considered from dentists in all fields of practice.
Where applications are made by dentists who are not in university employment, the Foundation advises thatapplications should include appropriate supervisoryarrangements involving an independent experiencedresearcher.
The Foundation will favour projects, which will yieldresults of direct clinical relevance.
Shirley Glasstone Hughes Memorial Prize for Dental Research
Application formsand further information areavailable from:
BDA Awards Officer,Members’ Services DepartmentBritish Dental Association, 64 Wimpole Street, London W1G 8YSTel: 020 7563 4174Email: [email protected]
The closing date for applications is Friday 30th April 2004.
07p391-394.qxd 09/03/2004 16:59 Page 394
shilpa
Rectangle

BRITISH DENTAL JOURNAL VOLUME 196 NO. 8 APRIL 24 2004 449
PRACTICE
Orthodontics. Part 12: Combined orthodontictreatmentD. Roberts-Harry1 and J. Sandy2
Dentistry is becoming more sophisticated and capable of providing much higher treatment standards than ever before.Treatments previously considered impossible can now be achieved as a direct consequence of these advances. However, thisincreased complexity of treatment also means that the different branches of dentistry have, as a necessity, become more andmore specialised. It is important that the specialities collaborate in a systematic focused way to ensure the optimal treatmentoutcome with the minimum burden of care for the patient.
1*Consultant Orthodontist, OrthodonticDepartment, Leeds Dental Institute,Clarendon Way, Leeds LS2 9LU; 2Professorin Orthodontics, Division of Child DentalHealth, University of Bristol Dental School,Lower Maudlin Street, Bristol BS1 2LY*Correspondence to: D. Roberts-HarryE-mail: [email protected]
Refereed Paperdoi:10.1038/sj.bdj.4811174© British Dental Journal 2004; 196:449–455
● The dental specialities can collaborate with the treatment of complex cases● Joint treatment planning is essential● A clear treatment plan must be agreed by all parties prior to treatment starting● Responsibility for each treatment stage must be agreed in advance● Combined treatment can produce high quality treatment outcomes in complex cases
I N B R I E F
Recent advances in dentistry, coupled withpatients’ increased expectations and demands,means that some areas of clinical practice havebecome more specialised. An individual dentistis unlikely to have the necessary skills andexpertise to undertake all aspects of treatment.In the management of complex cases joint plan-ning between the orthodontist and the otherdental specialities is important if a satisfactorytreatment outcome is to be obtained. The dentalspecialities cannot work in isolation, and joint-working relationships should be fostered. Whilstorthodontists may be highly skilled in movingteeth, they are heavily dependent on other dentaldisciplines if optimal treatment outcomes are tobe achieved in complex cases.
There are many areas in which orthodontictreatment may be of help to other dental special-ities. Some of these are as follows:
• Missing teeth• Traumatised teeth• Periodontal problems• Occlusal problems• Surgical problems
MISSING TEETHThe choice in these cases is usually to recreatespace for the prosthetic replacement of missingteeth, or to close the space instead.
If an upper central incisor is missing then theusual choice is to open up the space and put insome form of prosthesis. If the space is closedand the lateral incisor is placed in the centralincisor site, then camouflage is difficult because
of the small width of the lateral that results in anunsightly emergence angle of the crown. Incases where an upper incisor is missing, thespace may need to be re-distributed. The patientin Figure 1 had a partial upper denture, and itwas difficult to restore the site with a bridgebecause of the inclination of the upper lateralincisor and the generalised spacing in the upperlabial segment. Fixed appliances were thereforeused to re-distribute the space in the upper arch.In order to maintain the appearance, a bracketwas fitted to a denture tooth. At the completionof treatment the patient was fitted with an upperremovable retainer carrying a denture tooth.Note the proximal metal stops on the upper rightcentral and upper left lateral incisor, to prevent a space re-opening during retention. Finally a bonded bridge restored the site.
When lateral incisors are missing the choice isnot so clear-cut, and often depends on theamount of spacing the patient has, the buccalocclusion and the shape and colour of thecanines. Opening the space for prostheticreplacement produces optimal aesthetics but hasthe disadvantage of the maintenance involvedwith this type of restorative treatment. Closingthe space obviates the need for false teeth butthis may produce a less satisfactory appearance.
Where there is considerable space, the buc-cal occlusion is well inter-cuspated and thecanine has a pointed cusp tip then the usualtreatment is to open the spaces. Closing spaceswill affect the buccal occlusion, and if it is awell interdigitated Class I then this may not bethe best option. The shape of the canines is
12
ORTHODONTICS1. Who needs
orthodontics?2. Patient assessment and
examination I3. Patient assessment and
examination II4. Treatment planning5. Appliance choices6. Risks in orthodontic
treatment7. Fact and fantasy in
orthodontics8. Extractions in
orthodontics9. Anchorage control and
distal movement10. Impacted teeth11. Orthodontic tooth
movement12. Combined orthodontic
treatment
VERIFIABLE CPD PAPER
NOW AVAILABLE AS A BDJ BOOK
08p449-455.qxd 24/03/2004 10:27 Page 449

