
8526708 Renal Anatomy
51
Renal Anatomy and Physiology By: Wong Ann Cheng MD (UKM) MRCPCH (UK)
-
Upload
fluturefluturas -
Category
Documents
-
view
219 -
download
0
Transcript of 8526708 Renal Anatomy
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 1/51
Renal Anatomy and
PhysiologyBy: Wong Ann Cheng
MD (UKM) MRCPCH (UK)
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 2/51
Renal Anatomy and Physiology
Macroscopic anatomy Embrology
Gross
Procedures Investigations
Microscopic anatomy Glomerular
Tubular
Physiology
Excretory function
Nitrogenous metabolic
waste: urea, uric acid, creat
Homeostatic function
Water and salt regulation
Renin angiotensin
mechanism
Acid/ base balance
Endocrine function
Erythropoeitin
Prostaglandin
Calcitrol

7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 3/51
Embrology
Early development andevolution
Pronephros
Mesonephros
Metanephros
Ascent and abnormalities
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 4/51
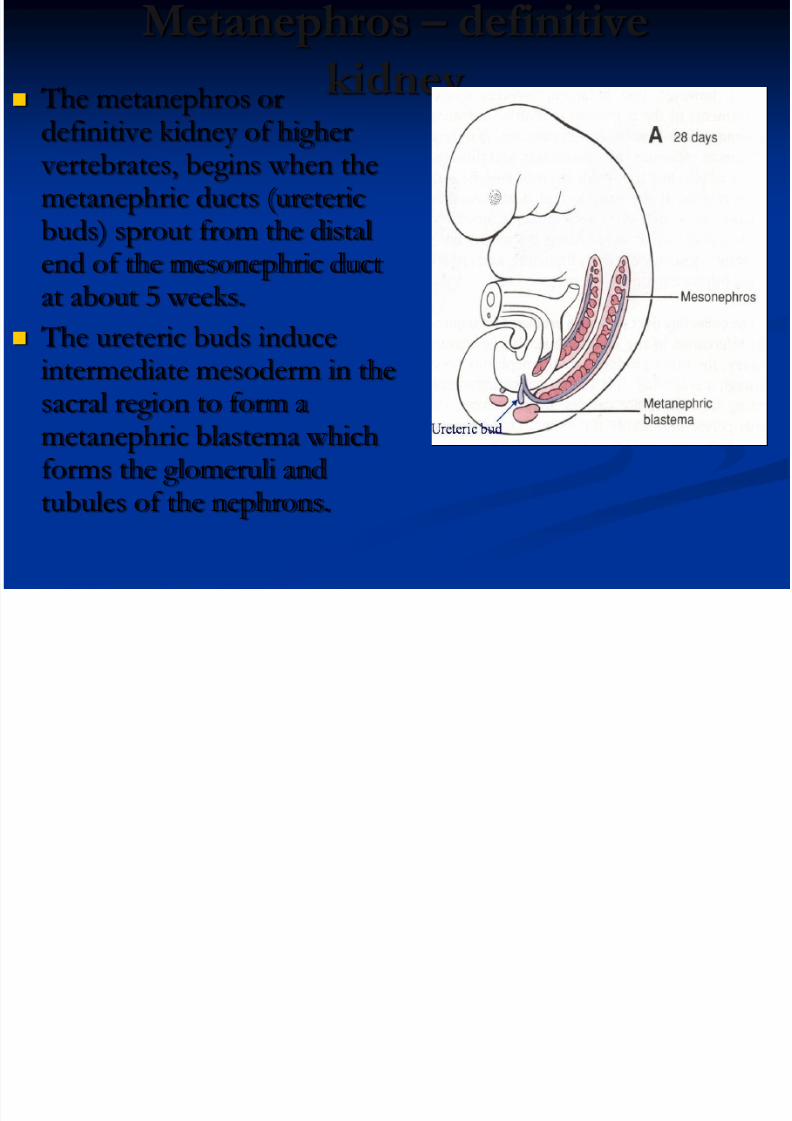
Metanephros –
definitive
kidney The metanephros or
definitive kidney of higher vertebrates, begins when themetanephric ducts (uretericbuds) sprout from the distal
end of the mesonephric ductat about 5 weeks.
The ureteric buds induceintermediate mesoderm in the
sacral region to form ametanephric blastema whichforms the glomeruli andtubules of the nephrons.
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 5/51
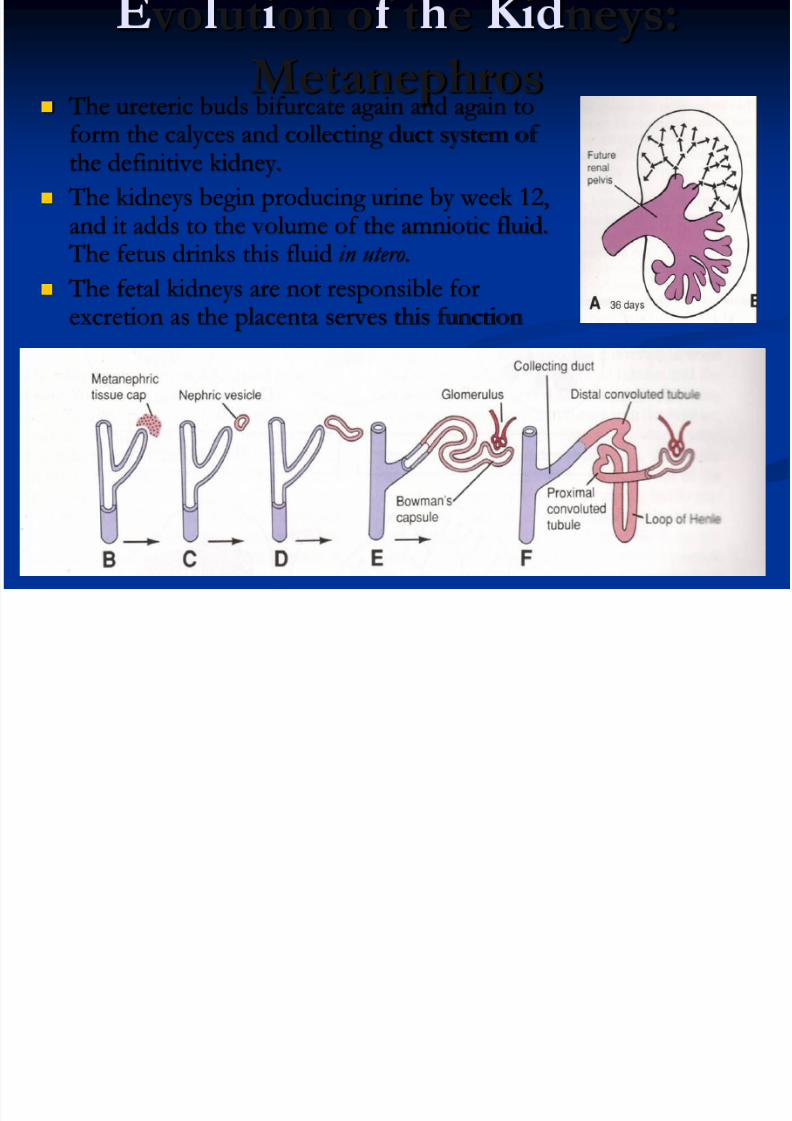
vo ut on o t e neys:Metanephros
The ureteric buds bifurcate again and again to
form the calyces and collecting duct system of the definitive kidney.
The kidneys begin producing urine by week 12,and it adds to the volume of the amniotic fluid.
The fetus drinks this fluid in utero.
The fetal kidneys are not responsible forexcretion as the placenta serves this function
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 6/51
Ascent of the
Kidneys
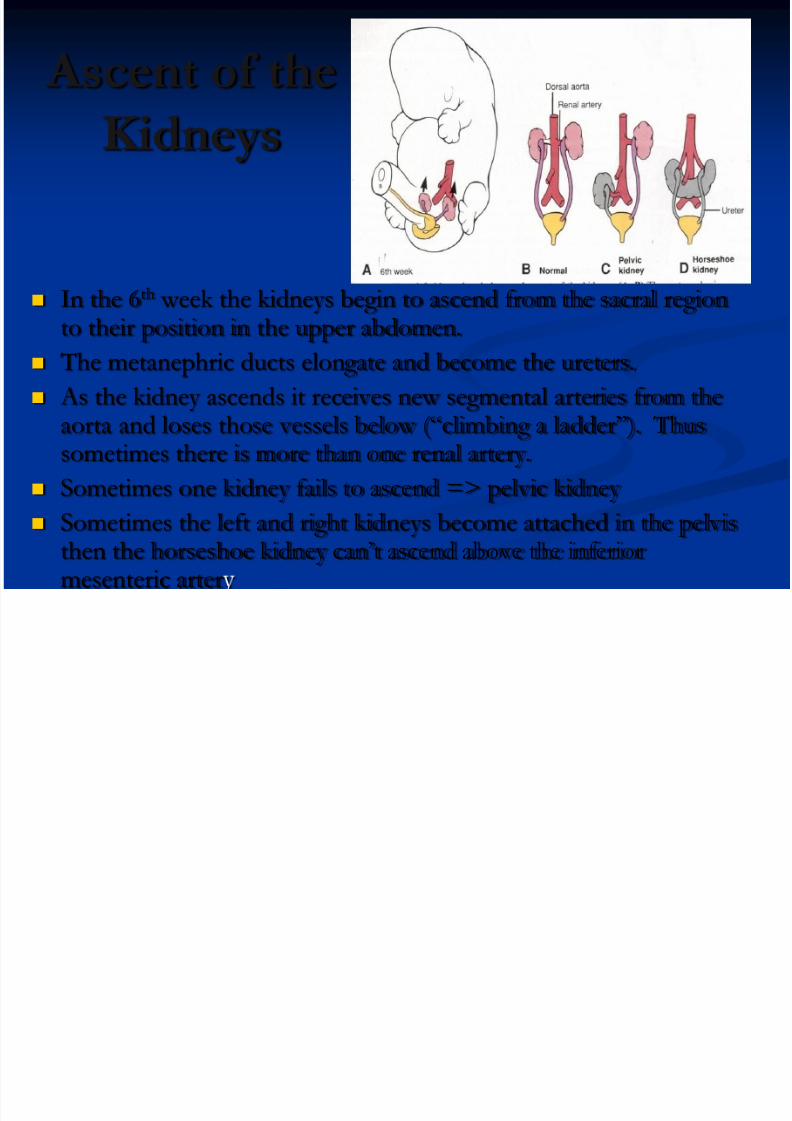
In the 6th week the kidneys begin to ascend from the sacral regionto their position in the upper abdomen.
