8890 Cal Center Drive • Sacramento, CA 95826 Toll Free ...
5
"Premier Access Dental, has grown as a result of a successful balance between competitive rates, solid coverage, flexible plan design and superior service." 1 Toll Free Phone: 888-326-3210 8890 Cal Center Drive • Sacramento, CA 95826 A special note about Plus Plans: Our Plus Plans give employers the opportunity to provide a quality dental plan at a reduced cost. Members have the flexibility to go to any dentist, but may experience higher out-of-pocket expenses when using a non-network dentist. Premier Access will allow up to the Maximum Allowable Charge, accordingly to the fee schedule for non-network dentists. Charges in excess of the Fee Schedule will be the member’s responsibility. For example, if a non-network dentist charges $100 for a cleaning and the allowance on the fee schedule is $40, Premier Access will pay the applicable percentage of $40. The remaining balance is the member’s responsibility. Members also have access to the Premier Access PPO and PCN networks! These dentists offer dental care at a discounted rate (contracted rates for PPO and PCN dentists are 30% or more, below usual charges). Additionally, the PPO and PCN dentists cannot “balance bill” our members for amounts greater than their contracted rate. Premier Access Insurance Company strongly encourages our members to use PPO and PCN dentists to maximize benefits and reduce out-of-pocket expenses. Please see included fee schedule, then multiply the fee by the benefit percentage provided in your plan to determine the maximum Premier Access will pay for your dental care. Dated at ______________ this ______________ day of _______________________, 20______ Authorized Employer Signature ___________________________________________________ Agent Signature__________________________________________________________________ Group Name_____________________________________________________________________
Transcript of 8890 Cal Center Drive • Sacramento, CA 95826 Toll Free ...

"Premier Access Dental, has grown as a result of a successful balance between competitive rates, solid coverage, flexible plan design and superior service."
1
Toll Free Phone: 888-326-3210
8890 Cal Center Drive • Sacramento, CA 95826
A special note about Plus Plans:
Our Plus Plans give employers the opportunity to provide a quality dental plan at a reduced cost. Members have the flexibility to go to any dentist, but may experience higher out-of-pocket expenses when using a non-network dentist. Premier Access will allow up to the Maximum Allowable Charge, accordingly to the fee schedule for non-network dentists. Charges in excess of the Fee Schedule will be the member’s responsibility. For example, if a non-network dentist charges $100 for a cleaning and the allowance on the fee schedule is $40, Premier Access will pay the applicable percentage of $40. The remaining balance is the member’s responsibility.
Members also have access to the Premier Access PPO and PCN networks! These dentists offer dental care at a discounted rate (contracted rates for PPO and PCN dentists are 30% or more, below usual charges). Additionally, the PPO and PCN dentists cannot “balance bill” our members for amounts greater than their contracted rate.
Premier Access Insurance Company strongly encourages our members to use PPO and PCN dentists to maximize benefits and reduce out-of-pocket expenses. Please see included fee schedule, then multiply the fee by the benefit percentage provided in your plan to determine the maximum Premier Access will pay for your dental care.
