A Case of Pheochromocytoma Initially Manifesting as Acute...
4
150 http://jsms.sch.ac.kr A Case of Pheochromocytoma Initially Manifesting as Acute Myocardial Infarction Seung Seok Chae 1 , Joon Tae Kang 1 , Young Keun Ahn 1 , Ran Hong 2 , Joon Woo Kim 3 1 Department of Internal Medicine, Chonnam National University Hospital, Gwangju; 2 Department of Pathology, Chosun University Hospital, Gwangju; 3 Department of Internal Medicine, Mokpo Jung-Ang General Hospital, Mokpo, Korea Pheochromocytomas are rare catecholamine-secreting neuroendocrine tumors arising from chromaffin cells in the adrenal me- dulla. Typical classic triad are consisted of headaches, palpitations, and profuse diaphoresis. But some patients with pheochromocy- tomas have other cardiovascular manifestations such as left ventricular hypertrophy, congestive heart failure, and cardiac arrhyth- mia. Rarely, pheochromocytomas manifest as acute myocardial infarction leading to delayed diagnosis and treatment. We experi- enced one case of pheochromocytoma initially manifesting as acute myocardial infarction which showed normal coronary artery on coronary angiography. Pheochromocytoma should be suspected and evaluated in patients with acute myocardial infarction whose coronary angiography shows normal coronary without definite thrombosis. Keywords: Pheochromocytoma; Acute myocardial infarction; Coronary angiography INTRODUCTION Pheochromocytoma is neuroendocrine tumor releasing ca- thecholamines such as norepinephrine, epinephrine, and dopa- mine and being one of the etiologies of secondary hypertension. Typical triad of symptoms is consisted of headache, diaphoresis, and palpitation. However, persistent or paroxysmal hypertension is the only feature of pheochromocytoma instead of these typical symptoms in many patients. In addition to hypertension, other cardiovascular manifestations such as left ventricular hypertro- phy, congestive heart failure, and cardiac arrhythmia are observed in patients with pheochromocytoma. Rarely, pheochromocytoma manifests as acute myocardial infarction leading to delayed diag- nosis and treatment. When patients with pheochromocytoma who present this rare cardiovascular manifestation without typi- cal symptoms visit the emergency room, doctors can miss the hid- den pheochromocytoma and let the patient’ s prognosis get worse leading to being diagnosed at autopsy. We experienced one case of pheochromocytoma initially manifesting as acute myocardial in- farction which showed normal coronary artery on coronary angi- ography. So early diagnosis is very important for appropriate treat- ment and prognosis of the patients. CASE REPORT A 49-year-old woman visited emergency room complaining of retrosternal pain who was transferred from local hospital with the impression of acute coronary syndrome. On past history, she had been taking medicine for type 2 diabetes. At admission, her blood pressure was 90/60 mm Hg and his pulse rate was 102 per minutes. On laboratory findings, each creatine kinase-myocardial band (CK-MB) and troponin-I were elevated by 55.0 ng/mL and 0.065 ng/mL. After follow-up, CK-MB was slightly decreased by 48.3 ng/ mL but troponin-I was increased by 0.078 ng/mL. There were about 2 mm ST segment depression with T-wave inversion on pre- cordial leads and inferior leads on electrocardiography at admis- sion day (Fig. 1A). On echocardiography, ejection fraction was de- creased by 40% and left ventricular hypertrophy with wall motion Soonchunhyang Medical Science 21(2):150-153, December 2015 pISSN: 2233-4289 I eISSN: 2233-4297 CASE REPORT Correspondence to: Joon Woo Kim Department of Internal Medicine, Mokpo Jung-Ang General Hospital, 623 Yeongsan-ro, Mokpo 58615, Korea Tel: +82-61-280-3114, Fax; +82-61-282-3750, E-mail: [email protected] Received: Aug. 14, 2015 / Accepted after revision: Sep. 24, 2015 © 2015 Soonchunhyang Medical Research Institute This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/).
Transcript of A Case of Pheochromocytoma Initially Manifesting as Acute...