The metanephric ducts elongate and become the ureters.
As the kidney ascends it receives new segmental arteries from theaorta and loses those vessels below (“climbing a ladder”). Thussometimes there is more than one renal artery.
Sometimes one kidney fails to ascend => pelvic kidney
Sometimes the left and right kidneys become attached in the pelvis
then the horseshoe kidney can’t ascend above the inferiormesenteric arter
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 7/51
Position of
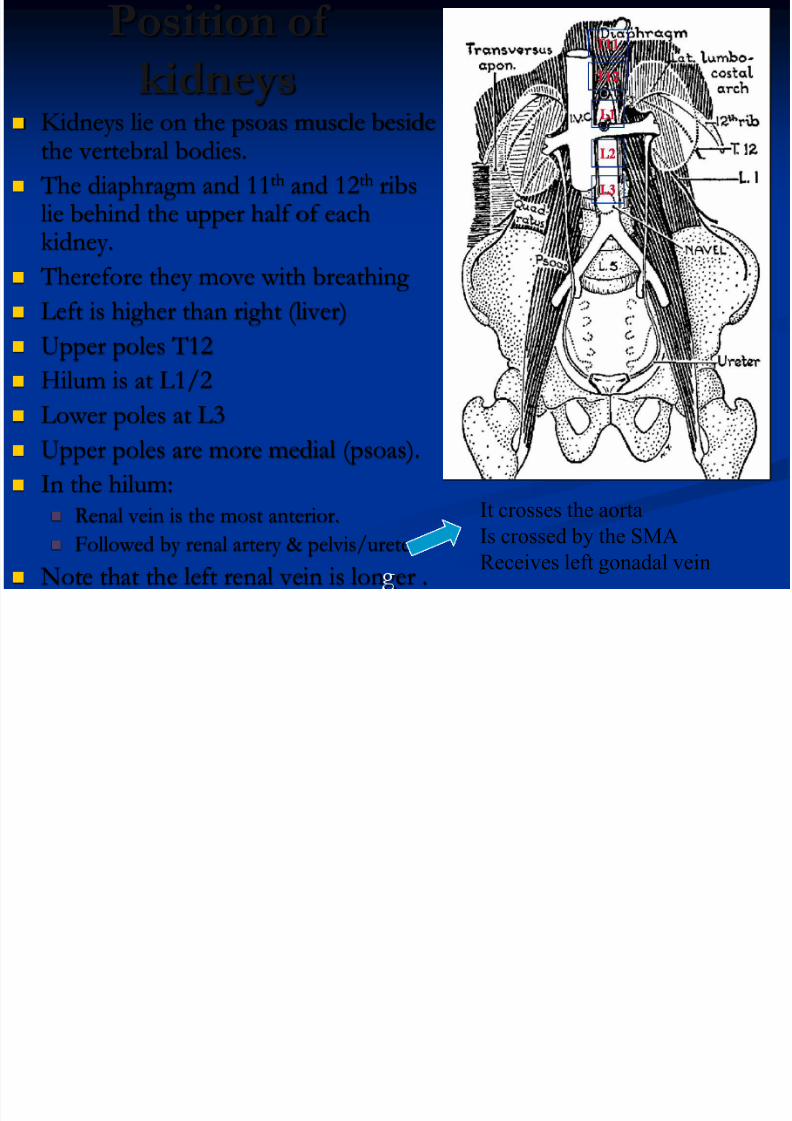
kidneys Kidneys lie on the psoas muscle beside
the vertebral bodies.
The diaphragm and 11th and 12th ribslie behind the upper half of eachkidney.
Therefore they move with breathing Left is higher than right (liver)
Upper poles T12
Hilum is at L1/2
Lower poles at L3 Upper poles are more medial (psoas).
In the hilum: Renal vein is the most anterior.
Followed by renal artery & pelvis/ureter Note that the left renal vein is lon er .
It crosses the aorta
Is crossed by the SMA
Receives left gonadal vein
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 8/51
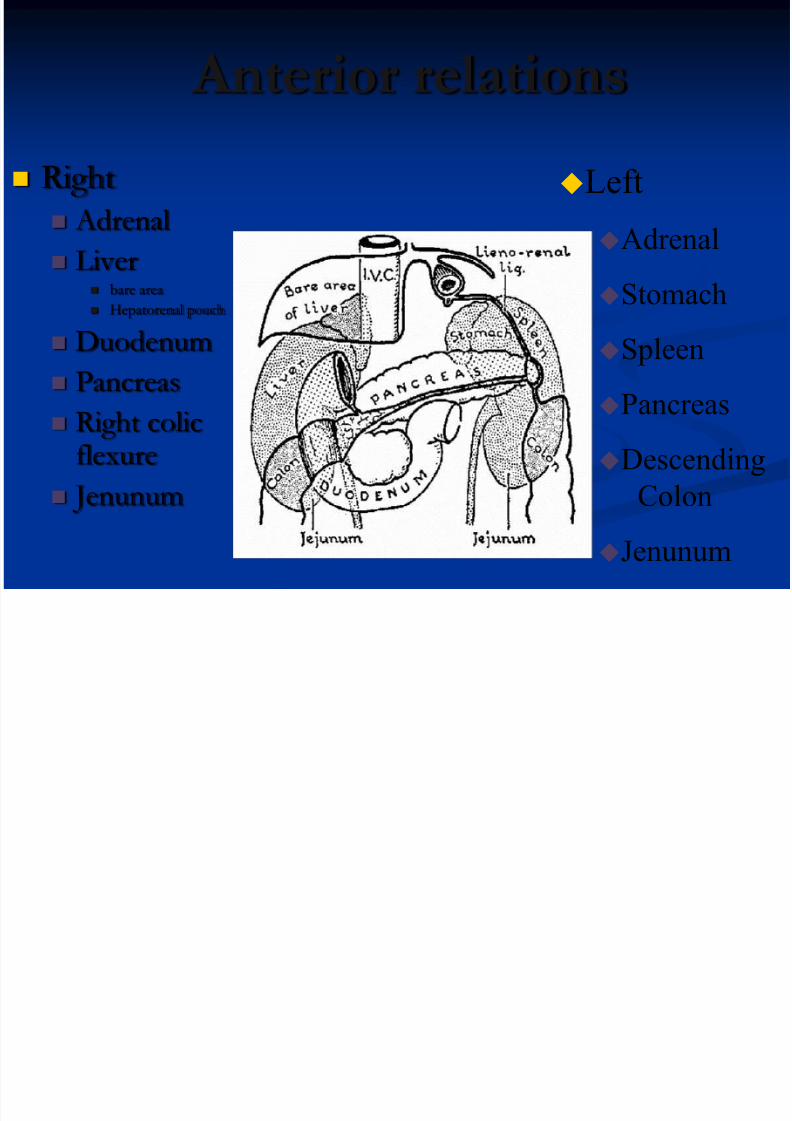
Anterior relations
Right Adrenal
Liver bare area
Hepatorenal pouch
Duodenum
Pancreas
Right colicflexure
Jenunum
Left
Adrenal
Stomach
Spleen
PancreasDescending
Colon
Jenunum
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 9/51
Macroscopic anatomy
