
A clinic-based mammography intervention targeting inner-city women
8
A Clinic-Based Mammography Intervention Targeting Inner-City Women Victoria Taylor, MD, MPH, Befi Thompson, PhD, Daniel Lessler, MD, MHA, Yutaka Yasui, PhD, Daniel Montano, PhD, Kay M. Johnson, MD, Janice Mahloch, RN, Mary Mullen, BA, Sue Li, PhD, Gloria Bassett, RN, Harold I. Goldberg, MD OBJECT/VE: The objective was to evaluate the effect of a clinic-based intervention program on mammography use by inner-clty women. DESIGN: A randomized controlled trial employing firm sys- tern methodology was conducted. SETTING: The study setting was a general internal medicine clinic in the university-affiliated county hospital serving metropolitan Seattle. PARTICIPANTS: Women aged 50 to 74 years with at least one routine clinic appointment (when they were due for mare- mography) during the study period were enrolled in the trial (n = 314). INTERVENTIONS: The intervention program emphasized nurs- ing involvement and included physician education, provider prompts, use of audiovisual and printed patient education materials, transportation assistance in the form of bus passes, preappointment telephone or postcard reminders, and rescheduling assistance. Control firm women received usual care. MEASLrREMENTS AND MA/N RESULTS: Mammography com- pletion within 8 weeks of clinic visits was significantly higher among intervention (49%) than control (22%) firm women (p < .001). These effects persisted after adjustment for potential confounding by age, race, medical insurance coverage, and previous mammography experience at the hos- pital (odds ratio 3.5; 95% confidence interval 1.9, 6.5). The intervention effect was modified by type of insurance cover- age as well as prior mammography history. Process evalua- tion indicated that bus passes and rescheduling efforts did not contribute to the observed increases in screenln~ participation. CONCLUSIONS: A cllnic-based program incorporating physi- cian education, provider prompts, patient education materi- als, and appointment reminders and emphasizing nursing in- volvement can facilitate adherence to breast cancer screening guidelines among inner-city women. Received from the Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, Wash. (VT, BT, YY, JM, SL); Department of Health Services (VT, BT, DL), De- partment of Medicine (DL, KMJ, MM, GB, HIG), and Department of Epiderniology (KMJ), University of Washington, Seattle, Wash.; and Battelle Research Institute, Seattle, Wash. (DM). Address correspondence and reprint requests to Dr. Taylor: Cancer Prevention Research Program, Fred Hutchinson Cancer Research Center (MP-702), 1100 Fairview Ave. IV, Seattle, WA 98109. 104 KEY WORDS: mammography; clinic-based intervention; inner- city women. J GEN INTERN MED 1999;14:104-111. B reast cancer is the most common form of malignancy among women, and only lung cancer causes more deaths. ~ In 1992 data showed that 12% of all American women will be diagnosed with breast cancer during their lifetime, and nearly 4% will die from the disease, a Al- though there is no proven method for the primary preven- tion of breast cancer, it has been clearly demonstrated that mammographic screening reduces mortality among women aged 50 years and older.~.2 As a result the Na- tional Cancer Institute has issued cancer control objec- tives for the year 2000, which include the provision of reg- ular mammography to at least 60% of older women. 3 Adherence to breast cancer screening guidelines has risen steadily over the last decade; however, low-income, minority, and inner-city women consistently demonstrate utilization rates that are well below those of the general population. L3-8 Whitman et al. reported, for example, that only 14% of age-eligible women attending three inner-city Chicago clinics had been mammographically screened in the previous year. 8 Similarly, Bastard et al. found that only 21% of women aged 50 years and older who received care at medical facilities operated by the Los Angeles Department of Health Services were receiving routine lTlainiilogralTis. 5 Among women who have not had a recent mammo- gram, the reasons most often cited are not knowing it is necessary and lack of physician recommendation. 7 At least 80% of older women, including those from hard-to- reach groups, however, regularly visit a physician. 9.~~ Therefore, the greatest potenUal for increasing mammog- raphy compliance may lie with interventions that take ad- vantage of contacts with the health care system to edu- cate and motivate patients. The National Coordinating Committee on Clinical Preventive Services has provided a framework for the successful implementaUon of screening maneuvers in primary care settings. This group proposed that a clinical environment that facilitates and supports screening activities requires use of patient tracking and provider reminder systems, the availability of health edu- cation materials to foster patient knowledge and interest, and formalization of nursing involvement.Zz We developed a multifaceted mammography intervention, based on these principles, and implemented the program in an inner-city primary care clinic. In this article we present the results of a randomized trial, using firm system methodology, to
-
Upload
victoria-taylor -
Category
Documents
-
view
214 -
download
2
Transcript of A clinic-based mammography intervention targeting inner-city women

A Clinic-Based Mammography Intervention Targeting Inner-City Women Victoria Taylor, MD, MPH, Befi Thompson, PhD, Daniel Lessler, MD, MHA, Yutaka Yasui, PhD, Daniel Montano, PhD, Kay M. Johnson, MD, Janice Mahloch, RN, Mary Mullen, BA, Sue Li, PhD, Gloria Bassett, RN, Harold I. Goldberg, MD
OBJECT/VE: The objective was to evaluate the effect of a cl inic-based intervent ion program on mammography use by inner-cl ty women .
DESIGN: A randomized controlled trial employing firm sys- tern methodology was conducted.
SETTING: The s tudy se t t ing was a general internal medic ine cl inic in the university-aff i l iated county hospital serving metropol i tan Seatt le .
PARTICIPANTS: Women aged 50 to 74 years wi th at least one routine cl inic appo intment (when t h e y were due for mare- mography) during the s tudy period were enrolled in the trial (n = 314).
INTERVENTIONS: The intervent ion program emphasized nurs- ing invo lvement and included phys ic ian education, provider prompts, use of audiovisual and printed patient educat ion materials, transportation ass i s tance in the form of bus passes, preappointment te lephone or postcard reminders, and rescheduling ass is tance . Control firm women received usual care.
MEASLrREMENTS AND MA/N RESULTS: Mammography com- plet ion wi th in 8 w e e k s of cl inic v is i t s was s ignif icantly
higher among intervent ion (49%) than control (22%) firm women (p < .001). These effects persisted after adjustment for potent ia l confounding by age, race, medical insurance coverage, and previous mammography experience at the hos- pital (odds ratio 3.5; 95% conf idence interval 1.9, 6.5). The intervent ion effect was modif ied by type of insurance cover- age as wel l as prior mammography history. Process evalua- tion indicated that bus passes and rescheduling efforts did not contribute to the observed increases in screenln~ participation.
