A Characterization of Children's Intuitive Theories of Drug Action
18
This article was downloaded by: [Northeastern University] On: 26 October 2014, At: 16:04 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Applied Developmental Science Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/hads20 A Characterization of Children's Intuitive Theories of Drug Action Elizabeth P. Davies , Carol K. Sigelman , Lisa J. Bridges , Cheryl S. Rinehart & Alberto G. Sorongon Published online: 04 Jun 2010. To cite this article: Elizabeth P. Davies , Carol K. Sigelman , Lisa J. Bridges , Cheryl S. Rinehart & Alberto G. Sorongon (2004) A Characterization of Children's Intuitive Theories of Drug Action, Applied Developmental Science, 8:2, 58-74, DOI: 10.1207/s1532480xads0802_1 To link to this article: http://dx.doi.org/10.1207/s1532480xads0802_1 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions
Transcript of A Characterization of Children's Intuitive Theories of Drug Action

This article was downloaded by: [Northeastern University]On: 26 October 2014, At: 16:04Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Applied Developmental SciencePublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/hads20
A Characterization of Children's Intuitive Theories ofDrug ActionElizabeth P. Davies , Carol K. Sigelman , Lisa J. Bridges , Cheryl S. Rinehart & Alberto G.SorongonPublished online: 04 Jun 2010.
To cite this article: Elizabeth P. Davies , Carol K. Sigelman , Lisa J. Bridges , Cheryl S. Rinehart & Alberto G. Sorongon(2004) A Characterization of Children's Intuitive Theories of Drug Action, Applied Developmental Science, 8:2, 58-74, DOI:10.1207/s1532480xads0802_1
To link to this article: http://dx.doi.org/10.1207/s1532480xads0802_1
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose ofthe Content. Any opinions and views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be reliedupon and should be independently verified with primary sources of information. Taylor and Francis shallnot be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and otherliabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

A Characterization of Children’s Intuitive Theories of Drug Action
Elizabeth P. DaviesSRI International
Carol K. Sigelman, Lisa J. Bridges, and Cheryl S. RinehartThe George Washington University
Alberto G. SorongonWestat, Inc.
In an attempt to devise a methodology for characterizing children’s intuitive theoriesof drug action, 217 children in Grades 1 to 6 were interviewed about how two sub-stances, alcohol and cocaine, cause behavioral changes in their users. Measurestapped both structure (Piagetian complexity of causal reasoning, coherence, and con-struction of a causal explanatory framework with nodes, links, and causal mecha-nisms) and content (a relevant biological ontology, mastery of propositions in a scien-tifically correct theory of drug action, and reliance on alternative theoretical models).Scores on all measures increased with age, especially between first and second gradeand third and fourth grade. Growth between third/fourth and fifth/sixth grades wasmore evident for cocaine, the less familiar of the two substances. Measures of struc-ture and content were correlated. Overall, elementary school age children appear ca-pable of framing causal explanations of drug action and possess relevant biologicalknowledge, particularly about the central role of the brain in mediating the effects ofdrugs on behavior. It remains to be seen whether programs guided by an intuitive the-ories perspective and designed to increase children’s understandings of how drugsalter behavior can contribute meaningfully to drug prevention efforts.
During the last 2 decades, researchers have demon-strated that young children are capable of causal, the-ory-like reasoning in domains such as physics, psy-chology, and biology (Carey, 1985; Gopnik &Meltzoff, 1997; Gopnik & Wellman, 1994; Wellman,1990; Wellman & Gelman, 1992). Their “intuitive the-ories” define domains, describe the causal relation-ships that operate within them, and organize do-main-specific knowledge (Wellman & Gelman, 1992).Although the Piagetian perspective on cognitive devel-opment emphasizes the complexity or sophistication ofchildren’s thinking at different ages (i.e., the structureof thought), the intuitive theories perspective directsattention to the content of thought as well.
A considerable body of research has focused on es-tablishing if and when children develop intuitive theo-
ries of biology (e.g., Au & Romo, 1999; Carey, 1985;Hatano & Inagaki, 1999; Keil, 1989; Solomon &Cassimatis, 1999). This work has often been framed interms of a debate about whether children “have a the-ory” or “lack a theory” of biology. It is likely, however,that different components and qualities of intuitive the-ories emerge at different ages (Gopnik & Meltzoff,1997). Surprisingly little research has attempted tocharacterize children’s biological theories, both struc-turally and substantively.
The research presented here examines age-relateddifferences in elementary school children’s thinkingabout a topic important to drug prevention efforts: thephysiology of drug action or how drugs have their ef-fects on behavior. Much of the literature on children’sknowledge of tobacco, alcohol, and drugs has focusedon command of basic facts (e.g., Austin & Nach-Fer-guson, 1995); motivations for use (Gaines, Brooks,Maisto, Dietrich, & Shagena, 1988); effects on cogni-tion, emotion, and behavior (e.g., Dunn & Goldman,1996; H. L. Johnson & Johnson, 1995); and long-termeffects on health (Sigelman et al., 2000). Less has fo-cused on their understanding of what happens insidethe body to account for such outcomes as slurredspeech or hyperactive behavior (but see Lieberman,Clark, Krone, Orlandi, & Wynder, 1992; Meltzer,
Applied Developmental Science2004, Vol. 8, No. 2, 58–74
Copyright © 2004 byLawrence Erlbaum Associates, Inc.
58
This work was partially supported by National Institute on DrugAbuse Grant R01 DA10578 and is based largely on Elizabeth P.Davies’s doctoral dissertation. Portions were presented at the 2001biennial meeting of the Society for Research in Child Development.
We thank the students and staff of the participating schools andDiane Leach, Kathleen Dwyer, Keisha Mack, Paige Danyliw, andPhilip Wirtz for their contributions.
Requests for reprints should be sent to Elizabeth P. Davies, SRIInternational, 333 Ravenswood Avenue, BN 177, Menlo Park,CA 94025. E-mail: [email protected]
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

Bibace, & Walsh, 1984; Sigelman et al., 1999). In par-ticular, little is known about children’s understandingof the causal mechanisms involved in drug action, es-pecially the role of the brain in mediating the effects ofdrugs on behavior.
This study involved creating a methodology forcharacterizing children’s intuitive theories in this andother areas, drawing on the work of Wellman (1990)and others (e.g., Au & Romo, 1996; Novak, 1990;Sigelman, Estrada, Derenowski, & Woods, 1996;Sigelman et al., 1999). Both the Piagetian and the intu-itive theories perspectives guided the design of ourconstructs, which distinguish the structure of chil-dren’s thinking from its content. To characterize thestructure of children’s theories independent of theircontent, we relied on one approach suggested by thePiagetian literature and on two of Wellman’s criteriafor the existence of an intuitive theory, coherence andcausal explanatory framework. Wellman’s third crite-rion for a theory, ontology, pertains to content or sub-stance. The substance of children’s theories was alsocharacterized in terms of the particular theoretical ar-guments made and the extent to which they are consis-tent with a scientifically correct theory of drug action.
Structural Characterization ofIntuitive Theories
Piagetian Complexity of CausalReasoning
Reciting factual information about a phenomenon isdistinct from understanding it conceptually (Liebermanet al., 1992). The concepts of invisible physiologicalprocesses and long-term cause–effect relationships areby nature complex and abstract, and a certain level ofcognitive maturity may be required to comprehendthem. Meltzer et al. (1984), Lieberman et al. (1992), andSigelman et al. (1999) characterized the level of com-plexity of children’s causal explanations of the conse-quences of different types of drug use in terms of levelsof thinking that correspond to Piaget’s (1929)preoperational, concrete operational, and formal opera-tional stages. Each set of researchers found, in accor-dance with Piagetian theory, that older children hadmore conceptually sophisticated beliefs than youngerchildren. Younger children tended to focus on external,concrete, and observable phenomena, whereas olderchildren more often explained how the consequences ofsubstance use come about, focusing on internal,unobservable bodily processes.
A similar approach to characterizing the complex-ity of children’s theories was used in this study. Re-sponses were characterized as more complex to theextent that the child conveyed a grasp of the internalcausal mechanisms underlying the drug’s observable
behavioral effect, regardless of the scientific accuracyof the account.
Coherence
Wellman (1990) defined coherence as a state inwhich all of the concepts of a theory are related to eachother in lawful ways. Hatano and Inagaki (1994) re-ferred to coherence as the organization of one’s knowl-edge into a logical line of thought. Coherence appearsto be the least studied and hardest to operationalize ofWellman’s (1990) three criteria; many researchersomit consideration of it altogether. Indeed, Wellmanand Gelman (1992) claimed that no study had shownchildren’s biological reasoning to be coherent byWellman’s definition. This study characterizes a theoryas coherent if it does not include tangents or pieces ofinformation that do not relate to the rest of a theory andif it does not contain contradictory information aboutthe constructs within it.
Causal Explanatory Framework
A theory also must have a causal framework thatgoes beyond mere description and offers explanations,interpretations, and predictions of phenomena (Gopnik& Wellman, 1994). Despite widespread recognition ofits importance, causal explanatory framework has re-ceived little attention from an intuitive theories per-spective, often being inferred from children’s patternsof responses to structured questions rather than mea-sured directly (Gelman & Kalish, 1993). Au and Romo(1999) criticized some researchers for claiming to havedemonstrated children’s causal understanding whenchildren have shown only an understanding of in-put–output relationships, or connections betweencause and effect. They argued that simply identifyingthat one event makes another occur without explaininghow does not constitute understanding of causal mech-anism.
With respect to drug action, a causal explanatoryframework would describe how an ingested drug altersan aspect of bodily functioning (or some other media-tor of the drug’s behavioral effect) and how change inthe mediator(s) in turn causes change in behavior (e.g.,staggering). But children may demonstrate causalthinking even when their explanations are scientifi-cally incomplete or incorrect (Keil, Levin, Richman, &Gutheil, 1999). For example, a child may know that adrug somehow alters the brain before knowing that thechanged brain is the cause of changed behavior. He orshe may also know that changes in the brain cause be-havioral change before knowing the underlying bio-logical mechanism. Alternatively, a child may believethat some other internal organ is involved and be ableto describe a plausible causal mechanism involving it.
59
DRUG ACTION
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