Dated at ______________ this ______________ day of _______________________, 20______
Authorized Employer Signature ___________________________________________________
Agent Signature__________________________________________________________________
Group Name_____________________________________________________________________
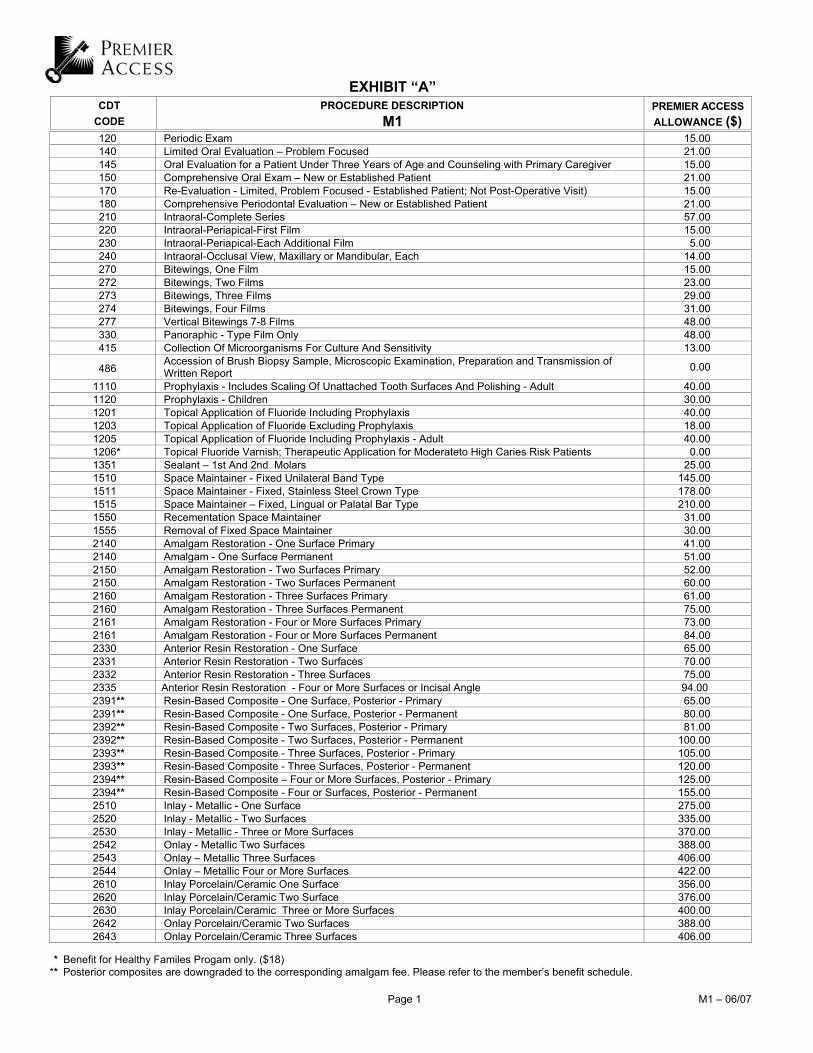
EXHIBIT “A”
CDT CODE
PROCEDURE DESCRIPTION M1
PREMIER ACCESS ALLOWANCE ($)
Page 1 M1 – 06/07
120 Periodic Exam 15.00 140 Limited Oral Evaluation – Problem Focused 21.00 145 Oral Evaluation for a Patient Under Three Years of Age and Counseling with Primary Caregiver 15.00 150 Comprehensive Oral Exam – New or Established Patient 21.00 170 Re-Evaluation - Limited, Problem Focused - Established Patient; Not Post-Operative Visit) 15.00 180 Comprehensive Periodontal Evaluation – New or Established Patient 21.00 210 Intraoral-Complete Series 57.00 220 Intraoral-Periapical-First Film 15.00 230 Intraoral-Periapical-Each Additional Film 5.00 240 Intraoral-Occlusal View, Maxillary or Mandibular, Each 14.00 270 Bitewings, One Film 15.00 272 Bitewings, Two Films 23.00 273 Bitewings, Three Films 29.00 274 Bitewings, Four Films 31.00 277 Vertical Bitewings 7-8 Films 48.00 330 Panoraphic - Type Film Only 48.00 415 Collection Of Microorganisms For Culture And Sensitivity 13.00
486 Accession of Brush Biopsy Sample, Microscopic Examination, Preparation and Transmission of Written Report 0.00
1110 Prophylaxis - Includes Scaling Of Unattached Tooth Surfaces And Polishing - Adult 40.00 1120 Prophylaxis - Children 30.00 1201 Topical Application of Fluoride Including Prophylaxis 40.00 1203 Topical Application of Fluoride Excluding Prophylaxis 18.00 1205 Topical Application of Fluoride Including Prophylaxis - Adult 40.00 1206* Topical Fluoride Varnish; Therapeutic Application for Moderateto High Caries Risk Patients 0.00 1351 Sealant – 1st And 2nd Molars 25.00 1510 Space Maintainer - Fixed Unilateral Band Type 145.00 1511 Space Maintainer - Fixed, Stainless Steel Crown Type 178.00 1515 Space Maintainer – Fixed, Lingual or