A clinical approach to movement disorders neurologist perspectives
44
By Dr. A.V. SRINIVASAN , M.D,D.M,PhD,DSc,FRCP(London),F.I.A.N,F.A.A.N. EMERITUS PROFESSOR THE TAMIL NADU DR MGR MEDICAL UNIVERSITY CHENNAI Former Professor and HEAD, INSTITUTE OF NEUROLOGY A CLINICAL APPROACH TO MOVEMENT DISORDERS-NEUROLOGIST PERSPECTIVES
-
Upload
webzforu -
Category
Health & Medicine
-
view
1.555 -
download
1
Transcript of A clinical approach to movement disorders neurologist perspectives

By
Dr. A.V. SRINIVASAN, M.D,D.M,PhD,DSc,FRCP(London),F.I.A.N,F.A.A.N.
EMERITUS PROFESSOR THE TAMIL NADU DR MGR MEDICAL UNIVERSITY
CHENNAI Former Professor and HEAD, INSTITUTE OF NEUROLOGY MADRAS MEDICAL COLLEGE
A CLINICAL APPROACH TO MOVEMENT DISORDERS-NEUROLOGIST
PERSPECTIVES

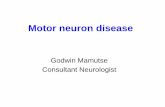
CORTEX
PUTAMEN
D2Enk
D1Sub P
GLOBUS PALLIDUS EXTERNA
SUBSTANTIA NIGRAPARS COMPACTA
SUB THALAMIC NUCLEUS
GLOBUS PALLIDUS INTERNA
PEDUNCULO PONTINE NUCLEUS
THALAMUSINDIRECT PATHWAY
DOPA
DOPA
GABA -
GLUTAMATE+
GLUTAMATE+
GLUTAMATE+
GABA
DI
RECT PATHWAY
NIGRA RETICULATA
BRAIN STEM
GLUT
AMATE
GABA
GABA
GABA
GLUTAMATE
GABA
SUB.
P

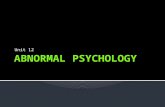
PREVALENCE OF MOVEMENT DISORDERSEssential tremor 415 (Haerer et al.,
1982)Parkinson’s disease 187 (kurland, 1958)Tourette’s syndrome 29-1052 (Caine et al., 1988)Dystonia 33 (Nutt et al., 1988)Hereditary ataxia 6 (Schoenberg, 1978)Huntington’s disease2-12 (Harper, 1992)Wilson’s disease 3 (Reilly and Hutchinson,
1993)Progressive supra-
nuclear palsy 2 (Golbe, 1994)
Rate are given per 100,000 population. For Parkinson’s disease, the rate is 347 per 100,000 for ages over 40 years (Schoemberg et al, 1985).

THE HIERARCHICAL LEVELS FOR RECOGNIZING THE VARIOUS DYSKINESIAS
Level A.Rhythmical Vs. Arrhythmical.Sustained Vs. Non-sustaine.Paroxysmal Vs. Continual Vs. Continuous.Sleep Vs. AwakeLevel BAt Rest Vs. with Action

THE HIERARCHICAL LEVELS FOR RECOGNIZING THE VARIOUS DYSKINESIAS
Level C Patterned Vs. non-patterned Speed : Slow vs. fast Amplitude : Ballistic vs. not ballistic Force : Powerful (painful) vs. easy-to-overcome Suppressibility Vocalizations Self mutilation Complex movements Combinations of varieties of movements Sensory component Continual means over and over again: continuous
means unbroken.

Table –2: DIFFERENTIAL DIAGNOSIS OF RHYTHMICAL AND ARRHYTHMICAL HYPERKINESIASRHYTHMICAL VS. ARRHYTHMICAL
Tremor Akathitic movemntsResting AthetosisPostural BallismAction ChoreaIntention DystoniaDystonia Tremor Hemifacial spasmDystonia myorhythmia Hermifacial spasm

Tabel –2: DIFFERENTIAL DIAGNOSIS OF RHYTHMICAL AND ARRHYTHMICAL HYPERKINESIASRHYTHMICAL VS. ARRHYTHMICAL
Myoclonus, segmental Arrhythmic myoclonus
Epilepsia partialis continua StereotypyMyoclonus, Oscillatory TicsMoving toes/fingersMyorhythmiaPeriodic movements in sleepTardive dyskinesia (tardive stereotypy)

TABLE – 3: DIFFERENTIAL DIAGNOSIS OF SUSTANED HYPERKINESIAS
SUSTAINED CONTRACTIONS VS. NON-SUSTAINED
OR POSTURES CONTRACTIONRigidity All othersDystoniaCculogyric crisisParoxysmal dystoniaDystonic ticsSandifer’s syndromStiff – personNeuromyotoniaCongenital torticollisOrthopedic torticollis

