A Case of Rodenticide Poisoning
51
A CASE OF JAUNDICE PROF.DR.K.H.NOORUL AMEEN’S UNIT ( M 4) DR.M.ARIVUMANI
-
Upload
stanley-medical-college-department-of-medicine -
Category
Health & Medicine
-
view
4.387 -
download
21
Transcript of A Case of Rodenticide Poisoning

A CASE OF JAUNDICE
PROF.DR.K.H.NOORUL AMEEN’S UNIT ( M 4)
DR.M.ARIVUMANI

20 yrs old Mr.Dhanasekar was referred from vinayaka missions medical college hospital salem to GSH on 8.10.11
On 4.10.11 He was taken to a private hospital near salem with c/o vomiting,abdominal pain,giddiness
On the suspicious history given by parents Stomcah wash was given at the primary care hospital and he was referred to VMMCH.

At VMMCH patient was managed on conservative lines.On 2nd day of admission patient developed jaundice with altered liver parameters.
On probing the patient came out with h/o ingestion of rodenticide poison ON 1.10.11(4 days prior)
(RATOL)

He was managed conservatively with N-acetyl cysteine, dextrose, vitamin k etc

Since the patients jaundice was progressively increasing he was referred to SMCH for liver transplantation.

Patient on 8.10.11 got admitted in our IMCU with c/o yellowish discolouration of eyes
h/o abdominal pain h/o vomiting h/o anorexia no h/o fever no h/o pedal edema,
no h/o abdominal distension

no h/o bleeding manifestation no h/o altered sensorium /seizures Past history no h/o jaundice in the past no h/o blood transfusion

On admission patient was conscious,oriented afebrile,not dyspnoeic icteric no cyanosis,no clubbing,no pedal
edemaVitals PR-88/min RR-24/min BP-100/60mmhg

CVS S1 S2 heard,no murmurRS –NVBS heard,no crepsP/A-Right hypochondrial tenderness + no organomegalyCNS- NFND

CBC
4.10.11 7.10.11 8.10.11 13.10.11
15.10
Hb 15.5 14.2 14.1 14.0 13.8
TC 6400 7200 6100 6500 5800
PCV 46.5 42.6 42 42 41.4
PLT 219000 75000 68000 120000 150000

RFT WITH ELECTROLYTES
4.10 6.10 8.10 18.10
SUGAR 90 110 85 104
UREA 36 25 26 32
CREATININE
0.4 0.8 0.7 0.6
SODIUM 131 133 129 134
POTASSIUM
5.2 6.4 5.2 4.5
CHLORIDE 103 98.6 90
BICORBONATE
18 22 23

LFT
4/10 6/10 8/10(sp 3)
9/10 12/10 18/10
Total bilirubin
18.2 17.2 11.6 20.1 16.9 11.6
direct
9.9 9.3 8.93 8.9 8.3 5.1
indir 8.3 7.9 2.67 11.2 8.6
SGOT 2240 750 480 138 77 164
SGPT 1556 335 910 99 236 161
SAP 239 720 558
GGT 76 64
Total protein
6.5 4.6 5.2
albumin
3.1 3.0 3.1

4/10 7/10 8/10 9/10 12/10 18/10
PTTestControl
>2min13sec
42sec12.5sec
37sec13sec
26sec12sec
20sec11sec
13.4sec
PTTTestControl
53sec24.7sec
23sec 48sec 45sec 40sec 30sec
INR 3.3 2.8 2.2 1.8 1.3

ABG-COMPENSATED RESPIRATORY ALKALOSIS
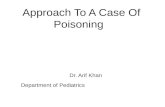
URINE
Colour Yellow
Appearance Cloudy
Specific gravity 1.010
PH 7.0
Protein Negative
Sugar Nil
Ketone Absent
Rbc Nil
Pus cells 2-5
Epithelial cell 2-3
BS/BP Positive
Urobilinogen increased

Serum LDH- 383U/L(135-225U/L) Reticulocyte count-2.3 % HBsAg-negative HIV-negative Anti HCV-negative Anti HEV-negative ANA-negative Serum cerruloplasmin 30mg/dl
Peripheral smear RBC-erythropenia with predominantly
normochromic normocytic RBC WBC-mild leukocytosis + Platelets-mild thrombocytopenia seen.