150 http://jsms.sch.ac.kr
A Case of Pheochromocytoma Initially Manifesting as Acute Myocardial InfarctionSeung Seok Chae1, Joon Tae Kang1, Young Keun Ahn1, Ran Hong2, Joon Woo Kim3
1Department of Internal Medicine, Chonnam National University Hospital, Gwangju; 2Department of Pathology, Chosun University Hospital, Gwangju; 3Department of Internal Medicine, Mokpo Jung-Ang General Hospital, Mokpo, Korea
Pheochromocytomas are rare catecholamine-secreting neuroendocrine tumors arising from chromaffin cells in the adrenal me-dulla. Typical classic triad are consisted of headaches, palpitations, and profuse diaphoresis. But some patients with pheochromocy-tomas have other cardiovascular manifestations such as left ventricular hypertrophy, congestive heart failure, and cardiac arrhyth-mia. Rarely, pheochromocytomas manifest as acute myocardial infarction leading to delayed diagnosis and treatment. We experi-enced one case of pheochromocytoma initially manifesting as acute myocardial infarction which showed normal coronary artery on coronary angiography. Pheochromocytoma should be suspected and evaluated in patients with acute myocardial infarction whose coronary angiography shows normal coronary without definite thrombosis.
Keywords: Pheochromocytoma; Acute myocardial infarction; Coronary angiography
INTRODUCTION
Pheochromocytoma is neuroendocrine tumor releasing ca-thecholamines such as norepinephrine, epinephrine, and dopa-mine and being one of the etiologies of secondary hypertension. Typical triad of symptoms is consisted of headache, diaphoresis, and palpitation. However, persistent or paroxysmal hypertension is the only feature of pheochromocytoma instead of these typical symptoms in many patients. In addition to hypertension, other cardiovascular manifestations such as left ventricular hypertro-phy, congestive heart failure, and cardiac arrhythmia are observed in patients with pheochromocytoma. Rarely, pheochromocytoma manifests as acute myocardial infarction leading to delayed diag-nosis and treatment. When patients with pheochromocytoma who present this rare cardiovascular manifestation without typi-cal symptoms visit the emergency room, doctors can miss the hid-den pheochromocytoma and let the patient’s prognosis get worse leading to being diagnosed at autopsy. We experienced one case of pheochromocytoma initially manifesting as acute myocardial in-
farction which showed normal coronary artery on coronary angi-ography. So early diagnosis is very important for appropriate treat-ment and prognosis of the patients.
CASE REPORT
A 49-year-old woman visited emergency room complaining of retrosternal pain who was transferred from local hospital with the impression of acute coronary syndrome. On past history, she had been taking medicine for type 2 diabetes. At admission, her blood pressure was 90/60 mm Hg and his pulse rate was 102 per minutes. On laboratory findings, each creatine kinase-myocardial band (CK-MB) and troponin-I were elevated by 55.0 ng/mL and 0.065 ng/mL. After follow-up, CK-MB was slightly decreased by 48.3 ng/mL but troponin-I was increased by 0.078 ng/mL. There were about 2 mm ST segment depression with T-wave inversion on pre-cordial leads and inferior leads on electrocardiography at admis-sion day (Fig. 1A). On echocardiography, ejection fraction was de-creased by 40% and left ventricular hypertrophy with wall motion
Soonchunhyang Medical Science 21(2):150-153, December 2015 pISSN: 2233-4289 I eISSN: 2233-4297
CASE REPORT
Correspondence to: Joon Woo KimDepartment of Internal Medicine, Mokpo Jung-Ang General Hospital, 623 Yeongsan-ro, Mokpo 58615, KoreaTel: +82-61-280-3114, Fax; +82-61-282-3750, E-mail: [email protected]: Aug. 14, 2015 / Accepted after revision: Sep. 24, 2015
© 2015 Soonchunhyang Medical Research InstituteThis is an Open Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/).

A Case of Pheochromocytoma Initially Manifesting as Acute Myocardial Infarction • Chae SS, et al.
