86
10
Arksornnukit et al Clinical Implications Denture teeth made of different materials and with different cuspal angulations showed varying amounts and patterns of pressure distri- bution. Zero-degree denture teeth may be considered an option for patients with atrophied residual ridges as they provide lower pres- sure transmission compared to cusped denture teeth. Statement of problem. Pressure transmission and distribution under denture bases may be variable depending on the different materials and cuspal angulations of denture teeth. Purpose. The purpose of this study was to evaluate pressure transmission and distribution under impact load using denture teeth made with different materials and cuspal angulations. Material and methods. Three types (acrylic resin, microfilled composite resin, and ceramic) and 4 different cuspal angulations (0 degree, 20 degree, 33 degree, and 35 degree) of denture teeth were evaluated. Pressure transmission, distribution, and maximum pressure (n=10) were observed with pressure-sensitive sheets under an impact load. Data were statistically analyzed with 2-way ANOVA (α=.05) to determine significant interactions between denture tooth materials and cuspal angulations with respect to pressure transmission, followed by 1-way ANOVA (α=.05) to examine how materials and angulations jointly affected the pressure. Two 1-way ANOVAs were performed on the acrylic resin and ceramic denture teeth with the inclusion of 20-degree denture teeth groups. Tukey HSD and Tamhane’s post hoc tests were used to evaluate data differences among groups. Results. Denture tooth materials and cuspal angulations had significant interactions with respect to average pressure (P<.001) and maximum pressure transmission (P=.007). Zero-degree denture teeth showed significantly lower aver- age and maximum pressures than 33- and 35-degree denture teeth for all 3 denture tooth materials (P<.001). Denture teeth with greater cuspal angulations demonstrated significantly higher average pressure transmission for all ceramic denture teeth groups (P<.05). Conclusions. Pressure transmission and distribution varied among denture teeth made of different materials and with different cuspal angulations. Cusped denture teeth presented significantly higher average pressure and maximum pres- sure transmission compared to 0-degree denture teeth. (J Prosthet Dent 2011;105:127-136) Pressure transmission and distribution under denture bases using denture teeth with different materials and cuspal angulations Mansuang Arksornnukit, DDS, MS, PhD, a Thitima Phunthikaphadr, DDS, b and Hidekazu Takahashi, DDS, PhD c Chulalongkorn University, Bangkok, Thailand; Tokyo Medical and Dental University, Tokyo, Japan Financial support for this study was provided by the 100 th Anniversary of Chulalongkorn University Fund (Ratchadaphiseksomphot Endowment Fund). a Associate Professor, Department of Prosthodontics, Faculty of Dentistry, Chulalongkorn University. b Graduate student, Department of Prosthodontics, Faculty of Dentistry, Chulalongkorn University. c Associate Professor and Chair, Advanced Biomaterials, Division of Oral Health Sciences, Tokyo Medical and Dental University. Although removable prostheses are provided to enable oral masti- catory function and to improve the quality of life for edentulous pa- tients, 1 studies have demonstrated that alveolar ridge resorption is com- monly observed in denture wearers. 2-4 The resorption of residual ridges is a chronic, slowly progressing, irrevers- ible, and cumulative process. 5 The magnitude and pattern of the resorp- tion have also shown variation. 2,4 The
-
Upload
raul-miranda -
Category
Documents
-
view
84 -
download
6
Transcript of 86

Arksornnukit et al
Clinical ImplicationsDenture teeth made of different materials and with different cuspal angulations showed varying amounts and patterns of pressure distri-bution. Zero-degree denture teeth may be considered an option for patients with atrophied residual ridges as they provide lower pres-sure transmission compared to cusped denture teeth.
Statement of problem. Pressure transmission and distribution under denture bases may be variable depending on the different materials and cuspal angulations of denture teeth.
Purpose. The purpose of this study was to evaluate pressure transmission and distribution under impact load using denture teeth made with different materials and cuspal angulations.
Material and methods. Three types (acrylic resin, microfilled composite resin, and ceramic) and 4 different cuspal angulations (0 degree, 20 degree, 33 degree, and 35 degree) of denture teeth were evaluated. Pressure transmission, distribution, and maximum pressure (n=10) were observed with pressure-sensitive sheets under an impact load. Data were statistically analyzed with 2-way ANOVA (α=.05) to determine significant interactions between denture tooth materials and cuspal angulations with respect to pressure transmission, followed by 1-way ANOVA (α=.05) to examine how materials and angulations jointly affected the pressure. Two 1-way ANOVAs were performed on the acrylic resin and ceramic denture teeth with the inclusion of 20-degree denture teeth groups. Tukey HSD and Tamhane’s post hoc tests were used to evaluate data differences among groups.
Results. Denture tooth materials and cuspal angulations had significant interactions with respect to average pressure (P<.001) and maximum pressure transmission (P=.007). Zero-degree denture teeth showed significantly lower aver-age and maximum pressures than 33- and 35-degree denture teeth for all 3 denture tooth materials (P<.001). Denture teeth with greater cuspal angulations demonstrated significantly higher average pressure transmission for all ceramic denture teeth groups (P<.05).
