
8-Hour NAIC Long-term Care & Partnership Training · © 2008-2015 Sandi Kruise Insurance Training,...
234
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 8-Hour NAIC Long-term Care & Partnership Training Sandi Kruise Insurance Training a division of Sandi Kruise Inc www.kruise.com 1-800-517-7500
Transcript of 8-Hour NAIC Long-term Care & Partnership Training · © 2008-2015 Sandi Kruise Insurance Training,...

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved.
8-Hour NAIC Long-term Care &
Partnership Training
Sandi Kruise Insurance Training a division of Sandi Kruise Inc
www.kruise.com 1-800-517-7500

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 1
Table of Contents
Chapter One - Overview of Long-term Care .................................................................................... 2
Chapter Two - Long-Term Care Planning ..................................................................................... 27
Chapter Three – Public Programs to Pay for Long-term Care ....................................................... 41
Chapter Four – Overview of Long-term Care Insurance ................................................................ 98
Chapter Five - Long-term Care Insurance Features, Benefits and Provisions ............................. 122
Chapter Six - Long-term Care Insurance Premiums, Underwriting and Claims ........................... 154
Chapter Seven - Alternative LTC Financing Options .................................................................. 183
Chapter Eight - New National Partnership Initiative and The Deficit Reduction Act (DRA) .......... 201

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 2
8-Hour NAIC Long-term Care & Partnership Training
Chapter One - Overview of Long-term Care
This chapter provides basic information about long-term care (LTC) and serves as the foundation for the subsequent chapters. After this chapter, agents should be able to answer the following questions:
What is Long-Term Care (LTC)? How do people receive LTC assistance? How likely is that a person will need LTC? How much does LTC cost? Who pays for LTC services?
What is Long-Term Care?
Long-term care (LTC) is a variety of services and supports to meet health or personal care needs over an extended period of time.
The goal of long-term care services is to help people maximize their independence and functioning at a time when they are unable to be fully independent.
Long term care is care that people need because they can no longer perform everyday tasks (activities of daily living) by themselves due to a chronic illness, injury, disability or the aging process. Long term care also includes the supervision they might need due to a severe cognitive impairment (such as Alzheimer’s disease).
While many people think of care in a nursing home when they hear the words “long-term care,” there is a much wider array of services to support people who need long-term care. Among them are in-home health care, adult day care centers, assisted living facilities, adult family care homes, continuing care retirement communities, and many others. In fact, most long-term care is provided at home, either by paid providers like home health aides, personal care workers or nurses and therapists, or even by unpaid caregivers such as family or friends.
Long-term care differs from acute care in that LTC services are intended primarily to maintain health status, while acute care aims to improve or correct a medical problem.
This type of care isn’t intended to cure people. It is chronic care that they might need for the rest of their life. They can receive long term care in their own home, a nursing home or another long term care facility, such as an assisted living facility.
People often confuse long term care with disability or short-term medical care. Long term care is not:
care that they received in the hospital or their doctor's office care they needed to get well from a sickness or an injury short-term rehabilitation from an accident recuperation from surgery

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 3
Definition of LTC by Impairment
Long-term care can be defined as the medical and non-medical support services needed by an individual with a prolonged illness or disability to perform activities of daily living (ADLs) or instrumental activities of daily living (IADLs).
Activities of Daily Living (ADLs) Instrumental Activities of Daily Living (IADLs)
Bathing Dressing Eating Using the Toilet Transferring Continence
Grocery shopping Laundry Preparing meals Housework Managing medication Transportation
Cognitive Impairment: loss in intellectual capacity
ADLs are the activities people usually do during a normal day such as getting in and out of bed, dressing, bathing, eating, and using the bathroom. IADLs are activities related to independent living and include shopping for groceries, preparing meals, performing housework, managing medications, managing money, and using a telephone.
Activities of Daily Living (ADLs)
Most long-term care is non-skilled personal care assistance, such as help performing everyday Activities of Daily Living (ADLs), which are:
The basic activities of caring for oneself:
Eating Dressing Bathing Toileting (using the bathroom) Transferring (moving back and forth from a bed to a chair) Continence (the ability of the body to control urination or bowel movements or both)
Insurance companies use the inability to perform a specified number of these ADLs to help determine eligibility for long term care insurance benefits.
Cognitive Impairment
Long-term care is needed when someone has a chronic illness or disability that causes them to need assistance with Activities of Daily. Illness or disability could include a problem with memory loss, confusion, or disorientation. This is called Cognitive Impairment and can result from conditions such as Alzheimer’s disease.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 4
A deterioration or loss in intellectual capacity that results in impairment in some or all of the following: short and long-term memory, orientation to people, place, and time, deductive or abstract reasoning (including judgment), and ability to perform activities of daily living.
Insurance companies use standardized tests to measure cognitive impairment to determine eligibility for long-term care insurance benefits.
In 2005, nearly one-half (45%) of nursing facility residents had dementia, and 20% had other psychological diagnoses.
Levels of Long Term Care
Long-term care encompasses many different types of services, which are sometimes grouped into the following levels:
Skilled care is medical or nursing care (such as help with medications, caring for bandages and wounds) and therapies (such as occupational, speech, respiratory, and physical therapy). It is usually delivered by a nurse, therapist or other trained professional. Less than 15 percent of all persons who need LTC require skilled care.
Personal care or custodial care is help with the ADLs, such as bathing and dressing. Most people who need LTC need personal care.
Supervisory care provides monitoring and supervision, a safe or controlled environment, and stand-by help with ADLs to ensure that individuals do not harm themselves or others. Supervisory care is often needed because of a severe cognitive impairment.
Risk of Needing LTC
Anyone can need long term care at any time in their life. Currently, 40% of people receiving long term care services are working age adults, between the ages of 18 and 64.2 Automobile and sporting accidents; disabling events such as strokes, brain tumors, and spinal cord injuries; and disabling illnesses such as multiple sclerosis and Parkinson’s disease are examples of injuries and ailments that can happen to anyone at any age.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 5
The need for long term care is most often associated with issues of aging. However, anyone can need long term care at any time. Everyone is susceptible to accidents, chronic illnesses, and disabilities that may require assistance with routine daily activities for an extended period of time.
Who Needs Long Term Care?
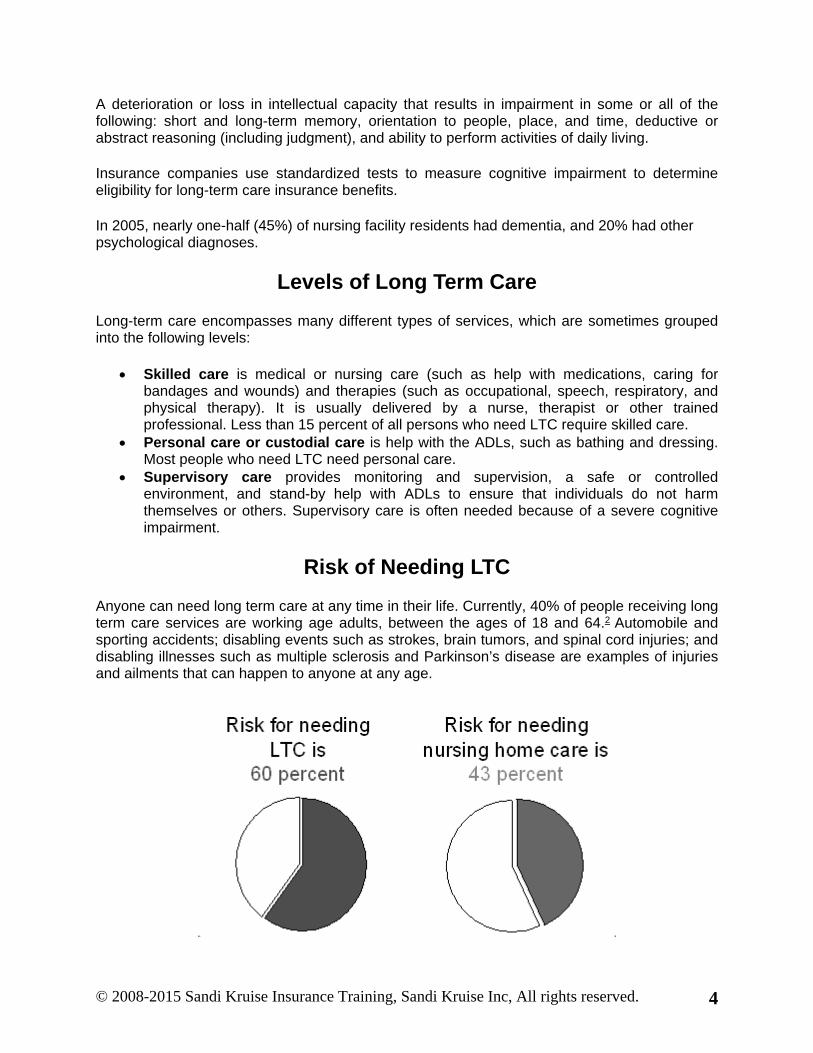
As people age and their average life span increases, the chances of needing long term care increase. After age 65, an American has more than a 60% chance of needing some form of long term care. In general, the longer someone lives, the higher their odds of needing long term care.
Approximately 60 percent of individuals age 65 and older will require LTC at some point in their lives. About 43 percent will require nursing home care. There are many factors that increase a person’s risk, including those listed below.
The probability of needing long-term care services increases with age.1 So as America ages, all sectors of the U.S. health and long-term care system – state and federal, public and private – are being asked to provide services to a growing population of older people with widely varying needs. More than two of five people age 65 or older (14 million) report having some type of functional limitation (sensory, physical, mental, self-care disability, or difficulty leaving home).2 Of these, six million are receiving long-term care services.3
1 O’Brien, Ellen (2005). “Long-Term Care: Understanding Medicaid’s Role for the Elderly and Disabled.” Kaiser Commission on Medicaid and the Uninsured, November, p. 1. 2 U.S. Census Bureau (2003). “Disability Status: 2000.” March, p. 3. 3 O’Brien, Ellen (2005). “Long-Term Care: Understanding Medicaid’s Role for the Elderly and Disabled.” Kaiser Commission on Medicaid and the Uninsured, November, p. 1.
A few years from now, the nation’s aging trend will accelerate, fueled by the large “baby boomer” generation. Between 2010 and 2040, Americans between the ages of 65 and 84 will grow by almost 31 million.4 And in a testament to the remarkable longevity gains of the last century, the age cohort of people 85 and older – those most likely to need services – is projected to grow by 9 million, accounting for 11 percent of the country’s total population gain of 83 million during that period.5
4 U.S. Census Bureau (2004). “U.S. Interim Projections by Age, Sex, Race and Hispanic Origin.” 5 U.S. Census Bureau (2004). “U.S. Interim Projections by Age, Sex, Race and Hispanic Origin.”
Risk Factors for Needing LTC
Age – Age is the single most important risk factor for needing LTC services. However, younger people can also need LTC. It is estimated that nearly 40 percent of all persons currently receiving LTC services are working-age adults between 18 and 64 years old.1
1 General Accounting Office. “Long-Term Care: Current Issues and Future Directions,” April 1995.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 6
Marital Status – Single individuals are more likely to need LTC services. This is due mostly to the fact that a single or widowed individual is less likely to be living with someone who can provide informal care.
Gender – Women are more likely to require LTC services. This is due partly to the fact that women often outlive their husbands and therefore are more likely to be older and single.
Lifestyle – Smoking, poor diet, stress, and/or a sedentary lifestyle may lead to chronic health conditions requiring LTC.
Health – Chronic conditions including emphysema, diabetes, or arthritis increase the risk of needing LTC.
Family History – Individuals with a family health history of physical or mental illness have an increased risk of needing LTC.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 7
Need for Long-Term Care
Age is not the only indicator of need for long-term care services and more livable communities. Other indicators include:
Living Alone. Nearly four out of 10 (38%) people age 75+ lived alone in 2005. Poverty. In 2005, more than one-half (54%) of people age 65+ lived at or below 300% of
the poverty line, an income level that places them at risk of needing public assistance. Education. Less than one out of five (18%) people age 65+ had a bachelor’s degree or
higher in 2005. Housing. Although almost 80% of people age 65+ owned their own homes in 2005,
about one out of four (26%) spent at least 30% of their income on housing. Among renters, more than half (54%) did.
Transportation. One out of eight people (12%) age 65+ did not have a vehicle in their household in 2005.
Nearly four out of 10 people age 75+ lived alone in 2005, and more than one-half of people age 65+ lived at or below 300% of poverty, an income level that places them at risk of needing public assistance.
Risk of Needing LTC by Age
Age is the most important risk factor for needing LTC services. The chart illustrates the percentage of individuals in each age group using LTC services during a 12-month period.
Source: Urban Institute, Long-Term Care: Consumers, Providers, and Financing. 2001.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 8
Risk of Needing Nursing Home Care by Age
Age is the most important risk factor for requiring nursing home care. The chart illustrates the percentage of individuals in each age group who needed nursing home care during a 12-month period.
Source: Urban Institute, Long-Term Care: Consumers, Providers, and Financing. 2001.
How Much Care Will Be Needed
It is difficult to predict how much or what type of care any one person might need. On average, someone age 65 today will need some long-term care services for three years. Service and support needs vary from one person to the next and often change over time. Women need care for longer (on average 3.7 years) than do men (on average 2.2 years). While about one-third of today's 65-year-olds may never need long-term care services, 20 percent of them will need care for more than five years.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 9
Length of Stay in a Nursing Home
The cost of long-term care surpasses the ability of most families to pay for it out-of-pocket. Thus, informal care and third-party payments are vital. The average length of stay for people living in nursing homes is just over two years,13 but there is great variability in the duration of stays, with about five percent of residents staying 5-10 years from the time of admission.14
13 Kaiser Commission on Medicaid and the Uninsured (2006). “Private Long-Term Care Insurance: A Viable Option for Low and Middle-Income Seniors?” February. 14 Elderweb (2006). “Average Length of Nursing Home Stay by Sex and Age at Admission.”
Care Needs Change Over Time – The LTC Continuum
Many people who need long-term care develop the need for care gradually. They may begin needing care only a few times a week or one or two times a day, for example, help with bathing or dressing. Care needs often progress as people age or as chronic illness or disability become more debilitating, causing them to need care on a more continual basis, for example help using the toilet or ongoing supervision because of a progressive condition such as Alzheimer’s disease. Some people need long-term care in a facility for a relatively short period of time while they are recovering from a sudden illness or injury, and then may be able to be cared for at home. Others may need long-term care services on an on-going basis, for example someone who is disabled from a severe stroke. Some people may need to move to a nursing home or other type of facility-based setting for more extensive care or supervision if their needs can no longer be met at home.
Someone who needs long-term care may need one or more of the following:
Services at home from a nurse, home health/home care aide, therapist, or homemaker; Care in the community; and/or Care in any of a variety of long-term facilities.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 10
Providers of Long Term Care
Individuals requiring skilled, professional LTC services can receive them in a variety of settings. In many cases, individuals will use a combination of different services in order to meet their LTC needs. For example, individuals may receive both formal home health care services and informal care from a family member or they may attend an adult day care program in addition to receiving home health care services.
Informal Care
Family (informal) caregivers - Family caregivers – spouses, daughters and daughters-in-law, sons, siblings, partners, and sometimes other relatives and friends – often volunteer to help with personal care, medication management, and a range of household and financial matters. Sometimes referred to as “informal caregivers,” they consistently provide the most care – an estimated $77 billion of the total $211 billion of long-term care services in 2004. (This value was determined by how much it would cost to replace the informal care with professional services.) Caregiving is a shared experience for millions of Americans, with a 2003 survey showing one in five families is involved in helping to support a frail elder or person with disabilities to live at home.21
21 National Alliance for Caregiving and AARP (2004). “Caregiving in the U.S.” April, p. 6.
Most LTC is provided in the home by informal unpaid caregivers. Informal care may be provided by family members, friends, or local social services agencies. One survey found that about 23 percent of Americans had provided unpaid LTC services in 1998.
Providing this care can be emotionally and financially burdensome for the caregiver. Many caregivers must juggle other responsibilities such as raising children and working full- or part-time.
To ease the burdens of caregiving, the federal government, through the Older Americans Act, and many states have created caregiver support programs. These programs typically provide counseling, information, and respite care to informal caregivers.
Source: Kaiser Family Foundation, Survey of Long Term Care from the Caregiver’s Perspective, 1998.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 11
Characteristics of Informal Caregivers
In today's society, children are more apt to live further away from their parents. In addition, many adult children are taking less vacation time and working longer hours. Taking care of a family member is a time-consuming commitment that often demands a significant number of hours from multiple family members.
Even if family members can find the time to provide caregiving to a family member, it often comes at a tremendous financial cost. Caregiving can cost the average caregiver in lost wages, pension benefits, and Social Security.
While having a family take care of them might be an option, it might be difficult to do without additional assistance.
The assistance offered by family caregivers often involves significant personal sacrifice.22 In order to prevent caregiver “burnout,” caregiver groups have organized in some states to advocate for flexible home care, respite care, financial advice, training and education in chronic care, and other forms of advice and support.23 Currently, however, only a modest amount of federal funding is available to support caregivers across the country. The largest program is the National Family Caregivers Support Program (NFCSP).24 By FY 2006, the NFCSP, which

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 12
provides funding to area agencies on aging to provide respite care, caregiver training and other support services, was funded at $162 million.
22 Friedland, Robert (2006). “Long-Term Care: Are Americans Prepared?” Testimony for the Special Committee on Aging, March 9, p. 15. 23 Family Caregiver Alliance (2006). “Caregiver Assessment: Principles, Guidelines and Strategies for Change.” April, p. 8-9. 24 U.S Senator Barbara Mikulski (2004). “Mikulski Pays Tribute to Caregivers, Urges Congress to Pass Alzheimer’s Bill that Would Provide Relief to Families.” Press release. October 5.
Most long term care services are provided by family members and friends. This type of care, informal care, also includes long term care services provided by unlicensed caregivers who are not arranged or supervised by a home care agency.
Formal Care
Formal Care
Home Care Community-Based Care Residential Care
Skilled Care Personal Care IADL Assistance
Adult Day Care Nursing Home Assisted Living Continuing Care
Retirement Community
Formal care is provided in a variety of different settings.
Home Care: Home care services may be provided by licensed nurses or home health aides. Care varies from skilled care, such as physical therapy or wound care, to personal care, such as assistance with eating or bathing, to IADL assistance, such as help preparing meals. Care can also be provided by unlicensed people who are trained in the field of long term care. This type of care is provided by a home health aide or homemaker arranged or supervised by a home care agency or provided by a nurse or therapist.
Community-Based Settings: Community-based services such as Adult Day Care Programs provide part-time care in a group setting. Services include health monitoring, therapy, meals, social services, and personal care.
Residential Settings: Nursing homes offer comprehensive services including skilled nursing care, therapy, personal care, and meals. Assisted living provides personal care, housekeeping, transportation, and assistance with ADLs to people who live on their own in a residential facility. Continuing Care Retirement Communities (CCRCs) are housing communities that provide different levels of care based on what each resident needs over time. This can range from independent living in an apartment to assisted living to full-time care in a nursing home.
Board and Care Homes are a type of group living arrangement designed to meet the needs of people who cannot live on their own. These homes offer help with some personal care services.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 13
Caregiver Workforce Issues
The United States is facing a critical shortage of LTC workers that will only intensify in the coming decades. Some of the contributing factors include:
High staff turnover rates: Turnover rates for nursing assistants caused by low wages, stressful working environments, and little respect.
Fewer informal caregivers available: Fewer families can rely on informal caregivers because adult children may not live near their elderly parents or may have other family or work responsibilities. This is increasing the demand for home health aides and other professional care providers. The responsibility of carrying for an elderly individual traditionally fell to the person’s adult children (typically to their adult daughters). Today, however, adult children often do not live near their parents, making such informal caregiving arrangements difficult or impossible. In addition, women are increasingly working outside of the home, giving them little time to care for an elderly parent. Because fewer families can rely on informal caregivers, demand for home health aides and other professional care providers is increasing.
Aging population: As the baby boomer generation ages and life expectancy increases, demand for LTC services will increase significantly. Unfortunately, the population growth for people between the ages of 20 and 64, who typically provide LTC services, will not match the growth rate of people needing the services.
Source: Stone, Robin, and Joshua Weiner. Who Will Care For Us? Addressing the Long-Term Care Workforce Crisis. October 2001.
Workforce Issues: Rural Areas
The shortage of LTC workers can be especially severe in rural and underserved areas. These areas must contend with additional factors such as:
Wages in rural areas are often significantly lower than wages available in urban areas. Fewer young nurses and LTC workers are willing to stay in rural areas, making it difficult
for facilities and agencies to replace their retiring workers.
Where Long-Term Care is Provided
The purpose of this section is not to imply that agents should be experts regarding all of these types of facilities and services. However, it is important for agents to know what types of LTC services are and are not covered by the policies they sell, how these services and providers are defined in the policy as well as any restrictions applying to coverage.
Long-term care, often associated with institutional care, is provided in many different settings. Most long-term care is actually provided at home – either in the home of the person receiving care or at a family member's home. There is also an increasing amount of long-term care available in the community through programs such as adult day service centers, which often supplement care at home or provide respite for family caregivers.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 14
Currently, 83% of long term care is provided in the home or community, while only 17% is provided in a nursing home.
For people who cannot stay at home, but who do not need the level of care provided in a nursing home, there are a variety of residential care settings, such as assisted living, board and care homes, and Continuing Care Retirement Communities (CCRCs). Nursing homes provide long-term care to people who need more extensive care, particularly those whose needs include nursing care or 24-hour supervision in addition to their personal care needs.
Home and Community-Based Services (HCBS)
Most people prefer to receive long-term care services in their own homes, and the use of home and community-based services is growing, but public assistance is still weighted toward institutional care. There were only 3 people receiving Medicaid aged/disabled waiver services for every 10 people receiving nursing facility services in 2002.
In only three states—Oregon, Alaska, and Washington—were there more people receiving aged/disabled waiver services than nursing facility services.
Medicaid HCBS participants grew significantly (26%) from 1999 to 2002, with an increase of 30% in aged/disabled waiver programs. In 2002, there were almost 2.4 million Medicaid HCBS participants, including 530,000 aged/disabled waiver participants. However, most spending for HCBS waiver services goes toward people with mental retardation and developmental disabilities, not aged and physically disabled populations.
Ten states—Alabama, California, the District of Columbia, Hawaii, Kentucky, Louisiana, Ohio, Oklahoma, Pennsylvania, and Tennessee—did not provide any Medicaid or state-funded public financing for persons in community-based group residential care settings such as assisted living and personal care homes in 2004.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 15
In addition, states reported about 130,000 people on waiting lists for aged/disabled waiver services in 2004. Over half (about 70,000) lived in Texas, but six more states—Wisconsin, Louisiana, North Carolina, Florida, Maryland, and Mississippi—had large waiting lists of more than 6,000 people.
While Medicaid HCBS utilization has increased, Medicare home health visits per user decreased 26% between 2000 and 2005. The average home health user received 27 home health visits in 2005, a reduction from 37 visits per user in 2000. In fact, every state experienced a decrease in Medicare visits per user. This decrease is significant because Medicare is the major payer for skilled home health care.
Medicare Home Health Visits Per User, 2000-2005
Data Source: Centers for Medicare and Medicaid Services, Medicare & Medicaid Statistical Supplement (2000-2002) and Medicare Home Health Utilization by State (2003-2005).
Home and community-based services (HCBS) describe a range of personal, support, and health services provided to individuals in their homes or communities to help them stay at home and live as independently as possible. Most people who receive long-term care at home generally require additional help from either family or friends to supplement services from paid providers. This is because so much of the care needed is personal care: help with activities such as bathing and dressing, help managing medications, or supervision for someone with a condition such as Alzheimer's disease.
Some of the Most Common Home and Community Services
Adult Day Service (ADS) Programs
ADS programs are designed to meet the needs of adults with cognitive or functional impairments, as well as adults needing social interaction and a place to go when their family caregivers are at work. They provide a variety of health, social, and other support services in a protective setting during part of the day. Adult day centers typically operate programs during

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 16
normal business hours five days a week; some have evening and weekend hours. These programs do not provide 24-hour care.
Case Managers/Geriatric Care Managers
Case Managers are health care professionals (typically nurses or social workers) who specialize in assisting people and their family with long-term care needs. This includes, but is not limited to assisting, coordinating, and managing long-term care services; developing a plan of care; and monitoring long-term care needs over extended periods of time.
Emergency Response Systems
Emergency Response Systems provide an automatic response to a medical or other emergency via electronic monitors. Those who live alone can wear a signaling device that they activate when they need assistance.
Friendly Visitor/Companion Services
Friendly visitor services are typically staffed by volunteers who regularly pay short visits (under two hours) to someone who is frail or living alone.
Home Health Care/Home Care
Home care and home health care are two different services, which may be provided by a single agency or separate agencies. Home health care typically includes skilled, short-term services such as nursing, physical or other therapies ordered by a physician for a specific condition. Home care services are most often limited to personal care services such as bathing and dressing, and often also include homemaker services such as help with meal preparation or household chores.
Homemaker/Chore Services
Homemaker/Chore services can help people with general household activities such as meal preparation, routine household care, and heavy household chores such as washing floors, windows or shoveling snow.
Meals Programs
Meal programs include both home-delivered meals (“Meals-on-Wheels”) and congregate meals, which are provided in a variety of community settings.
Respite Care
Respite Care gives families temporary relief from the responsibility of caring for family members who are unable to care for themselves. Respite care is provided in a variety of settings including in the home, at an adult day center, or in a nursing home.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 17
Senior Centers
Which provide a variety of services including nutrition, recreation, social and educational services, and comprehensive information and referral to help people find the care and services they might need; and
Transportation Services
Can help people get to and from medical appointments, shopping centers and access a variety of community services and resources.
Impact of LTC on Employers
The MetLife Caregiving Cost Study: Productivity Losses to U.S. Business 2006
Facility-Based Long-Term Care Services
There are numerous types of facility-based programs that provide a range of long-term care services. Some facilities provide only housing and related housekeeping, but many also include help managing medications, assistance with personal care, supervision and special programs for individuals with Alzheimer's disease, or 24-hour nursing care. The services available in each facility are often regulated by the state in which the facility operates (for example, some states do not allow some types of facilities to include residents who are wheelchair bound or who cannot exit the facility on their own in an emergency). Facility-based care is known by a wide variety of names, including board and care, assisted living, adult foster care, Continuing Care Retirement Communities (CCRCs), and nursing homes.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 18
Adult Foster Care
Adult foster care can be provided for individuals or for small groups of adults who need help functioning or who cannot live safely on their own. The foster family provides room and board, 24-hour availability, help managing medications, and assistance with Activities of Daily Living. Licensure requirements and the terminology used for this type of facility vary greatly from state to state.
Board and Care Homes
Board and care homes, also called residential care facilities or group homes, are smaller private facilities, usually with 20 or fewer residents. Most board and care homes accept six or fewer residents. Rooms may be private or residents may share rooms. Residents receive meals, personal care and have staff available 24 hours a day. Nursing and medical attention are usually not provided on the premises. State licensure and the terminology used for this type of facility vary greatly.
Assisted Living
Assisted living is designed for people who want to live in a community setting and who need or expect to need help functioning, but who do not need as much care as they would receive at a nursing home. Some assisted living facilities are quite small – with as few as 25 residents – while some can accommodate 120 or more units. Residents often live in their own apartments or rooms, but enjoy the support services that a community setting makes possible, such as:
up to three meals a day; assistance with personal care; help with medications, housekeeping, and laundry; 24-hour security and onsite staff for emergencies; and social programs.
The cost of assisted living varies widely, depending in part upon the services needed by the resident and the amenities provided by the facility. Assisted living is regulated in all states, however, the requirements vary.
Continuing Care Retirement Communities (CCRCs)
Continuing Care Retirement Communities (CCRCs) are also called life care communities. They offer several levels of care in one location. For example, many offer independent housing for people who need little or no care, but also have assisted living housing and a nursing facility, all on one campus, for those who need greater levels of care or supervision. In a Continuing Care Retirement Community, if someone becomes unable to live independently, they can move to the assisted living area, or sometimes they can receive home care in their independent living unit. If necessary, they can enter the onsite or affiliated nursing home. The fee arrangements for CCRCs vary by the type of community. In addition to a monthly fee, many CCRCs also charge a one-time “entrance fee” that may be partially or completely refundable (often on the sale of the unit).

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 19
Nursing Homes
Nursing homes, also called Skilled Nursing Facilities (SNF) or convalescent care facilities, provide a wide range of services, including nursing care, 24-hour supervision, assistance with Activities of Daily Living, and rehabilitation services such as physical, occupational, and speech therapy. Some people need nursing home services for a short period of time for recovery or rehabilitation after a serious illness or operation, while others need longer stays because of chronic physical, health or cognitive conditions that require constant care or supervision.
Families typically seek nursing home care when it is no longer possible to care for a person at home safely or when the cost of round-the-clock care at home becomes too great. Nursing homes are highly regulated. They must be licensed by state governments and many are also approved by HHS for Medicare/Medicaid payment.
Cost of Long-Term Care
Long-Term Care Cost Varies by Location
Following are key findings from the Genworth 2008 Cost of Care Survey, broken out by major category.
Nursing Homes: The average annual national cost of a private room in a nursing home is $209 per day, reflecting a 2 percent increase over 2007 rates. This remains the most costly care option. The most expensive per day room rate was found in Alaska ($539) and the least expensive was found in Louisiana ($119).
Assisted Living: A private one-bedroom unit in an assisted living facility has an average monthly cost of $3,008, a 11 percent increase since 2007. The most expensive one-bedroom unit was found in Massachusetts ($4,753 per month) and the least expensive was found in North Dakota ($1,609 per month).
Home Care: The average hourly rate for Medicare/Medicaid certified and state licensed home health aides is $38 an hour, a cost that translates to a $79,040 per year for 40 hours per week.
SOURCE Genworth Financial, Inc 2008
When family members provide informal care at home, costs are harder to estimate. The caregiver may have to leave his or her job and often suffer from emotional stress. These costs don’t show up in economic statistics.
There are variations in costs based on the type and amount of care needed, the provider used, and where they live. Home health and home care services, provided in two-to-four-hour blocks of time referred to as “visits,” are generally more expensive in the evening, or on weekends or holidays. The costs of services in some community programs, such as adult day service programs, are often provided at a per-day rate, but vary based on overhead and programming costs. Many care facilities charge extra for services provided beyond the basic room-and-board charge, although some may have “all inclusive” fees.
Many care facilities charge extra for services provided beyond the basic room-and-board charge, although some may have “all inclusive” fees.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 20
Payment for LTC
Long-Term Care Financing
Medicaid spent $94.5 billion on long-term care services in 2005, which means that roughly one-third (31%) of total Medicaid expenditures of $300 billion went toward long-term care. Medicaid long-term care spending increased by 38% over the five-year period since 2000, while total Medicaid spending increased 55% over the same period. In addition, the rate of long-term care spending growth has slowed since 2000.
Out of the total Medicaid long-term care expenditures, about one-half went toward nursing facilities, with 37% going toward HCBS and 13% toward Intermediate Care Facilities for the Mentally Retarded (ICF-MR). Although most Medicaid long-term care spending goes toward institutional care, four states—Oregon, New Mexico, Alaska, and Vermont—spend 60% or more on HCBS and five other states spend 50% or more. In contrast, Mississippi and the District of Columbia spend the lowest percentage on HCBS—under 20%.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 21
Medicaid nursing facility care costs more than twice as much as HCBS. Medicaid spending per HCBS recipient was about $10,500 in 2002, and spending per nursing facility beneficiary was about $24,000 in 2003. In comparison, Medicaid spending per aged/disabled waiver recipient was about $7,300 in 2002.
The Medicaid program requires that nursing facility residents have a personal needs allowance of a minimum of $30 per month. Eight states—Alabama, Hawaii, Illinois, Missouri, North Carolina, Oregon, South Carolina, and Virginia—allowed only the minimum of $30 in 2006.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 22
The U.S. average was about $48 per month, and ten states allowed at least $60 per month, led by Arizona with $90, three times the minimum.
Medicaid has the lowest payment rates for nursing facility care. Private payment rates per day are 45% less for assisted living than nursing facility care.
Medicare Spending on Long Term Care by type of service, 2005 in the US
Long Term Care Financing Year U. S. Total Medicaid Spending (millions)
2000 2005 % Change
$194,347 $300,305 +55
Medicaid Long-term Care Spending (millions)
2000 2005 % Change
$68,568 $94,500 +38
Medicaid Nursing Facility Spending (millions
2000 2005 % Change
$39,583 $47,238 +19
Medicaid HCBS Spending (millions)
2000 2005 % Change
$19,130 $35,159 +85
Medicaid Aged/Disabled Waiver Spending (millions)
2000 2005 % Change
$2,966 $5,134 +73
Who Pays for Long-term Care?
Out-of-pocket payments - Out-of-pocket payments covered 21 percent of total long-term care services for the elderly in 2004, according to CBO. For institutional care, this amounted to $36 billion and for home care, $8 billion.20
20 Holtz-Eakin, Douglas (2005). “The Cost and Financing of Long-Term Care Services.” Statement for the Subcommittee on Health, Committee on Energy and Commerce, U.S. House of Representatives. Congressional Budget Office, April 27, p. 5.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 23
Long-term care services are paid for by many different sources including Medicaid, personal savings, Medicare, and private LTC insurance. Most people who need LTC pay out of their own income and savings.
Between 2010 and 2040, the number of elderly between the ages of 65 and 84 will grow by almost 31 million people; c and the age cohort of people 85+ will grow by 9 million. d
c U.S. Census Bureau (2004). “U.S. Interim Projections by Age, Sex, Race and Hispanic Origin.” d U.S. Census Bureau (2004). “U.S. Interim Projections by Age, Sex, Race and Hispanic Origin.”
After adjusting for inflation, overall spending on long-term care is projected to increase from $123 billion in 2000 to $346 billion in 2040.e
e Congressional Budget Office (1999). “Projections of Expenditures for Long-Term Care Services for the Elderly.” March, p. 4.
Consumer surveys have revealed some common misunderstandings people have about which public programs pay for long-term care services. Many people believe they can rely on Medicare to pay for any long-term care services they will need. However, Medicare only pays for long-term care if someone requires skilled services or recuperative care for a short period of time. Medicare does not pay for what comprises the majority of long-term care services – non-skilled assistance with Activities of Daily Living.
Medicaid is the joint Federal and state program that pays for the largest share of long-term care services, but only if they meet financial and functional criteria. Other Federal programs such as the Older Americans Act and Veterans Affairs pay for some long-term care services, but only for specific populations and in specific circumstances.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 24
Most forms of employer-sponsored or private health insurance, including Health Maintenance Organizations (HMO) or managed care, follow the same general rules as Medicare. If they do cover long-term care, it is typically only for skilled, short-term, medically necessary care. Therefore most people who need long-term care end up paying for some or all of their care on their own out of their income or assets.
There are, however, an increasing number of private payment options that help to cover the costs of long-term care services. These include long-term care insurance, reverse mortgages, and other options.
It is important to understand the differences among the public programs and private financing options for long-term care services. Each public program and each private financing source has its own rules for what services it covers, eligibility requirements, co-pays, and premiums.
Payment for Nursing Home Care
Medicaid is the primary payer for most nursing facility residents. Almost two-thirds (65%) of nursing facility residents had Medicaid as the primary payer in 2005. Only one out of eight (13%) had Medicare, which only covers short stays. The remaining nursing facility residents had other sources of payment such as private long-term care insurance or out of pocket.
About 1.46 million residents of all ages lived in 16,435 nursing facilities in 2005. Only 3.5% of people age 65+ lived in nursing facilities. Out of a total of 1.71 million nursing facility beds, the occupancy rate was 85%, representing a slight decrease from 2000. Nearly one-half of nursing facility residents (45%) had dementia, and one out of five had other psychological diagnoses.
Despite the cognitive and physical frailties of nursing home residents, direct care nursing hours averaged less than 4 hours per patient day in 2005. Out of the average 3.7 direct care hours per patient day, Certified Nursing Assistants provided the bulk of this care at 2.3 hours. Ombudsmen, on average, oversaw more than 2,300 long-term care facility beds in 2004.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 25
If it is counted, assistance that is provided by family caregivers is the largest single source of financing for long-term care, followed by Medicaid and Medicare. Individuals also spend billions of dollars out-of-pocket, while private long-term care insurance accounts for a relatively small portion of expenditures.15
15 Holtz-Eakin, Douglas (2005). “The Cost and Financing of Long-Term Care Services.” Statement for the Subcommitttee on Health, Committee on Energy and Commerce, U.S. House of Representatives. Congressional Budget Office, April 27, p. 5.
Case Study 1: Sam
An individual is likely to use several sources over the course of their care to pay for their LTC services.
The case study illustrates how Sam’s nursing home care was paid by several different sources. First, he exhausted the benefits available to him under Medicare and then exhausted his personal savings. At the end of the case study, his nursing home costs are being paid by two sources: Medicaid and his personal income.
Sam is an 82 year-old widower with an income of $2,000 per month and savings of $14,500. He suffered a stroke and was hospitalized for several weeks. Following his hospital stay, he is discharged to a skilled nursing facility, where he will stay indefinitely. The nursing home charges $150 per day or $4,500 per month.
His nursing home stay is paid for as follows:
First 20 days: Medicare covers all costs. Days 21 to 34: Medicare and Personal Income.
Sam pays $124 per day ($1,736 for 14 days) and Medicare pays the rest. He uses his regular monthly income to cover his portion of the costs.
Days 35 to 184: Personal Income/Savings
On Day 35, Sam’s doctor decides he no longer needs skilled care (only personal care) so his care is no longer covered by Medicare. Sam will be responsible for the cost of his nursing home care. His monthly nursing home bill is $4,500 and his monthly income is $2,000, so he must pay $2,500 per month from his savings. With $14,500 in savings, Sam must spend $12,500 before he is eligible for Medicaid. He can pay for five more months (150 days) of his stay ($12,500/$2,500).
Days 185 and beyond: Personal Income/Medicaid.
Sam has exhausted his savings. He can now “spend-down” his income to qualify for Medicaid. His nursing home costs are now covered by a combination of his income and Medicaid.
The case study illustrates how Sam’s nursing home care was paid for by several different sources as he first exhausted the benefits available to him under Medicare and then his

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 26
personal savings. At the end, his nursing home costs are being paid by two sources: Medicaid and his personal income. If Sam stays 2.5 years (the average nursing home stay), his LTC payment sources would be: 52% paid by his own income and savings, 3% by Medicare, and 45% by Medicaid.
Case Study 2: Margaret
Individuals who need LTC assistance often rely on a variety of sources in order to meet their needs.
The case study illustrates how Margaret has used a combination of formal care (provided by her home health aide) and informal care (provided by her daughter, a church volunteer, and local social service agencies) to meet her current LTC needs.
Margaret is an 85 year-old woman who lives alone but within a short drive of her adult daughter, Allison. She has a LTC insurance policy. Margaret has begun to experience difficulty in performing some activities of daily living, including bathing and dressing, as well as some instrumental activities of daily living, including grocery shopping, paying her bills, and preparing meals. Margaret, with the help of her daughter, makes the following arrangements to address her LTC needs:
Bathing and Dressing
Because Margaret does not need skilled nursing care or therapy services, she does not qualify for home health care coverage under Medicare. However, her LTC insurance policy will cover up to $50 per day for home care, allowing Margaret to have a home health aide come to her home each day to help her bathe and dress.
Grocery Shopping
Margaret’s daughter, Allison, will help her do most of her grocery shopping. But because Allison sometimes travels for business, they contact Margaret’s church to find a volunteer who will take Margaret shopping and look in on her when Allison is out of town.
Paying Bills
Allison will now pay Margaret’s bills and keep her financial, legal, and medical records in order.
Preparing Meals
Margaret and Allison have dinner together twice per week and Margaret has lunch twice per week at her senior center. To supplement this, they make arrangements with the local Meals on Wheels program to have lunch delivered to Margaret’s home three times per week. For her other meals, Allison will help Margaret prepare meals on the weekend that she can reheat for herself during the week.
The case study illustrates how Margaret has used a combination of formal care (provided by her home health aide) and informal care (provided by her daughter, a church volunteer, and local social service agencies) to meet her current LTC needs.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 27
Chapter Two - Long-Term Care Planning
People Need to Plan for LTC
“There are four kinds of people in the world: Those who have been caregivers Those who currently are caregivers Those who will be caregivers And those who will need caregivers.”
Former First Lady Rosalynn Carter, Published by LTC Financial Partners, Kirkland Washington
Baby boomers and seniors alike would do well to provide for their own care, independent of relying on relatives, and a long term care insurance policy would help provide the funds to pay for the care you may need.2
2 The Wall Street Journal, 2/21/01
Baby-boomers overwhelming deny it could happen to them
There will be a rapid growth in the number of persons age 60 and over as the Baby Boomers begin turning 60 in 2006.
Although baby boomers have a very positive view of aging, there is an overwhelming level of denial regarding the likelihood of needing long-term care.
Source: STAT Research Survey study conducted by Center for Aging Research and Education: Commissioned by the GE Center for Financial Learning, 6/28/01
Aging Population & Projections
From 2005 to 2020, the population age 65 or older and the population age 85 or older will increase by almost one-half (48% and 43% respectively), and the youngest seniors age 65 to 74 will increase by 70%.
The growth of the overall population age 65+ over the next two decades will be largely due to the baby boomers born between 1946 and 1964, but the growth among those age 85 or older is largely due to increased longevity. In 2005, more than 15 percent of the population was age 65 or older in Florida, West Virginia, and Pennsylvania, the oldest of the states. By 2020, 42 states are projected to exceed that number.
Although the proportion of older Americans is increasing in every age bracket, it is the oldest-old who are most likely to need long-term care. North Dakota and Rhode Island had the largest percentages of populations over the age of 85 in 2005. In 2020, North Dakota, Iowa, and South Dakota are projected to have the highest percentages.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 28
Not only is America aging, but the aging population is racially and ethnically diverse, with 19 percent of people age 65+ reporting that they are non-white or Hispanic. Minority aging populations in Hawaii (Asian) and the District of Columbia (Black) outnumber whites. More than one out of the three older people in New Mexico, California, and Texas—the states with the highest proportion of Hispanic elders—define themselves as minorities.
This chapter provides an overview of the advantages of planning ahead for long-term care (LTC) needs, why people do not plan and ways to encourage and support people’s attention to the need to plan. At the conclusion of this chapter, agents will be able to:
Explain the benefits of planning ahead for possible future LTC needs; Identify obstacles to planning; Describe what motivates people to do advance planning for possible LTC needs; and Identify some of the ways in which agents can help support and motivate planning.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 29
Planning for LTC
Financial issues Care options Lifestyle and living arrangements Home modification Legal issues
No one wants to think about when they might need LTC. It is natural that thinking about needing LTC and “planning ahead” is often postponed, sometimes until it is too late.
Most people learn about LTC the hard way – when they or a loved one needs care. However, LTC needs are best met when they are planned for in advance. Planning ahead gives individuals time to talk with their family about preferences and concerns, to research care options in the community, and to give some thought to preferred types of services and providers. Furthermore, planning ahead gives individuals the time to plan for how they will pay for care – which can be very costly – in a way that does not deplete the financial resources available for a spouse or other family members.
Some of the specific advantages of planning ahead include:
Preserving assets and income for uses other than paying for LTC services. This allows a person to ensure quality of life for a spouse or other family member and to preserve and pass on an estate to heirs.
Providing choice over care options and control over where and how they receive LTC.
Improving quality of life. This results in less emotional and financial stress on individuals and their families.
Easing the burden of providing care by loved ones. Family members can still be involved in the daily care routine, but they can be a supplement rather than being the only source of care, which is emotionally and physically demanding.
Maintaining independence. Choices for care outside a facility and being able to stay at home as long as possible are enhanced if individuals plan ahead, including a plan for how to pay for care options that are less likely to be covered by payers of last resort, such as Medicaid.
Planning for LTC needs is not only about financial issues of how one will pay for care. It includes other important considerations, such as care options, lifestyle and living arrangements, home modifications, and legal issues.
If financial issues are not considered, it might be more difficult to plan for these other considerations. For example, care options are more limited if an individual has limited financial means to pay for care. However, thinking ahead and considering preferences and needs is also important.
Planning ahead for long-term care is important because there is a good chance someone will need some long-term care services if they live beyond the age of 65. About 60 percent of people over age 65 require some services, and the likelihood of needing care increases as they age.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 30
Planning ahead helps ensure people will have a range of options when they need long-term care, making it more likely that they will have more choice and control over where and how they receive services.
Planning ahead is important because the cost of long-term care services often exceeds what the average person can pay from income and other resources. By planning ahead, people may be able to save their assets and income for uses other than long-term care, including preserving the quality of life for their spouse or other loved ones. With planning, there is a greater likelihood of being able to leave an estate to their heirs, because they are less likely to use up their financial resources paying for care.
An agent’s role is important to help motivate planning:
Make consumers aware of the risks, cost and who pays for LTC. This is critical to motivate planning, and probably one of the major reasons people do not plan ahead for LTC needs – they simply do not realize that it is something they need to or should be worrying about.
Remind consumers of the advantages of planning. Help consumers learn the facts about LTC and the advantages of planning ahead by
talking about real life LTC stories. Those lessons are more effective than impersonal facts or statistics.
Have consumers make a list of what is important to them with regard to LTC issues. Some questions to ask include: Where do they want to get care? What do they think about relying on family? What care options do they want to learn more about?
Remember that there is no “right or wrong” about how to plan or what is included in the plan – these are personal decisions and each individual is different.
There are many resources on the Internet and in the media. Some are useful consumer resources such as www.medicare.gov or the National Association of Insurance Commissioner (NAIC) Shopper’s Guide to LTC. The media has tended to focus on the “horror stories” and “what went wrong” about LTC rather than emphasize the advantages of planning or the positive aspects of various planning options.
Components of Planning for LTC
Planning for LTC requires both awareness and action. o Awareness means being aware of the risks and costs of needing LTC. o Action refers to having the knowledge and motivation to do something about it.
Both of these components are critical for planning.
Why Plan Ahead
There are many reasons why it is important to plan ahead for LTC needs.
Financial considerations are important, but control over care choices and independence from relying on family are equally or even more important.
LTC planning does not take the place of having family members involved in caring for their loved ones. It helps ensure that individuals and their families have other choices.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 31
Why People Don’t Plan Ahead
Even though there are important advantages to planning ahead, people still often do not do so. Even when people are aware of and acknowledge these advantages, there are still emotional and logistical barriers to planning ahead. Some factors are more important for certain people than others, but all play some part. They include:
Lack of awareness of the risks of needing care. While awareness is growing, many people still do not realize that the chance of needing LTC in the future is as high as six out of 10.4 Considering the “risks” that people insure and plan for everyday, it is extraordinary to think that people are not planning for something with such a high probability of occurring.
Lack of awareness of the costs of care and who pays. Even if people do acknowledge the risks, many do not realize that LTC is expensive and that existing insurance, such as Medicare, health plans, or disability coverage does not pay for LTC. Some people understand that Medicaid pays for LTC, but do not understand the eligibility requirements and the nature of choice and coverage available under Medicaid.
Most people do not realize that, if they need LTC for an extended time, it is most likely to be paid for out-of-pocket. Consumer publications review the “government programs” that pay for LTC, but people are likely to skip the “fine print” that goes into more detail about when government programs will and will not pay. People do not understand that LTC is much more than skilled care. They often think that Medicare will cover most of their LTC needs because skilled care is paid for by Medicare. Another source of confusion is the “pie chart” showing that Medicare and Medicaid pay for the majority of care. While this is true on an aggregate basis, most people with income and assets will pay for extended LTC out-of-pocket.
Denial. Many people avoid thinking about or discussing the possibility that they might be disabled or dependent. Many hope that it will not happen to them.
Competing priorities. There are many day-to-day issues as well as long-range plans that require attention, such as saving for college or handling a pressing medical or financial situation. Planning for LTC is often lower priority than other planning priorities.
Difficulty discussing LTC issues. While it is difficult for people to acknowledge that LTC is a possibility in the future, it is also especially difficult to talk with family about LTC issues. However, talking with family is an important part of planning. Adult children feel “guilty” prying into their parents’ lives by discussing plans they may have made. Will their parents think they are trying to shirk their responsibilities to care for their aging parents? Or that they are trying to “insure their inheritance”? Similarly, elderly parents do not want to burden their adult children with the responsibilities for caregiving as they age. Thus, both elderly parents and adult children avoid discussing this important issue.
Understand the benefits of planning. While many people acknowledge the benefits of planning or at least recognize them, they may not have internalized the benefits enough to act on them. Often, other barriers to planning interfere.
Understand how to plan. The “How To” is an important factor for people who need help in planning ahead for LTC. Fear of doing it wrong, or making a mistake or simply not knowing how to begin can hold someone back. People are concerned with “scams” that prey on their worries about health and aging. LTC needs.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 32
What Motivates Planning
Most people learn about long-term care the hard way – when they or a loved one needs care. While most of us do not like to think about it, long-term care needs do arise. And those needs are best met when they are planned for.
Having some LTC experience with loved ones is an important motivating factor because someone who has experienced LTC first hand understands the risks and costs, and the advantages of planning ahead.
Attitudes appear more important in predicting who will and will not plan ahead than demographics. People who understand and acknowledge the risks and costs of needing LTC in the future, and who perceive the value of planning ahead, are much more likely to plan. People who plan ahead for LTC needs are also more likely to be “planners” in other aspects of their lives.
Assess the Risk of Needing Long-Term Care Services
While people can never know for certain if they will need long-term care, assessing their risk factors can help them understand if they are at a higher or lower risk. They might begin by talking with their doctor about whether they might be at increased risk based on medical and family history or lifestyle choices. They will gain a better understanding of risks, and may be able to help decrease their risk. They should also review other risk factors, such as gender.
Think about Where They Want to Receive Care
If they were to need care for an extended period, where would they want to receive it? If they need more information on long-term care services, review the list of services and providers. One way to find out what services are in the community is by contacting the Administration on Aging's Eldercare Locator.
Talk with Their Family
Do they have family (spouse, adult children, and siblings) or friends who would want to or be able to care for them if they became ill or disabled for a long time? How would they feel about relying on their help?
Review Current Insurance Coverage
Does their current health care insurance pay if they need to be in a nursing home or need care at home for an extended illness? Unless they have purchased a specific long-term care insurance policy, their existing medical coverage, Medicare, Medicare supplement, or HMO will provide little if any coverage for long-term care. Review the policies they have with them to learn what is covered and what is not.
Decide if They Can or Want to Pay for Long-Term Care Privately
If they don't have coverage for long-term care or prefer to pay out of their own resources, would they be able to cover all the costs from their retirement income and savings? Think about the