CONCLUSIONS: A cllnic-based program incorporating physi- cian education, provider prompts, pat ient educat ion materi- als, and appointment reminders and emphas iz ing nursing in- volvement can facilitate adherence to breast cancer screening guidel ines among inner-city women.
Received from the Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, Wash. (VT, BT, YY, JM, SL); Department of Health Services (VT, BT, DL), De- partment o f Medicine (DL, KMJ, MM, GB, HIG), and Department of Epiderniology (KMJ), University of Washington, Seattle, Wash.; and Battelle Research Institute, Seattle, Wash. (DM).
Address correspondence and reprint requests to Dr. Taylor: Cancer Prevention Research Program, Fred Hutchinson Cancer Research Center (MP-702), 1100 Fairview Ave. IV, Seattle, WA 98109.
104
K E Y WORDS: mammography; clinic-based intervention; inner- c i ty women. J GEN INTERN MED 1999;14:104-111 .
B reast cancer is the most common form of mal ignancy
among women, and only lung cancer causes more
deaths. ~ In 1992 data showed tha t 12% of all American
women will be diagnosed with breas t cancer dur ing their
lifetime, and nearly 4% will die from the disease, a Al-
though there is no proven method for the primary preven-
t ion of breas t cancer, it has been clearly demonstra ted
that mammographic screening reduces mortality among
women aged 50 years and older.~.2 As a resul t the Na- tional Cancer Inst i tute has issued cancer control objec-
tives for the year 2000, which include the provision of reg-
u la r mammography to at least 60% of older women. 3
Adherence to breas t cancer screening guidelines has r isen steadily over the last decade; however, low-income,
minority, and inner-city women consistent ly demonstra te
utilization rates that are well below those of the general
population. L3-8 Whi tman et al. reported, for example, that
only 14% of age-eligible women a t tending three inner-ci ty
Chicago clinics had been mammographical ly screened in the previous year. 8 Similarly, Bastard et al. found that only
21% of women aged 50 years a nd older who received
care a t medical facilities operated by the Los Angeles
Depar tment of Health Services were receiving rout ine lTlainiilogralTis. 5
Among women who have not had a recent mammo-
gram, the reasons most often cited are not knowing it is necessary and lack of physician recommendation. 7 At
least 80% of older women, including those from hard-to- reach groups, however, regularly visit a physician. 9.~~
Therefore, the greatest potenUal for increasing mammog- raphy compliance may lie with intervent ions that take ad-
vantage of contacts with the heal th care system to edu-
cate and motivate patients. The National Coordinating Committee on Clinical Preventive Services has provided a
framework for the successful implementaUon of screening
maneuvers in primary care settings. This group proposed
that a clinical envi ronment tha t facilitates and supports
screening activities requires use of pat ient t racking and
provider reminder systems, the availability of health edu-
cation materials to foster pat ient knowledge and interest,
and formalization of nu r s i ng involvement.Zz We developed
a multifaceted mammography intervention, based on these principles, and implemented the program in a n inner-ci ty
primary care clinic. In this article we present the results
of a randomized trial, us ing firm system methodology, to

JGIM Volume 14, February 1999 105
evaluate the impac t of our in tervent ion p rogram on mam-
mography complet ion rates.12.~3
METHODS
Study Sett ing
Our s tudy set t ing was Harborview Medical Center, a county-owned hospi ta l delivering comprehensive medical services to res idents of inner-c i ty metropol i tan Seattle. A low-income al lowance is in effect a t the hospi ta l whereby pat ients wi thout i n su rance coverage are charged for ser- vices on a sl iding scale depending on their abil i ty to pay; this al lowance sys tem is appl ied to charges for mammog-
raphy. The hospi ta l also accepts the Medicare a s s ignment rate as payment in full. Washington State manda te s cover- age of mammographic screening by commercial insurers
and extends m a m m o g r a p h y benefi ts to Medicaid recipi- ents. Harborview Medical Center 's insti tutional guidelines
for m a m m o g r a p h y spec i fy tha t women in their fifties should be screened annual ly , and women aged 60 through 74 years should be screened every 2 years .
The intervent ion p rogram was implemented and eval- uated in the hospi ta l ' s Adul t Medicine Clinic, which pro- r ides ambula to ry care to pa t ien ts aged 18 yea r s and older. It is staffed by genera l internis ts , in ternal medicine
residents, and mid-level prac t i t ioners (Table 1}. The ma- jority of visits are for rout ine medical management . Acutely ill pa t ients are usua l ly seen in a sepa ra te u rgen t care clinic or the hospi ta l ' s emergency depar tment . Because Harborview Medical Center opera tes o ther clinics specifi- cally for immigran ts and refugees, few of the Adul t Medi- cine Clinic pa t ien ts a re non-Engl i sh speakers .
All University of Wash ing ton hospi ta ls , inc luding Harborview Medical Center, par t ic ipate in a d i s t r ibu ted computer ne twork with a centra l da t a repository. This da-
tabase p roduces pa t i en t profile repor ts (which include ba- sic demographic information, pr incipal diagnoses, and current medicat ions) tha t are a t t ached to medical cha r t s
a t the t ime of each pa t ien t visit. As pa r t of th is project, a prevent ion registry component of the repor t was opera- tionalized. Specifically, the date of each pa t ien t ' s l a s t m a m m o g r a m (or a s t a t emen t indica t ing the hospi ta l had no record of m a m m o g r a p h y completion) au tomat ica l ly ap-
pea r s on the report . The hospi ta l ' s compute r sys tem is also used to ma in ta in and upda t e clinic appo in tmen t
schedules . Finally, i t enables the hospi ta l ' s radiology de- p a r t m e n t to keep up- to -da te records of pa t ien ts ' mam- mography s ta tus .