Conclusions. Pressure transmission and distribution varied among denture teeth made of different materials and with different cuspal angulations. Cusped denture teeth presented significantly higher average pressure and maximum pres-sure transmission compared to 0-degree denture teeth. (J Prosthet Dent 2011;105:127-136)
Pressure transmission and distribution under denture bases using denture teeth with different materials and cuspal angulations
Mansuang Arksornnukit, DDS, MS, PhD,a Thitima Phunthikaphadr, DDS,b and Hidekazu Takahashi, DDS, PhDc
Chulalongkorn University, Bangkok, Thailand; Tokyo Medical and Dental University, Tokyo, Japan
Financial support for this study was provided by the 100th Anniversary of Chulalongkorn University Fund (Ratchadaphiseksomphot Endowment Fund).
aAssociate Professor, Department of Prosthodontics, Faculty of Dentistry, Chulalongkorn University.bGraduate student, Department of Prosthodontics, Faculty of Dentistry, Chulalongkorn University.cAssociate Professor and Chair, Advanced Biomaterials, Division of Oral Health Sciences, Tokyo Medical and Dental University.
Although removable prostheses are provided to enable oral masti-catory function and to improve the quality of life for edentulous pa-
tients,1 studies have demonstrated that alveolar ridge resorption is com-monly observed in denture wearers.2-4 The resorption of residual ridges is a
chronic, slowly progressing, irrevers-ible, and cumulative process.5 The magnitude and pattern of the resorp-tion have also shown variation.2,4 The

128 Volume 105 Issue 2
The Journal of Prosthetic Dentistry Arksornnukit et al
cause of resorption process is com-plex; Kordatzis et al6 have reported that the number of edentulous years, initial height of the mandible, and the number of dentures used are not as-sociated with the amount of resorp-tion. Even though the increase in residual ridge resorption seen in den-ture wearers has been attributed to pressure from prostheses,3 it was sug-gested that a proper amount of pres-sure within the limits of physiological tolerance, applied in the direction of normal forces to a particular region, could stimulate bone apposition.7
Ortman8 considered bone resorp-tion to be a normal process that is balanced by bone apposition; this process may be either physiologic or pathologic depending on multiple factors. If pressure from denture pros-theses alters the blood supply of the bone or causes inflammation to the mucoperiosteum, bone resorption may occur. Matsuo et al9 reported that a pressure of 27 to 68 g/cm2 caused fibroblasts to increase intra-cellular calcium which, in turn, initiat-ed the alveolar bone remodeling. Berg et al10 also suggested that, to keep blood circulation normal, a continu-ous mechanical pressure higher than 1.3 kPa should not be transferred to the denture-supporting tissues. Ac-cording to the authors of these stud-ies, dentures should be designed and fabricated with an emphasis on pres-ervation of the remaining oral struc-tures, and efforts should be made to lower stresses to residual alveolar ridges.
Prosthesis fabrication requires care in each step, and one key factor is the selection of suitable denture teeth for each patient. Various types of poste-rior artificial tooth forms for dentures are commercially available.11 For some dentists, the science of choosing arti-ficial teeth is an automatic procedure based on regular use of particular materials or a philosophy acquired in dental school or clinical practice. Nevertheless, a more rational ap-proach for tooth selection should be based on the physical properties of
dental materials and the anatomic and physiologic requirements of the patient.11
The task of choosing proper den-ture teeth for dentures has resulted in 2 primary considerations, materi-als11,12 and the forms of the denture teeth.13-16 Investigators have consid-ered posterior tooth forms13-16 and cuspal angulations,17,18 with several studies evaluating the effectiveness of and patient satisfaction with dif-ferent occlusal forms of denture teeth.15,16,18-21 Some authors reported that patients provided with com-plete dentures having lingualized or anatomic posterior occlusal forms expressed significantly higher levels of satisfaction compared to patients with dentures with 0-degree posterior occlusal forms.16,19 The subject groups in the study, however, were not strati-fied for age, gender, degree of residual ridge resorption, denture experience, or previous type of denture occlusal scheme, and the authors considered this a weakness of the investigation.16
Diverse opinions about different occlusal schemes with various poste-rior tooth forms have also been intro-duced.22-24 Cusped denture teeth are commonly chosen by clinicians for balanced occlusal schemes in com-plete dentures. Boucher22 stated that cusped teeth provide an easy oppor-tunity to acquire bilateral (cross-arch) balanced occlusion, which is difficult to achieve with cuspless teeth. The reason behind the concept of bilat-eral balanced occlusion is to prevent rocking movements via additional balancing contacts on molars during protrusive and laterotrusive move-ments.23 Some authors suggest using canine guidance to prevent parafunc-tional activities in complete denture patients.24
Investigators have previously ex-amined residual ridge resorption in complete denture patients with ana-tomic, nonanatomic, and semiana-tomic posterior teeth.25,26 The results showed that the anatomic occlusal group had significantly less resorption compared to the nonanatomic group,
and less denture movement from rest position to centric occlusion over a 5-year period. These authors25,26 sup-ported the use of anatomic posterior occlusion to enhance the stability and decrease the amount of mandibular bone resorption. In contrast, some dentists believe that nonanatomic posterior occlusion is the most prac-tical and reasonable solution for all edentulous patients, especially for pa-tients with flat residual ridges.27
According to the authors of pre-vious studies investigating posterior occlusal forms of denture teeth, there has been little focus on pressure be-neath denture bases with different cuspal angulations.13,17 Transmission of masticatory forces directly to the edentulous residual ridges should be measured to determine whether more or less cuspal angulation would be preferable. Lopuck et al28 used a pho-toelastic stress analysis to examine the stress patterns under dentures. The authors suggested that a flat occlu-sal scheme transferred slightly lower forces to the residual ridge compared to other cuspal forms. Chowdhary et al17 investigated the stress gener-ated beneath complete dentures us-ing denture teeth with different cus-pal angulations. These authors used finite element analysis and found greater magnitudes of stresses in 33-degree and 20-degree cusp teeth, respectively, whereas 0-degree teeth showed the least. Swoope and Kydd29 used electronic strain gauges to study the effect of different cusp forms and occlusal surface areas on complete denture base deformation. The au-thors suggested that angle reduction of posterior teeth cusps decreased the deformation of complete denture bases, which, in turn, reduced the horizontal stress to residual ridges. These studies,17,29 however, did not clearly demonstrate the amount and pattern of pressure distribution be-neath denture bases because finite element analysis is a mathematical technique for finding approximate so-lutions, and strain gauges are suitable for specific site measurements.

