A CASE OF MISMANAGED CERVICAL FRACTURE IN A ... - Spine … Fracture in... · limbs . MRI AT THE...
22
A CASE OF MISMANAGED A CASE OF MISMANAGED CERVICAL CERVICAL FRACTURE IN A PATIENT OF FRACTURE IN A PATIENT OF ANKYLOSING SPONDYLITIS ANKYLOSING SPONDYLITIS
Transcript of A CASE OF MISMANAGED CERVICAL FRACTURE IN A ... - Spine … Fracture in... · limbs . MRI AT THE...
A CASE OF MISMANAGED A CASE OF MISMANAGED CERVICALCERVICAL
FRACTURE IN A PATIENT OF FRACTURE IN A PATIENT OF ANKYLOSING SPONDYLITISANKYLOSING SPONDYLITIS
INTRODUCTIONINTRODUCTION
• Spine fractures occur with minor trauma in Spine fractures occur with minor trauma in patients with ankylosing Spondylitis. patients with ankylosing Spondylitis.
• They are highly unstable with a high They are highly unstable with a high incidence of neurological deficit. incidence of neurological deficit.
• Appropriate stabilization is the best option Appropriate stabilization is the best option in such cases. in such cases.
• Laminectomy further destabilizes the Laminectomy further destabilizes the fracture.fracture.
CASE HISTORYCASE HISTORY
• Age-70 yearsAge-70 years• Sex- maleSex- male• Known case of ankylosing spondylitis and Known case of ankylosing spondylitis and
diabetes mellitusdiabetes mellitus• History of fall while walking .History of fall while walking .• Patient developed weakness of all four Patient developed weakness of all four
limbs limbs

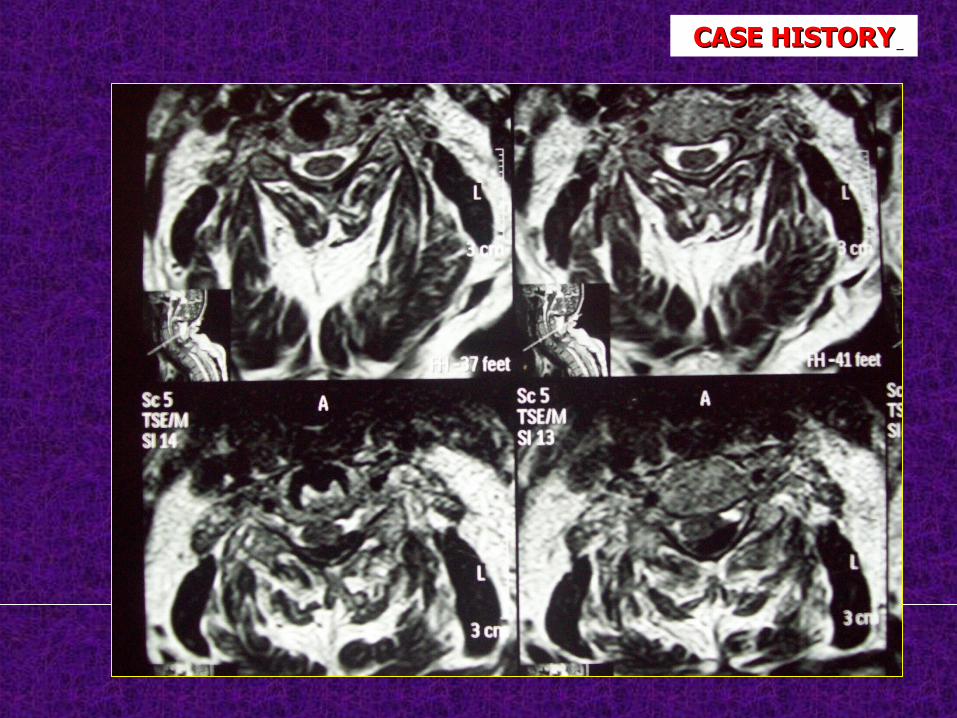
MRI AT THE TIME OF INJURYC6-7 extension compression injury stage 4 with minimal anterolisthesis ( Allen Fergussen classification ).
CASE HISTORYCASE HISTORY
CASE HISTORYCASE HISTORY
• He was treated elsewhere with C7 laminectomy.He was treated elsewhere with C7 laminectomy.
• Subsequently patient improved and started Subsequently patient improved and started walking with support.walking with support.