Palatal Bar Type 210.00 1550 Recementation Space Maintainer 31.00 1555 Removal of Fixed Space Maintainer 30.00 2140 Amalgam Restoration - One Surface Primary 41.00 2140 Amalgam - One Surface Permanent 51.00 2150 Amalgam Restoration - Two Surfaces Primary 52.00 2150 Amalgam Restoration - Two Surfaces Permanent 60.00 2160 Amalgam Restoration - Three Surfaces Primary 61.00 2160 Amalgam Restoration - Three Surfaces Permanent 75.00 2161 Amalgam Restoration - Four or More Surfaces Primary 73.00 2161 Amalgam Restoration - Four or More Surfaces Permanent 84.00 2330 Anterior Resin Restoration - One Surface 65.00 2331 Anterior Resin Restoration - Two Surfaces 70.00 2332 Anterior Resin Restoration - Three Surfaces 75.00 2335 Anterior Resin Restoration - Four or More Surfaces or Incisal Angle 94.00 2391** Resin-Based Composite - One Surface, Posterior - Primary 65.00 2391** Resin-Based Composite - One Surface, Posterior - Permanent 80.00 2392** Resin-Based Composite - Two Surfaces, Posterior - Primary 81.00 2392** Resin-Based Composite - Two Surfaces, Posterior - Permanent 100.00 2393** Resin-Based Composite - Three Surfaces, Posterior - Primary 105.00 2393** Resin-Based Composite - Three Surfaces, Posterior - Permanent 120.00 2394** Resin-Based Composite – Four or More Surfaces, Posterior - Primary 125.00 2394** Resin-Based Composite - Four or Surfaces, Posterior - Permanent 155.00 2510 Inlay - Metallic - One Surface 275.00 2520 Inlay - Metallic - Two Surfaces 335.00 2530 Inlay - Metallic - Three or More Surfaces 370.00 2542 Onlay - Metallic Two Surfaces 388.00 2543 Onlay – Metallic Three Surfaces 406.00 2544 Onlay – Metallic Four or More Surfaces 422.00 2610 Inlay Porcelain/Ceramic One Surface 356.00 2620 Inlay Porcelain/Ceramic Two Surface 376.00 2630 Inlay Porcelain/Ceramic Three or More Surfaces 400.00 2642 Onlay Porcelain/Ceramic Two Surfaces 388.00 2643 Onlay Porcelain/Ceramic Three Surfaces 406.00
* Benefit for Healthy Familes Progam only. ($18) ** Posterior composites are downgraded to the corresponding amalgam fee. Please refer to the member’s benefit schedule.
