A. BALLOT INITIATIVESPropositions 52, 55 and 56 with a request that the materials be shared with...
27
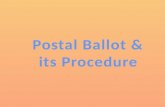
September 2, 2016 TO: Hospital Association of Southern California Board of Directors FROM: C. Duane Dauner, President/CEO SUBJECT: CHA REPORT A. BALLOT INITIATIVES The “real” political season runs from September 6 to November 8. Top on CHA’s priority list is Proposition 52, followed by Propositions 55 and 56. CHA is opposed to Proposition 53 (voter approval of revenue bonds) and Proposition 64 (legalization of marijuana). A report and request for action will be presented. Hospitals will be given information on Propositions 52, 55 and 56 with a request that the materials be shared with trustees, medical staff members, employees and volunteers. 1. Proposition 52: Medi-Cal Funding and Accountability Act of 2016 – Sponsor/Support CHA’s ballot initiative, the Medi-Cal Funding and Accountability Act of 2016 (Act), qualified for the November, 2016, General Election. It was the first initiative to qualify for the ballot and will appear as the second measure for consideration of long list of 17 statewide initiatives for the voters’ action. Proposition 52 removes the current statutory sunset date for the hospital fee program, thereby making the program and all of the statutory provisions permanent. Among the statutory provisions, this initiative would make permanent the limit on the amount the state can take for the General Fund, the construct of the fee program (both the fee side and the payment mechanisms), and the source of data and information used to develop the program, land of great importance – it prohibits the state from making any payment cuts to hospitals’ Medi-Cal rates. The Act allows for future changes by the Legislature with a two-thirds majority and only to further the purposes of the Act, including obtaining or maintaining federal approval. The Act will protect more than $4 billion ($3 billion to hospitals $1 billion to the state annually. Attached are two infographics that describe Proposition 52.
Transcript of A. BALLOT INITIATIVESPropositions 52, 55 and 56 with a request that the materials be shared with...

September 2, 2016
TO: Hospital Association of Southern California Board of Directors
FROM: C. Duane Dauner, President/CEO
SUBJECT: CHA REPORT
A. BALLOT INITIATIVES
The “real” political season runs from September 6 to November 8. Top on CHA’s priority list is
Proposition 52, followed by Propositions 55 and 56. CHA is opposed to Proposition 53 (voter
approval of revenue bonds) and Proposition 64 (legalization of marijuana).
A report and request for action will be presented. Hospitals will be given information on
Propositions 52, 55 and 56 with a request that the materials be shared with trustees, medical staff
members, employees and volunteers.
1. Proposition 52: Medi-Cal Funding and Accountability Act of 2016 –
Sponsor/Support
CHA’s ballot initiative, the Medi-Cal Funding and Accountability Act of 2016 (Act),
qualified for the November, 2016, General Election. It was the first initiative to qualify
for the ballot and will appear as the second measure for consideration of long list of 17
statewide initiatives for the voters’ action. Proposition 52 removes the current statutory
sunset date for the hospital fee program, thereby making the program and all of the
statutory provisions permanent.
Among the statutory provisions, this initiative would make permanent the limit on the
amount the state can take for the General Fund, the construct of the fee program (both the
fee side and the payment mechanisms), and the source of data and information used to
develop the program, land of great importance – it prohibits the state from making any
payment cuts to hospitals’ Medi-Cal rates. The Act allows for future changes by the
Legislature with a two-thirds majority and only to further the purposes of the Act,
including obtaining or maintaining federal approval. The Act will protect more than $4
billion ($3 billion to hospitals $1 billion to the state annually.
Attached are two infographics that describe Proposition 52.

HASC Board of Directors – CHA Report Page 2
September 2, 2016
2. Proposition 55: The California Children’s Education and Health Care Protection
Act of 2016 – Co-Sponsor/Support
CHA is a co-founder of a coalition to extend the Proposition 30 (2012) income tax
increases for 12 years, which are scheduled to expire on December 31, 2018. The
California Children’s Education and Health Care Protection Act of 2016 would raise and
estimated $5-$11 billion annually in tax revenues –dependent on the state’s economy.
The initiative calls for the majority of the funding to be directed to education (K-12 and
community colleges) according to the current Proposition 98 formula. The balance of the
funding includes allocations to the state’s Rainy Day Fund, the General Fund, and to the
Medi-Cal program for critical, emergency, acute and preventive healthcare services to
children and their families, provided by doctors and hospitals. More than $1 billion is
expected to be raised for hospitals and physicians, with a maximum of $2 billion in any
single year for Medi-Cal.
These new Medi-Cal funds would help reduce the amount of fees being paid by hospitals
in order to maximize federal funds.
Attached is an infographic that describes Proposition 55.
3. Proposition 56: California Healthcare, Research and Prevention Tobacco Tax Act of
2016 – Co-Sponsor/Support
CHA is a founding member of a coalition to reduce the consumption of tobacco products.
The coalition is sponsoring an initiative which increases the tax on tobacco and tobacco
products to an equivalent of $2 per pack including e-cigarettes and vaping devices.
Eighty-two percent of the funding from the initiative would be directed to the Department
of Health Care Services to increase funding for the Medi-Cal program. The balance of
the funding would be used for education, research, tobacco cessation programs and
graduate medical education. The initiative would raise $1.5 billion in new tax revenue.
B. PRIORITY ISSUES
1. Medicaid Managed Care Rule and the Hospital Fee
The Centers for Medicare & Medicaid Services (CMS) issued a final rule aimed at
modernizing the Medicaid and the Children’s Health Insurance Program (CHIP)
regulations to reflect changes in the usage of managed care delivery systems.
The final rule phases out the ability of states to use pass-through payments by allowing
states to direct managed care organization (MCO), pre-paid inpatient health plan (PIHP)
and pre-paid ambulatory health plan (PAHP) expenditures only based on the utilization,
delivery of services to enrollees covered under the contract, or the quality and outcomes
of services. However, because CMS recognizes that pass-through payments are often an

HASC Board of Directors – CHA Report Page 3
September 2, 2016
important revenue source for safety-net providers and some commenters requested a
delayed implementation of the provision at §438.6(c), the final rule will allow transition
periods for pass-through payments to hospitals, physicians and nursing facilities to enable
affected providers, states, and managed care plans to transition pass-through payments
into payments tied to services covered under the contract, value-based payment
structures, or delivery system reform initiatives without undermining access for the
beneficiaries they serve.
CHA is working with the Department of Health Care Services (DHCS) to find ways to
implement the new rule with as little disruption to the hospital fee program as possible.
There are still many unanswered questions about the meaning of parts of the rule. At a
very early indication, it appears that there are two potential pathways to implement the
changes needed. The first is to phase out the “pass-through” payments by ten percent per
year starting July 1, 2018. This would leave 90 percent of the funding “status quo” for
the first year of transition, then decreasing each year over the next ten years. The
managed care payments would continue to pass through the plans as they do now, but
would gradually phase this method out over ten years. A new method would need to be
developed for the phased out funding. A concern with leaving the legacy approach in
place is that we would be forced into a new calculation for measuring the size of the
funding pool, which is expected to limit the amount of money that would pass through.
A second option is to transition to a “directed payment” approach. The new rule allows
for DHCS to direct the plans to pay a flat amount (per day), just as the current program
does today. Two concerns with this method are that the days must be current as opposed
to historical, and the payments must be made to “network providers”. CHA and DHCS,
along with the hospital constituent groups, are working on possible solutions to these
potential issues. With this method, the calculation of the total funding is similar to the
current method and there would not be a significant variation in the size of the directed
payments from what has been experienced in the program to date.
There are many other issues and concerns that are being studied and solutions being
explored. As the discussions continue between CHA and DHCS we will keep hospitals
informed.
2. Health Care Workplace Violence
Cal/OSHA released a revised version of the proposed Healthcare Workplace Violence
Prevention Regulations on August 2. The 15-day comment period closed on August 17
and CHA submitted comprehensive comments. Thereafter, Cal/OSHA released a second
revised version of the proposed regulations. CHA will submit comments relating to the
most recent changes. The final proposed regulations will be considered by the
Cal/OSHA Standards Board at its October 20, 2016 meeting. Assuming the final version
is adopted at that time, the regulation would take effect on January 1, 2017. However,
the proposed regulations now have delayed implementation dates for most aspects,
including plan development, hazard identification and correction, training and reporting.