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 10/51
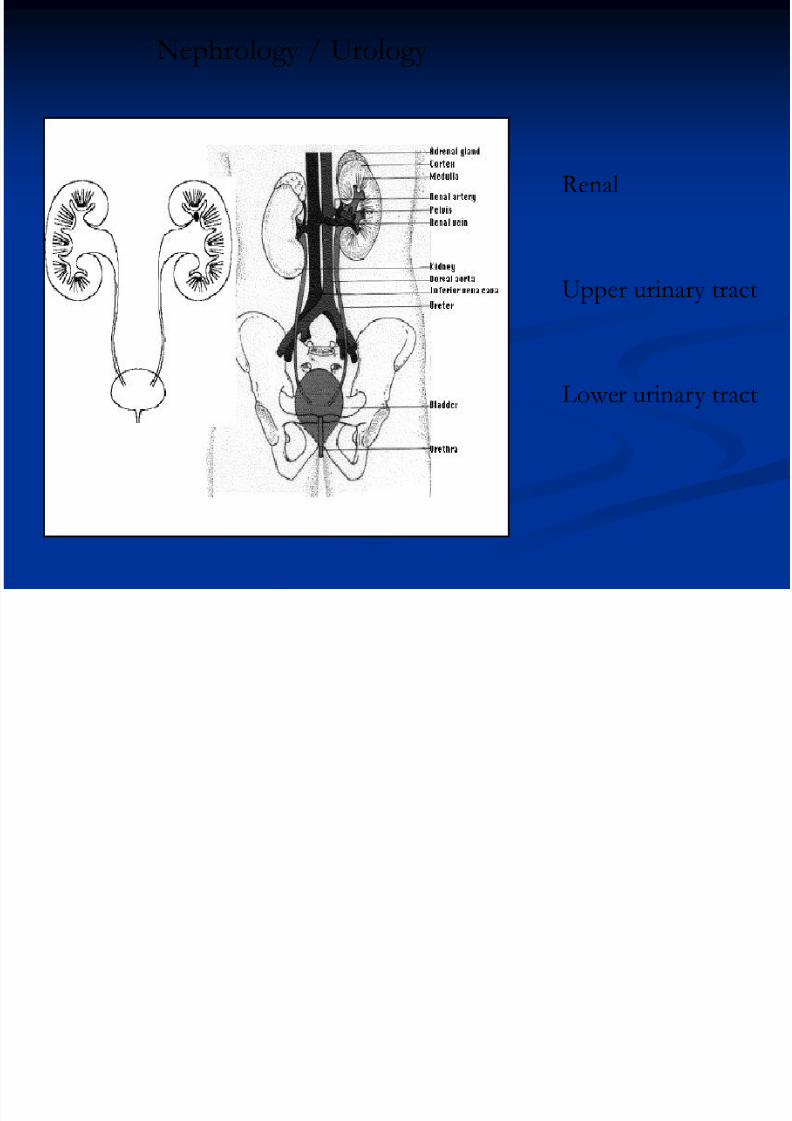
Upper urinary tract
Renal
Lower urinary tract
Nephrology / Urology
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 11/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 12/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 13/51

7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 14/51
Retroperitoneal organ
Weight: 150gm each
Size: ~clenched fist sizeLocation
Right: hilum at L1-2
Left: hilum at L1
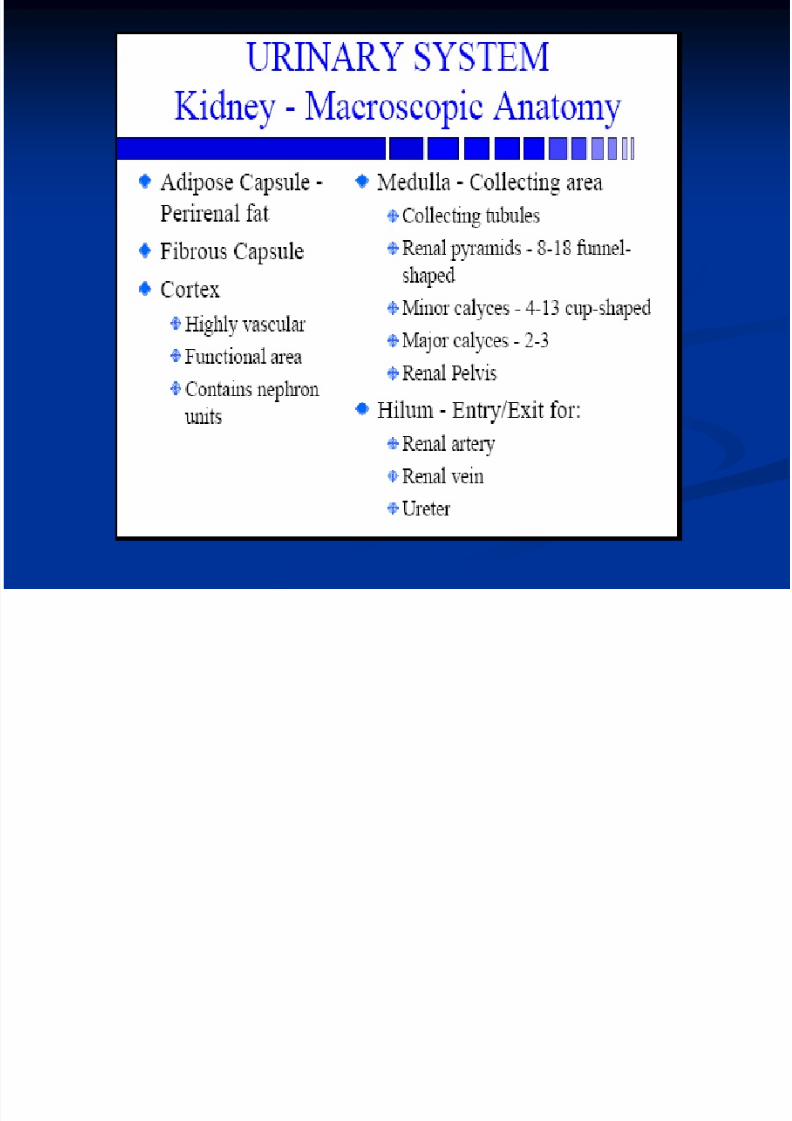
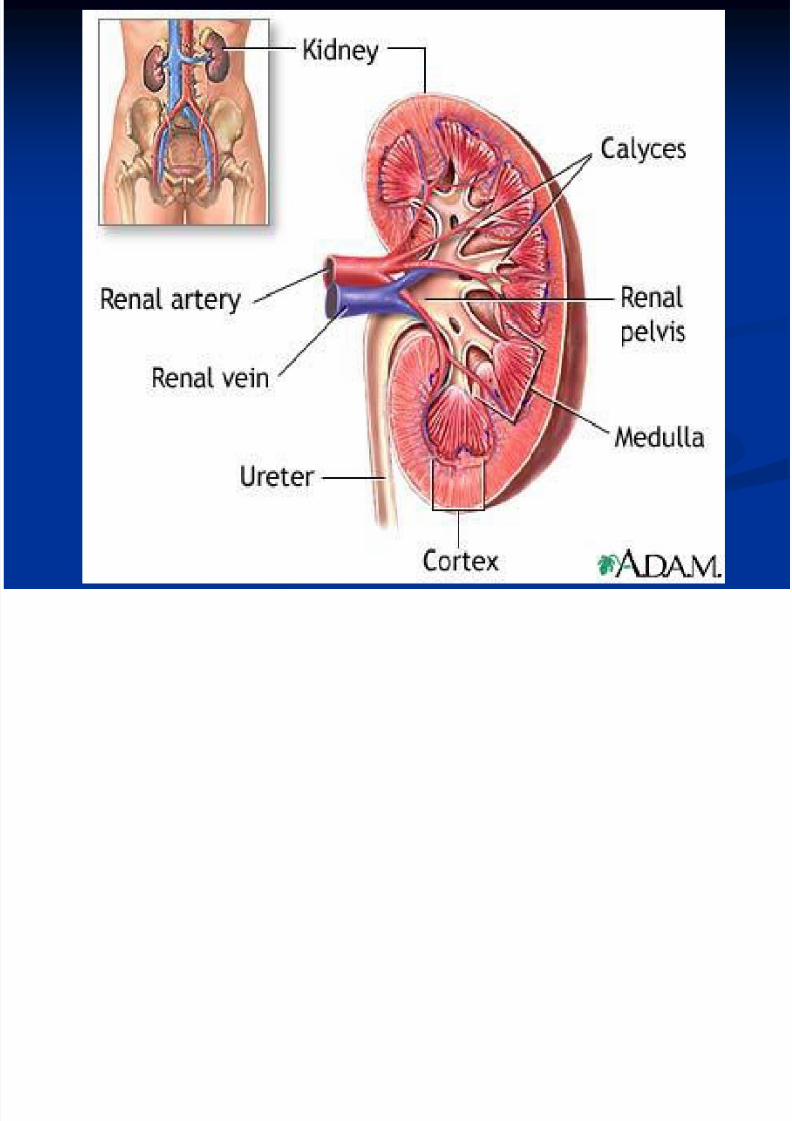
Divided into cortex and medulla
Each ~1million unit nephrons and kidney cannotregenerate new nephrons.
Physiologic anatomy
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 15/51
Two Paired Organs:
Early in pregnancy, the kidneys become two distinct but paired organs.
(1 in 1,000) only one kidney develops called congenital agenesis .
Shaped Like Beans:
The kidneys are bean shaped.
(1 in 400), the two kidneys fuse into a single horseshoe kidney
Located in Your Lower Back:
The kidneys lie in the retroperitoneum on either side of the spine.
Some people are born with ectopic kidney , not proper location.
Roughly the Size of Your Fist: On the average, the kidneys are about 11-12 cm in length, 7-8 cm wide, 2-
3 cm thick and weigh about 1/4 to 1/3 pound each.
If large, it suggests congestion or inflammation.
If small, it suggests scarring.