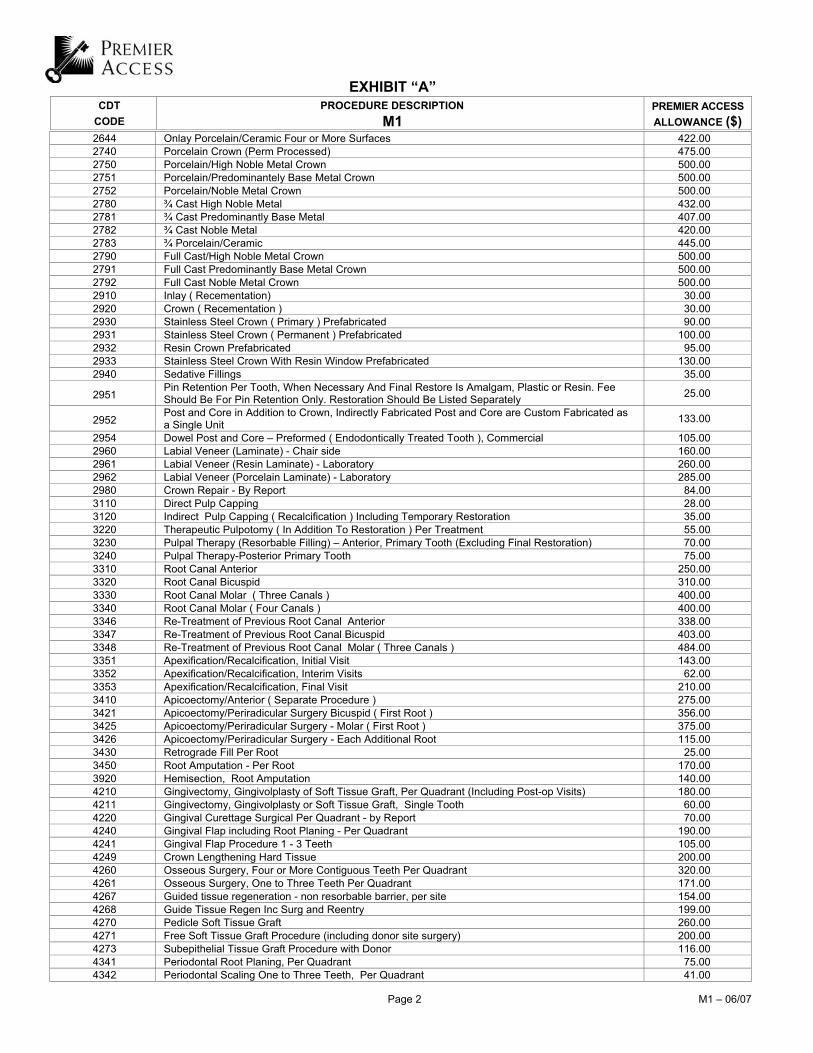
EXHIBIT “A”
CDT CODE
PROCEDURE DESCRIPTION M1
PREMIER ACCESS ALLOWANCE ($)
Page 2 M1 – 06/07
2644 Onlay Porcelain/Ceramic Four or More Surfaces 422.00 2740 Porcelain Crown (Perm Processed) 475.00 2750 Porcelain/High Noble Metal Crown 500.00 2751 Porcelain/Predominantely Base Metal Crown 500.00 2752 Porcelain/Noble Metal Crown 500.00 2780 ¾ Cast High Noble Metal 432.00 2781 ¾ Cast Predominantly Base Metal 407.00 2782 ¾ Cast Noble Metal 420.00 2783 ¾ Porcelain/Ceramic 445.00 2790 Full Cast/High Noble Metal Crown 500.00 2791 Full Cast Predominantly Base Metal Crown 500.00 2792 Full Cast Noble Metal Crown 500.00 2910 Inlay ( Recementation) 30.00 2920 Crown ( Recementation ) 30.00 2930 Stainless Steel Crown ( Primary ) Prefabricated 90.00 2931 Stainless Steel Crown ( Permanent ) Prefabricated 100.00 2932 Resin Crown Prefabricated 95.00 2933 Stainless Steel Crown With Resin Window Prefabricated 130.00 2940 Sedative Fillings 35.00
2951 Pin Retention Per Tooth, When Necessary And Final Restore Is Amalgam, Plastic or Resin. Fee Should Be For Pin Retention Only. Restoration Should Be Listed Separately 25.00
2952 Post and Core in Addition to Crown, Indirectly Fabricated Post and Core are Custom Fabricated as a Single Unit 133.00
2954 Dowel Post and Core – Preformed ( Endodontically Treated Tooth ), Commercial 105.00 2960 Labial Veneer (Laminate) - Chair side 160.00 2961 Labial Veneer (Resin Laminate) - Laboratory 260.00 2962 Labial Veneer (Porcelain Laminate) - Laboratory 285.00 2980 Crown Repair - By Report 84.00 3110 Direct Pulp Capping 28.00 3120 Indirect Pulp Capping ( Recalcification ) Including Temporary Restoration 35.00 3220 Therapeutic Pulpotomy ( In Addition To Restoration ) Per Treatment 55.00 3230 Pulpal Therapy (Resorbable Filling) – Anterior, Primary Tooth (Excluding Final Restoration) 70.00 3240 Pulpal Therapy-Posterior Primary Tooth 75.00 3310 Root Canal Anterior 250.00 3320 Root Canal Bicuspid 310.00 3330 Root Canal Molar ( Three Canals ) 400.00 3340 Root Canal Molar ( Four Canals ) 400.00 3346 Re-Treatment of Previous Root Canal Anterior 338.00 3347 Re-Treatment of Previous Root Canal Bicuspid 403.00 3348 Re-Treatment of Previous Root Canal Molar ( Three Canals ) 484.00 3351 Apexification/Recalcification, Initial Visit 143.00 3352 Apexification/Recalcification, Interim Visits 62.00 3353 Apexification/Recalcification, Final Visit 210.00 3410 Apicoectomy/Anterior ( Separate Procedure ) 275.00 3421 Apicoectomy/Periradicular Surgery Bicuspid ( First Root ) 356.00 3425 Apicoectomy/Periradicular Surgery - Molar ( First Root ) 375.00 3426 Apicoectomy/Periradicular Surgery - Each Additional Root 115.00 3430 Retrograde Fill Per Root 25.00 3450 Root Amputation - Per Root 170.00 3920 Hemisection, Root Amputation 140.00 4210 Gingivectomy, Gingivolplasty of Soft Tissue Graft, Per Quadrant (Including Post-op Visits) 180.00 4211 Gingivectomy, Gingivolplasty or Soft Tissue Graft, Single Tooth 60.00 4220 Gingival Curettage Surgical Per Quadrant - by Report 70.00 4240 Gingival Flap including Root Planing - Per Quadrant 190.00 4241 Gingival Flap Procedure 1 - 3 Teeth 105.00 4249 Crown Lengthening Hard Tissue 200.00 4260 Osseous Surgery, Four or More Contiguous Teeth Per Quadrant 320.00 4261 Osseous Surgery, One to Three Teeth Per Quadrant 171.00 4267 Guided tissue regeneration - non resorbable barrier, per site 154.00 4268 Guide Tissue Regen Inc Surg and Reentry 199.00 4270 Pedicle Soft Tissue Graft 260.00 4271 Free Soft Tissue Graft Procedure (including donor site surgery) 200.00 4273 Subepithelial Tissue Graft Procedure with Donor 116.00 4341 Periodontal Root Planing, Per Quadrant 75.00 4342 Periodontal Scaling One to Three Teeth, Per Quadrant 41.00
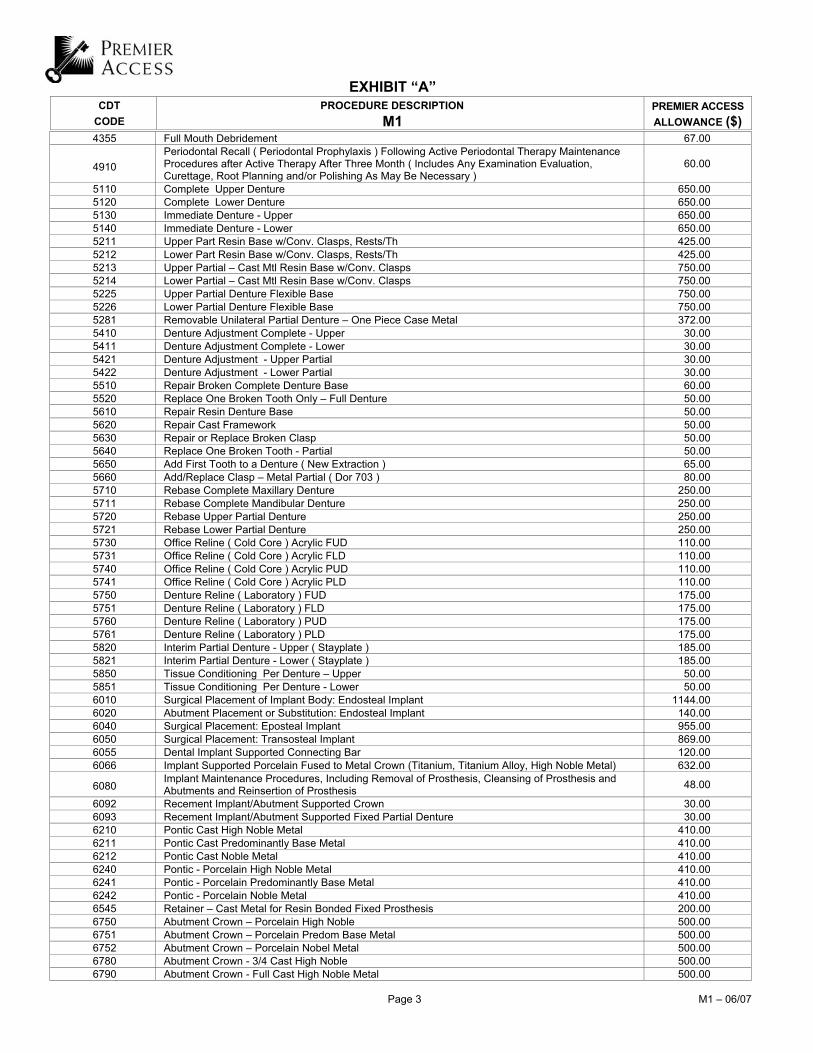
EXHIBIT “A”
CDT CODE
PROCEDURE DESCRIPTION M1
PREMIER ACCESS ALLOWANCE ($)
Page 3 M1 – 06/07
4355 Full Mouth Debridement 67.00
4910 Periodontal Recall ( Periodontal Prophylaxis ) Following Active Periodontal Therapy Maintenance Procedures after Active Therapy After Three Month ( Includes Any Examination Evaluation, Curettage, Root Planning and/or Polishing As May Be Necessary )
60.00