HASC Board of Directors – CHA Report Page 4
September 2, 2016
Given this time line, hospitals and health systems should begin the assessment and
planning process. To assist members, CHA and the Regional Associations are providing
regional roundtables to allow hospitals to share information about the challenges of
implementation efforts, as well as best practices. CHA also is developing a guidebook
that will be available once the regulations are final, and will host a webinar to review the
final regulations.
3. Physician Leadership Program
Due to the tremendous success of the inaugural California Physician Leadership Program,
CHA and the Regional Associations, will begin the second session on October 7, 2016.
We have exceeded our target of 30 physicians and have expanded the class to
accommodate additional participants.
This educational program was created to challenge and grow physician leaders, advance
hospital physician alignment and to assist in the transforming the healthcare delivery
system. We partnered with the USC Marshall School of Business to offer a balance of
academic faculty and industry experts and the program is tailored to the unique California
health care delivery system. The 14-day program takes place on a Friday and Saturday
from October to April, on the USC campus. Physicians can earn up to 105 AMA PRA
Category 1 Credits™ of CME awarded by the USC Keck School of Medicine.
It is not too late to enroll a physician in exclusive certificate program. For more
information, go to: www.calhospital.org/CA-physician-leadership.
C. FEDERAL REPORT -
1. Congressional Update
Congress adjourned for the summer recess from July 16 to September 6 and is in session
until early October. CHA’s advocacy efforts continue to be focused on securing clarity
and relief for the hospital outpatient department payment changes (site neutral) and will
join the American Hospital Association (AHA) Advocacy Day in Washington, DC on
September 13.
2. Regulatory Update
The last year of any administration is always packed. This year the Obama
administration has to put is mark on implementation of the Affordable Care Act (ACA).
The Department of Health & Human Services (HHS) has issued an onslaught of
additional regulations this summer, with more still on the HHS agenda slated to be
completed by the end of the year. Most significant is the implementation of additional
alternative payment models for hospitals, MACRA and revisions to the Medicare
Conditions of Participation. This activity coupled with the legislation around site neutral

HASC Board of Directors – CHA Report Page 5
September 2, 2016
payments has created opportunities for CHA to respond through the rulemaking process.
CHA encourages members to participate in CHA member forums to stay informed of the
changing landscape and how changes may impact your organization.
Announcements regarding CHA member forums and new regulations are featured daily
in CHA News. In addition, all current and pending regulations impacting hospitals and
post-acute care providers, including summaries, power point presentation and dates for
member forums are listed on our website at www.calhospital.org/regulatory-tracker.
Below is a summary of current regulatory activity impacting hospitals and post-acute care
providers.
(a) CY 2017 Outpatient Prospective Payment System Proposed Rule; Site Neutral
Payment Proposal
CMS issued its proposed rule on the calendar year (CY) 2017 outpatient
prospective payment system (OPPS). As expected, CMS proposed policies to
implement Section 603 of the Bipartisan Budget Act of 2015, which effects site
neutral payments for new off-campus provider-based hospital outpatient
departments under the Medicare program. A detailed summary of the proposed
rule is available at www.calhospital.org/cy2017-opps-proposed-summary.
That law requires that, with the exception of dedicated emergency department
services, services furnished in off-campus hospital outpatient departments
(HOPDs) that began billing under the OPPS on or after November 2, 2015 no
longer be paid under the OPPS; instead there would be no payment made directly
to the hospital by Medicare for CY 2017. In the proposed rule CMS proposes
that:
(i) Existing off-campus HOPDs that expand their services to include new
clinical families would now receive the lower site-neutral rate for those
services (the non-facility rate under the Medicare Physician Fee
Schedule);
(ii) Any existing off-campus HOPD that relocates after November 2 would
lose its excepted or “grandfathered” status and be subject to site-neutral
payments; and
(iii) Only if a hospital, in its entirety, has a change of ownership and the new
owners accept the existing Medicare provider agreement from the prior
owner, would the hospital’s off-campus HOPDs be able to maintain their
excepted status. Individual excepted off-campus HOPDs would not be
permitted to be transferred from one hospital to another and maintain their
excepted status.

HASC Board of Directors – CHA Report Page 6
September 2, 2016
CHA has concerns with the implementing policy included in the proposed rule
and is working with national stakeholders, including the AHA and federal
lawmakers, to safeguard appropriate payment and allow for expanded access to
community-based outpatient services. CHA held a member forum on the Section
603 provisions to solicit member input for our comments, which are due
September 6. www.calhospital.org/sites/main/files/file-
attachments/section_603_member_forum_presentation_final.pdf.
In addition, the proposed rule includes a number of other policies, including a
proposed update to OPPS rates, which CMS estimates will result in a 1.6 percent
payment increase for hospitals paid under the OPPS in CY 2017. CMS proposes
25 new comprehensive ambulatory payment classifications (C-APCs), many of
which are major surgery APCs within the various existing C-APC clinical
families. CMS also proposes refinements to its packaging policies as well as its
policies on device-intensive procedures.
The proposed rule also makes changes to quality and performance programs, as
well as changes to the Medicare EHR Incentive program for hospitals and critical
access hospitals (CAH).
(b) FFY 2017 Inpatient Prospective Payment System Final Rule
CMS issued its FFY 2017 inpatient prospective payment system final rule,
providing an annual rate update of 0.95 percent to hospitals paid under IPPS.
Among the other policies finalized in the rule, CMS addressed its proposals
related to the use of Worksheet S-10 in the methodology for distributing Medicare
disproportionate share hospital (DSH) uncompensated care payments and
implementation of the Notice of Observation Treatment and Implications for Care
Eligibility (NOTICE) Act of 2015, as described in more detail below.
CMS Does Not Finalize Use of S-10 Data in Medicare DSH Methodology
In response to advocacy by CHA and other stakeholders, CMS postponed its
proposal to incorporate Worksheet S-10 data into Factor 3 computing for FFY
2018 and is proceeding with revisions to the worksheet’s cost report instructions.
CMS notes in the final rule that it expects data from the revised Worksheet S-10
to be available for use in the near future, and no later than FFY 2021. When
computing Factor 3 in FFY 2018 and subsequent years, CMS intends to explore
whether an alternative proxy for uncompensated care could be used until it
determines that data from the revised Worksheet S-10 can be used for this
purpose. CMS had proposed a three-year transition, beginning in FFY 2018 with
a combination of Worksheet S-10 and proxy data, and ending in FFY 2020 when
only Worksheet S-10 data would have been used to compute the uncompensated
care payment amounts distributed.