Study Des ign
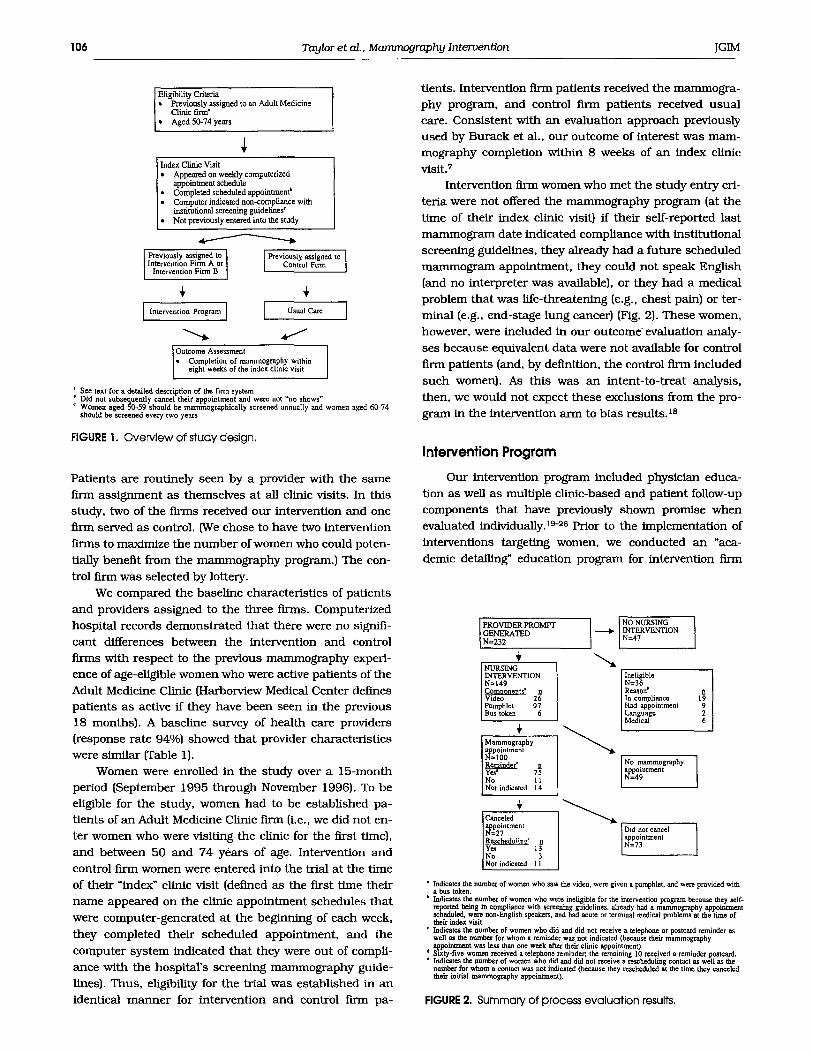
Our s tudy protocol was approved by the Universi ty of Wash ing ton Ins t i tu t ional Review Board. ~4 An overview of
the s tudy design is provided in Figure 1. We conducted a randomized controlled tr ial us ing firm sys tem methodol- ogy. This approach has been successful ly appl ied to clini-
cal, educat ional , and hea l th services r e sea rch in a variety of sett ings. 12,1a,ls-17 Randomized tr ials b a s e d on the firm sys tem utilize ongoing randomiza t ion of all new pa t ien ts and providers to equivalent group prac t ices or firms. Ran- domized tr ials can then be conduc ted by mak ing an ex- per lmenta l change in some firms while ma in ta in ing u s u a l care in other firms. The effect of any change is evaluated
by compar ison between intervent ion and control firm pa- t ients, la A detai led descr ip t ion of firm sys tem methods has previously been provided by C e b u l ) 2
Since 1987 the Adul t Medicine Clinic a t Harborvtew Medical Center has opera ted as three firms. Specifically, pa t i en t s are randomized to one of three f irms at the t ime of thei r first clinic visit, In addit ion, all providers are ran- domized to one of the f irms before they s t a r t providing pa- t ient care in the Adult Medicine Clinic (blocking is u sed to ensure each firm has a s imilar n u m b e r of interns, second- yea r res idents , th i rd-year res idents , a n d a t t end ing physi - cians). Therefore, there should be no differences in the types of pa t ien ts or types of care provided across firms.
Table I. Provider Characteristics at Baseline*
Intervention Intervention Firm A~ Intervention Firm B~ Firms A and B
Characteristic (n = 19) (n = 15) Combined (n = 34) Control Firmw
(n = 15)
Age (mean), years 33 33 33 34 Male, n (%) 8 {42) 9 (60) 17 (50) 9 (60) Level of training, n (%)
Attending physician 8 (42) 7 (47) 15 (44) 6 (40) Resident 10 (53) 7 (47) 17 (50} 8 (53) Mid-level 1 (5) 1 {7) 1 (6) 1 (7)
Weekly clinic sessions (mean), n 1.4 1.0 1.2 1.1
*Racial characteristics of providers were not collected. No statistically signt.ficant differences occurred acrossfirms. tall intervention flrm A providers completed the survey. I~wo interventlon.firm B providers did not complete the survey. ~One control f irm provider did not complete the survey.
106 Taylor et at., Mammography Intervention JGIM
Elig~il i ty Criteria �9 Previously assigned to an Adult Medicine
Clinic firm" '~ Aged 50-74 years
Index Clinic Visit �9 A p p e a ~ on weekly computerized
a l ~ i n t m e a t schedule �9 Completed scheduled appointment b * Computer indicated non-compliance with
institutional screening guidelines * �9 Not previously entered into the study
Previously assigned to [ Intervention Firm A or
Intervent on Firm B
Previously assigned to ] Control Firm
r r
te entionpro rao i [ ]
Outcome Assessment �9 Completion of mammography within
eight weeks of the ndex clinic vie t
' See text for a detailed description of the firm system ) Did not subsequently cancel their appointment and were not "no shows" r Women aged 50-59 should be mammographically screened annually and women aged 60-74
should be screened every two years
FIGURE 1. Overview of study design.
Patients are routinely seen by a provider with the same
firm ass ignment as themselves a t all clinic visits. In this
study, two of the firms received our intervention and one
firm served as control. (We chose to have two intervention
In-ms to maximize the n u m b e r of women who could poten-
tially benefit from the mammography program.) The con-
trol firm was selected by lottery.