We conceptualize the causal explanatory frame-work of an intuitive theory as a chain of events consist-ing of nodes and links that join them, followingNovak’s (1990) concept mapping approach. As Au andRomo (1999) emphasized, if children have a completeintuitive theory, they should be able to articulate a spe-cific causal mechanism through which a change oc-curs. However, evidence of causal thinking would bemissed if specifying a mechanism were the sole crite-rion (Keil et al., 1999). For example, a child who men-tions some mediator between drug ingestion and a be-havioral outcome presumably has a better grasp ofcausal relationships than does a child who only reiter-ates that taking a drug causes a behavioral effect. De-scribing a link between ingestion of a substance andthe mediator is a type of causal knowledge (e.g., thedrug gets into the bloodstream and thereby travels tothe brain). Likewise, a child may be able to link an in-termediate factor to the ultimate outcome before he orshe can articulate a specific causal mechanism con-necting the two. The study presented here measurescausal understanding such that these different elementscan be assessed independently. Both the Piagetiancomplexity of causal reasoning measure and the causalexplanatory framework measure assess the child’sability to frame a causal explanation. However, thecausal explanatory framework measure is based on adifferent theoretical perspective; does not necessarilyrequire a grasp of internal, physiological processes(e.g., the casual links and mechanisms proposed couldall operate at the cognitive and/or behavioral levels);and does not require appreciation of interactionsamong multiple causal factors as the Piagetian measuredoes. Finally, for all of the structural measures de-scribed here, the correctness of the child’s responses isirrelevant.
Substantive Characterization ofIntuitive Theories
In addition to structure, intuitive theories have con-tent, describable in terms of ontology, scientific cor-rectness, and type of theoretical argument made.
Ontology
An ontology defines the entities or things that makeup a category, and each theoretical domain has aunique ontology (Gelman, 1996). In their studies of in-tuitive biology, Hatano and Inagaki (1994) referred toontology as knowledge that enables one to specify ob-jects to which principles of biology are applicable(e.g., living things vs. artifacts). Knowledge of the on-tology of a given domain is therefore necessary for or-ganizing one’s knowledge in a theoretically relevantway. Gelman (1996) concluded that preschool-age
children have a biological ontology in that they knowthat some things are subject to biological laws,whereas other things are not. However, errors in the ap-plication of this ontology (e.g., in judgments as towhich things are biological) are seen in children wellbeyond the preschool years, suggesting that completemastery of a biological ontology may not be achieveduntil later in childhood.
For the current research, the ontology for the do-main of drug action was defined as a biological onecomprising relevant internal body parts (e.g., blood,brain). It was assumed that children must know thatthese entities are involved somehow in drug action tohold the ontology necessary for a biological intuitivetheory of drug action.
Elements of a Scientific Theory
Other than Springer (1995) and Sigelman et al.(1999), few researchers have systematically assessedthe correctness of children’s intuitive theories.Sigelman et al. (1999) assessed children’s knowledgeof drug action, following Novak (1990), by specifyingstatements or propositions that together represent afactually correct theory and then assessing the extent towhich children incorporate each proposition in theirresponses to open-ended and closed-ended questions.In this study, seven elements of a scientific theory ofdrug action were defined—for example, mention of thecorrect route taken by the drug into the body, the brainas the intermediate organ on which the drug acts, andthe fact that the effect of the drug on the brain causesthe change in behavior.
Theory Type
A final way to characterize children’s theories is todescribe the types of causal arguments they make. Pre-vious research on concepts of disease and understand-ings of drugs points to several different types of intu-itions that children may have about drug effects(Crider, 1981; Kistner et al., 1996; Lieberman et al.,1992; Meltzer et al., 1984; Sigelman et al., 1996;Sigelman et al., 1999). For example, children may ex-press a behavioral theory, relying on behavioral con-cepts and the beliefs and desires characteristic of intu-itive theories of psychology to explain drug effects(Carey, 1985; Kistner et al., 1996). Likewise, the find-ings of Sigelman et al. (1999) suggest that some chil-dren may hold a peripheral theory of drug action, em-phasizing the direct effects of a substance on the arms,legs, or other peripheral body parts involved in particu-lar behaviors without implicating the brain. Further, assuggested by the findings of Nagy (1953), childrenmay hold an undifferentiated theory, knowing that adrug enters the body and does some kind of harm butbeing unable to specify the anatomical parts or pro-
60
DAVIES ET AL.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

cesses involved. Children may also hold a vital organstheory, emphasizing vital organs that are not central toexplaining drug effects, such as the heart, liver, orlungs (particularly if they confuse smoking with otherforms of substance use). Finally, children may hold abrain theory of drug action, correctly emphasizing therole of the brain in causing behavioral effects.
In the study presented here, children’s responses tointerview questions were classified into the five theorytypes just described. It was assumed that these theorytypes can be ordered along a continuum, in which theleast sophisticated theories describe events wholly out-side the human body and the most sophisticated theo-ries identify the brain as the most causally importantorgan. Further, we allowed for the possibility that chil-dren may have intuitions representing multiple theorytypes simultaneously (Bibace, Sagain, & Dyl, 1998).
Hypotheses
We expected to find grade differences in scores onall measures used in the study. Specifically, in termsof structure, we hypothesized that children’s theorieswould demonstrate greater Piagetian complexity ofcausal reasoning, become increasingly coherent, andutilize a more elaborate causal explanatory frame-work with increasing grade. Likewise, we expectedthe content of children’s theories to become more so-phisticated and more scientifically accurate with in-creasing grade level in terms of mastery of a relevantbiological ontology and of elements of a scientifictheory. In addition, reliance on the relatively unso-phisticated behavioral, peripheral, and undifferenti-ated theory types was expected to decrease with in-creasing grade level, whereas reliance on the moresophisticated vital organ and brain theory types wasexpected to increase. Finally, based on previous workpointing to an interdependence of cognitive structureand content (e.g., Lieberman et al., 1992), we ex-pected structural measures to be moderately corre-lated with substantive ones. Theories of two drugs,cocaine and alcohol, were examined separately in aneffort to assess the generalizability of findings acrosssubstances. One substance is relatively unfamiliar andone relatively familiar; one is a stimulant and theother a depressant.
Method
Participants
Participants were 217 children in first through sixthgrade at two Catholic parochial schools in suburban ar-eas near Washington, DC. Parental consent was ob-tained for 220 children. Three children refused to par-
ticipate, yielding a sample size of 217 and a total par-ticipation rate of 59.8% (217 out of 363 targeted forparent consent packages). The two schools did not of-fer formal drug education programs at the time of datacollection.
Most demographic information was obtained fromparents’ responses to a brief questionnaire (n = 212).Not all demographic characteristics were known for allparticipants. Girls comprised 53.7% of the sample (n =116) and boys 46.3% (n = 100); 52.6% were minoritystudents (n = 112, 5.6% Asian, 39.0% Black, 5.6%Hispanic, and 2.3% other), and 47.4% were White stu-dents (n = 101). Among parents who responded to thedemographic survey, 17.1% had a high school diplomaor the equivalent, 20.3% had an associate’s degree orhad attended technical school, 14.7% had some collegeeducation, 26.3% had a college degree, and 20.3% hadreceived some graduate training or an advanced or pro-fessional degree. Educational attainment was unknownfor 1.3% of parents.
In view of the fact that grade-related trends in thedata were generally linear and to simplify analyses,participants were divided into three grade groups: firstand second graders (n = 78), third and fourth graders (n= 68), and fifth and sixth graders (n = 70 for alcohol, n= 69 for cocaine). Mean ages were 6.8 years for first-and second-grade students, 8.7 years for third- andfourth-grade students, and 10.7 years for fifth- andsixth-grade students. Students at the three grade levelsdid not differ significantly in terms of gender or parenteducation. However, ethnic makeup differed signifi-cantly across grade levels, χ2(2, N = 217) = 8.30, p <.05. The minority–White split was relatively evenamong third and fourth graders (52.9% White vs.47.1% minority), but minority students greatly out-numbered White students in the first and second grades(63.6% minority vs. 36.4% White), whereas the re-verse was true in the fifth and sixth grades (39.7% mi-nority vs. 60.3% White). Although this ethnicity andgrade confound is not desirable and required control-ling for ethnicity in analyses of grade differences, eth-nicity was generally not associated with scores on themeasures.
Procedure
Four research assistants gave a brief overview of theresearch in each participating classroom (13 in all).Each child was given a parent consent packet to takehome and return with a parent’s consent or decline. Thepacket included a letter explaining the project (with anendorsement by the school principal), a brief parentsurvey containing demographic items, and a consentform granting permission for the child to be inter-viewed.
After providing a signed parent consent form, eachstudent met individually with a trained interviewer,
61
DRUG ACTION
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