HASC Board of Directors – CHA Report Page 7
September 2, 2016
CHA is pleased that CMS will postpone implementation of S-10 data in the DSH
methodology. In comments on the proposed rule and in a meeting with CMS
leadership, as well as HHS Secretary Burwell’s staff, CHA urged CMS not to
finalize its proposal and instead ensure the accuracy of the uncompensated care
data reported on Worksheet S-10 through a hospital-specific data audit. CHA
also urged the agency to revise the worksheet’s instructions and educate providers
and contractors on its use, to promote shared understanding and consistent
reporting.
(c) NOTICE Act Implementation and the Medicare Outpatient Observation Notice
(MOON)
The Office of Management and Budget (OMB) will accept comments on the
updated Medicare Outpatient Observation Notice (MOON) and instructions
through September 1, according to information now posted with the updated
MOON. The NOTICE Act requires hospitals and CAHs to provide written and
oral notification to Medicare beneficiaries receiving observation services as
outpatients for more than 24 hours. CHA hosted a member forum on August 23
to review and discuss CHA draft comments on the notice. A copy of that
presentation is on our website at http://www.calhospital.org/resource/cha-
member-forum-medicare-outpatient-observation-notice-moon. Under the final
rule, the notification requirements will take effect no later than 90 calendar days
after the updated MOON is approved by OMB. The MOON and instructions are
available at https://www.cms.gov/Regulations-and-
Guidance/Legislation/PaperworkReductionActof1995/PRA-Listing-Items/CMS-
10611.html.
The California state legislature passed a related piece of legislation SB 1076
Hernandez (D-Azusa), which requires notification of specified patients who are
on observation status. The bill would require hospitals to provide a written notice
to a patient on observation status and is being cared for in an inpatient unit of a
hospital or in an observation unit, or following a change in a patient’s status from
inpatient to observation, as soon as practicable. The notice shall state that while
on observation status, the patient’s care is being provided on an outpatient basis,
which may affect his or her health care coverage reimbursement. If enacted, the
provisions of SB 1076 would take effect January 1, 2017. CHA does not believe
as written that this legislation would conflict with the federal regulatory
requirements of the NOTICE Act as described above. SB1076 is on the
Governor’s desk.
(d) Proposed Bundled Payment Model for Cardiac Care, Updates to CJR
CMS issued a proposed rule that would implement a new mandatory episode-
based bundled payment model for cardiac care and expanding the current
Comprehensive Care for Joint Replacement (CJR) model to include surgical

HASC Board of Directors – CHA Report Page 8
September 2, 2016
treatments for hip and femur fractures beyond hip replacement. In addition, CMS
proposes to implement a new model to test incentive payments for cardiac
rehabilitation services.
Similar to the CJR model, the new episode-based payment models would hold the
hospital in which a Medicare fee-for-service (FFS) patient is admitted for a heart
attack; bypass surgery or surgical hip or femur fracture treatment accountable for
cost and quality for the inpatient stay and 90 days post-discharge. CMS proposes
that the first performance period for the models would be July 1, 2017, through
December 31, 2018.
CMS proposes to test the cardiac care model in 98 randomly selected
metropolitan statistical areas (MSAs). While CMS provides an analysis of which
MSAs are eligible to be selected, the agency does not plan to release the
selections until the final rule is issued. CMS has listed the following California
MSAs as included in the pool for possible random selection: Chico, Fresno, Los
Angeles-Long Beach-Anaheim, Modesto, Redding, Riverside-San Bernardino-
Ontario, Sacramento-Roseville-Arden Arcade, Salinas, San Diego-Carlsbad, San
Francisco-Oakland-Hayward, San Jose-Sunnyvale-Santa Clara, San Luis Obispo-
Paso Robles-Arroyo Grande, Santa Maria-Santa Barbara, Santa Rosa, Visalia-
Porterville and Yuba City. CMS proposes to test the hip and femur fracture
episodes in the same 67 MSAs as the CJR program. The current California MSAs
subject to the CJR program include Los Angeles-Long Beach-Anaheim, Modesto
and San Francisco-Oakland-Hayward.
As with previous bundled payment programs, all providers continue to receive
FFS payments during the model testing period. However, hospitals will be
provided a hospital-specific target price based on a blend of historical and
regional data for the episode of care, to be reconciled with actual spending at the
end of the performance year. Hospitals with spending under the target would be
eligible to receive the savings from Medicare, while those with spending over the
target price would be required to pay back Medicare. CMS proposes to phase in
implementation of risk, including no repayment for losses and a 5 percent cap on
gains in the first performance year. Hospitals also will be assessed on quality
measures; hospitals that provide higher quality care will be eligible for a greater
share of savings.
In addition, CMS proposes to test the impact of providing incentive payments for
cardiac rehabilitation and intensive cardiac rehabilitation services in the 90-day
period post-discharge. The cardiac rehabilitation incentive model would compare
the impact of the incentive in 45 MSAs selected for the cardiac episode-based
bundled payment models with 45 MSAs not selected to participate in the bundled
payment models. CMS would pay an initial payment of $25 per the first eleven
rehabilitation services, and $175 per service after the initial eleven, with limits on
sessions per Medicare coverage.

HASC Board of Directors – CHA Report Page 9
September 2, 2016
Finally, CMS proposes to provide new tracks for the CJR model and the proposed
cardiac episode-based bundled payment models that would allow partnering
physicians to qualify for advanced alternative payment model (APM) incentives
under the Medicare Access and CHIP Reauthorization Act. In addition, CMS
intends to build on the Bundled Payments for Care Improvement Initiative by
creating a new voluntary bundled payment model in 2018 that also would
potentially expand options for advanced APMs.
CHA will host a member forum to provide an overview of the proposed rule and
to solicit member input for comments, which are due October 3. The member
forum is scheduled for September 16 from 10-11:30 a.m. (PT). To register, visit
www.surveymonkey.com/r/cardiacbundle. A CHA summary highlighting key
provisions of the proposed rule, along with a more detailed summary prepared by
Health Policy Alternatives as well as additional resources is available at
www.calhospital.org/resource/episode-payment-model-resources is available at
www.calhospital.org/epm-proposed-summary.
CHA also encourages CJR providers to attend CHA’s Implementing CJR Seminar
– a hold a one-day intensive program on October 25 in Los Angeles to provide
health care teams with the knowledge needed to manage patient care, foster
physician alignment and develop effective partnerships with post-acute care
providers. To learn more, visit www.calhospital.org/implementing-cjr.
(e) CMS Issues Overall Star Ratings on Hospital Compare
CMS released its new hospital star ratings on the Hospital Compare website.
CMS states that these ratings reflect comprehensive quality information about
hospital care, summarizing 64 quality measures into a rating system of one to five
stars. However, CHA and hospital associations nationwide have opposed the
ratings system as it ignores social determinants of health, such as the hospital’s
community and patient income, unfairly penalizing teaching hospitals and those
serving higher numbers of the poor. The star ratings conflict with other rating and
ranking systems, causing confusion for patients and their families, and a recent
analysis by an independent expert found that the assumptions upon which the
current model is based are flawed. CHA, along with other state associations and
AHA, urged CMS to work with hospitals to validate the methodology or withhold
publication. CHA remains committed to sharing quality and safety information
and — through the Hospital Quality Institute — aims to accelerate the rate of
patient safety and quality care improvement for all Californians.
(f) Temporary Suspension of Two-Midnight Claims Review Update
Earlier this year, CMS announced a temporary suspension of reviews of claims
spanning less than two midnights by quality improvement organizations (QIOs),

HASC Board of Directors – CHA Report Page 10
September 2, 2016
with the intent to improve program standardization. CMS has now clarified the
instructions for medical review of claims affected by this suspension, and intends
to limit these reviews to a six-month look-back period from the date of admission.
CHA and other state hospital associations raised concerns that the delays in the
reviews were limiting hospitals’ ability to rebill a denied claim. In a recently
released FAQ, CMS states that Medicare FFS claims that are outside the six-
month look-back period will be paid under Part A, regardless of whether they
were formally denied. Claims that are outside the six-month look-back period,
but were not formally denied, also will be paid under Part A. Claims within the
six-month look-back period that were not formally denied will be reviewed when
CMS resumes QIO reviews. Those in the same time frame that were formally
denied are being re-reviewed by the QIO to determine whether the initial review
decision was consistent with the two-midnight policy in effect at the time of the
hospital admission. CHA remains concerned that, despite this change, the QIOs
are still challenged in meeting their deadlines for timely reviews. CHA is
currently reviewing this detailed guidance and seeks member input on the
operational concerns it may raise for hospitals. The FAQ is available at
http://qioprogram.org/review-claims-affected-temporary-suspension-bfcc-qio-
short-stay-reviews-faqs.
(g) Proposed Rule Updated Medicare Claims Appeal Process
HHS has issued a proposed rule that would make changes to the Medicare claims
appeal process. The changes are intended to address the backlog of appeals
currently pending at the Office of Medicare Hearings and Appeals. Among the
proposals is provision to permit the chair of the Departmental Appeals Board to
designate certain decisions as precedential. Additionally, to help address the
backlog of appeals, CMS proposes to permit attorney adjudicators to issue
decisions on appeals when the decision can be issued without an Administrative
Law Judge (ALJ) conducting a hearing under regulations. Other proposals include
clarifying the application of the Part 405 rules to other appeals processes
established in regulations, such as the Medicare Advantage program grievance
and appeals rules and Quality Improvement Organization reconsiderations and
appeals.
CHA commented on the proposed rule, expressing disappointment that the
proposed rule is limited in scope and lacks meaningful reforms that would
significantly impact the current backlog of 750,000 claims as of April 30. CHA
continues to support the Medicare Audit Improvement Act of 2015 (H.R. 2156),
which would meaningfully impact the current flow of claims coming through the
appeal process. CHA does not support the agency’s proposal for selecting
precedential decisions. Further, CHA opposes the agency’s proposal to eliminate
the 90-day deadline for issuing an administrative law judge decision, as CHA
believes the agency has significantly overreached its regulatory authority and that