We compared the basel ine characteristics of pat ients
and providers assigned to the three firms. Computerized
hospital records demonstra ted that there were no signifi-
cant differences between the intervent ion and control firms with respect to the previous mammography experi-
ence of age-eligible women who were active pat ients of the
Adult Medicine Clinic (Harborview Medical Center defines pat ients as active ff they have been seen in the previous
18 months). A basel ine survey of health care providers (response rate 94%) showed that provider characteristics
were similar (Table 1).
Women were enrolled in the s tudy over a 15-month
period (September 1995 through November 1996). To be
eligible for the study, women had to be established pa- t ients of an Adult Medicine Clinic firm (i.e., we did not en-
ter women who were visiting the clinic for the first tame),
and between 50 and 74 years of age. Intervention and
control firm women were entered into the trial at the time
of their "index" clinic visit (defined as the first t ime their
n a m e appeared on the clinic appoin tment schedules tha t
were computer-generated at the beginning of each week,
they completed their scheduled appointment , and the
computer system indicated that they were out of compli-
ance with the hospital 's screening mammography guide-
fines). Thus, eligibility for the trial was established in an
identical m a n n e r for intervent ion and control firm pa-
tients. Intervention firm patients received the mammogra- phy program, and control firm patients received usua l
care. Consistent with an evaluation approach previously used by Burack et al., our outcome of interest was m a m - mography complet ion within 8 weeks of an index clinic visit. 7
Intervention firm women who met the study entry cri-
teria were not offered the mammography program (at the
time of their index clinic visit} if their self-reported last
mamrnogram date indicated compliance with institutional
screening guidelines, they already had a future scheduled
mammogram appointment, they could not speak English
{and no interpreter was available}, or they had a medical
problem that was life-threatening (e.g., chest pain} or ter-
minal (e.g., end-stage lung cancer} {Fig. 2}. These women,
however, were included in our outcome ~ evaluation analy-
ses because equivalent data were not available for control
firm patients {and, by definition, the control firm included
such women}. As this was an intent-to-treat analysis,
then, we would not expect these exclusions from the pro-
gram in the intervention arm to b ias results. 18
lnteNention Program
Our intervention program included physician educa-
tion as well as multiple clinic-based and patient follow-up
components that have previously shown promise when evaluated individually. 19-28 Prior to the implementat ion of
interventions targeting women, we conducted an "aca-
demic detailing" education program for intervention firm
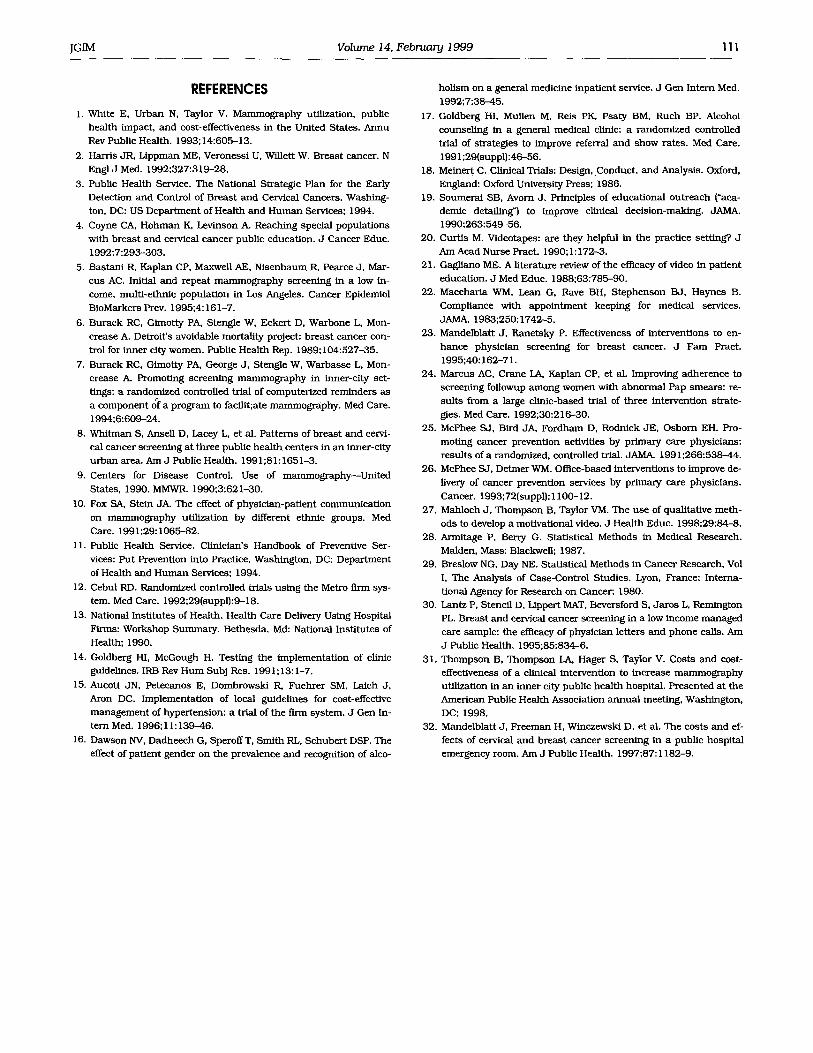
PROVIDER PROMPT NO NURSING I GENERATED t, I=N 47RVENTION I I,N._=232
NURSING INTERVENTION N=149 Comnonents' n Video 26 Pamphlet 97 Bus token 6
Mammography appointment N=IO0
I Reminder" n
l Ye# 75 NO 11 Not indicated 14
Canceled appointment N=27 Rescbedulin~ * n IYes No Not indicated I 1
--.., Ineligible N=36 Reason ) R In compliance 19 Had appointment 9 Language 2 Medical 6
No i~ammography I appomtment N=49
Did not cancel appointment I N=73
' Indicates the number of women who saw the video, were given a pamphlet, and were provided with a bus token.
b Indicates the number of women who were ineligible for the intervention program because they self- being in compliance with screening guidelines, already had a mammogrephy appointment
uled, were non-English speakers, and had acute or terminal medical problems at the time of their index visit. Indicates the number of women who did and did not receive a telephone or postcard reminder as well as the number for whom a reminder was not indicated (because their mammography al[;pointment was less than one week after their clinic appointment). Sixty-five women received a telephone reminder; the remaining I0 received a reminder postcard.
�9 Indicates the number of women who did and did not receive a rescheduling contact as well as the anmbet for whom a contact was not indicated (because they rescheduled at the time they canceled their initial mammography appointment).