PRACTICE
450 BRITISH DENTAL JOURNAL VOLUME 196 NO. 8 APRIL 24 2004
important because if they are pointed they willlook unsightly adjacent to the central incisor.Although the tips of the teeth can be trimmedto improve their appearance, this is not alwaysthe best choice. Figure 2 shows a case withspacing in the upper arch due to developmen-tally absent upper lateral incisors. The uppercanines have very pointed tips and it would bedifficult to modify the shape of these teeth tomake them resemble lateral incisors. In addi-tion, the buccal occlusion would make spaceclosure very difficult. Therefore, space in theupper arch was recreated to allow prostheticreplacement. An upper fixed appliance withcoil springs at the upper lateral incisor sitesaccomplished this task. At the completion oftreatment, an upper retainer with denture teeth
was used to restore the missing sites. Thisretainer was worn for a year prior to definitiverestoration with adhesive bridgework.
If the canine teeth are more amenable tomasking, and the buccal occlusion is not wellinter-cuspated with less spacing in the upperarch, then consideration can be given to spaceclosure. Figure 3 shows a case where this wasaccomplished, again using a fixed appliance andthe tips of the canines subsequently trimmed. Agood aesthetic appearance was achieved, but itis worth noting the slightly different colour ofthe canines in relation to the central incisors. Ifnecessary, this can then be masked with veneers.Before the decision to open or close spaces ismade, consultation with a restorative dentist orthe patient's GDP is a pre-requisite.
Fig.1a,b A patient with a missing upper left central incisor,which has been replaced with an inadequate denture
Fig. 1c A fixed appliance with a denture tooth to mask the space
Fig. 1e A retainer with a denture tooth. Note the proximalmetal stops. If these are not used there is a risk of the teethsliding past the denture tooth.
Fig. 1f A bonded bridge was placed 1 year after the removal ofthe fixed appliance
Fig. 1d The space has been redistributed
08p449-455.qxd 24/03/2004 10:29 Page 450

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 8 APRIL 24 2004 451
TRAUMATISED TEETHTraumatised, fractured, intruded or avulsedteeth may sometimes benefit from an orthodon-tic input. Teeth, which are fractured or intruded,may need extrusion, and this can be accom-plished by using a number of different appli-ances and techniques. Figure 4 is an example ofan upper appliance being used to extrude twounerupted upper incisors as an interceptive formof treatment. The upper permanent lateral inci-sors had already erupted; a clear sign that some-thing was wrong. A supernumerary tooth, pre-venting the eruption of the central incisors, wasfirst removed and brackets bonded to the centralincisors. A modified palatal arch was then fittedand attached to the central incisor brackets withwire ligatures. The ligatures were gently activatedto extrude the teeth. Once the teeth had eruptedthe remaining dentition was then allowed todevelop prior to definitive orthodontic treat-ment. A similar technique can also be used toextrude fractured roots so that post-crowns canbe placed on the teeth.
If upper incisors are traumatised and have apoor prognosis it is occasionally possible totransplant teeth to restore these sites. The mainprinciples of transplantation have been welldocumented by Andreasen1 and provided theseare followed, success rates in excess of 90% canbe expected. Premolars are good teeth to replaceupper central incisors because they often havethe same width at the gingival margin as theteeth they are replacing. Figure 5 shows an
Fig. 2a A patient with missing upper lateral incisors andspacing
Fig. 2c Following removal of the fixed appliance Fig. 2d A retainer with denture teeth was fitted and worn forone year prior to definitive restorative treatment
Fig.2b A fixed appliance with coil springs to re-open thespaces for the lateral incisors
Fig. 3a Another case with missing upper lateral incisors
Fig. 3b Because the spaces were small these were closed up using afixed appliance
08p449-455.qxd 24/03/2004 10:30 Page 451