• Then 5 months after surgery, patient developed Then 5 months after surgery, patient developed a progressive neurological deficit and had a progressive neurological deficit and had progressive quadriparesis with bowel and progressive quadriparesis with bowel and bladder involvementbladder involvement
• Then patient came to ISIC for further treatmentThen patient came to ISIC for further treatment
CASE HISTORYCASE HISTORY
NEUROLOGICAL EXAMINATION ON NEUROLOGICAL EXAMINATION ON PRESENTATIONPRESENTATION
MOTOR MOTOR Right Right left left• C5 C5 5 5 5 5• C6C6 3 4 3 4• C7 C7 1 1 3 3• C8C8 1 1 3 3• T1T1 1 1 3 3• L2 3 3L2 3 3• L3 4 4L3 4 4• L4 5 5L4 5 5• L5 5 5L5 5 5• S1 5 5S1 5 5
SENSORY - SENSORY - INTACTINTACT PASPAS - PRESENT - PRESENT VACVAC - PRESENT - PRESENTASIA IMPAIRMENT SCALE - DASIA IMPAIRMENT SCALE - D
CASE HISTORYCASE HISTORY

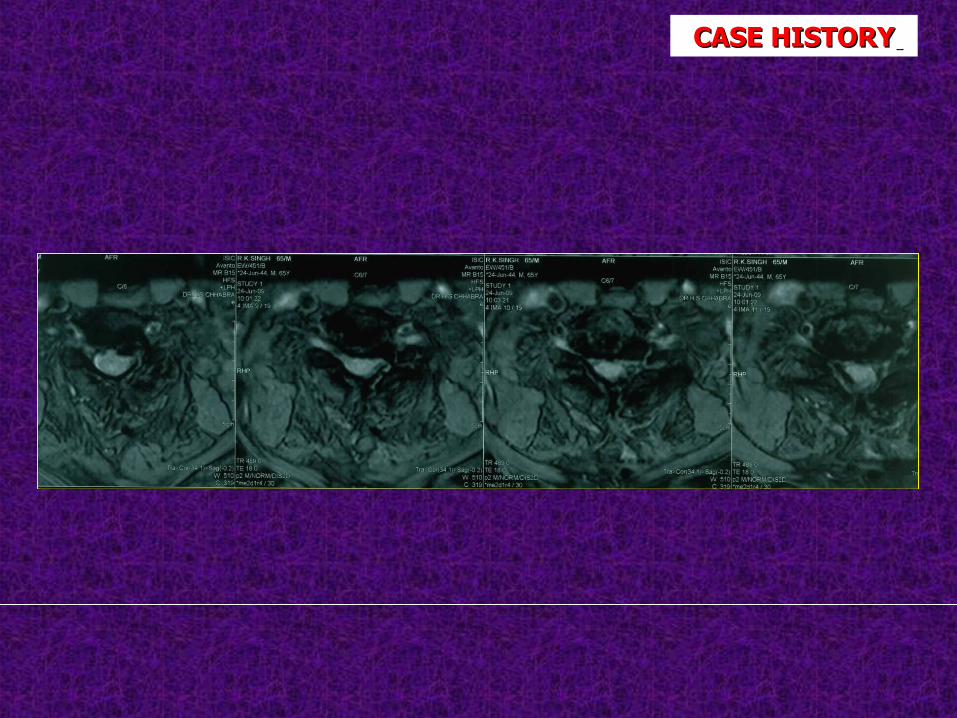
MRIMRI : C6 & C7 HAVE MALUNITED IN A DISPLACED POSITION : C6 & C7 HAVE MALUNITED IN A DISPLACED POSITION WITH SUBSEQUENT NEURAL COMPRESSIONWITH SUBSEQUENT NEURAL COMPRESSION
INVESTIGATIONSINVESTIGATIONS CASE HISTORYCASE HISTORY
CASE HISTORYCASE HISTORY
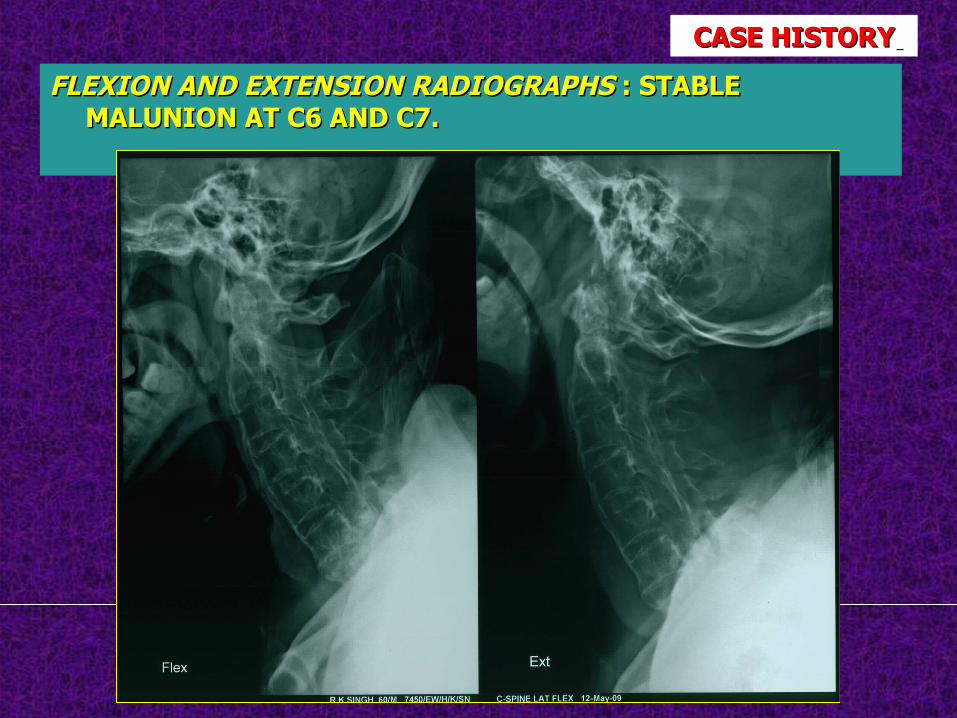
FLEXION AND EXTENSION RADIOGRAPHSFLEXION AND EXTENSION RADIOGRAPHS : STABLE : STABLE MALUNION AT C6 AND C7.MALUNION AT C6 AND C7.
CASE HISTORYCASE HISTORY
TREATMENTTREATMENT
Through anterior approach , C6 andThrough anterior approach , C6 and C7 corpectomy was done ,cordC7 corpectomy was done ,cord
decompressed , mesh cage with bonedecompressed , mesh cage with bone graft kept and stabilizationgraft kept and stabilization