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 33
financial resources they have and how they feel about using them to pay for long-term care. This could include various sources of income (for example, Social Security, pension, interest income, dividends from investments, payments from an IRA or 401 (k)), as well as cash, savings, stocks and bonds, and their home.
Investigate Future Insurance or Benefits They May Qualify For
It is important to know and understand what their future benefits will and will not cover, if they are not yet retired. For those who only have Medicare, even with a Medicare supplemental plan, most of their long-term care services may not be covered. If they have limited resources, now or in the future, Medicaid may pay for their services.
Other Resources that Can Help Cover Long-Term Care Expenses
Most people currently don't have coverage or do not have enough private funds to pay for all their long-term care needs, particularly if service needs are extensive or last a long time. There are an increasing number of private payment options available for this purpose. Two of the more common options are long-term care insurance and reverse mortgages. Review private financing options carefully to ensure that they understand all the details, eligibility requirements, and costs.
Home Modifications Might Help People Stay in Their Home Longer
Most people prefer to remain in their own homes and consider alternatives only if their care needs cannot be met at home. Modifying a home is an important option that can improve their safety and help them perform daily activities such as bathing and cooking. Home modifications range from grab bars in the bathroom and improved lighting to handrails and wider doorways for wheel chair access, or even adding a bathroom on the first floor of a two-story home for someone no longer able to climb stairs.
Some state and local governments have programs to provide loans and grants to help people pay for home modifications.
Consider Moving to a More Suitable Environment
Perhaps moving to a new home will best help people meet their future needs. Consider the variety of options such as moving to a house, condominium, or apartment that is all on one level, or that has elevators instead of stairs. Perhaps they would prefer a small, easy-to-care-for apartment with basic modifications already in place.
Other housing options include Group Homes/Board and Care Facilities, Assisted Living Facilities, and Continuing Care Retirement Communities.
Review or Prepare Helpful Legal Documents
People can simplify things for themselves and their family by gathering important documents, such as their health care proxy, their will, a list of financial accounts and institutions, and keeping them in one place. Leave copies with their attorney and at least one friend or family member.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 34
Agents should remind and assist clients to review plans periodically to be sure that they are still appropriate. Make changes as necessary.
Create a Health Care Proxy or Advance Directive to express their wishes for care in the event that they become seriously ill or disabled.
An Advance Directive is a way for people to tell their family and their caregivers what type of care they would like to have if they are too ill to speak or decide for themselves. There are many different terminologies including Health Care Directive, Advanced Directive, Living Will, and Medical Power of Attorney. Sometimes a Health Care Directive or Advance Directive refers to the combination of a Living Will and a Medical Power of Attorney.
A Living Will allows them to convey their wishes regarding medical and health care treatment when they are unable to communicate those wishes themselves. In a Living Will, they state their wishes in writing, but do not name a person to speak on their behalf.
A Medical Power of Attorney allows them to designate someone to make health care decisions for them when they are unable to do so.
LTC Cost as an Issue – Cost of Care vs. Cost of Insurance
Cost is important and sometimes people feel “trapped” between the high costs of care and the perception of the high cost of planning.
The cost of planning might refer to the emotional and logistical costs of taking the time to think about and plan for LTC needs. It may also refer to the cost of various LTC products.
Interestingly, people often overestimate the cost of LTC insurance. The average premium for people who buy LTC insurance with an average age of 67 is
$1,500 in annual premium.
Planning Case Studies
Below are some examples of how people might plan for long-term care before they need care. While these are fictional illustrations, they represent a variety of real-life situations.
Mrs. F is 81. She has osteoporosis, arthritis, and high blood pressure. Otherwise she is basically healthy, but frail. She lives on a limited, fixed income and does not have significant assets to draw upon to help her meet her long-term care needs. She has been living in a modest one-bedroom rental unit, but is finding it difficult to maintain her apartment on her own.
Plan:
Pay for modifications to daughter's home (outfit spare bedroom and second bathroom for mom).
Move in with daughter. Establish "Advance Directive" and create "Durable Power of Attorney".
Mrs. W is 78. Since having a stroke several years ago, she depends on a wheelchair to get around. She and her husband still live in the three-bedroom house they bought when they were

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 35
first married. The home's value has increased dramatically since they bought it and they paid off the mortgage a few years ago. The upkeep of such a large home is taking a toll on both her and her husband.
Plan:
Sell home and use the resulting proceeds to move to a Continuing Care Retirement Community.
With no children, they decided to establish a Charitable Remainder Trust to pay for their care with the remainder of the trust after they both pass away to the San Diego Zoological Society.
Mr. C is an 82 year old widower. He lives in the modest home in which he raised his children. He has prostate cancer and has had a pacemaker for the past two years. At this point he is still able to take care of all his physical needs and he is very keen on remaining at home to receive the care he needs, because of all the wonderful family memories it holds for him. But his income and assets may not be enough to pay for the care he needs at home.
Plan:
Stay at home and receive care there if necessary. Pay for care with a combination of savings and a reverse mortgage.
Son and daughter to coordinate care and repay the reverse mortgage loan amount upon his death or when and if he needs to permanently move out of the home. His children can keep the house in the family if they wish, after paying off the loan amount or they can sell the home and keep any additional funds from the sale of the home that exceed the loan amount to be repaid.
At 46, Ms S had the opportunity to purchase long-term care insurance as a Federal employee. She chose coverage that will allow her to be cared for at home, in an assisted living facility, or in a nursing home if necessary. She bought the policy now since the cost is based on her age when she buys it. Waiting would only mean higher premiums and the possibility that she might develop a health condition that would cause her to be declined for the insurance. She does not want to have to rely on her family to pay for or provide care for her if and when she needs it. She likes being independent and having peace of mind that comes from planning ahead.
Plan:
Purchase long-term care insurance, which she pays for through an automatic deduction from her paycheck.
Prepare a living will so that her family will know her preferences and wishes for care and life support if she becomes unable to communicate or carry out her preferences on her own.
Speak with daughter and niece and specify her preferences for care.
Role of LTC Agents in Planning for Long-Term Care
Know the financing options for LTC services. Through training, agents should have a good understanding of the financing options for LTC services, including those that are specific to their

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 36
State. By understanding the options and how they can be applied to individual circumstances, agents can help guide the consumer to make a decision that best meets their needs.
Be objective and impartial. Agent’s role is to listen to what the consumer is saying and to provide the pertinent facts. Even if they have firm convictions about the consumer should do, or what is best, it is their responsibility to simply tell the consumer what the options are. Any decision to buy or not is the responsibility of the consumer.
Help the consumer either broaden or narrow the options. Depending on the individual consumer, it may be important for him or her to consider unexplored options or narrow them down to fit circumstances. Not every consumer needs to know everything about LTC financing options. By listening carefully, agents can help the consumer start down the right road.
When in doubt, refer. No one can know everything about LTC. The agent’s job is to help the consumer understand that there are options; explain those options to the best of their ability, and to appropriately refer the consumer to other experts (such as accountants or attorneys) for more assistance.
Understand Your Client
Everyone’s circumstance is different Listen to consumers and allow them to make their own decisions Agents should place their values aside and allow consumers to make their own
decisions. Agents should assess the consumer’s knowledge, and provide appropriate information.
Common Barriers to Planning
Research indicates that there are many barriers that prevent people from planning for their LTC needs. Understanding these barriers will help agents to motivate consumers. There are four general types of barriers:
Knowledge Structural Perception Social and Cultural
Knowledge Barriers
Many people underestimate the likelihood of needing LTC services and the cost of care. Another common misconception is that Medicare will cover LTC services. Emphasize
that Medicare pays only 20 percent of LTC costs and that Medicaid coverage is limited.5 Many individuals have negative views of nursing homes and assume LTC refers only to
nursing home care. Emphasize that LTC includes other services such as home health care and assisted living.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 37
Overcoming Knowledge Barriers
Make sure consumers have a clear understanding of what LTC is. Clarify the misperception that LTC is just about nursing home care.
Clarify that LTC encompasses a range of service settings, including home health care and assisted living.
It is important to emphasize that Medicare does not pay for most LTC services and that Medicaid coverage is limited.
By clarifying common misconceptions, agents will help consumers get a better grasp of their situation and recognize the need to begin planning.
Structural Barriers
LTC financing options are complex. Individuals may become overwhelmed by the amount of information and decide to delay dealing with the issue until a later date.
Many people with low incomes may not be able to afford LTC insurance and are unaware of other planning options.
Overcoming Structure Barriers
Be patient with clients. Do not overwhelm consumers with too much information. LTC insurance is one option. There are other financing options also available.
Perception Barriers
Denial. One of the most prevalent consumer perceptions is that they will never personally be affected by LTC needs or find him or herself in a LTC situation. Among adult children, there is a tendency to believe that their parents are still young, will remain healthy and will not need LTC.
Fear. Some individuals fear needing LTC services or being in an LTC situation. Feeling Overwhelmed. Active planning is usually triggered by a family crisis or a life-
altering event. During or after this period of stress, individuals tend to be overwhelmed by the amount of information available. They may also find that their options are limited due to lack of planning, which may add to their feeling of being overwhelmed.
Unfortunately, many families and individuals wait until they are faced with a LTC crisis to seek help. At this stressful time, individuals are often overwhelmed by the amount of information presented and by the need to make a fast decision. In addition, their choices may be limited due to lack of planning.
Reluctance to Purchase another Insurance Product. Negative impressions people have about LTC insurance generally focus on the cost of the premium and perception that the price exceeds the value of the coverage. In addition, for some, there is also a stigma attached to purchasing another health insurance product.
Competing Priorities. Competing priories such as children’s education or caring for an elderly parent may delay planning.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 38
Provide appropriate referrals. Emphasize to consumers that there are many organizations that can help them find the appropriate services.
Overcoming Perception Barriers
Help consumers relate to the need to start planning by describing a situation where LTC services planning helped an individual deal with an unexpected event. Personalize the information by asking them if they know someone who needed LTC services and what those persons decided to do.
Appeal to consumers’ sense of independence and emphasize quality of life. Show empathy for a consumer’s situation. Introduce one topic at a time, and always follow-up each topic with questions to make
sure that consumers understand the information presented. Emphasize the benefits of advanced planning. Do not present options that may not be available to the consumer.
Social & Cultural Barriers
Culture and background shape people’s perception of aging and the role of the family in providing care for the elderly. For instance, research shows that African-Americans and Hispanics tend to think that LTC services will be covered by Medicare, current health insurance coverage, or pension plans. A recent AARP study shows that large numbers of Hispanics, African-Americans, and Asian-Americans care for their parents or other aging relatives.6 Specifically, 42 percent of Asian-Americans, 34 percent of Hispanics and 28 percent of African-Americans surveyed by AARP serve as the primary caregiver to their parents.
In addition, immigrants may have difficulty with English and lack familiarity with the U.S. health care system, which may make planning seem even more daunting.
Communication and Comprehension Issues. Elderly individuals may suffer from cognitive impairment and thus may not understand the LTC options available to them. Furthermore, language and literacy barriers may also lower consumers’ ability to comprehend their options fully.
Misperception of Assistance Provided by Family Members. Many people believe that family members will provide LTC assistance. Research shows that Native Americans and Hispanics are more likely than Caucasians to rely on their family to provide for their LTC needs. Reliance on adult children is especially prevalent among Asian-Americans.
Overcoming Social & Cultural Barriers
Keep in mind that people from different cultures may have varying beliefs and ideas about LTC needs and services.
Asian-Americans, Native-Americans, and Hispanics focus more heavily on family relationships. LTC discussions should focus on the benefits of planning to the family, such as financial security, emotional and physical relief, and maintaining quality relationships.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 39
Some immigrants may not be familiar with the U.S. health care system. The individual may come from a country where there is a universal health care system, and may erroneously assume that Medicare will pay for all LTC services. Provide a brief overview of the health care system emphasizing that Medicare pays for a limited amount of LTC services.
When working with an individual who is not fluent in English, speak clearly and avoid using technical terms. Arrange for an interpreter if needed.
Avoid generalizations. Keep in mind that everyone’s situation is different. As always, listen carefully to a consumer’s specific needs.
Planning Information and Resources
Information about long-term care planning is available from many sources.
The state or local department of aging: Look for “aging” or “human services” in the local government blue pages of the phone book for the number. Specific resources to ask for include State Health Insurance Assistance Programs, and in many states Aging and Disability Resource Centers (ADRC).
The National Association of Insurance Commissioners' (NAIC) Shopper's Guide. The State Insurance Department will have information about long-term care insurance in
the area. They also often offer a shoppers' guide to long-term care insurance. The Administration on Aging's national Eldercare Locator (1-800-677-1116, weekdays
9:00 a.m. to 8:00 p.m. (ET)) provides information including where to find specific services and supports in the community.
Long-Term Care Clearinghouse
Part of the DRA – Directed by HHS and is charged with:
Educating consumers about LTCI; Providing objective information to assist consumers Maintaining a list of states with partnerships that provide reciprocity
Funding for the Clearinghouse is set at $3 million annually from FY 2006 through FY 2010. The clearinghouse is an attempt to provide objective information to consumers to consider their LTC options based on their particular circumstances. Information is established to educate consumers on availability or limitations of coverage for LTC under Medicaid.
Will also provide contact information for obtaining State-specific information on LTC coverage, including eligibility and estate recovery requirements, and provide objective information to assist consumers with decision-making process for determining:
whether to purchase LTCi or pursue other private market alternatives
Agents should include contact information for additional objective resources on planning for LTC needs.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 40
http://www.longtermcare.gov/LTC/Main_Site/index.aspx
Own Your Future Long-Term Care Awareness Campaign
A joint federal-state initiative to increase awareness about the importance of planning for future long-term care needs. A letter discussing the importance of long-term care planning, signed by the Governor, is sent to households with members between the ages of 45 to 70.
The Long-Term Care Planning Kit is available to residents of all states; however, specific additional activities complement the campaign in the participating states. When someone from a campaign state orders the Long-Term Care Planning Kit, they also receive an insert to the kit with information about planning resources and long-term care information services in their state.
Another key component of the "Own Your Future" Campaign is a Governor's press conference to launch the Campaign. The press conference is held concurrent with the mailing of the Governor's letter. The purpose of the press conference is to generate local media interest in the campaign and reinforce the message being sent to targeted households in the letter from the Governor.
Other State Resources
Many states are now creating websites specifically to educate consumers about the LTC Partnership Programs. Check with your state’s Department of Insurance or Commerce and Department of Health Services.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 41
Chapter Three – Public Programs to Pay for Long-term Care
This chapter provides a general overview of the public options available to pay for long-term care (LTC). Medicare and Medicaid are the two major public funding sources for LTC. The Medicare program however provides limited LTC coverage. State Medicaid programs provide a more generous benefit package for LTC services than Medicare; however these services are limited to individuals who lack the financial resources to pay for their own care.
Upon completion of this chapter, agents should be able to explain when and under what conditions public programs will pay for LTC services.
Payment Sources for Long-Term Care
Someone with sufficient income and assets, is likely to pay for long-term care needs on their, out of those private resources. For those who meet functional eligibility criteria and have limited financial resources, or deplete them paying for care, Medicaid may pay for care. If they require primarily skilled or recuperative care for a short time, Medicare may pay. The Older Americans Act is another Federal program that helps pay for long-term care services. Some people use a variety of payment sources as their care needs and financial circumstances change.
Long-Term Care
Service
Medicare Private Medigap Insurance
Medicaid Pay on Their Own*
Nursing Home Care
Pays in full for days 0-20 if in a Skilled Nursing Facility following a recent hospital stay. If the need for skilled care continues, may pay for days 21 through 100 after a co-payment
May cover the $124/day co-payment if the nursing home stay meets all other Medicare requirements.
May pay for care in a Medicaid-certified nursing home if they meet functional and financial eligibility criteria.
If they need only personal or supervisory care in a nursing home and/or have not had a prior hospital stay, or if they choose a nursing home that does not participate in Medicaid or is not Medicare-certified.
Assisted Living Facility (and similar facility options)
Does not pay Does not pay In some states, may pay care-related costs, but not room and board
They pay on their own except under Medicaid if eligible.
Continuing Care Retirement Community
Does not pay Does not pay Does not pay They pay on their own
Adult Day Services
Not covered Not Covered Varies by state, financial and functional eligibility required
They pay on their own except under Medicaid if eligible.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 42
Home Health Care
Limited to reasonable, necessary part-time or intermittent skilled nursing care and home health aide services, and some therapies that are ordered by their doctor and provided by Medicare-certified home health agency. Does not pay for on-going personal care or custodial care needs only (help with activities of daily living).
Not covered Pay for, but states have option to limit some services, such as therapy
They pay on their own for personal or custodial care, except under Medicaid, if eligible.
National Spending on Long-Term Care
The total amount spent on long-term care services in the United States (in 2003) was $183 billion. This does not include care provided by family or friends on an unpaid basis (often called “informal care.”) It only includes the costs of care from paid providers.
On an aggregate basis, the biggest share, 48 percent, is paid for by Medicaid. On an individual basis, however, “who pays for long-term care” can look very different. This is because people with their own personal financial resources do not qualify for Medicaid unless they use up their resources first paying for care, so-called “spending down”. Those who have reasonable income and assets will most likely pay for care on their own.
Also, while Medicare overall pays for 18 percent of long-term care it only pays under specific circumstances. If the type of care needed does not meet Medicare's rules, Medicare will not pay and they are likely to pay for care on their own.
Public Programs that Pay for Long-Term Care
A number of public programs provide help paying for long-term care services. Each program has specific rules for what types of services it covers, how long one can receive services,

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 43
eligibility for coverage, and, in some cases, cost sharing. For example, some programs, such as the Older Americans Act, focus on home- and community-based services, while the Medicare program only pays for some short-term nursing home stays or home health care. The following section provides information on some of the major public programs that may help pay for long-term care services.
Medicare
Established in 1965, Medicare is a social insurance program, like Social Security, that provides health and financial security for individuals age 65 and older and for younger people with permanent disabilities. Prior to 1965, roughly half of all seniors lacked medical insurance; today, virtually all seniors have health insurance under Medicare.
Key Facts about Medicare
Medicare is a federal government program that covers 35.8 million Americans age 65 and older.
Source: Centers for Medicare and Medicaid Services (2006). “2006 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Introduction: Highlights.” May 1, p.2.
It also covers 6.7 million people with disabling illnesses.
Source: Centers for Medicare and Medicaid Services (2006). “2006 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Introduction: Highlights.” May 1, p.2.
By the year 2030, when the youngest of the baby boomers will have turned 65, the rolls of Medicare beneficiaries will have swelled to 78 million – almost double the 2005 enrollment.
Source: Centers for Medicare and Medicaid Services (2006). “2006 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds”. May 1, p. 34.
Annual Medicare expenditures by the federal government are expected to almost double between 2007 and 2017, from $428 billion to $851 billion.
Source: Congressional Budget Office (2007). "The Budget and Economic Outlook: Fiscal Years 2008 to 2017." January, p. 54. Years refer to calendar years, unless otherwise noted.
There were 3.9 workers for every Medicare beneficiary in 2004. By 2030, however, there will be only 2.4 workers paying taxes to cover each Medicare beneficiary for Medicare Part A, which covers most hospital care.
Source: Centers for Medicare and Medicaid Services (2006). “2006 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds”. May 1, p. 58.
Medicare provides health insurance coverage to almost 44 million people – approximately 37 million people age 65 and older and another 7 million people with permanent disabilities who

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 44
are under age 65. The program helps to pay for many important health care services, including hospitalizations, physician services, and a new prescription drug benefit. Individuals contribute payroll taxes to Medicare throughout their working lives and generally become eligible for Medicare when they reach age 65, regardless of their income or health status.
Comprising 13 percent of the federal budget and 19 percent of total national health expenditures in 2006, Medicare is often a significant part of discussions about how to moderate the growth of both federal spending and health care spending in the U.S. With the dual challenges of providing needed and increasingly expensive medical care to an aging population and keeping the program financially secure for the future, discussions about Medicare are likely to remain prominent on the nation’s agenda in the years to come.
Source: The Medicare share of the federal budget is from Congressional Budget Office (CBO), Budget and Economic Outlook: Fiscal Years 2008 to 2017, January 2007. The Medicare share of national health expenditures is projected for 2006, from Christine Borger, et al, Health Spending Projections through 2015:Changes on the Horizon, ”Health Affairs Web Exclusive, 22 February 2006.
Characteristics of People with Medicare
Medicare covers a population with diverse needs and circumstances.
While many beneficiaries enjoy good health, a quarter or more have serious health problems and live with multiple chronic conditions, including cognitive and functional impairments. Many Medicare beneficiaries live on modest incomes and most depend on Social Security as their primary source of income. Almost half of all Medicare beneficiaries (47 percent) had an income below 200 percent of poverty ($20,420/individual and $27,380/couple in 2007), and 12 percent had an income below 100 percent of the poverty level.
There is a high prevalence of chronic conditions, cognitive impairments, and functional limitations among the Medicare population. 36 percent of all Medicare beneficiaries have three or more chronic conditions. Among the most common are hypertension and arthritis. More 29 percent of all beneficiaries have a cognitive or mental impairment that limits their ability to function independently. Approximately one in six (16 percent) beneficiaries have functional limitations as defined as two or more limitations in activities of daily living, such as eating or bathing.
Although the majority of the Medicare population is over age 65, about 15 percent are under age 65 and permanently disabled. These individuals tend to have lower incomes than other beneficiaries. About 40 percent are dually eligible for both Medicare and Medicaid. Because of their disabilities, they tend to have relatively high rates of health problems, including functional limitations and cognitive impairments.
Most beneficiaries live at home, but 5percent live in a long-term care setting. Five percent (2.2 million) of Medicare beneficiaries live in a long-term care setting, such as a nursing home or assisted living facility, with higher rates for beneficiaries ages 85+ (20 percent). More than two-thirds of beneficiaries living in long-term care settings are women.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 45
Nearly half of all Medicare beneficiaries have incomes below 200 percent of the federal poverty level (FPL), but poverty rates are especially high among those in racial/ethnic minority groups, women, people under-65 with disabilities, and those ages 85 and older.
More than 70 percent of African American and Hispanic beneficiaries live on an income below twice the poverty level, and more than a third of these beneficiaries have incomes below the poverty level. By contrast, 28 percent of White beneficiaries have an income below twice the poverty level and 12 percent have incomes below poverty. Nearly two-thirds of all underage 65 beneficiaries with disabilities live on income below twice the poverty rate, and more than a third live in poverty. Among seniors, poverty rates tend to rise with age. Close to six in ten beneficiaries age 85 and older live on income below twice the poverty level. Poverty rates are substantially higher among women on Medicare than men. More than half of all female Medicare beneficiaries live on income below twice the poverty rate, substantially higher than the rate for men on Medicare.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 46
Poverty among the Medicare Population, 2005
Note: In 2005, the federal poverty thresholds for people 65 years and older were $10,210 for an individual and $13,690 for a couple. SOURCE: U.S. Census Bureau, Current Population Survey, 2006 Annual Social and Economic Supplement.
Overview of Medicare
Medicare is a federal health insurance program for people over the age of 65 and individuals with certain disabilities or permanent kidney failure. Congress established the Medicare program in 1965 under the Social Security Act. It was designed to help pay hospital and physician bills to help ensure health care in old age or in the event of disability. Most people think that Medicare pays for LTC, but it was never intended to cover LTC services.
Medicare is generally available for people over age 65 and the disabled. It only pays limited amounts for skilled care following a hospital stay and it is not intended to cover care that assists people with activities of daily living for long periods of time. Specifically, Medicare covers the first 100 days of skilled care in a nursing home after a hospital stay of at least 3 days and as long as they enter a nursing home within 30 days of leaving the hospital. Medicare covers some home health care for the treatment of an illness or injury.
Medicare’s Coverage of LTC
Medicare’s nursing home benefit is limited to post-acute care Medicare’s home health benefit is limited to the need for skilled nursing care on an
intermittent bases, or for specific therapies (e.g., physical or speech therapy)

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 47
Skilled nursing care (e.g., help with medications or care for bandages and wounds) is the only type of nursing home care covered by Medicare. Other types of care, such as help with the everyday activities of daily living (e.g., bathing or dressing), are not covered.
Medicare is a federal program that, according to the program’s trustees, helped about 42 million Americans with their medical bills in 2006 – including bills for hospital care, physician care and care by certain other health care professionals.1 Medicare services are available to all those 65 years or older who are U.S. citizens or legal residents living in the U.S. for five years in a row.2 Also eligible are individuals younger than 65 with certain conditions or permanent disabilities, described below.3
1 Congressional Budget Office (2007). "The Budget and Economic Outlook: Fiscal Years 2008 to 2017." January, p. 54. Years refer to calendar years, unless otherwise noted. 2 Medicare Rights Center. “Q&A: Eligibility.” 3 The Henry J. Kaiser Family Foundation. (2002). “Medicare's Disabled Beneficiaries: The Forgotten Population in the Debate over Drug Benefits.” (2002).
Like Social Security, Medicare depends on today’s workers paying the costs of today’s beneficiaries (referred to as the “pay as you go” system). Employers and employees each pay a Medicare tax of 1.45 percent of the employee’s income for beneficiaries’ hospital care.
But Medicare doesn’t cover all of beneficiaries’ medical expenses. In fact, it pays for only two-thirds of the cost of the services it does cover, and it provides no coverage at all for items such as dental care, eyeglasses and hearing aids.4 It also doesn’t cover long-term care.
4 Davis, Karen; Marilyn Moon; Barbara Cooper; Cathy Schoen (2005). “Medicare Extra: A Comprehensive Benefit Option For Medicare Beneficiaries.” Health Affairs, Oct. 4.
Most beneficiaries are in Medicare’s “original” or “traditional” fee-for-service program. But a growing number (almost 15 percent in 2006) are enrolled in Medicare managed care plans, under the Medicare Advantage program.5
5 Congressional Budget Office (2006) “Fact Sheet for Cob’s March 2006 Baseline: Medicare.”
Medicare Eligibility
Part A
Most people age 65 and older are automatically entitled to Part A if they or their spouse are eligible for Social Security payments and have made payroll tax contributions for 10 or more years (40 quarters). Individuals do not need to meet an income or asset test to qualify for Medicare. Adults under age 65 with permanent disabilities who receive Social Security Disability Income (SSDI) payments for 24 months are eligible for Medicare before they turn 65, even if they have not made payroll tax contributions for 40 quarters. People with end-stage renal disease (ESRD) or Lou Gehrig’s disease are eligible for Medicare benefits as soon as they begin receiving SSDI payments, without having to wait 24 months. Individuals entitled to Part A do not pay premiums for covered services. Individuals age 65 and over who are not entitled to Part A benefits, such as those who did not pay enough Medicare taxes during their working years, can pay a monthly premium to enroll.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 48
Part B
Part B is voluntary, but about 95 percent of beneficiaries with Part A are also enrolled in Part B. For most individuals who become entitled to Part A benefits, enrollment in Part B is automatic unless the individual declines enrollment. Individuals age 65 and older who are not entitled to Part A benefits may enroll in Part B. With the exception of the working aged who may delay enrollment because they receive employment-based coverage, those who do not sign up for Part B when they are first eligible typically pay a penalty for late enrollment, in addition to the regular monthly premium, for the duration of their enrollment in Part B.
Part C
Beneficiaries may generally elect to enroll in a Medicare Advantage plan on an annual basis between November 15 and March 31 of the following year.
Part D
To get Part D benefits, beneficiaries may enroll in a stand-alone prescription drug plan or Medicare Advantage prescription drug plan. The enrollment period for stand-alone prescription drug plans runs from November 15 to December 31 of each year. Individuals can enroll in a Medicare Advantage plan from November 15 through March 31 of the following year. Similar to Part B, there is a permanent premium penalty for late enrollment for individuals who go for an extended period of time without drug coverage that is at least comparable to the Part D standard benefit (known as “creditable coverage”).
Anyone age 65 or older is eligible for Medicare, if the person is a U.S. citizen or a legal non-citizen residing in the U.S. for five continuous years at the time they apply for the program. As of 2005, 35.8 million Medicare beneficiaries fit this description.6
6 Centers for Medicare and Medicaid Services (2006). “2006 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Introduction: Highlights, p. 2.” May 1.
The program also covered 6.7 million people under age 65 with disabling conditions.7 Most people who qualify for cash benefits under Social Security Disability Insurance (SSDI) can obtain Medicare-covered services after a two-year wait.8 Individuals with end stage renal disease or amyotrophic lateral sclerosis (ALS, also known as Lou Gehrig’s disease) have shorter waiting periods, or none.9
7 Centers for Medicare and Medicaid Services (2006). “2006 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Introduction: Highlights.” May 1, p.2. 8 Centers for Medicare and Medicaid Services, Medicare Enrollment Reports, National Trends 1966-2005, 9 Medicare Rights Center. Q&A: Eligibility.
Medicare is a Federal program designed to cover health care for people age 65 and older, people under age 65 with certain disabilities, and people of all ages with end-stage renal disease (permanent kidney failure requiring dialysis or a kidney transplant.) It only covers

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 49
medically necessary care and focuses on medical acute care (doctor visits and hospital stays) or short-term services for conditions expected to improve.
The Different Parts of Medicare
The law that governs Medicare divides it into four parts, covering different types of health care and with different sources of funding.
Part A – Hospital Insurance
Part A, also known as the Hospital Insurance (HI) program, covers inpatient hospital services, skilled nursing facility, home health, and hospice care. Part A is funded by a dedicated tax of 2.9 percent of earnings paid by employers and workers (1.45 percent each). In 2006, Part A accounted for approximately 40 percent of Medicare benefit spending. An estimated 43.4 million people were entitled to Part A in 2007.
Funding for Medicare comes primarily from payroll tax revenues, general revenues, and premiums paid by beneficiaries. Medicare is funded as follows:
Part A, the Hospital Insurance (HI) Trust Fund, is financed largely through a dedicated tax of 2.9 percent of earnings paid by employers and their employees (1.45 percent each). In 2007, these taxes are estimated to account for 86 percent of the $216 billion in revenue to the Part A Trust Fund.
Part A helps pay for in patient care provided to beneficiaries in hospitals and short-term stays in skilled nursing facilities, and also covers hospice care, post-acute home health care, and pints of blood receive data hospital or skilled nursing facility. Most beneficiaries do not pay a monthly premium for Part A services, but pay a deductible before Medicare coverage begins. In 2007, the Part A deductible for each “spell of illness” is $992 for an inpatient hospital stay. Beneficiaries typically pay a coinsurance for benefits covered under Part A, including extended inpatient stays in a hospital ($248 per day for days 61-90) or skilled nursing facility ($124 per day for days 21-100). There is no co-payment for home health visits.
Part B – Medical Insurance
Part B, the Supplementary Medical Insurance (SMI) program, helps pay for physician, outpatient, home health, and preventive services. Part B is funded by general revenues and beneficiary premiums ($93.50 per month in 2007). In 2006, Part B accounted for 35 percent of benefit spending. Beginning in 2007, Medicare beneficiaries who have annual incomes over $80,000 ($160,000 per couple) pay a higher, income-related Part B premium ranging from $105.80 to $161.40. The income thresholds are indexed annually to limit the number of beneficiaries who would be subject to the higher premium in subsequent years. Part B benefits are subject to an annual deductible ($131 in 2007). Most Part B services are subject to a coinsurance of 20 percent. Part B is voluntary; some beneficiaries (such as the working aged who receive employer-sponsored health care) delay enrollment until they retire. An estimated 40.6 million people were enrolled in Part B in 2007.
Part B, the Supplementary Medical Insurance (SMI) Trust Fund, is financed through a combination of general revenues and premiums paid by beneficiaries. Premiums are

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 50
automatically set to cover 25 percent of revenues in the aggregate. In 2007, Part B revenue is estimated to be $194 billion.
Part B helps cover physicians’ services, outpatient medical and surgical services and supplies, physical, occupational and speech therapy, diagnostic tests, and some preventative and durable medical equipment (DME). Part B also covers some home health care services not already covered under Part A; it covers some home care for a beneficiary who is not covered by Part A, when there was no prior hospital admission, or if the care exceeds 100 days.
Some beneficiaries with low incomes and assets are not required to pay the monthly Part B premium (or cost-sharing requirements), because they qualify for additional assistance under the Medicare Savings Programs.
Part C - Medicare Advantage
Part C, the Medicare Advantage program, allows beneficiaries to enroll in a private plan, such as a health maintenance organization (HMO), preferred provider organization (PPO), or private fee-for-service (PFFS) plan. These plans receive payments from Medicare to provide Medicare-covered benefits, including hospital and physician services, and in most cases, prescription drug benefits. Part C is not separately financed, and accounted for 14 percent of benefit spending in 2006. As of January 2007, 8.3 million beneficiaries are enrolled in Medicare Advantage plans.
Medicare Advantage plans cover all of the benefits provided under Parts A, B, and D (the Medicare prescription drug benefit), and sometimes additional benefits not otherwise covered. Medicare Advantage plans are paid a fixed monthly amount for each beneficiary enrolled.
Part D - Medicare’s prescription drug benefit
Part D helps pay for out patient prescription drug coverage through private health plans. Plans are required to provide a “standard” benefit or one that is actuarially equivalent, and may offer more generous benefits. In general, individuals who sign up for a Part D plan pay a monthly premium, along with cost-sharing amounts for each prescription.
Individuals with modest income and assets are eligible for additional assistance with premiums and cost-sharing amounts. Part D is funded by general revenues, beneficiary premiums, and state payments, and accounted for 8 percent of benefit spending in 2006. As of January 2007, nearly 24 million beneficiaries are enrolled in a Part D plan.
Part D is financed through general revenues, beneficiary premiums, and state payments for dual eligibles (who received drug coverage under state Medicaid programs prior to 2006). In 2007, Part D revenue is projected to be $64 billion, 78 percent of which will be from general revenues.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 51
Excluded or Limited in Medicare
Despite the important protections provided by Medicare, there are significant gaps in Medicare’s benefit package. In addition to the fairly high cost-sharing requirements for covered benefits, Medicare does not pay for many relatively expensive services and supplies that are often needed by the elderly and younger beneficiaries with disabilities. Most notably, Medicare does not pay for custodial long-term care services either at home or in an institution, such as a nursing home or assisted living facility. Although many beneficiaries have supplemental insurance to help cover these expenses, they may still face significant out-of-pocket costs to meet their medical and long-term care needs. Here are some of the services that Medicare does not cover (although some are covered by Medicare supplemental, or Medigap, policies which many beneficiaries purchase separately).10
10 Medicare Rights Center “What Medicare Covers.”
Acupuncture Dental care Care outside the United States Most chiropractic services Cosmetic surgery Custodial care (unless skilled nursing care is provided) Eyeglasses (except after cataract surgery) Hearing aids (except certain implants for extreme hearing loss) Long-term care Personal care services Private duty nursing

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 52
Medicare Modernization Act of 2003
As part of the Medicare Modernization Act of 2003 (MMA), Medicare expanded coverage under its managed care plans so that such plans are available to nearly every senior nationwide. The MMA aimed to provide drug coverage exclusively through private plans, with some exceptions, and one of the ways seniors were to receive their drug coverage was by enrolling for all-inclusive coverage in the health maintenance organizations, preferred provider organizations and other private plan options authorized by Medicare.
The Congressional Budget Office (CBO) projects that managed care enrollment will expand to 17.5 percent of beneficiaries in 2016, from 14.7 percent in 2006.11 The percentage could go even higher if the Medicare prescription drug benefit turns out to be more popular than the CBO expects.
11 Congressional Budget Office (2006). “Fact Sheet for CBO’s March 2006 Baseline: Medicare.”
Medicare Provides Limited Coverage for LTC Services
What Medicare Covers
Medicare provides coverage of basic health services including care in hospitals and other settings, physician services, diagnostic tests, preventive services and, as of 2006, also includes an outpatient prescription drug benefit. Beneficiaries generally pay varying deductibles and coinsurance amounts that are indexed to increase annually.
Generally, Medicare does not pay for most long-term care. Medicare does not pay for personal or custodial care (help with Activities of Daily Living), which is the greatest part of long-term care services. Medicare will help pay for a limited skilled nursing facility stay, hospice care or home health care for those who meet certain conditions described below.
Medicare will pay for care in a skilled nursing home when someone:
Has had a recent prior hospital stay of at least three days, Is admitted to a Medicare-certified nursing facility within 30 days of their prior hospital
stay, and Needs skilled care such as skilled nursing services and/or physical or other types of
therapy.
If all these conditions are met, Medicare pays a portion of the costs for up to 100 days. For the first 20 days, Medicare pays 100 percent of skilled nursing facility costs. For days 21-100, individuals pay their own expenses up to $124/day (as of 2007) and Medicare pays the balance, if any. People must pay 100 percent of costs for each day in a skilled nursing facility stay after day 100.
Medicare payments for home health care are limited to reasonable and necessary part-time or intermittent skilled nursing care and home health aide services as well as physical therapy, occupational therapy and speech-language pathology that are ordered by their doctor and provided by a Medicare-certified home health agency. It also includes medical social services, durable medical equipment (such as wheelchairs, hospital beds, oxygen, and walkers), medical

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 53
supplies, and other services. Unlike nursing home services, there is no co-pay for home health. There is also no limit on the duration of service as long as services continue to be medically necessary and their doctor requests or reorders these services at least every 60 days.
Hospice care is covered for people with a terminal illness, generally individuals who are not expected to live more than six months. Services include drugs for symptom control and pain relief, medical and support services from a Medicare-approved hospice provider, and other services not otherwise covered by Medicare (such as grief counseling). Hospice care is usually provided in the home (which may include a nursing home if that is where they live) or in a hospice care facility. However, Medicare does cover some short-term hospital and inpatient respite care ¾ care provided to a hospice patient to allow the usual caregiver to rest.
Medicare Nursing Care
There are three different levels of nursing care Medicare only pays for the first one:
Skilled care is medical or nursing care (such as help with medications, caring for bandages and wounds) and therapies (such as occupational, speech, respiratory, and physical therapy). Skilled care is usually delivered by a nurse, therapist or other trained and licensed professional. Most people think of skilled services when they think of LTC. But the reality is that less than 15 percent of all persons who need LTC require skilled care.
Personal care or custodial care is help with the everyday activities of daily living, such as bathing and dressing. The goal of personal care is to provide help with activities that an individual is unable to perform on his/her own. Most people who need LTC need this type of personal care, not skilled care.
Supervisory care provides monitoring and supervision, a safe or controlled environment and stand-by help with activities of daily living to ensure that individuals do not harm themselves or others. Supervisory care is often needed because of a severe cognitive impairment.
Skilled Nursing Facility Care (SNF)
The skilled nursing facility benefit is a limited benefit provided by Medicare. Most of the LTC services that people need are not skilled care, which is the only type of LTC care Medicare will cover.
SNF care is designed to help rehabilitate patients following hospitalization, and is time-limited The Skilled Nursing Facility (SNF) benefit was originally enacted to extend hospital care for patients recovering from an acute illness, but who could be more economically served in a skilled nursing facility.
Medicare will only pay for skilled nursing care or rehabilitative services under very limited circumstances:
The beneficiary’s physician has determined that the beneficiary needs daily skilled care; The beneficiary’s care begins within 30 days of a hospital stay of at least three (3) days
for the same condition. However, about 50 percent of the people who need nursing home care do not first require care in a hospital;

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 54
The beneficiary receives care only in a Medicare-certified skilled nursing facility and must be placed in a Medicare-certified bed. Note: Not all nursing homes are Medicare-certified.
For each benefit period*, Medicare provides limited payment for skilled nursing home care as follows:
Medicare pays for 100 percent of eligible charges for the first 20 days The beneficiary makes a daily co-payment ($124 for 2007) for days 21-100. Medicare
pays the balance of costs, if any. Medicare payments end after 100 days.
However, most people do not require 100 days of skilled care in a nursing facility. Generally, after a couple of weeks of skilled care, they have stabilized and require only custodial care. In most cases, Medicare pays for less than three weeks of skilled care.
*A benefit period begins when an individual is admitted to the hospital and ends when that individual has been released from the hospital or skilled nursing facility (SNF) for 60 consecutive days, or when he or she has remained in a SNF but has not received daily skilled care.
Future Medicare Enrollment and Financing
In 2006, Medicare benefit payments totaled $374 billion, accounting for 13 percent of federal spending.
Inpatient hospital services comprised the largest share of Medicare benefit payments (34 percent), followed by physician and other outpatient services (24 percent). Spending on the new prescription drug benefit accounted for 8 percent of total benefit payments in 2006. With the addition of prescription drug coverage, the composition of Medicare expenditures is changing. CBO projects that by 2010, prescription drugs will account for 20 percent of Medicare benefit payments.
Net federal spending on Medicare is projected to increase from $374 billion in 2006 to $564 billion in 2012, according to CBO. The annual growth in Medicare spending is influenced by factors that affect health spending generally, including increasing volume and utilization of services and higher prices for health care services.
SOURCE: Congressional Budget Office, Medicare Baseline, March 2006.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 55
Medicare’s share of national personal health care expenditures varies by type of service, reflecting benefits covered and services used by the Medicare population.
Medicare spending is highly concentrated among a small share of beneficiaries. A small share of the Medicare population accounts for a majority of Medicare spending. Ten percent of beneficiaries accounted for more than two-thirds of Medicare spending in 2003.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 56
Medicare spending varies by eligibility category. In 2003, Medicare spending for each beneficiary averaged $5,694. Per capita payments were nearly $1,000 higher for the elderly ($6,191) than they were for under-65 beneficiaries with disabilities ($5,325). Per capita spending was highest for those beneficiaries with ESRD -$48,947 on average in 2003–who comprise less than one percent of the total Medicare population.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 57
Looking to the future, Medicare is expected to face significant financing challenges due to the aging of the U.S. population, the declining ratio of workers to beneficiaries, increasing health care costs, and various economic factors. A number of measures are used to assess the long-term financial status of Medicare.
Medicare spending as a share of gross domestic product (GDP) is one of several measures reported by the Medicare Trustees in their annual report to the Congress. With the aging population and expected increases in overall health care costs, Medicare spending is projected to grow at a faster rate than the overall economy. If current trends continue, Medicare expenditures as a share of GDP are projected to rise from 3.1 percent of GDP in 2007 to 7.3 percent of GDP in 2035.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 58
Medicare Benefits and Cost-Sharing Requirements, 2008
PART A
Deductible $1024 per benefit period Inpatient hospital
Days 1-60 No coinsurance Days 61-90 $256 per day Days 91-150 $512 per day After 150 days $512 per day for 60 lifetime reserve days
Skilled nursing facility Days 1-20 No coinsurance Days 21-100 $128 per day After 100 days Not covered
Home Health No coinsurance; no limit on number of visits Hospice Copayment of up to $5 for outpatient drugs and 5%
coinsurance for inpatient respite care Inpatient psychiatric hospital Up to 190 days in a lifetime
PART B
Deductible $135 Physician and other medical services
MD accepts assignment 20% coinsurance MD does not accept assignment 20% coinsurance, plus up to 15% above the Medicare-
approved fee Outpatient hospital care Coinsurance or copayment based on diagnosis Ambulatory surgical services 20% coinsurance Diagnostic tests, X-rays, and lab services 20% coinsurance Durable medical equipment 20% coinsurance Physical, occupational, and speech therapy 20% coinsurance; benefit limit of $1,780 Clinical diagnostic laboratory services No coinsurance Home health care No coinsurance; no limit on number of visits Outpatient mental health services 50% coinsurance One-time “Welcome to Medicare” physical 20% coinsurance Preventive services
Flu shots, Pneumococcal vaccines No coinsurance; one flue shot per flu season limit Hepatitis B vaccine; colorectal and prostate cancer screenings; pap smears; mammograms; abdominal aortic aneurysm (AAA) screenings
Deductible and coinsurance waived for certain preventive services such as colorectal cancer screenings and AAA screenings
Bone mass measurement, diabetes monitoring; glaucoma screening
20% coinsurance
PART D
Information below applies to the standard Part D benefit design in 2008. Benefits and cost-sharing requirements typically vary across plans. Beneficiaries receiving low-income subsidies pay reduced cost-sharing amounts. Deductible $275 Initial coverage (up to $2,400 in drug costs) 25% coinsurance Coverage gap or “doughnut hole” 100% coinsurance (no coverage) Catastrophic coverage (above $3,850 in out-of-pocket spending)
5% coinsurance
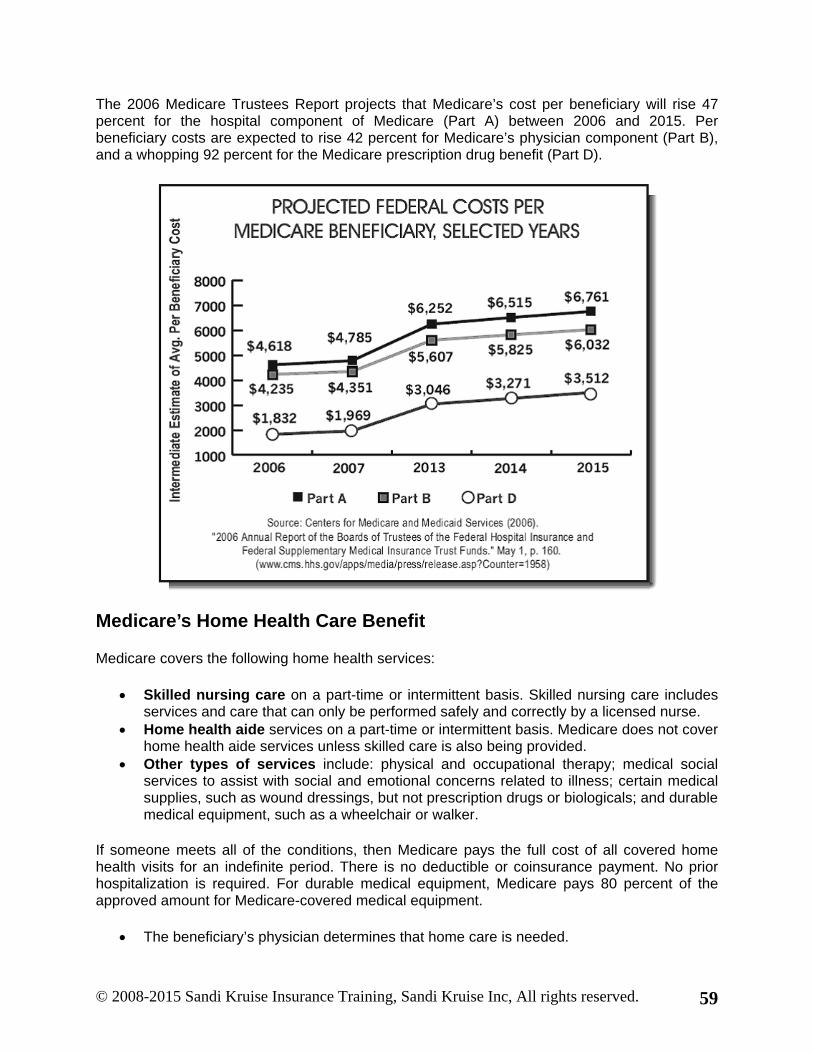
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 59
The 2006 Medicare Trustees Report projects that Medicare’s cost per beneficiary will rise 47 percent for the hospital component of Medicare (Part A) between 2006 and 2015. Per beneficiary costs are expected to rise 42 percent for Medicare’s physician component (Part B), and a whopping 92 percent for the Medicare prescription drug benefit (Part D).
Medicare’s Home Health Care Benefit
Medicare covers the following home health services:
Skilled nursing care on a part-time or intermittent basis. Skilled nursing care includes services and care that can only be performed safely and correctly by a licensed nurse.
Home health aide services on a part-time or intermittent basis. Medicare does not cover home health aide services unless skilled care is also being provided.
Other types of services include: physical and occupational therapy; medical social services to assist with social and emotional concerns related to illness; certain medical supplies, such as wound dressings, but not prescription drugs or biologicals; and durable medical equipment, such as a wheelchair or walker.
If someone meets all of the conditions, then Medicare pays the full cost of all covered home health visits for an indefinite period. There is no deductible or coinsurance payment. No prior hospitalization is required. For durable medical equipment, Medicare pays 80 percent of the approved amount for Medicare-covered medical equipment.
The beneficiary’s physician determines that home care is needed.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 60
The beneficiary requires at least one of the following medically-necessary types of care: intermittent skilled nursing care, physical therapy or speech-language therapy, or a continuing need for occupational therapy.
The beneficiary is homebound (unable to move outside the home without assistance). Home care is provided by a Medicare-certified home health care agency.
To be homebound means that leaving home takes considerable and taxing effort. A person may leave home for medical treatment or short, infrequent absences for non-medical reasons, such as a trip to the barber or to attend religious services.
Intermittent or part-time means skilled nursing and home health aide services furnished any number of days per week as long as they are furnished (combined) less than 8 hours each day and 28 or fewer hours each week (or, subject to review on a case-by-case basis as to the need for care, less than 8 hours each day and 35 or fewer hours each week).
Medicare’s Home Health benefit does not cover:
24-hour a day care at home Meals delivered to the home Homemaker services such as shopping, cleaning and laundry Non-skilled personal care services, such as bathing, eating or dressing
Medicare Supplement Insurance
Medicare supplement insurance policies (also called Medigap Insurance) are designed to cover some of the “gaps” in Medicare. These gaps refer to Medicare co-pays and deductibles. Medigap insurance enhances their hospital and doctor coverage, but does not extend to long-term care coverage. For the small portion of nursing home stays that qualify for Medicare coverage, a Medigap insurance policy may cover the daily Medicare co-payment ($124/day for days 21-100). Medigap insurance is not intended to meet long-term care needs and provides no coverage for the vast majority of long-term care expenses.
Many Medicare beneficiaries have some type of supplemental insurance coverage to help fill the gaps in Medicare’s benefit package and help with Medicare’s cost-sharing requirements. Today, employer and union-sponsored plans remain a leading source of supplemental coverage, providing retiree health benefits to about one in four Medicare beneficiaries.
Medicaid, the federal-state program that provides health and long-term care coverage to low-income Americans, is a source of supplemental coverage for more than 7 million Medicare beneficiaries. These beneficiaries are known as dual eligibles because they are dually eligible for Medicare and Medicaid.
Medicaid helps to make Medicare affordable for low-income beneficiaries, given gaps in the benefit package, premiums, deductibles and other cost-sharing requirements.
Medigap policies – also called Medicare supplements – are sold by private insurance companies and help cover Medicare’s cost-sharing requirements and fill gaps in the benefit package. Medigap policies assist beneficiaries with their co-insurance, co-payments, and

