9.50 - 10.35 Mark Laslett Patho-Anatomic Sources
78
Sources and Causes of Chronic Low Back and Referred Leg Pain Mark Laslett Mark Laslett PT, PhD, Dip.MT, Dip.MDT PT, PhD, Dip.MT, Dip.MDT PhysioSouth, Christchurch, New Zealand PhysioSouth, Christchurch, New Zealand 2006 Congress Danish Physiotherapy Association 2006 Congress Danish Physiotherapy Association Odense, Denmark. March 24 Odense, Denmark. March 24 - - 25 25
-
Upload
nelsonrodriguezdeleon -
Category
Documents
-
view
222 -
download
1
description
sij
Transcript of 9.50 - 10.35 Mark Laslett Patho-Anatomic Sources

Sources and Causes of Chronic Low Back and Referred Leg Pain
Mark LaslettMark LaslettPT, PhD, Dip.MT, Dip.MDTPT, PhD, Dip.MT, Dip.MDT
PhysioSouth, Christchurch, New ZealandPhysioSouth, Christchurch, New Zealand
2006 Congress Danish Physiotherapy Association2006 Congress Danish Physiotherapy AssociationOdense, Denmark. March 24Odense, Denmark. March 24--2525

© Mark Laslett 2006
Sources of Back & Leg PainSources of Back & Leg Painendplate
annularfailure
annularfissure
Z-jointcapsule
Intervertebral DiscIntervertebral DiscNerve Root / duraNerve Root / duraZZ--JointJointSacroiliac JointSacroiliac JointButtock & HipButtock & HipMusclesMuscles

© Mark Laslett 2006
Causes of Back and Leg PainCauses of Back and Leg Pain
InjuryInjurySustained loadingSustained loadingGradual tissue Gradual tissue degradationdegradationSpinal stenosisSpinal stenosisPeripheral artery diseasePeripheral artery diseaseNeoplasmsNeoplasmsInstabilityInstabilityRheumatic diseaseRheumatic disease

© Mark Laslett 2006
PrevalencePrevalence
10%
Nerve Root
15%Z-Joint
13%SIJ
2%Stenosis
21%
? & others
39%Disc
DiscNerve RootZ-JointSIJStenosis? & others

© Mark Laslett 2006
Discogenic painDiscogenic pain
Reacts to Reacts to preferentially to preferentially to specific loading specific loading (directional (directional preference)preference)
Reacts nonReacts non--preferentially to preferentially to loading
Mechanically mediatedMechanically mediated
Chemically mediatedChemically mediated
loading

© Mark Laslett 2006
Directional PreferenceDirectional Preference
Can be identified using:Can be identified using:repeated movementsrepeated movementssustained loadingsustained loadingMDT assessment (McKenzie)MDT assessment (McKenzie)
One direction progressively increases or One direction progressively increases or peripheralizes pain distributionperipheralizes pain distributionAnother direction progressively reduces or Another direction progressively reduces or centralizes pain distributioncentralizes pain distribution

© Mark Laslett 2006
Directional PreferenceDirectional Preference
Common Common (Donelson R et al 1991)(Donelson R et al 1991)
43% respond preferentially to extension43% respond preferentially to extension11% respond preferentially to flexion11% respond preferentially to flexion11% respond preferentially asymmetric extension or 11% respond preferentially asymmetric extension or lateral flexionlateral flexion
CentralizationCentralizationAt least 20% in chronic cases (single assessment)At least 20% in chronic cases (single assessment)Over 50% in general LBP (over 3Over 50% in general LBP (over 3--5 days)5 days)

© Mark Laslett 2006
MDT AssessmentMDT Assessment
Test movements / Test movements / positions are positions are standardizedstandardizedTherapist Therapist overpressure, overpressure, mobilization and mobilization and manipulation used as manipulation used as methods to increase methods to increase loading in a specified loading in a specified directiondirection

© Mark Laslett 2006
PeripheralizationPeripheralizationCentralizationCentralization