Soonchunhyang Medical Science 21(2):150-153 http://jsms.sch.ac.kr 151
abnormality was noted (Fig. 1B). Moreover, follow-up blood pres-sure was decreased to 70/40 mm Hg. As persistent retrosternal pain, increased cardiac enzymes, and left ventricular dysfunction suggested high risk acute myocardial infarction, emergent coro-nary angiography was performed and showed normal coronary ar-teries. Though patient’s clinical diagnosis was acute myocardial in-farction, coronary angiography was not matched with it. After re-peating patient’s history, we found that she was heard about high blood pressure at another hospital and she had taken some medi-cines for perimenopausal symptoms such as headache and palpita-tions. Also fluctuation of her systolic blood pressure from 220 mm Hg at local hospital to 70 mm Hg at emergency room was noted. All of these findings (fluctuation of blood pressure, headache, and palpitation) suggested that she might have secondary hypertension associated with increased catecholamines. On abdominal ultraso-
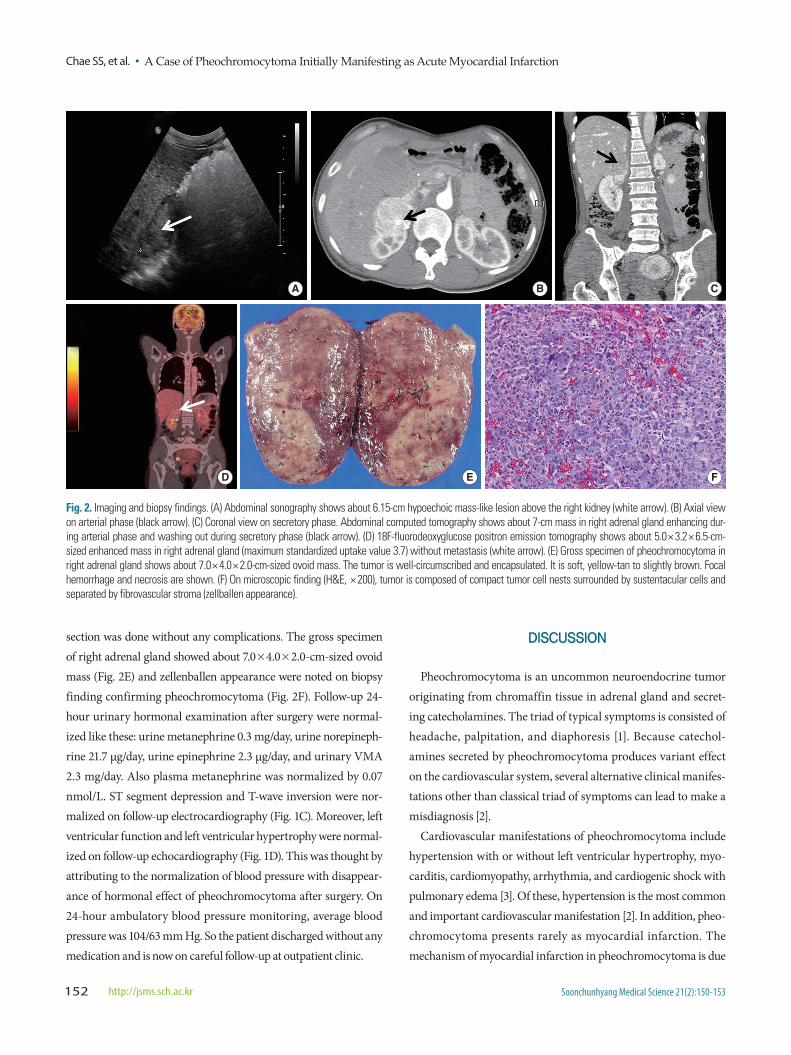
nography, about 6.15-cm-sized hypoechoic mass was found in right adrenal gland (Fig. 2A). Serial abdominal computed tomography also showed about 7-cm-sized mass in right adrenal gland (Fig. 2B, C). On 24-hour urinary hormonal examination, the results were as like these: urine metanephrine 16.3 mg/day (<0.8 mg/day), urine norepinephrine 2,783.4 mg/day (range, 15 to 80 μg/day), urine epi-nephrine 30.3 μg/day (range, 0 to 20 μg/day), and urine vanillyl-mandelic acid (VMA) 33.5 μg/day (range, 0 to 8 μg/day). Also plas-ma metanephrine was 16.70 nmol/L (<0.9 nmol/L). So the diagno-sis of pheochromocytoma were made by patient’s clinical manifes-tation, abdominal imaging, and 24-hour urinary hormonal exami-nation. As 10% of pheochromocytoma could have malignancy and multiple metastases, 18F-fluorodeoxyglucose positron emission to-mography were done but didn’t showed multiple metastases (Fig. 2D). After 2 weeks of α-blocker medication, successful surgical re-
A B
C D
Fig. 1. Electrocardiographic and echocardiographic findings. (A) Electrocardiography on admission day shows ST depression with T wave inversion in V2-6, lead II, III, and aVF. (B) Echocardiography on admission day shows left ventricular hypertrophy. (C) Abnormal electrocardiographic findings on admission day was normalized after surgery. (D) On follow-up echocardiography, left ventricular hypertrophy is disappeared after surgery.