who described the study and answered any questions,emphasizing that responses would be kept confidentialand that students could choose not to answer any ques-tion. Students who then agreed to participate signed achild assent form. Individual interviews were con-ducted at the child’s school, either during school hoursor during the child’s after-school care program. Fivetrained research assistants conducted the interviews.All were female; four were White, and one was AfricanAmerican.
The interviews, conducted in two sessions, con-tained open-ended questions followed by structuredones. The same questions were asked about alcoholand cocaine. Order of presentation was counterbal-anced, so that approximately half of the sample re-ceived questions about alcohol first (51.2%), and ap-proximately half received questions about cocaine first(48.8%). During the first session, students received allof the open-ended questions about both drugs, the sub-ject of this analysis. Interviewers took notes on chil-dren’s responses and audio-taped them so that theycould later be transcribed.
Questions Eliciting IntuitiveTheories of Drug Action
Responses to two open-ended items with standardprobes, each asked about both drugs, were used to cre-ate measures of each of the constructs of interest in thisarticle. The first item was used to identify each child’snotion of a specific behavioral effect of drug usage.Children were asked, “Well, let’s pretend that a teen-ager just drank lots of beer [took lots of cocaine orcrack]. What do you think drinking lots of beer [takinglots of cocaine or crack] will do to him?” Interviewersused probes to encourage children to exhaust theirideas regarding possible effects and to clarify vague re-sponses and listened for references to behavioral ef-fects (effects classified as cognitive, motoric, affective,or pathological).
The purpose of the second question was to exposechildren’s intuitive theories of drug action by inducingchildren to describe a chain of events beginning withingestion and ending in the specific behavioral effect.The first behavioral effect mentioned by the child wasused as the specific behavioral effect of focus. If a childhad not mentioned a behavioral effect, the default ef-fect “have trouble paying attention” was used to askthis question: “Okay, you just told me that drinking lotsof alcohol [taking cocaine or crack] will make thisteenager [experience first behavioral effect mentioned /have trouble paying attention]. Well, how exactly willdrinking lots of beer [taking cocaine or crack via what-ever method of ingestion the child identified in a previ-ous question] make this teenager [experience specificbehavioral effect mentioned]?” Interviewers used sev-eral standard probes to exhaust children’s intuitions
and to fill in gaps in children’s causal descriptions,identify any causal mediators, and clarify the orderingof events mentioned.
If a child failed to mention any bodily events, inter-viewers used the probe, “Does anything happen insidethe teenager’s body to make him or her [experiencespecific behavioral effect mentioned]?” Children whoanswered yes were asked to elaborate, and childrenwho answered no were asked, “What does happen?”When children responded vaguely, interviewers drewout more information with probes such as, “Can youtell me more about what you mean by that?” “Whichhappens first?” “How does that work?” or “How does[first event] make [second event] happen?” As the goalof the question was to identify a complete causal chainbeginning with ingestion and ending with behavior, in-terviewers also asked, “How does drinking the alcohol[taking the cocaine] make [event] happen?” and “Howdoes [event] make [specific behavioral effect] hap-pen?” Interviewers cycled through these probes untilthe chain was complete or the child’s ideas were ex-hausted.
From these two unstructured items, coding systemswere developed to measure the six constructs of inter-est. The constructs (Piagetian complexity of causalreasoning, coherence, causal explanatory framework,relevant biological ontology, elements of a scientifictheory, and theory type) were the basis for characteriz-ing the structure and content of children’s intuitive the-ories of the effects of alcohol and cocaine.
Measures of Theory Structure
Piagetian complexity of causal reasoning. Thelevel of sophistication of the child’s causal reasoning,independent of its scientific accuracy, was measuredon a 0 to 7 scale, adapted from the work of Meltzer etal. (1984). Table 1 outlines the scoring system and in-cludes examples from actual interviews. Higher scoresindicate a sophisticated grasp of the internal causalmechanisms behind the drug’s observable behavioraleffect. Sophisticated responses include statements at-tributing the change in behavior to the drug’s action onat least one internal organ and elaborate descriptions ofcausal mechanisms linking ingestion of the drug, thedrug’s action on the internal organ(s), and the resultantbehavioral effect.
Coherence. The coherence of children’s theories,or the extent to which their theories contain interrelatedconcepts, was assessed through two dichotomous vari-ables. The first assessed the consistency of the child’sstatements as evidenced by an absence of self-contra-dictions (e.g., his brain slows down and he gets real hy-per), reversing and changing the type of organ damagedone (e.g., “the heart beats slow” is later inexplicablychanged to “the heart beats fast”), or switching drugs
62
DAVIES ET AL.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