5110 Complete Upper Denture 650.00 5120 Complete Lower Denture 650.00 5130 Immediate Denture - Upper 650.00 5140 Immediate Denture - Lower 650.00 5211 Upper Part Resin Base w/Conv. Clasps, Rests/Th 425.00 5212 Lower Part Resin Base w/Conv. Clasps, Rests/Th 425.00 5213 Upper Partial – Cast Mtl Resin Base w/Conv. Clasps 750.00 5214 Lower Partial – Cast Mtl Resin Base w/Conv. Clasps 750.00 5225 Upper Partial Denture Flexible Base 750.00 5226 Lower Partial Denture Flexible Base 750.00 5281 Removable Unilateral Partial Denture – One Piece Case Metal 372.00 5410 Denture Adjustment Complete - Upper 30.00 5411 Denture Adjustment Complete - Lower 30.00 5421 Denture Adjustment - Upper Partial 30.00 5422 Denture Adjustment - Lower Partial 30.00 5510 Repair Broken Complete Denture Base 60.00 5520 Replace One Broken Tooth Only – Full Denture 50.00 5610 Repair Resin Denture Base 50.00 5620 Repair Cast Framework 50.00 5630 Repair or Replace Broken Clasp 50.00 5640 Replace One Broken Tooth - Partial 50.00 5650 Add First Tooth to a Denture ( New Extraction ) 65.00 5660 Add/Replace Clasp – Metal Partial ( Dor 703 ) 80.00 5710 Rebase Complete Maxillary Denture 250.00 5711 Rebase Complete Mandibular Denture 250.00 5720 Rebase Upper Partial Denture 250.00 5721 Rebase Lower Partial Denture 250.00 5730 Office Reline ( Cold Core ) Acrylic FUD 110.00 5731 Office Reline ( Cold Core ) Acrylic FLD 110.00 5740 Office Reline ( Cold Core ) Acrylic PUD 110.00 5741 Office Reline ( Cold Core ) Acrylic PLD 110.00 5750 Denture Reline ( Laboratory ) FUD 175.00 5751 Denture Reline ( Laboratory ) FLD 175.00 5760 Denture Reline ( Laboratory ) PUD 175.00 5761 Denture Reline ( Laboratory ) PLD 175.00 5820 Interim Partial Denture - Upper ( Stayplate ) 185.00 5821 Interim Partial Denture - Lower ( Stayplate ) 185.00 5850 Tissue Conditioning Per Denture – Upper 50.00 5851 Tissue Conditioning Per Denture - Lower 50.00 6010 Surgical Placement of Implant Body: Endosteal Implant 1144.00 6020 Abutment Placement or Substitution: Endosteal Implant 140.00 6040 Surgical Placement: Eposteal Implant 955.00 6050 Surgical Placement: Transosteal Implant 869.00 6055 Dental Implant Supported Connecting Bar 120.00 6066 Implant Supported Porcelain Fused to Metal Crown (Titanium, Titanium Alloy, High Noble Metal) 632.00
6080 Implant Maintenance Procedures, Including Removal of Prosthesis, Cleansing of Prosthesis and Abutments and Reinsertion of Prosthesis 48.00