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 61
deductibles for Medicare-covered services. In 2003, a quarter of all Medicare beneficiaries had an individually purchased Medicare supplemental insurance policy.
Medicare Advantage plans are a source of supplemental coverage for people on Medicare. As of January 2007, more than 8 million Medicare beneficiaries are enrolled in Medicare Advantage plans. Most MA plan enrollees receive prescription drug coverage through their plan. Many receive additional benefits and face lower cost-sharing requirements than they would under traditional Medicare.
Another 2 million beneficiaries receive supplemental assistance (including prescription drug benefits) through the Veterans Administration and other government programs.
Case Study 1: Ella When Ella first turned 65 years old, she enrolled in Original Medicare and also purchased a supplemental plan (Plan C). She suffered a stroke and was hospitalized for two weeks. Following her hospital stay, she is discharged to a skilled nursing facility for rehabilitation for four months (120 days). The nursing home charges $150 per day or $4,500 per month.
Her nursing home stay is paid for as follows:
First 20 days: Medicare covers all costs.
Days 21 to 100: Medicare and Medicare Supplemental Plan C
Her supplemental plan pays the Medicare co-payment of $124 per day, and Medicare covers the remaining $35 per day. Days 101 to 120: Personal Income/Savings Medicare and Medicare Supplemental coverage end at day 100. Ella’s nursing home bill is $3,000 ($150 x 20) and her monthly income is $2,000, so she must pay $1,000 from her savings.
The case study illustrates how Ella’s nursing home care was paid for by several different sources, including a supplemental plan. Note that a supplemental plan does not provide any additional coverage for LTC services that is not already covered by Medicare. After 100 days in the skilled nursing facility, Medicare coverage ends. Coverage for the skilled nursing facility care co-insurance amount for days 21-100 provided by the supplemental plan also ends.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 62
Medicaid
Overview
Medicaid is a federal entitlement program that provides free or low-cost health and long-term care coverage to certain categories of low-income Americans. States design their own Medicaid programs within broad federal guidelines.
Medicaid Population
Medicaid covers 55 million low-income Americans, including children and parents in working families, children and adults with severe disabilities, and low-income Medicare beneficiaries known as “dual eligibles.” Medicaid beneficiaries largely lack access to private insurance or, in the case of dual eligibles, need services that Medicare does not provide.
Medicaid Services
Medicaid covers a broad range of health and long-term care services, but benefits vary widely by state. Medicaid is a particularly important source of comprehensive care for children, and of long-term care, mental health services, and care needed by people with disabilities. Most services are provided through private health care delivery systems.
Medicaid Cost
Medicaid spending totaled about $316 billion in 2005. Medicaid spending is sharply skewed; 4% of beneficiaries with very high costs account for nearly half of total expenditures. About 70% of Medicaid spending is attributable to the elderly and disabled, who comprise one-quarter of all enrollees.
The federal government matches state Medicaid spending at least dollar for dollar; currently, the federal government funds about 57% of all Medicaid spending. Federal matching funds are available to states on an uncapped basis. On average, states spend about 18% of their general funds on Medicaid; the Medicaid program accounts for 8% of total federal outlays.
Introduction
Since Congress established the Medicaid program in 1965, it has become a linchpin in our health care system, covering health and long-term care services for many of the sickest and poorest Americans. In 2003, 55 million people were covered by Medicaid. In the absence of the program, the vast majority of its beneficiaries would join the ranks of the nearly 47 million uninsured. Medicaid accounts for 18% of total national spending on personal healthcare. The program is the dominant source of financing for long-term care, paying over 40% of the national bill for nursing home care and for long-term care. It is also the largest source of public funding for mental health and substance abuse services. The Medicaid program is an essential source of financing for safety-net providers that serve the uninsured and many in the low-income population. Finally, Medicaid is a major engine in state economies, supporting millions of jobs.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 63
Medicaid operates as more than 50 separate programs – one in every state, the District of Columbia, and the U.S. Territories – each with its own policies and procedures. Although each individual Medicaid program has distinctive attributes, they all have in common fundamental elements that are defined in federal law.
Read more about Medicaid at http://www.cms.gov/medicaid/ .
Medicaid is the primary public financing source for LTC. Each state has its own rules and regulations, but federal law requires each state to have a minimum benefits package. Medicaid provides substantial coverage for LTC services. Medicaid-financed services reached an estimated 60 million people in 2006.a
a Congressional Budget Office (2006). “Medicaid Spending Growth and Options for Controlling Costs.”
In 2004, Medicaid spent $288 billion b in combined federal and state funds, and estimated total spending in 2006 is $320 billion. c
b Kaiser Commission on Medicaid and the Uninsured (2006). “The Medicaid Program at a Glance.” May. c Borger,Christine et al. (2006). “Health Spending Projections through 2015: Changes on the Horizon.” Health Affairs, 25; w61-w73.
Medicaid is the largest insurer of people requiring nursing home care. h
h O’Brien, Ellen (2005). “Medicaid coverage of nursing home costs: Asset shelter for the wealthy or essential safety net?” Georgetown University Long-Term Care Financing Project, May, p. 1.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 64
Medicaid spends an estimated $320 billion a year in combined federal and state funds, 8 and accounts for about 17 percent of all U.S. health expenditures. 9
8 Borger,Christine et al. (2006). “Health Spending Projections through 2015: Changes on the Horizon.” Health Affairs, 25; w61-w73. 9 Kaiser Commission on Medicaid and the Uninsured (2006). “The Medicaid Program at a Glance.” May.
During the next 10 years, the Congressional Budget Office (CBO) projects that federal Medicaid spending (excluding the state share) is on track to double, from an estimated $190 billion in FY 2006 to $363 billion by 2015.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 65
Persons Covered by Medicaid
Medicaid covers more than 40% of non-elderly Americans living in poverty and about a quarter of the near-poor. Medicaid is a safety-net health coverage program for low-income individuals and families who often lack access to job-based health insurance, cannot afford the high and rising premiums for private coverage, or are excluded from private insurance based on their health status.
Medicaid covers more than 7 million of Medicare’s almost 44 million enrollees. About 1 in 6 Medicare beneficiaries, based on their low income, are also covered by Medicaid. Compared with other Medicare enrollees, these “dual eligibles” are much poorer and in worse health. Medicaid provides financial protection for dual eligibles by covering Medicare’s premiums and cost-sharing. Medicaid also covers important services that Medicare limits or does not cover, especially long-term care, improving access to needed care for these low-income and high-need seniors and people with disabilities. Medicaid finances close to 40% of the total expenditures associated with dual eligibles.
To qualify for Medicaid, individuals must meet income and asset requirements and also fall into one of the categories of eligible populations. In order to receive federal matching funds, state Medicaid programs must cover certain “mandatory” populations, including pregnant women and children under age 6 with family income below 133% of poverty (the poverty level was $21,200 for a family of four in 2008), school-age children (age 6-18) with family income below 100% of poverty, parents with income below states’ July 1996 welfare eligibility levels (often below 50% of poverty), and most elderly and persons with disabilities receiving Supplemental Security Income (SSI), for which the income eligibility standard is 74% of the poverty level.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 66
States have broad flexibility to expand Medicaid eligibility beyond federal minimum standards to cover additional “optional” groups. Optional eligibility groups include pregnant women, children, and parents with income exceeding the mandatory thresholds; persons with disabilities and the elderly up to 100% of poverty; persons residing in nursing facilities with income below 300% of the SSI standard and “medically needy” individuals who have high health expenses relative to their income. Medicaid eligibility varies widely from state to state.
2008 HHS Poverty Guidelines
Persons in Family or Household
48 Contiguous States and D.C. Alaska Hawaii
1 $10,400 $13,000 $11,960
2 14,000 17,500 16,100
3 17,600 22,000 20,240
4 21,200 26,500 24,380
5 24,800 31,000 28,520
6 28,400 35,500 32,660
7 32,000 40,000 36,800
8 35,600 44,500 40,940
For each additional person, add
3,600 4,500 4,140
Source: Federal Register, Vol. 73, No. 15, January 23, 2008, pp. 3971–3972
Medicaid Services
State Medicaid programs must cover certain “mandatory services” enumerated in federal law in order to receive federal matching funds. Most Medicaid beneficiaries are entitled to receive the following services if they are determined to be medically necessary by the state Medicaid program or a managed care organization with which the state contracts:
Physician services Hospital services (inpatient and outpatient) Laboratory and x-ray services Early and periodic screening, diagnostic, and treatment (EPSDT) services for individuals
under 21 Medical and surgical dental services Rural and federally-qualified health center services Family planning Pediatric and family nurse practitioner services Nurse midwife services Nursing facility services for individuals 21 and older Home health care for persons eligible for nursing facility services

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 67
States can choose to cover certain additional services and are entitled to receive federal matching funds for these “optional” services. Commonly offered optional services include:
Prescription drugs Clinic services Dental and vision services and supplies Prosthetic devices Physical therapy and rehab services TB-related services Primary care case management Nursing facility services for individuals under 21 Intermediate care facilities for individuals with mental retardation (ICF/MR) services Home-and community-based care services Respiratory care services for ventilator-dependent individuals Personal care services Hospice services
Many of the benefits offered at state option are particularly important for persons with disabilities and the elderly.
The scope of Medicaid benefits varies considerably across the states. States have substantial discretion in designing their Medicaid benefit packages. While federal law requires that Medicaid benefits are covered subject to medical necessity, the definition and application of those standards varies from state to state. States also define the amount, duration, and scope of coverage for each benefit. For example, states can limit the number of physician visits or prescription drugs they will cover.
Until recently, federal law required that states offer the same Medicaid benefits to all enrollees statewide. Under provision enacted in the Deficit Reduction Act of 2005 (DRA) States now have authority to replace their Medicaid benefits (including mandatory services) with a “benchmark” package for most children and certain other groups. Benchmark packages include the standard Blue Cross Blue Shield Plan offered to federal employees, the benefits offered to state employees, the coverage offered by the largest commercial HMO in the state, and any coverage approved by HHS Secretary. Most groups, including people with long-term care needs, cannot be required to enroll in benchmark coverage, but states can provide for voluntary enrollment. States cannot offer benchmark coverage to any “expansion” groups to whom eligibility was extended after the DRA was enacted.
Medicaid is the nation’s major source of coverage and financing for long-term services and supports. Nearly 10 million Americans, primarily the elderly and people with severe disabilities, need long-term care. However, neither Medicare not private insurance covers substantial long-term care benefits; Medicaid is generally the sole source of assistance for these high-cost services. In 2004, Medicaid financed more than 40% of the estimated $158 billion spent nationally on long-term care. In recent years, both state initiatives and federal legislation have emphasized increasing the availability and use of home and community-based alternatives to institutional long-term care.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 68
States can charge premiums and cost-sharing in Medicaid, subject to federal limitations. Historically, federal Medicaid law sharply limited the use of premiums and cost-sharing in the program, but the DRA expanded states’ discretion in this regard. States are prohibited from charging premiums to Medicaid beneficiaries in specified groups and certain services are also exempt, regardless of a beneficiary’s income (e.g. care provided to institutionalized individuals and those in hospice). For others below poverty, cost-sharing remains limited to nominal levels, but the DRA permits higher cost-sharing for those above poverty (including children). Cost-sharing and premiums combined cannot exceed 5% of family income for any family.
Medicaid Long-Term Care Services
Medicaid is the largest public payer for long-term care, and finances services for the majority of nursing home residents.16 The most recent expenditure data available, from 2004, show that the program paid $37 billion of the $92.4 billion tab for institutional care of the elderly. Medicaid also spent $11 billion for home and community-based care for the elderly.17
16 Kaiser Commission on Medicaid and the Uninsured (2006). “Private Long-Term Care Insurance: A Viable Option for Low and Middle-Income Seniors?” February, p. 2. 17 Holtz-Eakin, Douglas (2005). “The Cost and Financing of Long-Term Care Services.” Statement for the Subcommittee on Health, Committee on Energy and Commerce, U.S. House of Representatives. Congressional Budget Office, April 27, p.
Medicaid pays for long-term care services in both institutional settings and in the home. It begins paying for these services when Medicaid's general requirements, functional eligibility requirements, and financial eligibility requirements have been met and approved.
Medicaid pays for nursing facility services for all eligible people over age 21 as well as home health care for people who would need to be in a nursing home if they did not receive the home care services. Under the DRA, states may now cover home care without the requirement that a person must first meet the SNF eligibility requirement.
Most of the money that Medicaid spends on long-term care goes to institutional care. However, increasingly states are offering in-home alternatives. These alternative programs pay for things such as homemaker services, personal care, or case management. They do not pay for room and board.
A person, who receives Medicaid, may choose their doctor, home health aide service, or nursing home based on location, ethnic or religious orientation, reputation, or any other parameter. However, not every nursing home or health care provider accepts Medicaid patients. Some facilities choose only to provide care to private paying patients. Others may not participate in the Medicaid program, because they do not comply with Medicaid standards. In some states there is a shortage of Medicaid beds, so they might have to go on a waiting list or be admitted to a nursing facility that is not their first choice or is located far from their family and friends.
Medicaid Eligibility Requirements for Long-Term Care
To qualify for Medicaid, people need to meet three categories of requirements:

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 69
General Medicaid Eligibility Requirements Functional Requirements Financial Requirements
Medicaid's General Eligibility Requirements
Medicaid recipients must:
Be age 65 or older or permanently disabled or blind; and Meet U.S. citizenship or immigration rules; and Be a resident of the state where they apply.
Medicaid's Age and Disability Rules
Someone age 65 or older does not have to meet any other medical requirements if they meet functional eligibility criteria. They need to provide proof of age by giving the state documentary evidence that shows their date of birth.
Someone under age 65 may qualify for Medicaid long-term care coverage if they meet Medicaid's disability requirements or are blind. Medicaid's definition of disability includes a physical or mental condition that prevents them from doing enough work or the type of work that is necessary for their support. The qualifying condition must be expected to last for at least a year or to result in death. They must meet both Medicaid's disability requirements and functional eligibility requirements since the rules for the two differ.
Those who are eligible for disability benefits under the Social Security or Supplemental Security Income (SSI) programs, automatically meet these requirements. If they are not eligible for one of these benefits, the state's disability review team decides if they meet its disability rules. People must complete an application that asks about their medical, educational, and work history. The state also looks at medical records and may ask them to see their own physicians or have medical tests performed. They may need more time than usual to process the Medicaid application.
State Residency Requirements
Usually for Medicaid eligibility purposes, people are a resident of the state where they live and intend to remain. There is no length-of-time requirement for residency and they cannot be denied Medicaid solely because they didn't establish residence in the community before they entered an institution. In addition, people cannot lose eligibility for Medicaid solely because they are temporarily absent from the state.
There are specific requirements where states must pay for services even though the individual is absent from his or her state of residency. For example, if an agency of one state places them in an institution in another state, they remain a resident of the state that made the placement, not the state where they are institutionalized.
When a competent individual leaves a facility in which he or she was placed by a state, the person's state of residence is the state where he or she is located with the intent to remain permanently or for an indefinite period.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 70
Citizenship and Immigration Status
To be eligible for Medicaid long-term care coverage, a person must be either:
A United States citizen or national; or An alien who was admitted to the United States legally and has the required entry
documents. In some cases, even if someone meets these requirements, they are not eligible for Medicaid for five years after entering the United States.
Undocumented immigrants are not eligible for Medicaid long-term care services.
Those who meet Medicaid's General Eligibility Requirements, must also meet Medicaid's Functional Eligibility Requirements, and Financial Eligibility Requirements.
Medicaid's Functional Eligibility Requirements
To receive long-term care services under Medicaid, an individual must be assessed and determined to be in need of long-term care. A medical specialist in the state evaluates their care needs. This evaluation is done in conjunction with their Medicaid application but not by the same person who evaluates their financial eligibility.
As part of this assessment, the specialist determines if they need nursing home care or if they are a candidate for home and community-based services.
The need for long-term care is generally determined by whether they can perform the Activities of Daily Living on their own, or whether they need assistance from another person. These activities include bathing, dressing, using the toilet, transferring (to or from bed or chair), caring for incontinence, and eating. They meet Medicaid's Functional Eligibility Criteria, they cannot receive long-term care services under Medicaid regardless of how poor they are.
A medical specialist evaluates applicant’s care needs to determine if they meet functional eligibility criteria. Since there are few Federal parameters that are required to define functional eligibility, individual states define functional eligibility for their Medicaid programs. They typically consider the need for assistance with Activities of Daily Living such as bathing or eating, skilled care needs, or a combination of the two. Examples of skilled care are feeding tube maintenance, intravenous feeding, dressing changes, oxygen administration, frequent injections, and other services that require the supervision and care of a nurse or physician.
Functional eligibility for home and community-based services may be the same as, or less stringent than, the requirements for institutional care. In the past, states were not allowed to use less stringent requirements for home- and community-based care. However, as of January, 2007, a change in Federal law not only allows, but encourages states to elect less stringent functional eligibility criteria that will serve even people who do not require nursing home level care.
States must provide written notification of functional eligibility decisions. If authorization is denied, they must provide the reason for the denial and provide the opportunity to appeal the decision.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 71
Those who meet a state's Functional Eligibility Criteria must also meet its General Eligibility Requirements, and Financial Eligibility Requirements.
Financial Eligibility Requirements
Medicaid eligibility is complicated, and each state is different Financial eligibility criteria apply to both income and resources (assets) Medicaid spousal impoverishment rules have greatly enhanced financial protections for
community spouses Assets of married applicants are treated jointly, while income is generally treated
separately Spousal impoverishment rules were enacted in 1989 under the Medicare Catastrophic
Coverage Act.
The eligibility rules for Medicaid are complicated in many states. Each state establishes rules for eligibility, subject to broad federal guidelines.
Income and Resources
Since Medicaid is a means-tested program, people qualify for the program based on financial need. Eligibility is subject to an extensive set of requirements, including income and resource criteria. Generally, states establish a standard (the dollar amount below which an individual or family qualifies for coverage) and a method by which income and resources are counted for the purposes of applying the standard.
Generally, for married couples, both incomes are considered separately when determining eligibility. Where income is distributed jointly to both spouses, it is assumed that each spouse has an equal interest. Assets for couples, on the other hand, are treated jointly.
The income standard, for example, may be $866 per month, which is 100 percent of the federal poverty level (FPL) for an individual in 2008. The resource standard is generally $2,000 for individuals and $3,000 for couples.
States will assess both available income and available assets in determining whether someone qualify for the Medicaid program.
Assets
Some assets are considered while other assets are excluded and not counted.
Exempt assets include a certain amount of equity in a primary residence, personal belongings, one motor vehicle, property which is essential to self support, life insurance with a face value under $1,500, certain burial arrangements, and assets held in specific kinds of trusts. Unless specifically excluded, any other real or personal property that they and their spouse own is counted in the Medicaid eligibility determination.
Assets that are jointly held by the person applying for Medicaid and other persons are generally apportioned equally among all owners.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 72
Under the Deficit Reduction Act of 2005, families who have equity exceeding $500,000 in their homes can be deemed ineligible for Medicaid long-term care, unless some of the equity is converted to cash, or a spouse or dependent continues to live in the home. f
f Health Policy Alternatives (2005). “S. 1932, Deficit Reduction Act of 2005. Summary of the Conference Agreement: Medicare, Medicaid and other Health-Related Provisions.” Dec., p. 17.
Countable and Non-Countable Resources (Assets)
Medicaid eligibility rules make a distinction between “countable” and “non-countable” resources. Countable resources include assets such as cash, bank accounts, stocks and bonds, life insurance, and real and personal property (with some exceptions). Non-countable resources, or those assets not counted in determining eligibility for Medicaid, include a certain amount of equity in the home, burial plots, and personal belongings.
Asset levels vary from state to state. States have the option to raise the minimum amount.
In most states, an individual can retain only about $2,000 in countable assets. In most states, married couples can only retain about $3,000 in countable assets, if they
are still living in the same household. If one spouse lives in an institution and the other spouse is still living in the community,
Federal law allows the community spouse to keep more assets. In general, the community spouse is allowed to keep half of the married couples' combined assets, subject to both a minimum amount and a maximum amount. In 2008, the maximum is $104,400 and the minimum is $20,880, which varies by state.
If their assets exceed the amount allowed by Medicaid, the application will be denied. The state will tell them the amount of excess assets.
People have the right to appeal the state's determination if they feel it was incorrect or they can reduce assets to become eligible in the following ways:
Convert the funds to noncountable assets such burial arrangements. Pay existing debts such as insurance and taxes. Spend the money on medical needs and day-to-day maintenance needs of themselves
and their spouse.
Transfer of Assets for Medicaid Eligibility
Many people attempt to "spend down" their assets to state required levels or try to transfer their assets to family members to become eligible for Medicaid. States now have the authority to examine a Medicaid applicant's past 5 years of finances and impose penalties. (State requirements vary; contact the state Medicaid office for details.)
Under Federal law, people may not transfer assets to others (for example, children) for the purpose of qualifying for Medicaid coverage of long-term care services. Doing so may result in a significant penalty period during which they are unable to receive Medicaid payment for long-term care services, even if their assets have been totally depleted.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 73
A transfer of assets is giving away property for less than it is worth. An asset includes all income, real property, and personal property to which they and
their spouse are entitled whether or not they actually receive it. If they transfer assets, Medicaid may not pay for nursing home or other long-term care
services.
Permissible Asset Transfers
Certain asset transfers, such as a transfer to a spouse or a disabled or blind child, are not considered disqualifying transfers.
Lookback Period
Medicaid will look at all asset transfers made in the five-year period prior to their Medicaid application. This period is referred to as a “lookback period.”
Example:
Brad Davis is an 85-year-old widower with a history of heart disease. In June 2006, he gave each of his two granddaughters $10,000 after learning he would need open heart surgery. Two months later he had a stroke and had to be admitted to a nursing home. He had enough in savings left to pay for nursing home care for five months, but then needed to apply for Medicaid in February 2007. His eligibility worker determines he meets all Medicaid requirements in March 2007, but decides his gift to his grandchildren is a disqualifying transfer of assets. He had given away assets ($20,000) for less than fair market value (he received nothing in return).
The Omnibus Budget Reconciliation Act (OBRA) of 1993 and the Deficit Reduction Act of 2005 changed the law regarding transfers. Transfers are subject to the following guidelines:
Look-back period for transfers to determine eligibility for Medicaid: All transfers are subject to a 60-month look-back period. The penalty period based on transfers can be unlimited.
Penalty Period Calculation
The penalty period is calculated by dividing the uncompensated value of a transfer by the average cost per month of nursing home care.
Total uncompensated value = Number of months for which Average facility cost/month Medicaid will not pay
Example:
Four years ago, Mrs. Ivers transferred an asset worth $50,000 to one of her children. The average cost of care in her state is $5,000 per month. Her penalty period is determined by taking the asset of $50,000 and dividing by $5,000, resulting in a 10-month penalty period in which she would be ineligible for Medicaid.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 74
Penalty Period
Asset transfers are typically penalized by disqualifying the applicant from becoming eligible for payment for nursing home and other long-term care services for a specified period of time.
Transferring assets may result in disqualification, and people may not have any resources to pay for long-term care services.
Income
Some income is considered countable income, while other income may not be counted.
If someone is in a nursing home, Medicaid counts only the income of the person applying for long-term care services. Unlike the asset determination, their spouse's income is not counted. However, after the state has determined they are eligible for Medicaid, it will decide how much they have to pay toward the cost of care and how much income they can keep. If they are married, they may be allowed to provide a monthly allowance to their spouse to ensure that he or she has adequate income to live on, before they are required to contribute to the cost of their own care. Their spouse's income will be counted in determining the amount of this allowance.
If someone is receiving long-term care services in their home, the income of their spouse may or may not be counted, depending on the eligibility options their state has chosen.
Income is anything received that can be used to purchase food and shelter. Income can include regularly received payments such as Social Security, veterans' benefits, pensions, salaries, wages, or interest from savings or checking accounts. It also includes payments to which they are entitled whether or not they actually receive them. For example, if someone gets $500 a month from a trust that could pay $1000, Medicaid counts $1000 as income. If they and their spouse are jointly paid income (such as rental income), the state divides the amount evenly, allocating half to them and half to their spouse.
Eligibility in States with Income Cap
Federal law allows people in nursing homes that live in income cap states to create an income trust. These trusts are formally called "qualifying income trusts" but are more commonly referred to as Miller trusts (after a court case brought by a person with that name). These income trusts let them make monthly deposits of any income that exceed their state's income cap to the income trust. As a result, they keep their income under the applicable income cap. They are required to name the state as beneficiary of any amount remaining in the trust after they die.
Share of Cost
Even after they qualify for Medicaid coverage, people are still required to contribute to pay part of the cost of long-term care services.
Those who are in a nursing home, are required to contribute most of their income to the cost of care, except for a small personal needs allowance.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 75
Those who are living at home may be required to pay part of the cost of the home and community-based services received.
Personal Needs Allowance
Once eligible for Medicaid, beneficiaries must contribute all income above the state personal needs allowance to the cost of care. For individuals in nursing homes or other institutions, Medicaid requires that states reserve a personal needs allowance from the individual’s income. This income is used to cover various personal care items not included in the institution’s basic charge. Personal care items include clothing, personal care items (e.g., toothpaste or shampoo), social support (e.g., telephone or stationery), and occasional outings. States generally set aside $30 to $90 a month for personal care items.
Medicaid allows people to keep a small amount of money for monthly personal needs, such as haircuts, in a nursing home. This amount must be at least $30 ($60 for a couple), but states can allow larger amounts.
If they are receiving home- and community-based services, the state must take into account their food and shelter costs in addition to any personal needs when it sets this amount. The allowed amount varies from state to state but is usually a percentage of the Supplemental Security Income (SSI) standard ($637 as of January 2008).
Medicaid makes allowances in certain instances for medical expenses and health insurance premiums, and for home maintenance when they are expected to be able to leave a nursing home within six months.
The medical expense allowance lets them keep money for medical expenses not paid for by third parties. These include health insurance premiums such as Medicare and other necessary medical or remedial care expenses that are not paid by Medicaid.
The home maintenance allowance lets them keep money for maintenance of their home when their physician certifies they are able to return home within six months. States are not required to provide this allowance. Those states that do must decide the amount that is allowed.
Spousal Impoverishment Provision
Medicaid law includes a provision to prevent spousal impoverishment, a situation that leaves the spouse in the community (called the community spouse) with little or no income or resources while the other spouse requires institutional, home, or community-based care. These guidelines were included in the Medicare Catastrophic Care Act of 1988 and were among the provisions retained when the rest of the act was repealed in 1989.
Asset Eligibility
The spousal impoverishment provision is applied when a spouse enters a skilled nursing facility or other institutional care facility and is expected to remain for at least 30 days. When the couple applies for Medicaid, an assessment of the couple’s total countable resources is made. This amount is used to determine the spousal share, which is one-half of the couple’s resources.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 76
Exempt assets are not counted and all other resources of the couple are added together. A minimum allowable retention amount and a maximum amount are established each year by the Centers for Medicare & Medicaid Services (CMS) and indexed to inflation. States can set their own protected assets amounts within the federally established minimum and maximum amounts. The community spouse can keep the minimum amount of resources or one-half the total up to a maximum limit. In 2008 the minimum is $20,880 and the maximum is $104,400.
Income Protection
Those who are married may be allowed to provide a monthly allowance to their spouse to ensure that he or she has adequate income, before they are required to contribute to the cost of their own care.
Their spouse, however, is not required to contribute any of his or her income to the cost of the ill spouse care, if they are not living in the same household. The community spouse’s income is not considered to be available for the institutionalized spouse. Any income received in the community spouse’s name belongs to him or her. If income is received in joint names, half will be assigned to each spouse.
Under the spousal impoverishment provision, income received by the institutionalized spouse can be used to provide additional income for the community spouse. Income may be made available to the community spouse up to an allowance limit that is updated each year.
In order to determine the amount of income protected for use by the community spouse, the total income of the institutionalized spouse is determined and then the following items are deducted:
A personal needs allowance A community spouse’s monthly income allowance. A family monthly allowance, if applicable. An amount for medical expenses incurred by the institutionalized spouse.
Minimum Monthly Maintenance Allowance - Spouse (MMMNA)
The income allowance for the community spouse is based on a formula in Federal law. This amount cannot be more than $2,610 per month (as of January 2008) unless they obtain a court order in a greater amount for the support of a spouse.
The allowance includes:
Standard maintenance amount; and Allowance for shelter expenses.
Shelter expenses include rent, mortgage, taxes, insurance, condominium maintenance fees, and utilities.
The total of the standard maintenance amount and shelter expenses is called the minimum monthly maintenance needs allowance and is compared to the community spouse's gross income. If the community spouse's income is less than this amount, the difference becomes the

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 77
spousal allowance. If the community spouse's income is greater than this amount, there is no allowance.
Example:
Mrs. Jones, the community spouse, receives $800 per month from Social Security. This is her sole income. Her monthly expenses for mortgage, taxes, insurance, and utilities are $1,021. The state determines her allowance as follows.
$2,610 (minimum monthly maintenance needs allowance) - 800 (Mrs. Jones' income) $1,810 (spousal income allowance)
Her husband can give her $1,810 of his income each month for her needs. If his income is less than this amount, all of his income will be available to her. Either spouse may appeal the amount of the spousal allowance if they feel it is inadequate and would result in financial hardship. The maximum amount of $2,610 is adjusted each January to reflect changes in the Consumer Price Index.
Medicaid Allowance for Other Family Members Living in Their Home
Medicaid makes an allowance for family members living in the home with their spouse. Family members include minor children as well as children, parents, or siblings they are allowed to claim as dependents for income tax purposes. This varies by state and the calculation is beyond the scope of this course. Clients should be referred to their attorneys and/or the state Medicaid office for further details.
Medicaid Waivers
States often request federal permission (called “waivers”) to deviate from some aspect of federal law. Sometimes states apply for waivers to provide services to categories of people who would not otherwise qualify under federal law; another common reason is to deliver services that could not otherwise be offered. In general, waivers are required to be “budget neutral” over the life of the waiver.29
29 Schneider, A., et al, “The Medicaid Resource Book” (2002). Published by the Kaiser Family Foundation. July, p. 82.
There are two main types of waivers, each named after the section in the Social Security statute that authorizes it: 1115 waivers, which are statewide, and 1915(c) waivers. Both are time-limited (usually for three or five years) and can be renewed.30 Home and community-based waivers under section 1915(c) have often been used to allow states to offer a more comprehensive package of services than they otherwise could to individuals needing substantial assistance to live in the community – e.g., case management and habilitation (services that teach individuals the skills necessary to live in non-institutional settings), adult day care and respite care. In 2006, 254 home and community-based services (HCBS) waivers were operating.31
30 “Medicaid Waivers.” National Association of State Medicaid Directors. 31 Kaiser Commission on Medicaid and the Uninsured, “Charting a Course for Medicaid: Future

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 78
Directions in Long-Term Care Coverage” (2006). Background briefing charts, Long-Term Care roundtable.
States have also used waiver authority to develop “Cash and Counseling” programs, which allow beneficiaries to control their own budgets for hiring a personal care assistant and to purchase supplementary services aimed at promoting independence.33
33 Alliance for Health Reform (2006). “Cash & Counseling Moves into the Mainstream.” April, p.1
Spending, Enrollment and Coverage Trends in Medicaid
The Congressional Budget Office predicts that Medicaid spending will grow by more than 8 percent a year over the next decade. But rising health care costs are also an issue of concern for private insurers, other health care programs, and the economy as a whole.
Medicaid is tied to the fiscal health of states, and the growth in state revenues has been variable in recent years. This led to some state cutbacks in eligibility and benefits during the last five years. Despite this, the post-9/11 economic downturn and other factors spurred rises in Medicaid enrollment and spending. Between FY 2004 and FY 2005 alone, state Medicaid expenses went up 12.8 percent and federal Medicaid expenses increased 4.7 percent.
Applying for Medicaid
Applying for Medicaid for long-term care services requires:
Filling out an application form; Providing documentation that verifies general and financial eligibility requirements; and Being assessed for functional eligibility;
Those who own a home will be asked to provide documentation to the state that verifies both current fair market value and any encumbrances on the home such as mortgages or equity loans. The state may ask for documents such as a current tax bill, real estate appraisal, or copies of their mortgage to satisfy these requirements.
Where there is evidence of significant asset reduction, applicants may be asked to provide evidence of how that money was disposed of. If they are married and in a nursing home, they must also provide documentation of the amount of assets they owned when they first entered the nursing home, since that will be the basis for establishing how much their spouse is able to keep.
People may apply on their own behalf or may designate someone else to apply for them, such as a family member, attorney, or a friend. If someone is applying on their behalf, that person should be familiar with their situation, able to answer all eligibility questions, and have access to financial records.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 79
When to Apply for Medicaid
Deciding when to apply depends on their medical situation, their marital status, and the complexity of their finances. If their finances are straightforward, they may not need as much time as someone with complex finances.
The Medicaid agency has 45 days to process their application (90 days where a disability determination must be made). However, timeframes may be longer if they are not able to provide all the required documentation in a timely manner.
Once they are determined to be eligible for Medicaid, the agency provides them with a written notice of the date of eligibility and the amount they must contribute to the cost of care. Once eligible, their continued eligibility is reviewed at least annually. That process is much simpler since they only need to provide documentation of current income and assets.
If they are found to be ineligible, the Medicaid agency must notify them in writing of the reason for the denial and give them the opportunity to appeal the decision.
Medicaid Estate Recovery
When a person who has been on Medicaid dies, states are required, under Federal law, to recover from that person's estate, up to the total amount spent by Medicaid on that person's behalf when he or she was alive. States must recover from the estates of permanently institutionalized people of any age as well as from the estates of individuals age 55 or older on whose behalf the state paid Medicaid benefits.
For purposes of estate recovery, estates are defined as all real and personal property and other assets included in an individual’s estate. The primary asset in estates from which states seek recovery is the Medicaid beneficiary’s home.
Recovery may only be made after the death of the individual. Recovery can also occur from the estate of living recipients who are in a nursing home and who have been certified that they cannot reasonably be expected to be discharged and return home.
Potentially Subject to Estate Recovery
States are required to recover from all probated estates, and they can recover from any property that is in the estate, including the home. States may also recover from assets that pass to heirs outside of probate, such as annuities and trusts.
State Notice about Estate Recovery
States are required to notify people when they apply for Medicaid that their estate may be subject to estate recovery. They must also notify the estate when they begin the recovery process.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 80
Estate Recovery Process
After a Medicaid recipient dies, estate recovery usually begins with a letter sent to a surviving family member and/or the estate executor informing them of the state's claim on the recipient's estate.
States must notify affected survivors and/or the executor of the estate when initiating the estate recovery claim. The notice must be person specific and, at a minimum, provide the reason for the claim, the potential amount of the claim, the process for applying for a hardship waiver, hearing and appeal rights, and the procedures for collection. States implement these requirements in a variety of ways that differ based on the aggressiveness of their estate recovery process and/or the limitations imposed by their own state laws.
Amount Recoverable from Their Estate
If they received care in a facility, the amount recovered is the amount Medicaid spent for their nursing home or other institutional care including care provided in a skilled care facility or intermediate care facility for the mentally retarded. If they were age 55 or older when they received Medicaid, the amount recovered also includes the amount Medicaid spent for home- and community-based care and any related hospital or prescription drug services.
At their option, states may also recover for payment of any other medical services it provided to them such as vision or dental care.
Example:
Bill Hanks began to receive Medicaid when he was 45 and became paralyzed in a swimming pool accident. He was able to stay at home with the help of community-based services until he was 52. He then entered a nursing home and died when he was 56. After his death, the estate recovery unit determined the recoverable costs as follows:
Age Recovered Amount
45-51 No recovery (he was under 55 and not in a nursing home).
52-54 The cost of his nursing home care but not other services such as vision care.
55-56 The cost of his nursing home care and all other services provided to him.
The total amount recovered may not exceed the amount Medicaid paid for services. Nor can the recovered amount exceed the amount remaining in the estate after the claims of other creditors, as defined by state law, have been satisfied. Such claims may include mortgages, taxes, and child support arrears among others. Some states also have provisions in their state laws that expressly prohibit Medicaid recovery from the decedent's homestead.
Family members or heirs cannot be asked to use their own funds to satisfy Medicaid claims with the exception of estates that include the homestead. Since home equity may be subject to estate recovery, survivors may have to sell the home or retain the home and use their own funds, up to the amount of the home's equity value, to satisfy the Medicaid claim.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 81
Exempt from Estate Recovery
Before initiating recovery, the state has to determine if any exemptions apply that would prohibit or defer recovery initiatives.
Certain estates are exempt. The most notable exemption is that estates that pass to a surviving spouse are exempt from recovery, as long as the spouse is alive. States, however, may recover from the spouse's estate after his or her death.
There are a few other exemptions as well, such as when estate recovery would cause undue hardship on the heirs to the estate.
Medicaid is prohibited from making recovery of any of their assets if someone is survived by their:
Spouse; or Child under the age of 21; or Child of any age who is blind or disabled.
These protections apply regardless of where their spouse or child lives. They do not have to live in the home to protect it or any other assets. These protections last until the death of the surviving spouse or child or the loss of protected status for the child (for example, a non-disabled child turns 21) at which time the state may make a claim against any assets remaining in the estate.
Example:
Hank Waters died at 72 and was survived by his wife, Evelyn. He had been in a nursing home for the last three years and received Medicaid during the entire length of his stay. At the time of his death, he and Evelyn owned a home in Massachusetts. His wife was the beneficiary of a $100,000 term life insurance policy, and Evelyn had $25,000 left in a savings account that she had been allowed to keep when Hank applied for Medicaid. When Hank died, Evelyn decided she wanted to winter in Florida. Her home, the proceeds from the life insurance and her savings are all exempt from recovery while she is alive, and she is free to spend the money as she chooses.
Adjustment or recovery can only be made after the death of their surviving spouse, if any, and only if they do not have a surviving child under age 21, or a blind or disabled child of any age. States may recover when there are adult surviving children who are not blind or disabled.
Exemptions from Estate Recovery for Partnership Policies
States are not allowed to make recovery for long-term care expenses from the estate of Medicaid recipients who resided in a state participating in the Long-Term Care Partnership Program and owned qualifying long-term care insurance. These states have added provisions to their Medicaid rules that give people financial incentives to purchase private long-term care insurance that meets the requirements of their state's program. These incentives include an increase in the amount of assets a Medicaid applicant can have and an exemption from estate recovery of those assets.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 82
Medicaid Treatment of the Home
A home up to $500,000 (or $750,000) depending on the state where the applicant, spouse, or dependent child lives is exempt when applying for Medicaid. Any contiguous property to the home is also exempt. The home loses its exempt status if the owner moves out of the home without the intent to return, and no spouse or dependent child is living in the home. The definition of “intent to return home” differs by state. The intent to return home is a subjective, not an objective intent. For example, if an applicant is in a nursing home, the applicant’s home remains exempt as long as there is “subjective intent” to return home. This intent may be expressed in a letter or affidavit signed by the person, or by written statements of relatives or friends who have personal knowledge of the applicant’s intent to return home.
The exemption of the home is one of the most misunderstood and confusing eligibility issues. While the home is exempt (or considered as a non-countable asset) for eligibility determination, the state can place a lien (a legal claim on property because of a debt) on the home to recover Medicaid-related costs.
Medicaid Lien on the Home
States may put a lien on their home if they are in a nursing home or other medical institution and are not expected to be able to return home. The purpose of the lien is to ensure that the state is notified if they try to sell or give away the property while they are still alive. A lien secures the property for recovery. It is placed on the property after the death of the person receiving Medicaid.
A lien may not be placed on their home when any of the following individuals there:
Spouse; Child under the age of 21; Child of any age who is blind or disabled; or Sibling provided he or she jointly owns the home and lived there for at least one year
before they were admitted to the medical institution.
They may transfer the ownership share in the home to any of these relatives while they are still alive without affecting Medicaid eligibility.
Sale of the Home
If someone sells a home after a lien has been put on it, they must use the equity from the home to repay Medicaid for medical assistance provided while they were institutionalized. If the amount due Medicaid is greater than the proceeds from the sale, then the reduced amount is used to satisfy the lien. The recovered amount cannot exceed the net proceeds from the sale of the home after the claims of other creditors, as defined by state law, have been satisfied. Such claims may include mortgages, taxes, and child support arrears among others.
Since states have different policies regarding liens, agents and clients should contact their state for more specific information on their state’s policy with regard to liens. Medicaid is constantly evolving. Whether Congress changes the law, or states obtain waivers to provide services

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 83
differently than would otherwise be allowed, there are always new developments in Medicaid. That’s why it is important to seek competent legal advice before transferring or selling assets.
Transfer of Assets
Applies penalties to person who transfers assets within 60 months before applying for Medicaid
Medicaid rules establish penalties for transfer of assets for less than the fair market value. Asset transfers made prior to applying for Medicaid, which are made with the sole purpose of becoming eligible for Medicaid, invoke penalty periods during which eligibility is denied.
In order to ensure that Medicaid applicants apply their assets to the cost of their care rather than give them away to gain Medicaid eligibility sooner, new rules established penalties for transfer of assets for less than the fair market value. Transfers completed within the look-back periods (how long the government looks back) will be reviewed to see if the applicant received compensation equal to fair market value. Transfers will not affect Medicaid eligibility, if legal time limits are met. However, any uncompensated value can be used in calculating a penalty period during which Medicaid will not pay for nursing facility costs.
Home and Community-Based Services (HCBS)
There have been considerable shifts in funding in most states away from institutional care settings to community-based settings since the enactment of the Home and Community Based Services (HCBS) waiver program. The HCBS waiver program has been one of the fastest growing components of the Medicaid program. All states have at least one HCBS waiver program. In December 2003, there were 274 different HCBS waiver programs in operation. HCBS waiver programs are intended to provide alternative services to persons who would otherwise be at risk of entering a nursing home. Recipients of HCBS waiver services must qualify for nursing home coverage but elect HCBS care instead.
One of the innovations of the HCBS waiver program is that states can institute new types of services to provide support to people in community-based settings. States cannot, however, cover room and board costs under an HCBS waiver. Examples of alternative services include case management, homemaker or home health aide service, personal care services, adult day health, respite care, or home modification - all of which can help pay for LTC related costs in the home.
How Much Does Medicaid Cost?
In 2005, total federal and state Medicaid spending was $316.5 billion. More than 96% of total Medicaid spending is for benefits and supplemental payments to hospitals serving a disproportionate share of low-income or uninsured patients (DSH). Medicaid provides a substantial share of health care financing in the U.S. In 2005, Medicaid accounted for:
18% of total national spending on personal health care 17% of national spending on hospital care 13% of national spending on professional services 44% of national spending on nursing home care

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 84
19% of national spending on prescription drugs
Medicaid expenditures are distributed across an array of acute and long-term care services, DSH payments, and administrative expenses. In 2004, Medicaid spending on services and DSH totaled $288.1 billion. Almost 60% was attributable to acute care, about 35% to long-term care, and 6% to DSH.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 85
Medicaid spending per enrollee varies considerably by eligibility group. In 2003, the per capita cost for children covered by Medicaid was $1,400, compared to $1,800per adult, $12,000 per disabled enrollee and $10,000 per elderly enrollee. Higher per capita expenditures for disabled and elderly beneficiaries reflect their intensive use of acute and long-term care services.
Children and their parents make up the majority of the Medicaid population, but the lion’s share of Medicaid spending goes toward services for the elderly and people with disabilities. Children, parents, and pregnant women makeup 75% of the Medicaid population but they account for only 30% of Medicaid spending on services. The elderly and disabled, who make up the remaining quarter of the Medicaid population, account for about 70% of Medicaid spending on services.
Nearly half of Medicaid spending is attributable to 4% of Medicaid beneficiaries. Medicaid enrollees, who, due to their health care needs and utilization incur very high costs, account for a large share of total Medicaid spending. In 2001, the 4% of Medicaid enrollees with costs exceeding $25,000 accounted for 48% of total Medicaid spending. Disabled beneficiaries with costs at this level alone accounted for one-quarter of Medicaid spending. This pattern holds in each major eligibility group: a small share of enrollees account for a very large share of spending.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 86
A significant share of Medicaid spending is attributable to dual eligibles, low-income seniors and people with disabilities who are enrolled in both Medicare and Medicaid. While dual eligibles make up 14% of the Medicaid population, their health and long-term care costs accounted for 40% of Medicaid spending on services in 2003. Most Medicaid spending on behalf of dual eligibles is for long-term care.
Long-term care users account for half of Medicaid spending. Only 7% of Medicaid beneficiaries use long-term care services, but these enrollees account for 52% of Medicaid spending because of their high of both acute and long-term care services.
Medicaid finances 18% of total national spending on personal health care. Medicaid pays almost one-fifth of the national bill for personal health spending, and it is a key source of financing for major categories of services. The Medicaid program is by far the largest funding source for nursing home care in the nation.
Funding for Medicaid
Medicaid is financed jointly by the federal government and the states. The federal government matches state Medicaid spending at least dollar for dollar. The federal share of Medicaid spending is determined by the Federal Medical Assistance Percentage (FMAP), which varies by state, based on state per capita income relative to the national average. The FMAP is at least 50% in every state and is higher in relatively poor states, reaching 76% in the poorest state. Consistent with the federal guarantee of Medicaid coverage for all eligible individuals, federal Medicaid matching dollars are guaranteed to states as needed, on an uncapped basis. This approach directs funding based on actual, rather than predicted, need.
The federal government funds about 57% of all Medicaid spending. The Medicaid program accounts for 8% of total federal outlays and 44% of all federal grants to state and local governments. Federal matching dollars support states’ ability to meet the health needs of the

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 87
low-income population.
States commit substantial resources to Medicaid. On average, states spend about 18% of their general funds on Medicaid, making it the second largest item in state budgets, following elementary and secondary education. Medicaid costs are a recurrent issue at the state level, as states have a limited fiscal capacity, strain during economic downturns to meet increased demands for Medicaid coverage with declining state revenues, and must balance their budgets.
Changes in Medicaid
Medicaid: Financial Eligibility Rules for Long-term Care Get Tougher
Because Medicaid is a means-tested program with strict financial limits on beneficiaries’ income and assets, an individual must exhaust nearly all of his or her own financial resources before qualifying for assistance.26.
26 O’Brien, Ellen (2005). “Long-Term Care: Understanding Medicaid’s Role for the Elderly and Disabled.” Kaiser Commission on Medicaid and the Uninsured, November, p. ii.
States have considerable discretion to set income and asset limits for long-term care eligibility. Those who have higher incomes may also qualify in some states – but only if they can show they have medical expenses that reduce their monthly income down to the state’s threshold for financial eligibility.27 More than half of states have elected to offer this option, known as the “medically needy” program.28
27 Mollica, Robert (2005). “Fact Sheet: Community Living Exchange. Medically Needy Individuals.” National Academy for State Health Policy, October. 28 AARP Public Policy Institute (2004). “Private Long-Term Care Insurance: The Medicaid Interaction.” Issue Brief #68. May, p. 3.
Limitations on the financial assets a person may keep before Medicaid will pay for services can be as low as $2,000. The value of a person’s household goods, car and burial funds are not