FIGURE 2. Summary of process evaluation results.

]GIM Volume14, Februanj1999 107
providers. 19 A chief resident in internal medicine met indi-
vidually with each physician and discussed the effective- ness of mammography, screening guidelines, breast cancer risk factors, and women's barriers to screening. Women
were offered the clinic-based intervention components be-
fore seeing their health care provider. The project employed
a project nurse who worked in the clinic 20 hours per week. Clinic-based intervention activities were imple-
mented by this research nurse when she was available, and by the regular clinic nurs ing personnel at other times.
(The regular clinic nurses were trained by the project nurse
prior to intervention implementation.) All follow-up inter-
vention activities were implemented by the research nurse.
As described above, our intervention program included a computer-generated provider mamrnography prompt
that routinely appeared on intervent ion firm pat ient pro-
file reports (for those women never screened at the hospi- tal or out of compliance with ins t i tu t ional guidelines for
interval screening). A separate nu r s ing prompt form (that
included a brief series of process evaluation questions)
was also at tached to the front of pat ient charts. If pat ients
agreed to a mammogram appointment , the nurse high- lighted the pat ient profile prompt and at tached a com-
pleted radiology depar tment mammography request form
for physician signature, Whenever possible, mammogram
appointments were scheduled before women left the clinic.
When discussing nmmmography, nurses invited women
to watch a motivational video, provided an informational
pamphlet, and offered t ranspor ta t ion ass is tance (in the
form of bus passes) to facilitate completion of scheduled
screening appointments . Our video, which was developed
for the project u s ing qualitative data Fmdings, follows a
woman through her first mammogram and emphasizes
role modeling. 27 It uses a "talk show" format with three
women panel is ts giving their reasons for not having mam-
mography, and members of the audience providing testi- monials addressing each barrier; a female physician pan- elist also participates in a short discussion about breast
cancer screening. Barriers addressed in the video include concerns about embar ra s smen t and pain in association
with mammography, perceptions tha t mammograms can
cause cancer, beliefs about the necessity of mammogra- phy for women without a family history of breas t cancer,
and lack of physician recommendat ion for breas t cancer
screening. The pamphle t addresses key facts us ing a
ques t ion-and-answer format (e.g., "Do I need a mammo-
gram? Yes, research shows tha t all women over 50 clearly benefit from regular mammograms.").
Those women who scheduled a mammogram appoint-
ment more t h a n a week after their index clinic visit re-
ceived a telephone or postcard reminder (depending on
whether or not they could easily be reached by telephone).
In addition, the radiology depar tment computerized data-
base was systematically accessed to check whether each
woman at tended her scheduled mammogram appoin tment
and, ff not, whether she had rescheduled the appointment
herself. Those pat ients who had neither at tended nor re-
scheduled mammography were contacted by the project
nurse and encouraged to make another appointment.
Data Collection and Analysis
We ascertained each woman 's age, race, heal th insur-
ance coverage, and prior history of mammography (yes vs no) at Harborview Medical Center through linkage with
the hospital 's computer network. (Prior mammography at
the hospital was our bes t estimate of whether women had
or had not previously been screened.) Similarly, the com-
puterized system was accessed to determine ff women did or did not complete mammography within 8 weeks of their visit to the Adult Medicine Clinic.
We used the • test and, when necessary, Fisher 's
Exact Test to compare the characteristics (i.e., age, race,
insu rance coverage, and previous mammography experi- ence) of intervention and control fLrm pat ients as weU as
the proportions of intervention and control women who
received marnmography within 8 weeks of their index
clinic visit. 2s Uncondit ional logistic regression techniques
were used to examine the intervent ion effect after adjust-
ing for demographic covariates (i.e., ma in effects model).
To assess any differential intervent ion effect among sub- groups (e.g., by race), an interact ion term for s tudy a rm
(intervention vs control) and the relevant demographic co-
variate was added to the ma in effects model and tested. 29 We also compared the intervention effects among women
who received the clinic-based intervent ions from the
project nu r se and those who received intervent ions from
regular clinic nu r s i ng personnel .
During February 1996, a low-intensity, direct marl
~ te rven t ton (invitational letter) targeting intervent ion firm
(but no t control firm} women who were out of compliance
with insti tutional screening mammography guidelines was
initiated. Women were identified for the direct marl ihter- vention at 6-month intervals, based on month of birth. Because the letters could have reinforced the clinic-based
mammography program, we also examined the propor- t ions of intervention and control women who completed
mammography within 8 weeks of their index among the
subgroups of intervention firm women who did and did not receive a direct marling before, or within 8 weeks of their index clinic visit.
Finally, a process evaluat ion was conducted to assess
the delivery of the intervent ion program components . This
involved recording, for each intervent ion woman, whether
the program was init iated as well as which intervention
components were actually provided (e.g., provider educa-
tion, pamphlet, bu s pass, and appoin tment reminder).
RESULTS
Study Group Characteristics
During the 15-month s tudy period, 314 women were
emered into the randomized trial: 129 from intervention

108 Taylor et al_, Manunography Intervention JGIM
f inn A, 103 from intervention firm B, and 82 from the con-
trol firm (Table 2). TWo thirds (66%) of the women were in their fkfLies (as would be expected because of the differen- tial inst i tut ional screening mammography guidelines for
the 50-59 and 60-74 age groups). The majority of s tudy part icipants were either African American (39%) or white
{42%). The remainder were Asian, Native American, or of
mixed race. Ninety percent of the s tudy group had com-
mercial insu rance (24%), Medicaid (31%), or Medicare
(35%) coverage. Less t h a n one half (46%) of the s tudy
part icipants had previously been mammographically
screened at the hospital. The age distr ibutions as well as
the mammography history of intervention and control firm women were similar. Some significant differences were de-
tected, however, between the intervention and control firm
women. Fewer African Americans and whites, bu t more Asians and Native Americans were in the intervention
firms than the control funn. Twice the n u m b e r of interven-
tion firm compared to control firm women had commercial
insurance. Fewer had Medicare or Medicaid.
