A case of bilateral cleft of the face
5
A CASE OF BILATERAL CLEFT OF THE FACE By JOHN POTTER, F.R.C.S.Ed. Children's Department, Newcastle General Hospital INTRODUCTION THIS case is presented not only because it is an uncommon type of congenital facial defect, but also as it shows in much greater degree than bilateral hare lip the effects of absence of union between the central and lateral parts of the face. Keith (194 o) states that there is no case of cleft of the face at the Royal College of Surgeons, and refers to partial cleft faces recorded by Schwalbe. Herbst and Apfflestaedt (193o) show partial and unilateral cases, but not an identical case. Davis (1935) reviews I,OOO cases of congenital defects of the face, and illustrates one case similar to that here recorded. The relative incidence of the various congenital defects of the face is clearly shown in his paper. CASE REPORT William R., first seen at the age of i8 days, was the third child of healthy parents, the father being aged 35 years and the mother 29. There was no family history of deformity, and the previous children, both males, were normal. FIG. I FIG. 2 FIG. 3 Pre-operative. Aged 6 weeks. Pregnancy and delivery had been uneventful, and his weight at birth was 9-~- lb. Apart from the condition of the face and palate, to be described, the infant appeared healthy, and subsequent mental and physical development have been normal. The appearance of the face was made striking and repugnant by a bilateral cleft. On each side this extended from the medial end of the lower eyelid to the lateral side of the premaxilla. There was also complete cleft of the lip and alveolar margin, but this passed lateral to the nose, contrasting with the condition in hare lip, where the cleft passes into the floor of the nose. The central part of the face protruded at a level much higher than normal, the tip of the nose being on a level 209
-
Upload
john-potter -
Category
Documents
-
view
221 -
download
1
Transcript of A case of bilateral cleft of the face

A CASE OF BILATERAL CLEFT OF THE FACE
By JOHN POTTER, F.R.C.S.Ed. Children's Department, Newcastle General Hospital
INTRODUCTION
THIS case is presented not only because it is an uncommon type of congenital facial defect, but also as it shows in much greater degree than bilateral hare lip the effects of absence of union between the central and lateral parts of the face.
Keith (194 o) states that there is no case of cleft of the face at the Royal College of Surgeons, and refers to partial cleft faces recorded by Schwalbe. Herbst and Apfflestaedt (193o) show partial and unilateral cases, but not an identical case. Davis (1935) reviews I,OOO cases of congenital defects of the face, and illustrates one case similar to that here recorded. The relative incidence of the various congenital defects of the face is clearly shown in his paper.
CASE REPORT
William R., first seen at the age of i8 days, was the third child of healthy parents, the father being aged 35 years and the mother 29. There was no family history of deformity, and the previous children, both males, were normal.
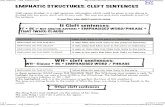
FIG. I FIG. 2 FIG. 3 Pre-operative. Aged 6 weeks.
Pregnancy and delivery had been uneventful, and his weight at birth was 9-~- lb.
Apart from the condition of the face and palate, to be described, the infant appeared healthy, and subsequent mental and physical development have been normal.
The appearance of the face was made striking and repugnant by a bilateral cleft. On each side this extended from the medial end of the lower eyelid to the lateral side of the premaxilla. There was also complete cleft of the lip and alveolar margin, but this passed lateral to the nose, contrasting with the condition in hare lip, where the cleft passes into the floor of the nose. The central part of the face protruded at a level much higher than normal, the tip of the nose being on a level
209

.210 B R I T I S H J O U R N A L OF P L A S T I C SURGERY
with the eyes. The nasal airways were normal, and have remained so. The nose was much shorter than usual. There was a complete bilateral cleft of the palate. The lacrimal system was grossly abnormal. The inner canthus of each eye was unformed, the caruncle and puncta being absent, and the upper lid was notched at the site usually occupied by the punctum. There was no lacrimal sac, and the nasolacrimal duct was represented by an open cleft covered by pink epithelium, heaped up at the edges. The eyes were normal and moved normally (Figs. i, 2 , and 3).
FIG. 4 FIG. 5 One year old.
Radiography of the skull was not undertaken ,at the time, but at the age of I8 months showed no abnormality.
T rea tmen t . - -The abnormalities having presumably been present from the second month of foetal life, early operation was deemed essential to repair the defect and allow normal muscle pull to have its effect in restoring the relationships .of the face to a semblance of normality.
I. The first operation was performed when the child was 6 weeks old (W. E. M . W . ) . The left cleft was repaired first. The edges of the cleft and .covering mucous membrane were excised, and sutured carefully, after wide undermining of the tissues. The hard palate was repaired at the same time, using the method described by Veau in " Division Palatine," suturing the mobilised hard palate flap to the vomerine mucosa flap.
2. The second operation was performed six weeks later (J. P.). The right cleft and hard palate were repaired by the same method as used on the left side. The cleft in the lip on the right side was repaired at the same time by a modified Blair-Brown-Miranlt repair, as described by Wardill (I943).
3. The cleft in the lip on the left side was repaired in a similar manner six weeks later (J. P.) (Figs. 4 and 5).
4. The cleft palate was repaired at the age of I2 months (J. P.), using a V-Y push-back repair and pharyngoplasty as described by Wardill (I937).
5. At the age of 2 years the lower eyelid, on each side, was freed up at its :inner end into normal position, and a small flap was rotated from the inner end o f the upper eyelid to fill the defect (J. P.). This removed the downward and inward direction of the inner ends of the eyelids, which had been present since birth.