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 88
counted in determining assets if the person is married, and the spouse is not also in an institution. Community spouses are allowed to keep additional resources.29 Until passage of the Deficit Reduction Act (DRA), the full value of a person’s home was also exempted from Medicaid means-testing rules.
Often, individuals enter a nursing home as a private pay patient, financing the cost of the care by using assets. Once he or she has spent down to the asset limit, Medicaid begins to pay for nursing home care. During the 1990’s, some analysts began expressing concern that “Medicaid millionaires” were hiding assets and improperly giving away money and sheltering assets to make themselves eligible for Medicaid services.30 Some members of Congress agreed, and this belief – combined with the concern of many states that future long-term care costs will prove unmanageable – contributed to enactment of new financial eligibility rules as part of the DRA.31
29 Centers for Medicare and Medicaid Services. “Spousal Impoverishment.” 30 Wall Street Journal editorial, “Medicaid for Millionaires (February 24, 2005, p. A14). 31 Health Policy Alternatives (2005). “S. 1932, Deficit Reduction Act of 2005. Summary of the Conference Agreement: Medicare, Medicaid and other Health-Related Provisions.” Dec, p14.
Medicaid Home and Community-Based Care Growing
States have moved dramatically over the past decade to provide more long-term care in community settings, rather than in institutions. Between 1994 and 2004, spending on home and community-based services (HCBS) for beneficiaries of all ages rose from $8 billion to $32 billion, and from 19 percent of all Medicaid long-term care services to 36 percent.32
32 O’Brien, Ellen (2005). “Long-Term Care: Understanding Medicaid’s Role for the Elderly and Disabled.” Kaiser Commission on Medicaid and the Uninsured, November, p. ii.
HCBS waivers authorized under section 1915(c) of the Social Security Act have allowed many states to develop and offer a more comprehensive package of services than they otherwise could to individuals needing substantial assistance to live in the community. Those services include case management and habilitation (services that teach individuals the skills necessary to live in non-institutional settings), adult day care respite care and others. Enrollment in HCBS waivers has been steadily rising over time, with the most recent enrollment data, from 2002, showing nearly a million beneficiaries were receiving services under 1915(c) waivers. In 2006, 254 HCBS waivers were operating.33
33 Kaiser Commission on Medicaid and the Uninsured, “Charting a Course for Medicaid: Future Directions in Long-Term Care Coverage” (2006). Background briefing charts, Long-Term Care Roundtable.
With the enactment of the Deficit Reduction Act in 2005, states can now offer HCBS services as a state option without having to seek a waiver. The trend among states to expand home and community-based services has been gaining momentum.
A few states are now embarking on major reforms of the way Medicaid long-term care services are designed and delivered in order to give greater emphasis to non-institutional services.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 89
Self-directed care models, like the Cash and Counseling Demonstration, are growing rapidly in state LTC systems. These models put “purchasing power” in the hands of persons who actually receive the services. “Cash and Counseling” programs have allowed beneficiaries to control their own budgets for hiring a personal care assistant (in some cases a family member) and to purchase supplementary services aimed at promoting independence.55
55 Alliance for Health Reform (2006). “Cash & Counseling Moves into the Mainstream.” Apr, p. 1.
The outcomes of the initial three Medicaid demonstration programs in Arkansas, New Jersey and Florida showed that beneficiaries controlling their own budgets were significantly more satisfied with their care arrangements than beneficiaries receiving traditional agency-based home care services.56 Under the DRA, all states can now offer this option.
56 Alliance for Health Reform, “Cash & Counseling Moves Into the Mainstream” (2006).
Summary
Medicaid is an integral component of the nation’s health care system, covering almost 1 in every 5 Americans and financing almost 1 in every 5 dollars of personal health care spending. The program’s 55 million diverse beneficiaries include children and parents in low-income working families, low-income adults and children with disabilities, and low-income seniors.
Most non-elderly Medicaid beneficiaries lack access to other coverage. They work in jobs that don’t offer insurance, or they are not eligible for it, or they can’t afford private insurance premiums. Most Medicaid enrollees with disabilities also lack access to private insurance or have health and/or long-term care needs that private insurance cannot adequately meet.
Dual eligibles rely on Medicaid to pay their Medicare premiums and cost-sharing and to cover expensive gaps in Medicare benefits, especially for long-term care. Without Medicaid, the vast majority of the program’s beneficiaries would join the ranks of the 47 million uninsured or would be under-insured for services and supports that are essential to meet their needs.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 90
Older Americans Act Programs
Administered by the AoA/DHHS, 56 State Units on Aging, 655 Area Agencies on Aging, 244 Tribal Organizations and 29,000 Community Service Providers
Provides a broad range on community-based services, including home delivered and congregate meals to persons over the age of 60
Administration on Aging (AoA) programs are administered separately from state Medicaid programs—different agencies, different rules, different providers.
The Older Americans Act is a Federal program designed to organize, coordinate, and provide home and community-based services to older adults and their families to help elders remain in the community as independently as possible.
The Older Americans Act provides funding, through state and local agencies known as the Aging Network, for a range of services that include nutrition programs in the community and for homebound elderly; programs for Native American elders; services for low-income minority elders; health promotion and disease prevention activities; in-home services for frail elders; services that protect the rights of older persons such as the long-term care ombudsman program; and services and supports for family caregivers. While there are no specific financial eligibility criteria for Older Americans Act services, they are generally targeted for low-income, frail seniors over age 60, and minority elders and seniors living in rural areas.
Local agencies, called Area Agencies on Aging (AAAs), in collaboration with State Agencies on Aging, plan and develop service and support programs based on the needs of elders and families in their respective areas. More information on Older Americans Act programs can be found on the Administration on Aging website.
The Older Americans Act (OAA) created the primary vehicle for organizing, coordinating and providing community-based services and opportunities for older Americans and their families. All individuals 60 years of age and older are eligible for services under the OAA, although priority attention is given to those who are in greatest need. Many states target these resources to persons who are not poor enough to qualify for Medicaid, but who still need help.
The following provides an overview of the range of support services available to older residents in their communities through the OAA and other federal, state, and local programs.
Case Management. Case management services are aimed at providing a single access point in the community to reduce the distance an individual must go to initiate entry into the service system.
In-Home Services. In-Home Services encompass a wide range of supporting services offered to individuals who are homebound due to illness, functional limitations in activities of daily living, or disability.
Home Health. Home health care is recognized as an increasingly important alternative to hospitalization or care in a nursing home for patients who do not need 24-hour day professional supervision.
Homemaker. Homemaker service is extended to individuals who are unable to perform day-to-day household duties (e.g., light housekeeping or laundry) and have no one available to assist them.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 91
Adult Day Care. Adult day care programs offer a lower cost alternative to institutionalization for newly or chronically disabled adults who cannot stay alone during the day, but who do not need 24-hour inpatient care.
Legal Assistance. Legal services help older persons experiencing problems in civil matters to obtain advice, counseling, information or representation. Services are provided either by a licensed attorney or trained paralegal.
Housing. Housing services are aimed at providing older persons with a wide variety of assistance related to financing, building, maintaining, and locating housing.
Respite Care. The provision of short-term relief (respite) to families caring for their frail elders offers tremendous potential for maintaining dependent persons in the least restrictive environment.
Residential Repair and Renovation. These programs help older people keep their housing in good repair before problems become major.
Long-Term Care Ombudsman Program. Long term care ombudsmen, state and local, work cooperatively with nursing homes and board and care facilities to improve the quality of life for residents. They serve as patient's rights advocates, investigating and negotiating resolutions to concerns voiced by residents in matters of resident services and care. To find out more about the program, visit http://www.ltcombudsman.org or call (202) 332-2275.
Pension Counseling. Pension counseling projects are designed to reach out, educate and promote pension awareness and protection among older individuals, as well as encourage better financial planning.
Veterans Affairs - LTC Benefits
The Department of Veterans Affairs (VA) health system makes certain long term care services available to veterans based on a priority ranking system, with highest priority given to those with severe service-related disabilities.
VA-funded long term care may be worth investigating, especially for veterans with service-related disabilities and/or limited incomes and assets. Keep in mind, however, that in addition to the priority ranking system, the availability of long term care services from the VA may be subject to funding limitations and may vary by geographic area.
The Veterans Administration (VA) system may provide LTC for service-related disabilities or for certain eligible veterans and/or their spouses. Nearly 65,000 veterans received LTC in 2003 through inpatient programs of VA or state veteran’s homes.
However, there are typically waiting lists for VA nursing homes, making access to veterans’ LTC services very limited. The VA also provides a small “aid and attendance” benefit for at-home care. It could provide some limited nursing home care if the disability is service-related and if they can get access to an appropriate facility or a small amount of financial assistance for home care or adult day health. Obviously, this is not a potential resource for the majority of individuals.
For those who qualify, the benefits can provide financial assistance for some LTC costs. Co-payments may apply depending on the veteran’s income level. Middle-income veterans who need LTC for non-service-related conditions may find it difficult to access VA benefits for LTC.
In 1999, the Veterans Millennium Health Care and Benefits Act expanded VA health programs including many that may be of use to aging veterans with long- term care needs. The Act

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 92
requires that the VA provide LTC to veterans with combined disability rating of 70 percent or greater and to those who need care due to service-related disabilities.
The Act also requires the VA to provide greater access to community-based LTC programs. These programs include geriatric evaluation, adult day care, respite care and other non-institutional alternatives for nursing home care.
The VA has a Housebound and Aid and Attendance Allowance Program that provides cash grants to eligible disabled veterans and surviving spouses in lieu of formally provided homemaker, personal care and other services needed for assistance in Activities of Daily Living and other help at home.
Visit the Department of Veterans Affairs to view available programs and services or download a Veterans Benefits fact sheet. Call the VA at 1-800-827-1000 to obtain information about available services in their area.
For more information on eligibility for VA benefits, please visit www.va.gov/elig.
PACE Program
Programs of All-Inclusive Care for the Elderly (PACE) programs integrate Medicare and Medicaid in one managed care plan. It is an optional benefit under both Medicare and Medicaid that focuses entirely on older people who are frail enough to meet their state’s standards for nursing home care and are able to live in the community setting without jeopardizing their health and safety.
PACE is a former Medicare demonstration program that is now available to beneficiaries in 19 states who live at home but need nursing-home level care. PACE is jointly financed by Medicare and Medicaid, and uses capitated funding from both programs to provide comprehensive acute and long-term care. These services are often delivered in adult day care centers and at home.
Source: Centers for Medicare and Medicaid Services (2005). “Program of All Inclusive Care for the Elderly.” December
PACE includes comprehensive medical and social services that can be provided at an adult day health center, home and/or inpatient facilities. For most patients, the comprehensive service package permits them to continue living at home while receiving services, rather than be institutionalized. An interdisciplinary team (i.e., primary care physician, nurse, social worker, dietitian, PACE Center Manager, home care coordinator, personal care attendant, and driver) assesses participant needs, develop care plans, and deliver all services, which are integrated into a complete health care plan. PACE is available only in states that have chosen to offer PACE under Medicaid.
Eligibility Requirements: In general, participants must be at least 55 years old, live in the PACE service area and be certified as eligible for nursing home care by the appropriate state agency. There may be other eligibility requirements to obtain PACE benefits.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 93
Cost: Each plan has different premium requirements. All plans have co-payments for certain services.
For more information about cost and benefits, and to determine if your state offers the PACE program, view the Medicare Personal Plan Finder at http://www.Medicare.gov.
Social/Health Maintenance Organizations (S/HMOs)
A Social HMO is an organization that provides the full range of Medicare benefits offered by standard HMOs, plus additional LTC services which may include care coordination, prescription drug benefits, chronic care benefits covering short term nursing home care, a full range of home and community based services such as homemaker, personal care services, adult day care, respite care, and medical transportation.
At the time this was written, there were four S/HMOs participating in this program:
Kaiser Permanente (Portland, Oregon) SCAN (Long Beach, California) Elderplan (Brooklyn, New York) Health Plan of Nevada (Las Vegas, Nevada)
Eligibility Requirements: Beneficiaries must live in areas where S/HMO is offered. Eligibility requirements differ with each program.
Cost: Each plan has different premium requirements. All plans have co-payments for certain services. To obtain cost and benefit information, visit the Medicare Health Plan Compare tool at http://www.medicare.gov for specific details.
Before making any health plan decisions, they should contact the plan directly at the phone number listed on the website.
State Managed Long-Term Care Programs
Some Medicaid programs cover LTC services under and managed care model
Arizona Long-Term Care System (ALTCS) Minnesota Senior Health Options (MSHO) Wisconsin Family Care Texas Star+Plus
Managed care models hope to create efficiencies and improve quality by integrating services in a bundled capitation rate. Managed LTC organizations also have financial incentives to deliver care more efficiently.
At the time this was written, four State Managed Long-Term Care Programs provided assistance for the elderly or disabled who need LTC services. The benefits, eligibility and costs of each program vary. Below are short descriptions of each of the programs.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 94
Arizona Long Term Care System (ALTCS)
ALTCS is Arizona’s LTC program for those who are elderly or disabled and need nursing home level care. ALTCS helps pay for nursing home care or special care that allows participants to remain in their own home. Long-term care services include:
Nursing home care Attendant care Home health nursing or respite care in participant’s home or other community setting Hospice care
Eligibility Requirements: To be eligible for ALTCS a person must:
Be physically disabled, developmentally disabled, blind or 65 years of age or older, and have a medical need for nursing level care.
Be a U.S. citizen or a qualified immigrant as determined by the Immigration and Naturalization Service (INS).
Be a resident of Arizona. Have a Social Security Number or apply for one. Live in their own home or in an approved facility. Meet income and resource limits.
Enrollment Process: The first step is to fill out a Part I Application and a Part I Supplement, which can be obtained by calling an ALTCS office. A list of phone numbers can be obtained on the ALTCS website at the following address: http://www.ahcccs.state.az.us/Contacts/altcs.asp
Part I of the application requires an individual’s name, address, age, and types of benefits the individual is receiving, such as Medicare or Supplemental Security Income (SSI) from Social Security. It must be signed and mailed, or taken to the nearest ALTCS office.
Individuals may give someone else permission to apply for him/her, including relatives and friends. If a legal representative, such as a public fiduciary or legal guardian has been named to act on the individual’s behalf, he or she must apply for ALTCS for the individual.
Part II of the application will ask the individual several questions to determine financial eligibility. Some questions may include:
Do you live in Arizona? How old are you? Are you married? Are you disabled? Are you a U.S. citizen or a lawfully admitted immigrant? If not, what is your non-citizen
status? How much money do you earn or receive each month? Do you own a home or other real property? How much money do you have in the bank or in other investments? Do you have a trust? Have you transferred assets in the past three years?

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 95
Do you have health insurance?
Cost: Premiums vary depending on the financial situation of the individual. In many cases, there will be no cost to the beneficiary.
Minnesota Senior Health Options (MSHO)
MSHO is a health care program for seniors, age 65 and over, who are eligible for Medical Assistance (MA) and Medicare. People with only MA can also join. Long-term care services that are offered include, but are not limited to:
Durable medical equipment Prescription drugs Personal care attendant services Home health services Home- and community-based services (Elderly Waiver) Nursing home care Transportation Interpreter services
Eligibility Requirements: To be eligible for MSHO, they must:
Be a Minnesota resident. Be eligible for MA and enrolled in both Medicare Parts A and B or eligible for only MA. Be 65 years or older. Live in one of the following counties: Anoka, Carver, Dakota, Hennepin, Mille Lacs,
Ramsey, Scott, Sherburne, Washington, and Wright.
Enrollment Process: Contact one of the MSHO health plans listed below:
Medicare (952) 992-2345 or 1-800-906-5432 (toll free) or 1-800-234-8819 (TTY) Metropolitan Health Plan (612) 347-3300 or 1-800-647-0550 (toll free) or 1-800-627-
3529 (TTY) Care Minnesota (612) 676-3554 or 1-800-203-7225 (toll free) or 1-800-688-2534 (TTY)
Cost: This program is at no additional cost to the beneficiary. If the individual has medical assistance spend down, waiver obligation or a deductible for the Prescription Drug Program, the individual will receive a letter from the Minnesota Department of Human Services directing the individual how much to pay.
Wisconsin Family Care
Family Care is a comprehensive LTC program designed to help frail elderly manage and pay for their long-term needs. It is being piloted in nine counties. Family Care has two major organizational components:
Aging and disability resource centers designed to be single entry points where older people and people with disabilities and their families can get information and advice about a wide range of

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 96
resources available to them in their local communities. These resources include benefits counseling, information about community resources and emergency response.
It is now offered in the following counties: Fond du Lac, La Crosse, Milwaukee (serving the elderly population only), Portage, Richland, Kenosha, Marathon, Trempealeau, and Jackson.
Care management organizations (CMOs) provide medical and LTC assistance to eligible beneficiaries.
CMOs now offer packages in five counties: Fond du Lac, La Crosse and Portage counties, Milwaukee (serving the elderly population only), and Richland.
Eligibility Requirements: To be eligible for Family Care, they must:
Have LTC service needs, Be an older adult or an adult with a disability, Live in a Family Care pilot county, Meet financial eligibility requirements. Medicaid-eligible individuals automatically meet
the financial eligibility criteria for Family Care.
Individuals who are not financially eligible for Medicaid may still qualify for Family Care based on their cost of care. Individuals receiving the Family Care benefit may be required to pay a cost share to the CMO.
Enrollment Process: Contact the resource center. For a list of phone numbers, go to http://www.dhfs.state.wi.us/LTCare/Generalinfo/Where.htm#RC.
An enrollment specialist will assess whether or not the applicant meets the eligibility requirement. If the person is eligible and decides on Family Care, the enrollment specialist finishes the enrollment process and notifies the CMO of the enrollment date
Texas STAR+PLUS
STAR+PLUS is a Texas Medicaid pilot project designed to integrate delivery of acute and LTC services through a managed care system. Currently, it is only available in Harris County (Houston). Long-term care services provided by the HMOs may include:
Adaptive aids, Adult foster home services, Assisted living, Emergency response services, Medical supplies, Minor home modifications, Nursing services, Respite care and therapy (occupational, physical and speech-language).
Care coordination is an integral STAR+PLUS service. The Care Coordinator is responsible for coordinating the individual’s acute and long term care, even if the individual is a dual eligible who receives Medicare from a provider that is not affiliated with the STAR+PLUS HMO's Medicare risk product.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 97
Eligibility Requirements: To be eligible for this program, they must:
Be a Texas resident living in Harris County. Be an older adult or someone with a physical or mental disability Be qualified for SSI benefits or for Medicaid.
Enrollment Process: Medicaid recipients who are eligible for STAR+PLUS receive an enrollment packet through the mail. This packet contains information about STAR+PLUS, instructions for completing the enrollment form and information about the managed care organizations they can choose. Individuals can return their enrollment form via mail, complete an enrollment form at an enrollment event or presentation, or call the enrollment broker and enroll via phone.
Individuals have 30 days after receiving an enrollment packet to make a selection before being assigned a health plan and provider. Any individuals who do not make their own enrollment choices are assigned a health plan and primary care provider (except for Medicare beneficiaries, who are assigned only a health plan.) The process of assigning individuals is called the "default" process. Individuals who are defaulted may still make a choice about their health plan and PCP, although these individuals must receive their Medicaid services through the assigned plan and provider until they contact the enrollment broker and make a selection. Individuals may change plans each month.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 98
Chapter Four – Overview of Long-term Care Insurance
This chapter provides an overview of long-term care (LTC) insurance. The purpose is to inform agents on the benefits of insurance and who should consider buying coverage. It provides background information on available LTC products and the insurance companies offering them. First this chapter reviews the very important fact that a long-term care insurance policy is a contract and that agents must understand and be able to explain to their clients how the terms and conditions in the contract will affect what is and is not covered in the policy, how claims will be handled, and how their choices will be limited or expanded.
At the conclusion of this chapter, agents will be able to:
Explain the benefits and potential drawbacks of having LTC insurance coverage; Help consumers determine if it is appropriate for them to consider buying coverage; Explain why people buy LTC insurance and concerns they may have about making the
purchase; and Describe the current state of the LTC insurance market, the types of coverage most
people buy today, and the size and nature of the market.
Long Term Care Insurance
Long term care insurance is a reliable method of paying for long term care expenses. Long term care insurance is an insurance product which pays for long term care services in many settings, such as at home, a nursing home, assisted living facility, and adult day care facility.
Many people elect to buy long term care insurance so they will not need to deplete their savings should they need long term care services. Long term care insurance can help ensure that financial resources and support are in place when they need them.
How Long Term Care Insurance Works
First, the person must apply for coverage. Those who are approved for coverage, pay their premiums, and meet the insurance carrier’s criteria for benefit payment, will be reimbursed for covered long term care services up to the amount of daily benefit after they satisfy the Waiting Period.
People generally buy LTC insurance while they are still relatively healthy and independent, prior to their actual need for care. If care is needed, the policy pays all or part of the cost of certain types of care for a specified period of time, or up to a pre-set dollar amount. Some policies offer “unlimited” coverage.
Where Does Long Term Care Insurance Cover Care
While some plans only pay for care in a nursing home or assisted living facility, other plans also cover long term care received in their own home or other settings. Most people receive long term care in settings outside of a nursing home. If they want to remain in their own home or have family members or friends who will be able to assist them in a caregiving role, they should consider an Option that can provide benefits for care in the home and other settings outside of a
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 99
nursing home. If lower premiums are more important to them than receiving care at home, consider a Facilities-Only Option.
Typically, LTC insurance pays for care in a wide variety of settings including facility care, home care, and community-based care, although some people purchase more limited coverage that focuses only on one type of care setting.
What Is an Insurance Contract?
In sales, in underwriting, in claims, and in most other areas of health insurance, the insurance contract is a fundamental element that affects the actions taken and the decisions made. Therefore, to understand how insurance works, it is essential to understand exactly what a legal contract is and specifically what an insurance contract is.
A contract is a voluntary, written, legally binding agreement between two parties (persons or other entities such as businesses or government agencies). An insurance contract is an agreement between an insurer and a policyholder by which the insurer agrees to compensate the policyholder for a loss in return for the premiums paid to the insurer. The provisions of a policy spell out all the terms and conditions of the arrangement and the rights and obligations of the parties.
The Basic Elements of a Contract
All contracts must have these four elements to be legally binding:
Consideration, Meeting of the minds, Capacity to contract, and Offer and acceptance.
Consideration
The term consideration refers to what each party to a contract does or gives in exchange for what the other party does or gives. In the case of an insurance contract, the consideration made by the prospective policyholder (the applicant) is the submission of the application for insurance and the payment of the premium. The consideration made by the insurer is its promise to pay the benefits described in the policy. For a contract to be valid, consideration must be made by each party to the other.
Meeting of the Minds
The parties to a contract must reach a meeting of the minds—that is, both parties must have the same understanding of the agreement and of their respective obligations and rights under the contract.
Meeting of the minds requires that both parties have good faith. Good faith means that neither of the parties has the intention of deceiving or taking unfair advantage of the other party. Without good faith, the parties do not truly have the same understanding of the agreement and

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 100
so a meeting of the minds has not been reached. If it can be shown that either party was not acting in good faith, the contract can be declared invalid and rescinded (cancelled).
Sometimes there is no meeting of the minds because important information is missing or incorrect. Through no fault of his own one of the parties does not have an accurate understanding of the terms of the agreement. For example, if the medical history submitted by the policyholder is inaccurate, the insurer will not have a clear understanding of the risk. Or if the explanation of benefits is not clear and accurate, the policyholder will not have a clear understanding of what she may expect in the event of a loss. Although such cases can result from bad faith and the intent to defraud, they may also result from an honest mistake. In either case, a party may seek a modification or a rescission of the contract.
Capacity to Contract
To form a valid contract, both parties must have the ability to understand its terms. Without this capacity there can be no meeting of the minds. Persons are assumed to have this capacity unless they are minors or determined by a court to be mentally incompetent or if they were under the influence of drugs or alcohol at the time they entered into the contract.
Offer and Acceptance
Offer and acceptance means simply that one party makes an offer and the other party accepts it as made. For example, a prospective policyholder may make an offer to buy insurance by submitting an application for a certain policy and paying the premium. The insurer may accept this offer by approving the application, accepting payment, and issuing the requested policy.
Alternatively, the insurer may reject the applicant’s offer and end negotiations. Or the insurer may reject the offer by making a counteroffer, so that negotiations continue. For example, the insurer may reject the application by a certain person for a standard policy but propose instead a modified policy (for example, with a higher premium rate or with a special exclusion). The applicant may then accept or reject the counteroffer. Whenever an offer or counteroffer is made, the second component—acceptance by the other party—must occur for the creation of a binding contract. Generally a time limit applies for acceptance.
The Contract, the Policy, and the Application
The words insurance contract and insurance policy are often used interchangeably in the insurance industry. However, there is a distinction. An insurance contract normally consists of both the policy written by the insurer and the application for insurance submitted by the policyholder.
The policy contains information about the terms of the coverage that the insurer will provide. These terms, expressed in the provisions of the policy, are also the provisions of the contract.
The application contains information about the prospective policyholder, which they furnish to the insurer for underwriting purposes. Underwriting is the process whereby an insurer evaluates the circumstances of the applicant, decides whether or not to provide coverage to the applicant, and determines the terms of any coverage that it will provide.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 101
If representations made by the applicant are false, that is, if the information supplied in the application is inaccurate or incomplete, the insurer may rescind the contract. However, if an answer on the application is clearly ambiguous or incomplete, it is the insurer’s responsibility to obtain clarification at the time of underwriting and before it issues the policy.
If the insurer does not obtain clarification before issuing the contract in such a case, it may not have the right to rescind the policy later, even if it learns that the ambiguous answer contained false information.
LTC insurance
LTC Insurance must be bought in advance of LTC need Pays some or all LTC expenses Covers variety of care settings Policies differ in terms of covered services, provisions and coverage amounts Newer products greatly improved over earlier ones
Private Long-term care policies help pay for the cost of both nursing home and home care. The growth of this market has been relatively slow. In 2004, according to CBO, private insurance accounted for about four percent of long-term care spending on the elderly.25
25 Holtz-Eakin, Douglas (2005). “The Cost and Financing of Long-Term Care Services.” Statement for the Subcommittee on Health, Committee on Energy and Commerce, U.S. House of Representatives. Congressional Budget Office, April 27, p. 5-6.
Long-term care insurance is there to pay for the catastrophic expenses associated with an unanticipated need, in case it should occur. It provides peace of mind and financial protection. It is a product that is designed to be maintained for the long-term, unlike other insurance, which is often priced and renewed on a year-to-year basis. Coverage does not have to “build-up” in order to access benefits, as might occur with other cash accumulation products.
There are many different types of LTC insurance policies. When comparing policies, there are differences in terms of how much coverage is provided, the circumstances under which benefits will be paid, and the specific services that are covered. However, since the passage of the Health Insurance Portability and Accountability Act (HIPAA) in 1996, there is more standardization across policies in terms of the criteria for receiving benefits and important consumer protection provisions.
In general, most policies:
Pay a set amount per day for covered care. This is called the Daily Benefit Amount. Individuals can choose their preferred Daily Benefit Amount, based upon their personal situation and the cost of care where it is expected to be received. (Some policies offer a weekly or monthly amount instead of a daily limit.)
Pay benefits for a specified time period, or up to a total dollar amount. This is called the Total Coverage Amount (also referred to as the Lifetime Maximum). Individuals may choose their preferred Total Coverage Amount. Choices can range from as little as one year of benefit to unlimited coverage.
Require individuals to complete an Elimination Period (Deductible Period), during

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 102
which they are eligible for and receive services before beginning to make benefit payments. Most policies allow individuals to select their Elimination Period (e.g., 0, 20, 30, 60, 90 or 100 days).
Benefits of LTC Insurance
It is important to remember that LTC insurance has both financial and “emotional” benefits.
Financial benefits are important and include preserving income and assets. Emotional benefits (e.g., peace of mind, control over care choices, independence, and
staying at home for care) are often more critical to people than the financial benefits.
For most people, the decision of whether or not to buy LTC insurance is not only about whether it makes good financial sense. Having LTC insurance provides financial protection, choice, control, and peace of mind.
LTC insurance can:
Help pay some or all of the cost of an individual’s LTC needs; Help protect all or a portion of accumulated assets; Provide financial security for spouses, should one spouse require costly LTC; Enable one to pass on their home or estate to an heir; Provide peace of mind; Reduce or eliminate the reliance on Medicaid; Provide control over LTC choices and care options, including expanding alternatives to
nursing home care (e.g., assisted living facility care, home health care, or adult day care);
Provide an alternative to relying on family or friends to provide needed care; and Provide a way to “pre-pay” for future LTC needs which costs less since risks and costs
are pooled with many other insured persons. This means that an individual pays much less over time than if paying for care without insurance. This can help protect income, in order to live comfortably in later years, rather than draining that income to pay for care needs.
Potential Drawbacks
There are some potential drawbacks to LTC insurance that should be considered. First, some people might not qualify for coverage, based on their current health status. While, on average, more than 80 percent of all applicants are approved for coverage, someone who currently needs LTC or has a serious, chronic degenerative condition such as Parkinson’s disease will not qualify. Others have competing needs for their financial resources and delay the decision, feeling that it is not the “right time” to buy coverage, if there are other priorities for their financial resources. In addition, the premiums may not be affordable. Finally, some people worry about whether the policy will pay benefits as promised and whether they have chosen the right type and amount of coverage for their needs.
It is also important to remember that, while insurance pays for many LTC costs, individuals might have costs that exceed the amount of insurance coverage purchased, or that they might

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 103
incur expenses that are not covered. So, it is important to plan ahead for these expenses as well.
With and Without a Policy
WITH A POLICY WITHOUT A POLICY
They have a professional to plan for their care at home, which provides services related to their particular sickness, illness.
A family member must make a decision about who will be caring for them, who will be paying and where.
Their family can be part of the care plan, but they will not have to be the planners.
Their family must find the caregivers that they need in order to stay at home.
They will have the money to pay for long term care without having to deplete the family savings.
They could be forced to take up to $40,000 a year (or more) for the family nest egg).
Their loved ones can carry on a more normal life.
The family members involved with their care will be responsible for their needs. They may come to resent them.
Their family will attend to their needs out of love instead of out of obligation.
The family will have no other choice but to deal with their problem at their expense.
Will be able to choose which facility or stay at home, whichever is more appropriate.
Family may have to make choices based on ability to pay.
May be able to stay home longer. May enter a nursing home earlier than they want to.
May be able to leave some of what they have worked so hard for to their family.
May have to use up a large portion of assets to pay for the care needed
Will be able to stay with their children without depending on them for all of their care.
Because children have busy lives, they may not be able to keep parents in their own home and provide for them.
Can feel good knowing that all of the money they have worked so hard for will not be used up in a few short years.
A primary reason for financial failure among seniors today is the cost of long-term care
Less friction between family members. One person won’t have the sole responsibility of care giving.
Family members often resent one or the other for not doing their part when a parent needs help.
To Buy or Not to Buy?
Who should consider LTC Insurance?
There is no easy rule-of-thumb to guide consumers in deciding whether LTC insurance is right for them. While some “facts” are important – such as level of income and accumulated assets, age, and health – many intangibles are also important to the decision. These include how

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 104
consumers feel about relying on family or friends for care, how important it is to them to be able to receive care at home, how they feel about leaving an estate, and many other issues.
LTC insurance is not right for everyone. Individuals who already need LTC will probably not qualify for insurance. In addition, LTC insurance may not be appropriate for individuals who have little income, few assets, or already qualify for Medicaid. Generally, individuals should consider buying LTC insurance if they:
Have Assets to Protect
While there is no “hard and fast” number, some financial experts recommend considering insurance if one has $50,000 or more in non-housing assets. Even people who have significant wealth often choose to buy insurance rather than “self-insuring” so they can protect more of their assets.
Are not Eligible for Medicaid
Those who are eligible or close to qualifying for Medicaid are not suitable LTC prospects.
Can afford the Premiums
Those who can afford the premiums for the type and amount of coverage they believe best suits their needs. Again, there is no single threshold, since affordability depends on how important the protection and peace of mind is to the individual. Some financial experts recommend that the premium cost should not exceed 7 percent of income. Individuals should take into account whether their current income is expected to increase, decrease, or remain constant over time. Finally, it is also important for individuals to consider if they can afford the premium today and in the future.
Agents should emphasize that “affordability” means different things to different people. While the “7% of income” measure is often mentioned, in reality some people are willing to spend varying amounts on LTC insurance, based on how important the purchase is to them. Those with lower incomes may need and want to spend more than 7 percent of their income on LTC insurance as an important way to protect their assets and have freedom of choice in receiving care. About two-thirds of people who buy LTC insurance use some portion of their savings to pay for LTC insurance, so an affordability index that only looks at income is not realistic.
Percent of Income Used to Buy LTC Insurance
Income Category % of Income Used
Under $20,000 4% to 12%
$20,000 to $35,000 2% to 7%
$35,000 to $50,000 1% to 4%
Greater than $50,000 1% to 3%

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 105
Are in Reasonably Good Health
People must be healthy enough to meet the insurance underwriting guidelines to qualify for the policy.
Are Concerned with the Possibility of Someday Needing LTC
While no one can predict future needs, someone with a family history of longevity and/or chronic health conditions may feel more “at risk” of needing LTC in the future. Or, someone who does not want to or cannot rely on family or friends for care may believe it is more important to have insurance to cover the costs of paid care.
Who Should Not Buy?
Already needs LTC Limited income and assets Qualifies (or near qualifying) for Medicaid Age makes premium not affordable Has family willing and able to provide care (considering “unknowns” of the future) Current health condition makes them not insurable The major reasons not to buy LTC insurance are related to consumers’ health and
financial circumstances. For consumers with few assets to protect who already qualify for Medicaid or are close
to qualifying, purchasing LTC insurance may not make sense.
Helping People Decide
While financial considerations are not the only important ones, they are a good place to begin. All tax-qualified LTC plans require agents to determine the financial suitability of a sale before the insurer can accept an application. Many states require insurance companies to use a “Suitability Personal Worksheet” and provide the consumer with a document called “Things You Should Know Before You Buy.” Both of these documents are intended to help the consumer decide whether LTC insurance is appropriate.
The “Personal Worksheet” (also called the Suitability Worksheet) is a good tool to use to begin thinking about whether LTC insurance is appropriate. The worksheet addresses financial conditions, but does not help consumers to think about risk, family situation, care options, and other reasons to buy. Therefore, it is important to consider other factors when discussing the findings from the worksheet.
The “Things You Should Know Before You Buy” sheet is helpful and it reminds clients that the Medicare and Medicaid programs do not pay for most LTC.
Agents should keep in mind the other reasons people buy LTC insurance. Having control over care choices and being able to receive care at home rather than in a facility are enhanced when someone pays for their LTC privately or with LTC insurance. Consumers should also think about their family situation. What impact would an extended LTC need have on the financial and emotional health of their family? Does the consumer have family living nearby who would be willing and able to provide care if needed? Remind consumers that family circumstances can

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 106
change and they may not have the same family support at the time they need care as they have today.
The insurance company cannot refuse to sell a policy based on their answers on the Personal Worksheet. Consumers also have the right to refuse to provide the financial information requested on the Personal Worksheet. Consumers cannot be refused simply because they elect not to provide financial information to the insurer.
Suitability – Personal Worksheet
Tax qualified plans must use the Suitability Personal Worksheet as part of the application process.
Consumers do not have to provide confidential or financial information. Consumers cannot be declined for coverage based on the answers in the worksheet. This is a guide to help consumers decide if the purchase makes sense for them. Different states have different requirements for form’s appearance and how it is used.
SAMPLE - NAIC Long-Term Care Insurance Personal Worksheet
People buy LTC insurance for many reasons. Some don’t want to use their own assets to pay for long-term care. Some buy insurance to make sure they can choose the type of care they get. Others don’t want their family to have to pay for care or don’t want to go on Medicaid. But LTC insurance may be expensive, and may not be right for everyone.
By state law, the insurance company must fill out part of the information on this worksheet and ask you to fill out the rest to help you and the company decide if you should buy this policy.
Premium Information
Policy Form number(s)______________
The premium for the coverage you are considering will be [$_________ per month, or $_______ per year,] [a one-time single premium of $____________.]
Type of Policy: (noncancellable/guaranteed renewable):__________________________
The Company’s right to increase premiums:__________________________________
[The company cannot raise your rates on this policy.] [The company has a right to increase premiums on this policy form in the future, provided it raises rates for all policies in the same class in this state.] [Insurers shall use appropriate bracketed statement. Rate guarantees shall not be shown on this form].
Rate Increase History
The company has sold LTC insurance since [year] and has sold this policy since [year]. [The company has never raised its rates for any long-term care policy it has sold in this state or any

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 107
other state]. [The company has not raised its rates for this policy form or similar policy forms in this state or any other state in the last 10 years.] [The company has raised its premium rates on this policy form or similar policy forms in the last 10 years. Following is a summary of the rate increase(s).]
Drafting Note: A company may use the first bracketed sentence above only if it has never increased rates under any prior policy forms in this state or any other state. The issuer shall list each premium increase it has instituted on this or similar policy forms in this state or any other state during the last 10 years. The list shall provide the policy form, the calendar years the form was available for sale, and the calendar year and the amount (percentage) of each increase. The insurer shall provide minimum and maximum percentages if the rate increase is variable by rating characteristics. The insurer may provide, in a fair manner, additional explanatory information as appropriate.
Questions Related to Your Income
How will you pay each year’s premiums?
From my Income From my Savings\Investments My Family will pay
[Have you considered whether you could afford to keep this policy if the premiums were raised, for example, by 20%?]
Drafting Note: The issuer is not required to use the bracketed sentence if the policy is fully paid up or is a noncancellable policy.
What is your annual income? (check one)
Under $10,000 $[10-20,000] $[20-30,000] $[30-50,000] Over $50,000
Drafting Note: The issuer may choose the numbers to put in the brackets to fit its suitability standards.
How do you expect your income to change over the next 10 years? (check one)
No change Increase Decrease
If you will be paying premiums with money received only from your own income, a rule of thumb is that you may not be able to afford this policy if the premiums will be more than 7% of your income.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 108
Will you buy inflation protection? (Check one)
Yes No
If not, have you considered how will you pay for the difference between future costs and your daily benefit amount?
From my Income From my Savings\Investments Family will pay
The national average annual cost of care in [insert year] was $[46,000], but this figure varies across the country. In ten years the national average annual cost would be about $[_____] if costs increase 5% annually.
Drafting Note: The projected cost can be based on federal estimates in a current year. In the above statement, the second figure equals 163% of the first figure.
What elimination period are you considering? Number of days______ Approximate cost $________ for that period of care
How are you planning to pay for your care during the elimination period? (Check one)
From Income From my Savings\Investments Family will pay
Questions Related to Your Savings and Investments
Not counting your home, about how much are all of your assets (your savings and investments) worth? (check one)
Under $20,000 $20,000-$30,000 $30,000-$50,000 Over $50,000
How do you expect your assets to change over the next ten years? (check one)
Stay about the same Increase Decrease
If you are buying this policy to protect your assets and your assets are less than $30,000, you may wish to consider other options for financing your long-term care.
Disclosure Statement

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 109
The answers to the questions above describe my financial situation. or I choose not to complete this information. (Check one)
I acknowledge that the carrier and/or its agent (below) has reviewed this form with me including the premium, premium rate increase history and potential for premium increases in the future. [For direct mail situations, use the following: I acknowledge that I have reviewed this form including the premium, premium rate increase history and potential for premium increases in the future.] I understand the above disclosures. I understand that the rates for this policy may increase in the future. (This box must be checked).
Signed: ___________________________________ _____________________________ (Applicant) (Date)
[I explained to the applicant the importance of completing this information. Signed: ___________________________________ _____________________________ (Agent) (Date)
Agent’s Printed Name: ________________________________________]
[In order for us to process your application, please return this signed statement to [name of company], along with your application.] [My agent has advised me that this policy does not seem to be suitable for me. However, I still want the company to consider my application].
Signed: ___________________________________ ____________________________] (Applicant) (Date)
Drafting Note: Choose the appropriate sentences depending on whether this is a direct mail or agent sale.
The company may contact you to verify your answers.
Drafting Note: When the LTC insurance Personal Worksheet is furnished to employees and their spouses under employer group policies, the text from the heading “Disclosure Statement” to the end of the page may be removed.
SAMPLE – NAIC Things You Should Know Before You Buy LTC Insurance
Long-Term Care
A LTC insurance policy may pay most of the costs for your care in a nursing home. Many policies also pay for care at home or other community settings. Since policies can vary in coverage, you should read this policy and make sure you understand what it covers before you buy it.
You should not buy this insurance policy unless you can afford to pay the premiums every year. Remember that the company can increase premiums in the future.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 110
The Personal Worksheet includes questions designed to help you and the Company determine whether this policy is suitable for your needs.
Medicare
Medicare does not pay for most long-term care.
Medicaid
Medicaid will generally pay for long-term care if you have very little income and few assets. You probably should not buy this policy if you are now eligible for Medicaid.
Many people become eligible for Medicaid after they have used up their own financial resources by paying for long-term care services.
When Medicaid pays your spouse’s nursing home bills, you are allowed to keep your house and furniture, a living allowance, and some of your joint assets.
Your choice of long-term care services may be limited if you are receiving Medicaid. To learn more about Medicaid, contact your local or state Medicaid agency.
Shopper’s Guide
Make sure the insurance company or agent gives you a copy of a book called the National Association of Insurance Commissioners’ “Shopper’s Guide to Long-Term Care Insurance.” Read it carefully. If you have decided to apply for LTC insurance, you have the right to return the policy within 30 days and get back any premium you have paid if you are dissatisfied for any reason or choose not to purchase the policy.
Counseling
Free counseling and additional information about LTC insurance are available through your state’s insurance counseling program. Contact your State Insurance Department or Department on Aging for more information about the senior health insurance counseling program in your state.
The Long-Term Care Insurance Market
The number of LTC insurance policies sold has grown at an average rate of approximately 18 percent annually between 1987 and 2001. Today 137 insurance companies offer LTC insurance to a rapidly growing marketplace. Still, only 14 companies represent over 80 percent of all the policies in force.
More than 100 insurance companies currently offer this type of coverage, although about 20 companies account for about 75 percent of all the policies currently in force. While there are many basic features in common, policies differ greatly in terms of the services covered, key policy provisions, the coverage amounts, and the premium cost.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 111
Market Segments by Types of LTC Insurance Policies
Individual (about 80% of all LTC policies) Association-sponsored group (small segment of the market) Employer-sponsored group about 15%) Sponsored by Continuing Care Retirement Community (small segment of the market)
Most LTC insurance is sold directly to individuals age 55 and over by agents, brokers, or financial planners meeting one-on-one with consumers. This “individual market” represents 80 percent of all the LTC policies currently sold.
A smaller but growing segment of the market is the group market, where LTC protection is sold to younger, working age adults as an “employee-pay-all” voluntary benefit through their employer. The typical buyer is a 46-year old employee. Since LTC insurance premiums are based on the age at the time of purchase and are designed to remain constant over one’s lifetime, average premiums are much lower in the employer-sponsored group market than in the individual market, where buyers are older.
A small segment of the group market is policies sold to association members (e.g., American Medical Association or American Bar Association) that offer a group discount of usually between 10 and 15 percent. The offering may be more limited choices than if the policy was bought directly from an agent. However, the same underwriting process is used as if bought from an agent.
Employer-sponsored plans are the fastest growing segment, but currently only comprise about 15 percent of all policies. Employers usually do not pay any part of the premium, but make the coverage available and premiums are paid through payroll deductions. Underwriting is often simplified for employees who are actively at work (i.e., not on leave).
Only a small portion of LTC policies today (approximately five percent) is provided as a rider to a life insurance policy.
Individual vs. Group Long-Term Care Insurance
Most people buy long-term care insurance individually from an insurance agent, financial planner or broker. States regulate which companies can sell long-term care insurance and the products that they can sell.
Another option for some people is to buy long-term care insurance offered through their employer. Many private and public employers, including the Federal government, offer group long-term care programs as a voluntary benefit. Employers do not typically contribute to the premium cost (as they do with health insurance), but they often negotiate a favorable group rate. In some cases there may be enhanced benefits and more related underwriting.
For those who are currently employed, it may be easier to qualify for long-term care insurance through their employer than purchasing a policy on their own.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 112
Why People Buy Long-Term Care Insurance
People buy LTC insurance for a variety of reasons – to avoid relying on others, to help them pay
for needed care, to preserve assets, and to protect their family’s quality of life.1
Source: Long-Term Care Group, Inc., 2003.
The most significant reasons for purchasing LTC insurance are fiscally related. Research shows that other important reasons include not wanting to burden loved ones and peace of mind.
Why People Buy
5% 5%
30%
25%
15%
10%
10%Freedom of Choice
Likely to Need
Protect Savings
Not Be Burden
Peace of Mind
Protect Lifestyle
Guarantee Affordability
Source: HIAA and Long Term Care Group, 2003.
There are many non-financial reasons why people consider LTC insurance. It is also important not to focus only on financial concerns. While financial concerns are important, they are not the only factors to consider.
Why People Do Not Buy Long-Term Care Insurance
People also cite different reasons for why they do not buy LTC insurance. It is important to identify these reasons, since part of the agents role is to help people overcome the denial, confusion, or misinformation that may be a barrier to planning ahead for LTC needs and considering LTC insurance.
Cost is one of the major reasons people do not buy LTC insurance. Confusion about which specific coverage features or type of policy is best is often encountered. Some consumers may be “waiting for better policies” and others are uncertain whether they can trust insurance companies to provide the coverage that they promise.
When someone says, “LTC insurance costs too much,” they might also mean that they do not yet perceive the value of coverage relative to the price. Or that they are considering coverage options that cost more than what they believe they can afford. Agents should help people

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 113
understand the value of LTC insurance and that it may be possible to find a less costly coverage option that will still provide adequate coverage appropriate to their needs.
Reasons People Give For Why They Did Not Buy LTC Insurance
Source: HIAA, 1990, 1995, 2000.
Buyers vs. Non-Buyers
Lack of knowledge of risk of requiring LTC at some point in the future, of the costs of purchasing a policy, and of who pays for LTC is the most important reason people do not buy.
Buyers understand that the government (Medicare or Medicaid) is unlikely to pay, that the individuals must pay, and that needing LTC is likely. They also believe it is important to plan ahead and are likely to have had some family or personal experience with LTC.
Personal LTC experience helps people “learn” these critical facts that then motivate interest in planning ahead. Non-buyers differ from buyers on each of these factors.
Although many people do not “plan ahead” for how they will manage their future LTC needs, some people certainly do plan ahead by purchasing LTC insurance. Seven studies conducted since 1987 help in understanding the key differences between buyers and non-buyers. These studies identify the motivators as well as the barriers to planning ahead.
In the individual market, buyers tend to be younger than non-buyers (age 67 versus age 71) and are more likely to be female (55 percent versus 52 percent). Conversely, in the employer group market, buyers tend to be slightly older than non-buyers (age 51 versus age 49), and are more likely to be male (38 percent versus 33 percent). No consistent differences emerge with respect to marital status across these studies.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 114
Demographic Differences between Buyers and Non-Buyers
Characteristic Buyers Non-Buyers
Individual Market - age 67 years 71 years
Employer Group Market - age 51 years 49 years
Individual Market - gender 55% female 52% female
Employer Group Market – gender 38% male 33% male
Source: Aggregate response to numerous surveys. Long Term Care Group, Inc. 2001.
Buyers are more likely to be college graduates, have higher income and greater assets, and have a higher propensity to save (through IRAs, mutual funds, or annuities). Buyers are more likely than non-buyers to perceive their health as “excellent.” Buyers are also less likely to have children living nearby.
While demographic differences between buyers and non-buyers exist, attitudes more consistently differentiate buying behavior. Buyers say that it is important to plan ahead for LTC needs and that, without insurance, they would pay on their own for LTC. Buyers are also much more likely to have had a personal experience with LTC and to see themselves at risk of needing LTC.
Attitudes of Buyers vs. Non-Buyers
Attitudes Buyers Non-Buyers
Self will pay 67% 35%
Likely to need LTC 65% 55%
Important to plan ahead 80% 48%
Have had family experience with LTC 40% 30%
Source: Aggregate response to numerous surveys. Long Term Care Group, Inc. 2001.
Suitability Case Study
Consider the suitability of LTC insurance for this married couple.
David and Leslie Phillips, 62 years old Two grown children living out of state David’s income = $65k Assets not counting property = $27k Have 401 K, IRAs and mutual funds for financial support in retirement

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 115
Mother-in-Law in nursing home after disabling stroke
What do you recognize about their personal and financial situation that signals whether or not it would make sense for them to consider LTC insurance?
Possible Answer: This couple has adequate income and assets to protect; has a “planning and saving” mentality, which fits well with LTC insurance; has experience with LTC in the family, thus are sensitive and receptive to the issue. In addition, David is likely to need care first, so they might want to have insurance to be sure that the cost of his care needs does not limit the financial resources available to Leslie, as she will likely outlive him.
Suitability Case Study
Consider the suitability of LTC insurance for this person.
Pauline Watson, age 77, widowed Grown daughter lives nearby Assets (CDs and savings) = $47k Monthly income after rent and other expenses = $750/month Does not expect income to increase Reasonably good health
What aspects of her situation raise concerns about whether she should buy LTC insurance?
Possible Answer: Pauline could move in with daughter for care if needed, or get help from daughter. She does not have much income or assets to protect. She is older so premiums are less affordable.
What reasons might this person have for buying insurance?
Possible answer: Pauline may not want to rely on her daughter. She may have a desire to “pass on estate,” even if modest. She is still in good health. An option may be to purchase facility care only coverage to pay most catastrophic expenses and her daughter could provide home care if needed.
Benefit Payment in Long-Term Care Insurance
Benefit Payment Method
There are three models in terms of how the daily or monthly benefit is paid:
reimbursement (or expense-incurred), indemnity, and disability (or cash).
Different types of LTC insurance offer different benefit programs. Some insurance companies offer more than one approach.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 116
Reimbursement Approach
This is the most prevalent approach because it is also the least costly. The policy pays 100 percent of LTC expenses up to a preset amount chosen when coverage is purchased. If an individual has chosen a nursing home daily benefit of $150/day, and is receiving care in a nursing home that costs $100/day, the policy will pay $100/day. If the nursing home care costs $120/day, then the policy would pay $120/day. But if an individual was in a nursing home that costs more than the $150/day benefit amount selected, the policy would pay the expenses, but only up to the $150/day benefit limit.
Most policies today use reimbursement approach, which is less costly and more efficient for the insured. The policy only pays as much as incurred in expenses – not more.
The reimbursement (or expense-incurred) model is the most common. In this model, the insured is reimbursed for the expenses he incurs that are covered by the policy, up to the daily or monthly benefit amount. In other words, the daily or monthly benefit amount serves as an upper limit on benefits, and for this reason it is sometimes referred to as the maximum daily (or monthly) benefit.
Example
Marianne has a reimbursement LTCI policy with a daily benefit of $200. For several months she receives home healthcare services costing $80 daily, and the insurer pays her $80 per day. Later she needs more home care, and her expenses total $125 per day. The insurer now pays $125 per day. Still later she enters a nursing home where care costs $220 per day, and the insurer pays the full daily benefit, $200.
Indemnity Approach
Some policies pay a set amount per day for care, based on the amount chosen when coverage is purchased. The amount paid, in this approach, does not vary based on the costs of care. So, if an individual is in a nursing home that costs $100/day, and has chosen a policy with an indemnity benefit of $150/day, the policy would pay $150/day. However, the additional $50 can be used as the individual wishes. Most insurers who use an indemnity approach will only use that approach for facility care; the policy would use the reimbursement approach for home and community care expenses.
Most indemnity policies only pay flat amount for facility care and do not pay for home care. These policies are intended to cover the “extra charges” beyond room and board. But many reimbursement plans include “extras” in the expenses that can accumulate for reimbursement.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 117
Under the disability (or cash) model the benefit is paid when the insured meets a benefit trigger whether he is actually incurring expenses for long-term care services or not. Under the indemnity model the insured must both meet a benefit trigger and be receiving services covered by the policy for benefits to be paid.
Examples:
Norma has an LTCI policy that covers facility care on an indemnity basis and has a daily benefit of $200. For several months she receives nursing home care costing $150 daily; later she needs more care, and the daily nursing home charge is $180; still later she receives care costing $220 per day. The insurer pays the daily benefit amount of $200 for all days on which Norma meets a benefit trigger and is receiving services covered by the policy, regardless of the cost of those services.
Disability Approach
A smaller number of policies offer a “disability payment approach.” In this approach, the policy makes a cash payment for each day that an individual is disabled (i.e., need help with ADLs or have a cognitive impairment), even if the individual does not receive any paid care or LTC services on that day. The “cash” can be used to pay for non-licensed or family caregivers, or anything an individual wants. While the disability approach allows more flexibility to use the benefit payments in any way one wishes, it also costs more – about 40 percent more than the reimbursement approach.
The disability model is more expensive (about 40 percent more). It is less critical today than in prior years because policies today now cover a broad range of care settings and provider types. When disability products first emerged in 1980s, it was not the case – so having a cash payment made more sense then than it does today. Still, it is simpler to understand and to administer. It provides advantages to a younger person, because there is more uncertainty regarding what LTC services and providers may exist in the future than today. This approach gives more flexibility to pay for care without everything having to be defined in the policy contract.
The indemnity model is most commonly used for facility care only, with the reimbursement model applied to other types of care. The disability model is often used for non-facility care only, with the reimbursement or indemnity models applied to assisted living or nursing home care.
Oliver has an LTCI policy that pays for home care on a disability basis and has a daily benefit of $150. For a several months he meets the physical impairment benefit trigger of the policy, but instead of receiving paid services, he is cared for by his daughter. Later he receives paid home healthcare services costing $80 daily, and still later he receives home care costing $125 per day. The insurer pays the daily benefit amount of $150 for all days on which Oliver meets a benefit trigger, whether he is receiving paid services covered by the policy or not, and regardless of the cost of any services may he receive.
Benefit Payment Methods – Case Study
Here is an example of how benefit payments would vary under each of these different payment approaches:

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 118
Marie’s LTC policy has a maximum home care benefit amount of $100/day. Marie has had a disabling stroke that has left her unable to bathe, dress, or get to and from the toilet without the help of another person. Marie lives at home and receives care from a Home Health Care Agency for six hours each day from Monday through Friday. In the evenings and weekends, her husband provides the care she needs.
Marie’s care costs $84 per day, with a total for one week of care of $420.
The reimbursement policy pays 100 percent of her $84/day expenses, up to the home care benefit amount she has selected of $100/day. Since Marie’s expenses are less than $100/day, her policy pays her $84/day – exactly the amount of her expenses. The weekly benefit total she receives is $420/week. Her weekly expenses for care are $420.
The indemnity policy pays $100/day for each day that Marie receives paid services. Her policy pays $100/day for each of the five days in the week that Marie receives paid care. The weekly benefit total she receives is $500. Her weekly expenses for care are $420.
The disability policy pays $100/day for each day that Marie is disabled, whether or not she receives paid care or family care. Her policy pays $100/day for seven days of the week. The weekly benefit total she receives is $700. Her weekly expenses for care are $420.
Payment Method Weekly Care Expenses
Weekly Benefit Payment
Difference (Net Payment To Marie)
Reimbursement $420 $420 $0
Indemnity $420 $500 $80
Disability $420 $700 $280
Because most policies use a “pool of dollars” approach, in this example, Marie’s coverage will last longer under the reimbursement approach than the other payment methods since her total lifetime “pool of dollars” is only being reduced by the actual amount of expenses she incurs, not by the full benefit amount paid under the other approaches. This is because her actual expenses are less than the daily benefit amount. This concept is described more fully in the section on Total Coverage Amount and how long the “pool of dollars” will last.
Case Study
Marie is in nursing home that costs $120/day
Reimbursement policy pays her actual expenses up to $150/day o Policy pays $120 for Marie’s nursing home care
Indemnity policy pays $150/day o Policy pays fixed amount, so pays Marie $150/day
Disability policy pays Marie $150 per day o Marie decides to move out of the nursing home and live with her daughter o Marie continues to receive $150 per day from her policy event though she is not
incurring and LTC expenses and is receiving care from her family

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 119
Keep in mind that with all of these policy types, the most that she will get from any of these policies is $150/day, even if her costs are higher.
Payment Method Daily Care ExpensesDaily Benefit
Payment Difference (Net
Payment to Marie)
Reimbursement $120 $120 $0
Indemnity $120 $150 $30
Disability $120 $150 $30
Things to Consider
Reimbursement approach is more cost-effective (and most common) Indemnity approach gives more additional flexibility to pay for some “extras” that might
not otherwise be covered Disability approach gives the most flexibility, but costs about 40% more in premiums
Tax Treatment of LTC Insurance
A vast majority of LTC insurance sold today is federally-tax qualified (TQ). It offers more standardized policy terms and consumer protection features.
Congress passed the Health Insurance Portability and Accountability Act (HIPAA) in 1996 to ensure that long term care insurance policies that meet certain standards receive favorable tax benefits.
For these tax-qualified long term care insurance plans, benefits received are generally not considered taxable income and buyers can also deduct long term care insurance premiums as medical expenses to the extent that they itemize their deductions and their total qualified medical expenses exceed 7.5% of their annual adjusted gross income.
Under a tax-qualified plan, benefits are payable when a licensed health care practitioner certifies that they are unable to perform at least two activities of daily living without substantial assistance for a period expected to last at least 90 days.
Policyholders are also eligible for benefits if they require substantial supervision to protect themselves due to a severe cognitive impairment such as Alzheimer’s disease.
Here are the specific rules for an individual to take a tax deduction for their LTC insurance premium. First, an individual must have medical expenses, including the premium that exceeds 7.5 percent of adjusted gross income. If so, the amount of the premium that one can deduct depends on their age. These amounts increase with inflation each year.
Age Maximum Deduction (2008)
<40 $310
41-50 $580
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 120
51-60 $1,150
61-70 $3,080
71+ $3,850
Per Diem: $270 (2008)
Tax-Qualified vs. Non-Qualified
Many companies only offer tax-qualified plans. But if someone is considering buying from a company that offers both options, here are some things to think about. In the long run, it is probably best to buy a TQ plan. If someone buys an NQ plan, they are taking a chance that they may be required to pay taxes on the benefit payments you receive. They also would not be able to deduct premium payments (even if they otherwise qualify for the 7.5 percent medical expense deduction.) There are small differences between a TQ and NQ plans, but the potential tax advantages outweigh these differences.
Often there is not much difference between TQ and NQ plans.
TQ plans have added advantage that one can be certain that benefits are tax-free and premiums may be deductible if one qualifies.
The differences between these plans are minimal, but some difference in access to benefits.
Some short-term disabilities (lasting less than 90 days) may be covered under NQ but not TQ.
“Medical necessity” benefit condition does not really add much, if anything, to benefit access since LTC is not about “medical” need.
The few companies who offer NQ coverage charge the same premium for TQ and NQ. TQ policies must use at least five of the six ADLs and cannot require loss of more than
three ADLs as basis for paying benefits. Severe cognitive loss is a basis for receiving benefits in a TQ plan.
Tax Qualified (TQ)
Premiums deductible, in certain circumstances Benefits tax free Must use at least 5 of the 6 ADLs and cannot require loss of more than 3 ADLs as basis
for paying benefits Severe cognitive loss as basis for benefits Disability expected to last at least 90 days Cannot use “medical necessity” as basis for paying benefits
Non-Qualified (NQ)
Premiums not tax deductible No IRS decision on whether benefits are taxable as income Does not have to base benefits on ADL loss

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 121
Does not have to use cognitive loss as basis for benefits and no prescribed definition of cognitive loss
Can cover short-term disability (<90 days) Can use “medical necessity” as basis for benefits

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 122
Chapter Five - Long-term Care Insurance Features, Benefits and Provisions
This chapter takes a closer look at the features, benefits, and policy provisions of long-term care (LTC) insurance. At the conclusion of this chapter, agents will:
Know what services are typically covered in a LTC insurance policy–and which are excluded
Understand how products have evolved and improved over the years. Become familiar with the typical structure and amounts of coverage that is available for
consumers to select. Understand how “inflation protection” works and why it is important to consider in
choosing a LTC insurance policy. Understand the “pros” and “cons” of different approaches to “inflation protection.” Learn about other important policy provisions like the elimination period, premium waiver
and the role of care coordination
Policy Improvements
Today’s LTC insurance policies have undergone major improvements, such as the types of benefits covered and consumer protection features. Consumers considering buying today have better choices and coverage than the earlier policies offered.
Cover wide range of non-institutional care options (i.e. Assisted Living and home care) Sound basis for paying benefits Help people find services - Care coordination Enhanced consumer protection features
Features and Benefits
Covered Services Benefit Amounts Inflation Protection Nonforfeiture Provisions Elimination Period (deductible) Premium Waiver Care Coordination Other Coverage Options Policy Procedures and Other Provisions Consumer Protection Features
Covered Services
Long-term care policies vary in terms of the specific services they will cover and the nature and extent of coverage provided for those services. The vast majority of coverage sold today is “comprehensive” in that it provides benefits both for facility-based care and for care at home or in the community. This is in contrast to the earliest LTC policies, which emphasized institutional

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 123
care and provided little or no coverage for care at home. Today about 70 percent of policies sold are “comprehensive” in terms of the care settings and services covered.
The best way to understand which services are covered and which are not is to review the Outline of Coverage and, if possible, a specimen policy. The Outline of Coverage will summarize the services covered and the benefit amounts for each service, as well as any important exclusions or limitations on coverage (e.g., whether care provided by immediate family can be covered or is excluded).
Applicants choose the type of coverage they prefer – “comprehensive” or “facility care only.” Most policies today are comprehensive, but some people prefer to buy facility-care-only policies. These pay for care in a nursing home or assisted living facility, but not for care at home or in the community. These policies may still include hospice or respite care. Facility-care-only policies cost less than comprehensive policies, and if people prefer and have family or friends to provide care at home, they may only need the policy to reimburse them for paid care in a facility if and when they need it.
“Facility Care Only” or “Comprehensive policy”
Most people who buy LTC insurance (70 percent) buy comprehensive care policies, which cover both facility care and care at home or in the community. Comprehensive policies include:
Nursing home Assisted living Home care Adult day care Respite care Hospice care Supportive services
Some people however prefer “facility care only” coverage because it is less expensive and covers the most catastrophic of LTC costs – care in a nursing home.
Today’s facility care policies also include coverage for nursing home and assisted living facility care.
Older people or those with family members who can provide care at home are more likely to buy “facility care only” policies.
Facility Care
Different types of facilities are covered.
Licensed Nursing Home
Nursing home care is generally provided in a licensed facility, but is not limited to Medicare-certified or skilled care facilities only. Some LTC policies will also cover care in a non-licensed nursing facility, such as a Christian Science care facility or a private, non-licensed nursing home associated with a Continuing Care Retirement Community (CCRC).

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 124
Assisted living facilities
Assisted living facility is a general term describing a broad range of care facilities that combine care and residential living. These facilities are generally more “independent” than nursing home care. Residents may have their own room or apartment, but receive supportive and personal care services from the facility.
Each LTC policy defines the specific care-related criteria that an “assisted living facility” must meet in order to be covered. This is important since there are significant differences across states in how such facilities are licensed and what they are called. It is also important to describe the services and features that qualify a facility as a covered “ALF” since the objective of LTC insurance is to pay for care-related services and supports for someone who is chronically ill (needs help with Activities of Daily Living (ADL) or has a cognitive impairment). The intent of LTC insurance is not to pay for rent or independent living costs – whether at home or in an assisted living environment.
An example of how a LTC policy might define a covered ALF is shown below.
An Assisted Living Facility means a facility that is engaged primarily in providing on-going care and related services and meets all of the following requirements:
It provides services and care on a continuous twenty-four (24) basis sufficient to support the needs resulting from the inability to perform the ADL or a Severe Cognitive Impairment;
It has trained and ready-to-respond staff actively on duty in the facility at all times to provide the services and care;
It makes and keeps records of all care and services provided to each resident;
It provides at least three meals a day to all residents and accommodates special dietary needs;
It is licensed by the appropriate licensing agency, if licensing is required by the state, to provide residential services and Maintenance or Personal Care Services for at least six inpatients in one location;
It has formal arrangements with a Physician or Nurse to furnish medical care in case of an emergency; and
It has appropriate procedures to provide onsite assistance with prescription medications.
Typical Comprehensive Long-Term Care Insurance Benefit
In addition to nursing facilities and assisted living facilities policies that provide “comprehensive” coverage include the following types of home and community care services and settings:
Home health care; Personal care Homemaker services Adult day care;

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 125
Hospice care; and Respite care
Some policies may pay for services or devices to support people living at home:
Equipment such as in-home electronic monitoring systems Home modification, such as grab rails and ramps Transportation to medical appointments Training for a friend or relative to learn to provide personal care safely and appropriately
Some policies provide payment for family members or friends to help care for them, but may do so on a limited basis or only in relation to the costs that the family member incurs.
Many policies provide a care coordinator, usually a nurse or social worker in the community. The care coordinator can meet with them and discuss their specific personal situation. The care coordinator helps arrange for and monitors their care needs on an ongoing basis, if they want that kind of help.
The majority of policies sold today are comprehensive policies, which cover care and services in a variety of long-term care settings:
Their home, including skilled nursing care, occupational, speech, physical and rehabilitation therapy, as well as help with personal care, such as bathing and dressing. Many policies also cover some homemaker services, such as meal preparation or housekeeping, in conjunction with personal care services.
Home and Community Care
When choosing a policy, it is important to consider who can provide care at home, what types of services in the policy help support informal (family) caregivers, and where hospice and respite care can be provided. While most people prefer care at home, being able to receive temporary respite care in a facility might be a less costly option for some families.
Home care includes a broad range of services including:
Home Health Care - Skilled nursing care and occupational, speech, physical, respiratory, and other therapies);
Personal care - help with ADL from a home health aide or personal care worker; and Homemaker services - such as meal preparation or housekeeping.
It is important to review the policy language to understand who can provide care at home. Allowing care to be provided by independent providers helps enhance consumers’ access to care at home, but it is also important for them to be sure that the provider coming into their home is trustworthy and qualified by training and experience to provide the care they need.
Policies may limit home health care to services provided by a licensed home health care agency, but do not require that the agency be Medicare-certified. However, many LTC policies allow care at home to be provided by “independent providers” which may include nurses, therapists, personal care workers, or homemakers who are qualified by

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 126
training and experience to provide such care but who are not working through or affiliated with a home health care agency.
“Homemaker” services are paid for only if they are provided in conjunction with personal care needs. Some policies cover homemaker services (e.g., laundry and housekeeping help) even if that is the only service received. Polices may also pay for this type of care when it is provided as part of a visit to help an individual with bathing or dressing. Regardless, the policy will not pay for homemaker services unless an individual receiving them has a qualifying level of impairment – needing help with 2 or more ADLs or suffering from a cognitive impairment.
Adult day health care is covered, but a senior center that is only focused on “social events” and does not have the staff or training to meet personal care needs would not qualify. Policies also generally pay for care in (and transportation to/from) an adult day health care center, which provides personal care, assistance with medication and/or supervision, and support during the day.
Hospice Care
Most LTC policies provide benefits for “hospice care” for individuals who are both terminally ill and who need LTC. These benefits include personal care support and services (both at home and in a facility). The policy does not pay for physician care, pain medications, or other “medically-related” care. These services are generally covered under Medicare hospice care benefit.
An LTC policy supplements other “hospice care” programs; it is not a substitute for traditional hospice care. An individual must also need help with ADLs (or have cognitive loss) and be terminally ill to receive hospice care as part of a LTC policy. Some LTC policies allow an individual to access hospice care benefits without requiring them to satisfy the elimination period.
Respite Care
Respite care is designed specifically for people who only need care for a short amount of time each year because they have family, friends, or other unpaid caregivers who can meet their care needs.
Most LTC policies pay for temporary care while family members or unpaid caregivers take “time off” from their caregiving responsibilities. Respite care may be provided in a facility or at home. Generally, individuals can receive respite care in any of the LTC service settings that the policy covers.
Many policies limit the amount of respite care to 15 to 30 days each year and do not usually require insureds to first meet an elimination period in order to access these benefits. If care is needed for longer than the brief “respite” needed to support family caregivers, then an individual can satisfy the elimination period and begin to receive covered services on an on-going, extended basis.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 127
Things to Consider
Individuals should read the Outline of Coverage and policy language, rather than relying on the marketing brochure to understand “what is covered”.
It is important to understand how services are defined and the conditions that must be met by providers. This level of detail is not usually in the marketing information.
Individuals should understand that LTC insurance policies do not pay for “rent” or independent living costs. While policies cover assisted living facilities, this does not mean that they will pay an individual’s monthly fees if that person is not receiving personal care and does not meet the policy’s “benefit triggers”.
Individuals should explore the benefits that are available to help support informal/family caregivers.
Long-Term Care Insurance Exclusions
Like all insurance, long-term care policies have exclusions. These are listed in the policy and state laws often regulate what exclusions are allowed. Long-term care policies typically exclude the following (even if the insured meet all the other requirements of the policy):
Care or services provided by family member unless the family member is a regular employee of an organization that is providing the treatment, service or care; and the organization they work for receives the payment for the treatment, service or care; and the family members receives no compensation other than the normal compensation for employees in his or her job category; Most policies provide training and support for these informal caregivers, but do not pay benefits when they receive care from someone who is not a paid caregiver.
Care or services for which no charge is made in the absence of insurance; Care or services provided outside the United States of America, its territories or
possessions. However, a growing number of policies now have an international care benefit that can provide care outside of the United States;
Care or services that result from war or act of war, whether declared or not; Care or services that result from an attempt at suicide (while sane or insane) or an
intentionally self-inflicted injury; Care or services for alcoholism or drug addiction (except for an addiction to a
prescription medication when administered in accordance with the advice of their Physician);
Treatment provided in a government facility (unless otherwise required by law); Services for which benefits are available under Medicare or other governmental
program (except Medicaid), any state or federal workers' compensation, employer's liability or occupational disease law, or any motor vehicle no-fault law
Most policies require that the facility, agency or individual providing care meet certain minimum standards with respect to quality, safety, and training. For example, a nursing home that is not licensed but operates in a state that requires licensure, would not be covered.
Long-term care policies focus on paying for the types of services and providers that someone needs when they cannot perform their Activities of Daily Living or when they have a Cognitive Impairment, so they do not pay for care or services unrelated to these needs, such as hospital stays or prescription medications.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 128
Some policies pay for prescription drugs provided while they are in a care facility (but not at home), and some policies pay for transportation costs to help them get to medical appointments when they are physically or cognitively impaired.
Some policies provide coverage for care related to everyday household needs such as housekeeping, laundry, meals, and managing medications, so-called “instrumental activities of daily living,” but only when they receive that help as part of the help them get from a formal care provider assisting with Activities of Daily Living. So most policies do not pay for in-home help if all they need is help with housekeeping, meals, laundry, transportation and the like.
Finally, long-term care policies do not pay for items provided solely for their comfort or convenience, for example a television in their nursing home room or a visit to the facility's hair care salon.
Private Insurance Does NOT Cover LTC
Private Health Insurance or Health Maintenance Organization (HMO)
Most forms of health insurance (such as the private health insurance or Health Maintenance Organization (HMO)) follow the same general rules as Medicare. If they do cover long-term care, it is typically only for skilled, short-term, medically necessary care. Like Medicare, the skilled nursing home stay must follow a recent hospitalization for the same or related condition. Coverage in a Skilled Nursing Facility is limited to 100 days. Home care is also limited to medically necessary, skilled care. Custodial or personal care is never covered. However, most people who need long-term care need custodial or personal care.
Medicare Supplement Policies ("Medigap")
Medicare supplement insurance policies (also called Medigap Insurance) are designed to cover some of the “gaps” in Medicare. These gaps refer to Medicare co-pays and deductibles. Medigap insurance enhances the hospital and doctor coverage, but does not extend to long-term care coverage. For the small portion of nursing home stays that qualify for Medicare coverage, a Medigap insurance policy may cover the daily Medicare co-payment ($128/day for days 21-100). Medigap insurance is not intended to meet long-term care needs and provides no coverage for the vast majority of long-term care expenses.
Disability Insurance
Disability income insurance is designed to replace a portion of the income people lose if they’re unable to work due to accident or injury. It provides no additional benefits to specifically pay for long term care expenses. Disability benefits do not cover either medical care or long-term care. Most disability insurance policies do not provide any benefits after the insured is over age 65 – exactly when they are more likely to need long-term care.
Health Savings Account (HSA)
An HSA (health savings account) is an account established to pay for qualified medical expenses, including qualified long term care costs and long term care insurance premiums. Contributions and withdrawals are tax-free for qualified expenses.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 129
By law, HSAs are available to people who enroll in an HDHP, are not Medicare enrolled, are not covered by another health plan, or are not claimed as a dependent on someone else’s Federal tax return. The health plan credits a portion of the health plan premium to the HSA. People have the option to make additional tax-free contributions to their account, so long as total contributions do not exceed the limits established by law, generally the plan deductible.
Features of an HSA include:
HSA contributions are tax-deductible Interest earned on the HSA account is tax-free Withdrawals for qualified medical expenses are tax free Unused funds and interest are carried over, without limit, from year to year They own the HSA and it is theirs to keep — even when they change plans or retire The HSA is administered by a trustee/custodian
Daily, Monthly, and Weekly Benefits
Long-term care insurance policies have a benefit amount per day or month (or sometimes per week). A person buying a policy selects the benefit amount, which typically ranges from $4050 to $350-500 per day and from $1,000-1,500 to $8,000-15,000 per month. Within these ranges, the daily amounts the purchaser can select are in increments of $1, $5, or $10, depending on the company, and the monthly amounts are usually based on units of $100.
Many policies (especially newer ones) pay a monthly benefit instead of a daily benefit, and some policies pay a weekly benefit. A monthly or weekly benefit allows for greater flexibility in meeting expenses.
Example
Joyce has a reimbursement policy with a daily home care benefit of $100. Her family provides much of her care, so on Saturdays and Sundays she needs no paid services. On Mondays, Wednesdays, and Fridays a home health agency provides services costing $150, and on Tuesdays and Thursdays the agency provides services costing $75. Her total expenses for the week are $600, but because she can receive no more than her daily benefit of $100 for any one day of care, she receives $450 in benefits and must pay the other $150 out of her own pocket.
Now let us assume Joyce has a reimbursement policy with a weekly benefit of $700. Her weekly expenses fall below this amount, so she receives $600 in benefits.
A monthly or weekly benefit may cost slightly more than an equal daily benefit, but it can enable an insured to cover more services with the same benefit amount.
Facility Care and Home Care
Some policies pay the same benefit amount for different types of care, while others pay different amounts. When amounts differ, the home care benefit is often defined as a percentage of the facility benefit (normally from 50 to 100 percent). The purchaser often selects this percentage, and of course the higher the percentage, the higher the premium. Some advisors recommend choosing at least 75 percent or (if possible) 100 percent, since most people prefer to remain at

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 130
home as long as possible and extensive home care services can be expensive. On the other hand, those seeking to hold down the premium may be able to get by with a lower percentage, especially if family members are available to provide some care.
Daily Benefit Amounts
People can select the amount they want their LTC policy to pay for care each day. All policies provide a choice of the amount paid for nursing home care. Many policies pay the same amount for care in an assisted living facility as for nursing home care. Benefit amounts for “facility care’ generally range from $50 per day to $500 per day or more.
Many policies also allow consumers to choose the amount they want the policy to pay for care at home. Or they may simply decide whether they want the “benefit amount” for home care to be the same as the facility care amount (100%) or if they want the home care benefit to be lower than the facility care amount. Typical choices other than 100% are 50%, 60%, 75%, or 80%. Some policies simply have one benefit amount that applies to all covered services.
A higher home care benefit amount makes it easier to pay for “round the clock” care at home. However, this level of coverage costs more. Most people receiving care at home usually do not need 24-hour formal care, especially if there are family members or friends who can help by supplementing paid care.
Choosing a Daily Benefit Amount
To help individuals decide what daily benefit amount (DBA) is appropriate, it is important to look into the costs in their area (or the area in which they plan to live when they need care). Ask friends or family who have needed care, or call some nursing homes, assisted living facilities or home care agencies to get a sense of area costs. Costs can vary quite a bit from one provider to another.
To help consumers select the DBA that makes sense for them, this chart shows the average costs of nursing home care in each state. This can vary from city to city.
Daily, Weekly or Monthly Benefit Amount
While most LTC policies pay expenses up to the daily benefit amount selected, some policies are more flexible. These policies have a weekly or monthly limit, not a daily limit, on how much they will pay. This allows insureds to spend more on care on days when they might not have any family care (e.g., Monday through Friday while a spouse is at work), and spend less or nothing on days when family care is available. A weekly or monthly limit approach results in a greater amount of home care costs being covered than with a daily benefit limit approach.
Example:
Leo needs 8 hours of home care each day Monday through Friday, costing $80 per day. He does not need any paid care on the weekend when his wife is home.
His weekly home care costs is $400 (5 x $80 per day).

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 131
Policy Daily or Weekly Limit?
Amount Paid Expenses Not Covered
Policy A Daily limit up to $60 per day
$60/day x 5 days = $300/week
$400 - $300 = $100/week
Policy B Weekly limit up to $60 x 7 = $420
Expenses up to $420/week
None. Policy pays all $400/week since the weekly limit of $420 has not been reached.
Example - Comparison of Daily Benefit and Weekly Benefit
Scenario:
Leo needs 8 hours of home health care on Monday to Friday It Costs $80/day On the weekend, he can get care from family Leo’s expenses are 5 X $80 = $400
This illustrates the advantages of a policy with a weekly home care benefit to cover one’s LTC expenses versus a policy with a daily benefit.
Many people who need care receive more care on some days of the week than other days. For example, on the weekends, Leo gets care from his family. But on the weekdays, he needs care 8 hours per day.
Policy A Daily Benefit
Policy A pays home care expenses up to $60/day Policy A pays Leo $300 for the week of care ($60 x 5 days) He has an additional $100 of expenses that the policy will not cover
Policy B Weekly Benefit
Policy B pays home care expenses up to weekly maximum of $420 ($60/day x 7 days/week)
Policy B reimburses all of Leo’s costs of $400 because it is less than his weekly maximum of $420
The weekly benefit approach pays an amount based on the number of days in the week in which Leo is disabled (i.e., needs help with 2 or more ADLs or has a cognitive impairment). This approach pays him more overall. Leo can then use the additional payment to cover the higher costs of care he incurs on days when family care is not available.
Many states specify the minimum amount of benefit that can be sold. This ensures that coverage amounts are meaningful based on costs of care. Consumers should also keep in mind that home care and assisted living facility care often cost less than nursing home care. However, for 24-hour care at home, costs could be higher. Long-term care insurance does not have to cover all the costs to still be meaningful. It is important for consumers to cover what is important to them.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 132
Things to Consider
Consumers should consider several factors in selecting benefit amounts for their coverage. o Cost of care in their area o Cost at specific facilities or providers o Family or friends who might help with care o Policy with weekly or monthly home care benefit
Consumers can generally reduce their benefit amount if they have over bought, but it may be difficult to increase the benefit amount if there are changes in health status.
Summary of 2008 LTC Costs Nationwide
Homemaker Services (Non-Medicare Certified, Licensed)
Provide “hands-off” care such as helping with cooking and running errands. Often referred to as “Personal Care Assistants” or “Companions.” This is the rate charged by a non-Medicare certified, licensed agency.
National average hourly rate of $18 4% increase over 2007 Five-year annual growth of 2%1
Home Health Aide Services (Non-Medicare Certified, Licensed)
Provide “hands-on” personal care, but not medical care in the home with activities such as bathing, dressing, and transferring. This is the rate charged by a non-Medicare certified, licensed agency.
National average hourly rate of $19 3% increase over 2007 Five-year annual growth of 1%1
Home Health Aide Services (Medicare Certified)
Provide “hands-on” personal care and sometimes skilled care associated with a nurse visit in the home. Assist with activities such as bathing, dressing, and transferring. This is the rate charged by a Medicare certified agency.
National average hourly rate of $38 18% increase over 2007 Four-year annual growth of 7%2
Adult Day Health Care
Provides social and other related support services in a community-based, protective setting during any part of a day, but less than 24-hour care.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 133
National average daily rate of $59
Assisted Living Facility (Private One Bedroom)
Provides “hands-on” personal care as well as medical care for those who are not able to live by themselves, but do not require constant care provided by a nursing home.
National average monthly rate of $3,008 11% increase over 2007 Five-year annual growth of 6%1
Nursing Home (Semi-Private Room)
Provides skilled nursing care 24-hours/day.
National average daily rate $187 4% increase over 2007 Five-year annual growth of 4%1
Nursing Home (Private Room)
Provides skilled nursing care 24-hours/day.
National average daily rate $209 2% increase over 2007 Five-year annual growth of 4%1
1 Represents the compound annual growth rate based on data from 2004-2008. 2 Represents the compound annual growth rate based on data from 2005-2008.
Lifetime Maximum Benefit
LTCI policies normally have limits on the total amount the insurer will pay in benefits during the life of the policy. Some older policies have a benefit period, a maximum amount of time benefits will be paid, and some have different benefit periods for different types of care. (For instance, a policy might pay for nursing home care for four years and home care for two years) or an unlimited period of years. But most policies today have a lifetime maximum benefit (commonly called a pool of money). Under this approach an insured receives benefits until the total amount received for all types of care reaches a maximum amount stipulated by the policy, regardless of how much time has elapsed. The insured chooses this amount at the time of purchase.
Some insurers have the purchaser choose among round dollar amounts, such as $100,000, $200,000, or $500,000. Other companies define the pool of money as the daily or monthly benefit amount multiplied times a certain period of time, and the purchaser chooses among options such as two, three, four, five, six, and ten years. For example, an insured might choose a daily benefit of $200 and a lifetime maximum based on three years. His pool of money would be calculated by multiplying $200 times 365 days times three years, yielding $219,000.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 134
However, it must be understood that while the number of dollars in the pool of money may be based on the payment of certain maximum benefits for a certain period, benefits are not limited to that period, as with a benefit period. As stated above, the insured receives benefits until he has received the maximum dollar amount, regardless of the time elapsed. If an insured spends less than the daily benefit amount on some days, the unspent balance remains in his pool of money, and this allows him to receive benefits beyond the time period on which the pool of money was based on. There are also unlimited “pool of money” policies available. With these the only “cap” is on the daily, weekly or monthly maximum benefit, not on the lifetime benefit amount.
Example
Barbara buys a reimbursement LTCI reimbursement long-term care insurance policy and chooses a daily benefit of $150 and a lifetime maximum based on five years. Her pool of money is $273,750 ($150 daily benefit X 365 days X 5 years = $273,750).
Suppose Barbara enters a nursing home and receives her full $150 daily benefit every day for five years. At the end of five years, she will have spent $273,750, and her benefits will end.
Now suppose that instead of going into a nursing home, Barbara receives limited home healthcare services and needs only $100 of benefits per day. At the end of five years, she will have spent $182,500 ($100 X 365 days X 5 years), leaving $91,250 in her pool of money ($273,750 minus $182,500). In this case, Barbara will continue receiving benefits beyond five years. She will receive benefits either at home or in a facility for as long as there is still something left in her pool of money.
Finally, suppose that Barbara has an older policy with a five-year benefit period instead of a pool of money. Barbara will receive benefits for no more than five years, even if she receives less than her daily benefit amount on many days during those five years.
Under the NAIC Long-Term Care Insurance Model Act, the lifetime maximum of an LTCI policy must provide at least 12 months of benefits, and some states have 24- or 36-month minimums. Some policies (called lifetime policies) have an unlimited lifetime maximum. The insured can continue receiving the daily or monthly benefit amount indefinitely.
Most benefits have specific dollar limits on certain coverages such as home modification, devices, or caregiver training.
They choose a Maximum Lifetime Benefit or total lifetime amount they want the policy to provide. Policies typically offer a choice of lifetime dollar amounts – for example $100,000 or $300,000. The dollar amounts may correspond to a period of time. For example, a three-year policy at $100/day of benefits would provide $109,500 worth of care.
Pool of Dollars Approach
Most policies pay LTC expenses up to a total coverage amount (or lifetime maximum benefit). Today, most LTC policies specify an overall dollar amount that applies to all covered services as the “total coverage amount.” Older policies limit coverage to a specified number of days (or

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 135
years), rather than dollars, or specify separate limits by each type of service (e.g., pay for up to two years of home care and up to four years of nursing home care).
The policies today provide more flexibility, allowing consumers to decide how they want to spend the overall dollar limit on any of the covered services. A consumer can use the benefit all for home care, or all for facility care, or any combination, up to the overall dollar limit.
How the Pool of Dollars is Calculated
The “total coverage amount” is usually calculated by multiplying a number of years times 365 days per year times the nursing home daily benefit amount chosen.
Example:
3 years x 365 days x $100/day = $109,500 or 3 years x 365 days x $150/day = $164,250 or 5 years x 365 days x $100/day = $182,500 or 5 years x 365 days x $150/day = $273,750
Not all choices are available from all insurers, but generally, consumers can choose from as little as one year of coverage to as much as 10 years of coverage.
How Long Benefits Will Last
The duration of the benefits depends on type, amount, and frequency of care received. The advantage of the “pool of dollars” design is that consumers can stretch how long benefits last if care is received less often than everyday or costs less than the policy’s daily maximum.
Consumers can “stretch” the length of their benefits by receiving care that costs less than the daily maximum or deciding that care is not needed on a daily basis. This allows consumers to be in control of their benefits and how long they last.
Some people think a “three-year policy” only lasts for the three years. However, agents should help consumers understand that it is actually 1095 days worth of care and that days do not have to be consecutive. The limit is an overall dollar amount based on a factor of “three years” not literally limited to three years.
Example - This example illustrates the flexibility of “pool of dollars” policies.
Total Coverage Amount of $109,500
Nursing Home ($100/day)
Assisted Living ($100/day)
Home Care ($50/day)
Minimum: At least 3 years, if care is received everyday at $100/day
At least 3 years, if care is received everyday at $100/day
At least 6 years, if care is received every day at $50/day
Stretching the Benefit
Would last 4 years if care costs $75/day
Would last 4.3 years if care costs $70/day
Would last 14 years if only needed care 3 days/week
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 136
Benefits will never last shorter than the “multiplier amount.” Thus, a “three-year plan” will never last less than three years worth of days of care. But, it can often last longer.
Most people will use a combination of care types over the continuum of care. Someone may use home care for a period of time, then move into an assisted living facility and finally into a nursing home with the pool of dollars. That is one of the advantages of the “pool of dollars” approach.
Case Study for Pool of Dollars
Participants should calculate how long benefits would last under the following scenarios.
Total Coverage Amount: $109,500 Nursing Home Daily Benefit: $100/day Assisted Living Facility Benefit: $100/day Home Care Benefit: $ 50/day
1. Scenario A: A Policyholder receives care in a nursing home which costs $100/day for care and they are there everyday. How long will their benefits last?
2. Scenario B: Same as above except they find a less costly nursing home that charges $80/day. How long will their benefits last?
3. Scenario C: They receive care at home every day which costs $50/day for care. How long will the benefits last?
4. Scenario D: Someone receives care at home 4 times a week which costs $50/day (or $200/week). How long will the benefits last?
5. Scenario E: Someone receives care in a nursing home which costs $150/day for care and they are there everyday. How long will the benefits last?
6. Will their benefits ever be used up more quickly than 3 years? Why not?
7. Name some ways to “stretch” how long the benefits last?

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 137
Answers
1. Scenario A: [Answer: 3 years] 2. Scenario B: [Answer: 3.75 years] 3. Scenario C: [Answer: 6 years] 4. Scenario D: [Answer: 10.5 years] 5. Scenario E: [Answer: 3 years] 6. [Answer: No. Because the most that can be paid on any day is $100/day even if care
costs more than that. So, $109,500 divided by $100/day will always be 3 years. Benefits can’t be used up any faster than $100/day.]
7. [Answer: By receiving care at less cost that the full daily benefit amount or by receiving care less often than every single day of the week.]
Lifetime/Unlimited Coverage
Many policies offer “unlimited” or lifetime coverage option Benefits last as long as people need care No overall dollar limit, but daily limits still apply
About one-third of people buying LTC insurance today buy “unlimited” coverage that lasts as long as they continue to need care. This type of policy is more expensive, but it is appropriate for people who want to be sure they never run out of coverage. This type of policy may be appropriate for younger consumers who might need LTC longer, especially if they begin to need care when they are still young. However, consider a consumer who bought “three-years worth of coverage”. If care lasted for four years, this person had coverage for 75 percent of his or her care needs. And, if it was a partnership policy, they would probably be eligible for Medicaid when coverage ran out.
While 80 percent of people who enter nursing homes stay five years or less, lifetime coverage can provide peace of mind that care needs will not outlast benefits. However, not everyone can afford lifetime/unlimited coverage. Each person has to select the coverage amount that best meets their “comfort level” and their ability to afford the premiums. There is no “one size fits all.”
Inflation Protection in Long-Term Care Insurance
The cost of long-term care services has increased steadily for many years, and this trend is expected to continue.
Looking ahead, the American Council of Life Insurers projects that if the cost of nursing home care keeps climbing at an annual rate of 5.8 percent (the average rate of increase since 1990) for another several years, by 2030 the average cost of a year of nursing home care will be $108,000 (in 2005 dollars).12
12 American Council of Life Insurers (2005). “Long Term Care Insurance or Medicaid: Who Will Pay for Boomers’ Long-Term Care?”
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 138
Inflation protection is one of the most important topics within LTC insurance. It is important to consider how inflation affects the costs of LTC and the value of the coverage that is bought today. Most people buy coverage many years before they might need it. But the costs of care increase each year Thus, those who do not plan for the effects of inflation may find their coverage is inadequate in the future.
Long-term care is different than “medical care.” While medical care is very "high tech,” LTC is much more “high touch.” LTC costs depend heavily on the labor market, while health care costs typically depend on the cost of “technology” involved in medical care
Individual, tax-qualified LTC policies must offer inflation protection to each applicant. Group policies usually let the sponsoring group policyholder (e.g., the employer) decide whether and how to include inflation protection in the policy.
Those buying an LTCI policy generally have the opportunity to purchase optional provisions that protect against inflation. And although it adds to the premium price, inflation protection can be one of the most important features of an LTCI policy, especially for those purchasing coverage many years before they expect to need benefits.
Automatic Inflation Protection
An Automatic Inflation Option means that the limit of insurance will increase each year by a set rate (e.g., 5% annually). While the initial premium is higher with this option, people will not have to think about future inflation increases, since they are automatic, with no commensurate increase in premium.
Be sure clients know the set rate and if the increase is simple or compound. A compound increase provides the most protection, but costs more. On the other hand, the compound rate provides better protection when the need for the benefit is not expected to occur for 15 or more years, as is the case with younger buyers of LTCI.
With automatic inflation protection, benefit amounts are increased every year at a set rate with no action by the insured required and with no corresponding increase in premium. The increases generally inflate both the daily/monthly benefit amounts, as well as the lifetime benefit maximums. There may be differences in how the companies calculate the inflation on the lifetime maximum benefit if there have been claims filed and benefits used during the life of the policy. Agents must read the policies carefully and fully understand the method used so they can explain it to their clients.
In most LTCI policies, automatic inflation increases continue for the life of the policy. However, a few policies have limitations. Some impose a cap on benefits of double the original amount, and others stop automatic increases after 20 years or when the insured reaches a specified age (such as 80 or 85). An automatic inflation protection option generally also increases a policy’s lifetime maximum benefit.
Types of Inflation Protection
There are three basic approaches to inflation protection – two are automatic and the third is optional.
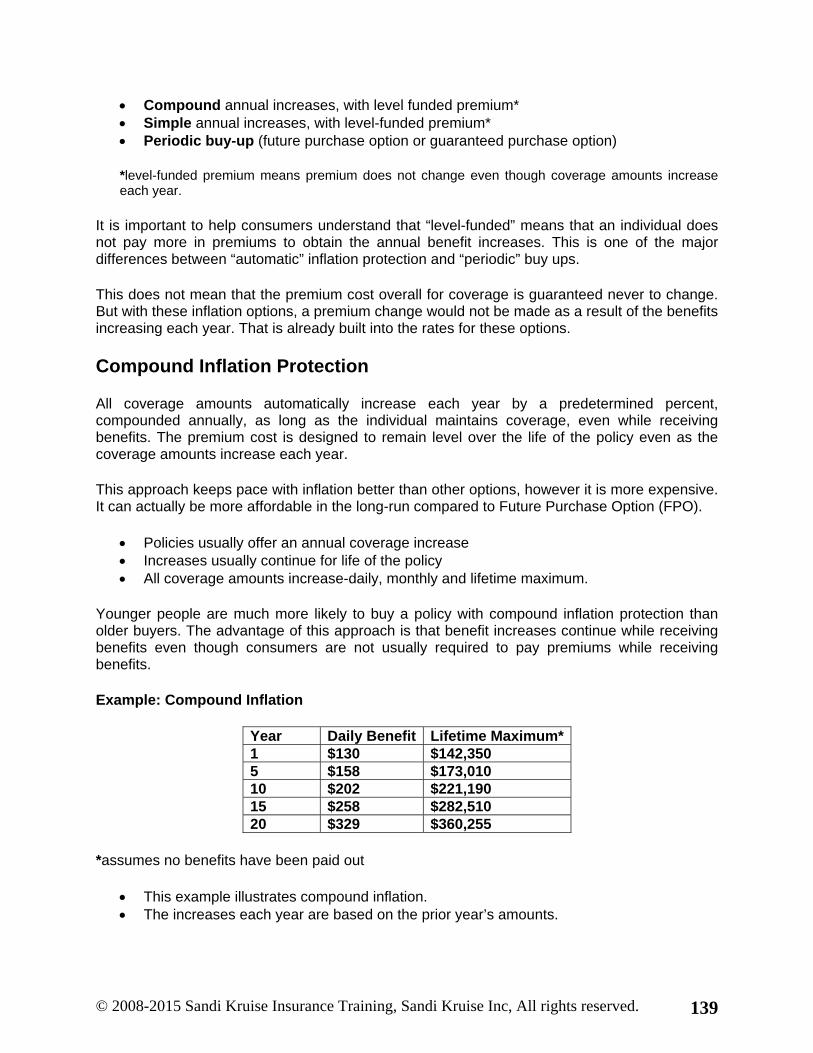
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 139
Compound annual increases, with level funded premium* Simple annual increases, with level-funded premium* Periodic buy-up (future purchase option or guaranteed purchase option)
*level-funded premium means premium does not change even though coverage amounts increase each year.
It is important to help consumers understand that “level-funded” means that an individual does not pay more in premiums to obtain the annual benefit increases. This is one of the major differences between “automatic” inflation protection and “periodic” buy ups.
This does not mean that the premium cost overall for coverage is guaranteed never to change. But with these inflation options, a premium change would not be made as a result of the benefits increasing each year. That is already built into the rates for these options.
Compound Inflation Protection
All coverage amounts automatically increase each year by a predetermined percent, compounded annually, as long as the individual maintains coverage, even while receiving benefits. The premium cost is designed to remain level over the life of the policy even as the coverage amounts increase each year.
This approach keeps pace with inflation better than other options, however it is more expensive. It can actually be more affordable in the long-run compared to Future Purchase Option (FPO).
Policies usually offer an annual coverage increase Increases usually continue for life of the policy All coverage amounts increase-daily, monthly and lifetime maximum.
Younger people are much more likely to buy a policy with compound inflation protection than older buyers. The advantage of this approach is that benefit increases continue while receiving benefits even though consumers are not usually required to pay premiums while receiving benefits.
Example: Compound Inflation
Year Daily Benefit Lifetime Maximum*1 $130 $142,350 5 $158 $173,010 10 $202 $221,190 15 $258 $282,510 20 $329 $360,255
*assumes no benefits have been paid out
This example illustrates compound inflation. The increases each year are based on the prior year’s amounts.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 140
Example:
With five percent compound inflation, it takes about 15 years for benefit amounts to “double.” For example, if an individual buys a policy paying $100/day today, in 15 years, the benefit will grow to about $200/day.
Simple Inflation Protection
Simple inflation protection is similar to compound inflation protection except for the rate and amount of the annual increase.
Simple inflation means it is a fixed dollar amount increase each year. It is usually based on a percent of the original benefit amount. If an individual buys a $100/day policy, a five percent simple increase only adds $5 of
benefit each year. Continues for life of the policy (usually even while the insured is receiving benefits) Costs less than compound because benefits increase more slowly
Simple inflation increases are reasonably close to the compound inflation increases initially, but do not keep pace with inflation in the long run.
Compound inflation protection better matches the way costs of care increase. But simple inflation protection increases are reasonably close to the compound increases for the first 10 years of coverage. Simple inflation protection may be more appropriate for older buyers who may be closer to needing care than someone who buys coverage in their 40’s or 50’s.
The simple rate option costs less, since in the long run it results in significantly smaller benefit increases. However, during the early years of the policy benefit increases are almost as great as with the compound rate. Therefore, the simple rate option is probably sufficient for a person who is likely to need benefits fairly soon, such as someone who is already elderly when the policy is purchased.
Example: Simple Inflation
Year Daily Benefit Lifetime Maximum*1 $130 $142,350 5 $156 $178,820 10 $188 $205,860 15 $221 $241,995 20 $253 $277,035
The amount of the increase each year is exactly the same as the year before.
*assumes no benefits have been paid out

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 141
Coverage Increases with Compound vs. Simple Inflation Protection
Year Daily Benefit Amount (DBA)
Total Coverage Amount
Compound Simple Compound Simple 1 $130 $130 $142,350 $142,350 5 $158 $156 $173,010 $178,820
10 $202 $188 $221,190 $205,860 15 $258 $221 $282,500 $241,995 20 $329 $253 $360,255 $277,035
Guaranteed Purchase Option
Another kind of inflation protection is the guaranteed purchase option (GPO) (also called the future purchase option or FPO). This feature gives the insured the right to purchase additional coverage to keep up with rising costs. Specifically, at set intervals (such as every year or every three years), the insured has the option of increasing benefit amounts. He does not have to reapply for coverage and submit evidence of insurability, as he would without the guaranteed purchase option. If an insured does increase his benefits, his premium is also increased. The increase in premium is based on the amount of the benefit increase and new premium amount is based on the existing premium amount plus the premium for the new additional benefit amount. The new benefit amount increment is priced based and on the policyholder’s attained age at the time of the change.
The guaranteed purchase option is included in some policies at no additional cost. Under some policies the insured pays a higher premium simply to have this option, whether or not they ever use it to raise benefits.
A policy with a guaranteed purchase option usually has a lower premium than a comparable policy with automatic inflation protection. But the GPO inflation protection usually does not work well for those buying a policy when they are relatively young. Many years of increasing the benefit amount enough to keep up with inflation requires larger and larger premium increases, eventually making the policy unaffordable. The 5 percent automatic inflation protection option, on the other hand, gives the insured a known, budgetable premium.
In addition, the GPO is subject to certain limitations. If an insured declines a certain number of opportunities to increase coverage, most insurers stop offering them. And an insurer generally makes no further increases available after the insured becomes eligible for benefits.
For those who buy their coverage 20, 10 or even 5 years before they use it, the benefit amount they choose will almost certainly be too low to cover the increased costs of care. That’s why most plans offer inflation protection.
Future Purchase Options (FPO)
This option (also called Benefit Increase Option, Guaranteed Purchase Option, or CPI Increase) allows consumers to buy additional coverage amounts on a periodic schedule, to keep benefits in step with the rising costs of care. Generally, every two or three years, the insurance company

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 142
will offer their members an opportunity to purchase additional coverage at an additional premium cost without having to provide proof of insurability. With this approach, they would pay an additional premium cost every time they choose to accept the offer of additional coverage.
The FPO is the predominant approach to inflation protection in the employer group market. However, a growing number of employer-sponsored LTC insurance programs now also an offer of compound inflation protection.
A Future Purchase Option allows people to choose to increase their benefits periodically, such as every second or third year. Each time they buy additional coverage, their premium will go up. If they accept the option regularly and haven’t become eligible for benefits, they don’t have to show proof of good health.
However, if they decline the option a certain number of times — even once with some plans — they may have to provide medical information satisfactory to the insurance company to have access to the inflation increases again.
The initial premium is lower under this option, but it will increase significantly if the insured accepts a number of these inflation offers.
Periodic Benefit Increase vs. Automatic Inflation Protection
$27 $32 $39 $48 $62 $82 $111 $154
$220
$321
$474
$706
$0
$100
$200
$300
$400
$500
$600
$700
$800
Plan Purchased at age 45 Plan Purchased at age 65
Mon
thly
Pre
miu
m
45 48 51 54 57 60 63 66 69 72 75 78 Age
$400
$105
$285
$208 $159
$126
$0
$50
$100
$150
$200
$250
$300
$350
$400
$450
65 68 71 74 77 80 Periodic Benefit Increase Option Built-in Inflation Protection Option
Age
How FPO Works
Every two or three years, the insurer offers additional coverage amounts. The additional coverage might be a flat dollar amount (e.g., $10 to $25) or might be a
percentage increase over the existing coverage amounts (e.g., 5 percent per year since the last offer.
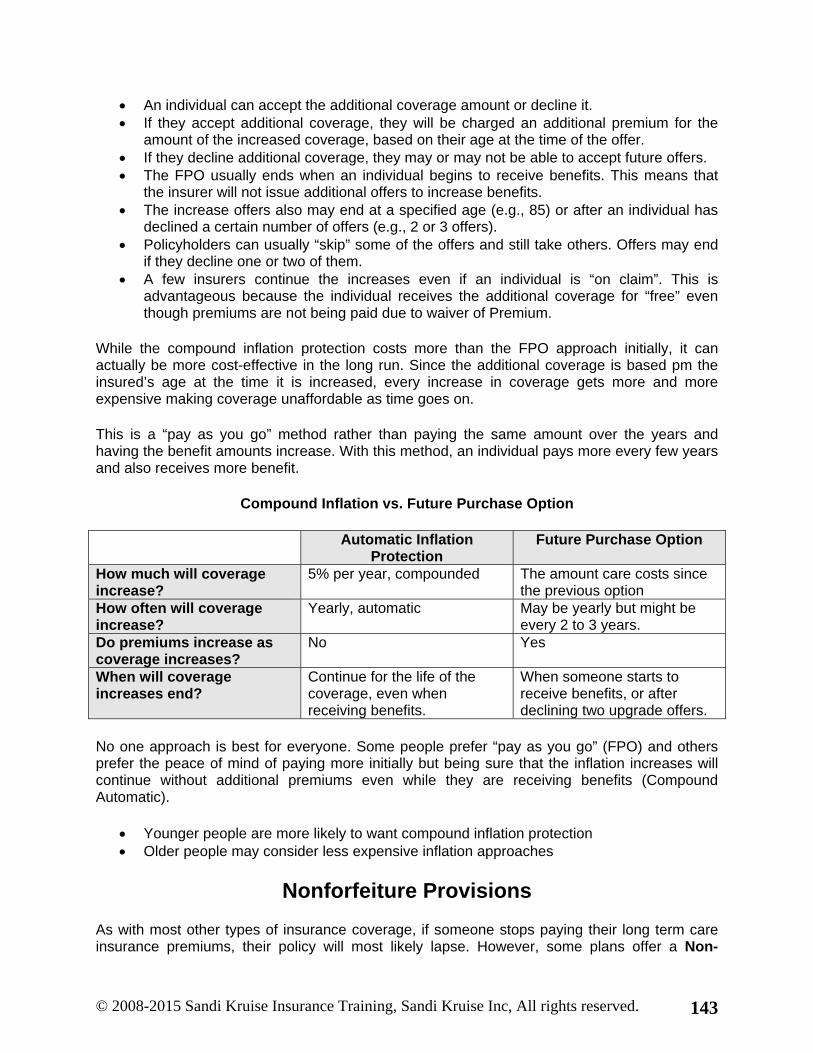
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 143
An individual can accept the additional coverage amount or decline it. If they accept additional coverage, they will be charged an additional premium for the
amount of the increased coverage, based on their age at the time of the offer. If they decline additional coverage, they may or may not be able to accept future offers. The FPO usually ends when an individual begins to receive benefits. This means that
the insurer will not issue additional offers to increase benefits. The increase offers also may end at a specified age (e.g., 85) or after an individual has
declined a certain number of offers (e.g., 2 or 3 offers). Policyholders can usually “skip” some of the offers and still take others. Offers may end
if they decline one or two of them. A few insurers continue the increases even if an individual is “on claim”. This is
advantageous because the individual receives the additional coverage for “free” even though premiums are not being paid due to waiver of Premium.
While the compound inflation protection costs more than the FPO approach initially, it can actually be more cost-effective in the long run. Since the additional coverage is based pm the insured’s age at the time it is increased, every increase in coverage gets more and more expensive making coverage unaffordable as time goes on.
This is a “pay as you go” method rather than paying the same amount over the years and having the benefit amounts increase. With this method, an individual pays more every few years and also receives more benefit.
Compound Inflation vs. Future Purchase Option
Automatic Inflation Protection
Future Purchase Option
How much will coverage increase?
5% per year, compounded The amount care costs since the previous option
How often will coverage increase?
Yearly, automatic May be yearly but might be every 2 to 3 years.
Do premiums increase as coverage increases?
No Yes
When will coverage increases end?
Continue for the life of the coverage, even when receiving benefits.
When someone starts to receive benefits, or after declining two upgrade offers.
No one approach is best for everyone. Some people prefer “pay as you go” (FPO) and others prefer the peace of mind of paying more initially but being sure that the inflation increases will continue without additional premiums even while they are receiving benefits (Compound Automatic).
Younger people are more likely to want compound inflation protection Older people may consider less expensive inflation approaches
Nonforfeiture Provisions
As with most other types of insurance coverage, if someone stops paying their long term care insurance premiums, their policy will most likely lapse. However, some plans offer a Non-