O u t c o m e E v a l u a t i o n
As presented in Table 3, nearly one half of the inter-
vention firm women (49%) completed mammography within
eight weeks of their index clinic visit, compared with 22%
of the control fn-m women (p < .00 I). A statistically signif-
icant intervention effect was observed for intervention
firm A (55% completed mammography) versus the control
firm (p < .001) as well as for intervention firm B (41%
completed mammography) versus the control firm (p <
.01). Bivariate comparisons of mammography completion
rates among subgroups of women indicated that our in-
tervention effect was significant for the 50-59 and 60-74 age groups, African-American and white women, pat ients with Medicare coverage, and the u n i n s u r e d (p < .05). In addition, the intervention program was effective for
women with (p < .001) and without (p = .06) a history of
mammographic screening at the hospital.
Multivariate analyses showed that after ad jus tment for age, race, insurance coverage, and previous mammog-
raphy, intervention firm women had more t han three
t imes higher odds of part icipating in screening within 8
weeks of their index clinic visit t h a n control firm women
(odds ratio 3.5; 95% confidence interval 1.9, 6.5). Insur- ance coverage modified the intervent ion effect (p < .01);
women with Medicare coverage or no insurance demon-
strated greater effects t h a n those with commercial insur -
ance or Medicaid. Previous mammography at Harborview
Medical Center also enhanced the intervent ion effect (p =
.07). Our logistic regression analyses showed no signifi-
can t differential intervention effect by age group or race
(i.e., interact ion terms for those demographic variables
were not significant).
Fifty-eight percent of the intervent ion firm women
saw the project nu r se (as opposed to one of the regular
clinic nurses). The intervent ion effect was similar among
women who received intervent ion program components
from the project nu r se (47% completed mammography
within 8 weeks) and pat ients seen by a regular clinic
nurse (51% completed mammography). Our results indi-
cate that the direct mail intervent ion had no reinforcing
effect. Specifically, 47% of the women who received a
mailing prior to, or within 8 weeks of their index clinic
Table 2. Characteristics of Patients Entered into the Study
Characteristic
Intervention Intervention Intervention Firms A and B Control
Firm A Firm B Combined Firm (n = 129), (n = I03), (n = 232), (n = 82),
n (%) n (%) n (%) n (%)
All Women (n = 314),
n (%)
Age 50-59 years 86 (67) 62 (60) 60-74 years 43 (33) 41 (40)
Race*t African American 55 (43) 33 (32) White 49 (38) 44 (43) Othert 25 (19) 26 (25)
Insurance*t Commercial 36 (28) 28 (27) Medicaid 36 (28) 33 {32) Medicare 44 (34) 35 (34) None 13 {10) 6 (6)
Previous mammography t Yes 63 (49) 38 (37) No 66 (51) 65 (63)
148 (64) 58 (71) 84 (36) 24 (29}
88 (38) 35 (43) 93 {40) 40 (49) 51 (22) 7 (9)
206 {66} 108 (34)
123 (39) 133 (42)
58 (18)
64 (28) 10 (12) 74 (24) 69 (30) 29 (36) 98 (31) 79 {34) 32 (39) i 11 (35) 19 (8) 11 (14) 30 (10)
101 (44) 44 (54) 131 (56) 38 (46)
145 (46) 169 (54)
*Significant difference for intervention f irms A and B combined versus control f irm (p ~ .05). tSignificant difference for intervention f irm B versus control f i rm (p < .05). ~Asian or Native American.

]GIM Volume 14, February1999 109
Table 3. Mammography Completion Rates by Patient Characteristics
Characteristic
Completed Mammography, (@/0) Intervention Control
Firms Firm (n = 232) (n = 82)
Age 50-59 years* 52 28 60-74 years* 40 8
Race African American* 48 20 White* 43 23 Other 57 29
Insurance Commercial 53 50 Medicaid 42 34 Medicare* 46 6 None* 58 9
Previous mammography Yes* 63 23 Noi 37 21
All women* 49 22
*[email protected]~t difference for intervention firms and control firm ~ < .05). Difference for intervention firms and control firm ~ <. I 0).
visit completed mammography compared with 50% of the patients who did not receive a mailing.
Process Evaluation
Our process evaluation focused on monitoring deliv- ery of the intervention components . All b u t 3 (91%) of the
35 intervention firm providers participated in our aca-
demic detailing program. Figure 2 summarizes process
evaluation resul ts for the 232 intervent ion firm women
who had a provider prompt generated on their pat ient profile. Nurses at tempted to initiate the intervent ion pro-
gram for 185 (80%) of these patients. (Women did not re- ceive the intervent ion when the clinic was particularly
busy, or when float nu r se s who were unfamil iar with the program staffed the clinic.} Because 36 of these women were found to be ineligible, nu r se s actually discussed mammography with 149 women; 49 of the women who re- ceived our intervent ion declined a mammography ap-
pointment. Fifteen (32%) of the 47 women with a provider
prompt on their pat ient profile, b u t no nu r s ing interven-
tion, completed screening. In comparison, 86 (58%) of the
patients who received the nu r s ing intervention had a
mammogram within 8 weeks of their index clinic visit. It is
of note tha t only 1 of the 13 intervention firm women who
received a reschednling contact (after canceling their ini-
tial mammogram appointment) participated in screening.
DISCUSSION
Burack et al. reported resul ts in 1994 from a ran-
domized trial of a program to enhance mammography
participation in five clinics serving residents of inner-ci ty
Detroit7 A "limited" intervention (physician breas t cancer control educat ion and el imination of out-of-pocket mam-
mography expenses for patients) was compared with a
~full" intervention that included all the elements of the
limited intervent ion as well as computer-generated physi- c ian prompt sheets, pat ient reminders prior to scheduled
mammography appoin tments (at two sites), and a n ap- po in tment rescheduling system. Compared with the lim-
ited intervention, full intervention was associated with a
significant absolute increase in mammography comple-
t ion of 18% (compared with 27% in our study). The pro-
portions of physician prompt forms re turned with their
process evaluation sections completed (indicating the pro-
r ider reminder had been acted upon) varied from 39% to
78% by project site (compared with 80% of the process evaluation forms completed by nu r se s at our one s tudy
site). Between 10% and 25% of women initially declined
mammography appoin tments (compared with 33% at our
one s tudy site). Finally, consis tent with our findings, re-
scheduling efforts did not contr ibute to enhanced mam-
mography participation.