discussed in mid-interview. The second assessed uni-formity of thought, the extent to which the ideas in thechild’s explanation contribute to a single line of reason-ing. Explanations that lack uniformity of thought in-clude many tangents and pieces of information that arenot tied into the explanation. Each variable was scored 0(no credit) or 1 (credit); the two scores were summed toform a coherence score with a range of 0 to 2.
Causal explanatory framework. Five variablesmeasured the extent to which a student’s theory in-cluded the “links” and “nodes” required to construct acausal explanatory framework:
1. An intermediate factor or mediator between drugingestion and the behavioral effect (i.e., a node inthe causal chain, such as the brain; e.g., “It proba-bly will go up to the brain and mess it up.”).
2. A route of the drug to at least one intermediatefactor (the first link in the causal chain; e.g.,“Like when he’s, when he’s drinking it, it haspipes, like pipes in his, in his throat. And it goesdown, it can make his heart hurt.”).
3. A mechanism by which the drug affects an in-termediate factor or a behavior (e.g., “Thechemicals that are in the beer will make him hitpeople.”).
4. A change, caused by the drug, in an intermedi-ate factor (e.g., “It destroys the brain cells.”).
5. A mechanism linking an intermediate factor toa behavioral effect (e.g., “If he takes cocaine, itwill mess up his brain, so that the brain won’tbe able to tell the other parts to move right.”).
These variables were scored such that studentscould receive no credit (0 points), credit for offering a
vague description (1 point), or credit for offering anelaborate description (2 points). For example, a vaguedescription of the brain as an intermediate factor mightbe “the drug goes to the head where the brain is”whereas an elaborate description might be “it goes tothe part of the brain that controls how you talk.” Vari-ables were scored regardless of scientific accuracy.Scores on the five 0 to 2-point variables were added toform an index ranging from 0 to 10.
Measures of Theory Content
Relevant biological ontology. Children received1 point for each of five relevant anatomical parts thatthey mentioned, yielding a possible score of 0 to 5. Foralcohol, the five relevant body parts were the mouth,throat, stomach, blood, andbrain; for cocaine, theywerethe nose, throat, lungs, blood, and brain. These bodyparts were selected based on the rationale that alcoholcomes in a beverage that people drink and that cocainemay be ingested either by sniffing or by smoking. Thecontexts in which these body parts were mentioned didnot need to be scientifically correct for children to re-ceive credit.
Elements of a scientific theory. Using an ap-proach similar to that used by Sigelman et al. (1999), weassessed the extent to which children’s theories were ac-curate by scoring a 1 (presence) or 0 (absence) in theiranswers of seven propositions that are part of a scientifi-cally correct theory of drug action. Items were summedto form a score with a range of 0 to 7. To achieve a scoreof 7, a child had to mention the following:
63
DRUG ACTION
Table 1. Description of Codes for Piagetian Complexity of Causal Reasoning Scale
Code Responses Reflecting Level of Child’s Causal Reasoning
0 No response, don’t know, circular logic or mere repetition of the behavioral effect.1 Behavioral effects attributed to non-specific body effects (e.g., “alcohol wrecks your body,” “it hurts inside his body”).2 Behavioral effects attributed to changes in body exterior (e.g., “his arms would hurt”) or general somatic effects (e.g., headache,
stomachache), with no reference to internal physiological processes.3 Internal organs (e.g., heart, lungs, stomach, brain) mentioned, but not used to explain change in behavior.4 Drug is said to have behavioral effects through effects on internal organ(s) (e.g., “The beer messes up the brain and if his brain is
messed up, that messes up the way he learned how to drive”), but no articulation of specific damage/change to the organ or of themechanism through which damage/change to the organ results in behavior change.
5 Elaborate description of internal organ damage/change (e.g., “alcohol makes the brain tired”) but only vague link between change inorgan and behavioral effect or elaborate description of how the drug’s effect on the internal organ causes the behavioral effect (e.g.,“[alcohol] goes up to your brain and makes him very dizzy … the brain waves send the wrong messages to his legs so he walksawkwardly”) but only vague description of damage to the internal organ.
6 Both an elaborate description of the internal organ damage/change and an elaborate description of how the drug’s effect on theinternal organ causes the behavioral effect (e.g., “alcohol might go up to the brain and start eating it up and making it rot. It eatsaway important parts and those important parts help you act normal and not go out of control. And that’s when you start acting notnormal …”).
7 Provided more specific details regarding pathway of the drug, elaborated on the physiological effects of using the drug, and integratedthe physiological changes with the behavioral or psychological ones. Explanations demonstrate understanding that the body is aninterdependent system.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

1. The correct method of entry of the substanceinto the body (drinking for alcohol, sniffing orsmoking for cocaine).
2. The throat or stomach as a route taken by alco-hol or the throat, nose, or lungs as a route takenby cocaine.
3. The bloodstream as the means of passage of thedrug.
4. The brain as an intermediate organ on whichthe drug acts.
5. A correct effect on the brain (alcohol slows, co-caine speeds the brain).
6. The concept that the drug affects a specific partof the brain involved in the specific behavior.
7. The concept that the change in the brain is whatcauses the change in behavior.
Theory type. Finally, children’s responses werescored for the presence or absence of five types of theo-ries. A behavioral theory type is indicated by state-ments about behavioral (“If he drinks a lot of wine, Ithink he’s going to kill people.”), social (“His mom anddad will get angry at him.”), or psychological events(“He would go crazy.”) resulting from drug use. It isalso indicated by statements about perception (“Hewon’t be able to see straight.”) and cognition (“Hewon’t know how to do his ABCs.”), including use ofone psychological effect to explain another. A periph-eral theory type included statements about peripheralbody parts, including the arms, legs, toes, and fingers.Responses that demonstrated a vague idea that drug in-gestion does something to, or affects something inside,the body, including references to making the personsick or causing common physical symptoms, werecoded as reflecting an undifferentiated theory type(e.g., “It gets inside his body and messes it up.”). A vi-tal organ theory included statements about an organother than the brain (e.g., heart, lungs, liver, intestines,stomach, or blood; e.g., “His lungs start getting black… they’re like black, brown something.”). Finally, abrain theory was coded when the explanation referredto the brain or parts (real or fictional) of the brain.
For each theory type, two dichotomous variableswere created. The first distinguished whether the childreferred to any concepts represented by the theorytype, and the second distinguished whether the childused concepts from the theory type as mediators of abehavioral effect. For example, a child who said “Thealcohol messes up his brain” would receive credit formentioning a brain theory concept. If the child said“When his brain is messed up, he can’t think clearly, sohe gets a bad grade,” credit for a brain theory mediatorwould also be given.
Interrater reliability. Fifty-two (24%) of the in-terviews were independently coded by two trained rat-
ers. Interrater reliability was then estimated by com-puting kappa coefficients, which correct for chanceagreement. The average kappa was .66 for the two co-herence items, .72 for the causal explanatory frame-work variables, .92 for the relevant biological ontologyvariables, .74 for the scientific correctness items, and.78 for the theory type variables.
To generate the 8-point ordinal scale tappingPiagetian complexity of causal reasoning, all inter-views were independently scored by two coders,scores were then compared, and discrepancies wereresolved through discussion before final scores wereassigned. Percentages of exact agreement betweenthe two raters’ independent codings were 67.3% foralcohol and 63.6% for cocaine. Correlations betweenscores assigned by the two coders were .84 for alco-hol and .80 for cocaine, suggesting that even thoughraters did not always agree precisely, they often per-ceived similar levels of complexity.
Results
Grade Group Differences
Table 2 presents means by grade group for Piagetiancomplexity of causal reasoning, coherence, causal ex-planatory framework, relevant biological ontology, el-ements of a scientific theory, and theory type. Gradegroup differences were analyzed through a multiple re-gression analysis for each dependent variable. Becauseof the significant associations between ethnicity andgrade reported earlier, all analyses included ethnicity(White vs. minority) as a control variable. Two dummycodes were used to represent grade group. One dummycode represented the difference of first and secondgraders versus third and fourth graders, whereas thesecond represented the difference of the fifth and sixthgraders versus third and fourth graders.
Piagetian Complexity of CausalReasoning
The overall model for Piagetian complexity ofcausal reasoning was significant for both alcohol, R2 =.10, F(3, 207) = 7.46, p < .0001, and cocaine, R2 = .09,F(3, 207) = 7.18, p < .001. Controlling for ethnicity,third and fourth graders’ causal reasoning was signifi-cantly more complex than that of first and second grad-ers for both alcohol, β = –.22, t(209) = –2.81, p < .01,and cocaine, β = –.21, t(209) = –2.74, p < .01. Fifth andsixth graders did not differ significantly from third andfourth graders for either substance, although the trendfor alcohol was nearly significant (p < .07). (Inspectionof grade-by-grade means revealed that third gradersscored more like younger children and fourth gradersmore like older children; according to Duncan’s multi-
64
DAVIES ET AL.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

65
Table 2. Means and Standard Deviations for Intuitive Theory Measures
Alcohol (by Grade) Cocaine
1st and 2nda 3rd and 4thb 5th and 6thc 1st and 2nda 3rd and 4thb 5th and 6thc
M SD M SD M SD M SD M SD M SD
Piagetian complexity (max. 7) 2.83 1.33 3.48 1.49 3.94 1.30 3.00 1.32 3.62 1.38 4.06 1.30Coherence (max. 2) 1.47 .68 1.66 .54 1.69 .58 1.38 .74 1.62 .57 1.62 .60Causal explanatory framework (max. 10) 3.32 1.90 4.43 2.42 4.89 1.99 3.65 1.84 4.46 2.12 5.04 2.27Relevant biological ontology (max. 5) .78 .83 1.07 1.01 1.11 .94 .72 .80 1.25 .97 1.43 .93Elements of a scientific theory (max. 7) 1.35 .94 2.12 1.62 2.59 1.68 .83 1.10 2.00 1.48 2.67 1.45Theory type (max. 1)Behavioral .78 .42 .68 .47 .71 .46 .66 .48 .59 .50 .67 .47Undifferentiated .37 .49 .41 .50 .39 .49 .32 .47 .29 .46 .22 .42Vital organ .40 .49 .43 .50 .41 .50 .36 .48 .47 .50 .43 .50Brain .32 .47 .60 .49 .71 .46 .34 .48 .62 .49 .83 .38
Note: Because theory type variables are dichotomous (coded 0 and 1), each mean represents the proportion of children expressing the theory type. max. = maximum.an = 78. bn = 68. cn = 70.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