PRACTICE
452 BRITISH DENTAL JOURNAL VOLUME 196 NO. 8 APRIL 24 2004
example of a case where the upper incisors had apoor prognosis and were extracted. The lowerfirst premolars were then transplanted into theextraction sites. Veneers were then placed on thepremolars to produce a satisfactory treatmentoutcome. The advantage of transplantation overimplants is that transplantation can be under-taken at an early age and will grow as the patientgrows. If an implant were placed at this stage itwould, as the child grows, become graduallysubmerged. There is also a risk of ridge resorp-tion by waiting until the patient is old enough tohave an implant placed. In addition the cost oftransplantation is also considerably less than forimplants.
PERIODONTAL PROBLEMSWith advanced periodontal disease, teeth areprone to drift producing an unsightly appear-ance. The teeth can be realigned orthodontically,but prior to this it is essential that all pre-exist-ing periodontal disease is eliminated and thepatient can maintain a meticulous standard oforal hygiene. If treatment is undertaken in the
presence of active disease, very rapid bone losscan result.
Figure 6 shows a patient who had substantialvertical and horizontal bone loss, and as a con-sequence, drifting of the upper teeth hadoccurred, in particular the upper lateral incisor.Alignment of the teeth was achieved using fixedappliances. Near the completion of treatment aresidual black triangle was left between theupper incisors. This is quite a common problemin adults and is caused by the inability of thegingival tissue to regenerate and re-form aninter-dental papilla. In order to reduce the size ofthe black triangle, some inter-proximal reduc-tion was undertaken to reshape the mesial con-tact points of the incisors allowing the teeth tobe brought more closely together. Permanentretention is needed in situations like this becausethe tooth will drift as soon as the appliances areremoved.
OCCLUSAL PROBLEMSOrthodontics can be used to try and produce anoptimal occlusion, and there are many situa-tions in which this can be used.2 The occlusioncan be adjusted to provide canine guidance,and eliminate non-working side interferences.In situations where anterior open bites exist, itis occasionally possible to close these downwithout the need to resort to surgery.3
Sometimes the occlusion can damage theteeth and supporting tissues. Figure 8 is anexample of a patient with a unilateral cross biteextending from the upper central incisor to theterminal molar on the right hand side. Thistraumatic occlusion had produced substantialtooth wear. Treatment was carried out using anupper fixed appliance in conjunction with aquad helix to expand the upper arch, correctthe cross-bite and align the teeth. At the com-pletion of treatment the incisal tips wererestored with composite.
SURGERYThere is a limit to how much tooth movementcan be achieved, and in cases with severe skele-tal discrepancies, orthodontics alone is notcapable of correcting the incisor relationship,or improving facial aesthetics. In these circum-stances close liaison with an oral and maxillo-facial surgeon will be required. An outline ofthe processes involved and the orthodontistsrole in orthognathic surgery has recently beenreviewed.4
Figure 7 shows an example of a patient with aClass III skeletal pattern. There has been somedento-alveolar compensation with the lowerincisors retroclined and the upper incisors pro-clined in an attempt to make incisal contact.There is no scope for correcting the incisor rela-tionship further with orthodontics alone. A com-bined orthodontic/surgical protocol was estab-lished and the patient started treatment withfixed appliances, in order to decompensate theincisors. This made the incisor relationship andthe facial profile worse. Clearly, patients need to
Fig. 4a Thepresence of asupernumerarytooth preventedthe eruption of theupper centralincisors
Fig. 4b Thesupernumerary wassurgically removedand brackets bondedto the upperincisors. A modifiedtrans-palatal barwith wire ligatureswas used to extrudethe teeth
Fig. 4c Once theteeth weresuccessfullyextruded thedentition wasallowed to developprior tocomprehensivetreatment in thepermanentdentition
08p449-455.qxd 24/03/2004 10:31 Page 452