HASC Board of Directors – CHA Report Page 11
September 2, 2016
the proposal is inconsistent with current law. CHA’s comments are available at
www.calhospital.org/cha-news-article/cha-comments-proposed-rule-updating-
medicare-claims-appeal-process.
(h) CMS Informational Bulletin on Medicaid Managed Care Pass-Through
Payments
CMS recently issued an informational bulletin to address questions regarding the
ability of states to increase or add new pass-through payments under Medicaid
managed care plan contracts and capitation rates, and to describe CMS’ plan for
monitoring the transition of pass-through payments to approaches for provider
payment under Medicaid managed care programs that are based on the delivery of
services, utilization, and the outcomes and quality of the delivered services. A
May final rule updating Medicaid managed care requirements provides for a 10-
year phase-out of these payments. The bulletin is available at
www.medicaid.gov/federal-policy-guidance/downloads/cib072916.pdf.
(i) FFY 2017 Medicare Payment System Final Rules
In addition to the FFY 2017 IPPS final rule, CMS finalized a number of other
prospective payment system (PPS) regulations for FFY 2017. Summaries of the
final rules will be posted to CHA’s federal regulatory tracker when available at
www.calhospital.org/publication/cha-regulatory-tracker. Below are links to each
of the final rules:
(i) FFY 2017 LTCH PPS Final Rule: http://www.calhospital.org/cha-news-
article/cms-issues-final-rule-updating-ltch-pps-ffy-2017
(ii) FFY 2017 IRF PPS Final Rule: http://www.calhospital.org/cha-news-
article/cms-issues-inpatient-rehabilitation-facility-pps-final-rule
(iii) FFY 2017 SNF PPS Final Rule: http://www.calhospital.org/cha-news-
article/cms-issues-skilled-nursing-facility-pps-final-rule
(iv) FFY 2017 Hospice Wage Index Final Rule:
http://www.calhospital.org/cha-news-article/cms-issues-hospice-final-rule
D. STATE REPORT
1. 2015-2016 Legislative Sessions
The Legislature completed its work on August 31 for the second year of the two-year
session, with the Senate and Assembly debating hundreds of proposals in the final week
of the session. The following report includes the final actions for the 2016 legislative
session. The focus of attention will now move to the actions of the Governor, who has

HASC Board of Directors – CHA Report Page 12
September 2, 2016
until midnight on October 2 to sign, veto or allow bills to become law without his
signature.
2. CHA Sponsored Legislation
AB 1300 (Assemblymember Sebastian Ridley-Thomas, D-Los Angeles) would specify
that trained emergency room physicians and psychiatric professionals in non-designated
hospitals, when probable cause exists, have the authority to write/initiate an up to 72-hour
involuntary hold. It also would codify that the 5150 application form is valid in all
counties regardless if it is an original or a copy; clarify that all designated facilities are
required to accept, within their clinical capability and capacity, all individuals for whom
it is designated; and authorize improved sharing of patient information when emergency
services are provided. AB 1300 remained in the Senate Rules Committee.
CHA Co-Sponsored SB 867 (Senator Richard Roth, D-Riverside) would extend the
operative date of the Maddy Emergency Services Fund to January 1, 2027, and authorize
each county to establish an emergency services fund for reimbursement of costs related to
emergency medical services. SB 867 was signed by the Governor on August 19 (Chapter
147).
3. CHA Opposed Legislation
Oppose, Unless Amended AB 1843 (Assemblymember Mark Stone, D-Scotts Valley)
would prohibit all California employers from soliciting or using any information related
to an applicant’s juvenile criminal history record, from arrests to adjudications. Recent
amendments would allow health facilities to obtain juvenile adjudication information
related to sex or drug-related crimes, but not all felonies. AB 1843 is awaiting action on
the Governor’s desk.
Opposed, Unless Amended AB 2272 (Assemblymember Tony Thurmond, D-Richmond)
would require Cal/OSHA to develop, by June 1, 2018, rules to regulate plume — noxious
airborne contaminants generated as byproducts from specific devices used during
surgical, diagnostic and therapeutic procedures — and the evacuation of plume when it is
generated in acute care hospitals. AB 2272 is awaiting action on the Governor’s desk.
AB 2467 (Assemblymember Jimmy Gomez, D-Los Angeles) would require private
nonprofit general acute care hospitals, acute psychiatric hospitals, private for-profit
general acute care hospitals, hospital groups and hospital-affiliated medical foundations
to annually submit an executive compensation report for every executive employee
whose annual compensation exceeds $250,000 per year. As amended in committee, the
measure would require the collection and reporting of ethnicity, race, gender, sexual
orientation and gender identity information. AB 2467 failed passage by the full Assembly
on June 2.

HASC Board of Directors – CHA Report Page 13
September 2, 2016
SB 503 (Senator Ed Hernandez, D-Azusa) would address deficiencies in current law
identified by a judge in a recent court decision for the treatment of unrepresented patients
who lack capacity to make medical decisions. The bill would allow skilled nursing
facilities (SNFs) to continue to obtain consent for the care of a patient by using an
interdisciplinary team process, if the SNF provides a specified written notice to the
patient. The bill also requires that, prior to administering an antipsychotic drug to a SNF
patient, the SNF convene a hearing with the patient, the ordering physician, an
independent physician, a patient advocate and an interpreter (if necessary) to review the
medication order. The independent physician and advocate must meet a list of
qualifications; the physician must also issue a written decision. The advocate also must
meet a list of qualifications. The patient may not be billed for the services of the
independent physician, advocate or interpreter. California Department of Public Health
(CDPH), the bill sponsor, decided not to move the bill forward this year. SB 503 was
held in the Assembly Health Committee.
SB 938 (Senator Hannah-Beth Jackson, D-Santa Barbara) would require a patient with a
major neurocognitive disorder who has a conservator to ask a court for judicial approval
each time a physician orders a new or different antidepressant, sleeping pill, anti-anxiety
medication, antipsychotic or other psychotherapeutic drug. While well intentioned, this
bill would jeopardize patients’ access to timely and appropriate medical care, clog the
court system and result in higher medical and legal costs for these patients and their
families. CHA is working with a coalition — including the Alzheimer’s Association and
California Psychiatric Association — to narrow the bill’s scope and provide protections
for hospitals. CHA issued an Advocacy Alert on SB 938 on August 18. CHA urged
hospital leaders to call their Assembly Members to request a “No” vote on SB 938.
SB 938 was referred to the Assembly Inactive File on August 29.
4. CHA Support Legislation
AB 1306 (Assemblymember Autumn Burke, D-Inglewood) as amended by the author, no
longer includes the corporate practice ban, which would have prohibited CNMs from
being employed by a corporation (such as a hospital) or other “artificial legal entity.”
CHA supports AB 1306’s premise — that California’s more than 1,200 CNMs should
have authority to practice to the full extent of their certification, education and training.
As advanced practice registered nurses, CNMs’ scope of practice allows them to provide
comprehensive management of women’s health care, focusing primarily on pregnancy,
childbirth and the postpartum period. Their scope of practice also includes care of the
newborn, family planning and other gynecological needs throughout the life cycle.
Would remove the physician supervision requirement, allowing CNMs greater
independence in meeting the health care needs of the millions of individuals added to
California’s health care system by the ACA, facilitating timely access to quality care AB
1306 failed passage by the full Assembly on August 31.
AB 1518 (Committee on Aging and Long-Term Care) would increase access to the home
and community-based Medi-Cal Nursing Facility/Acute Hospital Waiver by increasing