TABLE – 4 DIFFERENTIAL DIAGNOSIS OF PAROXYSMAL AND NON-PAROXYSMAL HYPERKINESIS
Tics Ballism Athetosis
PKC Chorea Tremors
PDC Chorea Tremors
PDC Dystonic movemnts
Dystonic postures
Paroxysmal ataxia Myoclonus, arrhythmic
Myoclonous, rhythimic
Paroxysmal tremor
Stereotypy Tardive Stereotypy
Hypnogenic dystonia
Myokymia Tic status Jumpy stums
PAROXYSMAL VS . CONTINUAL VS. CONTINUOUS

TABLE – 5: DIFFERENTIAL DIAGNOSIS OF HYPERKINESIS THAT ARE PRESENT WHILE ASLEEP OR AWAKE
Hypnogenic Dyskinesias Palatal myoclonus All others Periodic mvts in sleep Ocular myoclonus Oculofacinomasticatory Myorhythmia Myokymia
APPEARS DURING SLEEP VERSISTS DURING SLEEP DIMINISHERS DURING SLEEP

TABLE – 6 : DIFFERENTIAL DIAGNOSIS OF HYPERKINESIAS THAT ARE PRESENT AT REST OR WITH ACTION
At rest only (disappears with action) Akathitic movemnts Paradoxical dystonia* Resting tremor Restless legs Orthostaic tremor*With action only Tremor, postural, action, intention Action dystonia Action myoclonus

TABLE – 6 : DIFFERENTIAL DIAGNOSIS OF HYPERKINESIAS THAT ARE PRESENT AT REST OR WITH ACTION
At rest and continues with action Athetosis Ballism Chorea Dystonia at rest* Jumpy stumps Moving toes/fingers Myoclonus at rest* Myokymia Pseudodystonias* Tics

TABLE 7: THE LOWEST HIERARCHICAL LEVELS IN DIFFERENTIATING THE HYPERKINESIS
PATTERNED NON-PATTERNED (I.E. SAME MUSCLE GROUPS) Dystonia All others Hemifacial spasm Moving toes/fingers Segmental myoclonus Myorhythmia Myokymia Tardive stereotypy Temor

SPEED : FAST VS SLOW
FASTEST INTERMEDIATE SLOWEST Myoclonus Chorea Athetosis Hyperekplexia Ballism moving toes/fingers Hemifacial spasm Jump stumps Myorhythmia Tremors Alkathitic movements Tradive Streotypy
AMPLITUDE: BALLISTIC VS NOT BALLISTIC Ballism Chorea and all others Jumpy stumps would be ballistic, but short Stump keeps the amptitude relatively small

Step 1Step 1 What are the Movements ?Step 2Step 2 Identify the overall syndromeStep 3Step 3 Decide the disease/Syndrome pattern
from differential diagnosisStep 4Step 4 If not, is it Odd dyskinesias?Step 5Step 5 Emphasis on clinical clues and
diagnostic pathwayStep 6Step 6 If primary movement disorder –
Principle investigationsStep 7Step 7 General PlanStep 8Step 8 Investigations for Symptomatic
Movement DisordersStep 9Step 9 Additional tests in specific clinical
syndromesStep 10Step 10 Guidelines for Movement Disorders in
children/Young Adults

STEP 1 – WHAT ARE THE MOVEMENTS
1. AKINETIC OR DYSKINETIC TREMOR JERKS Myclonus Chorea Tic SPASMS Dystonia Rhythmic / arhythmic
Stereo typed / in consistant Continous Action Paroxysms

STEP 2 – IDENTIFY WHAT IS THE OVERALL SYNDROME
Akinetic rigid syndrome Dystonic syndrome Choreic syndrome Tic syndrome Myoclonic syndrome

STEP 3 – WHAT IS THE CAUSE ?
Differential diagnosis of various syndrome
See standard text book

STEP 4 – ODD DYSKINESIAS
A. ODDTREMOR
Mid brain tremor Task specific tremor Neuro pathic tremor Dystonic tremor Primary orhtostatic tremor

STEP 4 – ODD DYSKINESIAS
B. ODD JERKS1.FOCAL MYOCLONUSAngio endothelion a s 1 root Toe jerks alone2.CORTICAL MYOCLONUSEncephalitis Jerks of posture Action myoclonus Stimulus sensitive myoclonus

STEP 4 – ODD DYSKINESIASB. ODD JERKS3. GIANT SOMATO SENSORYSyrinx Repetitive jerks lower limbs
4. HYPEREXPLEXIA5. ODD SPASMSPLMTHemidystonia

STEP – 5EMPHASIS ON CLINICAL CLUES AND DIAGNOSTIC PATHWAY
Encephalopathy and lowdensity lesions in MRI
No infection – Urea cycle defect mitochonrdial or pyruvate disorder, organic acid disorder
Organomegaly Wilson’s Gaucher’s Niemann Pick disease Galactosaemia
Peripheral Neuropathy Adreno myelo – leucodystrophy GM2 Gangliosidosis Krabbe’s disease
Meta Chromatic leukodystrophy Gaucher’s disease Mucolipidosis Mitochondrial disorders Myoclonus and epilepsy Lafora body disease ceroid lipo fuscinosis GM2
Gangliosidosis Gaucher’s disease Polychstic lipomembranous asteodysplasia Mitochondrial disease.