© Mark Laslett 2006
Validity of clinical findingsValidity of clinical findingsagainst provocation discographyagainst provocation discography
VariableVariable % Sensitivity% Sensitivity % Specificity% Specificity LR+LR+
CentralizationCentralization 4040 9494 6.96.9
Directional preferenceDirectional preference 4949 9191 5.75.7
Moderate or minor Moderate or minor extension lossextension loss
2727 8787 2.02.0
‘vulnerable in the neutral ‘vulnerable in the neutral zone’zone’
4141 8383 2.52.5
History of persistent pain History of persistent pain between episodesbetween episodes
3232 9292 4.14.1

© Mark Laslett 2006
Cecil MCecil MMale, age 39Male, age 39
9yrs pain worsening. Fell 2 9yrs pain worsening. Fell 2 metresmetres. .
Severely disabled. DRAM “distressed Severely disabled. DRAM “distressed somatic”somatic”
VAS: Now 99, best 4, worst 99VAS: Now 99, best 4, worst 99
Poor historian, speech impediment. Poor historian, speech impediment. Taking Taking VicodinVicodin

© Mark Laslett 2006
Cecil MCecil MLeft lateral shiftLeft lateral shift
Negative SIJ tests except sacral Negative SIJ tests except sacral thrust. Spring tests positive L5,4,3thrust. Spring tests positive L5,4,3
Neurological testing negative Neurological testing negative normal, Nerve tension tests negativenormal, Nerve tension tests negative
CentralisationCentralisation, DP to shift correction , DP to shift correction and extensionand extension

© Mark Laslett 2006

© Mark Laslett 2006

© Mark Laslett 2006
L5/S1 L4/5 L3/4

© Mark Laslett 2006

© Mark Laslett 2006
Beverly MBeverly MFemale, age 42Female, age 42
2yrs pain unchanging. Motor vehicle 2yrs pain unchanging. Motor vehicle accident restrained. accident restrained.
Moderately disabled. DRAM ‘at risk’. Moderately disabled. DRAM ‘at risk’.
VAS: Now 53, best 25, worst 64VAS: Now 53, best 25, worst 64
PT (5/12) NE, epidural and SIJ PT (5/12) NE, epidural and SIJ injections no benefitinjections no benefit

© Mark Laslett 2006
Beverly MBeverly MPositive Extension / Rotation testsPositive Extension / Rotation tests
One positive SIJ test, Spring test One positive SIJ test, Spring test positive L5positive L5
Nerve tension tests essentially Nerve tension tests essentially normal. Absent left TA reflex. normal. Absent left TA reflex. Normal muscle testsNormal muscle tests
peripheralisationperipheralisation

© Mark Laslett 2006

© Mark Laslett 2006

© Mark Laslett 2006

© Mark Laslett 2006
Chemically Mediated Chemically Mediated Discogenic painDiscogenic pain
Trauma Trauma –– acute & subacute painacute & subacute pain? Infection / discitis? Infection / discitis? Auto? Auto--immune reactionimmune reaction

© Mark Laslett 2006
George LGeorge LMale, age 52Male, age 52
5yrs pain worsening. Lifting lawnmower. 5yrs pain worsening. Lifting lawnmower.
Moderately DisabledModerately Disabled
DRAM ‘at risk’. DRAM ‘at risk’.
VAS: Now 67, best 69, worst 92VAS: Now 67, best 69, worst 92
PT (2/12) worse, epidural 2/7 relief, facet PT (2/12) worse, epidural 2/7 relief, facet injections/RF no benefitinjections/RF no benefit

© Mark Laslett 2006
George LGeorge LPositive Extension/Rotation testsPositive Extension/Rotation tests
Negative SIJ. Spring +Negative SIJ. Spring +veve L4 onlyL4 only
Neurologically normal, Nerve tension Neurologically normal, Nerve tension tests normaltests normal
No No centralisationcentralisation, peripheralisation, , peripheralisation, Directional PreferenceDirectional Preference

© Mark Laslett 2006

© Mark Laslett 2006

© Mark Laslett 2006

© Mark Laslett 2006
ZygapophysealZygapophyseal jointjoint
10%
Nerve Root
13%SIJ
2%Stenosis
21%
? & others
39%Disc
15%Z-Joint

