Actuarial Study of Retiree Health Liabilities Under GASB 74/75

A Buck Consultants webinar
Gail Levenson and Rich Stover
April 11, 2013
Retiree prescription drug program: time to move to an Employer Group Waiver Plan (EGWP)?
April 11, 2013

A Buck Consultants webinar April 11, 2013
Today’s areas of focus
• Overview of Medicare Part D plan
• Impact of health care reform and Medicare changes on retiree prescription drug options
• Benefits of an EGWP
• Implementation considerations
Rich StoverPrincipal, H&P
Gail LevensonPrincipal, H&P
2

A Buck Consultants webinar
Employer retiree Rx options pre-health care reform
Retiree Drug Subsidy (RDS)
• Plan sponsor continues current prescription drug program
• Plan sponsor receives a subsidy for maintaining prescription drug benefits that is Actuarially Equivalent (AE) to standard Part D benefit
• RDS covers 20% to 25% of prescription drug cost
• “Double” tax benefit for corporate employers
Employer Group Waiver Plan (EGWP)
• Employer contracts with a vendor (usually a PBM) to provide benefits that can “match” the employer’s current plan design
• Eligible for “direct subsidy” instead of RDS
• Advantageous for plan that cannot satisfy AE requirements
• Governmentals can reflect under GASB
April 11, 2013
4

A Buck Consultants webinar
EGWP: how it works
Employer PBM CMS
• Employer contracts with PBM
• Contract can be either self-insured or fully-insured
• PBM implements employer’s plan design
• PBM receives financial subsidy from CMS
• PBM plan passes back all subsidies (in a self-insured plan) and charges administrative fee
• PBM assumes CMS compliance responsibilities
April 11, 2013
5

A Buck Consultants webinar
Value of RDS and EGWP pre-health care reform
$
Retiree
Drug Subsidy
EGWP Plan
April 11, 2013
6

A Buck Consultants webinar
Employer retiree Rx options post-health care reform
Retiree Drug Subsidy (RDS)
• RDS payments taxable starting in 2013
- Reduces real value of RDS to taxable groups
• Standard Part D benefit donut hole phased out by 2020
- No impact to actuarial equivalence testing
Employer Group Waiver Plan Plus Wrap (EGWP+Wrap)
• Standard Part D benefit donut hole phased out by 2020
- Additional federal funds available to EGWP
- Direct subsidy
- Catastrophic reinsurance
- 50% brand discount from drug manufacturers in coverage gap
April 11, 2013
7
A Buck Consultants webinar
Medicare Reinsurance 80%
Pla
n P
ays
15
%
5%
Co
ins
Plan Pays
21%79%
Coinsurance
50%
PharmaDiscount
Pla
n P
ays
2.5
%
47
.5%
Coin
sura
nce
Plan Pays 75%
25
%
Coin
sura
nce
$325 Deductible
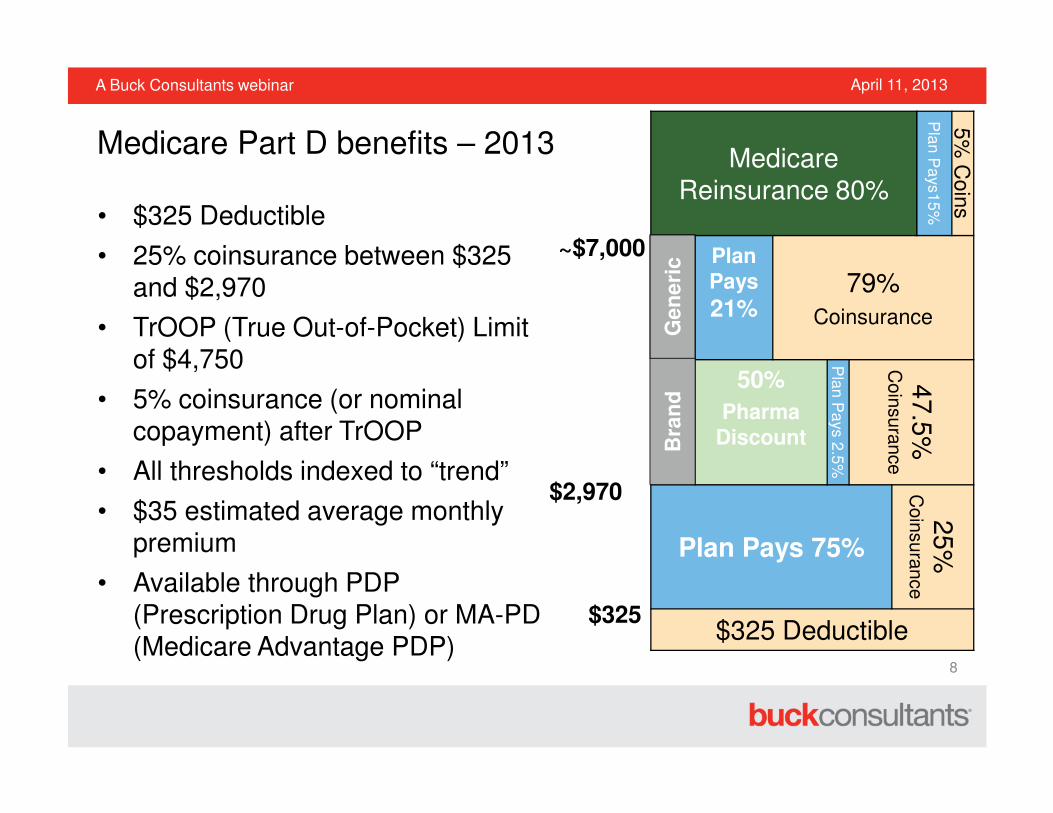
• $325 Deductible
• 25% coinsurance between $325 and $2,970
• TrOOP (True Out-of-Pocket) Limit of $4,750
• 5% coinsurance (or nominal copayment) after TrOOP
• All thresholds indexed to “trend”
• $35 estimated average monthly premium
• Available through PDP (Prescription Drug Plan) or MA-PD (Medicare Advantage PDP)
$325
$2,970
~$7,000
Ge
ne
ric
Bra
nd
Medicare Part D benefits – 2013
April 11, 2013
8