A group of investigators in Wisconsin in 1995 evalu-
ated a breas t cancer screening intervent ion targeting so-
cially disadvantaged women. 3~ Study part ic ipants were
randomized to intervent ion or control s tatus. The inter-
vent ion consisted of a physician reminder letter followed
by a telephone call from a health educator; telephone con-
tacts included barrier-specific counsel ing as well as as-
's istance with appoin tment scheduling. Mammography
completion rates were significantly higher among the inter-
vention group after 6 months. However, it should be noted that the s tudy populat ion was uniformly non-Hispanic
white and received care through a heal th main tenance
program.
Interventions to improve delivery of screening maneu- vers in the primary care setting have been variably suc-
cessful. In general, physician reminders have been most consistently effective in improving breas t cancer screen-
ing with reported increases in mammography util ization of between 5% and 20%. 23 In this project mammography completion rates among intervent ion firm women were
32% in association with physician educat ion and a pro- vider prompt on pat ient profile reports (10% greater t h a n
for control firm women), b u t 49% when the nu r s ing inter-
vent ion was also provided. This suggests tha t the nu r s ing
components had an effect over and above tha t of the pro-
vider educat ion and physician prompt.
Recently, increased a t tent ion has been given to the
use of videotapes in heal th education, and video equip-
men t is now commonplace in hospitals and medical clin-
ics. 2~ This method of heal th educat ion is also practical be-
cause after a modest initial inves tment the ongoing costs are relatively small. 2~ A relatively small proportion (17%}
of the pat ients who received our n u r s i n g intervent ion
watched the video. Qualitative information from the nu r ses involved with the project suggests tha t the video

l l 0 Taylor et al., M ~ r a p h y Intervention ]GIM
component was disruptive to pat ient flow during busy
clinic days (the video equipment was located in a waiting room cubicle), and women were concerned about "miss-
ing" their physician appo in tment while they were watch- ing the video. However, the research nurse also perceived
that the video saved time that might otherwise have been devoted to individual pat ient instruct ion. In some clinic
settings it might be possible to bui ld video viewing time
into appoin tments and provide a separate room for health
educat ion activities.
Marcus et al. tested several clinic-based interven-
tions, including t ranspor ta t ion assistance, designed to
improve adherence to screening follow-up among Los An-
geles women with abnormal Pap smears; over one quar ter
(27%) of the women who were given bus passes reported
us ing them, and this intervent ion signlficanfly improved
pat ient compliance. ~ Few of the women in our s tudy (4%)
accepted b u s passes. Reasons for the low usage may in-
clude concerns abou t the safety of public t ranspor ta t ion
among an older pa t ient populat ion (91% of women in the Los Angeles s tudy were less t h a n 45 years old), and the
availability of valet parking for pat ients seen at Harbor-
view Medical Center. In addition, the research nu r se re-
ported that some women had their own monthly bus
passes. It is possible tha t r e imbursement for taxicab fares
might be a more effective form of t ranspor ta t ion assis-
tance for women aged 50 years and over. There is relatively little information on the variation
in effectiveness of clinic-based mammography interven-
t ions across pat ient groups. 23 We found our program to
be effective for women in their fifties (23% absolute in- crease in mammography use) as well as older pat ients
(32% increase in use). It also appeared to enhance mam-
mography participation among women from diverse racial
groups. However, the intervent ion program had a differ- ential effect, depending on type of insurance coverage.
The absolute screening increases were subs tant ia l among
pat ients with Medicare (40%) and the un in su red (50%), bu t not for those with commercial insurance (3~ and
Medicaid (8~ It is possible tha t commercially insured
women responded to the intervent ion program, bu t chose to be screened at another health care facility.
A detailed analysis of the costs and cost-effectiveness
of our intervent ion program will be the subject of a future report. However, prel iminary analyses suggest tha t the cost of delivering the program components was approxi-
mately $200 per pat ient and $700 per additional mammo-
gram completed, al In comparison, Mandelblatt et al. re-
cently reported the costs of a nu r s ing intervent ion to
provide breas t cancer screening within the context of
emergency depar tment visits; the average cost per woman exceeded $1,800. 32
Ongoing randomizat ion of pat ients to firms does not
guarantee tha t similar populat ions will result, especially
when subgroups are targeted (e.g., one age group or gen-
der). In addition, "randomization decay" can occur from differential dropout rates tha t eventually lead to noncom-
parability of long-term patients. 12 In this s tudy the n u m -
bers of women entered into the s tudy varied by firm. (The
total n u m b e r of Adult Medicine Clinic pat ients assigned to each firm reflects the pat tern seen among women entered
into our trial.) There also were significant differences be-
tween the intervention and control firms with respect to
race and insurance coverage. Such differences should not theoretically occur in a firm system and suggest tha t ran-
domization decay had occurred in the Adult Medicine
Clinic. Therefore, our s tudy design should be considered quasi-experimental.
In firm trials behavioral change can be affected by
dominan t physicians dis tr ibuted asymmetrically across
fu-msJ 2 We did not collect data on the providers seen a t
index clinic visits. However, there are approximately 50
providers in the Adult Medicine Clinic, and the majority of
physicians spend only one half-day in the clinic each
week. Also, a significant intervent ion effect was seen in
both intervention firms. As a result, we cannot rule out
the possibility that one or a few physicians from each of these firms may be responsible for the intervent ion effect
reported.
In contras t to Burack et al., we only evaluated our in-
tervention program in one clinic. In addition, our s tudy
design excluded new pat ients as well as women whose ap-
poin tments did no t appear on the clinic schedule at the
beginning of each week. Therefore, pat ients who routinely
schedule appoin tments at short notice were not included
in the trial. Computerized hospital records indicate that
about 500 women aged 50 to 74 years complete clinic vis-
its in any 15-month period. Therefore, we estimate that
about one third of the age-eligible women who visited the
clinic dur ing our intervention period were not entered into
the study. Women who schedule their visits at short no-
tice may be less likely to participate in mammography
programs t h a n those who do not.
Unlike previously reported clinic-based initiatives,
our mammography program was based on recent recom- mendat ions from the National Coordinating Committee on Clinical Preventive Services.t1 Therefore, our primary re-
search objective was to assess the overall impact of an in-
tegrated set of mammography interventions. A limitation of the s tudy design was tha t it precluded an assessment
of the individual and interactive effects of program com- ponents. Further, it is unc lea r to what extent our findings are generalizable to other heal th care facilities serving so-
cially disadvantaged populat ions. However, our large in-
tervention effect suggests tha t a clinic-based mammogra-
phy intervention that emphasizes nu r s ing involvement
and incorporates physician education, provider prompts,
health educat ion materials, and pa t ient appoin tment re-
minders can enhance adherence to breas t cancer screen-
ing guidelines by inner-ci ty women.