ple range tests (Ott, 1993), Grades 1, 2, and 3 differedsignificantly from Grades 4, 5, and 6 on both mea-sures.)
Coherence
Mean coherence scores did not increase signifi-cantly with grade level for alcohol, R2 = .03, F(3, 208)= 1.97, ns, but did for cocaine, R2 = .05, F(3, 208) =3.70, p < .05. First- and second-grade students hadlower coherence scores than the two older gradegroups, which had identical means. Controlling forethnicity, the difference between first and second grad-ers and third and fourth graders was significant, β =–.16, t(210) = –2.05, p < .05.
Causal Explanatory Framework
Regression models predicting causal explanatoryframework scores were significant for both alcohol, R2
= .09, F(3, 208) = 6.81, p < .001, and cocaine, R2 = .07,F(3, 208) = 4.89, p < .01. As predicted, first- and sec-ond-grade students scored significantly lower thanthird- and fourth-grade students for both alcohol, β =–.25, t(210) = – 3.19, p < .01, and cocaine, β = –.18,t(210) = –2.25, p < .05. The scores of fifth and sixthgraders were not significantly higher than those ofthird and fourth graders.
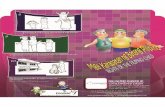
To illustrate the nature of grade differences incausal arguments, Figure 1 presents the percentagesof students in first and second grades and fifth and
sixth grades who received credit for mentioning eachof the five constructs used to create the causal explan-atory framework composite scores in their responsesabout alcohol. As can be seen initially, a majority ofstudents in both grade groups mentioned an interme-diate factor. Second, fewer than half of the students ineach grade group described a route between ingestionand an intermediate factor, although there was a sub-stantial increase in describing this link from theyoungest grade group to the oldest. Third, only asmall minority of students at either grade level de-scribed a mechanism by which alcohol changes themediator. Fourth, whereas only 39.7% of the youn-gest grade group attributed behavioral effects tochanges in an intermediate factor, 70% of the fifthand sixth graders did so. Finally, approximately threetimes as many fifth and sixth graders as first and sec-ond graders explained how changes in an intermedi-ate factor caused behavioral changes (34.3% vs.10.3%). Thus, although there were at least modest in-creases in all components of the causal explanatoryframework composite with age, grade-related in-creases in elaborated links between intermediate fac-tors and behavioral outcomes were especially evident.Children’s responses regarding cocaine yielded a verysimilar pattern of results.
For example, this first-grade student identifies anintermediate factor (the lungs), but she does not dis-cuss a route or tie a change in the intermediate factor toa change in behavior (I = interviewer; S = student):
66
DAVIES ET AL.
Figure 1. Percentages of first and second graders and fifth and sixth graders who provided causal linkages in their theories of alcoholaction.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

I: Well, how exactly will drinking lots of beermake the teenager act crazy?
S: Because it has alcohol in it.I: Does anything happen inside the teenager’s
body to make him or her act crazy?S: It won’t be healthy.I: Can you tell me more about that? Why won’t it
be healthy?S: Because the lungs.I: What about the lungs?S: The lungs wouldn’t feel, wouldn’t be very
good.I: And how would the lungs not being very good,
how would that make the teenager act crazy?S: Because of the alcohol.
In contrast, consider the explanation offered by thissixth-grade student:
I: How exactly will drinking lots of beer makethis teenager not be able to walk?
S: ’Cause when you can’t really see straight,you’ll be blurry and he won’t be able to seeyou and he’ll probably walk into something.
I: How does drinking lots of alcohol make thisteenager not be able to see straight?
S: It probably messes up his eyesight.I: And how does that work?S: It, like, it messes up his brain, another part of
the brain that makes the eyesight.I: And can you tell me just a little bit more about
what you mean by messes up part of the brain?S: Well, … it just messes up, like hurts it or
something. It makes it not work right. It affectspart of the brain somehow. That, like, the partsof the brain that make eyesight work and howto walk.
This sixth-grade student identifies the brain as an in-termediate factor and as a causal mediator in chang-ing behavior (i.e., in rendering someone unable towalk). Like most of his peers, however, he does notarticulate a specific mechanism responsible for achange in the brain; he knows only that alcoholsomehow damages the brain and that, in turn, itcauses a change in behavior.
Relevant Biological Ontology
The regression analysis testing for grade-level dif-ferences in relevant biological ontology scores was notsignificant for alcohol, F(3, 208) = 2.09, ns, but wassignificant for cocaine, R2 = .10, F(3, 208) = 7.72, p <.0001. As expected, first- and second-grade studentshad significantly lower scores on the ontology measurethan did third- and fourth-grade students, β = –.27,
t(210) = –3.45, p < .001. Contrary to expectations,third- and fourth-grade students did not differ signifi-cantly from fifth- and sixth-grade students, β = .08,t(210) = 1.06, ns.
Elements of a Scientific Theory
Regressions examining grade group differences andcontrolling for ethnicity in mentions of correct ele-ments of a scientific theory of drug action were signifi-cant for both alcohol, R2 = .11, F(3, 208) = 8.69, p <.0001, and cocaine, R2 = .24, F(3, 208) = 22.12, p <.0001. For alcohol, first and second graders mentionedsignificantly fewer elements than did third and fourthgraders, β = –.26, t(210) = –3.43, p < .001, whereas thedifference between the two older grade groups was notsignificant. For cocaine, first and second graders againmentioned fewer elements of a scientific theory thandid third and fourth graders, β = –.37, t(210) = –5.17, p< .0001; moreover, fifth and sixth graders mentionedsignificantly more elements than did the third andfourth graders, β = .19, t(210) = 2.66, p < .01.
Table 3 presents the percentages of students in eachgrade group who mentioned each of the elements of ascientific theory for alcohol and for cocaine. Grade-re-lated increases were evident for most of these vari-ables. However, the most striking grade differencesacross the two substances were in mentions that thesubstance acts on the brain, that it affects a specific partof the brain, and that changes in the brain are whatcause changes in behavior.
Theory Type
A large majority of students mentioned at least oneconcept from at least one of the hypothesized theorytypes (94.9% for alcohol, 95.3% for cocaine). As canbe seen in Table 2, mentions of concepts representingbehavioral theories and brain theories were most com-mon; some undifferentiated thinking and references tovital organ concepts were also evident at all grade lev-els. Peripheral thinking was rare, even among youngchildren; as a result, no analyses were conducted withthis variable.
Because the theory type variables were dichoto-mous, logistic regression analyses were conducted. Sig-nificant grade group differences were evident only forthe brain theory type, χ2(3, N = 213) = 25.93, p < .0001,for alcohol, and χ2(3, N = 211) = 36.44, p < .0001, for co-caine. Compared to third and fourth graders, first andsecond graders were less likely to mention the brain indiscussing alcohol effects, β = –.32, χ2(1, N = 213) =11.85, p < .001, whereas the two older grade groups didnot differ significantly. For cocaine, third and fourthgraders were more likely than first and second graders tomention the brain, β = –.29, χ2(1, N = 211) = 10.11, p <.01, but were less likely than fifth and sixth graders to doso, β = .26, χ2(1, N = 211) = 6.11, p < .05.
67
DRUG ACTION
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

68
Table 3. Percentage of Students by Grade Group Receiving Credit for Individual Items in the Elements of a Scientific Theory Scale for Alcohol and Cocaine
Alcohol (by Grade) Cocaine (by Grade)
1st and 2nda 3rd and 4thb 5th and 6thc 1st and 2nda 3rd and 4thb 5th and 6thc
Correct method of ingestion 57.7 51.5 61.4 12.8 44.1 42.0Correct route through body 24.4 16.2 15.7 12.8 23.5 20.3Blood is carrier of drug 3.8 20.6 15.7 2.6 14.7 17.4Drug acts on brain 30.8 60.3 71.4 30.8 58.8 84.1Correct drug effect 1.3 5.9 14.3 0.0 1.5 0.0Drug affects specific part of brain 3.8 14.7 20.0 5.1 13.2 30.4Changed brain causes behavior change 12.8 42.6 60.0 19.2 44.1 72.5
an = 78. bn = 68. cn = 70.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