HASC Board of Directors – CHA Report Page 14
September 2, 2016
the number of authorized waiver slots and requiring an expedited authorization process
for patients in acute care hospitals who are awaiting discharge to a SNF. AB 1518 was
placed on the Senate Inactive file.
AB 1568 (Assemblymember Rob Bonta, D-Alameda) along with SB 815 (Senator Ed
Hernandez, D-Azusa), would implement California’s section 1115(a) demonstration
waiver, titled “California’s Medi-Cal 2020 Demonstration.” The waiver renewal –
effective December 30, 2015, through December 31, 2020 – includes $6.2 billion of
initial federal funding to support the state’s Medi-Cal program. The waiver implements
the following programs: Public Hospital Redesign and Incentives in Medi-Cal, Global
Payment Program, Dental Transformation Initiative and Whole Person Care Pilots. The
waiver also contains several independent analyses of the Medi-Cal program and
evaluations of the waiver programs, including an assessment of access in the Medi-Cal
managed care program and studies of uncompensated care in California hospitals. AB
1568 was signed by the Governor July 1 (Chapter 42).
AB 1607 (Assembly Budget Committee) would extend the hospital quality assurance fee
by one year, to January 1, 2018. AB 1607 was signed by the Governor June 27 (Chapter
27).
AB 2024 (Assemblymember Jim Wood, D-Healdsburg) would authorize a CAH to
employ physicians, surgeons and doctors of podiatric medicine and charge for
professional services rendered by those medical professionals if the medical staff
concurs, by an affirmative vote, that such employment is in the best interest of the
communities the hospital serves. It would prohibit the CAH from directing or interfering
with the professional judgment of a physician or surgeon. AB 2024 is awaiting action on
the Governor’s desk.
SB 66 (Senator Connie Leyva, D-Chino/Mike McGuire, D-Healdsburg) would require
the Department of Consumer Affairs to make available, upon request by the Office of the
Chancellor of the California Community Colleges, information on every licensee so that
the Office of the Chancellor can better measure employment outcomes of students who
participate in career technical education programs and make recommendations as to how
these programs may be improved. The bill also urges the Chancellor to align these
measures with the performance accountability measures of the federal Workforce
Innovation and Opportunity Act. SB 66 is awaiting action on the Governor’s desk.
SB 323 (Senator Ed Hernandez, D-Azusa) would allow nurse practitioners to practice to
the full extent of their education and training to ensure access to health care delivery
systems for millions of Californians who now have access to coverage under the ACA.
SB 323 was not heard in the Assembly Business and Professions Committee June 28.
SB 815 (Senator Ed Hernandez, D-Azusa), along with AB 1568 (Bonta, D-Alameda),
would implement California’s section 1115(a) demonstration waiver, titled “California’s
Medi-Cal 2020 Demonstration.” The waiver renewal – effective December 30, 2015

HASC Board of Directors – CHA Report Page 15
September 2, 2016
through December 31, 2020 – includes $6.2 billion of initial federal funding to support
the state’s Medi-Cal program. The waiver implements the following programs: Public
Hospital Redesign and Incentives in Medi-Cal, Global Payment Program, Dental
Transformation Initiative and Whole Person Care Pilots. The waiver also contains several
independent analyses of the Medi-Cal program and evaluations of the waiver programs,
including an assessment of access in the Medi-Cal managed care program and studies of
uncompensated care in California hospitals. SB 815 was signed by the Governor July 25
(Chapter 111).
SB 1177 (Senator Cathleen Galgiani, D-Stockton) would authorize the healing arts board
of the Department of Consumer Affairs’ Substance Abuse Coordination Committee to
establish a physician and surgeon health and wellness program for the early identification
and appropriate interventions to support a physician or surgeon in his or her rehabilitation
from substance abuse. SB 1177 is awaiting action on the Governor’s desk.
SB 1273 (Senator John Moorlach, R-Costa Mesa) would clarify that California counties
may use funds from the Mental Health Services Act to provide outpatient stabilization
services to individuals voluntarily receiving those services, even when those who are
receiving services involuntarily are treated at the same facility. The Department of Health
Care Services (DHCS) issued a memo on July 20, 2016, which clarified and supported
the bill’s intention. SB 1273 was referred to the Assembly Inactive File on August 29.
5. Follow, Hot Legislation
AB 72 Assemblymember Rob Bonta, D-Alameda /Assemblymember Susan Bonilla, D-
Concord/Assemblymember Brian Dahle, R-Bieber/Assemblymember
Gonzalez/Assemblymember Brian Maienschein, R-San Diego/Assemblymember Jim
Wood, D-Healdsburg) addresses surprise billing for covered services at a contracting
health facility from a non-contracting individual health professional. AB 72 is similar to
AB 533 (Bonta, D-Alameda). This bill would require health plans to reimburse the non-
contracting health professional the greater of the average contracted rate or 125 percent
of the amount Medicare reimburses on a FFS basis for the same or similar services in the
general geographic region in which the services were rendered. Recent amendments to
the bill have placed obligations on health plans when reporting average contract rates and
maintaining network adequacy requirements. AB 72 is the new version of AB 533. AB
72 is awaiting action on the Governor’s desk.
AB 508 (Assemblymember Christina Garcia, D-Bell Gardens) would have established
the California Maternal Quality Care Collaborative (CMQCC) within CDPH. The bill has
been amended to require CDPH to prepare and submit to the Legislature an annual report
on maternal mortality and morbidity in California, including an analysis of maternal
deaths and severe maternal morbidity. The bill also would require CDPH to consider
existing resources, including opportunities for partnerships with other entities and the use
of physician volunteers. AB 508 was held in the Senate Judiciary Committee.

HASC Board of Directors – CHA Report Page 16
September 2, 2016
AB 533 (Assemblymember Rob Bonta, D-Alameda) attempts to address “surprise
billing” by out-of-network providers. The introduced version of the bill contained
ambiguities that could have been interpreted to impose obligations on network hospitals
to provide information they do not have and/or cannot obtain for noncontracted
physicians. Amended April 15 for clarification, the bill would apply only to
noncontracting individual health professionals, not to hospitals. AB 533 was placed on
the Assembly Inactive file August 31.
AB 1978 (Assemblymember Lorena Gonzalez, D-San Diego) would require Cal/OSHA
to develop a standard for workplace violence for janitorial workers as well as four-hour
training for any supervisor of janitorial workers. Would also create a registry for
janitorial contractors. AB 1978 is awaiting action on the Governor’s desk.
AB 2424 (Assemblymember Jimmy Gomez, D-Los Angeles) would create the
Community-based Health Improvement and Innovation Fund within the state treasury. A
target level of annual statewide investment from the fund would be established as a set
dollar amount per capita, to be allocated to the CDPH to support community-based
prevention of priority chronic health conditions throughout the state, including in the
form of competitive grants. AB 2424 was held on Suspense in the Senate Appropriations
Committee August 11.
AB 2439 (Assemblymember Adrin Nazarian, D-Sherman Oaks) would create a CDPH
pilot program to select four or fewer hospital emergency departments to offer HIV tests
to patients. CHA originally opposed the bill as an unfunded mandate and inappropriate
setting to conduct HIV tests, but removed opposition with amendments that made
hospital participation in the pilot program voluntary. AB 2439 is awaiting action on the
Governor’s desk.
AB 2640 (Assemblymember Mike Gipson, D-Carson) would add to the significant body
of existing laws on HIV testing and would require every medical provider who orders an
HIV test to provide information to specified patients about methods that prevent or
reduce the risk of contracting HIV, including pre-exposure prophylaxis and post-
exposure prophylaxis, consistent with guidance of the federal Centers for Disease Control
and Prevention.” CHA opposed this bill on the grounds that it codifies the practice of
medicine into law; however, an agreement was reached with the author to ensure
physician discretion is preserved. Recent amendments address CHA’s concerns. Our
position on AB 2640 is Neutral As, Amended. AB 2640 is awaiting action on the
Governor’s desk.
SB 586 (Senator Ed Hernandez, D-Azusa) would authorize DHCS, no sooner than July 1,
2017, to establish a Whole Child Model program, under which managed care plans
served by a county organized health system or regional health authority in designated
counties would provide California Children’s Services (CCS) services under a capitated
payment model to Medi-Cal eligible CCS children and youth. SB 586 extends the sunset
date on the CCS “carve out” to January 1, 2022, and until the evaluation required under