129February 2011
Arksornnukit et al
Criteria for measurement of pres-sure beneath denture bases have been offered by several investigators.30-32 Many methods and measuring devic-es have been developed. Strain gauges and pressure transducers are 2 of the most common pressure-recording devices. However, these 2 devices are only suitable for measuring pressure at specific sites. A pressure-sensitive sheet (Fuji Prescale Film; Fuji Photo Film Co, Ltd, Tokyo, Japan) has been used as a pressure-detecting device for measuring occlusal pressure, oc-clusal force, and occlusal contact areas.33,34 Recently, pressure-sensitive sheets were used for pressure mea-surement under denture bases to evaluate pressure transmission and distribution. Pressure distribution un-der impact load was reported to vary due to the differences in denture tooth materials.35 Pressure-sensitive sheets are useful in pressure measurement because they are easy to use for the evaluation of large pressure ranges and areas.33,34
The purpose of this study was to examine pressure transmission and distribution under denture bases us-ing denture teeth made of different materials with different cuspal an-gulations under an impact load, and
to determine whether there were any significant interactions between ma-terials and cuspal angulations with respect to the pressure transferred. The null hypotheses of the present study were that there would be no dif-ferences in pressure transmission and distribution using denture teeth with different materials and cuspal angu-lations, and no interactions between materials and cuspal angulations with respect to pressure transferred.
MATERIAL AND METHODS
Eighty pairs of maxillary and man-dibular right and left first molars of 3 different types (acrylic resin, micro-filled composite resin, and ceramic) and 4 different cuspal angulations (0, 20, 33, and 35 degree) of denture teeth were examined in this study. The combinations of materials and angula-tions are listed in Table I. The 20-de-gree acrylic resin and ceramic denture teeth were flattened to 0 degrees after completing the impact test and were described as the 0-degree acrylic resin and 0-degree ceramic denture teeth groups, respectively.
A simplified model of a tooth specimen was made of a denture tooth in an acrylic resin denture
base. The denture bases were made by using putty-type silicone impres-sion material (Provil Novo; Heraeus Kulzer GmbH, Hanau, Germany) as a mold. Melted wax was poured into the mold and each denture tooth was lowered into the wax using a surveyor (Ney Surveyor Parallelometer System; Dentsply Ceramco, Burlington, NJ) to ensure that the occlusal surface was parallel to the base. All speci-mens were then invested in denture flasks (Hanau; Water Pik, Inc, Ft. Col-lins, Colo), followed by conventional packing procedures36 using heat-po-lymerizing acrylic resin (Lucitone 199; Dentsply Trubyte, York, Pa). Long po-lymerizing cycles were used for acrylic resin packing procedures. The tem-perature was slowly raised from room temperature to 74°C and held for 9 hours. After completion of polymer-izing cycles, the flasks were allowed to cool to room temperature before deflasking. All specimens were then removed from the denture flasks and any flash was removed with a carbide bur (Abbott-Robinson HP Burs; Buf-falo Dental Mfg Co, Syosset, NY). The denture base of each tooth specimen was shaped to a size of 15 x 15 mm, with a thickness of 3 mm. The bases of the specimens were polished with
Acrylic resin0 degree20 degree
33 degree
Microfilledcomposite resin0 degree33 degree
Ceramic0 degree20 degree35 degree
* Teeth were prepared from 20-degree denture teeth after impact test.
M30M30
M30
M30M30
M30M30M30
—Shofu, Inc,
Kyoto, JapanShofu, Inc
Shofu, IncShofu, Inc
—Shofu, IncShofu, Inc
Mold ManufacturerType
Bioace Resin (modified)*Bioace Resin
Resin Kyushi
Endura PosteriorEndura Posterior
Bioace Ceramic (modified)*Bioace CeramicBioace Ceramic
Brand Name
Table I. Artificial denture teeth used

130 Volume 105 Issue 2
The Journal of Prosthetic Dentistry Arksornnukit et al
an automatic polishing machine (DPS 3200; Imptech, Boksburg, South Afri-ca) under a slow speed with constant water irrigation. The final polishing steps for all specimens were complet-ed by using 0.05-μm-particle-sized aluminum oxide slurry (Leco Corp, St. Joseph, Mich).
The same methods for prepar-ing each tooth specimen were used for both maxillary and mandibular denture teeth. After the impact test, the occlusal surfaces of the 20-de-gree acrylic resin denture teeth were carefully flattened and polished with up to 1200-grit silicon carbide pa-per (Silicon Carbide Grinding paper; Buehler, Düsseldorf, Germany) under water irrigation. For the 20-degree ceramic denture teeth, a polishing kit (Soft Diamonds Grinding and Buffing Wheels; Asami Tanaka Dental, Fried-richsdorf, Germany) was used for the final polishing procedure. Grinding and polishing procedures were per-formed on these denture teeth until flat occlusal surfaces were achieved. After the teeth were flattened, there were still some grooves on the occlu-sal tables. The surveyor was used to ensure that the flat occlusal surfaces were parallel to the base. These pol-ished specimens were the 0-degree denture teeth groups.