B I L A T E R A L C L E F T O F T H E F A C E 2 1 1
Success so far achieved can be seen from the illustration (Figs. 6, 7, and 8). Though the nose remains a little higher than normal, the relationships of the central and lateral parts of the face have considerably improved--evidence of the moulding which can take place after clefts have been closed surgically. The premaxilla is in good position, the palatal cleft defect is closed, the soft palate is giving a good nasopharyngeal closure. Scope for further operation, to close the notches in the upper lids and improve the scars, remains, but this is being deferred until the child is older.
FIG. 6 FIG. 7 FIG. 8 Two years old.
DISCUSSION
The salient feature in the case described is lack of union of the central part o f the face with the lateral masses. On each side the cleft involves superficial parts of the soft tissues only at its upper end, deepening as it descends so as to involve the full thickness of the lip, and being complete in the alveolus and palate, illustrating the view expressed by Frazer (i94 o) : " It must be understood that the cleft is only present where the maxillary process applies itself, in its growth to the surfaces of the nasal folds. Further back it is never present, the maxillary mesoderm being applied directly to the paraxial mesoderm without any (temporary) intervention of ectoderm."
The absence of the moulding forces which normally pull down the central portion of the face has led to this part being placed at a level much higher than normal, and with an anterior and upward projection.
Any attempts to explain the mechanism of the defects must be based on normal development, and the diagrams from Frazer's " Embryology" are reproduced for convenience of reference (Figs. 9 and IO).
Keith (I948) states that embryological parts unite in a manner similar to wounds, and that the exact causes of arrest of union are unknown, but that if union fails to occur, the subsequent growth moves them farther apart.
The old explanation of the defect would have been failure of fusion of the parts, but if this were the cause one would expect the cleft to pass into the floor of the nose.
A possible cause is an interference with the circulation of the area of the clefts during the sixth to eighth week of foetal life, causing a local necrosis in the tissues. The mtiology of cleft formation is reviewed by Braithwaite and Watson (I949).

212 B R I T I S H JOURNAL OF P L A S T I C SURGERY
K
0 m m
B c
FIG. 9
• c . ~ ? -
' C ~ . J
FIG. IO

BILATERAL CLEFT OF THE FACE 213
T h e l a c r i m a l a p p a r a t u s in th is case is absen t . T h e pa s sages a re n o t t r u l y a b s e n t , b u t a r e on t h e s u r f a c e l i n e d b y m u c o u s m e m b r a n e . T h e n o r m a l p r o c e s s o f f o r m a t i o n o f t h e n a s o l a c r i m a l d u c t has fa i l ed to o c c u r ( M a n n , 1937).
I would like to thank Mr W. E. M. Wardill for his help in the early treatment of this case, the medical and nursing staff of the Children's Department, Newcastle General Hospital, and Messrs Bailli&e, Tindall & Cox for permission to publish the illustrations from Frazer' s " Embryology."
REFERENCES
BRAITHWAITE, F., and WATSON, J. (1949). Brit. `7. Plastic Surg., 2, 38. DAVIS, W. (1935). Surg. Gynec. Obstet., 6I, 2Ol. FRAZER, J. E. (194o). " Manual of Embryology." London : Bailli~re, Tindall & Cox. HERBST, E., and APFFLESXAEDT, M. (1930). " Malformations of the Jaws and Teeth." London :
Oxford University Press. KEITH, Sir ARTHUR (i94o). Brit. `7. Surg., 28, 173. - - (1948). " H u m a n Embryology and Morphology." Sixth Edition. London: Edward
Arnold & Co. MANN, IDA (I937). " Developmental Abnormalities of the Human Eye." Cambridge University
Press. SCHWALBE. Quoted by Sir Arthur Keith (194o). WARDILL, W. E. M. (1937). Brit..7. Surg., 25, 97- - - - - (1943). Section on Hare Lip and Cleft Palate in Grey Turner 's " Modern Operative Surgery."
London : Cassell & Co. Ltd.


