A Buck Consultants webinar
Medicare Part D benefit changes for 2014
2013 2014
Deductible $325 $310
Initial Coverage Limit $2,970 $2,850
True Out-of-Pocket (TrOOP) $4,750 $4,550
Catastrophic coverage copayment for generic drugs
$2.65 $2.55
Catastrophic coverage copayment for brand-name drugs
$6.60 $6.35
April 11, 2013
9

A Buck Consultants webinar
Donut Hole Coverage
• Expanded generic and brand coverage
- Donut hole filled in by 2020
• 50% discount on brand drugs
- Discount determined after any PDP provided gap coverage
- Pharmacy discounts and additional federal subsidies make EGWP more valuable relative to RDS
Year Generic Benefit Brand Benefit Brand Discount
2011 7% 0% 50%
2012 14% 0% 50%
2013 21% 2.5% 50%
2014 28% 2.5% 50%
2015 35% 5% 50%
2016 42% 5% 50%
2017 49% 10% 50%
2018 56% 15% 50%
2019 63% 20% 50%
2020 75% 25% 50%
Medicare Part D benefits – 2011 and beyond
April 11, 2013
10

A Buck Consultants webinar
Tax exclusion
eliminated in 2013
50% brand discount
Direct subsidy and catastrophicreinsurance
$
Retiree Drug Subsidy
EGWP+Wrap Plan
Health care reform changes value of RDS and EGWP
April 11, 2013
11

A Buck Consultants webinar
0
250
500
750
1000
1250
1500
1750
2000
DS, Catastrophic, Brand Discount
Direct Subsidy (DS)
RDS
• Average annual external financing amounts expected per enrollee
• EGWP+Wrap will enjoy federal direct subsidy, catastrophic reinsurance and manufacturer brand discounts
Source for RDS and Direct Subsidy:2010 Annual Report of the Board of Trustees ofthe Federal Hospital Insurance and FederalSupplemental Medical Insurance Trust Funds (8/5/2010)
Brand discount is estimated.
Projected Part D External Financing for EGWP+Wrap vs. RDS
April 11, 2013
12