6092 Recement Implant/Abutment Supported Crown 30.00 6093 Recement Implant/Abutment Supported Fixed Partial Denture 30.00 6210 Pontic Cast High Noble Metal 410.00 6211 Pontic Cast Predominantly Base Metal 410.00 6212 Pontic Cast Noble Metal 410.00 6240 Pontic - Porcelain High Noble Metal 410.00 6241 Pontic - Porcelain Predominantly Base Metal 410.00 6242 Pontic - Porcelain Noble Metal 410.00 6545 Retainer – Cast Metal for Resin Bonded Fixed Prosthesis 200.00 6750 Abutment Crown – Porcelain High Noble 500.00 6751 Abutment Crown – Porcelain Predom Base Metal 500.00 6752 Abutment Crown – Porcelain Nobel Metal 500.00 6780 Abutment Crown - 3/4 Cast High Noble 500.00 6790 Abutment Crown - Full Cast High Noble Metal 500.00

EXHIBIT “A”
CDT CODE
PROCEDURE DESCRIPTION M1
PREMIER ACCESS ALLOWANCE ($)
Page 4 M1 – 06/07
6791 Abutment Crown - Full Cast Predom Base Metal 500.00 6792 Abutment Crown - Full Cast Noble Metal 500.00 6930 Bridge ( Recementation ) 52.00 6970 Post And Core In Addition To Fixed Partial Denture Retainer, Indirectly Fabricated 133.00 6972 Prefab Post and Core in Add to Bridge Retainer 105.00 6980 Bridge Repair By Report 90.00 7111 Coronal Remnants - Deciduous Tooth 46.00 7140 Extraction, Erupted Tooth or Exposed Root 61.00 7210 Surgical Removal of an Erupted Tooth 90.00 7220 Removal of Impacted Tooth ( Soft Tissue ) 120.00 7230 Removal of Impacted Tooth ( Partially Bony ) 160.00 7240 Removal of Impacted Tooth ( Complete Bony ) 195.00 7241 Removal of Impacted Tooth ( Complete Bony ) Unusual Surgical Complications 205.00 7250 Removal of Residual Root Totally Covered by Bone 96.00 7260 Closure of Oral Fistula of Maxillary Sinus 184.00 7270 Reimplantation and/or Stabilization of Accidentally Evulsed/Displaced Teeth and/or Alveous 174.00 7280 Crown Exposure With Attachment Placed for Orthodontic Traction 80.00 7281 Surgical Exposure of Impacted/Unerupted Tooth-Aid Erup. 60.00 7285 Biopsy of Oral Tissue Hard. 96.00 7286 Biopsy of Oral Tissue, Incisional, Soft 108.00 7310 Alveoloplasty ( in Addition to Removal of Teeth ) Per Quadrant 90.00 7320 Alveoloplasty No Extraction - per Quadrant 110.00 7340 Aveolopasty With Ridge Extension ( Secondary Eptheliazatioan ) 197.00 7410 Excision of Benign Lesion up to 1.25 cm 254.00 7411 Excision of Benign Lesion greater than 1.25 cm 434.00 7440 