STEP – 5EMPHASIS ON CLINICAL CLUES AND DIAGNOSTIC PATHWAYMacrocephaly Alexander’s disease metachromatic
leukodystrophy Muscle weakness and wasting Neuronal Intranuclear inclusion
disease Vertical supra Nuclear Palsy Niemann pick disease Gaucher’s Disease Cherry Red spotin Macula Sialidosis GM & GM2
gangliosidosis Memann Pick’s disease Dysmorphic features Mucopolysacridoses
Mucolipodiosis Investigations for primary
movement disorder

STEP – 6INVESTIGATIONS FOR PRIMARY MOVEMENT DISORDERS
Imaging (MRI) Exclusion of Wilson <50) Genentic testing Routine blood wing Biochemistry Syphilis

STEP – 7 GENERAL PLAN Extent of nervous system involvement Psychometric evaluation EEG (epilepti form discharges) ENMG (peripheral neruropathy) EMG and VEP

STEP – 8INVESTIGATIONS IN SYMPTOMATICMOVEMENTDISORDERS METABOLIC AND STORAGE DISORDERS
Metabolic encephalopathies categories and investigation
Metabolic Storage Disorders: Categories And Investigation
Degenerative And Systemic Disorders

STEP 9 : ADDITIONAL TEST TO SPECIFIC CLINICAL SYNDROMS
Smptomatic parkinsonism MSA (Anal or uretheral EMG) MRI – Low density in GB/Putamen MSA / PSP
SYMPTOMAIC TREMORS T3T4 – Thyrotoxicosis Peripheral Neuropathy Paraprotenemias Hg. Poisoning Unilateral tremors – opp. Basal ganglia,
Thalamus, Sub Thalamic body of Luys.

STEP 9 : ADDITIONAL TEST TO SPECIFIC CLINICAL SYNDROMS
SYMPTO, CHOREANeuroacanthocystosis – peripheral smear /CK T3,T4 – Thyrotoxicosis Polycythemia rubravira Calcium and magnesium metabolism Hyponatremia Auto immune disorders Syden ham’s chorea
SLE APLS Struct, lesion of Sub Thalamic Body of luy.

STEP 9 : ADDITIONAL TEST TO SPECIFIC CLINICAL SYNDROMS
SYMPTOMATIC TICNeurocanthocytosis
SYMPOTOMATIC MYOCLONUS
Establish the site of origin n the nervous system by electrophysiology
Lafora body disease Neuronal ceroid lipofuscinosis Sialidosis Mitochondrial disordersUnverricht Lundborg Disease

STEP 9 : ADDITIONAL TEST TO SPECIFIC CLINICAL SYNDROMS
SYMPT. DYSTONIA (RARE) Niemann Pick type C – Bone marow Sea blue histiocytes DRD Sandifer syndrome Atalanto axial subluxation (fixed painful torticollis)SYNDROME WITH CONTINOUS MUSCLE FIBRE
ACTIVITYDetailed ENMG study Episodic or paroxysmal movement disorders Video telemetry EEG / distinquish from epilepsy Paroxysmal spasm – M.S. Intermitant ataxias – Amino acid disorders

STEP 9 : ADDITIONAL TEST TO SPECIFIC CLINICAL SYNDROMS
INVASIVE INVESTIGATIONSSkin biopsy (Axilla) Muscle biopsy Peripheral nerve biopsyBrain biopsy

STEP – 10 :GUIDE LINES FRO MOVEMNET DISORDERS IN CHILDREN /YOUNG ADULTS
CHILDHOOD NEURODEGENERATIVE DISEASES THAT MAY PRESENT IN YOUNG ADULT LIFE WITH A MOVEMENT DISORDER
SPECIAL STUDIES TO BE CONSIDERED IN CHILDREN OR YOUN ADULTS WITH A SYMPTOMATIC MOVEMENT DISORDER








CONCLUSIONCONCLUSIONThe composition in this talk has been for the The composition in this talk has been for the
author a long struggle of escape, and so author a long struggle of escape, and so must the reading of it be for most readers if must the reading of it be for most readers if the author’s assault upon them is to be the author’s assault upon them is to be successful - A struggle of escape from successful - A struggle of escape from habitual modes of thought and expression. habitual modes of thought and expression. The ideas which are here expressed so The ideas which are here expressed so laboriously and extremely simple and should laboriously and extremely simple and should be obvious. The difficulty lies not in the new be obvious. The difficulty lies not in the new ideas, but in escaping from the old ones, ideas, but in escaping from the old ones, which ramify, for those brought up as most which ramify, for those brought up as most of us have been, into every corner of our of us have been, into every corner of our mindsminds



Dedicated to my family for making everything worthwhile

READ not to contradict or confute
Nor to Believe and Take for Granted
but TO WEIGH AND CONSIDER
THANK YOUTHANK YOU