done with cervical spine locking plate.done with cervical spine locking plate.
CASE HISTORYCASE HISTORY
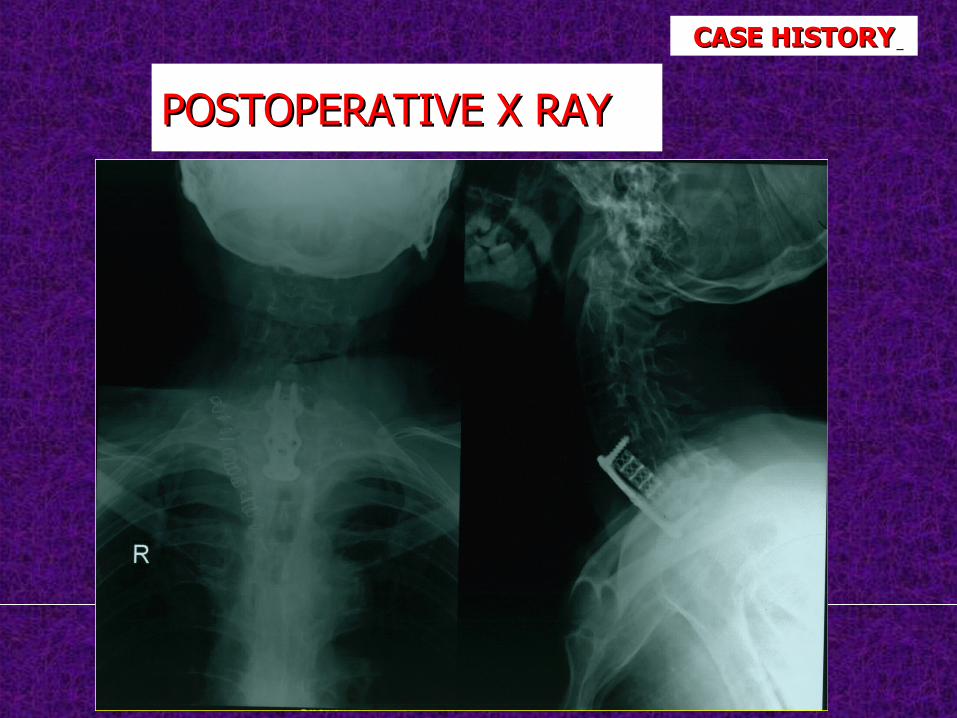
POSTOPERATIVEPOSTOPERATIVE X RAYX RAY
CASE HISTORYCASE HISTORY
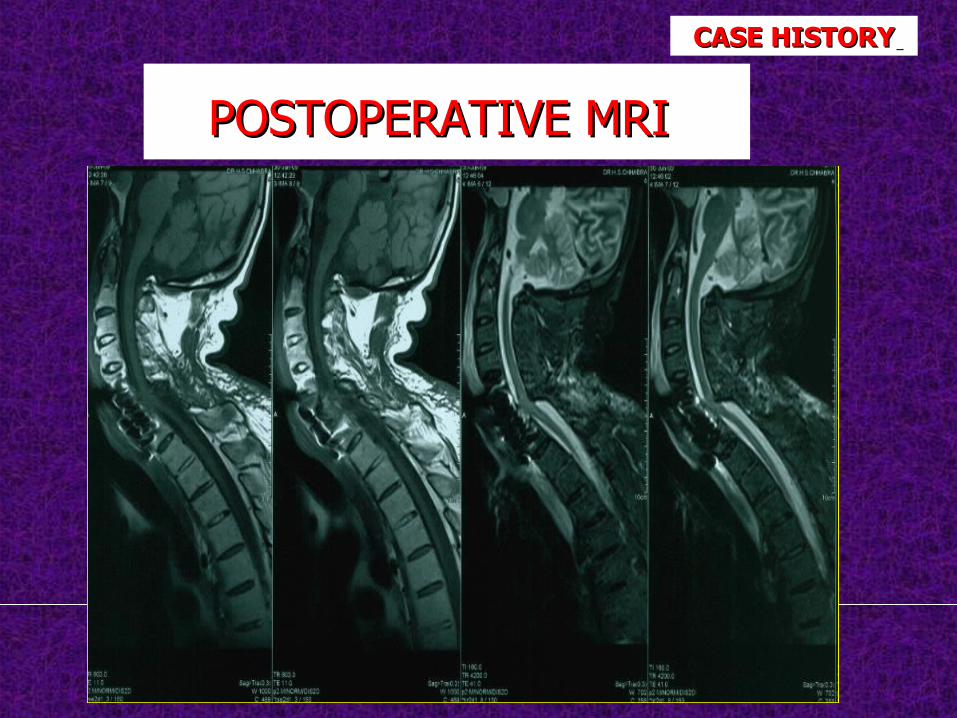
POSTOPERATIVE MRIPOSTOPERATIVE MRI
CASE HISTORYCASE HISTORY
POSTOPERATIVE STATUSPOSTOPERATIVE STATUS
• Postoperatively patient improved Postoperatively patient improved neurologically , had improved grip neurologically , had improved grip strength , and started walking with walker.strength , and started walking with walker.
• Comprehensive rehabilitation was started Comprehensive rehabilitation was started and patient was discharged after 15 days.and patient was discharged after 15 days.
CASE HISTORYCASE HISTORY
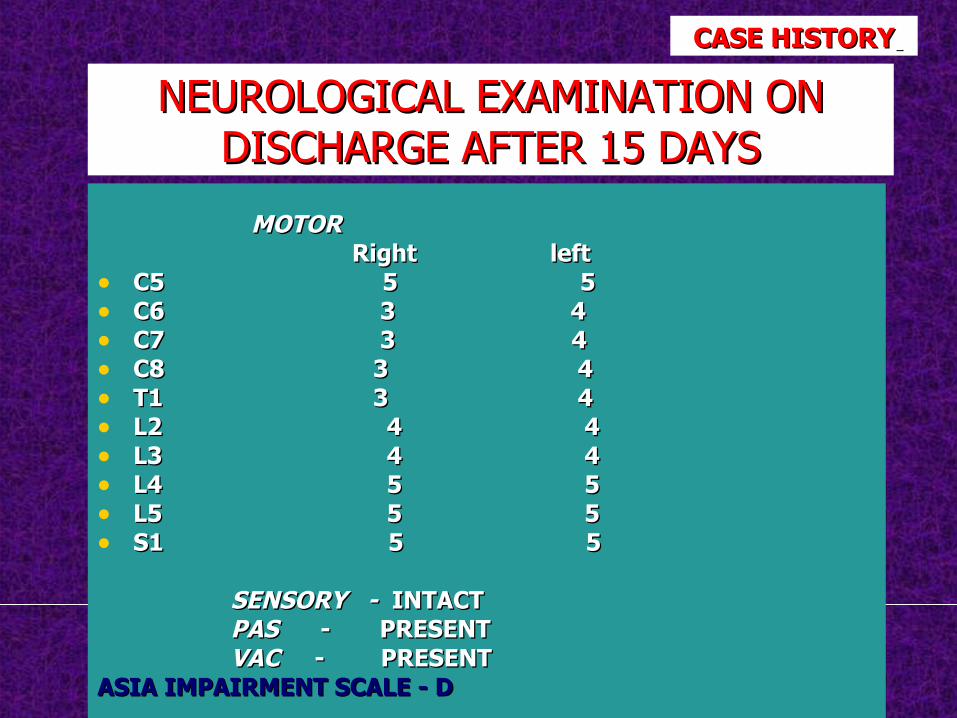
NEUROLOGICAL EXAMINATION ON NEUROLOGICAL EXAMINATION ON DISCHARGE AFTER 15 DAYSDISCHARGE AFTER 15 DAYS
MOTOR MOTOR Right leftRight left• C5 C5 5 5 5 5• C6C6 3 4 3 4• C7 C7 3 3 4 4• C8C8 3 4 3 4• T1T1 3 4 3 4• L2 4 4L2 4 4• L3 4 4L3 4 4• L4 5 5L4 5 5• L5 5 5L5 5 5• S1 5 5S1 5 5
SENSORY - SENSORY - INTACTINTACT PASPAS - PRESENT - PRESENT VACVAC - PRESENT - PRESENTASIA IMPAIRMENT SCALE - DASIA IMPAIRMENT SCALE - D
CASE HISTORYCASE HISTORY
On follow up at 2 months , patientOn follow up at 2 months , patient is walking with support and has is walking with support and has improved neurology.improved neurology.
CASE HISTORYCASE HISTORY

DISCUSSION
• There is a high incidence of spinal cord injury with fracture in patients with ankylosing spondylitis.