This work was supported by grant 62119 from the National Cancer Institute.
JGIM Volume 14, February 1999 111
REFERENCES
I. White E, Urban N, Taylor V. Mammography utilization, public health impact, and cost-effectiveness in the United States. Annu Rev Public Health. 1993;14:605-13.
2. Harris JR, Lippman ME, Veronessi U, Willett W. Breast cancer. N Engl J Med. 1992;327:319-28,
3. Public Health Service. The National Strategic Plan for the Early Detection and Control of Breast and Cervical Cancers. Washing- ton, DC: US Department of Health and Human Services; 1994.
4. Coyne CA, Hohman K, Levinson A. Reaching special populations with breast and cervical cancer public education. J Cancer Edue. 1992;7:293-303.
5. Bastani R, Kaplan CP, Maxwell AE, Nisenbaum R, Pearce J, Mar- cus AC. Initial and repeat mammography screening in a low in- come, multi-ethnic population in Los Angeles. Cancer Epidemiol BioMarkers Prev. 1995;4:161-7.
6. Burack RC, Gimotty PA, Stengle W, Eckert D, Warbone L, Mon- crease A. Detroit's avoidable mortality project: breast cancer con- trol for inner city women. Public Health Rep. 1989; 104:527-35.
7. Burack RC, Gimotty PA, George J, Stengle W, Warbasse L, Mon- crease A. Promoting screening mammography in inner-city set- tings: a randomized controlled trial of computerized reminders as a component o~f a program to facflit;ate mammography. Med Care.
1994;6:609-24.
8. Whitman S, Ansell D, Lacey L, et al. Patterns of breast and cervi- cal cancer screening at three public health centers in an inner-city urban area. Am J Public Health. 1991;81:1651-3.
9. Centers for Disease Control. Use of mammography--United States, 1990. MMWR. 1990;3:621-30.
10. Fox SA, Stein JA. The effect of physician-patient communication on mammography utilization by different ethnic groups. Med Care. 1991;29:1065-82.
11. Publie Health Service. Clinician's Handbook of Preventive Ser- vices: Put Prevention into Practice. Washington, DC: Department of Health and Human Services; 1994.
12. Cebul RD. Randomized controlled trials using the Metro firm sys- tem. Med Care. 1992;29(suppl):9-18.
13. National Institutes of Health. Health Care Delivery Using Hospital Firms: Workshop Summary. Bethesda, Md: National Institutes of Health; 1990.
14. Goldberg HI, McGough H. Testing the implementation of clinic guidelines. IRB Rev Hum Subj Res. 199 I;13:1-7.
15. Aucott JN, Petecanos E, Dombrowski R, Fuehrer SM, Laich J, Aron DC. Implementation of local guidelines for cost-effective management of hypertension: a trial of the fLrm system. J Gen In- tern Med. 1996;11:139-46.
16. Dawson NV, Dadheech G, SperoffT, Smith RL, Schubert DSP. The effect of patient gender on the prevalence and recognition of alco-
holism on a general medicine inpatient service, d Gen Intern Med. 1992;7:38-45.
17. Goldberg HI, Mullen M, Reis PK, Psaty BM, Ruch BP. Alcohol counseling in a general medical clinic: a randomized controlled trial of strategies to improve referral and show rates. Med Care. 1991;29(suppl):46--56.
18. Meinert C. Clinical Trials: Design, Conduct, and Analysis. Oxford, England: Oxford University Press; 1986.
19. Soumeral SB, Avorn J. Principles of educational outreach ("aca- demic detailing ") to improve clinical decision-maklng. JAMA. 1990;263:549-56.
20. Curtis M. Videotapes: are they helpful in the practice setting? J Am Acad Nurse Pract. 1990;1:172-3.
21. Gagliano ME. A literature review of the efficacy of video in patient education. J Med Educ. 1988;63:785-90.
22. Maccharia WM, Lean G, Rave BH, Stephenson BJ, Haynes B. Compliance with appointment keeping for medical services. JAMA. 1983;250:1742-5.
23. Mandelblatt J, Kanetsky P. Effectiveness of interventions to en- hance physician screening for breast cancer. J Fara Pract. 1995;40:162-71.
24. Marcus AC, Crane LA, Kaplan CP, et al. Improving adherence to screening foliowup among women with abnormal Pap smears: re- sults from a large clinic-based trial of three intervention strate-
gies. Med Care. 1992;30:216-30. 25. McPhee SJ, Bird JA, Fordham D, Rodnick JE, Osborn EH. Pro-
moting cancer prevention activities by primary care physicians: results of a randomized, controlled trial. JAM/L 1991;266:538-44.
26. McPhee SJ, Detmer WM. Office-based interventions to improve de- livery of cancer prevention services by primary care physicians.
Cancer. 1993;72(suppl): 1100-12. 27. Mahloch J , Thompson B, Taylor VM, The use of qualitative meth-
ods to develop a motivational video. J Health Educ. 1998;29:84-8. 28. Armitage P, Berry G. Statistical Methods in Medical Research.
Malden, Mass: Blackwell; 1987. 29. Breslow NG, Day NE. Statistical Methods in Cancer Research, Vol
I, The Analysis of Case-Control Studies. Lyon, France: Interna- tional Agency for Research on Cancer; 1980.
30. Lantz P, Stencil D, Lippert MAT, Beversford S, Jaros L, Remington PL. Breast and cervical cancer screening in a low income managed care sample: the efficacy of physician letters and phone calls. Am J Public Health, 1995;85:834-6.
31. Thompson B, Thompson LA, Hager S, Taylor V. Costs and cost- effectiveness of a clinical intervention to increase mammography utilization in an inner city public health hospital. Presented at the American Public Health Association annual meeting, Washington, DC; 1998.
32. Mandelblatt J, Freeman H, Winczewski D, et al. The costs and ef- fects of cervical and breast cancer screening in a public hospital emergency room. Am J Public Health. 1997;87:1182-9,


