Only a minority of children used any given theorytype concept as a mediator of behavioral effects. Foralcohol, behavioral mediators were used in the expla-nations of 5.1% of first and second graders, 11.8% ofthird and fourth graders, and 18.6% of fifth and sixthgraders, a nonsignificant grade difference. For bothsubstances, grade group differences in the percentageof children who referred to the brain as a mediator ofbehavioral effects were significant. For alcohol, 5.1%of first and second graders, 26.5% of third and fourthgraders, and 30.0% of fifth and sixth graders por-trayed the brain as a mediator. The difference be-tween first and second graders and third and fourthgraders was significant, β = –.52, χ2(1, N = 213) =11.26, p < .001, whereas the difference between thetwo higher grade groups was not. For cocaine, 11.7%of first and second graders, 30.9% of third and fourthgraders, and 42.0% of fifth and sixth graders de-scribed the brain as a mediator. As for alcohol, onlythe difference between the first and second gradersand the third and fourth graders was significant, β =–.32, χ2(1, N = 211) = 7.28, p < .01.
Relationships Among IntuitiveTheories Measures
Table 4 presents partial correlations between intu-itive theory measures that control for grade and ethnic-ity. Two measures tapping structure (Piagetian com-plexity of causal reasoning and causal explanatoryframework) and four of the content measures (relevantbiological ontology, elements of a scientific theory, vi-tal organ theory type mention, and brain theory typemention) were all significantly intercorrelated for bothalcohol and cocaine. By contrast, coherence and the re-maining two theory type variables—behavioral theorytype mention and undifferentiated theory type men-tion—were generally unrelated to other measures.
Discussion
The aim of this study was to develop and apply amethodology for characterizing children’s intuitivetheories of drug action in terms of both structure andcontent in the hope that the approach could be adaptedto the study of other intuitive theories as well. Studentswere asked to express, for both alcohol and cocaine,their intuitions about the chain of causal events be-tween ingestion of a drug and a specific change in be-havior caused by the drug’s use. Mastery of the quali-ties assessed by our measures generally increased withincreasing grade level, with differences between firstand second graders and third and fourth graders partic-ularly evident (although on the Piagetian complexity ofreasoning measure in particular, third graders per-formed like younger children and fourth graders like
older children). Significant differences between thirdand fourth and fifth and sixth graders were less com-mon and were more evident for cocaine than for alco-hol, probably because cocaine is the less familiar of thetwo substances. The brain proved to be prominent inchildren’s theorizing, increasingly so with age.
Structure
Consistent with the work of Meltzer et al. (1984),Lieberman et al. (1992), and Sigelman et al. (1999), thecomplexity, from a Piagetian perspective, of children’sreasoning about the causal mechanisms behind the ob-servable effects of substance use increased with age,such that by about age 9 (fourth grade) most childrengrasp the concept of internal, physiological causation.It may take until adolescence for children to think insystems terms about interacting causal factors withinthe body.
Whereas students’ explanations concerning alco-hol did not become more coherent with age, third-and fourth-grade students gave significantly more co-herent explanations of cocaine’s effects than did first-and second-grade students. The latter finding is con-sistent with Siegler and Thompson’s (1998) findingof age differences in the ability to make coherent pre-dictions about economic concepts. As noted by others(e.g., Gopnik & Wellman, 1994), however, measuringcoherence is problematic. The two-item measure usedhere may not have been sufficiently sensitive and reli-able to capture variations in the coherence of chil-dren’s thinking.
As recommended by Keil et al. (1999), this studyalso included a multifaceted causal explanatory frame-work measure, thereby allowing for the possibility thatstudents would demonstrate some elements of a com-plete causal explanation but not others. For both drugs,third and fourth graders were more successful thanyounger children at describing an intermediate factorbetween ingestion and a behavioral outcome, a routetaken by the drug to the intermediate factor, and acausal link tying a change in the intermediate factor ormediator to a change in behavior. By middle elemen-tary school, then, most students appear to recognizethat drug action entails more than a simple input–out-put relationship between ingestion and behavioralchange. They hypothesize that some intermediate fac-tor, usually the brain, connects the two, and their rea-soning then becomes more elaborate as grade level in-creases.
These findings are consistent with research indicat-ing that knowledge of differentiated body parts and in-tegrated physiological systems increases with age(Carey, 1985; Crider, 1981). Providing an elaborate de-scription of an intermediate factor suggests that a childknows that the interior body has different parts and candiscuss specific characteristics of one of these parts.
69
DRUG ACTION
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

70
Table 4. Significant Correlations Among Intuitive Theory Measures, Controlling for Ethnicity and Grade
Intuitive Theory Measures 1 2 3 4 5 6 7 8 9
1. Coherence — .18** –.21**2. Piagetian Complexity of Causal Reasoning .26*** — .73**** .43**** .55**** .24*** .50****3. Causal Explanatory Framework .16* .68**** — .55**** .63**** .31**** .43****4. Relevant Biological Ontology .47**** .52**** — .71**** .51**** .56****5. Elements of a Scientific Theory .59**** .62**** .71**** — –.17* .26*** .66****6. Behavioral Theory Type —7. Undifferentiated Theory Type .15* — .19**8. Vital Organ Theory Type .31**** .34**** .36**** .23*** —9. Brain Theory Type .53**** .44**** .60**** .69**** —
Note. Correlations among alcohol measures are below the diagonal; correlations among cocaine measures are above the diagonal.*p < .05. **p < .01. ***p < .001. ****p < .0001.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

Likewise, elaborating on a route taken by a drug im-plies knowledge that various body parts are somehowjoined or integrated. For example, one sixth-grade stu-dent appeared to understand that distinct body parts in-teract to cause behavioral change and could envision a“route” linking them:
I: How exactly will taking cocaine make theteenager hallucinate?
S: I think it gets into …it damages some of thebrain cells and that’s how you hallucinate.Sometimes it destroys the brain, some of thebrain cells, which triggers some of yoursenses, and you hallucinate.
I: Do you know how it gets in the brain cells?S: Because there’s a passage from your nose to
your brain so you can smell. That’s how thesense works … it triggers something to thebrain, so you know what you’re smelling.
However, only a minority of students, even in fifthand sixth grades, offered descriptions of a mechanismby which a substance causes change in an intermediatefactor. Although older children were more able thanyounger ones to posit a causal mechanism to explainthe effect of a damaged or changed intermediate factoron a behavior, most were nonetheless unable to do so.Thus understanding of causal mechanism may be oneof the last features to emerge in children’s intuitive the-ories of drug action. As suggested by Keil et al. (1999),children may understand general causal patterns beforethey fill in domain-specific details (in this case, aboutproperties of drugs that alter the brain’s functioningand about relationships between brain and behavior).The findings are also consistent with Springer,Ngyuen, and Samaniego’s (1996) finding that most 4-to 6-year-old children cannot express that rotting foodmakes people sick through the mechanism of decom-position, and with Au and Romo’s (1999) conclusionthat most fourth- through eighth-grade students fail tounderstand HIV as a living virus that reproduces insidethe human body and thereby acts as a biological causalmechanism.
This study might have led to a similar conclu-sion—that children lack the ability to construct acausal theory of drug action—had understanding ofcausal mechanism been the only aspect of causalthinking measured. Instead, our methodology allowedus to determine that many children, well before theycommand thought of the sort Piaget characterized asformal–operational or have knowledge of specificcausal mechanisms involved in drug action, can con-struct a logical, causal argument about how taking adrug might alter behavior. They do so by hypothesiz-ing a mediator and linking the drug to the mediatorand the mediator, in turn, to the behavioral change tobe explained. Overall, examination of the “links,”
“nodes,” and causal mechanisms within an intuitivetheorist’s causal explanatory framework reveals dif-ferent types of causal argumentation in children ofdifferent ages, independent of their factual knowl-edge. This approach also points to progress with agein moving beyond merely describing cause–effectlinks to explaining them. It remains to be seen, how-ever, what a “mature” theory of drug action lookslike; as Rosenblit and Keil (2002) observed, adults’explanations of phenomena are less coherent andcausally explicit than they believe.
Content
The findings reinforce Gelman’s (1996) positionthat, although young children may understand that avocabulary or ontology relevant to a domain exists,they do not necessarily know all that it includes.Knowledge of a relevant biological ontology for ex-plaining drug action increased with grade level for co-caine but not for alcohol. Mention of the brain in-creased significantly with grade level for both drugs,and mention of the blood also increased for cocaine.Overall, children mentioned few relevant body partsfor either substance. Awareness of the critical role ofthe brain is probably more important for developing anintuitive theory of drug action than having a completerelevant biological ontology. Intuitive theories re-searchers have repeatedly asserted that some types ofknowledge are more theoretically significant than oth-ers (Gopnik & Wellman, 1994) and that knowledge ofonly a few domain-specific premises can be sufficientto support an intuitive theory (Springer, 1995). Thesefindings suggest that children make a major theoreticalbreakthrough when they grasp that the brain is impli-cated when drugs change behavior.
Knowledge of elements of a correct scientific ex-planation of drug action was also more advancedamong older elementary school students than amongyounger students, consistent with other health re-search findings (Kistner et al., 1996; Lieberman et al.,1992; Sigelman et al., 1999). By third and fourthgrade, most children understand that drugs alter thebrain, and by fifth and sixth grade most understandthat changes in the brain cause changes in behavior indrug users. Finally, as in Sigelman et al. (1999),knowledge that alcohol depresses the brain increasedwith grade level. However, few children even in thefifth and sixth grades mentioned this, and many chil-dren had misconceptions about the specific physio-logical effects of drugs on the brain and of the brainon behavior. Very few, for example, understand thatcertain drugs are central nervous system stimulantsrather than depressants. Future studies should furtherspecify these misconceptions so that they can be ad-dressed in drug education programs.
71
DRUG ACTION
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