© Mark Laslett 2006
Zygapophyseal joint painZygapophyseal joint pain
16% have Z16% have Z--joint pain (Jackson et joint pain (Jackson et al 1988)(Schwarzer et al 1994)al 1988)(Schwarzer et al 1994)40% of older patients have Z40% of older patients have Z--Joint Joint pain (pain (ManchikantiManchikanti L et al 1999)L et al 1999)True prevalence is probably between True prevalence is probably between 55--10%10%

© Mark Laslett 2006
Zygapophyseal joint painZygapophyseal joint pain
There is no clinical facet / ZJ There is no clinical facet / ZJ ‘syndrome’‘syndrome’
Can only be diagnosed by controlled Can only be diagnosed by controlled ZJ blocks under fluoroscopic ZJ blocks under fluoroscopic guidanceguidance

© Mark Laslett 2006
Prediction of 95% pain reduction after Z joint block Prediction of 95% pain reduction after Z joint block Laslett M et al Laslett M et al –– in press)in press)
VariableVariable % % SensSens % Spec% Spec +LR+LR
Age>49Age>49 6262 7777 2.62.6
Onset pain Onset pain paraspinalparaspinal
7575 7272 2.72.7
Best walkingBest walking 3131 9292 3.63.6
Best sittingBest sitting 3333 9090 3.23.2
Positive ER testPositive ER test 100100 2222 1.31.3
SomatizationSomatization 4646 7070 1.51.5
NonNon--centralisationcentralisation 100100 1414 1.11.1

© Mark Laslett 2006
Clinical Prediction Rules of screening ZJ blockClinical Prediction Rules of screening ZJ blockNote: pretest odds approx 0.11 (prevalence 11%)Note: pretest odds approx 0.11 (prevalence 11%)
Clinical Prediction RuleClinical Prediction Rule %%SensSens %Spec%Spec
2 of 6 (excluding use of 2 of 6 (excluding use of centralisation data)centralisation data)
100100 3636
4 of 74 of 7 100100 5050
91913 of 5 (excluding MSPQ 3 of 5 (excluding MSPQ questionnaire and CP data)questionnaire and CP data)
8585

© Mark Laslett 2006
If Rule satisfied:If Rule satisfied:11%11%-->55% chance>55% chance
If Rule not satisfied:If Rule not satisfied:11% 11% -->2% chance>2% chance
Five fold improvement in probability of Five fold improvement in probability of a 95% pain reduction or not using the a 95% pain reduction or not using the rule.rule.
Pretest probability
Posttest probabilityLikelihood ratio
Fagan’s Fagan’s NomogramNomogram for 3 of 5for 3 of 5

© Mark Laslett 2006
Billie RBillie RMale 72ysMale 72ys4 months since chair broke and landed on 4 months since chair broke and landed on buttocks. buttocks. Severely disabled. DRAM ‘distressed Severely disabled. DRAM ‘distressed depressed’depressed’VAS 80 (now) 48 (best) 95 (worst)VAS 80 (now) 48 (best) 95 (worst)RF right facets 4 weeks ago abolished RF right facets 4 weeks ago abolished right sided pain. (R) THR, some (L)OA hipright sided pain. (R) THR, some (L)OA hip

© Mark Laslett 2006
Billie RBillie R
Positive Extension / Rotation testsPositive Extension / Rotation testsSIJ tests negative. Spring tests L3,4,5 SIJ tests negative. Spring tests L3,4,5 positive. Capsular pattern left hippositive. Capsular pattern left hipNormal nerve tension tests, LBP with left. Normal nerve tension tests, LBP with left. Absent left TA reflex, weak left quads and Absent left TA reflex, weak left quads and EHL.EHL.Only partial MDT exam because of OA hip Only partial MDT exam because of OA hip and THRand THR

© Mark Laslett 2006
Billie RBillie R
initialinitialpain drawingpain drawing
(pre(pre--examination)examination)

© Mark Laslett 2006
Billie RBillie R
(post(post--examination)examination)

© Mark Laslett 2006
Billie RBillie R
left L3 superior left L3 superior articular process at articular process at its junction with the its junction with the transverse process. transverse process.
Aspiration recovered Aspiration recovered no blood. ¼ cc no blood. ¼ cc
IohexolIohexol was instilled. was instilled. The contrast spread The contrast spread
at the base of the at the base of the SAP at the target SAP at the target
location for left L2 location for left L2 medial branch.medial branch.