HASC Board of Directors – CHA Report Page 17
September 2, 2016
the Whole Child Model program has been completed. SB 586 is awaiting action on the
Governor’s desk.
SB 1065 (Senator William Monning, D-Carmel) would require the court of appeal, in an
appeal of an order dismissing or denying a petition to compel arbitration involving a
claim under the Elder and Dependent Adult Civil Protection Act in which a party has
been granted a court preference, to issue its decision no later than 100 days after the
notice of appeal is filed, except as specified. Would also require the Judicial Council to
adopt rules implementing this provision and shortening the time within which a party
may file a notice of appeal in these cases. We have taken a Neutral position on SB 1065.
SB 1065 is awaiting action on the Governor’s desk.
Neutral as Amended, SB 1076 (Senator Ed Hernandez, D-Azusa) would create the
regulatory structure for hospitals wishing to provide observation services in a dedicated
unit. The bill states that observation patients may also be cared for in an inpatient unit or
in the emergency department. The observation unit must maintain the same nurse staffing
ratios as the emergency department. The bill clarifies that observation services are
triggered by a physician order, rather than potentially applying to all outpatient services.
The bill also requires patient notification when the patient is moved to observation status.
SB 1076 is awaiting action on the Governor’s desk.
SB 1195 (Senator Jerry Hill, D-San Mateo) provides requirements and procedures for the
Director of Consumer Affairs to review a decision or other action by a board under the
Department about a restraint of trade. Among other things, would prohibit the Board of
Nursing executive director from being a licensee of the board. SB 1195 was placed on the
Senate Inactive File on June 2.
SB 1365 (Senator Ed Hernandez, D-Azusa) would require a hospital that offers a service
in a hospital-based outpatient clinic to provide a notice to each patient when that service
is available in a non-hospital-based location. CHA took a Neutral position on that bill.
SB 1365 is awaiting action on the Governor’s desk.
Attached is a copy of the Key State Issues, dated September 2, 2016. It reflects final action by
the Legislature. Several bills are on the Governor’s desk awaiting action.
The 2017 session was highly successful. A report will be presented during the meeting.
CDD:rf
Attachments


PROPOSITION 52
6.7 Million Children
$3 Billion Federal Government (CMS)
$1 Billion State General Fund
$4 Billion Hospital Fee Payments to State
$6 Billion $3 Billion - Hospitals; $3 Billion - CMS
● Hospitals contribute money; state retains ¼
4.5 Million Low Income Working Families
● Federal government matches ¾ of contributions
● Politicians can’t divert the funds without a vote of the people
● No cost to consumers ● No new taxes
● Universally supported (Labor, business, Democratic and Republican parties, health care providers, elected officials – 1,000 in all
● Proven since 2009
WHAT MAKES PROPOSITION 52 WORK?
YES ON 52
1.8 Million Seniors
Hospital Services for
TESTED●TRIED●TRUE


Bill No. Author Location/Action CHA Position Staff Contact
Civil Actions
SB 1065 Monning
(D-Carmel)
Would require the court of appeal, in an appeal of an
order dismissing or denying a petition to compel
arbitration involving a claim under the Elder and
Dependent Adult Civil Protection Act in which a party
has been granted a court preference, to issue its
decision no later than 100 days after the notice of
appeal is filed, except as specified. Would also require
the Judicial Council to adopt rules implementing this
provision and shortening the time within which a party
may file a notice of appeal in these cases.
Awaiting action on the
Governor’s desk.
Neutral Jackie Garman/
Connie Delgado
Disaster Preparedness
AB 1562 Kim
(R-Fullerton)
Would provide a one-day window to purchase disaster
preparedness supplies without paying sales tax, giving
hospitals and medical centers the opportunity to
purchase a variety of items — such as evacuation
equipment, communications equipment and medical
supplies — with a tax break. The one-day sales tax
would also assist businesses in encouraging individual
and family preparedness among their employees,
which is foundational to organizational preparedness.
Additionally, this measure was amended to add a
sunset date of 2018 and would apply only to state
taxes.
Held on Suspense in
Assembly
Appropriations
Committee May 27.
Support Cheri Hummel/
Kathryn Scott
Emergency Services
SB 867 Roth
(D-Riverside)
Would extend the operative date of the Maddy
Emergency Services Fund to Jan. 1, 2027, and
authorize each county to establish an emergency
services fund for reimbursement of costs related to
emergency medical services.
Signed by the
Governor Aug. 19
(Chapter 147).
Co-sponsor BJ Bartleson/
Connie Delgado
AB 1774 Bonilla
(D-Concord)
Would repeal the laws requiring a clinical laboratory to
be licensed and inspected by CDPH, including the
licensing fee. Would also make other conforming
changes.
Held on Suspense in
Assembly
Appropriations
Committee May 27.
Support Cathy Martin/
Alex Hawthorne
AB 1843 Stone
(D-Scotts Valley)
Would prohibit all California employers from soliciting
or using any information related to an applicant’s
juvenile criminal history record, from arrests to
adjudications. Recent amendments would allow health
facilities to obtain juvenile adjudication information
related to sex or drug-related crimes, but not all
felonies.
Awaiting action on the
Governor’s desk.
Oppose,
Unless
Amended
Kathryn Scott/
Gail Blanchard-
Saiger
On Aug. 31, the Legislature completed the second year of its two-year session. This
report includes the final actions for the 2016 legislative session. Attention will now
focus on the Governor, who has until midnight on Sept. 30 to sign or veto bills, or
allow bills to become law without his signature. For an online version of this report
that can be filtered by topic and is updated daily, visit www.calhospital.org/key-state-
issues.
September 2, 2016
Health Facilities