ECG-normal Chest x ray- noraml USG abdomen-liver normal in size,normal
echo texture,ascites +(minimal),splenomegaly+

RATOL-Rodenticide poisoning(yellow phosphorus)
Acute liver failure-recovering

GASTROENTEROLOGIST OPINION
Opined as acute fulminant hepatitis (toxic) Conservative management
TREATMENT GIVEN
Intravenous dextrose Inj vitamin k 10mg iv od Inj ranitidine 50mg iv bd Cap.UDCA 300mg BD Other supportive measures FFP transfusion

RODENTICIDE POISONING
ORGANIC coumarins warfarins and superwarfarins. indandionesINORGANIC thallium sulphate yellow phosphorus zinc phosphide aluminium phosphide arsenic

COUMARINS AND INDANDIONES
Coumarins and indandiones depresses the hepatic synthesis of vitamin k dependent clotting factors.
They also increase the permeabilty of capillaries predisposing to haemorrhage.
Mostly present as epistaxis,bleeding gums,hematuria,echymoses.
Continuous Monitoring of PT is necessary.

Vitamin k1 phytonadione 12-25mg oral or 10mg parenterally.
Intravenous infusion of vtamin k1(aquamephyton) in saline or dextrose is recommended for continuous bleeding.
There is no need to begin therapy unless the INR> 2. No data exist to prove that such therapy prevents anticoagulation, although vitamin K therapy is shown to reverse anticoagulation once it develops.
With long-acting anticoagulants, treatment may need to be at much higher doses and for a protracted period of time

THALLIUM SULFATE
Insidious onset Early symptoms include
nausea,vomiting,bloody diarrhoea,stomatitis,salivation
Liver injury can occur Muscle
weakness,paresthesia,tremor,ptosis,ataxia, myoclonic jerks, Hypotension,ventricular arrythmias ARDS
PHOSPHORUS POISONING
Elemental phosphorus exists in two forms—red and yellow.
Red phosphorus is nonvolatile, insoluble, and unabsorbable, and therefore nontoxic when ingested.
Yellow phosphorus (also referred to as white phosphorus) is a severe local and systemic toxin causing damage to gastrointestinal, hepatic, cardiovascular, and renal systems

YELLOW PHOSPHORUS Yellow phosphorus is used as rodenticides and in
fireworks.
The most readily available source of yellow phosphorus today is rodenticides.
Rodenticides are available as powders or pastes containing 2 to 5% of yellow phosphorus.
Minimum dose 15mg; lethal dose 60mg (1mg/kg)
Mortality rate 27% to 48% .

Yellow phosphorus emits smoke(Phosphine gas) and has very strong garlicky odour. It can get absorbed through skin, mucus membrane, respiratory and gastrointestinal epithelium.
Bile salts are important for absorption of phosphorus. Because of water content and low oxygen tension, phosphorus remains stable in gut for longer period.
Phosphorus is a general protoplasmic poison causing cardiac, hepatic, renal, and multiorgan failure

The patient with yellow phosphorus intoxication passes through three stages.
FIRST STAGE- occurs during the first 24 hours in which patient is either asymptomatic or has signs and symptoms of local gastrointestinal irritation.
SECOND STAGE- occurs between 24 to 72 hours after ingestion. It is an asymptomatic period and the patient may be discharged prematurely. There may be mild elevation of liver enzymes and bilirubin in this stage

THIRD STAGE (ADVANCED) OCCURS AFTER 72 HOURS UNTIL THE RESOLUTION OF SYMPTOMS OR DEATH.
Hepatomegaly and jaundice appear-acute fulminant hepatic failure mandating liver transplantation.
Bleeding can occur due to coagulopathy and thrombocytopenia
Some patients may develop acute tubular necrosis and present with acute renal failure.

THIRD STAGE (ADVANCED) OCCURS AFTER 72 HOURS UNTIL THE RESOLUTION OF SYMPTOMS OR DEATH(CONT….)
Hemolysis can occur due to destruction of RBC’s by phosphorus
Central nervous system effects include changes in mental status like confusion, psychosis, hallucinations, and coma.
Cardiac toxicity includes hypotension, tachycardia, arrhythmias,toxic myocarditis and cardiogenic shock.

PATHOLOGY
Liver shows extensive hepatocyte periportal necrosis with balloon degeneration.
Acute Toxicity: Zone 1 necrosis +/- microvesicular steatosis.


ZINC PHOSPHIDE
Patients presents with same systemic toxicities encountered in yellow phosphorus poisoning jaundice,hepatic failure
Tetany due to hypocalcemia
Renal tubular damage
Arrythmias ,cardiomyopathy

MANAGEMENT
There is no specific antidote for yellow phosphorus. Treatment is directed at removal of the poison and supportive therapy.
N-acetyl cysteine can be tried if patient presents early.150mg/kg bolus,50mg/kg over 4 hours,then 100mg/kg over next 16hours.