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 16/51
Microscopic anatomy
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 17/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 18/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 19/51
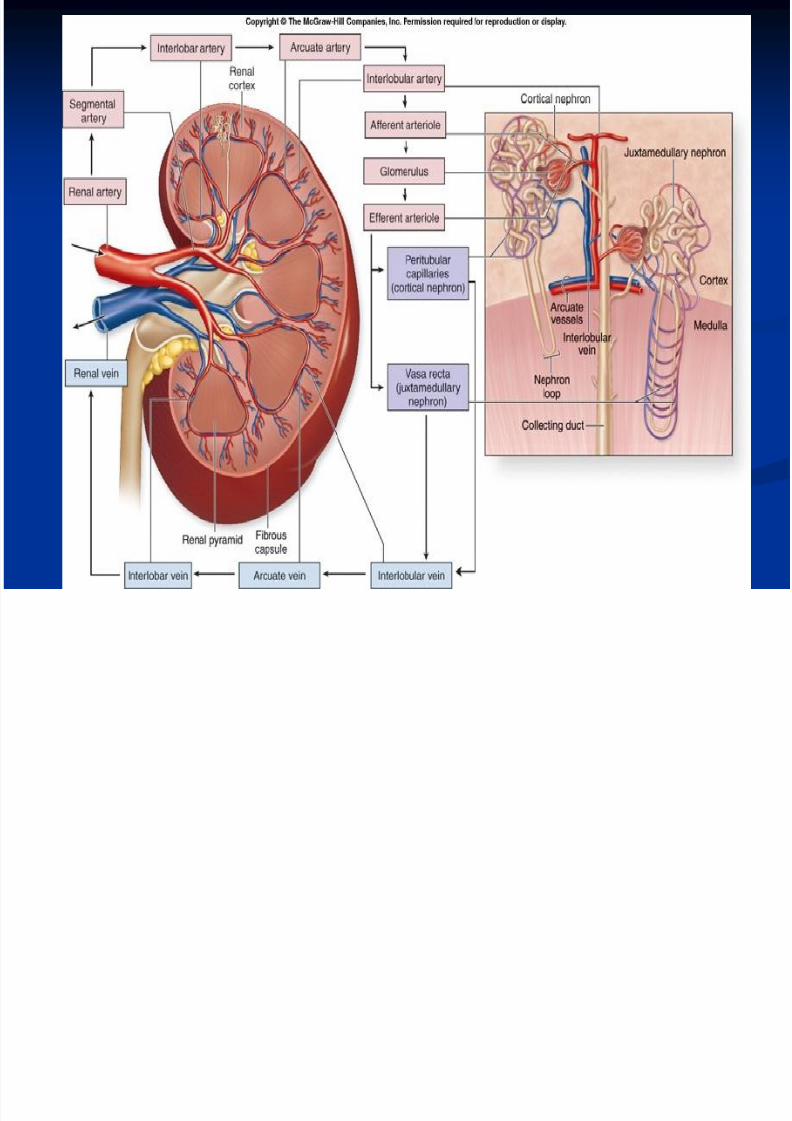
Total blood flow ~25% cardiac output.(1.2L/min)Renal
artery segmentalinterlobararcuateinterlobularafferent
Glomerulusefferent peritubular (vasa recta) veins
2 capillary bedsHigh presure system
hydrostatic pressure 60mmHg minus (32mmHg oncotic pressure +18 mmHg bowman hydrostatic pressure)
Renal cortex receives the most of the blood flow.
Renal medulla only receives 1-2% total blood flow
Renal blood supply
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 20/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 21/51

7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 22/51
GFR depends on
Starling force net pressure
1= capillary hydrostatic pressure.
2= bowman capsule
hydrostatic pressure
3= capillary oncotic pressure
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 23/51
GFR depends on
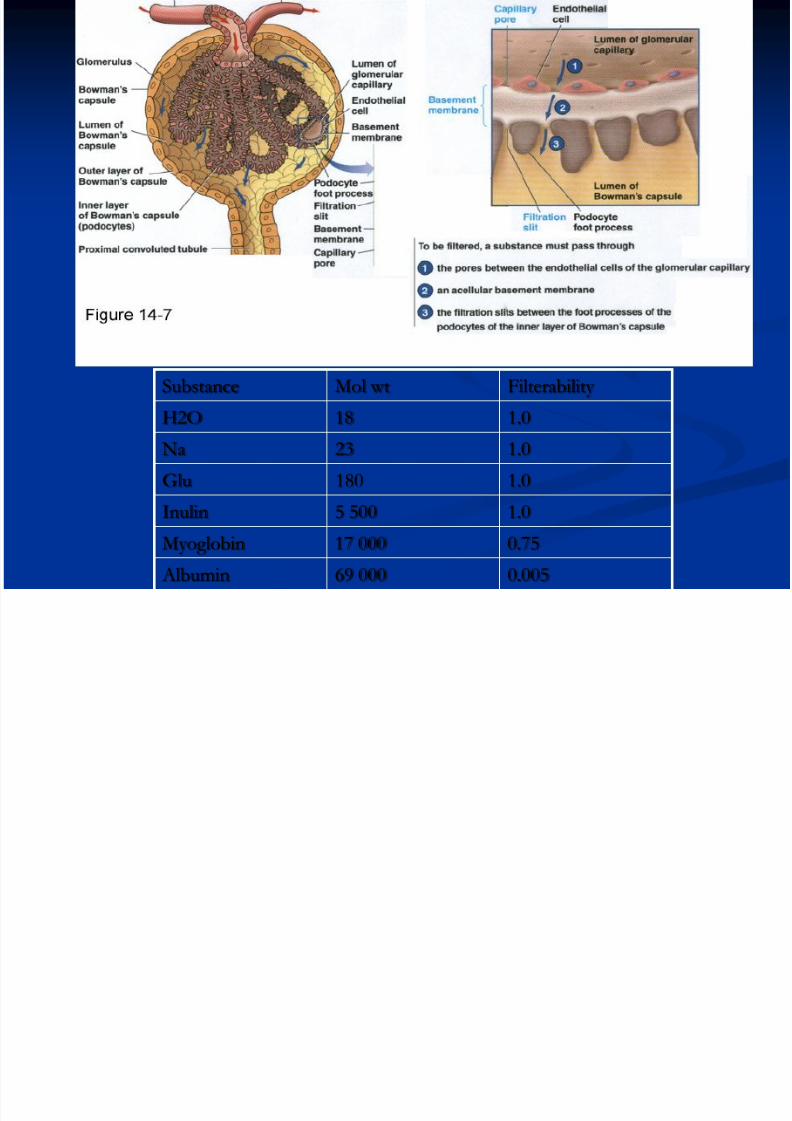
1. Glomerular permeability
-capillary and bowman capsule endothelium, glomerular basement
mambrane.
2. Number of functioning glomeruli and total capillary surface area
3. Glomerular capillary plasma flow
ultrafiltrate: plasma minus protein/fat
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 24/51
Use of clearance method to quantify
kidney function
The rates at which different substance are
cleared from plasma provide a useful way of
quantifying the effectiveness of which the
kidney excrete various substances
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 25/51
Renal clearance of a substance
Volume of plasma completely cleared of the
substance by the kidney per unit time
Provides a useful way to quantify the excretory
function of the kidneys
Can be used to quantify the rate at which blood
flow through the kidneys as well as the basic
function of the kidney, glomerular filtration rate,tubular reabsorption and tubular secretion
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 26/51
Cs x Ps = Us x Vs
Cs = clearance rate of a substance s
Ps = plasma concentration of the substance
V = urine flow rate Us = urine concentration of the substance
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 27/51
Cs = Us x V / Ps
Renal clearance of a substance is calculated from
the urinary excretion rate (Us x V) of the
substance divided by its plasma concentration
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 28/51
Inulin clearance
Can be used to estimate GFR
Substance existed that was freely filtered, not
absorped or secreted by the renal tubules, then
the rate at which the substance was excreted in
the urine (Us x V) is equal the rate at which the
substance was filtered by the kidneys (GFR x Ps)
GFR x Ps = Us x V
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 29/51
GFR = US x V / Ps = Cs
Inulin – polysaccharide molecule which
molecular rate of 5200
Not produced in the body
Found in the roots of certain plants.