© Mark Laslett 2006
Billie RBillie R
Post MBB L2,3Post MBB L2,3

© Mark Laslett 2006
Sacroiliac jointSacroiliac joint
2%Stenosis
21%
? & others
39%Disc
15%Z-Joint
10%
Nerve Root
13%SIJ

© Mark Laslett 2006
Sacroiliac joint syndromeSacroiliac joint syndrome
13% have SIJ pain 13% have SIJ pain (Bogduk 1997)(Bogduk 1997)
22.5% have SIJ pain 22.5% have SIJ pain (Bernard et al 1991)(Bernard et al 1991)
30% have SIJ pain 30% have SIJ pain (Schwarzer et al 1995)(Schwarzer et al 1995)
7% have SIJ pain 7% have SIJ pain (Laslett 1997)(Laslett 1997)
probably much lower ? 5% in chronic LBPprobably much lower ? 5% in chronic LBP
depends on sample depends on sample
PGP in pregnant women 21% (Albert H et al 2002)PGP in pregnant women 21% (Albert H et al 2002)

© Mark Laslett 2006
Composite pain drawings Composite pain drawings DreyfussDreyfuss et al 1996et al 1996
Patients with negative Patients with negative Patients with positive Patients with positive arthrogramsarthrograms arthrogramsarthrograms

© Mark Laslett 2006
Reliability of SIJ testsReliability of SIJ tests
% agreement% agreement KappaKappa value (Landis et al)value (Landis et al)
DistractionDistraction 88.288.2 0.690.69 substantialsubstantialTorsion (R)Torsion (R) 88.288.2 0.750.75 substantialsubstantialTorsion (L)Torsion (L) 88.288.2 0.720.72 substantialsubstantialThigh thrustThigh thrust 94.194.1 0.880.88 almost perfectalmost perfectCompressionCompression 88.288.2 0.730.73 substantialsubstantialSacral thrustSacral thrust 78.078.0 0.520.52 moderatemoderateCranial glideCranial glide 84.384.3 0.610.61 substantialsubstantial
Laslett M, Williams M. Spine 1994Laslett M, Williams M. Spine 1994

© Mark Laslett 2006
SIJ SIJ -- validity of test clustersvalidity of test clusters
Statistic 1 or more
positive tests
2 or more
positive tests
3 or more positive
tests
4 or more
positive tests
5 or more
positive tests
Sensitivity 1.00 0.9 0.9 0.6 0.27
Specificity 0.4 0.7 0.8 0.81 0.88
+LR 1.8 2.7 4.3 3.2 2.1
Laslett, Young, Aprill & McDonald, Manual Therapy 2005
Van derWurff2006
0.85
0.79
4.02

© Mark Laslett 2006
SIJ. Validity of >2 positive tests in non SIJ. Validity of >2 positive tests in non centraliserscentralisers
StatisticEstimate
Low 95% CI
High 95% CI
Sensitivity 0.91 0.62 0.98
Specificity 0.87 0.68 0.96
Positive Likelihood Ratio
6.97 2.70 20.27
Negative Likelihood Ratio
0.11 0.02 0.44
Laslett, Young, Aprill & McDonald, AJP, June 2003

© Mark Laslett 2006
Kristi GKristi GFemale, age 37 Female, age 37
2.5yrs pain worsening. Slipped & fell 2.5yrs pain worsening. Slipped & fell onto right hiponto right hip
Severely disabled. DRAM ‘distressed Severely disabled. DRAM ‘distressed depressed’depressed’
VAS: Now 87, best 70, worst 97VAS: Now 87, best 70, worst 97
PT/MT unchangedPT/MT unchanged