• This is due to higher instability of fractures. • This higher instability is due to due to long lever arms
formed due to fusion.
• There is high incidence of progressive neurological deficit after fractures, even improper transfers may increase the neurological deficit.
• In our case, an initially undisplaced fracture with no cord compression , was treated elsewhere with a laminectomy which led to further displacement and malunion in displaced position with subsequent cord compression.
• The patient presented with neurological deterioration .
• This sequence of events could have been avoided by a primary stabilization in the first instance.
• With subsequent decompression and stabilization, the patient improved neurologically
DISCUSSIONDISCUSSION
• Even trivial trauma causes fractures in patients with ankylosing spondylitis
• These fractures usually occur through the disc space as it is usually unossified.
• The best way to manage such patients is with early stabilization through either anterior or preferrably posterior multilevel stabilization.
DISCUSSIONDISCUSSION
CONCLUSIONCONCLUSION
• Spine fractures occur with minor trauma in Spine fractures occur with minor trauma in patients with ankylosing spondylitis .patients with ankylosing spondylitis .
• They are highly unstable with high They are highly unstable with high incidence of neurological deficit. incidence of neurological deficit.
• Appropriate early stabilization and Appropriate early stabilization and decompression is the best option in such decompression is the best option in such cases.cases.
• Laminectomy further destabilizes the Laminectomy further destabilizes the fracture and may lead to further fracture and may lead to further displacement and neurological deficits.displacement and neurological deficits.
• Laminectomy alone without stabilization is Laminectomy alone without stabilization is contraindicated in patients with fractures, contraindicated in patients with fractures, especially in patients with ankylosing especially in patients with ankylosing spondylitis.spondylitis.
CONCLUSIONCONCLUSION
REFERENCESREFERENCES
1.1. Michael Broom. Complications of fractures of cervical spine in Michael Broom. Complications of fractures of cervical spine in ankylosing spondylitis.Spine 1988, Volume 13, no. 7, 763-766.ankylosing spondylitis.Spine 1988, Volume 13, no. 7, 763-766.
1.1. Brent Graham. Fractures of the spine in ankylosing spondylitis.Spine Brent Graham. Fractures of the spine in ankylosing spondylitis.Spine 1989, Volume 14, no. 8, 803- 807.1989, Volume 14, no. 8, 803- 807.
1.1. Derek A Taggard. Management of cervical spinal fractures in Derek A Taggard. Management of cervical spinal fractures in ankylosing spondylitis with posterior fixation. Spine 2000, ankylosing spondylitis with posterior fixation. Spine 2000, Volume Volume 25, no. 16, 2035- 2039.25, no. 16, 2035- 2039.
44. Pradeep Thumbikaat. Spinal cord injury in patients with ankylosing . Pradeep Thumbikaat. Spinal cord injury in patients with ankylosing spondylitis.Spine 2007, volume 32 , no.26, 2989–2995.spondylitis.Spine 2007, volume 32 , no.26, 2989–2995.