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 8 APRIL 24 2004 453
Fig. 6a The patient complained that her teeth had moved andwere getting worse. She had extensive periodontal diseasethat needed addressing prior to any orthodontic treatment
Fig. 6c A dark triangle between the anterior teeth is acommon complication of treatment in adults. This is becausethe inter-dental papilla fails to regenerate
Fig. 6d Inter-proximal reduction (slenderizarition) of thecontact points helped to substantially reduce the gap andimprove the aesthetics
Fig. 6b Fixed appliances were then used to realign the teeth
Fig. 5a Both the upper central incisors had been badlydamaged after a fall
Fig. 5c The teeth were extracted and two lower premolarstransplanted into the extraction sites. The teeth were thenaligned with fixed appliances
Fig. 5d At the completion of fixed appliance treatmentveneers were placed on the transplanted teeth
Fig. 5b A peri-apicalradiograph indicatedthat the teeth had ahopeless prognosis
08p449-455.qxd 24/03/2004 10:33 Page 453

PRACTICE
454 BRITISH DENTAL JOURNAL VOLUME 196 NO. 8 APRIL 24 2004
Fig. 7a-d Pre-treatmentphotographs of a patient with aClass III incisor relationship andskeletal pattern. The problem isbeyond the scope oforthodontics alone because ofthe skeletal discrepancy
Fig. 7f-i The completed case
Fig. 7e Fixed appliances were used to decompensate theincisors and co-ordinate the arches prior to bi-maxillaryorthognathic surgery
08p449-455.qxd 24/03/2004 10:35 Page 454

PRACTICE
BRITISH DENTAL JOURNAL VOLUME 196 NO. 8 APRIL 24 2004 455
be advised of this prior to the commencement oftreatment. Once the incisors are decompensatedand the arches co-ordinated the patient is readyfor surgery. The maxilla was advanced 7 mmand the mandible set back by 6 mm, producingan overall change of 13 mm in the skeletal rela-tionship. In addition, because the patient had afacial asymmetry, the mandible was rotated inorder to correct this.
As dentistry becomes increasingly sophisti-cated with more treatment options availablethan ever before, no single specialty in dentistrycan work alone to provide the full range of treat-ment options. Some of the most interestingaspects of orthodontic treatment come from
working in a combined approach with one’s col-leagues and it is important to recognize andrespect the skills of other disciplines. Work ofthis nature can be amongst the most satisfyingboth for the clinician and the patient.
The authors thank Paul Cook for the use of figures 5(a-d)
1. Andreasen J O, Andreasen F. Textbook and color atlas oftraumatic injuries to the teeth. 3rd ed. pp671-690.Munksgaard, Copenhagen: Mosby, 1994.
2. Davies S J, Gray R M J, Sandler P J, O'Brien K D O.Orthodontics and occlusion. Br Dent J 2001; 191: 539-549.
3. Kim Y H. Anterior openbite and its treatment with multiloopedgewise archwire. Angle Orthod 1987; 57: 290-321.
4. Sandy J R, Irvine G H, Leach A. Update on orthognathicsurgery. Dent Update 2001; 28: 337-345.
Fig. 8a,b A right-sided cross bite has produced substantialocclusal wear. This would be impossible to correctrestoratively with this occlusion
Fig. 8c An upper fixed appliance with a quad helix was usedto expand the upper arch, correct the incisor relationship andalign the teeth
Fig. 8d At the completion of orthodontic treatmentthe teeth were restored with composite
Guest Leaders
Guest leaders in the BDJ are there to provide an opportunity for anyone involved indentistry (including patients) to write an appropriate comment for publication. Theseare published to accompany the usual Leader from the Editor
Submissions must be between 200 and 500 words, typed and double-spaced.Name, address and telephone number should be supplied, as well as your position inthe dental world.
For further help and guidance, please contact: The Editor, British Dental Journal, 64 Wimpole Street, London W1G 8YS or
E-mail: [email protected]
08p449-455.qxd 24/03/2004 10:42 Page 455
shilpa
Rectangle