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 144
forfeiture Benefit. A Non-forfeiture Benefit provides protection for those who cancel coverage. There are two types of nonforfeiture benefits.
Optional Nonforfeiture Provision (NFO)
A nonforfeiture option (NFO) is a policy provision which individuals can add to their LTC coverage for an additional premium. It provides a continuation of coverage, on a limited basis, in the event that an individual ceases paying premiums resulting in a lapse in coverage. This limited amount of additional coverage might give time to make “transition plans” for how to pay for continued care needs if the coverage has lapsed due to non-payment of premium and if the individual does not wish to reinstate the coverage.
Individual, tax-qualified policies are required to offer each applicant this nonforfeiture provision. Group policies may offer nonforfeiture to the sponsoring policyholder (e.g., employer) who can decide whether or not to include a NFO.
Most NFOs provide coverage equal to 30 times the nursing home daily benefit amount, or 100 percent of premiums paid to date at the time an individual stopped paying premiums and lapsed in coverage. This would provide about one month’s worth of continued coverage, or more, depending on the amount of premiums paid to date. Generally, a policy must be in-force for at least 3 years before the nonforfeiture provision applies.
Example:
Assume Jane’s premiums are $1,200/year. Jane has maintained her coverage for 5 years. Her current nursing home daily benefit amount is $150.
If Jane lets her coverage lapse by not paying premiums anymore, the value of her nonforfeiture benefit (assuming she had chosen to include this optional feature in her coverage initially) is:
The greater of $1,200 x 5 years = $6,000 or 30 x $150/day = $4,500
Contingent Nonforfeiture
Newer policies automatically include, at no charge, a Contingent Nonforfeiture benefit. This provides the same protection as the nonforfeiture option described above, except that it is triggered by a “substantial increase” in premiums, which causes someone to stop paying premiums. There is generally a state-mandated schedule defining the amount of the premium increase that is considered “substantial” enough to trigger the contingent nonforfeiture benefit. The amount of benefit is the same as described above – the greater of 30 times the daily benefit amount or 100 percent of premiums.
A growing number of states require LTC policies to include a Contingent Nonforfeiture Benefit. Many LTC policies include such a provision even where state law does not require it, simply to provide the same level and type of coverage in all states.
The schedule of “substantial premium increases” by age, which would trigger this benefit, is shown below.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 145
Triggers for a Substantial Premium Increase
% Increase Over % Increase Over % Increase Over Issue Age Initial Premium Issue Age Initial Premium Issue Age Initial Premium <29 200% 64 54% 75 30% 30-34 190% 65 50% 76 28% 35-39 170% 66 48% 77 26% 40-44 150% 67 46% 78 24% 45-49 130% 68 44% 79 22% 50-54 110% 69 42% 80 20% 55-59 90% 70 40% 81 19% 60 70% 71 38% 82 18% 61 66% 72 36% 83 17% 62 62% 73 34% 84 16% 63 58% 74 32%
Helping People Decide
If a policy includes a contingent nonforfeiture option, or if the policy allows an individual to decrease coverage in the event of a rate increase, then the additional protection of an optional nonforfeiture provision is very limited. It adds to the policy cost without providing significantly additional “protection” beyond what is already provided. The best strategy is to help consumers select a policy that they can continue to afford over time.
The Elimination Period of a Long-Term Care Insurance Policy
Usually, when a person covered by an LTCI policy meets a benefit trigger, they do not immediately begin to receive benefits. They must first satisfy an elimination period (sometimes called a “waiting period” or “deductible”). The elimination period functions like a deductible in other forms of insurance. It is designed to reduce an insurer’s benefit and administrative costs and thereby enable the insurer to offer a lower premium.
Benefits are paid after an elimination period has elapsed. This is the amount of time that must pass after a benefit trigger occurs but before they begin to receive payment for services. An elimination period is like the deductible they have on their car insurance, except it is usually specified as a period of time rather than a dollar amount. During the elimination period, they may have to pay for services themselves or other insurance, such as Medicare, will pay for some of their care. Some policies only require a benefit trigger and may not require them to receive paid care or pay for services to satisfy an elimination period.
The elimination period or “deductible” refers to the initial time period or amount of expenses incurred before the policy begins to pay benefits. The purpose of an elimination period is to help keep coverage more affordable and focused on care needs.
This does not mean an individual is left without care or support during the elimination period. It means that benefits do not begin on the day that care is needed. Some benefits can be provided even before meeting the elimination period.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 146
Most policies do not require satisfying the elimination period in order to receive Respite Care Benefits or Care Coordination Services. Some policies also waive the elimination period requirement for Hospice Care Services. Otherwise, unless they choose a “zero day” elimination period, they will have to meet this requirement for most other services covered under the policy.
An individual can generally choose the elimination period from several options including: 0, 30, 45, 60, 90, 100, 120, 180, or 365 days. The choices offered vary by insurance company and by state. Most people select a 60 or 90 day elimination period to help keep premiums affordable while still minimizing possible “out-of-pocket” expenses during the elimination period.
The longer the elimination period, the lower the premium will be. However, the longer the elimination period, the more the insured will pay out of pocket if they need care. For example, if an insured chooses a 90-day elimination period and has to pay for nursing home care for 90 days at $150 per day, they will pay a total of $13,500 before beginning to receive benefits. On the other hand, if they choose a 30-day elimination period, they will pay only $4,500. Each individual must weigh paying a higher premium for a short elimination period against paying a lower premium but having to fund care out of her own pocket during a long elimination period.
When the elimination period starts running differs by insurer. For some it starts as soon as the insured meets a benefit trigger, whether he incurs expenses covered by the policy or not. For others it starts only when the insured meets a benefit trigger and begins incurring covered expenses.
Examples
Dave has a 90-day elimination period that begins as soon as he meets a benefit trigger, whether or not he receives any paid services. He meets the policy’s physical impairment benefit trigger, and for 90 days his wife takes care of him and he does not pay for any services. At the end of 90 days, the elimination period is satisfied and he can begin receiving benefits. At that point he obtains paid services.
Margaret also has a 90-day elimination period, but hers does not begin until she both meets a benefit trigger and is receiving paid services covered by the policy. Unlike Dave, she must pay for care for 90 days before she can receive benefits.
Judy has a 60-day elimination period that counts only service days. On May 1 she begins receiving home healthcare services three days a week, so that it takes her 20 weeks to satisfy her elimination period.
David has a 60-day elimination period that gives him credit for every day of any week in which he receives covered services on at least one day. On May 1 he begins receiving home healthcare services three days a week. Every day of the week is counted, and he satisfies his elimination period in 60 calendar days.
Elimination Period Accumulation
Most modern policies allow days to be accumulated over the life of the policy. For example, if a person with a 90-day elimination period receives covered services for 70 days but then no longer needs care, the next time he meets a benefit trigger, those 70 days will count toward his

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 147
elimination period and he will need only 20 more days. But under some policies if the insured does not accumulate 90 days within a certain time (such as two years), he loses any days he has and must begin again.
Once in a Lifetime Elimination Period
Under most policies today the elimination period must be satisfied only once during the life of the policy. That is, an insured who satisfies the elimination period, receives benefits, then stops needing care, and after a extended time needs care again is not required to satisfy the elimination period again. But a few older policies require the insured to begin a new elimination period for each episode of care. For these “per episode” policies, generally, if 180 days pass without needing any care, a “new” episode of care will begin along with a new elimination period.
Zero Elimination Period
Some insurers offer the option of no elimination period (called a zero elimination period). Many newer policies offer the option of a zero elimination period for home care combined with a regular elimination period (often 90 days) for facility care. Sometimes under this approach the days on which home care is received are counted toward the facility elimination period, so that if a person receives home care for at least a few months before going into a nursing home, she will have already satisfied her facility elimination period.
Calendar Days or Service Days
Companies that require insureds to receive paid services during the elimination period differ in how they count days toward satisfying the period. Some take the service day approach—they count only the days on which services are provided. Others take the calendar day approach—they count all days while services are received, whether these services are provided every day or not.
It is important to help consumers understand the difference between calendar day and service day because it may result in little or no out-of-pocket expense during the elimination period with calendar day approach.
Service Day
Some policies count each day in which an individual receives specific services that would otherwise be covered under the policy (e.g., each day an individual receives home health care or care in a nursing home). This is called a Service Day Elimination Period.
Service day only counts days in which a covered service is received. A covered service is included in the policy (e.g., nursing home or home care day). A hospital stay is not covered, thus days spent in the hospital do not count as service days.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 148
Calendar Day
Other policies simply count each day someone is “disabled,” whether or not they received any paid care. This is called a Calendar Day Elimination Period.
A calendar day is any day an individual is disabled according to the policy definition (e.g., need help with 2 or more ADLs or have a cognitive impairment). It counts any day on which the insured is disabled (need help with ADLs or have cognitive loss) even if they do not receive any paid service or care
Extra Credit
Some policies use a hybrid approach. “Extra credit” is given by counting all seven days of the week even though the individual may have only used one, two or three days of home care in that same week. This helps satisfy the Elimination Period more quickly. Most policies do not require that the elimination period days be consecutive days of care but allows accumulation of days over a given time period (e.g., one or two years) or indefinitely.
An individual can satisfy the elimination period more quickly if a policy gives “extra credit” which means it might count days more quickly than just counting each day in which a covered service is received. Some policies count the entire week that an individual receives at least a certain number of days of care in that week. This is what “extra credit” means.
Expense During the Elimination Period
Medicare or other insurance might pay some of these expenses, but only if all the conditions for payments are met. Days in which Medicare or other insurance pays will usually still count toward satisfying the elimination period and reduce out-of-pocket costs
Many people prefer the premium savings of a longer elimination period (e.g., 90 days) however consumers must think about how they will pay out-of-pocket for this period. The structure of the elimination period also may make it easier to satisfy. The easiest ones to meet are:
Waiver of Premium (WP)
A waiver of premium feature allows policyholders to stop paying premiums once they are eligible for benefits and have satisfied the Waiting Period. Although most policies include this provision, it may vary from one policy to another.
Some plans waive premiums for nursing home care but not for home care. Others waive premiums in both instances. The insured normally resumes paying premiums if they recover and benefits stop.
Some policies begin premium waiver on the first day in which benefits are received. Other policies begin premium waiver after having received benefits for a certain number of days (e.g., 90 days).

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 149
While newer policies usually automatically include a premium waiver provision, some older policies require that this option be elected for an additional premium. Many policies do not waive premiums if receiving short-term, temporary benefits, such as respite care.
If an individual has paid premiums for a period in advance and then qualifies for “premium waiver,” premiums that have been paid for that period of time, or a credit against future premiums due will be refunded.
Care Coordination
A growing number of policies today include care coordination. These policies not only pay for care, but help people identify the services they need and arrange for care, if desired. Care coordination is not managed care. It is a voluntary, value-added component of many LTC policies.
The goals of care coordination is to help consumers receive the most value from their coverage by identifying appropriate and lower cost care options and to provide valuable support for family caregivers. When the time comes that an individual needs care, often it is difficult to know what to do, what the options are, or where to get help. Care coordination can provide options, answers, guidance, and reassurance. It can also help identify specific providers in the community that can meet an individual’s care needs.
A trained Care Advisor (a nurse or social worker experienced in LTC) meets with consumers by telephone or in person and gathers information about their physical, mental, social, and medical situation.
It is important to understand that care coordination is not managed care. Care coordination is meant to help individuals maximize their coverage and to find their way through the maze of care options at an emotional time. The consumer decides which and how much care to use, up to the benefit limits of their policy.
Care Coordination Approaches Vary
Insurers may both pay for and provide care coordination services, or they may just pay for these services and require consumers to find the “care coordinator” on their own. Many insurers that provide this service have a contract with the national network of care advisors in all parts of the country, so that they can find a trained professional who knows the services and providers in the insured’s area.
Some insurers only have telephonic support for care coordination, provided by a nurse or social workers on their staff in a central location. This type of care coordination is more impersonal when compared to service provided by someone on-site and local who can meet in person to better understand an individual’s care needs.
Sometimes the expenses associated with care coordination are deducted from the Total Coverage Amount (or Maximum Lifetime Benefit). There may be an overall policy limit on how much care coordination an individual can receive (e.g., $5,000 or 10 visits). Most insurers, however, provide and pay for this service without reducing the Total Coverage Amount or limiting the service, as long as the designated network of care advisors is used.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 150
Most people do not think about care coordination when they buy coverage, but it becomes important at the time they need care.
Plan of Care
The Care Advisor suggests a “Plan of Care” based on the specific care needs and family situation. The Plan of Care often suggests specific services and providers, although these suggestions are not “mandatory”. It generally provides the option for care at home or in a facility, depending on individual preferences and circumstances. Finally, the Plan of Care is not put into effect unless the individual and their family are comfortable with it, and it is modified as needs change.
Other Typical Coverage Features
There are a variety of other benefits often included in LTC policies. Most of these are included without additional charge. Most policies include the following:
Bed Reservation
Bed Reservation pays expenses to “reserve” the nursing home or assisted living facility bed while an individual is temporarily absent for a hospital stay or other reason. It is important to advise the insured how many days are covered as well as the conditions for payment.
Caregiver Training
Caregiver Training pays expenses to train an informal caregiver (family member or friend) to safely and appropriately provide personal care or similar services. There is usually a fairly low dollar limit for this coverage.
Informal Caregiver (Family Care)
Some policies pay expenses incurred when family or friends that provide care. Other policies will give cash payment each day an individual is disabled and receives care from an “informal caregiver” even if there are no expenses incurred. Coverage is usually limited to a percent of the total daily benefit and may have a lifetime limit. Since most families do not charge for the care they provide, most people do not incur expenses when they receive informal care.
Alternate Plan of Care
Alternate Plan of Care allows the policy to pay expenses not typically covered by the policy for alternative care or services that may emerge in the future or are unique to a location or situation. This provision helps coverage purchased today keep pace with a rapidly changing LTC service delivery setting. Services that did not exist today and are not written into the policy can still, on a case-by-case basis, be paid for under the policy in the future. The insurer does not “impose” alternate care on individuals – it is an optional feature provided if the insured agreed upon. It does not mean that the insurer will pay for any type of care. They will usually only agree to pay if no additional cost is involved.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 151
International Coverage
Some policies may also include international coverage. This is usually paid for on a short-term basis until an individual can return to the United States.
Coverage Options (Additional Premium Charge)
Return of Premium on Death Benefit
The most common approach is a return of 100 percent of premiums, less benefits paid, if death occurs before age 66. For each year thereafter, the amount of premium returned declines by 10 percent and there is no premium return if death occurs at age 75 or later. A more expensive version of this rider provides a full return of premium on death at any age. The premium return typically goes tax-free (if it is a tax-qualified policy) to the estate.
Return of premium on death is optional benefit. This option often attracts younger buyers or those in the employer market. This option costs more but it is ideal for people worried about losing the value of all their premiums if they end up never needing LTC.
Restoration of Benefits
This feature “restores” the total coverage amount or lifetime maximum to its full original amount even if benefits have been used, as long as the insured goes 180 days without any disability or care following the use of benefits. Since it is unlikely that someone who has used a significant amount of their benefits will recover to the point of being independent for 180 days and then subsequently require care, this benefit provision provides illusory coverage. Restoration of benefits has limited value and is an illusory benefit.
Dual Premium Waiver
This provision provides a waiver of premium for one spouse when the other spouse begins to receive benefits, assuming that both have maintained coverage under the policy for a specified time period (e.g., 10 years).
Surviving Spouse Premium Waiver
Similar to the above, this provides a premium waiver for a surviving spouse when the other covered spouse dies. This makes it easier for a surviving spouse to continue to maintain their coverage even if their financial circumstances may decline after the death of their spouse.
Spouse/Shared Care
This provision allows a married couple (or domestic partners) to share either an additional coverage amount or the entire amount of coverage they each have. This helps a couple obtain coverage in light of the uncertainty about which of them will need care and for how long.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 152
Consumer Protection Provisions
These are based on the Model Regulations and Model Act of the National Association of Insurance Commissioners.
The following important provisions are required in any tax-qualified LTC policy. Most states require these provisions in all LTC policies as well:
Guaranteed Renewable
Coverage can never be cancelled by the insurance company, nor can they refuse renewal, as long as an individual continues to pay premiums and the maximum benefit under the policy has not been exhausted.
Free-Look Period
Generally, a 30-day period following the receipt of the policy during which an individual may return it for any reason for a full refund of any premiums paid.
Third-Party Designee
An individual has the right to designate another person to receive notice of premiums due and payments missed so that a premium will not be accidentally missed if an individual is ill, traveling, or for any other reason.
Grace Period
An individual has up to 65 days after the date that the premium payment is due to make that payment. Coverage cannot be cancelled for non-payment until after the grace period has expired and until after the “third party designee” has also been notified.
Added Protection against Lapse (Extended Reinstatement)
If coverage lapses for non-payment of premium because the insured is “disabled” at the time (e.g., functional loss or cognitive impairment), they can automatically restore coverage if this is done within 5 months of the missed premium due date.
Conversion & Continuation of Group Coverage
Most group policies continue unchanged if an individual leaves the group but wants to maintain his or her coverage and “take it with them.” There is usually no change to the premium or the coverage. Some policies allow “conversion” to the same coverage on an individual basis. Premiums that were being paid through a means that is no longer available due to leaving the group (e.g., payroll deduction from a former employer), can be switched to being billed directly. A spouse insured through an employer group plan, maintains coverage even if there is a divorce and no longer married to the covered employee.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 153
Limited Right to Change Premiums
No insured can be singled out for a premium increase. Insurers can only raise rates if it is justified based on the experience of an entire class of insureds (e.g., all residents of a state in a given age with the same policy form and coverage type). Rate increases must be filed with and approved by the State Department of Insurance.
Right to Appeal or Reconsideration
If someone is denied coverage or benefits, they can appeal the decision and ask that it be reconsidered. Insurers have various levels of appeal, sometimes including an outside third-party, administrative law judge, arbitration, or other method.
Right to Increase Coverage or Acquire New Benefits (Step-Up)
An individual can apply to obtain new benefits or increase coverage. This is generally subject to underwriting (review of their health). An additional premium will be paid for the amount of the new benefits, but often this is a “blended rate” that gives credit for having been insured in the past from a younger age. This approach is a better approach than requiring an individual to drop existing coverage and to take out a new policy with the increased coverage or new benefits. This type of change would take place within an insurance company, not from one company to another.
Right to Decrease Coverage (Step-Down)
Many policies allow insureds to decrease coverage if they are interested in a more affordable premium or if circumstances change and different coverage is more appropriate. Many policies also offer this option automatically if there is a rate increase.
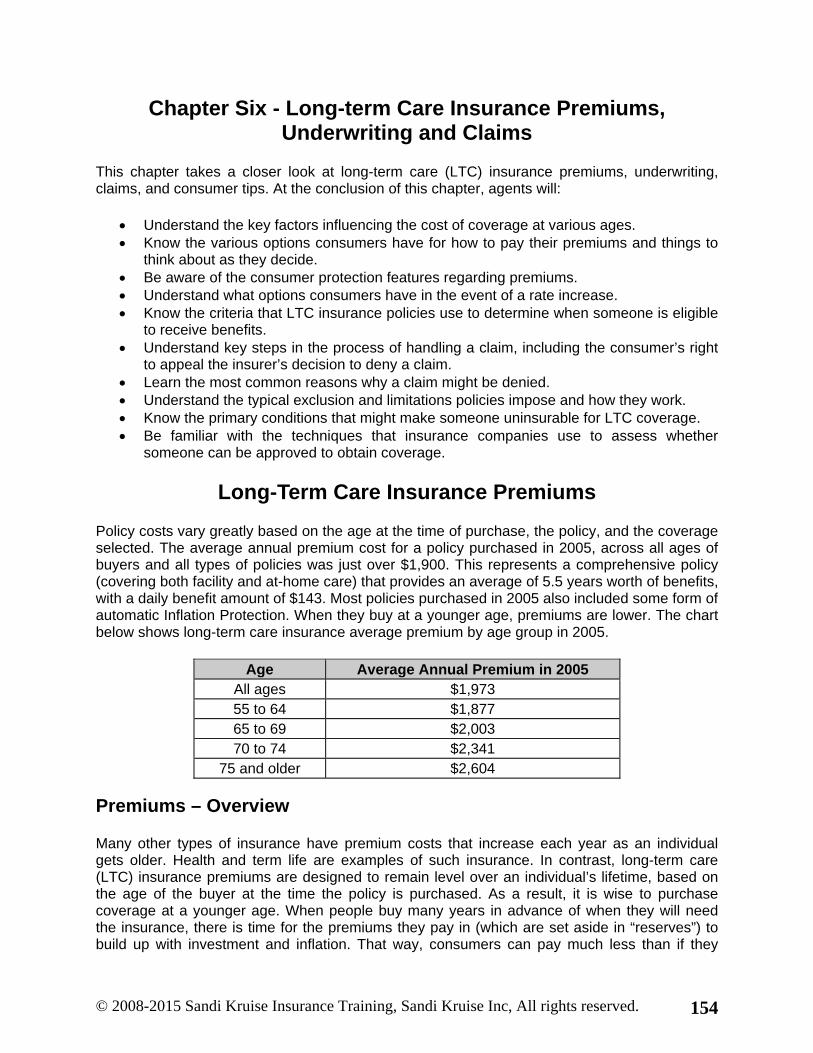
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 154
Chapter Six - Long-term Care Insurance Premiums, Underwriting and Claims
This chapter takes a closer look at long-term care (LTC) insurance premiums, underwriting, claims, and consumer tips. At the conclusion of this chapter, agents will:
Understand the key factors influencing the cost of coverage at various ages. Know the various options consumers have for how to pay their premiums and things to
think about as they decide. Be aware of the consumer protection features regarding premiums. Understand what options consumers have in the event of a rate increase. Know the criteria that LTC insurance policies use to determine when someone is eligible
to receive benefits. Understand key steps in the process of handling a claim, including the consumer’s right
to appeal the insurer’s decision to deny a claim. Learn the most common reasons why a claim might be denied. Understand the typical exclusion and limitations policies impose and how they work. Know the primary conditions that might make someone uninsurable for LTC coverage. Be familiar with the techniques that insurance companies use to assess whether
someone can be approved to obtain coverage.
Long-Term Care Insurance Premiums
Policy costs vary greatly based on the age at the time of purchase, the policy, and the coverage selected. The average annual premium cost for a policy purchased in 2005, across all ages of buyers and all types of policies was just over $1,900. This represents a comprehensive policy (covering both facility and at-home care) that provides an average of 5.5 years worth of benefits, with a daily benefit amount of $143. Most policies purchased in 2005 also included some form of automatic Inflation Protection. When they buy at a younger age, premiums are lower. The chart below shows long-term care insurance average premium by age group in 2005.
Age Average Annual Premium in 2005 All ages $1,973 55 to 64 $1,877 65 to 69 $2,003 70 to 74 $2,341
75 and older $2,604
Premiums – Overview
Many other types of insurance have premium costs that increase each year as an individual gets older. Health and term life are examples of such insurance. In contrast, long-term care (LTC) insurance premiums are designed to remain level over an individual’s lifetime, based on the age of the buyer at the time the policy is purchased. As a result, it is wise to purchase coverage at a younger age. When people buy many years in advance of when they will need the insurance, there is time for the premiums they pay in (which are set aside in “reserves”) to build up with investment and inflation. That way, consumers can pay much less than if they
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 155
began paying into the policy for coverage much closer to the time that care is needed. Long-term care insurance premiums are also designed to remain level even as people age and begin to need care so that people will not face prohibitively unaffordable premium increases precisely at the time when they most need to maintain and use their coverage.
Rate Increase – History
Although LTC premiums are designed to remain level, there have been rate increases on some policies, especially the earlier policies.
Poor underwriting or pricing assumptions that ultimately proved to be too optimistic are the primary reasons.
Most of the leading companies have had little or no rate increases.
Consumer Protection – Rate Stability Guidelines
Most insurers have not raised rates on existing coverage. However, since some insurers have had sizable rate increases, “rate stability” is an important area of concern for consumer protection.
The NAIC 2000 rate setting guidelines provide new standards for setting rates and make it more difficult for insurers to raise rates in the future.
Growing numbers of states adopted these new requirements. Many insurers follow these rules in all states, even though it is not required.
Lapse Rate
A lapse is the cancellation of coverage due to the non-payment of premiums. Lapse rates can be an important component of the pricing of long term care insurance plans. Consumer advocates and regulators fear that some insurance companies will sell policies to people who are probably not good candidates for purchasing the insurance and count on them to lapse their coverage.
By doing so, an insurance company has received premiums for a period of time but no longer faces the risk of paying out benefits. Use of a high lapse rate assumption in setting premiums can result in a lower-priced product and the use of a low lapse rate assumption in setting premiums can result in a higher-priced product.
Industry experience has shown that actual lapse rates for group long term care insurance products have been extremely low. While individual long term care insurance lapse rates appear to reach levels between 3% and 4%, the group long term care insurance lapse rates are generally in the 2% range. This has caused insurers to raise rates on many of the original policies, sometimes more than doubling the premium.
Consumer Protections
The following rules apply to all long-term care insurance policies:

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 156
Coverage cannot be cancelled or nonrenewed as long as the insured continues to pay premiums as they are due and have not used up the maximum policy benefits.
They have 30 days after receiving the policy to return it for a full refund. They have the right to designate another person to receive notice of premiums due and
payments missed so they won't accidentally miss a payment. They have up to 65 days after the date a premium payment is due to make payment.
Coverage cannot be cancelled for non-payment until after the grace period and until the “third party designee” has also been notified.
If coverage lapses for non-payment because the insured was “disabled” at the time, they can restore coverage within five months of the missed premium due date.
Those who have a group policy through their employer or association, can continue that coverage, unchanged, if they leave the group but want to maintain the policy.
A spouse insured through an employer group plan may maintain coverage even after a divorce.
LTC premiums are designed to remain level over the lifetime of the coverage, and are based on their age when they first buy the policy. The insurer can change rates on a group (or class) basis, but have only a limited right to do so, and the change must apply to an entire group or class. Someone cannot be singled out for a rate increase.
In most states, rate increases must be filed with and approved by the State Department of Insurance. Many states have adopted regulations that make it very difficult for an insurer to obtain approval for a rate increase.
Partly due to the way some companies have priced their products, rate increases have been made on some policies. Consumers should examine the history of rate increases made by companies they are interested in.
The National Association of Insurance Commissioners (NAIC) model guidelines were designed to ensure premium stability. The purpose of the NAIC guidelines is to avoid or limit the need for future rate increases.
Once insured, their premium will not change because they get older or their health changes or for any other reason related solely to the insured. Their premiums may only increase if they are among a group of policy holders whose premium is determined to be inadequate.
If the insured elects an increase in their benefits (such as with the Future Purchase Option), their premium would also increase. It is important to explain, while premiums are designed to remain level, rates can increase on a class basis. While the vast majority of insurance companies have not raised rates, they also cannot guarantee that they will not do so in the future. Some have imposed premium increases, but the right of insurers to raise rates after a buyer has taken out a policy is limited. The circumstances under which they can typically raise rates are:
The increase is actuarially justified based on claims experience for an entire class of insured individuals. A class refers to a group of individuals with the same characteristics, such as age, geographic location, and similar coverage.
No one person can be singled out for a rate increase based on age or health.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 157
The increase must be approved by the State’s Department of Insurance, or DOI (most states require this, but not all).
Most insured blocks have never had a rate increase. Rate increases among the top eight insurers (representing about 80 percent of covered lives) have been modest and infrequent.2 Some of the earliest experience with rate increases emerged because of poor underwriting practices or deliberate under-pricing to gain market share. Insurance companies today understand the importance of careful underwriting to ensuring rate stability and, therefore, invest in the time and technology necessary. Studies suggest that insurers, for the most part, are pricing correctly with respect to mortality and morbidity experience. In fact, claims experience for insurers who have invested in the time and technology to underwrite correctly has been better than expected, overall.
More recently, however, there has been concern about insurers’ assumptions about policy lapse rates and interest rates. Premium increases could be necessary if insurers’ assumptions about lapse rates prove incorrect. Even small differences between actual and expected rates on these critical assumptions are important. With the current downturn in the economy and lower interest rates, these concerns become even more important.
To address these important concerns, the National Association of Insurance Commissioners (NAIC) has adopted model “rate stability” guidelines, which do the following:
Require insurers to disclose to prospective buyers any prior rate increases they have made;
Make it more difficult for insurers to obtain a rate increase, including imposing fines and penalties, as a means of encouraging more conservative assumptions for initial pricing; and,
Require insurers to certify that their premiums will be adequate under “moderately adverse” circumstances.
While the newest generation of LTC products may offer consumers somewhat higher premiums than previous products, these provisions are designed to give consumers more confidence in the rate stability behind those premiums.
Coping with a Rate Increase
What options do consumers have if there is a rate increase? It depends on the administrative practices of the insurer and on provisions in the policy. Some policies will describe some of the options consumers have in the event of a rate increase. Other policies may not include such language but still might offer those options at the time of the increase. The first thing consumers should do, then, is to
check the policy and (2) call the company to ask if the following options are available:
2 Changes in Long-Term Care Industry: No Cause for Alarm. Kiplinger’s Retirement Report. June 2000.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 158
Contingent Nonforfeiture
Contingent nonforfeiture was more fully described in another chapter. This provision offers a limited amount of coverage in the event of lapse, even if consumers do not wish to continue to maintain their coverage.
Nonforfeiture Option
This optional feature provides similar (limited) coverage if a consumer chooses to drop the policy rather than accept the rate increase.
Decrease Coverage (Step-Down Provision)
Some policies allow a consumer to decrease coverage in return for keeping the premium affordable. For example, consumers might reduce the daily benefit amount or shorten their lifetime maximum coverage to offset the amount of the premium increase. Certain changes may be more appropriate than others given the consumer’s situation and preferences.
Cancel Policy & Replace
If, however, the consumer does not want to accept the rate increase under any circumstances, and does not want to exercise any other options available with the current insurer, then it may be advisable to seek alternative coverage. This should be a last resort strategy and it is critical that, before consumers drop coverage, they determine the following:
Whether they are still insurable. The cost of new coverage at their current age.
It is important to advise the insured not to drop existing coverage until they are approved for an acceptable level of alternative coverage.
Factors Impacting Premiums
Consumers usually need help selecting coverage features that they can afford. In order to help them, it is important to understand what types of coverage options are most desirable and appropriate for each client based on their particular needs. There is no such thing as a “one size fits all” LTC policy. Some people want very comprehensive coverage (e.g., lifetime coverage that pays for home care at 100 percent of the nursing home daily amount) and others are comfortable with paying some costs out of pocket, if as a result the premiums are more affordable. For this type of consumer, a 50 percent or 75 percent home care benefit and a shorter lifetime coverage amount (e.g., “3 years” or “5 years”) may make sense. Also, someone who expects to have family or friends who are willing to help supplement the care available under their policy may want to select less “comprehensive” coverage.
In states that have partnership policies, agents may find these special policies may help more people to afford coverage.
Some coverage features have a significant impact on premium cost while others do not. Consumers trying to decide on coverage should think more about the features that are

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 159
significant in driving costs up, rather than about those that impact costs less. Also, if a feature does not add significantly to the premium cost (e.g., restoration of benefits rider), then it probably does not add much value in terms of coverage. It is important for consumers to think twice about some of these “bells and whistles” to determine if they are really worth the additional premium cost.
Features with greater impact: Features with less impact:
Comprehensive vs. Facility Only Home care benefit amount Inflation protection Lifetime maximum Daily benefit amount Nonforfeiture
Return of premium on death Deductible Restoration of benefits Spousal benefits
Knowing which features have the greatest impact on rates is helpful if consumers are asking the agent’s help in structuring coverage with desirable features while keeping premiums affordable. Looking at alternatives within these features can help consumers come to a comfortable premium and coverage amount. For instance, choosing a nursing home benefit that pays 80 percent of the daily costs of care instead of 100 percent can save 20 percent in premium costs.
Premium Impact: 50% vs. 100% Home Care
Age 100% 50% Difference 45 $144 $114 +26% 55 $168 $133 +26% 65 $233 $19 +23% 75 $404 $339 +19%
This illustrates how benefit amount impact premiums at different age.
A 20 percent reduction in premiums is an important difference to consider, and a 50 percent home care benefit may still be a reasonable benefit amount.
Premium Impact – Daily Benefit
Age $100/day $150/day Difference 45 $144 $215 +49% 55 $168 $251 +49% 65 $233 $350 +50% 75 $404 $605 +50%
Choosing a slightly lower daily benefit amount ($100 instead of $110) is a good way to reduce premiums. For each 1 percent reduction daily benefit, there is generally a 1 percent reduction in premiums that choosing a $150/day nursing home benefit, instead of a $100/day benefit, increases premiums about 50 percent.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 160
Premium Impact – Lifetime Maximum
Age Lifetime “3 years” Difference
45 $144 $83 +73% 55 $168 $100 +67% 65 $233 $146 +60% 75 $403 $268 +50%
The difference in cost between “lifetime/unlimited” coverage and a “3-year” benefit maximum is about 65 percent, depending on age.
Premium Impact – Inflation Protection – 5% Comp. Periodic
Age Automatic Additions Difference 45 $144 $38 +282% 55 $168 $59 +184% 65 $233 $112 +108% 75 $404 $262 +54%
The feature that most significantly impacts premiums is inflation protection. Impact on premiums (e.g., inflation protection) may depend on issue age. At age 55, including 5 percent compound automatic inflation protection almost doubles premium costs, compared to a plan with only periodic upgrades for inflation. At age 75, the increase is about 50 percent.
Premium Impact – Deductible
Age 30 days 90 days Difference
45 $168 $144 +17% 55 $199 $168 +19% 65 $281 $233 +21% 75 $491 $404 +22%
This chart only shows only two of the many other options available.
Premium Impact – Spousal Benefit
Age Without With Difference 45 $144 $165 +15% 55 $168 $193 +15% 65 $233 $268 +15% 75 $403 $464 +15%
Features that have a smaller impact on premiums include the elimination period amount (about 20 percent difference for 30 days versus 90 days) and spousal benefits, such as surviving spouse premium waiver (15 percent) or a shared care rider (8 percent).

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 161
Premium Impact – Shared Care
Age Without With Difference 45 $104 $113 +8% 55 $125 $135 +8% 65 $180 $195 +8% 75 $327 $353 +8%
The shared care feature has a smaller impact on premiums of about 8 percent.
Long-Term Care Insurance Premium Options
Insurers offer different payment options. With most policies, people pay premiums according to a schedule selected (monthly, quarterly, semi-annually or annually). They may be able to have the premium automatically withdrawn from their bank account, pension check, or paycheck (if they obtain coverage through their employer). Typically people pay premiums until they begin to receive benefits. Then premiums are waived as long as they continue to receive benefits.
With most policies, people pay premiums as long as they are not receiving benefits. However, with some policies they pay premiums only for a specified period – most often 10, 15, or 20 years. For example, with the 20-year option, they pay a monthly premium for 20 years and then their coverage is fully paid up. If they begin to receive benefits before the 20-year pay period is over, they stop paying premiums while they are receiving benefits. If they recover and have not yet paid in for all 20 years, they resume payments. With some policies they only pay premiums until age 65.
A few companies offer a “Single Pay” option, in which clients pay for the insurance in one lump sum payment. While they are more expensive than traditional long-term care insurance, the advantage is that the single lump sum payment is the only premium required. These policies typically pay for long-term care expenses and also offer the option to include a death benefit for their heirs. Some states do not allow single-pay policies.
Most policies are designed to be “lifetime payment”. This means that consumers continue to pay premiums until they begin to receive benefits. Premiums are waived as long as they continue to receive benefits.
Some policies offer “limited pay” options. In this case, consumers pay premiums for a limited amount of time. The amount of each payment is higher, but it is possible for consumers to “pay up” before they would begin to receive benefits.
The “limited pay” options are:
Paid up at age 65. The consumers continue to pay premiums until age 65. Consumers who are over age 65 (or close to it) at the time they buy a policy would not have this option.
Twenty (20) Pay. A consumer pays premiums for the first 20 years of coverage. After that, a consumer is fully “paid-up” and no longer needs to pay premiums to keep coverage active. If consumers begin to receive benefits before the 20-pay period is reached, they would also stop paying premiums for the time they are receiving benefits.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 162
However, if consumers recover (and have not yet paid in full), they would have to resume payments.
Ten (10) Pay. This option is the same as the Twenty (20) Pay option, except consumers only pay premiums for 10 years.
Five (5) Pay. This option is the same as the Twenty (20) Pay option, except consumers pay premiums for 5 years.
Single Pay. Single Pay is the most expensive option. Consumers pay a single, large premium and are then fully “paid-up.” Consumers never have to pay additional premiums to maintain coverage.
The primary attraction of the limited pay policies is that they may limit consumers’ exposure to possible future rate increases. Once a consumer is “paid-up”, the insurance company cannot charge any additional premiums for coverage. (Agents should check the wording carefully in the policy since some insurance companies reserve the right to charge the consumer an additional premium in the event of a rate increase, even with a “paid-up” policy.)
The disadvantage of limited pay policies is that they cost much more than the amount a consumer would likely pay over a lifetime for a lifetime pay policy. In addition, not all companies offer limited pay policies. So, if consumers want to purchase a limited pay policy, they may have less choice. Some states are concerned about “limited pay” policies because they offer significantly higher sales commissions. States fear that agents may push these types of policies on consumers so that they can increase their commission.
Consumers should not select their policies according to the payment plans available.
It is important that consumers find the best insurance company and policy for them. Only then should they inquire about a limited pay policy. Consumers should also seriously evaluate how they feel about paying more in the short-run to protect against possible rate increases versus the amount and timing of premium costs as they age.
Consumers should think carefully before buying a limited pay policy. It is important for agents to clearly disclose all of the details to consumers if proposing this type of payment plan.
Premium Rate Classes
Some companies charge the same rate for everyone insured. Some have different rate classes based on health status. For instance, some companies have a discounted rate (usually 10-15 percent) for those in a “preferred” (or excellent) health status, while charging a uniform, higher rate for everyone else. Other companies have one rate for everyone, except for those in “substandard” (or poor) health. These policies might charge 20 percent to 100 percent more for people with certain high-risk health conditions.
Another practice is to accept a high-risk applicant, and not charge a higher premium. Instead, the company might limit the coverage the consumer can purchase (e.g., the insurer will only approve the consumer for a 90 day deductible instead of the 30 day deductible the consumer has requested, or the insurer will approve the consumer for 5 years of coverage instead of lifetime coverage). This is called a counter-offer. The insurance company agrees to insure the consumer, but only for a different amount or type of coverage than requested.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 163
Other companies have multiple rate categories: standard rates, preferred rates, and sub-standard rates. Some considerations for a consumer when choosing among companies with different rate classes include the following:
Consumers in less than standard health might find a better premium with an insurance company that does not have a preferred rate. Such consumers might have a lower premium in a plan with one rate for all policy members than if they buy from a company that has preferred rates for which they do not qualify.
Consumers should determine which rate category they qualify before committing to buy a certain policy. If consumers are quoted a preferred or standard rate, but then only qualify for the additional cost of a substandard rate, they might be better off buying from another company.
A health condition that one insurer considers substandard could be considered standard by another. Consumers should always shop around and not pay the added cost of a substandard rate unless it is the only way they can obtain coverage.
Not all companies offer rate classes. Consumers should compare the rates of a company that has rate classes with one that does not. Consumers in average or superior health may pay lower premiums with a company that does not have rate classes than with a company that does.
Preferred Standard and Substandard Categories
Most companies simply make a “yes” or “no” decision about whether an applicant qualifies for insurance coverage. Other companies, however, will identify some applicants as a preferred risk and give them a premium discount. Other companies may issue coverage to someone with some health conditions, which the insurer defines as sub-standard, and charge an additional premium for this person.
Preferred Risks
The criteria that might make someone a preferred risk vary across companies but generally include the following:
No uninsurable conditions No use of mechanical devices Does not require help with instrumental activities of daily living No medical condition with likelihood of progression No tobacco use within the last 1 to 5 years Height and weight within preferred range limitations
Sub-Standard Risk
Similarly, the definition of a substandard risk category varies greatly among the companies that employ rate category. Some companies issue standard coverage to someone with a condition that another company would classify as sub-standard with an added premium charge. Some possible conditions that might cause someone to be rated substandard include the following:
Congestive heart failure, stable and controlled with medication Angina (post-heart attack but stable)

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 164
Fibromyalgia Seizure disorder (well-controlled) Lupus (in remission) Cirrhosis (mild or moderate and controlled on medication) Diabetes (onset less than 35 years or greater than 10 years from first diagnosis) Malignant lymphoma (five years post-diagnosis)
Right to Decrease Coverage (Step-Down Provision)
Many policies allow insureds to decrease coverage if there is a rate increase in order to maintain current premium. Some insurers allow step-down for other reasons as well.
Example:
The insurer raises rates 10%, but the insured can keep the same premium by taking a 10% decrease in nursing home daily benefit (all other aspects of coverage stay the same)
The right to decrease coverage is an important consumer protection. This can be done anytime the insured feels the need to change to a more manageable premium. This is especially important if there is a rate increase so that the insured can maintain some coverage rather than allowing the policy to lapse.
Many insurers are allowing such coverage decreases. Insurers may give a “credit” when calculating the new rate by basing it on age when an individual first obtained coverage, even if it was many years ago.
Premium Discounts
Not Everyone Pays the Same Rate for Coverage
Couple’s Discounts
There are “discounts” for couples (married or domestic partners). Evidence shows that married couples have better claims experience. Discounts provided have some justification beyond just “marketing.”
Helps sell coverage to couples, Reflects lower risk when buyer is married From 10% to 25% or more Retain discount for life of policy Usually when both have policies, but approaches vary
Household Discount
Some insurers offer household discounts.
Group-sponsored discount (5% to 15%)

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 165
Some insurers offer discounts on group sponsored policies.
Sometimes “one price for all” is a more fair way to price coverage since no one group is subsidizing another group.
Underwriting
The purpose of underwriting is to assess the current functional and cognitive abilities of applicants and their risk of future disability. Premiums for an LTC product are based upon accepting individuals who are currently functional, independent, and have reasonable prospects of remaining that way for several years. The goal is to approve as many applicants as possible, while managing the risk effectively so that the premiums that have been established can remain fair and sustainable over time.
Because medical conditions alone often do not relate to a person’s risk of becoming disabled and needing LTC insurance, underwriting for LTC takes into account more than simply the presence or absence of certain medical conditions. The underwriting criteria generally focus on a combination of medical, functional and cognitive conditions or the interaction of conditions, which are known to represent a high-risk for needing LTC.
Criteria can also vary from one insurer to the next. Some insurers decline to offer coverage to people with conditions that are difficult to determine the extent of their illnesses. Other insurers may to look more carefully into applicants’ health conditions and are more likely to accept someone with a given health condition, if that condition is otherwise stable and well managed.
Typical “Uninsurable Conditions”
Some medical conditions will disqualify someone from being accepted into the program because of their usual and predictable progressive course. These conditions include chronic degenerative conditions such as Parkinson’s disease, multiple sclerosis, and dementia. Other medical conditions, such as cancer or heart attacks, may or may not disqualify an individual, depending in large part on other factors. Additional information on medical treatment, physical functioning and cognition is often needed to make a final determination in these situations. Taking the time to obtain additional information often means that the insurance companies can accept someone that they might have otherwise been inclined to decline, based solely on their medical condition. Additional underwriting information is important to benefit both the applicant and the insurance program.
Every insurance company has a list of conditions that the company considers uninsurable. Uninsurable conditions are specific conditions that have a strong predictive value for unstable or failing health and carry an equally strong probability of resulting in significant limitations in one’s ability to carry out activities of daily living (ADLs) in the next 48 to 60 months.9 An uninsurable condition can be a single condition that indicates the current need for LTC, such as an Alzheimer’s-type dementia, or a condition such as Parkinson’s disease that might currently be stable, but where there is a significantly elevated risk of functional decline in the future. Finally, there are also combinations of medical conditions that present an increased risk of future disability, such as a history of poorly controlled diabetes, hypertension and stroke. Insurers

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 166
differ in terms of the conditions that they consider uninsurable. The definition of uninsurable also depends upon whether an insurer offers only one rate class, or if it has a sub-standard risk category. A sub-standard risk category may allow an insurer to take applicants with conditions that another carrier might decline.
Qualifying to Purchase Long-Term Care Insurance
Some conditions mean a person won't qualify for long-term care insurance. However, insurance companies have different standards, so while they may be denied coverage by one company, another might accept them.
The most common uninsurable conditions include:
Currently use long-term care services. Already need help with Activities of Daily Living. Have Acquired Immune Deficiency Syndrome (AIDS) or AIDS Related Complex (ARC); Have Alzheimer’s type dementia, organic brain syndrome and all other forms of
dementia and cognitive dysfunction; Have a progressive neurological condition such as Multiple Sclerosis, Muscular
Dystrophy, Myasthenia Gravis or Parkinson's disease. Have had a stroke within the past 12 to 24 months or a history of strokes or multiple
Transient Ischemic Attacks (TIAs). Have metastatic cancer (cancer that has spread beyond its original site). Height and weight outside “acceptable” ranges; Amyotrophic Lateral Sclerosis (i.e., Lou Gehrig disease or ALS); Diabetes with complications such as renal failure, amputation, severe neuropathy; Use of certain adaptive devices such as a wheelchair, walker, four-pronged or quad
cane, motorized scooter, Hoyer lift or hospital bed.
Other health conditions are evaluated in deciding whether or not someone can obtain the insurance.
Insurers also carefully consider the type and amounts of medication the applicant takes, as this can play an important role in assessing an applicant’s insurability. There are specific medications that are commonly used to treat uninsurable conditions, while other medications may indicate a high-risk level of disease severity or instability. The applicant’s medication history is carefully evaluated during the underwriting process, so it is important that all of the applicant’s medications be listed on their application.
Once someone is accepted for coverage, coverage cannot be cancelled for any reason other than non-payment of premium due or if they have received the policy's maximum benefits. Those who develop one of these health conditions after coverage is effective would be covered for the care needed for that condition.
Underwriting Tools
The decision to accept or decline an applicant is generally made based on information from a variety of sources. In general, insurers will collect more information on older applicants, since they are likely to have more medical and other conditions that must be fully explored before

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 167
making an appropriate decision. The tools that are used to collect underwriting information are as follows:
Application Medical Records (also called Attending Physician Statement) Phone History Interview (PHI) Face-to-Face assessment (F2F)
Application
Some insurers have one application version for all applicants, while others may have different versions based on the age or employment status of the applicant. In general, individual insurance tends to have a “one size fits all” application called a long form. The long form includes a detailed section exploring medical conditions and health history. For employer-group policies, insurers are likely to have a short form or an abbreviated application (a modified guaranteed issue) for employees who are actively at work and under age 65 or 70. In the employer-group market, spouses of employees may also have a more abbreviated application form, but parents and retirees are likely to complete the same long form application that is typically used in the individual market.
Attending Physician Statement (APS)
Insurers do not require a medical exam or laboratory work in evaluating an application for LTC insurance. However, if the applicant has no recent medical records and has not seen a doctor within two years, the insurance company may require the applicant to have a physical exam.
Most insurers request a copy of medical records from an applicant’s primary care physician and sometimes they may also obtain records from one of the applicants’ specialists. Insurers typically request medical records from the past three years, but some review records as far back as five years. Often, the physician records provide additional insight into the stability, nature, and severity of medical conditions. This additional insight may enable insurers to accept someone whom they might otherwise decline. Sometimes the medical records will reveal a medical condition that was not disclosed on the application but which raises an insurability concern. If this happens, the condition would be investigated further before an underwriting decision is made.
The insurer generally pays any expense associated with obtaining medical records. Once they have given their authorization to release their medical information to the insurer, applicants are not required to take any further action. If applicants have not been seen by a physician in the last two years, they may be asked to have a physical exam by a physician of their choosing, the cost of which will be the responsibility of the applicants.
Phone History Interview (PHI)
Many insurers also use a telephone interview as an effective way to verify or clarify information provided on the application. This tool is generally focused on a certain age group (e.g., all applicants age 65 to 74 years may receive a Phone History Interview). This brief interview is conducted by a specially trained nurse and scheduled at a time convenient to the applicant. The nurse will ask questions about medications, medical conditions and the beneficiary’s ability to

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 168
function independently in everyday tasks such as bathing and dressing. The interview follows a structured format and generally requires about 20 minutes.
Face-to-Face (F2F) Interview
The face-to-face assessment takes place in the applicant’s home or other location, if the person’s own home is not convenient. The assessment is essentially a personal interview and it requires about 45 minutes. The interviewer asks the beneficiary about specific medical conditions, medications, and the beneficiary’s ability to function independently in routine tasks such as bathing, dressing, taking transportation, or meal preparation. The assessment also includes a brief memory test to evaluate cognitive abilities and may include some simple medical screening, such as blood pressure readings and weight and height. It is not a physical exam and there is no blood or urine testing required during the in-person interview.
Many insurers use the F2F assessment as a critical underwriting tool for the older age applicants. It has proven to be a very cost-effective tool for identifying high-risk applicants with respect to cognitive or functional loss, who might otherwise be accepted and present early claims. It also helps to more fully evaluate older applicants with multiple medical conditions because of the nature, stability and limited functional impact of those conditions. Without seeing the individual face-to-face, it would be too risky for the insurance company to accept them, based on medical history alone. Including a F2F assessment generally improves the risk pool and increases the acceptance rate.
The chart below shows how these evaluation tools are typically used. Each underwriting tool is described in more detail below.
Applicant Age APS PHI Face to Face Under 65 For specific conditions All applicants For specific conditions 65-74 All applicants All applicants For specific conditions 75 and older All applicants No All applicants
Employer Group Market Underwriting
Different underwriting methods because of younger average age and “actively at work” population
Larger employer plans may be “guaranteed issue” for all employees actively at work Many employer plans are “modified guaranteed issue” with only 2 to 5 underwriting
questions Underwriting may differ for people getting coverage through a sponsoring employer
group (Employer plans may require less or no underwriting) Some employer plans are “short from” applications with 5-10 underwriting questions Most employer plans do not use phone history interview, attending physician statement,
or face-to-face for employees Underwriting for spouses of employees, retirees, and parents generally the same as in
the individual market Underwriting may differ for people getting coverage through a sponsoring employer
group. Employer plans may require little or no underwriting.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 169
When there is no underwriting (called guaranteed issue) there may be limits on the amount of coverage sold and requirements that the person be actively at work (not on leave) when they apply.
Acceptance and Decline Rates
Underwriting acceptance rates vary significantly across insurance companies due to differences in their philosophy and experience, the types of products they market, their target markets (e.g., young applicants versus very old applicants), and their distribution systems (e.g., direct mail, group presentation or direct agent sales). All of these factors significantly influence the risks that will present themselves to insurers, how they evaluate the risk and their acceptance and denial rates.
The chart below illustrates representative industry acceptance rates, although individual company experiences will vary.
Age of Applicant Accept < 65 years 91% - 99% 65- 74 years 79% - 95% 75-84 years 64% - 92%
Source: Long Term Care Group (LTCG) Underwriting Analysis, 2002.
Right to Appeal
Any consumer that is declined for insurance is entitled to know the reasons why. The insurance company may communicate the reasons to the applicant directly or the company may release the information to the applicant’s physician.
Applicants must make the request for an appeal in writing. Any information the consumers can gather to address the request is helpful. Consumers might ask their physician to write a letter clarifying information about their current condition or perhaps provide additional information, which the insurance company may not have evaluated. If the decision to decline the request for coverage was based solely on the application, the consumer might ask for a telephone or in-person interview or provide a copy of medical records so that the insurer has a clear and more complete picture of the consumer’s health.
Consumers are, however, responsible for the costs associated with obtaining any additional medical information that they choose to provide to the insurance company to support the request for reconsideration.
Claims
Long-Term Care Insurance Benefit Triggers
When does a person covered by a long-term care insurance policy receive benefits from the policy? What conditions must be met?