After preparing all specimens, each pair of maxillary and mandibular denture teeth was arranged in a Class I occlusal relationship on the impact load testing apparatus. The occlu-
sion between maxillary and man-dibular denture teeth was evaluated by using articulating paper (Red/Blue articulating film; Ardent Intl, Inc, Ossining, NY). Occlusal adjust-ment was performed by the selective grinding procedure to obtain proper centric occlusion. Final polishing procedures for the different types of denture teeth were performed ac-cording to the material specification for each type of denture tooth.36 The occlusal contact areas were measured using pressure-sensitive sheets to en-sure that uniform occlusal contact areas were achieved for all groups. The maxillary and mandibular tooth specimens are shown in Figure 1.
Three types of pressure-sensitive sheets (Fuji Prescale Film, LW, LLW, and LLLW; Fuji Photo Film Co, Ltd, Tokyo, Japan) were used to detect pressure transmission and distribu-tion under denture bases in the pres-ent study. The measuring ranges of the 3 pressure-sensitive sheets, LW, LLW, and LLLW, are between 2.5 and 10.0 MPa, 0.5 and 2.5 MPa, and 0.2 and 0.6 MPa, respectively. The structure of the pressure-sensitive sheet consists of microencapsulated color-forming and color-developing materials. When contact pressure is applied to the sheet, a red-colored impression is formed in various den-sities according to the amount of pressure and pressure distribution. The maxillary denture tooth was at-tached to a weight and the pressure
was applied by dropping the weight freely onto the antagonist mandibu-lar denture tooth specimen, with the sheet placed underneath to measure average pressure, maximum pressure, and pressure transmission areas. The LLW sheet type was primarily used for pressure measurements. When aver-age or maximum pressure was found to be above or below its measuring ranges, LW or LLLW sheets were used, respectively.
All pressure-sensitive sheets ac-quired from the tests were analyzed with digital analysis software (Fuji-Film Pressure Distribution Mapping System FPD-8010E, v. 1.1; Fuji Photo Film Co, Ltd). According to the man-ufacturer, the accuracy of a pressure-sensitive sheet is ±10%. The authors of a previous study37 suggested that for the greatest accuracy and reliabili-ty, pressure-sensitive sheets should be analyzed within 8 hours of exposure to pressure. In the present study, pres-sure-sensitive sheets were analyzed immediately after testing to achieve maximum accuracy and reliability.
The impact drop test used in the present study was modified from that used in the previous study by Phunt-hikaphadr et al.35 A study conducted by Miyaura et al33 revealed that the average occlusal force for a complete denture patient was around 50 N us-ing pressure-sensitive sheets as mea-suring devices. Therefore, a load of 50 N was used in the present study. The maxillary denture tooth that was attached to the weight was freely dropped over a distance of 5 mm to-wards the mandibular denture tooth. A small piece of the LW pressure-sen-sitive sheet was placed at the occlu-sal contact interface to measure and confirm the occlusal force of 50 N. The impact load testing apparatus is shown in Figure 2.
Statistical software (SPSS v. 17.0; SPSS, Inc, Chicago, Ill) was used for statistical analysis. To assess signifi-cant interactions between denture tooth materials and cusp angula-tions, the 20-degree denture teeth groups were first omitted, and a
1 Maxillary and mandibular denture tooth specimens.

131February 2011
Arksornnukit et al
2-way ANOVA was used to determine interactions for 3 materials x 2 angu-lations (0, 33/35). The interaction and any significant main effects were tested with 1-way ANOVA (α=.05) to examine the joint effect of the mate-rial and cusp angulation on pressure transmission. Two separate 1-way ANOVAs were then performed on the acrylic resin and ceramic denture teeth groups with 20-degree denture teeth. Tukey’s Honestly Significant Difference (HSD) test was used for post hoc multiple comparison. The robust tests of equality of means and Tamhane’s post hoc test were used when equal variances could not be as-sumed.
RESULTS
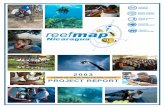
Representative pressure-sensitive sheets (LLW type) obtained from dif-ferent types of denture teeth with dif-ferent cuspal angulations are shown in Figure 3. Pressure-sensitive sheets (LLW type) acquired from the im-pact test showed some similarities as well as variations among groups. Different amounts and patterns of pressure distribution were demon-
strated (Fig. 3). Zero-degree denture teeth from all denture tooth material groups showed lower pressure trans-mission compared to cusped denture teeth. High and localized pressure transmission was observed in the 20- and 35-degree ceramic denture teeth groups.
Two-way ANOVA (Table II) indi-cated significant differences among materials (P<.001) and among cuspal angulations (P<.001), with a signifi-cant interaction between these 2 fac-tors (P<.001) with respect to average pressure transmission. A statistically significant interaction between mate-rials and angulations was also found in maximum pressure transferred (P=.007), with significant differences among materials (P=.041) and cus-pal angulations (P<.001). As for the pressure transmission area, signifi-cant differences were observed within the material (P<.001) and angulation (P<.001) factors; however, no signifi-cant interaction between these 2 fac-tors was shown (P=.104).