© Mark Laslett 2006
Kristi GKristi GPositive Extension / Rotation testsPositive Extension / Rotation tests
SIJ all strongly positive. Spring tests all SIJ all strongly positive. Spring tests all positivepositive
R SLR 80º R butt pain L SLR 85º no pain.. R SLR 80º R butt pain L SLR 85º no pain.. Neurologically normalNeurologically normal
Hip: full ROM but all movements painful. Hip: full ROM but all movements painful. FABER test +FABER test +veve..
no centralization, peripheralisation, no centralization, peripheralisation, Directional PreferenceDirectional Preference

© Mark Laslett 2006
Kristi GKristi G
Initial pain Initial pain drawingdrawing
(pre (pre examination)examination)

© Mark Laslett 2006
SIJ SIJ arthrogramarthrogram
Dorsal joint Dorsal joint capsulecapsule
Ventral joint Ventral joint capsulecapsule

© Mark Laslett 2006
Kristi GKristi G
pre &pre &post SIJpost SIJinjectioninjection
pain pain drawingdrawing

© Mark Laslett 2006
Kristi GKristi GRight SIJ fusion March 2002Right SIJ fusion March 2002
As of March 2003As of March 2003
good solid fusion CT demonstratedgood solid fusion CT demonstrated
usual pain abolishedusual pain abolished
functionally normalfunctionally normal
recurring R buttock ache (different) recurring R buttock ache (different) apparently coincident with menstrual apparently coincident with menstrual cyclecycle

© Mark Laslett 2006
Sacroiliac joint criteriaSacroiliac joint criteriano centralizationno centralization3 or more pain provocation tests provoke 3 or more pain provocation tests provoke familiar painfamiliar painLaslett & Williams 1994Laslett & Williams 1994Laslett, Young, Aprill, McDonald 2003Laslett, Young, Aprill, McDonald 2003Van Van derder WurffWurff P et al 2006P et al 2006

© Mark Laslett 2006
The sacroiliac joint testsThe sacroiliac joint tests
DistractionDistractionThigh thrustThigh thrustCompressionCompressionSacral thrustSacral thrustGaenslen’sGaenslen’s testtestPatrick’s FABER testPatrick’s FABER test

© Mark Laslett 2006
DistractionDistraction

© Mark Laslett 2006
CompressionCompression

© Mark Laslett 2006
Thigh ThrustThigh Thrust

© Mark Laslett 2006
Gaenslen’s Gaenslen’s testtest

© Mark Laslett 2006
Sacral thrustSacral thrust

© Mark Laslett 2006
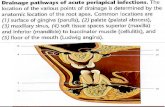
Nerve Root (Radicular) PainNerve Root (Radicular) Pain
13%SIJ
2%Stenosis
21%
? & others
39%Disc
15%Z-Joint
10%
Nerve Root

© Mark Laslett 2006
Stacie LStacie LFemale, age 22Female, age 22
Dominant pain: right buttock. Onset: Dominant pain: right buttock. Onset: same areasame area
3 months pain unchanging. Struck 3 months pain unchanging. Struck by moped while walkingby moped while walking
Severely disabled. DRAM ‘at risk’Severely disabled. DRAM ‘at risk’
VAS: Now 72, best 59, worst 83VAS: Now 72, best 59, worst 83
PT (4/52) worse. MRI. No surgeryPT (4/52) worse. MRI. No surgery

© Mark Laslett 2006
Stacie LStacie LPositive Extension / Rotation testsPositive Extension / Rotation tests
SIJ: Gaenslen’s positive all others negative. SIJ: Gaenslen’s positive all others negative. Spring tests positive at L5 & L4Spring tests positive at L5 & L4
R & L SLR +R & L SLR +veve 30º causing R leg pain, 30º causing R leg pain, absent R TA reflex. Normal muscle testsabsent R TA reflex. Normal muscle tests
Peripheralisation. Temporary & slight Peripheralisation. Temporary & slight centralisingcentralising effect. Not a effect. Not a centralisercentraliser..