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 170
Policies use objective measures to determine when someone needs long-term care. These are called “benefit triggers.” Most policies use Activities of Daily Living and Cognitive Impairment as triggers for benefits. The policy pays benefits when the insured needs help with two or more of the six Activities of Daily Living or when they have a Cognitive Impairment. Most policies reimburse the costs incurred for covered services up to a pre-set limit. Some policies simply pay a pre-set cash amount for each day that the insured meet the “benefit trigger” whether they receive paid long-term care services or not.
To receive benefits under an LTCI policy, a person covered by the policy (an insured) must meet at least one of certain conditions stipulated in the policy, known as benefit triggers. There are two common types:
Physical (or functional) impairment—the insured’s physical condition prevents them from performing a specified number of activities of daily living (ADLs), basic functions required for a person to take care of themselves.
Cognitive impairment—the insured suffers from a serious cognitive condition such that close supervision is necessary to protect their health and safety.
These benefit triggers are used because they are the most reliable indicators of when someone needs long-term care and because they can be measured in a relatively objective way that leads to a high degree of accuracy and consistency in determinations of eligibility for benefits.
In most cases, after an insured has met a benefit trigger, they must satisfy an elimination period before they can receive benefits.
LTC needs equate with ADL loss and Cognitive loss. Medical need is not a relevant concept when people need LTC. ADL loss and Cognitive loss are also the best measures of LTC need since they are reliably and objectively measured. Criteria for insurance benefits should be objective and reliable rather than arbitrary and difficult to define.
Tax-Qualified (TQ) and Non-Tax-Qualified (NTQ) Plans
There are small differences in the criteria for receiving benefits.
A TQ plan may not pay benefits if someone only needs care for a short time and is expected to recover from the current condition (e.g., if the disability or illness is not expected to last more than 90 days). This is an IRS requirement of all tax-qualified plans. A NTQ plan does not have this requirement. However, remember, that Medicare, health plan or Medicare supplement may pay for short-term, recuperative care. Most LTC needs are not short-term.
Non-tax qualified plans can include “medical necessity” as an additional criteria for receiving benefits, but LTC is not really “medically” related. There are not many situations where someone would have a “medical need” for LTC yet still be able to perform their ADLs, which is the standard used for TQ plans.
Finally, TQ plans must meet a greater number of additional consumer protection standards than those required of TQ plans. Although many NTQ policies also meet these standards, there is no guarantee since they are not required to.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 171
Tax Qualified (TQ) Policies – HIPAA
People need LTC when they cannot perform their everyday ADLs without the help of another person or when they suffer from problems with memory or orientation (defined as cognitive impairment).
The great majority of LTCI policies today are federally tax-qualified (TQ), and TQ policies must meet certain requirements of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) in relation to benefit triggers. All tax-qualified LTC policies use the following criteria for receiving benefits:
Standardized ADLs. HIPAA establishes six standard ADLs (bathing, dressing, toileting, transferring, continence, and eating) and precisely defines them. TQ policies must include at least five of these six and must use the HIPAA definitions. Also, policies must define a physical impairment as the inability to perform at least two of the standard ADLs without substantial assistance from another person.
Substantial Assistance. A TQ policy may define substantial assistance in two ways. “Hands-on” assistance is the physical assistance of another person without which the impaired individual would be unable to perform the ADL. “Stand-by” assistance is the presence of another person within arm’s reach of the impaired individual that is necessary to prevent, by physical intervention, injury to the individual while performing the ADL. For example, if a person cannot wash herself and must be washed by another, she needs “Hands-on” assistance with the ADL of bathing. If, on the other hand, she can take a bath without any help but needs someone there in case she falls getting into or out of the bathtub, she needs only “Stand-by” assistance. A TQ policy may require an insured to need “Hands-on” assistance, or it may require only a need for “Stand-by” assistance, or it may accept either standard, or it may use a more rigorous standard, but it may not use a standard less rigorous than “Stand-by” assistance.
The 90-day Certification Requirement. A licensed healthcare practitioner must certify that the insured’s inability to perform ADLs is expected to last at least 90 days. This provision is required because LTCI benefits are not intended for those unable to care for themselves for a short time while they are recovering from an illness or injury. (Medicare or medical expense insurance generally covers the care of those with temporary conditions.) There is no 90-day requirement for cognitive impairment since such impairments are not usually temporary.
Severe Cognitive Impairment. To qualify for benefits on a cognitive basis, the insured must suffer a severe cognitive impairment such that substantial supervision is needed to protect them from threats to their health and safety. A TQ policy cannot pay benefits for mild disorders such as the increased forgetfulness that often accompanies aging. HIPAA defines a severe cognitive impairment as a loss of or deterioration in intellectual capacity that is comparable to and includes Alzheimer’s disease and similar forms of irreversible dementia and that can be reliably measured by clinical evidence and standardized tests.
Medical Necessity. In the past “medical necessity” was a trigger in many LTCI policies. In the context of long-term care insurance, medical necessity means that a physician determines that a person has a need for long-term care. But this is no longer considered an appropriate way of determining need and may not be a benefit trigger of a TQ policy.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 172
Activities of Daily Living/Cognitive Impairment
Need the help of another person with a specified number of ADLS. The 6 ADLs are: bathing, dressing, toileting, transferring (from bed to chair), maintaining or caring for continence and eating. Needing help refers to both “hands-on” and “stand-by” help (supervision), although some policies may use the narrower requirement of hands-on help only.
Severe Cognitive Impairment. This refers to problems with memory and orientation to person, place, or time. It is measured by objective tools and tests. Alzheimer’s disease is an example of severe cognitive impairment.
Non-Qualified (NTQ) and Older Policies (prior to 1/1/97)
Many non-tax qualified (NQ) policies read very much like TQ policies and often use the same benefit criteria. The fact that most NQ policies cost the same as TQ policies suggests that there is no measurable difference in access to benefits under either.
Medical Necessity
Non-tax-qualified policies are also free to include medical necessity as an additional or alternative benefit criterion. An important point is that adding “medical necessity” to a policy does not really impact access to benefits and it might even “cloud” the issue since it is a poorly defined concept that is not reliably measured.
Medical necessity is an older term that does not correlate well with the need for LTC. If someone has a “medical need” for LTC (e.g., they are paralyzed or have severe movement restrictions due to phlebitis or arthritis), then they are most likely to also be unable to perform their ADLs. Some older policies and policies that are not tax-qualified may use medical necessity as a condition for receiving benefits. It is important to review how that term is defined in the policy and who can evaluate when medical necessity exists. Many people think that medical necessity is determined by the insured’s physician, but the language of the policy may actually give the right to evaluate medical need to the insurance company. Because of these ambiguities, this term is seldom used today and was not included as an appropriate benefit criterion in a federally tax-qualified policy.
Older policies refer to cognitive impairment. The addition of the word “severe” was imposed on tax-qualified plans. Insurers do not define or measure cognitive loss any differently than they did prior to the addition of the word severe. The word is used for consistency only.
Degree of Loss
Most policies have a single threshold for all benefits – typically loss in two or more of the six ADLs or severe cognitive impairment. Some policies may require a higher degree of loss for nursing home benefits (e.g., unable to perform three of six ADLs) than for home care, but that is fairly rare.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 173
Impairment involving 2 vs. 3 ADLs
Care needs are more difficult to anticipate and manage when there are 3 losses because typically, “toileting” is the third loss one experiences when losing ADLs. The insured’s care needs are changed from “scheduled” to “on-demand”.
There is a significant difference in care needs when a beneficiary has two versus three ADL limitations. The chart below shows the nature of care needs at each level. The addition of the third ADL loss – the ability to get to and from and use the toilet on one’s own – is critical in changing the type, frequency and cost of care.
# ADL Impairment
Which ADLs are Lost Nature of Care Needs
2 ADLs Bathing & Dressing Usually the first & second ADLs
Care needs can easily be scheduled. Might need care once a day or less often.
3 ADLs Bathing, Dressing and Toileting Toileting is usually 3rd ADL
Care must be “on demand” as needed several times a day.
Imposing a higher benefit criterion for nursing home benefits probably has little impact on access to benefits since most people in nursing homes already have at least three or more ADL losses or a cognitive impairment. In fact, the average number of ADL losses among nursing home residents is 3.3. However, a policy with a higher threshold for nursing home benefits would not pay for nursing home care if someone only needed help with two ADLs.
Most policies today include all six of the ADLs. If they omit bathing, as earlier policies sometimes did, there is significant impact on access to benefits as it makes it more difficult to access care at home. It is important to be sure that the policy being considered does include bathing as one of the ADLs evaluated.
Some older policies might have a higher ADL threshold for nursing home benefits than for other benefits. This is not really a problem since most people are not in nursing homes unless they have a higher degree of loss.
However, agents should be aware of the higher threshold for nursing home placements if they sell this kind of policy. This is important for someone who needs a more “social placement” in a nursing home when there is only a need for periodic care (2 ADLs). Most likely, the policy would not pay for the cost. A policy that requires impairment in 3 ADLs for assisted living facility care would impose an important limitation on coverage.
Some non-tax qualified or older policies (particularly in California) may include the term “ambulating” to refer to getting around. This term is not an ADL and including it generally does not enhance access to benefits. This is because the ADLs of bathing and dressing already take into account difficulty with getting around. If an individual cannot get to or from the bathroom, or in or out of the tub, the ADL “bathing” would apply. Employing a separate measure for “ambulating” does not add anything to the policy that is not already embedded in the six existing ADLs, unless they require impairment in at least 3 ADLs for assisted living.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 174
Processing Claims
The claims process is easier than most people think. Often, a phone call can start the process and the care coordinator will help the insured and their beneficiary through the process. A claim form may not even be required. Care coordination can begin right away and is not usually subject to the elimination period.
The claims process generally begins with a phone call to a special claims or customer service line the insurance company has specified. Customer service staff may do some “intake” over the telephone to understand the insured’s care needs. The staff may also send the policyholder a claim form and an authorization form to release medical records from a provider that can provide more detailed information about care needs. Some insurers begin the claims process without a claim form, thus minimizing the burden of paperwork on the policyholder. Others assign a care coordinator to help the policyholder with the claims process. In contrast, some insurers require the policyholder complete a claim form to start the process.
The insurer gathers the information it needs to verify if the policyholder is eligible for benefits. The insurer may perform an in-person assessment interview (conducted by a trained nurse or social worker) to learn more about the policyholder’s needs. The person completing the assessment collects information and passes it along to the insurer; they do not make a benefit decision.
Plan of Care
A plan of care is the list of long term care services and care the insured needs, developed by their Care Coordinator or other licensed health care practitioner in conjunction with them and/or their family. It will include the type, frequency, providers and cost of care.
Insurance companies will monitor and reassess their plan of care on a regular basis to ensure it continues to meet their needs and will make changes as necessary. This is usually done at least once every 6 to 12 months and is required for TQ policies.
A plan of care can also address the wide range of additional services available in the community to help them meet their long term care needs. Community-based services include friendly visitor programs, home-delivered meals, chore services, and adult day care centers. These additional services may be reimbursed by long term care insurance. Making use of these free or low cost services can help the insured’s benefits to last longer while still affording a high level of care.
Many insurers offer care coordination consultative services provided by registered nurses to enrollees and their qualified relatives at no additional cost. Under certain circumstances, Care Coordinators can authorize benefits for services and care that are not specifically defined as covered services.
Assignment of Benefits
Assignment of Benefits applies to LTC similar to the way it applies to other insurance. Consumers can request that the provider be paid directly by the insurer so he/she is not “in the middle.”
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 175
Claim Denials
While the experience across insurers may vary, the most common reasons for denying a claim request are:
The condition for which the claim is being made does not meet the definition of ADL or cognitive loss
Policy coverage has lapsed The service is not a covered service There is a duplicate claim for the same event The claim amount exceeds the coverage amounts in the policy
Fewer than 10 percent of claims are denied.
Sometimes people are “frail” and “at risk” and living alone and they or their family want to have a caregiver around “just in case.” In some circumstances, the person might need housekeeping help but not have ADL losses or cognitive loss. While those are important situations to support, they do not qualify for LTC benefits.
If a claim is denied, the policyholder is entitled to know the reason for denial and has the right to file an appeal for reconsideration. It is important for the policyholder to understand the reason for the denial. The policyholders should also be familiar with the language of the policy so that they are aware of the extent of their coverage under the policy.
Incontestability
This policy provision prevents coverage from being rescinded or benefits denied based on false information on the application after a specific time period, usually 2 years after policy effective date. Although insurers are limited in their ability to rescind coverage or deny benefits, it is still very important to answer all questions on the application truthfully and completely. Otherwise, the insurer can deny benefits or cancel coverage under certain circumstances.
Exclusions and Limitations
A policy may identify certain circumstances under which it will not pay benefits even if the policyholder might otherwise qualify for benefits. Most states specify in regulation which exclusions and limitations are allowed. The most common policy exclusions are:
War, felony, riot Attempted suicide Care for which no expense is incurred (provided free) Care provided in a government facility or paid for by workers’ compensation or similar Medicare co-payments and deductibles (tax-qualified plans are not allowed to pay)
These exclusions are fairly common but are not in all LTC policies.
Mental/nervous disorders (does not include Alzheimer’s) Alcohol/drugs
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 176
Care outside U.S. Care provided by family Care paid for under other LTC insurance or health insurance
Mental/Nervous Disorder Exclusion
Mental/nervous exclusions were quite common in older policies, although they were never meant to exclude coverage for Alzheimer’s or similar cognitive impairments. In more recent policies, mental/nervous exclusions generally refer to psychiatric conditions, such as manic depression or schizophrenia, as these conditions are already covered by health insurance and are not “long-term care.”
Five states (California, Texas, Massachusetts, Washington, and Wisconsin) currently do not allow mental/nervous exclusions and many of the leading insurers do not have this exclusion in any state. That does not mean that they will pay for purely psychiatric care, however. It means that if a policyholders need LTC, regardless of whether they also have a mental health condition, their care in a nursing home or at a home (as specified by the policy) will be covered without any exclusion or limitation because of the associated psychiatric condition.
Pre-Existing Condition Exclusion
Unlike older policies, most policies today do not exclude pre-existing conditions. A pre-existing condition is one for which consumers sought medical advice or treatment up to six (6) months prior to applying for coverage. A pre-existing condition exclusion is a limitation on coverage for period of time after it has been issued, but which pertains to a health condition the policyholder had prior to applying for coverage.
The Pre-Existing Condition Exclusions in a policy would limit, postpone or deny coverage if the policyholder requires LTC within the first six (6) months of coverage due to the pre-existing condition. This exclusion might take one of two approaches:
Postpone coverage and not pay for care until after the first 6 months of coverage, if the need for care emerges within the first 6 months and is due to the pre-existing condition. With this approach, coverage would begin in month seven.
Or they might not pay for care related to a pre-existing condition if care needs develop in the first 6 months after the policyholder obtains coverage. Even if the claim extends beyond the first 6 months, it would continue to be excluded with this approach.
The 2nd approach is much stricter than the 1st and is not allowed in most states. In the past longer periods of time were also common (i.e. 12-24 months) however all states now use 6 months. The policy language will generally indicate whether or not such an exclusion is a part of the policy. Some employer group plans that issue coverage without any underwriting might employ pre-existing condition exclusions, but most individual plans do not.
Coordination of benefits
Most LTC policies do not have this feature Can help people who are insured “stretch” their coverage by tapping into other coverage
they have first

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 177
Care Coordinator might help people “coordinate” so they can get more out of their LTC policy
Today, most policies do not coordinate with other coverage. But if they do, it can be a good thing since it will help the consumer’s LTC coverage last longer if there is another insurance that should and will pay first.
Suitability
Is Long Term Care Insurance Right for Your Client?
Long term care insurance is a good choice for many people, but not for everyone. People should consider long term care insurance if they have assets of at least $30,000 (excluding their home) and/or they have income they want to protect. They may also want to consider long term care insurance if they want to choose where to receive long term care and/or they don’t want to burden their family with caring for them.
People should not consider long term care insurance if they can’t afford the premiums. If they will be paying premiums with money received only from their own income, especially if the premiums will be more than 7% of their income.
If their sole income is from Social Security or Supplemental Security Income (SSI) or if they’re struggling to meet their basic monthly living expenses, this coverage probably won’t make sense for them. If they are buying this (type of) policy to protect their assets and their assets are less than 30,000, they may wish to consider other options for financing their long term care.
Good Candidate for LTC Insurance
Being a good candidate for buying coverage is about more than just financial issues, but affordability is important.
Has assets to protect or leave to others, or that have sentimental value Is able to afford monthly premiums Is unable or unwilling to pay out-of-pocket for a long duration of LTC Is not currently disabled or seriously ill, has a family history of longevity, and does not
have a health history/lifestyle suggesting increased risk for disabling disease or injury Wants to ensure independence and control over money and assets Has an income level too high to qualify for Medicaid
Unlikely Candidate for LTC Insurance
Agents must help people figure out if it is not appropriate for them to buy. Health and financial situation are the most important considerations.
Has few or no assets to protect Is unable to afford insurance premiums, now or in the future Is already disabled or has serious health problems Has an income level that meets Medicaid eligibility limits

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 178
Has enough assets to be self-insured and chooses that option Has no surviving loved ones to leave assets to
When Should Someone Apply for Long Term Care Insurance?
It is important for consumers to apply for long term care insurance when they’re in good health. Most long term care insurance plans list certain medical conditions, or combinations of conditions, that will prevent some people from being approved for coverage.
People can purchase long term care insurance at any time as long as they are able to meet medical underwriting rules.
Since the cost for this insurance is generally based on their age at the time of application, the younger they are when they apply, the lower their premiums will be.
They’ll need to weigh the availability of resources and their own personal financial needs to help decide when it’s best to apply for long term care insurance.
Outline of Coverage
The “Outline of Coverage” (OOC) is a summary of policy definitions, covered services, benefits, exclusions, and other policy provisions. It is a vitally important consumer disclosure document. Insurers are required to follow a state-mandated format and use specific language to explain coverage features in the OOC. Similarly, insurers are required to provide a potential buyer with the OOC before the agent can accept an application from that individual. This requirement is intended to encourage the individual to read the OOC and learn what is covered and what is not covered before they buy a policy. It is also designed to help consumers compare policies across insurance companies. This is why having a standardized approach to the information in the OOC is so important.
Key Disclosure Elements are Included in the Outline of Coverage
Caution Statement. This statement reminds the consumer that the insurer can deny benefits or rescind coverage if the applicant provides false information on the application. It reminds the consumer of the importance of fully disclosing and accurately answering all questions on the application.
Tax Statement. The OOC must indicate whether the LTC policy is tax-qualified or is a non-tax qualified LTC plan.
Guaranteed Renewability. The OOC states that coverage is guaranteed renewable. Limited Right to Change Premiums. The terms under which premiums can change are
summarized. Free Look Provision. The OOC reminds consumers that they can return their policy
within the first 30 days and receive a full return of the premium they paid. Definitions. The OOC defines key terms in the policy. Benefits and Exclusions. The OOC also briefly describes each benefit in the policy. Benefit Eligibility. The conditions for receiving benefits are described – this includes
specifics about the nature and degree of functional and cognitive loss that must exist in order to receive benefits.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 179
Limitations and Exclusions. The OOC is required to list the exclusions and limitations that apply. The OOC must explicitly state that Alzheimer’s disease is covered.
Inflation protection. Details on how the policy keeps pace with inflation under all the scenarios available to the buyer under the policy. Typically, the OOC shows how benefits and costs would change under each option over a 20-year period.
Premium information. The OOC generally provides a summary of the premium costs for various coverage choices or specifically for the options the individual is interested in choosing. The agent may write in the information specific to the buyer or the OOC may refer to the rate chart.
SHIP (HICAP) Contact. Some states require the OOC to inform people who to contact for free advice and counseling about LTC insurance and how to reach them.
Comparing Long Term Care Insurance Policies
Purchasing long term care insurance can be a difficult and an overwhelming process. It is important to compare policies and insurance companies carefully to determine which long term care insurance offering best meets their needs.
How Much Long Term Care Insurance Coverage is Needed?
There are several factors that should drive the decision.
First, consider the geographic area where they will most likely be receiving long term care services. The cost for services is generally higher in metropolitan areas.
Second, determine whether or not they’ll need a Comprehensive option that will provide benefits in a variety of settings or if a Facilities-Only option is better for their needs and budget.
Third, consider how much money they can contribute from their savings to help cover the cost of care and how much they are able to afford for long term care insurance premiums. They may be able to pay a portion of the cost of care in return for a lower coverage amount and lower premium.
Finally, take into consideration the rising cost of medical expenses by helping them to carefully select an inflation protection option.
Buying LTC insurance – Important Considerations
An important role of the agent includes helping people decide if they should buy LTC insurance and, if so, how to carefully and appropriately choose what to buy.
Help consumer determine why they want LTC insurance, how they will pay for it Address commonly asked questions Help people think about their objectives for having coverage as they consider whether
and what to buy.
Perhaps the client is a good candidate for buying LTC insurance; perhaps not.
Consider their need and/or motivation for LTC insurance. Consumers should not buy out of fear or emotion. The purchase should be made because it is a sound financial decision and is affordable.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 180
Is there enough income to pay a portion of care costs and then rely on a smaller LTC policy for the remainder? Consumers should not buy more than they think they might need. If consumers are concerned about the cost of the premium and do not mind paying some care costs on their own, they may buy a smaller policy and still benefit from coverage.
On the other hand, is enough coverage being purchased? Buying too little means the consumer is only slightly delaying the time when their own assets or income will be needed to pay for care. The consumer should think about how they are going to pay care costs that extend beyond the period for which they buy coverage.
Additionally, consumers should analyze the features available and select the features appropriate for them. There is no “one size fits all” policy.
Long-term care costs increase annually. Consumers should plan for charges besides room and board, such as supplies, medications, linens, and other auxiliary expenses that may not be covered by the policy. It is important to check the policy language to see if it pays only for room and board in a facility, or if other expenses are covered. The consumer must ask himself/herself the question “Is the daily benefit selected adequate to include these auxiliary costs? If not, would it be feasible to pay for them out of pocket? If not, how will they be paid?
It costs less to buy coverage at a younger age. As a result, the younger the consumer is at the time the policy is purchased, the better off they are financially.
Medical necessity clauses may hinder policy benefits. Most people need LTC because of custodial needs that are essentially non-medical. Also, if medical necessity is not clearly and objectively defined in the policy, it may be difficult for the policyholder to negotiate eligibility with the insurer for certain claimed benefits.
The consumer should make sure LTC insurance fit within their budget before purchasing a policy. The Suitability Personal Worksheet from the insurance company is a place to start, but ultimately the consumer must make their own decision about whether LTC coverage is affordable.
What to Look for in a Long Term Care Insurance Policy
Since there are so many different long term care insurance plans and insurance carriers who offer them, it’s important to make sure the plan they select will meet their foreseeable needs. Some plans cover facilities-only care, while others cover facilities care and home care.
When helping consumers to determine whether LTC insurance is the right choice to finance their long-term care needs, ask these important questions:
What is the financial rating of the insurance carrier? Does the carrier have a history of filing for rate increases with state insurance
departments? What inflation protection options are offered? Is the policy priced according to the most recent National Association of Insurance
Commissioners (NAIC) guidelines? (This helps ensure the plan's premium stability.)

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 181
Selecting an Insurance Company
The more carefully the policy is underwritten; the better off the consumer is in terms of future rate stability. Be wary of companies that say they will issue coverage quickly with few or no medical questions.
Several private companies or rating agencies conduct financial analyses of insurance companies and grade them. While these ratings carry no guarantee of accuracy, they can provide information on how some analysts view the financial stability of the company. Some rating agencies are:
A.M. Best Company (900) 420 – 0400 (toll call) www.ambest.com Standard & Poor’s (212) 208 – 1527 www.standardandpoors.com Duff & Phelps, Inc. (312) 368 – 3157 www.bankwatch.com Moody’s Investor Service (212) 553 – 1653 www.moodys.com Fitch Investor Services (212) 908 – 0500
Besides selecting a carrier with high ratings (A or better) from rating companies that have billions in assets, a consumer should ask a number of other questions:
How long they have been selling LTC insurance, and do they have a dedicated LTC division? A dedicated division indicates corporate support for a LTC product. Some newer companies can be very good but those that have been around longer have more data, extensive experience, and, larger risk pool.
Has the company’s business grown mostly through acquisition of other companies’ LTC business or through sales growth? The former is a concern since the insurer’s risk pool might not be as strong if they bought companies that were exiting the market due to pricing, underwriting, or other problems.
How thorough is the company’s underwriting process? A detailed application with use of other information like an Attending Physician’s Statement and face-to-face assessments are indications of careful underwriting which is important to rate stability.
Are the premiums based on the NAIC 2000 model for rate stability? The newest policies are more likely to comply, as are the policies currently for sale in the 20 or so states that have adopted the NAIC 2000 rate stability guidelines. Ask the company to verify in writing whether the pricing for the product complies or not.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 182
What is the insurer’s history of rate increases? What are the reasons for the increases? If the increases were on older policy forms that are designed and underwritten differently than what is currently being sold, this may not be an issue.
Does the insurer offer a policy with options in the event of a rate increase, i.e. decrease in coverage to maintain current premium, or Contingent Non-forfeiture?
Is credit of the applicant’s past insured status given if applicant decides to increase or decrease coverage in the future? Some insurers allow this, others make you drop the current coverage and buy the new coverage at the new age. This means paying higher premium amounts and the applicant may not pass underwriting.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 183
Chapter Seven - Alternative LTC Financing Options
This chapter provides an overview of alternative long-term care (LTC) financing options. The module explains the different options available, provides a broad overview of which clients may be best suited for each of the options, and provides considerations that agents should keep in mind when dealing with consumers.
At the conclusion of this chapter, agents will understand:
The alternatives financing options to LTC insurance Differences among these options The benefits and potential drawbacks of each option
Variety of Options
In addition to LTC insurance, many options are available to finance LTC expenses. This table above categorizes these options and identifies the type of consumer the option may be best suited for.
Home Equity Life Insurance
LTC Annuities
Trusts Assets/Income Other
Reverse Mortgage
Accelerated death Benefits
Deferred Medicaid Disability Trusts
Self Pay CCRC
Reverse Annuity Mortgage
Life settlements
Immediate Charitable remainder trusts
Medicaid Estate Planning
Sell Home Viatical Settlements
Special Purpose Loan
Leaseback Limited pay/LTC Policies
Use of Home Equity for LTC
Home equity is the difference between the appraised value of their home and what is owed on any mortgages. By the time someone needs long-term care they may have greatly reduced or paid off the home mortgage. The value of the home may also have risen beyond its original purchase price.
Choosing to tap home equity can be a big decision. The house may be their most valuable financial asset. There are many practical and financial factors to consider:
Should they sell the house or take out a home loan? It is important to balance health and safety issues with the desire for independence and a familiar setting.
If it makes sense to stay at home, what are the benefits and risks associated with different types of home loans?

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 184
How will using home equity affect their eligibility for public programs, should they be needed?
They should evaluate the use of home equity as part of their overall financial plans.
Tapping home equity typically involves taking out a loan that uses the home as the collateral to guarantee that they will repay the loan. There are several ways to use the equity in a home to pay for long-term care:
Reverse mortgages Conventional home equity loans Home equity conversions Reverse annuity mortgages Lease backs Home modification loans
There are usually significant upfront costs associated with any type of home loan. Homeowners who have an ongoing health problem need to decide if it is worth taking out a loan, since they may only be able to continue to live at home for a short time.
Reverse Mortgage (RM)
A reverse mortgage (RM) is a type of home equity loan that enables homeowners age 62 and over to convert some of the equity in their home (single family or condominium) into cash and continue to own and live in the home. It operates similar to a traditional mortgage, but in reverse. Instead of paying the lender, the lender pays the homeowner.
Unlike home equity loans, RMs do not require repayment of the principal, interest, or servicing fees as long as they live in the home. Since the borrower retains ownership, he or she is still responsible for taxes and repairs. When the homeowner dies or moves out, the loan is paid off by the sale of the property. An individual can never owe more than the home’s value. Any leftover equity goes to the homeowner or their heirs.
The amount borrowed is based on age, life expectancy, the equity in the home, the location of the home, and the interest rate. Maximums range from 50 to 75 percent of the home’s fair market value (depending on lender). There are no income or credit qualifications. However, the home must be completely or nearly paid off to qualify.
The RM proceeds may be paid in a lump sum, in monthly advances, through a line of credit or a combination of the three. This money is non-taxable. It does not count towards income or affect Social Security, Medicare, or Medicaid benefits as long as the RM payments are spent within the month they are received. However, interest on RM is not tax deductible until the debt is paid.
Important consumer protections:
Borrower(s) continue to own the house and can never be forced to leave as long as they maintain the home, and make property tax and hazard insurance payments.
They must first meet with a government-approved reverse mortgage counselor before their loan application can be processed or they incur any loan costs.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 185
Borrowers (or their heirs) will never owe more than value of the home at the time they sell the home or repay the loan, even if the value of their home declines.
Home Equity Conversion Mortgage (HECM)
Offered by Department of Housing and Urban Development (HUD) Federal Housing Authority (FHA) guaranteed loan Loan amount based on their age, value of home, equity in home, where they live,
interest rate, and payout method they select
The most widely available RM plan is the Federal Housing Administration's Government-insured Home Equity Conversion Mortgage (HECM) program. To qualify for a HECM loan, homeowners must be at least 62 and live in a single-family home or condominium that is their principal residence. Under this program, the amount of equity homeowners may borrow against depends on where they live, as well as on prevailing interest rates. Counseling is required before homeowners can apply for a HECM loan. This counseling allows homeowners to discover whether a reverse mortgage is really the best answer to their cash-flow problems.
Using a HECM to Pay for LTC Insurance
People can use the funds received from a reverse mortgage to pay for a wide array of in-home and community services and other expenses, such as home repairs and transportation, which can make it safer and more comfortable for people to live at home. However, long-term care expenses may be greater than the amount they can get in the reverse mortgage. They can also use the funds to purchase long-term care insurance. It may be hard for a married couple to purchase long-term care insurance or pay for long-term care costs for both people with the amount available from a reverse mortgage.
This plan offers several payment options:
Monthly loan advances for a fixed term, or for as long as they live in the home, A line of credit, or Monthly loan advances plus a line of credit.
Their heirs can keep the home by repaying the reverse mortgage. The heirs can also “keep the difference” if the home's sale price is greater than the reverse mortgage loan balance when it's time to repay the loan.
Examples:
HECM Reverse Mortgage – Loan Amounts
Sample loan amounts available - $120,000 home value (Philadelphia)
Age Lump Sum Monthly 62 $62,600 $350 67 $67,600 $400 72 $72,800 $450

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 186
Note differences in payment as a result of payment option and age.
Sample loan amounts available - $260,000 home value (Denver)
Age Lump Sum Monthly 62 $145,900 $819 67 $156,500 $918 72 $167,800 $1,047
Note differences in payment as a result of payment option and age.
HECM Reverse Mortgage – Closing Costs
Closing costs and interest can be financed within the loan Include mortgage insurance (2% of home value), origination fee (2% of home value) and
other closing costs (e.g., title search, appraisal, etc.) Costs vary, but in one example, for a $200,000 loan, costs range from $10,000 to
$14,000 Forward mortgage points are calculated as a percentage of the loan amount. Reverse
mortgage points are calculated as a percentage of the home value.
Lender-Insured
Lender-insured reverse mortgages offer monthly loan advances or monthly loan advances plus a line of credit for as long as an individual lives in his/her home.
Federal National Mortgage Association (FNMA)
This program may be available to people who have homes that are more expensive or who need to borrow more. The Federal National Mortgage Association (commonly known as Fannie Mae) has a program that grants larger reverse mortgages on home equity.
Homekeeper
One example is the Federal National Mortgage Association’s Homekeeper product.
Interest rates may be assessed at a fixed or adjustable rate. Additional loan costs can include a mortgage insurance premium (which may be fixed or
variable) and other loan fees. Loan advances from a lender-insured plan may be larger than those provided by FHA-
insured plans. Lender-insured reverse mortgages also may allow an individual to mortgage less than
the full value of his/her home, thus preserving home equity for later use by an individual or his/her heirs.
Loans may involve greater loan costs than FHA insured, or uninsured loans. Higher costs mean that the loan amount grows faster, leaving an individual with less
equity over time.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 187
Uninsured
The uninsured reverse mortgage is dramatically different from FHA and lender-insured reverse mortgages. It is important to keep in mind that most private reverse mortgages are not insured. Only the strength of the lender backs whatever promises it makes as to payments and other terms. Thus, if the objective of a RM is future income, rather than a lump sum up front, a federally insured program is better.
Provides monthly loan advances for a fixed term only – a definite number of years selected by an individual when the loan is first taken out.
The loan balance becomes due and payable when the loan advances stop. Interest is usually set at a fixed interest rate and no mortgage insurance premium is
required.
Qualifying for Reverse Mortgage
Reverse mortgage funds must be used to pay off any existing mortgage or other debt against the home and to make required home repairs. Borrowers can use the remaining funds for any purpose with no restrictions.
A reverse mortgage must be in first lien position, which makes it very difficult to borrow any more against the home once they have a reverse mortgage. They can refinance a reverse mortgage if the house increases significantly in value.
All potential borrowers must first meet with a HUD-approved reverse mortgage counselor before they can start the loan process. These counselors can provide information to help decide whether a reverse mortgage is right for them.
Comparing Forward vs. Reverse Mortgage
Conventional Mortgage Reverse Mortgage
Purpose Purchase a home Get cash from home equity
At the time of closing:
Owe a lot and have little equity in the home
Owe little and have lots of equity in the home.
During the loan: Make monthly payments. The loan balance decreases. Equity grows.
Receive monthly payments (as a lump sum, monthly payment, or line of credit). The loan balance rises. Equity decreases.
At the end of the loan:
Owe nothing. Have substantial equity in the home.
May owe a large amount. May have little or no equity in the home.
Closing costs Based on the amount of the loan Can be financed as part of loan.
Based on appraised value of the home. Can be financed as part of loan.
In short… Falling debt Rising equity
Rising debt Falling equity

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 188
Reverse Mortgage Annuity
In a RM annuity, part of the lump-sum loan amount obtained from the RM is used to purchase an annuity. Even if the borrower sells or moves from the home, annuity payments will continue. The loan must be paid off when the owner dies, sells or moves from the home. The annuity payments from the separately-purchased annuity can continue.
Considerations
Annuity payments may be taxable and affect eligibility for Supplemental Security Income and Medicaid.
Additional charges based on increases in the value of the home during the term of the loan may be included if an equity participation option is chosen by the borrower in order to lower the interest rate.
CAUTION: The term "reverse annuity mortgage" (RAM) is used to refer to reverse mortgages that are structured with a monthly income option. Consumers must be cautioned to fully understand what type of reverse mortgage they are considering so that the full impact of taxation issues, loan repayment requirements and monthly payment promises is understood.
Sell Home
One way of using the equity in one’s home to pay for LTC is to sell it. The proceeds can be invested to produce a continuous income, to pay for LTC expenses or to purchase a LTC insurance policy.
This option may be well suited to a single person who does not have any heirs or a couple that wants a lifestyle or location change. Someone who has the alternative of less costly living arrangements may also find this a viable option.
Many people are uncomfortable selling their major asset. However, this option is well-suited to a single person without heirs, a couple who wants a lifestyle or location change or someone who wants an alternative, less costly living arrangement.
One of the most difficult decisions someone may face as they age is whether it is time to leave their home and move to a more supportive setting such as an assisted living facility or nursing home. Consider several factors to decide whether staying at home makes sense. For many people, a house that was ideal 30 years ago may now be too difficult to handle alone. For suburban and rural elders, isolation can become a problem when driving is difficult. Deteriorating neighborhoods may also make an older person reluctant to go shopping or attend social activities. Getting good quality and reliable help, either from family caregivers or paid professionals, is another critical element.
Considerations:
Unable to pass home to heirs Proceeds may be insufficient to cover LTC expenses Market conditions

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 189
Proceeds can be invested to produce a continuous income, pay for LTC expenses or purchase insurance.
Sale–Leaseback Arrangement
A Sale–Leaseback is an arrangement where people sell their home to an investor, typically at below market value, and then remain in the home as a renter. They rent their home from the investor on a long-term lease. They no longer have to worry about maintenance of the home or paying taxes. People can use the proceeds from the home sale any way they like. The investor takes over the property once they stop living there.
A leaseback occurs when an investor purchases a home below market value and the investor agrees to rent the house to the seller on a long-term lease. The seller no longer has to worry about maintenance or repairs to the home or paying taxes, and the proceeds of the sale can be used as desired, to finance LTC needs or to purchase insurance.
The investor is partially reimbursed for giving a long lease through the difference between the selling price and a possibly higher fair market value. Long-term leases, or even a life estate, have definite economic value that can be reflected in the sale price of the home. The responsibility of taxes and property maintenance also falls on the investor. Possession of the property goes to the investor once the seller stops living there.
Considerations:
This may be an option to allow the home to stay in the family by allowing children to take on the role of investor and purchase the home from their parents.
Seller no longer has to worry about taking care of home or paying taxes Proceeds can be used as desired, e.g., to finance LTC needs or buy insurance Investor is responsible for taxes and property maintenance Children can be the investor and purchase home from parents, allowing it to stay in the
family Seller may have to pay taxes on proceeds of the sale Low-income homeowners may lose public assistance funds If property is neglected, seller may find it difficult to live there and not have funds or the
authority to correct the situation
Use of Life Insurance
There are financing options that allow access to the death benefit of a life insurance policy prior to death. Certain conditions and requirements apply; therefore, they are not appropriate for all consumers.
Accelerated Death Benefits Life Settlements Viatical Settlements Single Premium Life/LTC Policy

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 190
Accelerated Death Benefits (ADB)
An Accelerated Death Benefit is a life insurance death benefit paid in cash in advance, tax free. An ADB is a feature or rider included with some life insurance policies. It provides cash advances against the death benefit while they are alive. Sometimes people pay an extra premium to add this to their life insurance policy and sometimes it is included by the life insurance company for little or no cost.
There are different types of Accelerated Death Benefits, each of which serves a different purpose. Depending on the type of policy they have, people may be able to receive a cash advance of their life insurance policy's death benefit when:
They are terminally ill They have a life-threatening diagnosis, such as AIDS They need long-term care for an extended amount of time They are permanently confined to a nursing home and incapable of performing everyday
Activities of Daily Living
The amount of money people can receive from these types of policies varies, but typically the accelerated benefit payment amount is capped at 50 percent of the death benefit. Some policies, however, do allow them to access the full amount of the death benefit.
For ADB policies that have a long-term care benefit, the monthly benefit available for nursing home care is typically equal to two percent of the life insurance policy's face value, while the amount available for home care (if it is included in the policy) is typically half that amount. For example, if their life insurance policy's face value is $200,000, then the monthly payout available to them for care in a nursing home would be $4,000, but only $2,000 for home care. Some policies may pay the same monthly amount for care, regardless of where they receive the care.
When someone receives payments from an ADB policy prior to death, the amount received is subtracted from the amount payable to beneficiaries when they die.
Since benefits are more limited than typical LTC insurance policies, the amount may be insufficient to cover LTC costs, inflation protection is infrequently offered.
By using the benefit ahead of time, there may be nothing left for the survivors. There is a risk that the policy will lapse if premiums are not paid on the life insurance
policy. Consumers need to consider whether funds will continue to be available to pay premiums.
The payment may affect Medicaid eligibility.
Considerations:
Inflation protection is often not offered. If inflation protection is not included, the ADB payment may not be sufficient to cover their future long-term care costs. This means they would need additional means to pay for their care.
If someone wants to leave an inheritance, they should consider whether this is the right option. If they use the ADB feature for long-term care, there may be little or no death benefit remaining for survivors.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 191
This option may affect eligibility for Medicaid. Consumers should check with the state Medicaid agency for more information.
Life Settlements
Life Settlements give people the ability to raise cash by selling their life insurance policy. With a Life Settlement, a person sells their life insurance policy for its present value.
Life Settlements (also known as Senior Settlements, Elder Settlements or High Net Worth Settlements) give older individuals the ability to adapt to changes in health, goals or life circumstances. They may no longer need the death benefit because the original reason they purchased the insurance no longer exists (i.e. a mortgage or minor children) or the insurance premium may be unaffordable after retirement.
Females age 74 or older and males age 70 and over that have any type of life insurance can sell their policies to a life settlement company for the present value of the policy. Some companies may purchase the life insurance policy of a 65 year old if their life expectancy is in the 12-year range. The types of policies that can be sold are: group, individual, term, whole life, universal life, policies held in irrevocable life insurance trusts, buy-sell agreements, and “key-person” policies. In addition, one need not be dying or in poor health to take advantage of a Life Settlement.
The use of the proceeds is unrestricted and can be used for anything the person wishes. For example, LTC expenses can be paid for someone who may be otherwise uninsurable or LTC insurance can be purchased.
There are tax implications for this type of option. The difference between the settlement payment and the cash surrender value is taxed as a capital gain, while the difference between the total premiums paid and the cash surrender value is taxed as ordinary income. Consumers considering this option should discuss their individual situations with a tax professional.
While the popularity of Life Settlements has increased, they are not for everyone. Consideration should be given to the impact that the sale of the life insurance policy will have on the original beneficiaries who will not receive a death benefit. If cash is needed, a loan on the policy’s cash value or reduction of the death benefit in order to be able to afford to continue paying the premiums may be better options.
Considerations:
If LTC is not required, the settlement can be left as an inheritance or used for other purposes.
If money is used for LTC, there will be no death benefit for the survivors. Only requirement is age, therefore this is a viable option for healthy and unhealthy
people unlike other options using life insurance which require the person to be in poor health.
There are tax implications. Depending on the income status of the person, this may not be the best option. They should consult their tax advisor prior to taking a Life Settlement.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 192
Viatical Settlements
Largely in response to the AIDS epidemic in the 1980’s, viatical settlements and accelerated death benefits were created by the insurance industry to allow cash payouts prior to the death of the insured. The difference between a Life Settlement and a Viatical is a matter of time and health. A viatical is the sale of a policy by someone who has a life expectancy of two years or less while someone with a Life Settlement has a life expectancy of greater than two years but less than 13 years. The tax consequences also differ. Viatical settlements are usually tax-free, whereas Life Settlements are not.
Under a viatical settlement, the insured assigns the proceeds of his/her life insurance policy to an investor in exchange for a cash settlement, which is less than the value of the death benefit. The life expectancy of the insured is used to compute the cash settlement, with a higher percentage payout for those closer to death. The investor pays the premiums until the death of the insured, at which time the investor receives the death benefit of the policy.
Unlike the Life Settlement, money received from a Viatical Settlement is tax-free, provided the insured has a life expectancy of two years or less or are chronically ill, and provided the Viatical Company is licensed in the states in which it does business.
The National Association of Insurance Commissioners (NAIC) guidelines for the amount of the Viatical Payment that is appropriate, based on life expectancy are listed below.
The National Association of Insurance Commissioners (NAIC) has developed a Viatical Settlements Model Act governing the licensing and regulation of viatical companies. Many states have adopted this act in whole or in part. Agents and clients should check whether their state has adopted these guidelines. If adopted by states, viatical companies must be licensed by state insurance departments. Full disclosure, especially regarding tax implications, would be required. Viators would need to be informed that the sale of their death benefit may disqualify them for public assistance. The act establishes guidelines for the payment to the viator.
NAIC Guidelines for Viatical Payments
Life Expectancy Benefit 1–6 months 80% 6–12 months 70% 12–18 months 65% 18–24 months 60% Over 24 months 50%
Last Modified: 1/8/2007 9:31:21 AM
Other factors influencing the amount of the viatical payments are:
Insurer’s Rating – Lower payment to viator if life insurance company has an A.M. Best rating of B+ or lower