One-way ANOVA and post hoc multiple comparison tests were then performed to determine how mate-rials and angulations jointly affect
the average and maximum pressure transmission. One-way ANOVA re-vealed significant differences in aver-age pressure (P<.001) and maximum pressure transmission (P<.001) with respect to different materials and cuspal angulations. Means of average and maximum pressure transmission and multiple post hoc comparisons are shown in Table III. Thirty-five-de-gree ceramic denture teeth presented the significantly highest average pres-sure, jointly followed by 33-degree acrylic resin and microfilled compos-ite resin denture teeth, and 0-degree denture teeth presented the lowest average pressure. No statistically sig-nificant difference with respect to average pressure transmission was found between different types of tooth materials on 0-degree denture teeth (Table III). As for maximum pressure transmission of all 3 denture tooth materials, 33- and 35-degree showed significantly higher maximum pressure compared to 0-degree den-ture teeth. No significant differences were observed for 0-degree denture teeth (Table III).
Two 1-way ANOVAs were per-formed on the acrylic resin and ceram-ic denture teeth groups with 20-de-gree denture teeth. Means of average pressure, maximum pressure, and pressure transmission area for all an-gulations of acrylic resin and ceramic denture teeth are shown in Table IV. There were significant differences in average pressure transmission in the acrylic resin (P<.001) and ceramic denture teeth (P<.001) groups with respect to different cuspal angula-tions. However, no statistically signif-icant difference was found between 20-degree and 33-degree angulations in the acrylic resin denture teeth group (Table IV). Significant differ-ences in maximum pressure transmis-sion with respect to different cuspal angulations were found in both the acrylic resin (P<.001) and ceramic (P<.001) denture teeth groups. Maxi-mum pressure transmission observed for denture teeth with greater cuspal angulations was greater than that for
2 Impact load testing apparatus. Maxillary denture tooth was freely dropped from height of 5 mm to create 50-N load at occlusal surfaces.

132 Volume 105 Issue 2
The Journal of Prosthetic Dentistry Arksornnukit et al
3 Representative pressure-sensitive sheets under denture bases obtained from all groups.
Table II. Two-way ANOVA for materials (A) and cusp angulations (B) on average pressure, maximum pressure, and pressure transmission area (20-degree denture teeth groups omitted)
Average pressure
Materials (A)
Angulations (B)
A x B
Error
Maximum pressure
Materials (A)
Angulations (B)
A x B
Error
Pressure transmission area
Materials (A)
Angulations (B)
A x B
Error
2
1
2
54
2
1
2
54
2
1
2
54
df
0.236
3.413
0.210
0.082
2.00
139
3.25
16
3564
23522
657
7533
0.118
3.413
0.105
0.002
1.00
138.68
1.62
0.29
1782
23522
328
139
Squares SquareSum of Mean
78
2259
69
—
3.4
469
5.5
—
13
169
2.35
—
FSource
<.001
<.001
<.001
—
.041
<.001
.007
—
<.001
<.001
0.104
—
P
denture teeth with lower cuspal angu-lations. However, no significant dif-ferences were found between 20- and 33-degree angulations for acrylic res-in and 20- and 35-degree angulations for ceramic denture teeth groups.
The total denture base area calcu-
lated by the size of the denture base specimen was 225 mm2 (15 x 15 mm). The areas of colors developed on the sheet represent the pressure transmis-sion areas. Significant differences in pressure transmission areas with re-spect to different cuspal angulations
were found in the acrylic resin (F=26, df=2, P<.001) and ceramic (F=20, df=2, P<.001) denture teeth groups. Thirty-three-degree acrylic resin denture teeth exhibited significantly larger pressure transmission areas than 20- and 0-de-gree groups. As for the ceramic den-

133February 2011
Arksornnukit et al
ture teeth group, denture teeth with greater cuspal angulations presented significantly larger pressure trans-mission areas compared to denture teeth with lower cuspal angulations (Table IV).
DISCUSSION
Differences in pressure transmis-
sion and distribution using denture teeth made of different materials with different cuspal angulations were observed in this study; in addition, interactions were observed between tooth materials and angulations with respect to the pressure transferred. Therefore, the two null hypotheses were rejected.
Denture teeth used in the present
study were selected from the same mold and manufacturer to minimize the effect of size and shape of the specimens. In addition, all denture base resin fabrication was controlled to be the same in every specimen; thus, the results were compared only with respect to the different artificial denture teeth materials. All denture teeth with different angulations were
Table III. Means of average and maximum pressure transmission (MPa) and Tam-hane analysis (20-degree denture teeth groups omitted)
Table IV. Means of average pressure, maximum pressure, and pressure transmission area for all angula-tions of acrylic resin and ceramic denture teeth groups
Average pressure transmission
0-degree acrylic resin
0-degree microfilled composite resin
0-degree ceramic
33-degree acrylic resin
33-degree microfilled composite resin
35-degree ceramic
Maximum pressure transmission
0-degree acrylic resin
0-degree microfilled composite resin
0-degree ceramic
33-degree acrylic resin
33-degree microfilled composite resin
35-degree ceramic
Groups with same uppercase letters were not significantly different at P<.05.
0.36 (0.01)
0.37 (0.02)
0.37 (0.01)
0.76 (0.04)
0.76 (0.05)
1.01 (0.06)
1.71 (0.16)
1.63 (0.11)
1.57 (0.06)
4.28 (0.63)
4.50 (0.86)
5.25 (0.77)
Mean (SD) in MPa
A
A
A
B
B
C
A
A
A
B
B
B
Tamhane AnalysisDenture Teeth
Acrylic resin
0 degree
20 degree
33 degree
Ceramic
0 degree
20 degree
35 degree
Groups with same superscript lowercase letters were not significantly different at P<.05.