Must be administered IV to a patient to measure
GFR

7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 30/51
Other substances used to estimate
GFR
Radioactive iothalamate
Creatinine
By product of skeletal muscle metabolism
Present in plasma at relatively constant concentration
Does not require IV infusion
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 31/51
Creatinine clearance
Most widely used method for estimating GFR clinically
Creatinine not a perfest marker for GFR
A small amount is excreted by the tubules
The amount of creatinine excreted in the urine slightly exceeds the amount filtered
Overestimation of the plasma concentration
The creatinine clearance provides a reasonable estimateof the GFR

7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 32/51
Formula
GFR ( total plasma volume/min from capillary to bowman capsule ) 38× Ht( cm )/ plasma Creatinine (mcmol/L)
Normal adult- 120ml/min/1.73m2
Creat. clearance ( plasma volume removed /min by kidney ) Urine creatinine (mmol/L) × Urine volume (ml/min)/
plasma creatinine(mmol/L)
Normal: ♂ 90-140ml/min
♀ 80-125ml/min
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 33/51
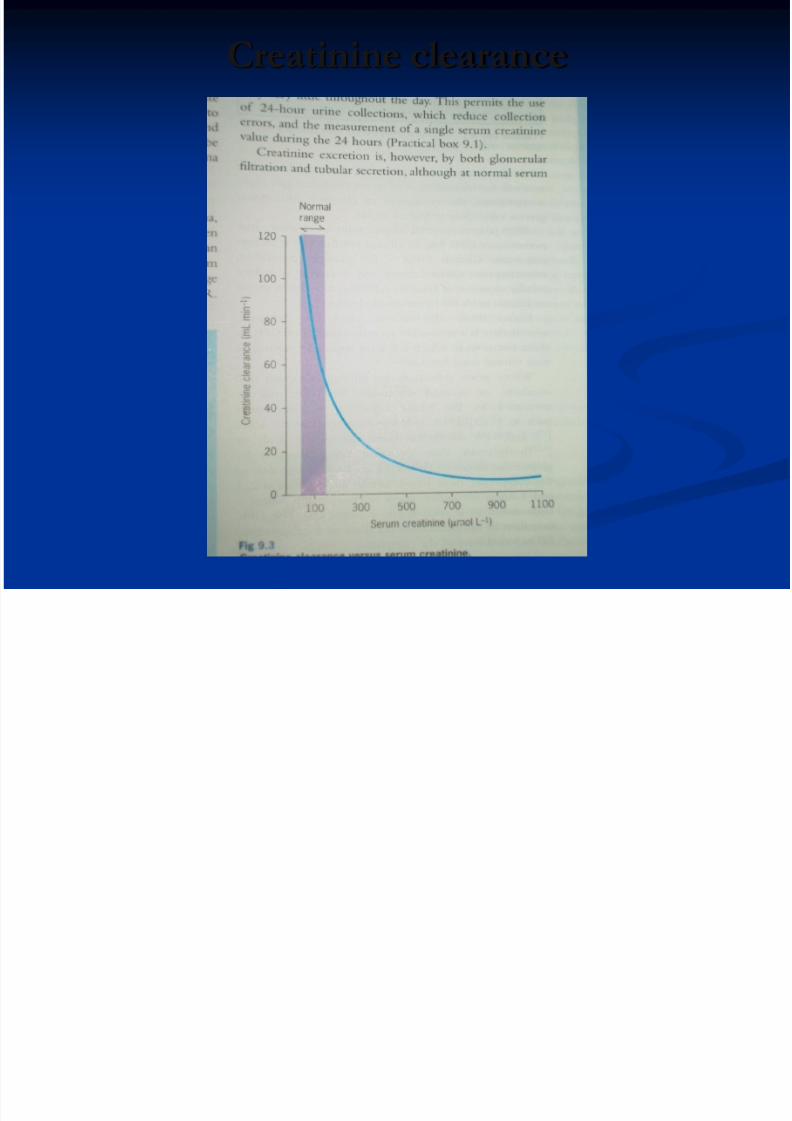
Creatinine clearance
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 34/51
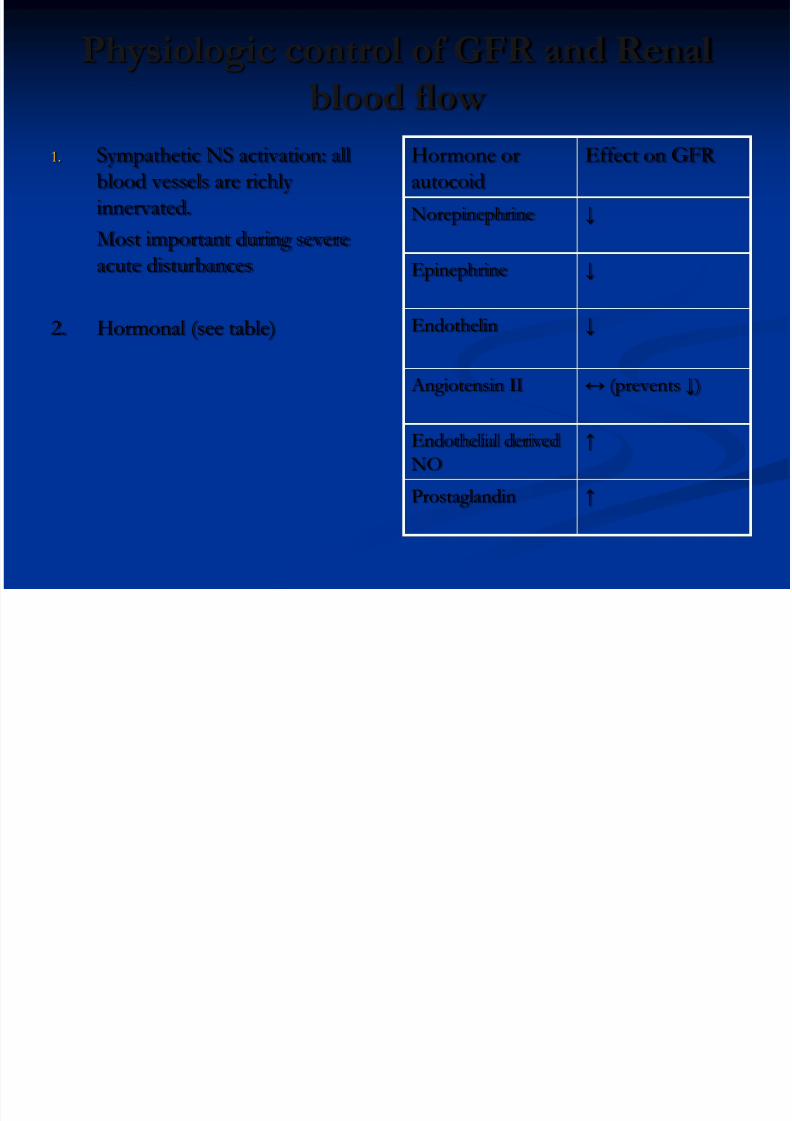
Physiologic control of GFR and Renal
blood flow
1. Sympathetic NS activation: all
blood vessels are richly
innervated.
Most important during severe
acute disturbances
2. Hormonal (see table)
Hormone or
autocoid
Effect on GFR
Norepinephrine ↓
Epinephrine ↓
Endothelin ↓
Angiotensin II ↔ (prevents ↓)
Endothelial derived
NO
↑
Prostaglandin ↑
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 35/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 36/51
Renin Angiotensin Aldosterone
System
Powerful mechanism for controlling pressure
Renin: small protein released by kidneys when
arterial pressure falls too low
Synthesized and stored in an inactive form called
prorenin in the JG cells of the kidneys
JG cells are modified smooth muscle cells located in
the walls of the afferent arterioles immediately proximal to the glomeruli
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 37/51
Two principal effects of
Angiotensin II that can elevate AP
Vasoconstriction – occursrapidly Intense in the arterioles
and less extent in veins
Constriction in arteriolesincreases peripheralresistance, raising AP
Mild constriction in veins
promotes increase venousreturn to the heart,helping the heart pumpagainst increase pressure
Decreased excretion of both salt and water – slowly increases the ECF
volume, increases AP
over period of hours anddays Even more powerful than
acute vasoconstrictor
mechanism in eventually returning AP back tonormal
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 38/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 39/51
Procedure anatomy
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 40/51
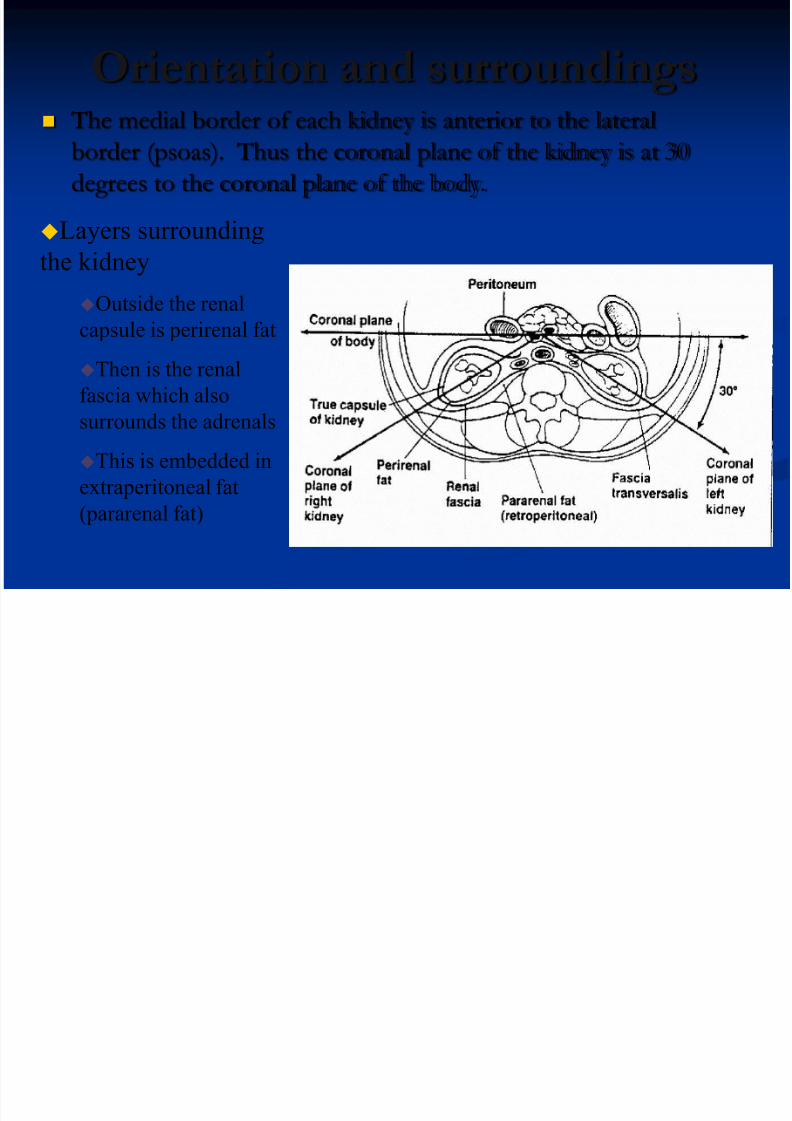
Orientation and surroundings The medial border of each kidney is anterior to the lateral
border (psoas). Thus the coronal plane of the kidney is at 30degrees to the coronal plane of the body.