California Hospital Association Key State Issues
Bill No. Author Location/Action CHA Position Staff Contact
AB 2743 Eggman
(D-Stockton)
Would require the California Department of Public
Health to establish and administer a pilot program to
create a website-based acute psychiatric bed registry
to collect, aggregate and display information about the
availability of acute psychiatric beds in psychiatric
health facilities in 10 counties.
Held on Suspense in
Assembly
Appropriations
Committee May 27.
Oppose Sheree Lowe/
Alex Hawthorne
SB 1076 Hernandez
(D-Azusa)
Would create the regulatory structure for hospitals
wishing to provide observation services in a dedicated
unit. The bill states that observation patients may also
be cared for in an inpatient unit or in the ED. The
observation unit must maintain the same nurse
staffing ratios as the ED. The bill clarifies that
observation services are triggered by a physician
order, rather than potentially applying to all outpatient
services. The bill also requires patient notification
when the patient is moved to observation status.
Awaiting action on the
Governor’s desk.
Neutral, As
Amended
Debby Rogers/
Connie Delgado
Labor
AB 1978 Gonzalez
(D-San Diego)
Would require Cal/OSHA to develop a standard for
workplace violence for janitorial workers as well as
four-hour training for any supervisor of janitorial
workers. Would also create a registry for janitorial
contractors.
Awaiting action on the
Governor’s desk.
Follow, Hot Gail Blanchard-
Saiger/ Kathryn
Scott
AB 2272 Thurmond
(D-Richmond)
Would require Cal/OSHA to develop, by June 1, 2018,
rules to regulate plume — noxious airborne
contaminants generated as byproducts from specific
devices used during surgical, diagnostic and
therapeutic procedures — and the evacuation of
plume when generated in acute care hospitals.
Awaiting action on the
Governor’s desk.
Oppose,
Unless
Amended
Gail Blanchard-
Saiger/ Kathryn
Scott
AB 2467 Gomez
(D-Los Angeles)
Would require private nonprofit general acute care
hospitals, acute psychiatric hospitals, private for-profit
general acute care hospitals, hospital groups and
hospital-affiliated medical foundations to annually
submit an executive compensation report for every
executive employee whose annual compensation
exceeds $250,000 per year. As amended in
committee, the measure would require the collection
and reporting of ethnicity, race, gender, sexual
orientation and gender identity information.
Failed passage on
Assembly Floor June 2.
Oppose Gail Blanchard-
Saiger/ Kathryn
Scott
SB 878 Leyva
(D-Chino)
Would require employers operating retail
establishments or restaurants, including cafeterias, to
provide at least seven days' notice of an employee’s
work schedule and further require additional pay to
employees when the employer alters that schedule
within the seven-day period.
Held on Suspense in
Senate Appropriations
Committee May 27.
Follow, Hot Gail Blanchard-
Saiger/ Kathryn
Scott
Health Facilities (continued)
Page 2

California Hospital Association Key State Issues
Bill No. Author Location/Action CHA Position Staff Contact
Managed Health Care
AB 72 Bonta
(D-Alameda)
Addresses surprise billing for covered services at a
contracting health facility from a noncontracting
individual health professional. AB 72 is similar to AB
533 (Bonta, D-Alameda). This bill would require health
plans to reimburse the noncontracting health
professional the greater of either the average
contracted rate or 125 percent of the amount Medicare
reimburses on a fee-for-service basis for the same or
similar services in the general geographic region in
which the services were rendered. AB 72 is the new
version of AB 533.
Awaiting action on the
Governor’s desk.
Neutral Deepa Prasad/
Alex Hawthorne
AB 533 Bonta
(D-Alameda)
Attempts to address “surprise billing” by out-of-network
providers. The introduced version of the bill contained
ambiguities that could have been interpreted to
impose obligations on network hospitals to provide
information they do not have and/or cannot obtain for
noncontracted physicians. Amended April 15 for
clarification, the bill would apply only to noncontracting
individual health professionals, not to hospitals.
Placed on Assembly
Inactive file Aug. 31.
Neutral, As
Amended
Deepa Prasad/
Alex Hawthorne
SB 932 Hernandez
(D-Azusa)
Would prohibit numerous provisions in contracts
between hospitals and health plans, as well as expand
the authority of the Department of Managed Health
Care to approve any merger, consolidation, acquisition
or purchase of control, directly or indirectly, between
any entity and any health care service plan.
Held on Suspense in
Senate Appropriations
Committee May 27.
Oppose Deepa Prasad/
Alex Hawthorne
Medi-Cal
AB 1568 Bonta
(D-Alameda)
Along with SB 815 (Hernandez, D-Azusa), would
implement California’s section 1115(a) demonstration
waiver, titled “California’s Medi-Cal 2020
Demonstration.” The waiver renewal – effective Dec.
30, 2015 through Dec. 31, 2020 – includes $6.2 billion
of initial federal funding to support the state’s Medi-Cal
program. The waiver implements the following
programs: Public Hospital Redesign and Incentives in
Medi-Cal, Global Payment Program, Dental
Transformation Initiative and Whole Person Care
Pilots. The waiver also contains several independent
analyses of the Medi-Cal program and evaluations of
the waiver programs, including an assessment of
access in the Medi-Cal managed care program and
studies of uncompensated care in California hospitals.
Signed by the
Governor July 1
(Chapter 42).
Support Anne McLeod/
Barbara Glaser
AB 1607 Assembly Budget
Committee
Would extend the hospital quality assurance fee by
one year, to Jan. 1, 2018.
Signed by the
Governor June 27
(Chapter 27).
Support Anne McLeod/
Barbara Glaser
SB 586 Hernandez
(D-Azusa)
Would authorize DHCS, no sooner than July 1, 2017,
to establish a Whole Child Model program, under
which managed care plans served by a county
organized health system or regional health authority in
designated counties would provide California
Children’s Services (CCS) services under a capitated
payment model to Medi-Cal eligible CCS children and
youth. SB 586 extends the sunset date on the CCS
“carve out” to January 1, 2022, and until the evaluation
required under the Whole Child Model program has
been completed.
Awaiting action on the
Governor’s desk.
Follow, Hot Amber Kemp/
Barbara Glaser
Page 3

California Hospital Association Key State Issues
Bill No. Author Location/Action CHA Position Staff Contact
Medi-Cal (continued)
SB 815 Hernandez
(D-Azusa)
Along with AB 1568 (Bonta, D-Alameda), would
implement California’s section 1115(a) demonstration
waiver, titled “California’s Medi-Cal 2020
Demonstration.” The waiver renewal – effective Dec.
30, 2015 through Dec. 31, 2020 – includes $6.2 billion
of initial federal funding to support the state’s Medi-Cal
program. The waiver implements the following
programs: Public Hospital Redesign and Incentives in
Medi-Cal, Global Payment Program, Dental
Transformation Initiative and Whole Person Care
Pilots. The waiver also contains several independent
analyses of the Medi-Cal program and evaluations of
the waiver programs, including an assessment of
access in the Medi-Cal managed care program and
studies of uncompensated care in California hospitals.
Signed by the
Governor July 25
(Chapter 111).
Support Anne McLeod/
Barbara Glaser
Medical Staff
AB 2024 Wood
(D-Healdsburg)
Would authorize a critical access hospital to employ
physicians, surgeons and doctors of podiatric
medicine and charge for professional services
rendered by those medical professionals if the medical
staff concurs, by an affirmative vote, that such
employment is in the best interest of the communities
the hospital serves. It would prohibit the critical access
hospital from directing or interfering with the
professional judgment of a physician or surgeon.
Awaiting action on the
Governor’s desk.
Support Peggy Wheeler/
David Perrott/
Barbara Glaser
SB 1177 Galgiani
(D-Stockton)
Would authorize the healing arts board of the
Department of Consumer Affairs’ Substance Abuse
Coordination Committee to establish a physician and
surgeon health and wellness program for the early
identification and appropriate interventions to support
a physician or surgeon in his or her rehabilitation from
substance abuse.
Awaiting action on the
Governor’s desk.
Support David Perrott/
Connie Delgado
Mental Health
AB 1300 Ridley-Thomas
(D-Los Angeles)
Would specify that trained emergency room
physicians and psychiatric professionals in non-
designated hospitals, when probable cause exists,
have the authority to write/initiate an up to 72-hour
involuntary hold. It would also codify that the 5150
application form is valid in all counties regardless if it is
an original or a copy; clarify that all designated
facilities are required to accept, within their clinical
capability and capacity, all individuals for whom it is
designated; and authorize improved sharing of patient
information when emergency services are provided.
AB 1300 passed the Senate Health Committee June
29 and was referred to Senate Rules Committee. It
will most likely remain in Senate Rules Committee.
Referred to Senate
Rules Committee.
Sponsor Sheree Lowe/
Barbara Glaser
Page 4