Excision of Malignant Tumor - Lesion Diameter up to 1.25 cm 448.00 7441 Excision of Malignant Tumor - Lesion Diameter greater than 1.25 cm 697.00 7450 Excision of Cyst, to 1.25cm 150.00 7451 Excision of Cyst, Larger Than 1.25cm 170.00 7460 Rem Nondont. Cyst/Tum up to 1.25cm 130.00 7461 Rem Nondont. Cyst/Tum Greater Than 1.25cm 300.00 7470 Removal of Exostosis Maxilla or Mandible 160.00 7471 Removal of Mandibulartori Per Quadrant 263.00 7472 Removal of Torus Palatinus 312.00 7473 Removal of Torus Madibularis 295.00 7510 Intraoral Incision and Drainage of Abscess ( Soft Tissue ) 50.00 7520 Extraoral Incision and Drainage of Abscess 362.00 7530 Incision and Removal Foreign Body from Soft Tissue 130.00 7540 Removal of Foreign Body from Bone ( Independent Procedure ) 144.00 7550 Sequestrectomy for Osteomylities or Abscess, Superficial 90.00 7560 Maxillary Sinusotomy for Removal of Tooth Fragment or Foreign Body 717.00 7910 Suture of Recent Small Wounds up to 5cm 116.00 7911 Complicated Suture up to 5cm 290.00 7912 Complicated Suture Greater Than 5cm 522.00 7960 Frenulectomy 160.00 7970 Excision of Hyperplastic Tissue, Per Arch 100.00 7971 Excision of Pericoronal Gingiva 60.00 7980 Sialolithotomy: Removal of Salivary Calculus, Intraorally 246.00 7981 Sialolithotomy: Removal of Salivary Calculus, Extraorally 246.00 7982 Dilation of Salivary Duct 662.00 7983 Closure of Salivary Fistula 632.00 8210 Appliance to Control Harmful Habits - Removable 250.00 8220 Appliance to Control Harmful Habits - Fixed 250.00 9110 Palliative ( Emergency ) Treatment of Dental Pain 35.00 9220 Anesthesia, General, One Half Hour 95.00 9221 Anesthesia, General, Each Additional 15 Minutes 30.00 9230 Nitrous Oxide 30.00 9240 Intravenous Sedation 85.00 9310 Special Consultation (Specialist Only – Separate Fee Only if Patient Not Treated by Consultant) 40.00 9430 Office Visit For Observation (during regularly scheduled hous) - No Other Services Performed 22.00 9440 Office Visit - After Regularly Scheduled Hours 45.00 9610 Therapeutic Parenteral Drug, Single Administration 18.00 9920 Behavior Management By Report 0.00 9930 Post-operative Visit – Complications ( E.G. Osteitis ) 0.00 9942 Repair and/or Reline of Occulusal Guard 60.00