Layers surrounding
the kidney
Outside the renal
capsule is perirenal fat
Then is the renal
fascia which also
surrounds the adrenals
This is embedded in
extraperitoneal fat
(pararenal fat)
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 41/51
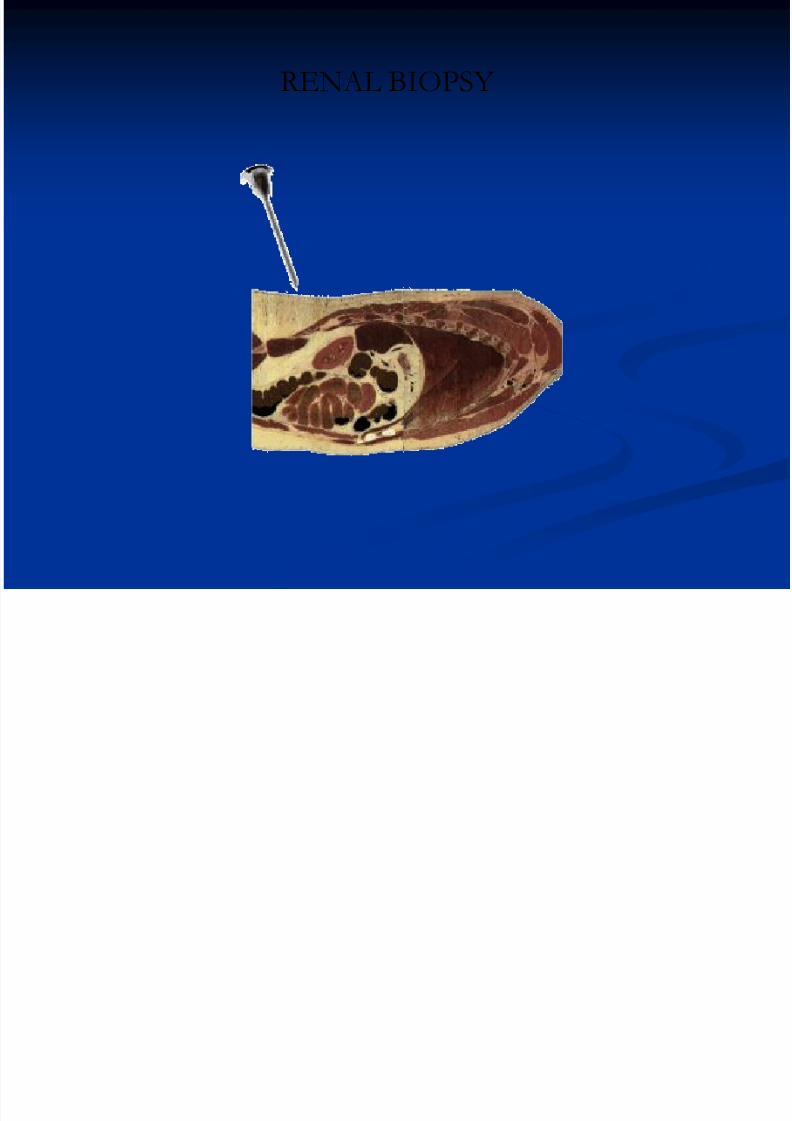
RENAL BIOPSY
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 42/51
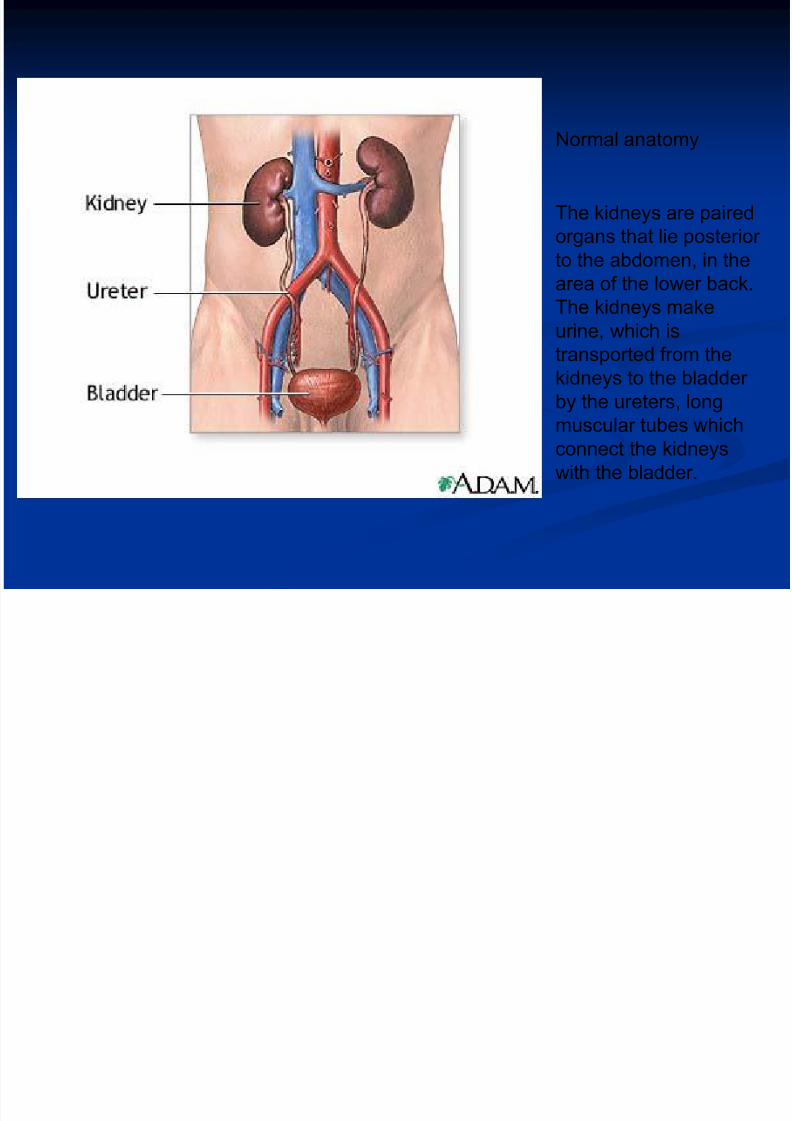
Normal anatomy
The kidneys are paired
organs that lie posterior
to the abdomen, in the
area of the lower back.The kidneys make
urine, which is
transported from the
kidneys to the bladder
by the ureters, long
muscular tubes whichconnect the kidneys
with the bladder.
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 43/51
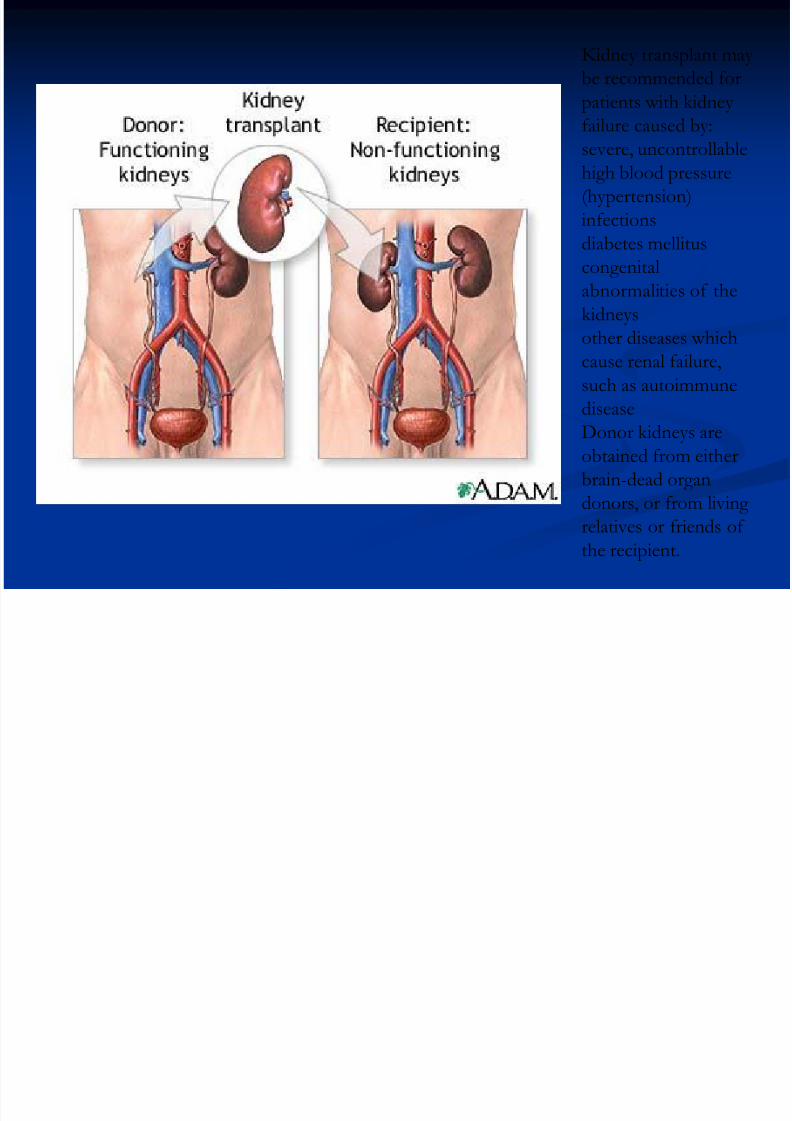
Kidney transplant may
be recommended for
patients with kidney
failure caused by:
severe, uncontrollablehigh blood pressure
(hypertension)
infections
diabetes mellitus
congenital
abnormalities of thekidneys
other diseases which
cause renal failure,
such as autoimmune
disease
Donor kidneys are
obtained from either
brain-dead organ
donors, or from living
relatives or friends of
the recipient.