0.36 (0.01)a
0.74 (0.08)b
0.76 (0.04)b
0.37 (0.01)a
0.87 (0.10)b
1.01 (0.06)c
Mean (SD) in MPaAverage Pressure
1.71 (0.16)a
4.01 (0.49)b
4.28 (0.63)b
1.57 (0.06)a
4.98 (0.60)b
5.25 (0.77)b
Mean (SD) in MPaMaximum Pressure
78.60 (14.02)a
86.00 (7.18)a
112.10 (10.73)b
68.60 (11.35)a
86.00 (10.62)b
105.10 (15.81)c
Mean (SD) in mm2Pressure Transmission area
Denture Teeth

134 Volume 105 Issue 2
The Journal of Prosthetic Dentistry Arksornnukit et al
selected from the same manufacturer, except for the 0-degree acrylic resin and 0-degree ceramic denture teeth, which were modified by the authors and manufactured according to in-formation presented in Table I. Both 20-degree acrylic resin and ceramic denture teeth were selected, flat-tened, and used as the 0-degree teeth groups as they were considered sim-pler to manipulate than their 33- and 35-degree counterparts.
The simplified models of maxillary and mandibular posterior denture teeth were fabricated with Angle’s Class I occlusal relationship in an at-tempt to simulate a normal occlusal relationship. Minor occlusal adjust-ments were made to achieve proper occlusion between maxillary and mandibular denture teeth, and this procedure is considered to be similar to clinical procedures. The same type (LLW) of pressure-sensitive sheet was used, primarily to determine the dis-tribution of pressure; therefore, the pattern of pressure distribution was clearly demonstrated in the present study (Fig. 3).
Both denture tooth materials and cuspal angulations had a significant influence on average and maximum pressure transmission, as statistically significant interactions were observed in the present study (Table II). Thirty-three-degree acrylic resin and micro-filled composite resin teeth presented about twice as much of the average pressure transferred compared to 0-degree denture teeth (Table III). In addition, 35-degree ceramic denture teeth displayed the significantly high-est average pressure in the test groups (Table III and IV). These results sug-gest that selecting proper denture tooth materials and angulations should be considered when pressure transmission under denture bases is a concern, such as when treating pa-tients with flat residual ridges.
The authors of a previous study35 discussed the role of the modulus of elasticity of denture tooth materials on pressure transmission. Denture teeth with low elastic modulus may
flex and absorb impact force and transfer less pressure to underlying structures. However, results from the present study showed that no signifi-cant differences were found in 0-de-gree denture teeth made of 3 different denture tooth materials (Table III). This finding revealed that 0-degree angulation may nullify the effect of the modulus of elasticity; this was confirmed by both the average and maximum pressure transmission re-sults (Table III).
When comparing 20-degree acryl-ic resin and ceramic denture teeth with teeth with other cuspal angulations, interesting results were observed. Twenty-degree acrylic resin denture teeth showed no significant differenc-es in average and maximum pressure compared to 33-degree acrylic resin teeth (Table IV). However, a signifi-cantly smaller pressure transmission area was observed for the 20-degree teeth (86.0 mm2) compared to the 33-degree teeth (112.1 mm2). These results suggest that 20-degree may be preferable to 33-degree acrylic resin teeth, as the smaller angula-tion resulted in smaller pressure ar-eas transferred to underlying denture bases. As for ceramic denture teeth, 20-degree teeth showed significantly lower average pressure than 35-de-gree teeth, while no significant differ-ence was found in maximum pressure compared to 35-degree teeth. Zero-degree ceramic teeth demonstrated significantly lowest average and maxi-mum pressure and smallest pressure transmission areas compared to 20- and 35-degree teeth. Zero-degree or 20-degree ceramic teeth appear to be the better choice compared to 35-de-gree teeth when ceramic denture teeth are indicated, as they showed better results in the measured parameters.
The results of the present study were in agreement with those of Chowdhary et al,17 who used the finite element analysis method to examine stress generated beneath complete dentures using denture teeth with dif-ferent cuspal angulations. The find-ings of the present study support the
concept that using denture teeth with lower or flatter cuspal angulations might be a desirable option because they transfer less force and pressure to the underlying structures. Mono-plane denture teeth, which provide less force and better pressure distri-bution, should be used in highly at-rophied alveolar ridges as they induce lower lateral forces than anatomic teeth.28,29
Most clinicians choose cusped denture teeth for balanced occlusal schemes in complete dentures, as Boucher suggested that it is easier to acquire bilateral balanced occlusion compared to cuspless teeth.22 Results from the present study suggest that choosing 33-degree acrylic resin or 33-degree microfilled composite resin denture teeth for bilateral balanced occlusion is better, because average pressure transmission was reduced when these materials and angulations were used (Table III). With respect to teeth made of acrylic resin, 20-de-gree angulations seem to be a better choice as compared to 33-degree an-gulations, as these cuspal angulations resulted in smaller pressure transmis-sion areas beneath the denture bases (Table IV). As for the monoplane oc-clusion concept, 0-degree denture teeth made of any of the 3 materials appear to be acceptable options, as there were no statistical differences in average and maximum pressure trans-mission found in the present study (Table III).
Pressure is defined as force per unit area. Matsuo et al9 suggested that alveolar bone remodeling is ini-tiated when a pressure of 27 to 68 g/cm2 is exerted on fibroblast cells. Berg10 also reported that to keep blood circulation normal, continu-ous mechanical pressure higher than 1.3 kPa should not be transferred to the denture-supporting tissues. The average and maximum pressure trans-mission observed in the present study ranged from 0.36 to 5.25 MPa (Ta-bles III and IV), which was higher than the pressures described in the previ-ously mentioned studies. However,

135February 2011
Arksornnukit et al
the size of the denture base specimen in the present study was only 225 mm2; therefore, it had a limited area to absorb the pressure. Maximum ex-tension of the denture bases within anatomical and physiological limits is strongly recommended to increase the supporting areas and minimize the pressure to the underlying bone beneath denture bases.