Chae SS, et al. • A Case of Pheochromocytoma Initially Manifesting as Acute Myocardial Infarction
Soonchunhyang Medical Science 21(2):150-153152 http://jsms.sch.ac.kr
section was done without any complications. The gross specimen of right adrenal gland showed about 7.0×4.0×2.0-cm-sized ovoid mass (Fig. 2E) and zellenballen appearance were noted on biopsy finding confirming pheochromocytoma (Fig. 2F). Follow-up 24-hour urinary hormonal examination after surgery were normal-ized like these: urine metanephrine 0.3 mg/day, urine norepineph-rine 21.7 μg/day, urine epinephrine 2.3 μg/day, and urinary VMA 2.3 mg/day. Also plasma metanephrine was normalized by 0.07 nmol/L. ST segment depression and T-wave inversion were nor-malized on follow-up electrocardiography (Fig. 1C). Moreover, left ventricular function and left ventricular hypertrophy were normal-ized on follow-up echocardiography (Fig. 1D). This was thought by attributing to the normalization of blood pressure with disappear-ance of hormonal effect of pheochromocytoma after surgery. On 24-hour ambulatory blood pressure monitoring, average blood pressure was 104/63 mm Hg. So the patient discharged without any medication and is now on careful follow-up at outpatient clinic.
DISCUSSION
Pheochromocytoma is an uncommon neuroendocrine tumor originating from chromaffin tissue in adrenal gland and secret-ing catecholamines. The triad of typical symptoms is consisted of headache, palpitation, and diaphoresis [1]. Because catechol-amines secreted by pheochromocytoma produces variant effect on the cardiovascular system, several alternative clinical manifes-tations other than classical triad of symptoms can lead to make a misdiagnosis [2].
Cardiovascular manifestations of pheochromocytoma include hypertension with or without left ventricular hypertrophy, myo-carditis, cardiomyopathy, arrhythmia, and cardiogenic shock with pulmonary edema [3]. Of these, hypertension is the most common and important cardiovascular manifestation [2]. In addition, pheo-chromocytoma presents rarely as myocardial infarction. The mechanism of myocardial infarction in pheochromocytoma is due
A B C
D E F
Fig. 2. Imaging and biopsy findings. (A) Abdominal sonography shows about 6.15-cm hypoechoic mass-like lesion above the right kidney (white arrow). (B) Axial view on arterial phase (black arrow). (C) Coronal view on secretory phase. Abdominal computed tomography shows about 7-cm mass in right adrenal gland enhancing dur-ing arterial phase and washing out during secretory phase (black arrow). (D) 18F-fluorodeoxyglucose positron emission tomography shows about 5.0× 3.2× 6.5-cm-sized enhanced mass in right adrenal gland (maximum standardized uptake value 3.7) without metastasis (white arrow). (E) Gross specimen of pheochromocytoma in right adrenal gland shows about 7.0× 4.0× 2.0-cm-sized ovoid mass. The tumor is well-circumscribed and encapsulated. It is soft, yellow-tan to slightly brown. Focal hemorrhage and necrosis are shown. (F) On microscopic finding (H&E, × 200), tumor is composed of compact tumor cell nests surrounded by sustentacular cells and separated by fibrovascular stroma (zellballen appearance).