© Mark Laslett 2006
Initial pain drawing
Pain VAS
Now: 72Best: 59Worst: 83

© Mark Laslett 2006

© Mark Laslett 2006
Disc extrusionL5 and S1 rootlets

© Mark Laslett 2006
Extruded material behindL5 vertebral body
Extruded material at the level of L4/5 disc

© Mark Laslett 2006

© Mark Laslett 2006

© Mark Laslett 2006
Lynn MLynn MFemale, age 59Female, age 59
8 months pain unchanging. Onset: NAR. 8 months pain unchanging. Onset: NAR. Midline LBP, but L groin pain doing Midline LBP, but L groin pain doing lunges. Dominant groin painlunges. Dominant groin pain
Severely disabled, Zung 14, MSPQ 1, Severely disabled, Zung 14, MSPQ 1, DRAM ‘normal’DRAM ‘normal’
VAS: Now 70, best 21, worst 77VAS: Now 70, best 21, worst 77
4/52 PT unchanged. MRI lumbar spine4/52 PT unchanged. MRI lumbar spine

© Mark Laslett 2006
Lynn MLynn Mworst standing / walking, best sitting. worst standing / walking, best sitting.
Positive extension rotation tests. SIJ: all Positive extension rotation tests. SIJ: all negative. Spring all negativenegative. Spring all negative
Neurologically normalNeurologically normal
Hip: nonHip: non--capsular pattern. Flex & lat capsular pattern. Flex & lat rotation most painful & limitedrotation most painful & limited
Repeated movementsRepeated movementsDirectional preference to repeated extensionDirectional preference to repeated extension

© Mark Laslett 2006
Lynn MLynn M
Initial pain Initial pain drawingdrawing
(pre examination)(pre examination)

© Mark Laslett 2006 Hip radiographsHip radiographs

© Mark Laslett 2006
Left hip Left hip arthrogramarthrogram

© Mark Laslett 2006
Mary CMary C
pre &pre &post hippost hipinjectioninjection
pain pain drawingdrawing

© Mark Laslett 2006
SummarySummary
There is no clinical ‘facet’ joint syndromeThere is no clinical ‘facet’ joint syndromeClinical diagnosis is possible for:Clinical diagnosis is possible for:
About 50% of discogenic pain (mechanical)About 50% of discogenic pain (mechanical)SIJ painSIJ painNerve root (radicular) painNerve root (radicular) painSpinal stenosisSpinal stenosisPeripheral vascular diseasePeripheral vascular disease

© Mark Laslett 2006
SummarySummaryZZ--joint pain can only be diagnosed using joint pain can only be diagnosed using controlled blocks but:controlled blocks but:
There are clinical indicators for positive and negative There are clinical indicators for positive and negative responses responses –– useful for patient selection of invasive useful for patient selection of invasive testingtesting
SIJ diagnosis confirmed only with double blocksSIJ diagnosis confirmed only with double blocksDiscogenic pain best diagnosed by provocation Discogenic pain best diagnosed by provocation discography, but this controversialdiscography, but this controversialSpinal stenosis Spinal stenosis confirmedconfirmed only by CT or MRIonly by CT or MRIPeripheral vascular disease confirmed by Peripheral vascular disease confirmed by angiographyangiography

© Mark Laslett 2006
Agreement between clinical Agreement between clinical diagnoses and available reference diagnoses and available reference
standardsstandards
BMC J Musculoskeletal Disorders 6:28,2005BMC J Musculoskeletal Disorders 6:28,2005216 patients. Chronic, disabled and distressed216 patients. Chronic, disabled and distressedSingle Single pathopatho--anatomic diagnosis in 66% by anatomic diagnosis in 66% by available reference standardsavailable reference standards13% chance of physiotherapist guessing correct 13% chance of physiotherapist guessing correct diagnosisdiagnosisClinical agreement achieved in 57%Clinical agreement achieved in 57%

© Mark Laslett 2006
ConclusionConclusion
The clinical examination is The clinical examination is useful, important, validuseful, important, valid

© Mark Laslett 2006