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 44/51
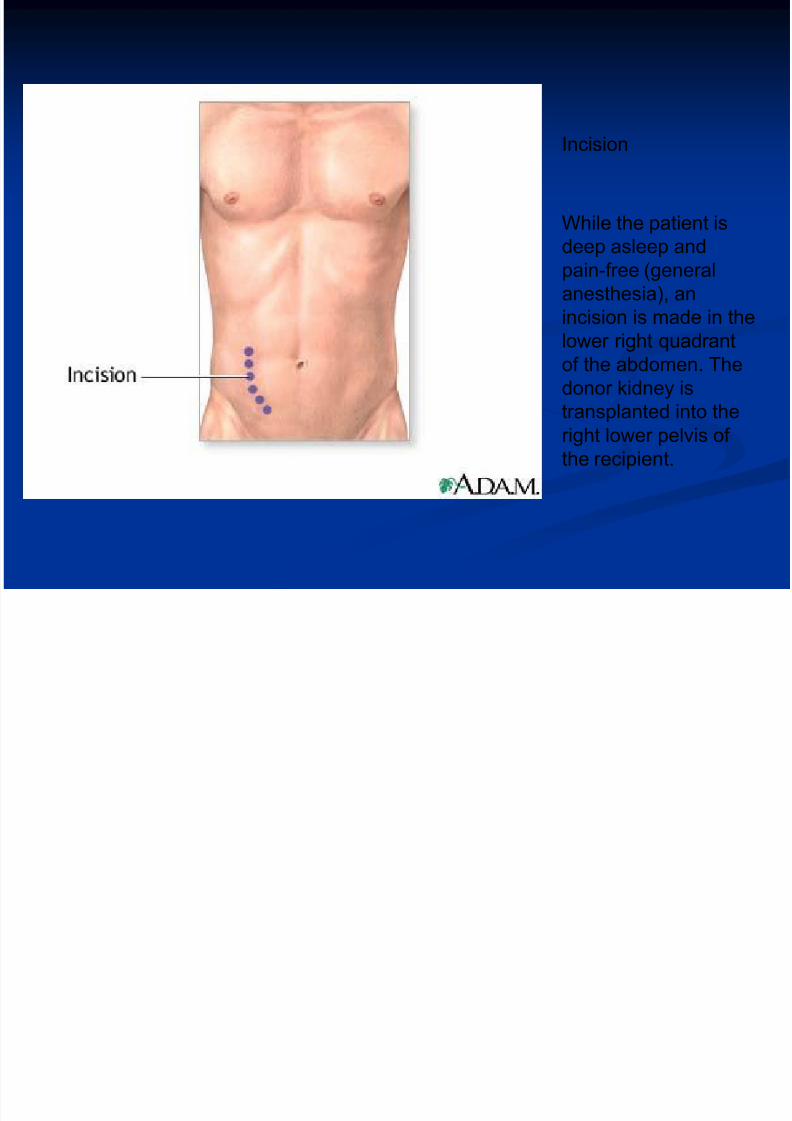
Incision
While the patient is
deep asleep and
pain-free (general
anesthesia), an
incision is made in the
lower right quadrant
of the abdomen. The
donor kidney is
transplanted into theright lower pelvis of
the recipient.
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 45/51
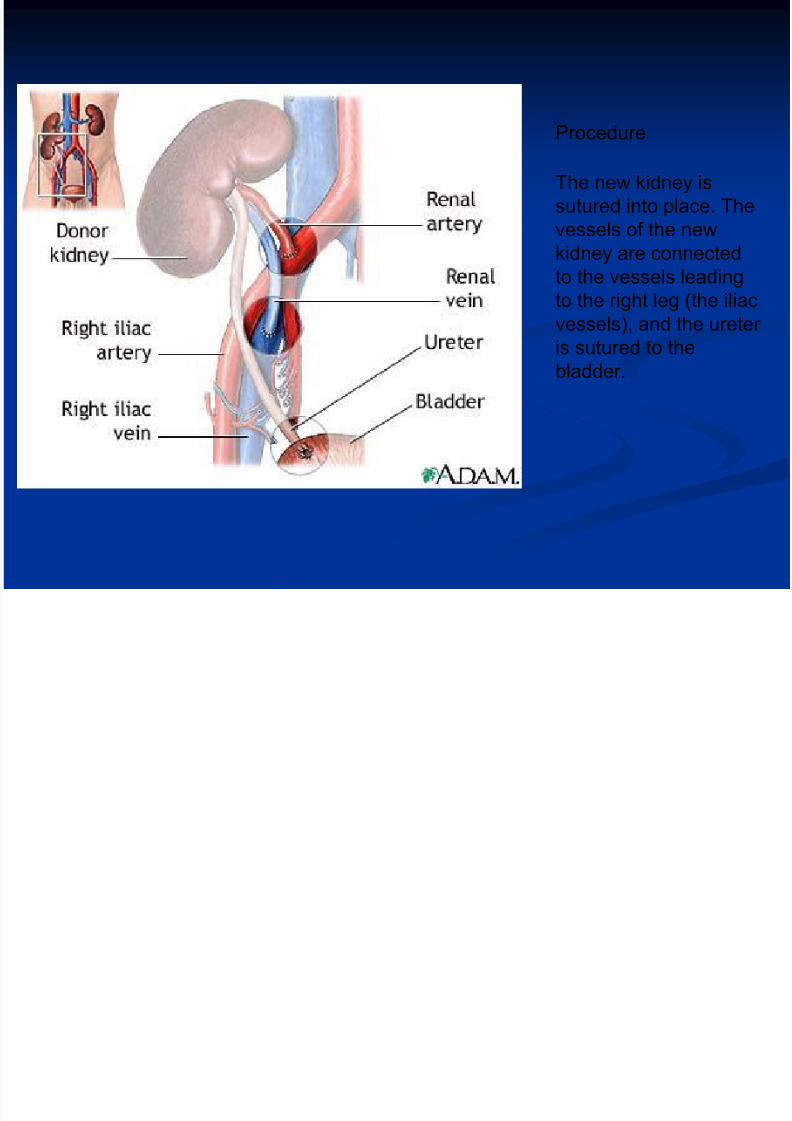
Procedure
The new kidney is
sutured into place. The
vessels of the new
kidney are connected
to the vessels leadingto the right leg (the iliac
vessels), and the ureter
is sutured to the
bladder.
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 46/51
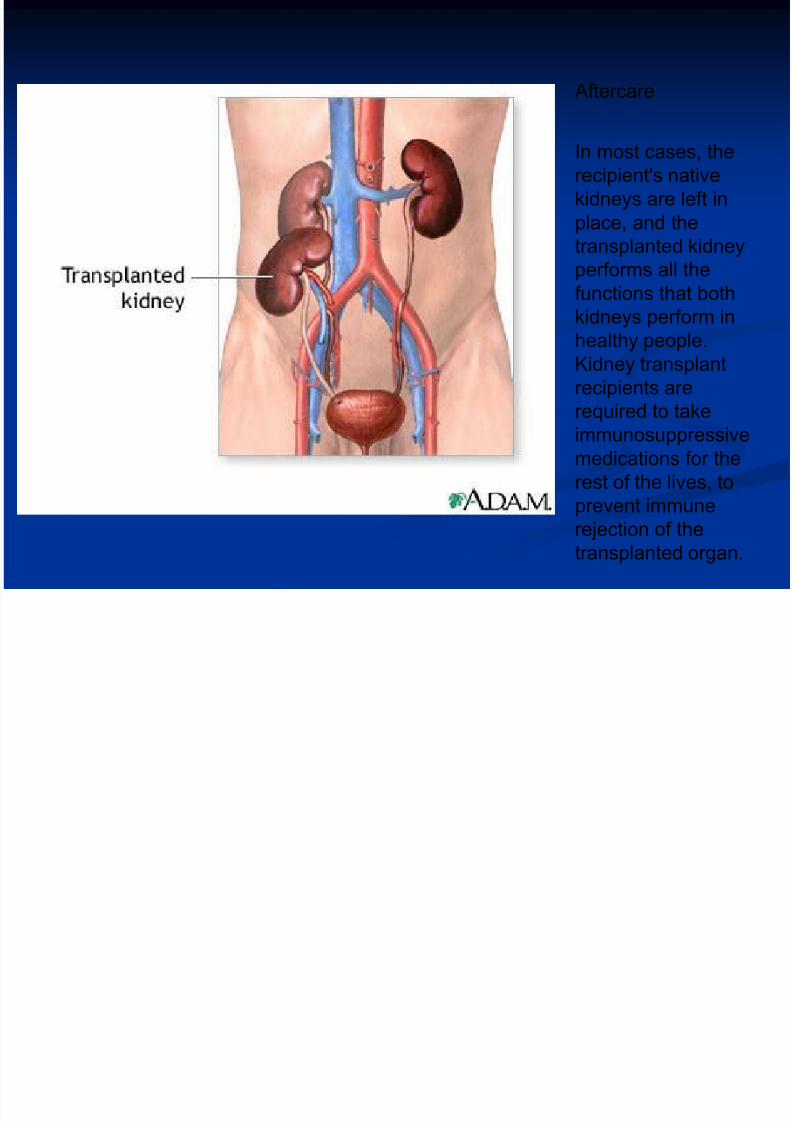
Aftercare
In most cases, therecipient's native
kidneys are left in
place, and the
transplanted kidney
performs all the
functions that both
kidneys perform in
healthy people.