A Case of Pheochromocytoma Initially Manifesting as Acute Myocardial Infarction • Chae SS, et al.
Soonchunhyang Medical Science 21(2):150-153 http://jsms.sch.ac.kr 153
to a myocardial oxygen demand-supply mismatch. Coronary vaso-spasm, increased afterload with vasoconstriction, tachycardia, and a direct toxic effect by catecholamines can aggravate this mismatch resulting in chest pain, electrocardiographic changes (ST-T seg-ment change), and increased cardiac enzyme in patients with nor-mal coronary angiography [4,5].
Kim et al. [6] reported two cases of pheochromocytoma associ-ated with acute myocardial infarction. In this report, increased cardiac enzyme, eletrocardiographic changes, and regional wall motion abnormalities on echocardiography were matched with acute myocardial infarction. But the results of coronary angiogra-phy were normal. Through the blood pressure fluctuation and par-oxysmal increase in heart rate during admission pheochromocyto-ma was suspected and confirmed by adequate diagnostic process.
In our case, the patient’s clinical manifestation were compatible with myocardial infarction. Moreover, coronary angiography of the patient was normal. With careful history taking, patient’s symp-toms attributed to perimenopausal syndrome which were eventu-ally associated with underlying pheochromocytoma and blood pressure fluctuation were suspected for relating to pheochromocy-toma and finally found to be compatible with it. This diversity of clinical manifestation of pheochromocytoma can delay the diagno-sis and result deleterious cardiovascular outcome.
The treatment of choice in pheochromocytoma is surgical re-section. Before surgery, α-blocking agent such as phenoxybenza-mine should be preceded for at least 14 days. But in patients with pheochromocytoma presenting as acute myocardial infarction, β-blocking agents can be used because of myocardial infarction and result in catastrophic effects on pheochromocytoma due to an un-opposed α-receptor stimulation aggravating patient’s outcome [5].
So our case emphasize the importance of considering pheochro-mocytoma as the differential diagnosis of patients with acute myo-cardial infarction without the evidence of coronary atherosclerosis on coronary angiography.
Pheochromocytoma is often fatal when doctors do not have a clinical suspicion as it can present as many other cardiovascular manifestations including acute myocardial infarction just like our case. In patients with acute myocardial infarction whose clinical feature cannot be exactly explained by the result of eletrocardiogra-phy, echocardiography, cardiac enzymes, and coronary angiogra-phy, doctors should have a high clinical suspicion for underlying pheochromocytoma, especially if there is blood pressure fluctua-tion. Early diagnosis and surgical treatment of an underlying pheo-chromocytoma can prevent the complication of this lethal but cur-able disease and result in good outcome without critical morbidity or mortality.
REFERENCES
1. Lenders JW, Eisenhofer G, Mannelli M, Pacak K. Phaeochromocytoma. Lancet 2005;366:665-75.
2. Liao WB, Liu CF, Chiang CW, Kung CT, Lee CW. Cardiovascular mani-festations of pheochromocytoma. Am J Emerg Med 2000;18:622-5.
3. Jayaprasad N. Pheochromocytoma presenting as acute myocardial in-farction. J Vasc Med Surg 2015;3:(1-3).
4. Werbel SS, Ober KP. Pheochromocytoma: update on diagnosis, localiza-tion, and management. Med Clin North Am 1995;79:131-53.
5. Menke-van der Houven van Oordt CW, Twickler TB, van Asperdt FG, Ackermans P, Timmers HJ, Hermus AR. Pheochromocytoma mimick-ing an acute myocardial infarction. Neth Heart J 2007;15:248-51.
6. Kim DS, Kim KR, Yoon HJ, Lee HK, Ryu JC, Kim DI, et al. Two cases of pheochromocytoma associated with acute myocardial infarction. Korean J Med 1999;57:357-63.