California Hospital Association Key State Issues
Bill No. Author Location/Action CHA Position Staff Contact
Mental Health (continued)
SB 938 Jackson
(D-Santa
Barbara)
Would require a patient with a major neurocognitive
disorder who has a conservator to ask a court for
judicial approval each time a physician orders a new
or different antidepressant, sleeping pill, anti-anxiety
medication, antipsychotic or other psychotherapeutic
drug. While well intentioned, this bill would jeopardize
patients’ access to timely and appropriate medical
care, clog the court system and result in higher
medical and legal costs for these patients and their
families. CHA is working with a coalition — including
the Alzheimer’s Association and California Psychiatric
Association — to narrow the bill’s scope and provide
protections for hospitals.
Placed on Assembly
Inactive file Aug. 29.
Oppose Sheree Lowe/
Alex Hawthorne
SB 1273 Moorlach
(R-Costa Mesa)
Would clarify that California’s counties may use funds
from the Mental Health Services Act to provide
outpatient stabilization services to individuals
voluntarily receiving those services, even when those
who are receiving services involuntarily are treated at
the same facility. The Department of Health Care
Services issued a memo on July 20, 2016, which
clarified and supported the bill’s intention.
Placed on Assembly
Inactive file Aug. 29.
Support Sheree Lowe/
Alex Hawthorne
Nursing Services
AB 1306 Burke
(D-Inglewood)
As amended by the author, no longer includes the
corporate practice ban, which would have prohibited
CNMs from being employed by a corporation (such as
a hospital) or other “artificial legal entity.” CHA
supports AB 1306’s premise — that California’s more
than 1,200 CNMs should have authority to practice to
the full extent of their certification, education and
training. As advanced practice registered nurses,
CNMs’ scope of practice allows them to provide
comprehensive management of women’s health care,
focusing primarily on pregnancy, childbirth and the
postpartum period. Their scope of practice also
includes care of the newborn, family planning and
other gynecological needs throughout the life cycle.
Would remove the physician supervision requirement,
allowing CNMs greater independence in meeting the
health care needs of the millions of individuals added
to California’s health care system by the Affordable
Care Act, facilitating timely access to quality care.
Failed passage by full
Assembly Aug. 31.
Support Jackie Garman/
BJ Bartleson/
David Perrott/
Connie Delgado
SB 323 Hernandez
(D-Azusa)
Would allow nurse practitioners to practice to the full
extent of their education and training to ensure access
to health care delivery systems for millions of
Californians who now have access to coverage under
the Affordable Care Act.
Held in the Assembly
Business and
Professions Committee
June 28.
Support BJ Bartleson/
Connie Delgado
SB 1195 Hill
(D-San Mateo)
Provides requirements and procedures for the Director
of Consumer Affairs to review a decision or other
action by a board under the Department about a
restraint of trade. Among other things, would prohibit
the Board of Nursing executive director from being a
licensee of the board.
Placed on Senate
Inactive File June 2.
Follow, Hot BJ Bartleson/
Connie Delgado
Page 5

California Hospital Association Key State Issues
Bill No. Author Location/Action CHA Position Staff Contact
Professional Workforce Education
SB 66 Leyva (D-Chino)/
McGuire (D-
Healdsburg)
As amended, would require the Department of
Consumer Affairs to make available, upon request by
the Office of the Chancellor of the California
Community Colleges, information on every licensee so
that the Office of the Chancellor can better measure
employment outcomes of students who participate in
career technical education programs and make
recommendations as to how these programs may be
improved. The bill also urges the Chancellor to align
these measures with the performance accountability
measures of the federal Workforce Innovation and
Opportunity Act.
Awaiting action on the
Governor’s desk.
Support Cathy Martin/
Alex Hawthorne
Public Health
AB 508 Garcia
(D-Bell Gardens)
Would have established the California Maternal
Quality Care Collaborative (CMQCC) within CDPH.
As amended, would require CDPH to prepare and
submit to the Legislature an annual report on maternal
mortality and morbidity in California, including an
analysis of maternal deaths and severe maternal
morbidity. The bill would also require CDPH to
consider existing resources, including opportunities for
partnerships with other entities and the use of
physician volunteers.
Held in Senate
Judiciary Committee.
Follow, Hot David Perrott/
Alex Hawthorne
AB 2424 Gomez
(D-Los Angeles)
Would create the Community-based Health
Improvement and Innovation Fund within the state
treasury. A target level of annual statewide investment
from the fund would be established as a set dollar
amount per capita, to be allocated to the California
Department of Public Health to support community-
based prevention of priority chronic health conditions
throughout the state, including in the form of
competitive grants.
Held on Suspense in
the Senate
Appropriations
Committee Aug. 11.
Follow Amber Kemp/
Kathryn Scott
AB 2439 Nazarian
(D-Sherman
Oaks)
Would create a California Department of Public Health
(CDPH) pilot program to select four or fewer hospital
emergency departments to offer HIV tests to patients.
CHA originally opposed the bill as an unfunded
mandate and inappropriate setting to conduct HIV
tests, but removed opposition with amendments that
made hospital participation in the pilot program
voluntary.
Awaiting action on the
Governor’s desk.
Follow, Hot David Perrott/
Debby Rogers/
Alex Hawthorne
AB 2640 Gipson
(D-Carson)
Would add to the significant body of existing laws on
HIV testing and would require every medical provider
who orders an HIV test to provide information to
specified patients about methods that prevent or
reduce the risk of contracting HIV, including pre-
exposure prophylaxis and post-exposure prophylaxis,
consistent with guidance of the federal Centers for
Disease Control and Prevention. CHA opposed this bill
on the grounds that it codifies the practice of medicine
into law; however, an agreement was reached with the
author to ensure physician discretion is preserved.
CHA had opposed this bill on the grounds that it
codifies the practice of medicine into law; however, an
agreement was reached with the author to ensure
physician discretion is preserved. Recent
amendments address CHA’s concerns.
Awaiting action on the
Governor’s desk.
Neutral, as
Amended
David Perrott/
Debby Rogers/
Alex Hawthorne
Page 6

California Hospital Association Key State Issues
Bill No. Author Location/Action CHA Position Staff Contact
Reimbursement
SB 1365 Hernandez
(D-Azusa)
Would require a hospital that offers a service in a
hospital-based outpatient clinic to provide a notice to
each patient when that service is available in a non-
hospital-based location.
Awaiting action on the
Governor’s desk.
Neutral Amber Ott/
Barbara Glaser
Skilled-Nursing Facilities
AB 1518 (Committee on
Aging and Long-
Term Care)
Would increase access to the home and community-
based Medi-Cal Nursing Facility/Acute Hospital Waiver
by increasing the number of authorized waiver slots
and requiring an expedited authorization process for
patients in acute care hospitals who are awaiting
discharge to a skilled-nursing facility.
Placed on Senate
Inactive File.
Support Pat Blaisdell/
Jackie Garman/
Barbara Glaser
SB 503 Hernandez
(D-Azusa)
As amended June 30, this bill would address
deficiencies in current law identified by a judge in a
recent court decision for the treatment of
unrepresented patients who lack capacity to make
medical decisions. The bill would allow skilled nursing
facilities (SNFs) to continue to obtain consent for the
care of a patient by using an interdisciplinary team
process, if the SNF provides a specified written notice
to the patient. The bill also requires that, prior to
administering an antipsychotic drug to a SNF patient,
the SNF convene a hearing with the patient, the
ordering physician, an independent physician, a
patient advocate and an interpreter (if necessary) to
review the medication order. The independent
physician and advocate must meet a list of
qualifications; the physician must also issue a written
decision. The patient may not be billed for the services
of the independent physician, advocate or interpreter.
CDPH, the bill sponsor, decided not to move the bill
forward this year.
Held in Assembly
Health Committee.
Oppose,
Unless
Amended
Lois Richardson/
Alex Hawthorne
Page 7