A Buck Consultants webinar
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
20
09
20
10
20
11
20
12
20
13
20
14
20
15
20
16
20
17
20
18
20
19
PDP & MA-PD RDS
“About 20% of beneficiaries
participating in Part D were
covered by [the retiree drug]
subsidy in 2009…. As a result of
[healthcare reform] changes, RDS
program participation is assumed
to decline quickly to about 2% in
2016 and beyond.”
Source: 2010 Annual Report of the Board of Trustees ofthe Federal Hospital Insurance and Federal
Supplemental Medical Insurance Trust Funds (8/5/2010)
Medicare Trustees expect RDS participation to decline
April 11, 2013
13

A Buck Consultants webinar
• Employer contracts with a vendor (usually a PBM) to provide prescription drug benefits that can “match” the employer’s current plan design through two Rx plans:
- EGWP provides standard Part D benefits
- Wrap Plan fills in the gaps to keep retirees whole
• This approach leverages Pharma discounts and government subsidies
- Can take advantage of the closing of the Medicare Part D donut hole
• Member disruption is limited (but not zero as with RDS)
- One ID card for two Rx plans –single transaction coordination of benefits
Employer Group Waiver Plan Plus Wrap (EGWP+Wrap): alternative to RDS
April 11, 2013
14

A Buck Consultants webinar
• $200 cost for brand drug
• 20% coinsurance
Rx Payment Coverage
Current Plan
EGWPEGWP +
Wrap
Gross Cost $200 $200 $200
Base Plan Pays $160 $160 $5
Discount N/A $20 $100
Wrap Plan Pays N/A N/A $55
Retiree Pays $40 $20 $40
EGWP examples – Plan design (in donut hole)
April 11, 2013
15

A Buck Consultants webinar
Recent regulatory guidance
• CMS guidance on wrap
- Guidance issued in 2012 appeared to eliminate need for wrap
- Subsequent CMS guidance confirms wrap is still required
• ACA guidance has clarified the application of various ACA fees and taxes to EGWPs
- Transitional reinsurance fee
- Insurer fee
• Insured wrap programs may be subject to state regulations
April 11, 2013
16

A Buck Consultants webinar
Risk ScoreCMS provides greater reimbursement to EGWP plans covering sicker retirees
Size of LIS PopulationCMS provides greater reimbursement for low-income retirees. These funds passed to the retiree
Contribution StrategyWhat savings are shared with retirees through contributions. Particularly under a “capped” retiree medical plan
Generic UtilizationCMS reimbursement to EGWP is independent of changes in generic substitution rates
Cash FlowCMS reimbursement via EGWP is provided substantially sooner than RDS annual filers
Admin FeesEGWP fees may not be very competitive yet; consider RDS admin costs as an offset
Discounts and RebatesEGWP is a separate contract from your normal Rx benefit; watch for lost economies with the non-Medicare population.
FormularyAny difference in formulary restrictions between RDS plan and ‘replicated’ EGWP plan could impact savings
Volatility EGWP provides the ability to gain stability in yearly costs by insuring
Key variables in financial analysis
April 11, 2013
17

A Buck Consultants webinar
Are you a candidate for an EGWP?
• An employer participating in the RDS program
• A non-taxable entity
• A taxable entity with little or no tax liability
• An employer offering prescription drugs to Medicare-eligible retirees
• A plan sponsor with a drug plan that does not pass the actuarially equivalence test for RDS
• A government entity that wishes to reflect Medicare D impact in its GASB 43/45 accounting
• A post-65 retiree program with more than 100 eligible retirees and dependents
April 11, 2013
18

A Buck Consultants webinar
Implementation considerations
• Number of post-65 Medicare-eligible retirees and Medicare-eligible dependents
- Fully insured vs self insured
- Minimum number of lives vary by PBM
- There are several PBMs who will self insure a relatively small number of retirees (e.g., 250)
• Internal resources to support implementation
• Timing of implementation: preferably 6 months
April 11, 2013
19

A Buck Consultants webinar
Clinical
• Formulary
- CMS requires certain drugs to be covered and others to be excluded
- Brand drugs covered on the formulary are limited to eligible drugs by manufacturers who agreed to participate in the coverage gap discount program. This list is updated periodically by CMS.
- PBM can perform formulary disruption analysis
- Formal formulary exception process available to retirees for non-formulary drugs (can cover in wrap)
• Special programs (e.g., step therapy, prior authorization, dose optimization, etc.) may be impacted
- CMS has more stringent requirements on the management of medications for the Med D program
Implementation considerations
April 11, 2013
20