The present study evaluated pres-sure transmission and distribution us-ing simplified models under vertical impact loads. A limitation was that pressures beneath denture bases were investigated using only one direction of force. The simplified model used in this study consisted of only one den-ture tooth in a small square resin block with no periosteum or bone beneath the denture base. The magnitude of pressure transmission might be modi-fied in the clinical setting as dentures have more denture base area com-pared to the simplified model used in the present study. Pressure transmis-sion and distribution under maxillary and mandibular complete dentures may also be different due to denture configuration, for example, the load-sharing function of the palate in max-illary dentures. Moreover, the 0-de-gree denture teeth of the acrylic and ceramic groups were modified from their 20-degree counterparts. The occlusal surfaces of these 0-degree denture teeth groups may not be the same as other manufactured mono-plane denture teeth; therefore, pres-sure transmission beneath denture bases may be slightly different. How-ever, this in vitro study has shown that under the same controlled condi-tions, denture teeth with smaller cus-pal angulations transferred less force through the denture base and, there-fore, may be considered preferable for compromised patients. Further stud-ies with conditions that more closely simulate the oral environment, as well as clinical studies, would be useful for evaluating and understanding pres-sure beneath maxillary and mandibu-lar dentures.
CONCLUSIONS
Within the limitations of the pres-ent study, the following conclusions were drawn.
1. Signif icant interactions were observed between denture tooth ma-terials and cuspal angulations with respect to average pressure (P<.001) and maximum pressure (P=.007) transmission.
2. Zero-degree denture teeth showed significantly lower average and maxi-mum pressure transmission compared to 33- and 35-degree denture teeth for all 3 denture tooth materials evaluated (P<.001).
3. Denture teeth with greater cuspal angulations demonstrated significantly higher average pressure transmission for all ceramic denture teeth groups (P<.05).
REFERENCES
1. Yoshida M, Sato Y, Akagawa Y, Hiasa K. Correlation between quality of life and denture satisfaction in elderly com-plete denture wearers. Int J Prosthodont 2001;14:77-80.
2. Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: a mixed-longitudinal study covering 25 years. J Prosthet Dent 1972;27:120-32.
3. Campbell RL. A comparative study of the resorption of the alveolar ridges in denture-wearers and non-denture-wearers. J Am Dent Assoc 1960;60:143-53.
4. Bergman B, Carlsson GE. Clinical long-term study of complete denture wearers. J Prosthet Dent 1985;53:56-61.
5. Atwood DA. Reduction of residual ridges: a major oral disease entity. J Prosthet Dent 1971;26:266-79.
6. Kordatzis K, Wright PS, Meijer HJA. Poste-rior mandibular residual ridge resorption in patients with conventional dentures and implant overdentures. Int J Oral Maxillofac Implants 2003;18:447-52.
7. Roberts WE, Huja S, Roberts JA. Bone modeling: biomechanics, molecular mecha-nisms, and clinical perspectives. Semin Orthod 2004;10:123-61.
8. Ortman HR. Factors of bone resorp-tion of the residual ridge. J Prosthet Dent 1962;12:429-40.
9. Nakago-Matsuo C, Matsuo T, Nakago T. Intracellular calcium response to hydraulic pressure in human periodontal ligament fibroblasts. Am J Orthod Dentofac Orthop 1996;109:244-8.
10.Berg T Jr, Chase WW, Ray K. Denture base pressure tests. J Prosthet Dent 1967;17:540-8.
11.Appelbaum M. Theories of posterior tooth selection: porcelain versus acrylic. Dent Clin North Am 1984;28:299-306.
12.Mercier P, Bellavance F. Effect of artificial tooth material on mandibular residual ridge resorption. J Can Dent Assoc 2002;68:346-50.
13.Ohguri T, Kawano F, Ichikawa T, Matsu-moto N. Influence of occlusal scheme on the pressure distribution under a complete denture. Int J Prosthodont 1999;12:353-8.
14.Inoue S, Kawano F, Nagao K, Matsumoto N. An in vitro study of the influence of oc-clusal scheme on the pressure distribution of complete denture supporting tissues. Int J Prosthodont 1996;9:179-87.
15.Sutton AF, Glenny AM, McCord JF. Interventions for replacing missing teeth: denture chewing surface designs in edentu-lous people. Cochrane Database Syst Rev 2005:CD004941.
16.Sutton AF, McCord JF. A randomized clini-cal trial comparing anatomic, lingualized, and zero-degree posterior occlusal forms for complete dentures. J Prosthet Dent 2007;97:292-8.
17.Chowdhary R, Lekha K, Patil NP. Two-dimensional finite element analysis of stresses developed in the supporting tissues under complete dentures using teeth with different cusp angulations. Gerodontology 2008;25:155-61.
18.Berg E. The influence of cusped and cusp-less teeth on patient satisfaction with com-plete dentures. A 2-year follow-up study. J Dent 1988;16:269-76.
19.Sutton AF, Worthington HV, McCord JF. RCT comparing posterior occlusal forms for complete dentures. J Dent Res 2007;86:651-5.
20.Clough HE, Knodle JM, Leeper SH, Pudwill ML, Taylor DT. A comparison of lingual-ized occlusion and monoplane occlusion in complete dentures. J Prosthet Dent 1983;50:176-9.