Kidney transplant
recipients are
required to takeimmunosuppressive
medications for the
rest of the lives, to
prevent immune
rejection of the
transplanted organ.
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 47/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 48/51
Kidney StructureNumber of Kidneys: agenesis
Shape of the Kidneys: horseshoe kidney
Location of the Kidneys: ectopic kidney.
Finding Kidney Stones, Cysts, and Masses
Kidney Stones: The kidney ultrasound is a useful screening test for kidney stones. Not all kidney stones can be seen onultrasound, but many can be. If a stone is causing ureter obstruction, there may be hydronephrosis.
Ureter Obstruction: A kidney ultrasound is routinely ordered to rule out obstruction in kidney failure. Impeding the flow of
urine can cause it to back up and dilate the ureters and kidneys. It should be noted that finding hydronephrosis doesn’tnecessarily mean there is an obstruction.
Kidney Cysts: The kidney ultrasound is very good at discovering kidney cysts, most of which are uncomplicated and
incidental findings. Some cysts look complicated or complex and may represent infection, bleeding or cancer. People withpolycystic kidney disease have multiple large cysts that replace normal tissue and destroys the kidneys.
Kidney Masses: The ability of kidney ultrasound to detect a kidney mass depends on its size. It is very good for large
masses (> 3 cm) but not so good for small tumors.
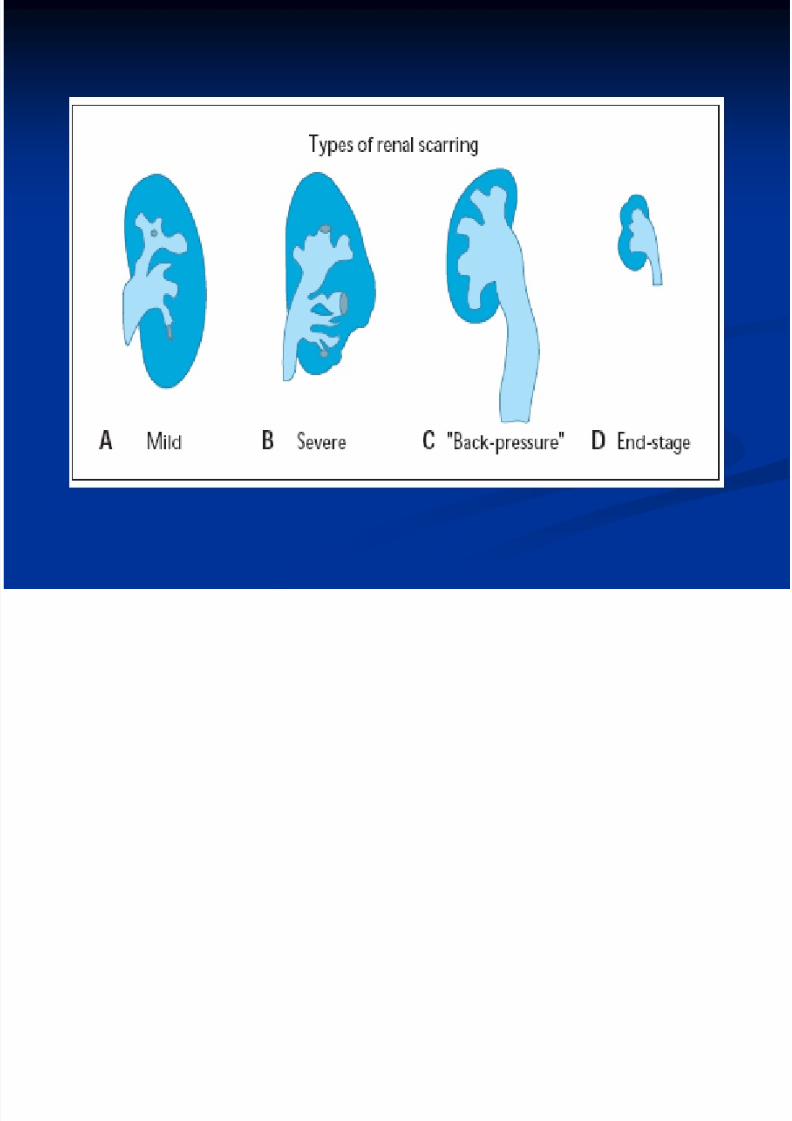
Signs of Kidney Chronic Disease
Kidney Size: On the average, the kidneys are about 11-12 cm in length, 7-8 cm wide, and 2-3 cm in thickness. If they arevery small, it suggests significant scarring and irreversible damage.
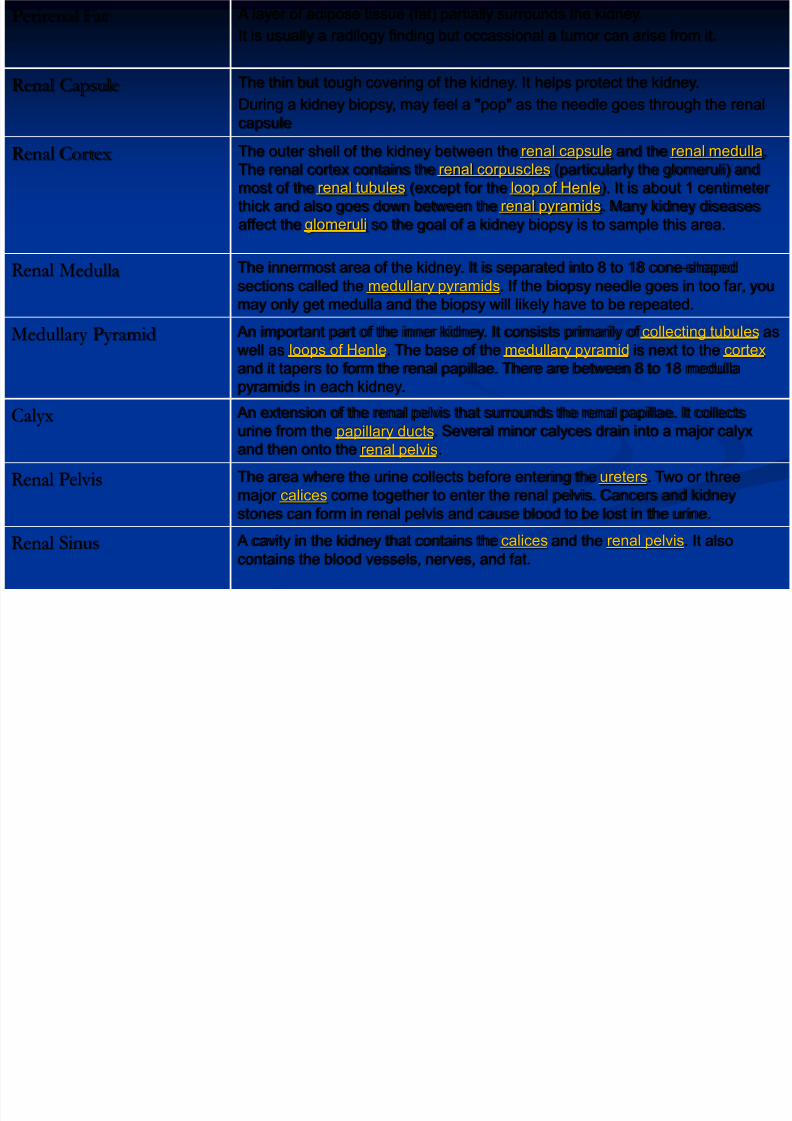
Thickness of the Cortex: The cortex is the outer shell of the kidney (about 1 cm in thickness) and contains all the glomeruli.
If it particularly thin, it suggests chronic kidney disease and may make it hard to biopsy. If it is thick, it may mean inflammationand congestion.
Echogenicity of the Cortex: Echogenicity refers to how the sound waves look when they bounce off something. It is often
said that it is not normal if there is a lot of echogenicity (compared to the liver). In reality, it is not a very reliable indicator of
kidney disease.
RENAL ULTRASOUND
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 49/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 50/51
7/28/2019 8526708 Renal Anatomy
http://slidepdf.com/reader/full/8526708-renal-anatomy 51/51
THANK YOU


