MANAGEMENT
Gastric lavage with potassium permanganate is recommended to convert the phosphorus to relatively harmless oxides.
0.1 to 0.2 % copper sulphate can be used.it will precipitate as copper sulphide and coat over phosphorus particles
charcaol can be used

vitamin k 10- 20mg iv in repeated dose Intravenous dextrose Fresh frozen plasma to correct coagulopathy. Non fatty purgatives like mgso4 to eliminate
phosphorus Avoid fatty foods since they promote
phosphorus absorption. IV steroids exchange transfusion(for hemolysis)-but it
does not prevent the onset of coma or increase survival.
PD/HD if renal failure develops.

Careful monitoring of hepatic and renal function and management of their failure is required.
Liver transplantation has been done in suitable candidates for acute hepatic failure

KINGS COLLEGE CRITERIA FOR LIVER TRANSPLANTATIONAcetaminophen-induced disease
Arterial pH <7.3 (irrespective of the grade of encephalopathy) or
Grade III or IV encephalopathy, and
Prothrombin time >100 seconds, and
Serum creatinine >3.4mg/dl

KINGS COLLEGE CRITERIA FOR LIVER TRANSPLANTATION(CONT…)
All other causes of fulminant hepatic failure Prothrombin time >100 seconds (irrespective of the
grade of encephalopathy) or Any three of the following variables (irrespective of
the grade of encephalopathy) Age <10 years or >40 years Etiology: non-A, non-B hepatitis, halothane hepatitis,
idiosyncratic drug reactions Duration of jaundice before onset of encephalopathy
>7 days Prothrombin time >50 seconds Serum bilirrubin >18 mg/dl

HEPATOTOXICITY OF METALS-THE CULPRITS
Aluminum Manganese Barium Phosphorus Cadmium Thallium Iron Zinc Arsenic Beryllium Chromium Gold Lead

HEPATOTOXICITY OF METALSALUMINUM
Non-caseating granulomas in patients on long
term hemodialysis (Kurumay et al, 1989)
Contributes to hepatic injury in patients on total
parenteral nutrition (Klein et al, 1984)

HEPATOTOXICITY OF METALSARSENIC (1)
Acute Toxicity Intrahepatic cholestasis Steatosis Zone 3 necrosis ↑ Mitotic activity Venocclusive disease

HEPATOTOXICITY OF METALSARSENIC (2)
Chronic Toxicity Hepatoportal sclerosis Systemic arterial disease Cirrhosis Angiosarcoma Hepatocellular carcinoma

HEPATOTOXICITY OF METALSBARIUM
Intravasation of BaSO4 enema into portal venous
system →portal pylephlebitis or liver abscess

HEPATOTOXICITY OF METALSCOPPER (1)
Acute Toxicity: Zone 3 necrosis; cholestasis; hypertrophy of Kupffer cells with erythrophagocytosis; copper accumulation in
Kupffer cells

HEPATOTOXICITY OF METALSCOPPER (2)
Chronic Toxicity: Epithelioid granulomas Cirrhosis with Mallory bodies resembling
Indian childhood cirrhosis Angiosarcoma

Indian J Pharmacol. 2011 May-Jun; 43(3): 355–356
Acute hepatic failure due to yellow phosphorus ingestion
Anupama Mauskar, Kunal Mehta, Leena Nagotkar, and Preeti Shanbag
Department of Pediatrics, Lokmanya Tilak Municipal General Hospital, Sion, Mumbai, India

J Assoc Physicians India. 2003 Aug;51:816-7. Rodenticide-induced hepatotoxicity. Karanth S, Nayyar V. Source Department of Critical Care Medicine, Airport
Road, Bangalore 560 017

Fernandez OU, Canizares LL. Acute hepatotoxicity from ingestion of yellow phosphorus-containing fireworks.
J Clin Gastroenterol. 1995;21:139–42.
Santos O, Restrepo JC, Velasquez L, Castano J, Correa G, Sepulveda E, et al.
Acute liver failure due to white phosphorus ingestion.
Annals of hepatology. 2009;8:162–5.

PURPOSE OF PRESENTATION Hepatotoxicity following acute poisoning with
rodenticides has been infrequently reported in literature
To emphasize the fact that this form of clinical
presentation is not unusual. All rodenticide poisoning are not due to coumarin
derivatives. Yellow phosphorus poisoning is benign in early
stage,becomes fulminant in 3rd stage. Identifying exact component of rodenticide is
mandatory before planning for discharge. LFT /PT should be mandatory in all cases. All rodenticide poisoning patients should be reviewed
atleast once with LFT values in a week time.

REFERENCES
Forensic medicine and toxicology R.N.Karmakar.
Medical toxicology Richard.C.Dart. Annals of hepatology april-june 2009.
THANK YOU