A Buck Consultants webinar
Plan design considerations
• No mandatory mail
- 90-day supply must be allowed at retail if a mail service benefit is offered
- May charge 3 copays for retail 90-day supply
• No mandatory generic
- No penalties allowed for dispensing brand when generic is available
• Catastrophic coverage
- Plan cannot exceed the CMS standard member cost-share limit of approximately 5%
- Benefit to both member and Plan as government reimburses 80% of the cost
April 11, 2013
21

A Buck Consultants webinar
How does the “Wrap” work?
• Covers drugs not included on the PBM’s Medicare Part D formulary
• Covers drugs excluded by Medicare, such as prescription drugs for cough and cold, erectile dysfunction , etc.
• Allows you to offer the same plan design available through your commercial plan, including copayments, coinsurance, and maximum out-of-pocket, if applicable
April 11, 2013
22

A Buck Consultants webinar
• Member Health Insurance Claim Number (HICN) required for eligibility
- Can be very difficult to gather HICNs
• Low income subsidies
- Provides premium and benefit assistance for low income participants
- Represents those up to 150% of the FPL
- Premium subsidies must be reimbursed directly to the individual within 45 days of receipt (on a monthly basis)
- Administrative challenge for most employers
• Benefit assistance happens at “point of service”
- Lower coinsurance/copays for low-income participants
- Plans reimbursed on an annual basis for the reduced costs to the participant
Employer administrative issues
April 11, 2013
23

A Buck Consultants webinar
Employer administrative issues (cont’d)
• High income penalties
- Individuals/couples making greater than $85,000/$170,000 pay higher premium for Medicare Part D coverage
- Determined by Social Security Administration (SSA) and happens directly through Social Security deductions
- Employer is not notified
- Employer can choose to reimburse retiree
• Late enrollment penalties
• Integrated deductibles/maximum out-of-pockets
- Will not work for EGWP plans
• Split Families
- EGWP and non-EGWP family members
- Each retiree must be provided separately
April 11, 2013
24

A Buck Consultants webinar
Member communications
• Integral part of a successful implementation
- Plethora of Medicare-required communication sent by PBM
- PBMs vary on what customization they will allow
- Customized employer communication recommended as other communication from government/PBM may be confusing and not applicable
- Recommend having comprehensive communication plan to coordinate between PBM-generated communication and employer-generated communication
April 11, 2013
25

A Buck Consultants webinar
• New Rx card/New “rules”
- Generally transparent and/or beneficial to retiree
• Late enrollment penalties and additional premium for high-income -disruptive
• Required communications to retirees
• Employer can not force retirees to enroll in EGWP– must allow them to opt out
• Medication Therapy Management Program (MTM)
- Auto-enroll required for those with certain conditions or drugs
- Participant can opt out
• Minor differences may exist in formulary, network, and therapeutic management
• Retiree confusion
Retiree issues
April 11, 2013
26

A Buck Consultants webinar
Case study
• Large self-funded employer
• Approximately 15,000 Medicare-eligible retirees
• Previously receiving RDS
• Implementation
- Implemented for 1/1/2013
- Started implementation in March 2012
• Savings
- Implemented Cash savings approximately $5 million over RDS
- The associated FAS Expense savings for 2012 were roughly $38 million
- Employer’s year-end 2011 APBO was reduced by $340 million due to the EGWP.
April 11, 2013
27

A Buck Consultants webinar
EGWP + Wrap Considerations
Pros:
• Economic savings expected with this approach
• Can account for now even if delay implementation to 2015
• Efficient approach to obtain federal Part D subsidies and the 50% brand discount
• Can replicate current level of Rx benefits
• No more RDS compliance
Cons:
• Can PBM administer almost seamlessly
• Communicating and implementing changes may be challenging
• Formulary control
• Restrictive generic not allowed
• Mandatory mail not allowed
• Caps on employer cost can limit employer savings
April 11, 2013
28

A Buck Consultants webinar
Next steps
• If you are considering moving to an EGWP
- Contact your Buck Account Executive to set up a call to discuss next steps
- Savings analysis
- EGWP 101 discussion
- Schedule a call with our EGWP experts
April 11, 2013
29

A Buck Consultants webinar
Join the conversation on Buck’s social media channelsblog.buckconsultants.com
linkedin.com/company/buck-consultants
twitter.com/buckconsultants
facebook.com/buckconsultants
www.buckconsultants.com