Finally, we assessed the inclusion in children’sthinking of concepts relevant to five classes of theoriesabout drug action. Contrary to predictions, the onlysignificant findings were grade-related increases in re-liance on the brain theory type. That older studentswere more likely than younger students to recognizethe relevance of the brain to drug action and to discussit as a causal mediator, parallels findings from othermeasures discussed earlier, as well as from previousstudies of children’s knowledge of the brain (C. N.Johnson & Wellman, 1982; Sigelman et al., 1999) andthe development of causal reasoning (Keil et al., 1999).
Siegler and Jenkins (1989) reported that childrencontinue to use lower level mathematical strategies asthey master more advanced ones, and Bibace et al.(1998) found that children hold different theories ofdisease simultaneously. Similarly, students in the cur-rent study continued to discuss less relevant conceptsof drug action, especially behavioral effects of druguse, even after identifying the brain as the most impor-tant concept. However, few children hypothesized thatthe behavioral effects of drugs are mediated entirely byother behaviors, cognitions, or emotions, thereforeproviding no support for Carey’s (1985) argument,since revised, that children younger than approxi-mately age 10 hold psychological rather than biologi-cal theories of biological phenomena.
The tendency to view the body in an undifferenti-ated way was relatively common, but it did not de-crease with age as hypothesized. In addition, older stu-dents were no more likely than younger ones to includevital organs such as the lungs in their explanations.Finally, few students at any grade level relied on the pe-ripheral theory type, arguing that drugs act directly onthe arms or legs to change behavior (but see Sigelmanet al., 1999).
Finally, the correlational findings shed light on therelationship between form and content in children’stheories. Setting aside limitations in the measure of co-herence and possibly in the measures of reliance on theleast mature theory types, structure (complexity ofcausal argumentation assessed in two conceptually dis-tinct but empirically correlated ways), and content (thefactual correctness of beliefs) appear to be moderatelycorrelated, even with grade and ethnicity controlled, afinding consistent with those of Lieberman et al.(1992) and Sigelman et al. (1999). Although somechildren construct tight causal arguments that are milesfrom the truth, and although others have many of theirfacts straight but cannot assemble them in a causal ar-gument, structural complexity and factual correctnessgenerally go hand-in-hand empirically. It is not yetclear whether the capacity to think complexly aboutcausal matters enables children to collect and under-stand relevant facts, whether the possession of relevantfacts enables children to construct more complex theo-ries, or both.
Methodological Shortcomings andStudy Limits
Because this research represents an exploratory at-tempt to characterize children’s intuitive theories ofdrug action, its measures were not all optimally sensi-tive and reliable, and they need validation. Moreover,as a cross-sectional study, the research presented herecannot claim to have uncovered true developmentalchanges. Finally, like several other studies of chil-dren’s beliefs about health issues (Lieberman et al.,1992; Meltzer et al., 1984), this study relied onopen-ended questioning to characterize children’sthinking. Although it provides rich qualitative data,this approach tends to disadvantage younger and lessverbal children (Kistner et al., 1996; Wellman &Gelman, 1992) and probably does not fully capture thesophistication of children’s intuitive understandings.
Future research should employ multiple method-ological approaches, both closed ended and openended, in studying the development of children’s theo-ries. Such research might begin with preschool-agechildren to determine when a brain-centered theory ofdrug action originates and what alternative theoriesyoung children may hold. Children might be asked toexplain in their own words particular effects of sub-stance use on behavior and then to respond to either–orquestions asking which of two alternative explanationsof an effect of substance use (e.g., central or peripheral,brain-centered or lung-centered) is most accurate. Ulti-mately, one might want to track understandings of drugeffects, attitudes toward drug use, and drug use behav-ior longitudinally every other year or so into the ado-lescent years in order to understand the evolution of re-lationships among knowledge, attitudes, and behavior.
Theoretical and PracticalContributions
This study offers a set of approaches for character-izing intuitive theories in the domain of drug actionthat can be applied to other domains of knowledge aswell. The common conceptualization of an intuitivetheory as a binary construct—as something childreneither have or do not have—appears to be insufficient,given the differential performance of the children westudied on different measures of qualities of intuitivethought. We believe too that it is useful to distinguishbetween setting forth a coherent and complex causalargument (structure) and having one’s facts straight(content), even though the two are correlated.
In addition to providing a methodology for charac-terizing intuitive theories, this study suggests that ele-mentary school children can reason theoretically aboutthe aspect of the larger domain of biological knowl-edge of interest to us, knowledge of the effects of usingdrugs. Even some of the youngest students appeared to
72
DAVIES ET AL.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