21.Rehmann P, Balkenhol M, Ferger P, Wost-mann B. Influence of the occlusal concept of complete dentures on patient satisfac-tion in the initial phase after fitting: bilat-eral balanced occlusion vs canine guidance. Int J Prosthodont 2008;21:60-1.
22.Boucher CO. Complete denture prosth-odontics--the state of the art. J Prosthet Dent 1975;34:372-83.
23.Lang BR. Complete denture occlusion. Dent Clin North Am 1996;40:85-101.
24.Grubwieser G, Flatz A, Grunert I, Kofler M, Ulmer H, Gausch K, et al. Quantitative analysis of masseter and temporalis EMGs: a comparison of anterior guided versus balanced occlusal concepts in patients wearing complete dentures. J Oral Rehabil 1999;26:731-6.
25.Winter CM, Woelfel JB, Igarashi T. Five-year changes in the edentulous mandible as determined on oblique cephalometric radiographs. J Dent Res 1974;53:1455-67.
26. Winter CM, Woelfel JB, Igarashi T. Five-year cephalometric study of mandibular ridge resorption with different posterior occlusal forms. Part I. Denture construc-tion and initial comparison. J Prosthet Dent 1976;36:602-23.
27.Jones PM. The monoplane occlusion for complete dentures. J Am Dent Assoc 1972;85:94-100.

136 Volume 105 Issue 2
The Journal of Prosthetic Dentistry Arksornnukit et al
28.Lopuck S, Smith J, Caputo A. Photoelastic comparison of posterior denture occlu-sions. J Prosthet Dent 1978;40:18-22.
29.Swoope CC, Kydd WL. The effect of cusp form and occlusal surface area on denture base deformation. J Prosthet Dent 1966;16:34-43.
30.Kubo K, Kawata T, Suenaga H, Yoda N, Shigemitsu R, Ogawa T, et al. Development of in vivo measuring system of the pressure distribution under the denture base of removable partial denture. J Prosthodont Res 2009;53:15-21.
31.Cutright DE, Brudvik JS, Gay WD, Selt-ing WJ. Tissue pressure under complete maxillary dentures. J Prosthet Dent 1976;35:160-70.
32.Watson CJ, Huggett R. Pressures recorded at the denture base-mucosal surface inter-face in complete denture wearers. J Oral Rehabil 1987;14:575-89.
33.Miyaura K, Morita M, Matsuka Y, Yamashita A, Watanabe T. Rehabilitation of biting abilities in patients with different types of dental prostheses. J Oral Rehabil 2000;27:1073-6.
34.Miyaura K, Matsuka Y, Morita M, Yamashita A, Watanabe T. Comparison of biting forces in different age and sex groups: a study of biting efficiency with mo-bile and non-mobile teeth. J Oral Rehabil 1999;26:223-7.
35.Phunthikaphadr T, Takahashi H, Arksorn-nukit M. Pressure transmission and distri-bution under impact load using artificial denture teeth made of different materials. J Prosthet Dent 2009;102:319-27.
36.Anusavice KJ. Phillips’science of dental ma-terials. 11th ed. Philadelphia: WB Saunders; 2003. p.721-58, 371-4.
37.Patterson R, Pogue D, Viegas S. The effects of time and light exposure on contact and pressure measurements using Fuji prescale film. Iowa Orthop J 1997;17:64-9.
Corresponding author:Dr Mansuang Arksornnukit Chulalongkorn UniversityBangkok, 10300THAILANDFax: +662 218 8534E-mail: [email protected]
AcknowledgmentsThe authors thank Shofu, Inc. Kyoto, Japan, for their generous donation of the artificial denture teeth used in the study. The authors also extend special thanks to Mr. Daniel Gill for his invaluable help with the final language editing.
Copyright © 2010 by the Editorial Council for The Journal of Prosthetic Dentistry.
Noteworthy Abstracts of the Current Literature
Mandibular overdentures retained by two implants: 10-year results from a crossover clinical trial comparing ball-socket and bar-clip attachments
Cune M, Burgers M, van Kampen F, de Putter C, van der Bilt A. Int J Prosthodont 2010;23:310-7.
Purpose. The aim of this study was to evaluate patient satisfaction and clinical and prosthetic outcomes of two-im-plant mandibular overdenture treatment with different attachment types after 10 years of function.
Materials and Methods. In a crossover clinical trial, 18 edentulous subjects with complaints regarding their man-dibular dentures received two implants and a new denture with magnet, ball-socket, or bar-clip attachments that were applied in a random order. At the end of the experiment, the attachment type of their choosing was fitted in the overdenture. After 10 years, 7 subjects with a ball-socket and 7 subjects with a bar-clip attachment were available for evaluation. The same questionnaire from 10 years before was completed, and subjects were asked to express their overall appreciation of their dentures on a visual analog scale (VAS). Six scales of denture complaints were construct-ed. Mean scale and VAS scores between initial evaluation and after 10 years were compared. In addition, marginal probing depths, Bleeding Index, and radiographic marginal bone loss were assessed.
Results. There was no marked difference in satisfaction between subjects with ball-socket– and bar-clip–retained two-implant mandibular overdentures at initial evaluation and after 10 years of function.
Conclusion. Patients’ appreciation of their implant-retained denture was and remained high over time. Clinical pa-rameters revealed healthy mucosal conditions and stable marginal bone levels, determined radiographically. Probing depths around implants provided with ball-socket attachments were slightly shallower than those with bar-clip attach-ments after 10 years of function (P < .05).
Reprinted with permission of Quintessence Publishing.