have many of the ingredients of a causal explanatoryframework for drug action. Moreover, most studentsused biological concepts to account for the action of al-cohol and cocaine, as they do to account for illness(e.g., Springer & Ruckel, 1992), and they did so with-out the aid of structured questions.
From an applied perspective, instruction aboutdrugs may prove more effective if grounded in an intu-itive theories framework that capitalizes on the ten-dency of children to seek meaningful explanations ofthe world around them. For the youngest elementaryschool students, instruction might begin with a rudi-mentary brain theory of drug action. Many of thesechildren already know that more is involved than an in-put–output association and appreciate that the brain isan important “node” in the causal chain. Thus, by firstand second grade it appears that children could learn atheory that posits that a drug somehow alters the brain,which in turn alters behavior. Because only a minorityof children at any grade level spontaneously mentionblood, it may also be appropriate to introduce the im-portant role of the bloodstream to the youngest stu-dents and to reinforce it to students in the upper gradelevels. This basic theory could then be built upon laterin elementary school by teaching students about otherlinks and nodes in the causal chain and helping themconstruct more elaborate explanations of the relation-ships among drugs, the brain, and behavior—for exam-ple, explanations referring to specific brain parts andfunctions and to stimulant or depressant effects on thenervous system. Even older elementary school chil-dren have much to learn, judging from the data pre-sented here.
Will teaching children a scientifically correct theoryof how alcohol and drug abuse can compromise func-tioning and health discourage them from using sub-stances, though? On one hand, many studies suggestthat knowledge-based or informational drug preven-tion programs, although they enhance knowledge,rarely change attitudes and behavior (Bangert-Drowns,1988; Hansen, 1992). Yet information about the effectsof drug and alcohol use is still considered a necessary,if not sufficient, component of comprehensive drugprevention interventions that emphasize social influ-ence processes and social-skill training (Hansen,1992). Indeed, evidence suggests that beliefs about thelikely effects of substance use and abuse do influencesubstance use behavior in adolescence (e.g., Smith &Goldman, 1994).
Moreover, our own unpublished data suggest that aprogram designed to teach children a coherent scien-tific theory of the effects of alcohol and cocaine thatfeatures the mediating roles of the circulatory systemand brain, although it had no effects on alcohol atti-tudes, intentions, and use, resulted in more negative at-titudes toward and lower intentions to use cocaine,even 1 full year later, than a control curriculum about
disease (Sigelman, Rinehart, Sorongon, Bridges, &Wirtz, 2003). In short, although informational drugprevention programs are unlikely to be a panacea, thereis merit in further research to determine which aspectsof knowledge are most closely associated with sub-stance use and abuse and whether educational pro-grams grounded in the intuitive theories perspectivewill prove more effective than earlier knowledge-basedprograms, many of which conveyed isolated factsabout drugs rather than a coherent explanation of howdrugs impair functioning.
In conclusion, this research has shown that chil-dren’s thinking about drug action has a certain degreeof theoretical structure and is grounded in basic biolog-ical facts. Through instruction that provides meaning-ful information about drug action and is appropriate tostudents’ levels of cognitive development, children cangain a theoretical foundation on which they may ulti-mately base decisions about using drugs. The intuitivetheories approach shows promise both for understand-ing the development of knowledge of health topics andfor advancing it.
References
Au, T. K., & Romo, L. F. (1996). Building a coherent conception ofHIV transmission: A new approach to AIDS education. In D.Medin (Ed.), The psychology of learning and motivation, 35(pp. 193–241). San Diego: Academic.
Au, T. K., & Romo, L. F. (1999). Mechanical causality in children’s“folkbiology.” In D. L. Medin & S. Atran (Eds.), Folkbiology(pp. 355–401). Cambridge, MA: MIT Press.
Austin, E. W., & Nach-Ferguson, B. (1995). Sources and influencesof young school-age children’s general and brand-specificknowledge about alcohol. Health Communication, 7, 1–20.
Bangert-Drowns, R. L. (1988). The effects of school-based sub-stance abuse education: A meta-analysis. Journal of Drug Edu-cation, 18, 243–264.
Bibace, R., Sagain, J. D., & Dyl, J. (1998). The heuristic value ofWerner’s co-existence concept of development. Journal of Ap-plied Developmental Psychology, 19, 153–163.
Carey, S. (1985). Conceptual change in childhood. Cambridge, MA:MIT Press.
Crider, K. (1981). Children’s conceptions of the body interior. In R.Bibace & M. Walsh (Eds.), New directions for child develop-ment: Children’s conceptions of health, illness, and bodilyfunctions (pp. 49–65). San Francisco, CA: Jossey-Bass.
Dunn, M. E., & Goldman, M. S. (1996). Empirical modeling of an al-cohol expectancy memory network in elementary school chil-dren as a function of grade. Experimental and ClinicalPsychopharmacology, 4, 209–217.
Gaines, L. S., Brooks, P. H., Maisto, S., Dietrich, M., & Shagena, M.(1988). The development of children’s knowledge of alcoholand the role of drinking. Journal of Applied DevelopmentalPsychology, 9, 441–457.
Gelman, S. A. (1996). Concepts and theories. In R. Gelman & T. K.Au (Eds.), Perceptual and cognitive development (pp.117–150). San Diego: Academic.
Gelman, S. A., & Kalish, C. W. (1993). Categories and causality. InR. Rasnak & M. L. Howe (Eds.), Emerging themes in cognitivedevelopment: Volume II: Competencies (pp. 3–32). New York:Springer-Verlag.
73
DRUG ACTION
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014

Gopnik, A., & Meltzoff, A. N. (1997). Words, thoughts, and theories.Cambridge, MA: MIT Press.
Gopnik, A., & Wellman, H. M. (1994). The theory theory. In L. A.Hirschfeld & S. A. Gelman (Eds.), Mapping the mind: Domainspecificity in cognition and culture (pp. 257–293). New York:Cambridge University Press.
Hansen, W. B. (1992). School-based substance abuse prevention: Areview of the state of the art in curriculum, 1980–1990. HealthEducation Research, 7, 403–430.
Hatano, G., & Inagaki, K. (1994). Young children’s naïve theory ofbiology. Cognition, 50, 171–188.
Hatano, G., & Inagaki, K. (1999). A developmental perspective oninformal biology. In D. L. Medin & S. Atran (Eds.), Folkbiology(pp. 321–354). Cambridge, MA: MIT Press.
Johnson, C. N., & Wellman, H. M. (1982). Children’s developingconceptions of the mind and brain. Child Development, 53,222–234.
Johnson, H. L., & Johnson, P. B. (1995). Children’s alcohol-relatedcognitions: Positive versus negative alcohol effects. Journal ofAlcohol and Drug Education, 40, 1–12.
Keil, F. C. (1989). Concepts, kinds, and cognitive development.Cambridge, MA: MIT Press.
Keil, F. C., Levin, D. T., Richman, B. A., & Gutheil, G. (1999).Mechanism and explanation in the development of biologicalthought: The case of disease. In D. L. Medin & S. Atran (Eds.),Folkbiology (pp. 285–319). Cambridge, MA: MIT Press.
Kistner, J., Ebertstein, I. W., Balthazor, M., Castro, R., Foster, K.,Osborne, M., et al. (1996). Assessing children’s conceptions ofAIDS. Journal of Pediatric Psychology, 21, 269–281.
Lieberman, L. D., Clark, N. M., Krone, K. V., Orlandi, M. A., &Wynder, E. L. (1992). The relationship between cognitive ma-turity and information about health problems among school agechildren. Health Education Research, 7, 391–401.
Meltzer, J., Bibace, R., & Walsh, M. E. (1984). Children’s concep-tions of smoking. Journal of Pediatric Psychology, 9, 41–56.
Nagy, M. H. (1953). Children’s conceptions of some bodily func-tions. Journal of Genetic Psychology, 83, 199–216.
Novak, J. D. (1990). Concept mapping: A useful tool for science ed-ucation. Journal of Research in Science Teaching, 27, 937–949.
Ott, R. L. (1993). An introduction to statistical methods and dataanalysis. Belmont, CA: Duxbury Press, Wardsworth PublishingCompany.
Piaget, J. (1929). The child’s conception of the world. New York:Harcourt, Brace & World.
Rosenblit, L., & Keil, F. (2002). The misunderstood limits of folkscience: An illusion of explanatory depth. Cognitive Science,26, 521–562.
Siegler, R. S., & Jenkins, E. (1989). How children discover newstrategies. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.
Siegler, R. S., & Thompson, D. R. (1998). “Hey, would you like anice cold cup of lemonade on this hot day?”: Children’s under-standing of economic causation. Developmental Psychology,34, 146–160.
Sigelman, C. K., Estrada, A. L., Derenowski, E. B., & Woods, T. E.(1996). Intuitive theories of human immunodeficiency virustransmission: Their development and implications. Journal ofPediatric Psychology, 21, 555–572.
Sigelman, C. K., Leach, D. B., Mack, K. L., Bridges, L. J., Rinehart,C. S., Dwyer, K. M., et al. (2000). Children’s beliefs about thelong-term health effects of alcohol and cocaine use. Journal ofPediatric Psychology, 25, 557–566.
Sigelman, C. K., Rinehart, C. S., Sorongon, A. G., Bridges, L. J., &Wirtz, P. W. (2003). Teaching a coherent theory of drug actionto elementary school children. Manuscript submitted for publi-cation.
Sigelman, C. K., Silk, A., Goldberg, F., Davies, E. P., Dwyer, K. M.,Leach, D., et al. (1999). Developmental differences in beliefsabout how alcohol and cocaine affect behavior. Journal of Ap-plied Developmental Psychology, 20, 597–614.
Smith, G. T., & Goldman, M. S. (1994). Alcohol expectancy theoryand the identification of high-risk adolescents. Journal of Re-search on Adolescence, 4, 229–247.
Solomon, G. E. A., & Cassimatis, N. L. (1999). On facts and concep-tual systems: Young children’s integration of their understand-ings of germs and contagion. Developmental Psychology, 35,113–126.
Springer, K. (1995). Acquiring a naïve theory of kinship through in-ference. Child Development, 66, 547–558.
Springer, K., Ngyuen, T., & Samaniego, R. (1996). Early under-standing of age- and environment-related noxiousness in bio-logical kinds: Evidence for a naïve theory. Cognitive Develop-ment, 11, 65–82.
Springer, K., & Ruckel, J. (1992). Early beliefs about the cause of ill-ness: Evidence against immanent justice. Cognitive Develop-ment, 7, 429–443.
Wellman, H. M. (1990). The child’s theory of mind. Cambridge, MA:MIT Press.
Wellman, H. M., & Gelman, S. (1992). Cognitive development:Foundational theories of core domains. Annual Review of Psy-chology, 43, 337–375.
Received January 1, 2003Final revision received June 9, 2003Accepted July 29, 2003
74
DAVIES ET AL.
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
16:
04 2
6 O
ctob
er 2
014