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 193
Waiver of Premium – Higher payment to viator because viatical company does not have to pay premium on policies that have a waiver of premium when the policyholder becomes disabled
Capitalization of the Viatical Company – Viator likely to get a better deal with a well-capitalized company
Case Diversification of Viatical Company – Viator likely to get a better offer from companies with a diversified consumer base
Tax Treatment, Legislation, Regulation
In 1995, legislation was passed that exempts both viatical settlements and accelerated death benefits from federal income tax. Under HIPAA 1996, viatical settlements are not subject to income and capital gains taxes.
Also in 1995, The Securities and Exchange Commission ruled that viatical settlements are securities and require registration. SEC maintains that if a firm solicits investors and represents viatical settlements as an investment, the firm is selling an unregistered security. It also ruled that if an agent refers a consumer to a viatical settlement firm, the person is considered to be selling insurance and is therefore not currently affected by SEC rulings.
Standard and Poor’s has developed criteria to rate securities issued by viatical settlement companies. Among the criteria used are:
Fair market value for the policy Company’s track record Licensing status of the companies offering to purchase
Single Premium Life/LTC Policies
Unlike traditional LTC policies that can require premiums (that are subject to change) to be paid for life or until care is needed, the Single Premium Life/LTC policies are funded through a lump sum payment, which is guaranteed not to change. The single premium deposit can be made with cash, CDs, money market accounts, non-qualified and qualified annuities, or IRAs and Keogh plans. Issue ages can vary based on the source of the premium. For example, an issue age of 59½ or higher might be required for transfers from qualified annuities, IRAs and Keoghs. In addition, the cash value from a life insurance policy may be moved into a combined policy without adverse tax consequences.
Minimum deposits can be in the $10,000-$20,000 range, but for a meaningful benefit based on today’s costs, the deposit should be in the $100,000 range for a 60-year old couple. If a person is willing to self-insure a portion of LTC expenses or have other ways of financing LTC, a smaller deposit can be made.
The lump sum deposit purchases a death benefit and at least double the amount becomes available for LTC expenses.
If LTC is needed immediately, the policy could pay as much as four years of benefits at 2 percent per month of the LTC amount.
The longer the policy is held without a claim, the more accumulation and the longer the benefit period becomes.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 194
Inflation coverage may be included in the lump sum deposit or paid separately and on a continuing basis, depending on the insurance company.
Considerations:
Age 80 is usually the maximum issue age. A joint policy can be issued if both people fall within certain age parameters. There are no age limits for benefit payments once the policy is issued. A certain amount of money is available each year and can be accessed without
surrender penalties (surrender penalties disappear after 10 years). Withdrawals are subject to income tax. Unlike traditional LTC insurance policies, this type of insurance policy pays a death
benefit.
Long-Term Care Annuities
An annuity is a series of regular payments over a specified and defined period of time. Annuities can help people pay for LTC who cannot qualify for LTC insurance due to age or health problems. There are two types of LTC annuities:
Immediate long-term care annuity Deferred long-term care annuity
LTC Annuities – Deferred
This annuity is available for persons up to age 85 and has seven broad health questions that most people can satisfy. One example of this hybrid product might consist of two funds. The first fund is for LTC expenses and it grows at a high interest rate with a five-year guarantee. It then grows at the current interest rate thereafter. The second fund grows at 3 percent guaranteed and is a regular cash fund.
The purpose of the separate LTC fund is to allow immediate use of the funds for licensed LTC services. Otherwise, early withdrawals from a regular deferred annuity are limited or can be penalized. The benefits might pay no more than actual expenses up to a monthly limit for a minimum of 36 months and begin after a 7-day waiting period. The amount of the monthly benefit is determined by dividing the LTC fund balance by a factor. A lifetime rider may be available for an additional premium.
An individual may make annual withdrawals of 10 percent from the cash fund to pay for additional expenses, such as prescription drugs, not covered as eligible expenses under the LTC fund. (Withdrawals greater than 10 percent may be penalized). Additionally, the cash fund is reduced proportionately when money is withdrawn from the LTC fund. For example, a $3,000 withdrawal from the LTC fund means a $1,500 withdrawal from the cash fund. If the LTC fund is not exhausted at the time of death, any remaining money in the cash fund will be passed to the beneficiary outside of probate.
There are available state-specific products may differ markedly from this example or may not even be available in the consumer’s state.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 195
Tax Rules
The long-term care portion of the annuity does not satisfy the requirements for a tax-qualified long-term care policy, so there is a risk of being taxed on the money from the fund that is used for long-term care expenses. A tax professional should be consulted when determining whether this option is the right choice to finance LTC costs.
There is also a type of hybrid deferred annuity/LTC product that would act as a standard deferred annuity with a LTC insurance rider attached. The LTC insurance rider could be accessed, after the passage of a six-year waiting period, through traditional ADL and cognitive impairment benefit triggers. It would pay monthly benefits based on a percentage of the amount that had accrued in the annuity portion but would not reduce the annuity portion of the contract. The money coming from the LTC insurance rider is the insurance company’s money, paid as a LTC benefit for up to three years; the money in the annuity portion is the consumer’s money, which could be accessed as a regular annuity to supplement the LTC insurance rider payments (or not, as needed). The money from the LTC insurance rider is considered taxable. Since there is no medical underwriting required, this might be an option for someone who is uninsurable under traditional LTC insurance with a condition that might not require care for six or more years (early stage Parkinson’s, for example).
Considerations
The benefit amount may not adequately cover all LTC expenses. This is especially likely if LTC is needed close to the time the annuity is obtained and before the fund has grown, or before the separate LTC insurance rider is available for access.
Enough money should be put into the annuity to accommodate inflation. Consumers should be advised to speak with a tax professional.
LTC Annuities – Immediate
For a single premium payment made to an insurance company, people receive a specified monthly income. It is available to them without regard to their health, so those who don't qualify for long-term care insurance because of age or poor health or are already receiving long-term care, they can still purchase an annuity. The single premium payment is converted to a monthly income stream that is guaranteed either for a specified period of time or for the life of the individual receiving the payments. The payout schedule varies based on the amount of the initial premium, their age, and gender. Generally, because of their longer life expectancy, females receive a smaller monthly payment over a longer period of time than do males of the same age.
Immediate annuities are available to people with uninsurable health conditions or those who may already be receiving LTC, as well as those in good health. A single premium payment is converted to a monthly income stream guaranteed for the life of the policyholder or for a minimum guarantee period, life plus a minimum guarantee period or even a joint and survivor annuity option. The named beneficiary or beneficiaries would receive a portion of the money if the policyholder died earlier than the expiration of the minimum guarantee period.
The annuity pay-out schedule is based on age and gender. With immediate annuities that are not medically underwritten, all things being equal, if a male and a female of equal age purchase
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 196
identical life annuities, the male will get a higher monthly stream of income than the female, since the female will be expected to live longer than the male.
If the annuity is medically underwritten, the person with impaired health would receive a larger monthly payout because of the actuarially-determined shorter life span of the individual. However, medically-underwritten annuities are fairly new to the U.S. and not available in every state.
(Note: Please see new rules regarding annuities under the DRA)
Trusts
A trust is a legal arrangement by which one person, the grantor, transfers assets to another, the trustee, for the benefit of one or more third parties, the beneficiary. The trustee holds title to the assets and manages them, acting in the best interest of the beneficiary. Trusts may provide some options to partially fund LTC needs.
One use of a trust is to provide flexible control of assets for the benefit of minor children. Another is to provide flexible control of assets for the benefit of an elderly or disabled person, including themselves or their spouse.
Types of Trusts for Long-Term Care
Medicaid Disability Trusts Charitable Remainder Trusts
Medicaid Disability Trusts
The purpose of a Medicaid Disability Trust is to enhance the quality of life of an individual with a disability who also qualifies for public benefits. Medicaid Disability Trusts are limited to disabled persons under age 65. With this type of trust, assets are managed by a non-profit organization. The trust may be established by a parent, grandparent or legal guardian for the benefit of the disabled person.
This is the only type of trust exempt from rules regarding trusts and Medicaid eligibility. All other irrevocable trusts currently created with the intent to transfer assets without spending down run the risk of being disqualified.
There are two types of Medicaid Disability Trusts; both are limited to disabled individuals.
Trust for Disabled Person under Age 65
It can be established by a parent, grandparent or legal guardian for the benefit of a disabled individual under 65. This trust might be set up to provide benefits to enhance the life of an individual who is qualified for public benefits. If Medicaid benefits are paid on behalf of the disabled individual, any amount remaining in the trust at the individual’s death is recoverable by the state up to the amount of such benefits.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 197
Pooled Trust Managed by a Non-Profit Association
Again, the purpose is to be able to use trust assets to enhance the life of the disabled individual while maintaining eligibility for public benefits. A separate account must be maintained for each beneficiary although funds are pooled for investment and management. Upon the beneficiary’s death, the state must be reimbursed for the Medicaid benefits paid on behalf of the beneficiary. The account is for the benefit of a disabled person who can be over 65 at the time of the establishment of the trust.
Medicaid benefits must be reimbursed upon the death of the recipient; therefore not all the money put in the trust will be sheltered. Consumers should be counseled to discuss this option with their legal and tax advisors. The trusts must be properly drafted to effectively accomplish the desired goal.
Charitable Remainder Trusts
These trusts allow people to use their own assets for long-term care with the added benefit of reducing taxes. This type of trust is typically used by wealthy people with specific types of assets that they donate to a public charity at fair market value. The individual making the donation receives a tax deduction on the amount that has been gifted. The donor then receives payments from the trust that can be used to pay for long-term care. Once the donor dies, the balance of the funds in the trust goes to the charity.
The funds available are based on the amount of their donation. These payments are only likely to be large enough to help pay for long-term care expenses for those who have donated a substantial amount of money to the charity.
Assets transferred to the trust are subject to a 60-month look-back period, which may make the grantor ineligible for Medicaid. However, since these are only used by wealthy individuals, it is highly unlikely that this would be an issue.
Assets and Income – Out of Pocket
Individuals with considerable investment assets and income may consider paying for their LTC needs as they arise or save for future LTC services. If an individual wanted to save enough money for LTC costs, an adequate level of assets would need to be set aside – in today’s dollars, approximately $325,000, is needed to fund a five-year nursing home stay. These assets should be invested to assure growth that will keep up with the rising costs of LTC. However, since it is unknown when LTC needs will occur and how long services will be required, it’s difficult to determine when investing should begin.
Self-insuring is not the same as insurance. It does not provide the short-term protection that an insurance policy does. Insurance protects people from the possible risk of needing LTC before adequate resources are accumulated to pay for it.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 198
Continuing Care Retirement Community (CCRC)
A Continuing Care Retirement Community (CCRC) is a community living arrangement, typically on a single campus, that provides housing, health care, and social services, usually for older people. CCRCs offer different levels of care ranging from independent housing to nursing home care.
A Continuing Care Retirement Community (CCRC) provides a full continuum of care in a variety of settings, allowing an individual to “age in place”. As the needs of the resident change, the services provided by the CCRC change from independent living to assisted living to nursing home care – all in the same location. The intent of most residents is to live the rest of their lives at the CCRC.
Usually, a resident pays an entrance fee and monthly payments to the community in exchange for housing and defined LTC services for their life. These fees vary by the size of the unit (studio, one- or two-bedroom, or larger) and by the location and type of the CCRC. A recent industry survey reports that average entrance fees for one- and two-bedroom apartments range between $59,000 and $121,000. These fees are subject to periodic increases as the operating costs of the complex increase.
A percentage of the entrance fee is usually reimbursed to the residents or their estates when they move or die. Typical refund rates may be 70 percent to 90 percent and is specified in the contract. The interest earned is not paid to the resident, although the resident may be responsible for paying income tax liability on the interest income.
The monthly service fee may be level for all residents or increase as the amount of care increases. Even under a uniform fee, costs normally increase over time, as costs rise. In many cases, LTC insurance is bundled into the monthly fee. The CCRC collects a benefit to provide LTC to the resident. Since the CCRC is planning on residents not needing care for a certain amount of time, in order to keep fees reasonable, residents must be relatively healthy to enter.
Types of CCRC Contracts
While similar in concept, contract provisions differ. It is important for a consumer to review the contract carefully to determine the services included in the entrance and monthly fees the resident is expected to pay. The contract should also state the conditions that allow for increases or decreases in monthly fees and procedures for adjusting fees when living accommodations change. If a resident moves to a nursing facility, the contract should state how long living quarters are maintained and the conditions under which the spouse stays in the living quarters. If the contract includes a termination clause, the terms and procedures should be clearly stated. Contract review requires legal and financial assistance.
All Inclusive Fee for Service Modified
Entrance Fee/
Monthly Payment
Covers housing and all LTC fees usually higher than for other types of CCRC.
Housing, social and recreational services. Access to LTC services. Less expensive than All Inclusive.
Housing, social services and physical assistance included along with a specified amount of nursing home care.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 199
Not Included/
Incremental
Medical services which are usually covered by Medicare or supplemental health insurance.
LTC and medical services are paid for by resident as required. None of the services are pre-paid.
Additional LTC services available for fee.
Note: Refer to the chapter covering the DRA for new rules regarding CCRC entrance fees.
Medicaid Estate Planning
Artificial Impoverishment for Medicaid Qualification Purpose
Medicaid planning is the legal practice of rearranging finances so that the Medicaid program pays for nursing home care and the individual’s assets are preserved through change of ownership.
In order to qualify for Medicaid, individuals must first spend down their assets and use the proceeds to pay for LTC before Medicaid begins to pay. Spend down means liquidating assets. States have different maximum asset levels that individuals may keep.
Some people reduce their assets by transferring them to family members or others, or set up irrevocable (unchangeable) trusts, instead of using these assets to pay for care. They hope to continue using the assets with the cooperation of their relatives or enable others to benefit from the assets.
However, Medicaid “look-back” rules apply when assets are transferred for less than fair market value by applicants for Medicaid and to transfers made by the applicant’s spouse or someone else acting on their behalf. Medicaid benefits may be withheld for a period of time determined by the amount of the transfer. These rules apply to “gifts” made 60 months or less before the application for Medicaid including transfers to trusts.
In most cases, Medicaid does not pay for home care or assisted living care. And since this is a welfare program, once on Medicaid, an individual does not have control over assets or where care can be received.
Note: Several changes have been made to rules regarding transfers of assets under the DRA.
Home Modification Loans
Some government agencies and communities make low interest loans available for home modifications that help make their home a safer and more supportive living environment. While these loans are used specifically for home modifications and not to pay for long-term care costs, often a home modification can help someone with a physical limitation or disability to cope more effectively at home. Home modification loans may make it possible for people to stay in their own home instead of having to move to a care facility. Home modifications include things such as the installation of ramps or grab rails. The loan is repaid when they no longer live at home.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 200
Evaluating Options
It's difficult to predict if or how much care someone will need, whether they will have family or friends who can provide some or all of their care, and how much care may cost. However, it's reasonably easy to predict that if you need extensive long-term care services or need services over a long period of time, they will have to pay for some or all of it out of their personal finances. That's why an increasing number of people are using private financing options to help them pay for long-term care if and when they need it.
Private long-term care financing options include long-term care insurance, trusts, annuities, and reverse mortgages. Which option is best for them depends on many factors including their age, their health status, their risk of needing long-term care, and their personal financial situation. The following charts summarize how age and health status may affect their eligibility for and choice of private financing options.
Case Study
For each scenario, determine the financing option(s) that may be considered. For each scenario, think about what else you might need to know about the individual before you could help them evaluate these possible financing options.
Mary is 65 and lives by herself. She owns her home and is in relatively good health. She’s concerned about her future because she has no family to take care of her if she needed LTC. What options might she consider? Why?
Philip is 77 and in poor health. He has considerable assets, owns his home and has 4 children. He doesn’t want to burden his children or his spouse with his LTC needs. What options might he consider? Why?
Connie is 83 and barely making ends meet. She owns her home and does not want to move. She has been diagnosed with Parkinson’s disease. What options might she consider? Why?

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 201
Chapter Eight - New National Partnership Initiative and the Deficit Reduction Act (DRA)
Learning Objectives
The Deficit Reduction Act What is Partnership Partnership & Medicaid Inflation Protection – and why it is important Suitability Plan Design Resources
Deficit Reduction Act of 2005
In February of 2006, Congress passed the Deficit Reduction Act (DRA). This legislation contained a number of provisions affecting Medicaid:
Changes Regarding exemption of Assets, Annuities and Home Equity Ownership Elimination of prior restrictions on the expansion of partnership programs Any state can now choose to implement a partnership program
Major Areas of LTC Reform in the DRA
Asset Transfers Long-Term Care Partnership Program Family Opportunity Act Money Follows the Person Demonstration Home and Community-Based (HCBS) Services Cash and Counseling
The DRA makes many extensive changes to long-term services policies in Medicaid. In some cases, such as changes in asset transfer rules, the effect of the DRA could be reduced eligibility for Medicaid. In others, including the State Long-Term Care Partnership Program and the Family Opportunity Act, the DRA might lead to more individuals qualifying for Medicaid and receiving access to Medicaid long-term services and supports. Other provisions of the DRA give states expanded flexibility in delivering long-term services and may lead to expanded access to community-based long-term services.
Asset Transfers
Requires states to lengthen the look-back period for asset transfers to establish Medicaid’s eligibility for nursing home coverage from 3 to 5 years and changes the start of the penalty from the date of the transfer to the date of Medicaid eligibility
Requires annuities to be disclosed and states to be named a beneficiary for cost of Medicaid assistance
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 202
Requires state to use the income first rule Excludes coverage for individuals with home equity in excess of $500,000 (or up to
$750,000 at state option), with an exception when a spouse or child with a disability is residing in the home
Mandatory “Income-First” Rule
The DRA requires states to use the “income-first” rule when determining the monthly income maintenance needs allowance for the community spouse. States must consider all income of institutionalized spouses to meet the minimum monthly maintenance needs allowance for community spouses
This change may have the effect of lowering the amount of income that can be retained by the community spouse.
In the past the short-fall in income was made-up by allowing the at-home spouse to retain more of the couple’s property that would produce additional income, even after the institutionalized spouse died. Now the at-home spouse will lose a substantial amount of income when the spouse passes away.
This could lead to greater financial insecurity for some couples, but could also increase Medicaid costs if it leads both spouses to end up as Medicaid nursing home residents. This makes having private LTC coverage is even more important, especially for a widow with little income of her own.
DRA Changes - Home Equity
Before DRA
The principal residence remains exempt as long as they live in the property or, if in a facility, they have the intent to return there
No limit on the amount of equity
After DRA
Individuals with more than $500,000 (states can increase the amount to $750,000) in home equity are not eligible unless home equity reduced
Can use a reverse mortgage or equity line to reduce homes equity Dollar amount will be increased, starting in 2011, based on CPI Applies as of January 1, 2006
Expansion of LTC Partnership Program
The DRA allows for expansion of a National Long-Term Care Partnership to all states. Now all states may establish a Long-Term Care Partnership program that requires certain policy benefits and provisions. As in the existing state Partnership Programs, purchasers of private Long-Term Care Partnership policies (so called PQ or Partnership-Qualified Policies) who exhaust their policy benefits may qualify for Medicaid while retaining a greater amount of their

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 203
assets than would have been possible under the usual state Medicaid “spend down rules.” The ability to retain additional assets, yet still use Medicaid as a “safety net” if private coverage does not suffice, is the incentive for more people to purchase at least a moderate amount of private coverage.
What Is The Partnership For Long-Term Care?
Partnership Public/Private Incentive/Protection for Individuals Provides dollar for dollar asset protection Prevents complete spend down
Why the Partnership was Developed
Many people believe that neither the private sector nor the public sector will be able to completely finance the cost of long-term care in this country; and that the only means to adequately address this need is some form sharing of costs and coverage between the public and private sectors.
The "Partnership for Long Term Care" program was designed to encourage the purchase of qualified LTC insurance by allowing the purchasers to protect some or most of their assets from Medicaid spend-down requirements.
The Partnership Program is also designed to reduce Medicaid expenditures by delaying or eliminating the need for some people to rely on Medicaid to pay for long-term care services.
Individuals, who buy partnership policies and eventually need long-term care services, first rely on benefits from their private long-term care insurance policy to cover long-term care costs before they access Medicaid.
They then receive dollar for dollar protection – meaning each dollar of benefits paid protects a dollar of assets

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 204
In 2003 national spending on long-term care totaled $183 billion…. It’s breaking the government’s bank. Nearly half of that was paid for by the Medicaid program.
Private insurance paid a small portion of long-term care expenditures – about $16 billion or 9% in 2003.
With the aging of the baby boom generation, long-term care expenditures are anticipated to increase sharply in coming decades. Policymakers are looking for ways to reduce long-term care spending by Medicaid and promote private insurance as a larger funding source and that is the impetus behind the Partnership Expansion

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 205
Growth of Medicaid LTC Payments
Few Americans Plan Ahead for LTC Needs
A recent survey by AARP shows that most people are less knowledgeable now about LTC costs and financing than they were 5 years ago! Let’s look at what’s happening ….
About 60% of all Americans will need some type of supportive services after age 65? Less than 10% of those age 50+ own a long term care insurance policy Women age 40-44 who never had children doubled (how much growth) from 1976-today
Is it any wonder that the government is worried? Not just about dollars, but also about awareness and lack of planning?
More People Getting Older – Living Longer
Longevity is increasing, the baby boom generation is nearing retirement age, and the portion of our population age 65+ is the fastest-growing segment of our society.
But while the number of older persons is expected to increase rapidly, demographic changes in families (more childless, one-child, and step-families) and increasing participation of women in the workforce suggest a likely decrease in provision of informal care for aging baby boomers.1
1 National Institute on Aging, Congressional Justification FY 2001

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 206
Family Caregivers not always Available
Geographic changes are also expected to make it more difficult to obtain care from family members or other relatives. In the past, family members lived close to each other and could rely upon each other for help.
But the extended family of yesteryear has all but vanished. Families are increasingly spread apart, with mom and dad living in one part of the country while their children often reside thousands of miles away.2
2 The Wall Street Journal, 2/21/01
The goal is to expand the Partnership concept to all states, while having reciprocity and uniformity of policy and program across states. In terms of asset protection, they would be allowed to keep $1 of assets for every dollar they receive in benefits from a Partnership policy. There are certain requirements which all Partnership policies must meet. For example, anyone age 60 or younger must include automatic inflation protection in their coverage. The existing four Partnership states are exempt from the new rules.
Expansion of LTC Partnerships
New state QSLTCI partnership programs may become effective, at the state’s discretion, as early as the first day of the first calendar quarter in which the state plan amendment was submitted to the HHS Secretary.
The programs implemented in the original four states varied in a number of areas, including their approach to Medicaid asset protection. The Partnership program contained in the DRA will be much more uniform both with other states and with the non-partnership policies within the state. This will assist both producers and consumers to understand and to decide which policy would best meet the needs of each client.
Qualification Requirements
Buyers must be resident of approved state Policy must be federally Tax-Qualified (HIPAA) Must meet specific consumer protection rules in NAIC model act and regulations Must include specific inflation protection based on client age Agents may be required to take specific continuing education to sell Partnership policies Reciprocity and Exchange still being developed
Dollar-for-Dollar Asset Protection
Partnership Programs under the DRA must use Dollar-for-Dollar asset protection models. For every dollar of benefit used, a dollar of assets is added to the amount of assets the state allows to be retained for Medicaid eligibility.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 207
Example:
Each dollar the policy paid in benefits equals one dollar of asset protection.
Person 2 is a policyholder with $200,000 in lifetime savings who bought a Partnership policy covering the same amount of long-term care benefits.
Person 4 might be someone who purchased a non-Partnership policy. When their coverage ran out, and they applied to Medicaid, they received no asset protection and had to spend down to $2,000.
For about the same premium they could have purchased a Partnership policy and kept their $200,000!
Please note: at this point we are purposely ignoring the effect of inflation.
Federally Tax Qualified
All Partnership policies must be Tax qualified policies, which constitute 95% of the market and allow for uniformity in the program nationwide.
Must be Tax-Qualified
Tax-Qualified Policies Non Tax Qualified Policies
Premiums can be included with other uncompensated medical expenses for deductions from income in excess of 7.5% of adjusted gross income up to a maximum amount adjusted for inflation.
Can’t deduct any portion of premiums.
Benefits that you may receive will not be counted as income.
Benefits that you may receive may or may not be counted as income.
The federal law requires you be unable to do 2 of 5 out of 6 possible ADLs without substantial assistance.
Policies can offer different types of benefit triggers. Benefit triggers not restricted to 2 of 6 ADLs.
200,000 0 200,000Person 4
500,000 500,0001,000,000Person 3
0 200,000200,000
Person 2
$0 $50,000$50,000Person 1
Medicaid
Spend Down
Requirement
Partnership
Insurance
Payouts
Assets

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 208
“Medical necessity” can’t be used as a trigger for benefits.
“Medical necessity” and/or other benefit triggers can be offered.
Disability from ADLs must be expected to last for at least 90 days.
Policies don’t require that disability be expected to last for at least 90 days.
For cognitive impairment to be covered, a person must require “substantial supervision.”
Policies don’t have to require “substantial supervision” for cognitive impairments.
Tax Deduction Eligible Long-Term Care Premium Limit by Age Group
The lesser of the following:
The amount paid for that person. The amount shown below – 2008 rates. (Use the person's age at the end of the year.)
Age 40 or younger–$310 Age 41 to 50–$580 Age 51 to 60–$1,150 Age 61 to 70–$3,080 Age 71 or older–$3,850
Source: Pub 535, www.irs.gov
NAIC Model Regulation
All policies must meet specific provisions of the NAIC 2000 model Act and Regulations, which have been adopted by 37 states. Many additional states have enacted legislation mirroring, and sometimes even exceeding, the consumer protection provisions in the NAIC Model Act & Regulations.
‘‘(i) In the case of the model regulation, the following requirements:
‘‘(I) Section 6A (relating to guaranteed renewal or noncancellability), other than paragraph (5) thereof, and the requirements of section 6B of the model Act relating to such section 6A.
‘‘(II) Section 6B (relating to prohibitions on limitations and exclusions) other than paragraph (7) thereof.
‘‘(III) Section 6C (relating to extension of benefits). ‘‘(IV) Section 6D (relating to continuation or conversion of coverage). ‘‘(V) Section 6E (relating to discontinuance and replacement of policies). ‘‘(VI) Section 7 (relating to unintentional lapse). ‘‘(VII) Section 8 (relating to disclosure), other than sections 8F, 8G, 8H, and 8I thereof. ‘‘(VIII) Section 9 (relating to required disclosure of rating practices to consumer). ‘‘(IX) Section 11 (relating to prohibitions against postclaims underwriting). ‘‘(X) Section 12 (relating to minimum standards). ‘‘(XI) Section 14 (relating to application forms and replacement coverage). ‘‘(XII) Section 15 (relating to reporting requirements). ‘‘(XIII) Section 22 (relating to filing requirements for marketing).
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 209
‘‘(XIV) Section 23 (relating to standards for marketing), including inaccurate completion of medical histories, other than paragraphs (1), (6), and (9) of section 23C.
‘‘(XV) Section 24 (relating to suitability). ‘‘(XVI) Section 25 (relating to prohibition against preexisting conditions and
probationary periods in replacement policies or certificates). ‘‘(XVII) The provisions of section 26 relating to contingent nonforfeiture benefits, if the
policyholder declines the offer of a nonforfeiture provision described in paragraph (4). ‘‘(XVIII) Section 29 (relating to standard format outline of coverage). ‘‘(XIX) Section 30 (relating to requirement to deliver shopper’s guide).
NAIC Model Act
‘‘(ii) In the case of the model Act, the following:
‘‘(I) Section 6C (relating to preexisting conditions). ‘‘(II) Section 6D (relating to prior hospitalization). ‘‘(III) The provisions of section 8 relating to contingent nonforfeiture benefits. ‘‘(IV) Section 6F (relating to right to return). ‘‘(V) Section 6G (relating to outline of coverage). ‘‘(VI) Section 6H (relating to requirements for certificates under group plans). ‘‘(VII) Section 6J (relating to policy summary). ‘‘(VIII) Section 6K (relating to monthly reports on accelerated death benefits). ‘‘(IX) Section 7 (relating to incontestability period).
Reciprocity
Reciprocity refers to recognition of partnership policies issued under one state’s program by another state. This allows the insured the ability to receive Medicaid care, services and asset protection in a state other than the one in which the policy was issued.
Agents should clearly explain to purchasers of partnership policies that they may not receive Medicaid asset protection if they move to and apply for Medicaid in another state that has not adopted reciprocity.
Exchanges
Exchanges refer to the consumer’s ability to exchange an older contract with a newer one that provides the partnership protections. Clients who previously purchased a non-partnership policy may have the ability, with the appropriate age required inflation protection, to be allowed to exchange that policy to a new Partnership Plan. Most states have exchange procedures and disclosure forms which agents must use with their clients and applicants.
Continuing Education for Agents
The NAIC consumer protection provisions specify that anyone selling Partnership Policies must have continuing education:

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 210
A one time 8 hour course on LTC insurance in general and curriculum specific to the new Partnership program
A 4 hour refresher course to be taken during each license period The exact requirements and deadlines for training may vary from state to state This may also be approved for CE credit by states
Benefits of Partnership
Both States and Consumers Benefit from Partnership Programs
The partnership allows for both the protection of wealth and the preservation of the Medicaid program. The consumer benefits by receiving quality care and retaining assets for their intended use.
The Partnership concept involves the sale of specified state approved policies that provide long-term care coverage. For every dollar of coverage paid under the policy, the insured can protect a dollar of assets that does not have to be spent or transferred to become eligible for Medicaid.
The asset protection offered through these products provides an incentive for consumers to purchase long term care insurance. This results in additional sales of policies to state residents, which in turn results in state Medicaid savings. It is estimated that for each additional long term care insurance policy sold, Medicaid saves $5,000 and Medicare saves $1,600.
Medicaid Review
A quick review of Medicaid:
How it interacts with LTC Funding Options How Partnership asset protection will help
How Medicaid Works
Within broad national guidelines provided by the Federal government, each state:
Establishes its own eligibility standards Determines the type, amount, duration and scope of services
o Covered services may include: Limited home care benefits, Assisted Living and Nursing Home care
o Non covered services may include: Full time home care, private rooms/nurses and Assisted Living room & board
Sets the rate of payment for services Administers its own program
Policyholders must apply for Medicaid – approval is not automatic when Partnership policy benefits run out

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 211
Mandatory & Optional Benefits
States are required to provide certain basic medical assistance services to eligible recipients including:
Inpatient and outpatient hospital care Health screening Diagnosis and treatment to children Family planning Physician services Nursing facility services to individuals over age 21
States may also elect to cover any of over 30 specified optional services including:
Prescription drugs Clinic services Personal care services and Services provided in intermediate care facilities for the mentally retarded Home and Community Care
Medicaid Payment for Long-term Care
Medicaid will pay for long-term care, but only after individuals have spent down most of their savings and income. To qualify, people are required to deplete their assets to be at or below the state's poverty level. Clients must apply for Medicaid to become eligible for public assistance and must:
Meet the Medicaid definition of disability; Be a citizen or have satisfactory immigration status; and Meet the Medicaid property and asset requirements.
Remember Partnership policies protect assets, NOT income.
Medicaid Certified Facilities
Once a resident is admitted to a Medicaid certified nursing home, however, he/she cannot be evicted simply because of a change from private pay or Medicare to Medicaid.
Although "duration of stay" requirements, i.e., making a resident pay privately for a set period of time, are illegal, nursing homes have a right to review potential residents' finances prior to admission. Having a LTC insurance policy that covers the first couple of years may make it easier for the person to get into the home of their choice to begin with.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 212
Medicaid Enrollees and Expenditures by Enrollment Group
Source: Urban Institute and Kaiser Commission on Medicaid and the Uninsured estimates based on 2003 MSIS data.
Medicaid Spending Aged & Disabled
While three-quarters of the program’s enrollees are children and adults, this group represents less than one-third of all program spending.
The aged and disabled represent a much smaller share of the enrollees but they utilize more (and more costly) acute and long-term care services and represent about 70 percent of program spending. With the current trends in demographics this will become even more lop-sided in the future.
Asset & Income Eligibility
To be eligible for Medicaid benefits a nursing home resident may have no more than:
$2,000 in “countable” assets and approximately $30-$40 in monthly income.
The spouse of a nursing home resident, called the “community spouse”, is limited to:
A percentage of the couple’s joint assets up to $104,400 in “countable” assets (2008) up to $2,610 per month of income (2008).
These figures vary by state and change each year to reflect inflation These are the maximum amounts allowed nationwide.
Income paid to a spouse and someone else, is assigned proportionately to the spouse. If there is no written document establishing ownership of the income, it is considered to belong equally to both spouses.
Enrollees Expenditures on benefits
Children 18%
Elderly 28%
Disabled 42%
Adults 12%
Children 49%
Elderly 11%
Disabled 14%
Adults 26 %
Total = 55 million Total = $234 billion

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 213
Income & Medicaid Eligibility
States also impose income limits that must be met in order for an individual to qualify for Medicaid long term care benefits. The new Partnership rules do not change this requirement nor do they change what services Medicaid pays for.
New provisions in DRA – Income First Method must be used before allowing more assets to be retained under hardship provisions. This means it will be harder for the community spouse to keep additional amounts of assets.
Asset Protection & Medicaid Eligibility
Example:
The following example illustrates the advantages of a Partnership policy. Let's say John is a single man who purchases a Partnership policy with a lifetime maximum of $100,000. John eventually requires long-term care, becomes eligible for benefits, exhausts his policy benefits, and applies for Medicaid. If John's policy was not a Partnership policy, in order to qualify for Medicaid, he would be entitled to keep only $2,000 in assets, which the state would also recover from his estate after his death. However, because John bought a Partnership policy, when he exhausts his policy benefits and applies for Medicaid, he can keep $102,000 in assets and the state will not recover those funds after John's death. Any assets John had over and above the $102,000 would have to be spent in order for him to be eligible for Medicaid.
Transfer of Property & Estate Recovery Under the DRA
There are new rules in DRA regarding start of Look-Back period as well as the length of the look back period.
Spousal Transfers – no look-back period Non-Spousal Transfers – 60 month look-back
These new provisions are being phased-in by the states.
There are also stricter rules regarding transferring property to another person, trusts, annuities, etc. in order to obtain Medicaid assistance. OBRA ‘93 made the penalty period unlimited in duration.
Reduced ability to use “Medicaid Planning” More incentive to purchase LTC Insurance
Penalty Period Changes Under the DRA
The DRA makes two substantive changes in how the penalty is assessed.
First, states were previously required to have a three-year look-back period for prohibited transfers and the DRA changes this to five years.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 214
Second, the start of the penalty is changed from the date that an asset transfer is made to the date that an individual otherwise would have become eligible for Medicaid.
The DRA also requires states to eliminate rounding down when determining the penalty period and it allows them to view many transfers in different months as one, large transfer, on which to base their calculations.
Penalty Example
Before DRA
Mr. Smith transferred $500,000 to a son 25 months prior to applying for Medicaid Serves penalty from the 25th to the 36th month, inclusive.
After DRA
Starts serving penalty on the date he applies for Medicaid With OBRA 93 in place (no limit on length of penalty), he would be ineligible for actual
number of months. ($500,000/$5,031=99 months)
Treatment of Annuities under the DRA
Annuities are financial instruments where a sum of money is transferred to the control of a financial institution that agrees to pay out a predetermined amount of money on a regular basis for the life of the owner of the annuity or for a predetermined period.
Prior to the DRA, annuities were often treated as unavailable assets, and not subject to a penalty. The DRA changes the treatment of annuities.
Annuities are treated as prohibited asset transfers subject to a penalty, unless:
The Medicaid applicant discloses the existence of annuities and They name the state as primary beneficiary of the remainder (at death of the
annuitant) for at least the value of Medicaid assistance provided.
Consideration of Income and Resources from an Annuity
The State may take into consideration the income or resources derived from an annuity when determining eligibility for medical assistance or the extent of the State’s obligations for such assistance.
This means that even if an annuity is not penalized as a transfer for less than fair market value it must still be considered in determining eligibility for Medicaid, including spousal income and resources, and in the post-eligibility calculation, as appropriate.
In other words, even if an annuity is not subject to penalty under the provisions of the DRA, this does not mean that it is excluded as income or resource.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 215
Partnership Medicaid Asset Protection
Insured is able to use benefit for any covered services and in any covered facility, anywhere in the US. Unlike property which was “exempt” for Medicaid eligibility, however, these assets are truly “protected”. They are not subject to estate recovery and can be passed to heirs upon the policyholder’s death
The amount of this asset protection, at any time, is equal to the sum of all benefit payments made for their care by this policy. Should they later apply for Medicaid or for other qualifying public long-term care benefits, they will not be required to expend these protected assets before becoming eligible.
Their protected assets will also be exempt from any claim the State may have against their estate to recover the cost of State-paid long-term care or medical services provided to them. This permanent asset protection is over and above the asset amounts Medicaid normally exempts for eligibility.
How Medicaid Asset Protection Works
When a claim is filed for covered long term care services they will be covered just like they would under any other qualified LTC policy.
The Added Benefit with Partnership Protection
If and when coverage runs out and care is still needed, policyholders can apply to Medicaid and keep one dollar of assets for every dollar that the policy paid in benefits
Medicaid Estate Recovery
Federal Law requires the State to recover against the estates of deceased Medicaid Beneficiaries (including their homes):
Anyone who received any nursing home care Any expenses incurred after age 55
The ER is barred from claiming:
during the lifetime of a surviving spouse; when there is a surviving child who is under the age of 21; when there is a surviving child who is blind or disabled.
If an individual has property (e.g., house, car, etc.) and/or assets that were exempt during the eligibility process the property or assets are NOT protected during estate recovery.
Upon their death, the State Medicaid Recovery Unit can place a lien and/or claim against the entire estate of the deceased for expenses incurred by the Medicaid program to recover those costs paid by the state.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 216
If the individual was married, a lien would not usually be placed until the remaining spouse dies or sells the property. Upon the death of the surviving spouse, ER may present a claim against the surviving spouse’s estate to collect the amount of Medicaid paid services provided to the predeceased spouse or the value of the assets received by the surviving spouse, whichever is less. Additionally, the ER claim is solely against the assets of the decedent, not against the personal assets of the heir(s).
In accordance with these and other statutes, the person responsible for the administration or disposal of the estate assets is required to notify Medicaid of the death of any individual who has or may have received Medicaid benefits.
Once notification of death is received, ER identifies those services or premiums paid for by Medicaid after the decedent’s 55th birthday. A claim is prepared reflecting these costs and is presented to the party handling the estate. The ultimate collection of the claim is limited to the lesser of the value of the estate assets or the amount of Medicaid paid services.
ER will reduce its claim by the amount of insurance benefits received under Partnership insurance policies.
State Partnership Long-Term Care Insurance Programs
Partnership Goals
Education Affordability Ease the burden of costs
Education
This program was implemented to help people understand the risks and costs of long term care. This program provides education to consumers and special support to insurance agents in an effort to help individuals realize their potential risk of needing LTC and how high quality LTC insurance provides a viable option for funding these costs.
Most People do not understand the Costs and Risks of LTC
In many surveys seniors state that they already have insurance to cover long-term care expenses because they misinterpreted the language of their health insurance policies. Be sure to point out to them that Medicare, Medicare Supplements and Health insurance only cover skilled nursing care and do not cover custodial care, the type of care most people need. If they are in doubt, have them get out their policy and go over it together pointing out exclusions and limitations.
Affordability
One of the main purposes of the Partnership Program is to help individuals plan ahead to meet their needs for nursing home or community care without fear of impoverishment and to motivate them to purchase high quality long-term care (LTC) insurance.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 217
Ease the burden of costs
The Partnership program was established as a public/private partnership to address the anticipated fiscal challenges that will be caused by the financial burden of long-term care in the twenty-first century.
Program Overview
The Partnership for Long Term Care is a public/private alliance between State governments and insurance companies. It was originally funded with $14 million in grants from the Robert Wood Johnson Foundation and now all four original State programs are now fully funded under their states' budgets. The program joins Medicaid with private Long Term Care insurance.
This program consists of Long Term Care insurance companies and states working in cooperation in order to create plans that are lower in cost and can provide better protection against impoverishment than those commonly offered today. An important and attractive feature of these plans is that once private insurance benefits are exhausted, special Medicaid eligibility rules are applied if additional coverage is necessary.
One of the major goals of these programs, are to encourage consumers to take responsibility for financing their long term care by purchasing insurance policies thereby alleviating the growing problem of persons transferring assets in order to be eligible for Medicaid coverage.
The insurers who participate in this program have certain, specific responsibilitiesand program standards. Participating Long Term Care policies must be of high quality. Among the standards required in each State are inflation protection, minimum benefit amounts, and agent training. Participating insurers are also required to provide the State with information on who is buying certified Partnership products and on the utilization of benefits.
Original Four States Partnership Models
The “Long-Term Care Partnership Program” was launched in 1987 in four states; California, Connecticut, Indiana and New York. Partnership policies explicitly offer purchasers partial or total asset protection from Medicaid means-testing requirements.
To date, results show that the profile of purchasers is relatively healthy and well-off, with about half of policyholders analyzed in three states reporting total assets greater than $350,000, and monthly incomes of $5,000 or greater. Both in design and in premium cost, Partnership policies in the four states differ significantly.
For example, in Connecticut, a comprehensive policy providing three years of coverage ($200/day for nursing home coverage and $200/day for community services, with a 90-day waiting period, and 5 percent inflation protection) costs $4,100 per year if purchased at age 65. By comparison, in New York, a typical policy (three years of nursing home care at $180 per day and six years of community-based care at $90 per day, with a 100-day waiting period and 5 percent inflation protection) costs $2,587 per year if purchased at age 65.59 Under the DRA, Partnership policies can now be sold in all states, and limited federal guidance for development of these policies has been issued.60

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 218
59 U.S. Govt. Accountability Office, GAO-05-1021R “Long-Term Care Partnership Program (Sept. 2005). http://www.gao.gov/new.items/d051021r.pdf Retrieved on June 21, 2006. 60 Centers for Medicare and Medicaid Services (2006). “Qualified Long-Term care Partnerships Under the Deficit Reduction Act of 2005” (July). http://www.nsclc.org/news/06/07/dra/LTCEnclosure%20.pdf Retrieved on July 30, 2006.
Three distinct asset protection models have emerged as outlined below. The models are similar in several respects but differ in the way Medicaid eligibility rules are altered. The following is a short synopsis of each.
Dollar-for-Dollar Model. After meeting a stringent set of criteria, Long Term Care insurance policies of varying length and scope are certified by the State insurance division. Partnership policies must cover at least one year at inception and pay a minimum per day benefit (different in each State). Once the benefits of the policy are exhausted, an application for Medicaid can be made using special eligibility rules. Every dollar paid out by an insurer through a Partnership policy will be deducted from the resources counted toward Medicaid eligibility. For instance, if a person receives $80,000 of Partnership insurance benefits, then $80,000 of assets will be protected in the Medicaid eligibility process. Once on Medicaid, an individual's income is devoted to the cost of care.
Total Assets Model. After meeting somewhat different criteria, Long Term Care insurance policies are certified by the State insurance department. Partnership policies must cover three years of nursing home care or six years of home health care. Policies must also pay a minimum per day benefit. Once the benefits of a Partnership policy are exhausted, the individual's assets will not be considered for Medicaid eligibility. Protection will be granted for all assets, but an individual's income must be devoted to the cost of care.
Hybrid Model. After meeting a stringent set of criteria, Long Term Care insurance policies of varying length and scope are certified by the State insurance division. Partnership policies must cover at least one year at issue and pay a minimum per day benefit. The initial amount of coverage purchased, and then later used, determines whether the policyholder earns "Dollar-for-Dollar" or "Total Asset" protection. If the initial amount of coverage purchased is equal to or more than, the State-set dollar amount in effect (for the policy effective year), then once the benefits of the policy are exhausted, assets are not considered in determining Medicaid eligibility. If the initial amount of coverage purchased is less than the State-set dollar amount, then every dollar paid out under the policy will be deducted from the resources counted toward Medicaid eligibility. Regardless of the type of asset protection earned, an individual's income must be devoted to the cost of care.
Omnibus Budget Reconciliation Act (OBRA) 1993
In 1993 federal law (OBRA) discouraged the further expansion of long term care insurance partnerships to additional states. States were prohibited from disregarding assets from estate recovery, one of the key elements in Partnership programs
The OBRA ‘93 contained language with direct impact on the expansion of partnership programs. The Act recognized the four initial state Partnership programs plus a future program in Iowa and a modified program in Massachusetts. These states were allowed to operate their Partnerships as planned because they had State plan amendments approved by Health and Human Services prior to May 14, 1993.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 219
States obtaining a State plan amendment after May 14th, 1993 could proceed with Partnership programs. However, they must also recover from the estates of all persons receiving services under Medicaid. The result of this language is that the asset protection component of the partnership was in effect only while the insured is alive. After the participant dies, the State must recover from their estate (including protected assets), the amount that Medicaid spent for the care of the individual. (The six states mentioned earlier are exempt from this requirement. This means that in the operational Partnership programs - CA, CT, IN, and NY - asset protection exists during Medicaid eligibility and also from Medicaid estate recovery efforts.)
OBRA also cites Partnership programs in its requirements for how "estate" shall be defined. States offering a Partnership program must use the specific definition of estate outlined in the law for Partnership participants.
Current Programs History & Success
Residents in four states are eligible to participate in a special public/private program that joins private long-term care insurance with Medicaid. The purpose of the program is to make the purchase of shorter term more comprehensive long-term care insurance meaningful by linking special policies (Partnership policies) with Medicaid. Partnership policies must meet special requirements that differ somewhat from state to state. Most states require that Partnership policies offer comprehensive benefits (cover institutional and home services), are Tax Qualified, and include an annual 5 percent compound Inflation Protection feature. Other aspects of the program are different from state to state.
Purchasers of these Partnership policies are allowed to retain a greater share of their assets should they need to apply for Medicaid after using their long-term care insurance benefits. States use different methods for determining the amount of assets participants can keep. If participants need to apply for Medicaid they will not be required to “spend down” to the same asset levels as those who did not purchase and use a Partnership policy. The following information is a general overview of the program. The state Partnership office or SHIP program can complete information.
A Short Summary of the Partnership Program in the Original RWJ Partnership States
In 1987, under a demonstration project funded by the Robert Wood Johnson Foundation 4 states: California, Connecticut, Indiana, and New York, developed partnership programs. The original four varied in a number of areas, including their approach to Medicaid asset protection. They were designed to encourage the purchase of private long-term care insurance, thereby potentially reducing future reliance on Medicaid as a funding source for long-term care services.
California
The California Partnership Program markets its product to individuals through agents, as well as to state employees and retirees as a benefit option via the California Public Employee Retirement System (CalPERS). Partnership policies sold in California must be Tax Qualified and meet a host of other regulatory requirements including an annual 5 percent compound inflation feature. Policies sold under this program must provide at least one year of long-term care coverage and must provide comprehensive benefits (institutional and home-based).

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 220
California allows Partnership participants to keep one dollar for every dollar of insurance benefits payments made on their behalf.
Connecticut
Connecticut Partnership policies are offered to individuals through insurance agents and to state employees through group insurance. Connecticut allows Partnership participants to keep one dollar for every dollar of insurance benefits payments made on their behalf. Partnership policies sold in Connecticut must be Tax Qualified and must include an annual 5 percent compound inflation feature. Policies must also provide at least one year of comprehensive benefits (institutional and home based). The Connecticut Partnership also offers a variety of Internet resources for long-term care planning in general and for the Partnership in particular.
Indiana
The Indiana Partnership uses two methods for determining the amount of assets that participants are allowed to keep.
It uses a Dollar-for-Dollar approach in which participants are allowed to keep one dollar of assets for every dollar of insurance benefits payment and a Total Assets approach in which participants buying a policy that meets or exceeds a specified minimum level are allowed to keep all their assets.
Partnership policies sold in Indiana must be Tax Qualified. Indiana Partnership policies must cover at least one year of benefits for those selecting the Dollar-for-Dollar approach and at least four years for those selecting the Total Assets approach. Participants selecting either approach must purchase policies that provide comprehensive benefits (institutional and home-based) and with a 5 percent annual compound inflation feature.
Data from Indiana suggest that when consumers are given the incentive of total asset protection, they are likely to purchase more insurance coverage. Prior to 1998, when Indiana introduced total asset protection as an option in addition to dollar-for-dollar asset protection policies, only 29 percent of policies purchased had total coverage amounts large enough to trigger total asset protection. In contrast, in the first quarter of 2005, 87 percent of policies purchased were large enough to trigger total asset protection.
New York
The New York Partnership used a Total Assets approach to determine how much of their assets participants are allowed keep and qualify for Medicaid. Participants must purchase a minimum of three years of institutional coverage (six years home care) to qualify as a Partnership policy. The policy must be Tax Qualified and must also include a 5% compound inflation protection feature. However, they now use a hybrid model.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 221
Long-Term Care Partnerships
Fast Facts
The Robert Wood Johnson Foundation initiated a demonstration program in 1987 to develop an innovative private-public Long-Term Care Partnership Program. California, Connecticut, Indiana and New York set up programs, and still operate them.
In 2006, Medicaid officials in 22 states reported that they were planning to implement such programs.
Among the goals of the Partnership program are to increase the number of middle-income people buying long-term care insurance policies, to help people buy better long-term care insurance policies, and to reduce cost growth in Medicaid.
Buying a Partnership policy that provides a certain dollar amount of benefits will allow the purchaser to disregard assets equal to the insurance payout in applying for Medicaid once the insurance coverage is exhausted.
Premiums for Partnership policies differ across states and are based on an applicant’s age, medical history and the scope of benefits purchased.
Sales of Partnership policies in the four original states opening programs have been relatively modest—249,000 since the Partnerships began, of which 201,000 policies were in force in 2006.
Source: AHIP - March 2007
Today’s patchwork of private and public financing of long-term care services is strained, with costs rising for the major payer—the federal-state Medicaid program—and for families of the individuals receiving services.
These cost pressures will only get worse. Between 2005 and 2030, when the youngest baby boomers reach retirement, the population of those age 65 and older will almost double from close to 37 million to more than 71 million, and will comprise almost 20 percent of the U.S. population.
Long-term care costs can be financially devastating for people with modest incomes. In 2006, the average annual cost of nursing home care was $75,190, and exceeded $100,000 in some areas. Paying for home care can also be expensive, at an average of $19 per hour in 2006.
Individuals and their families often assume, or hope, that Medicaid will pick up these costs when the time comes. They may be shocked to learn that persons seeking Medicaid help must usually spend almost all of their life savings on care before they qualify for Medicaid.
Private LTC Insurance
Private long-term care insurance could pay for many long-term care expenses. Yet today, private insurance accounts for only a small fraction of long-term care spending on the elderly—an estimated 3 percent in 2005.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 222
Some possible reasons why:
Private insurance for long-term care is a relatively recent insurance product. And many policies purchased years ago have not yet begun to pay benefits, so they don’t yet show up in statistics measuring sources of long-term care spending.
Many older people believe that Medicare covers long-term care. Some are unaware of their long-term care risks or deny any need to prepare financially
for those risks. Policies are expensive. Studies indicate that only 10 to 20 percent of the older
population can afford good quality private long-term care policies.
Long-Term Care Partnership Programs
The Long-Term Care Partnership Program was designed to encourage the purchase of private long-term care insurance. In states where the program is offered, individuals who purchase a policy and use up its benefits can then apply for Medicaid. If these individuals meet Medicaid’s criteria for income and degree of impairment, they can receive Medicaid-covered long-term care services while protecting some or all of their financial assets that would otherwise make them ineligible under Medicaid’s means testing requirements.
This arrangement is a “dollar-for-dollar” Partnership. The amount of protected assets equals the amount that the private insurance policy has paid out. Assets that may be protected under Partnership policies include assets Medicaid would otherwise require to be “spent-down”, such as cash savings, securities and most property, among other items. Partnership programs do not shelter income, such as Social Security and pension income.
Post-DRA: Changes in the Partnership Program
For more than a decade, federal rules discouraged states from adopting Partnership programs, because they required states to pursue estate recovery of Partnership-protected assets after a beneficiary’s death. But in 2005 Congress gave states the green light to adopt Partnerships as part of the Deficit Reduction Act (DRA). Following enactment of the DRA many states have decided to implement a program.
The DRA establishes a basic framework within which states must operate. A “qualified state partnership” is defined as an approved state plan amendment offering dollar-for-dollar asset protection.
During the next few years, decisions at the state level will affect whether and how insurers create Partnership products in many more states, and how consumers will react to them.
In fact, any new Partnership programs are likely to vary considerably from state to state. This may create problems for consumers who purchase a policy in one state and later move to another.
The Department of Health and Human Services (HHS) is charged with establishing a framework for reciprocity—a mechanism for one state to recognize how Partnership policies written in another are treated. But states can opt out of these standards simply by informing the HHS secretary.
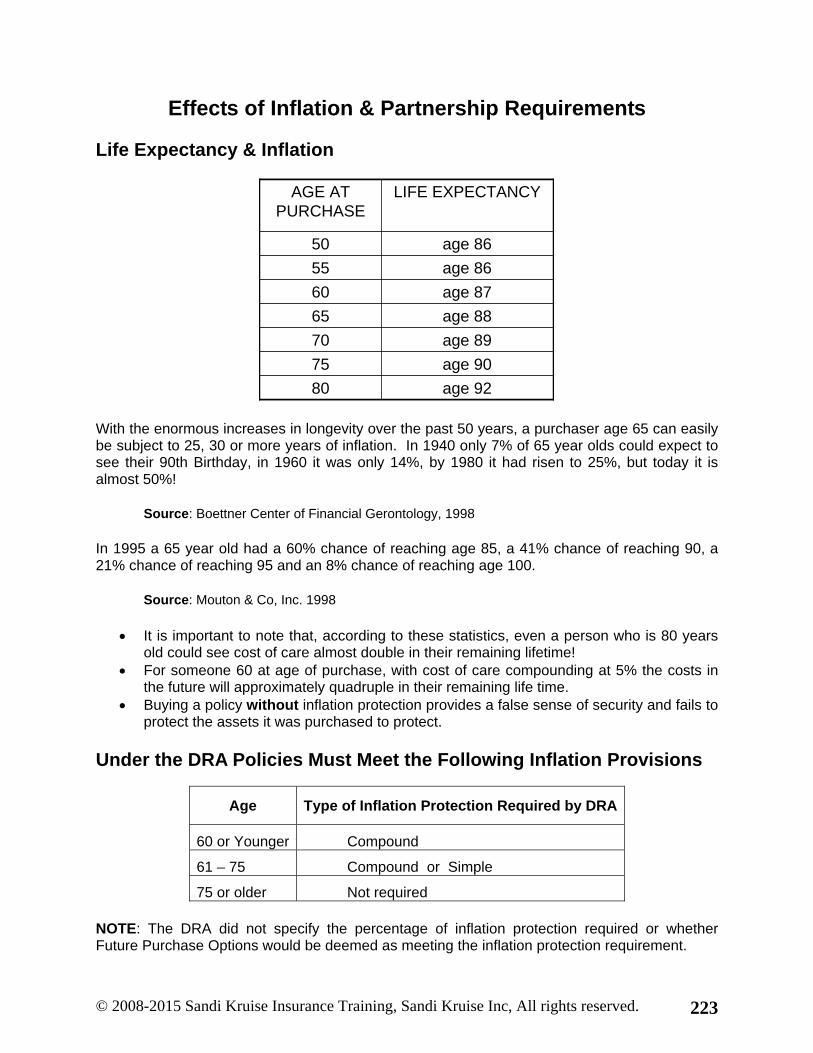
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 223
Effects of Inflation & Partnership Requirements
Life Expectancy & Inflation
age 9280
age 9075
age 8970
age 8865
age 8760
age 8655
age 8650
LIFE EXPECTANCYAGE AT PURCHASE
age 9280
age 9075
age 8970
age 8865
age 8760
age 8655
age 8650
LIFE EXPECTANCYAGE AT PURCHASE
With the enormous increases in longevity over the past 50 years, a purchaser age 65 can easily be subject to 25, 30 or more years of inflation. In 1940 only 7% of 65 year olds could expect to see their 90th Birthday, in 1960 it was only 14%, by 1980 it had risen to 25%, but today it is almost 50%!
Source: Boettner Center of Financial Gerontology, 1998
In 1995 a 65 year old had a 60% chance of reaching age 85, a 41% chance of reaching 90, a 21% chance of reaching 95 and an 8% chance of reaching age 100.
Source: Mouton & Co, Inc. 1998
It is important to note that, according to these statistics, even a person who is 80 years old could see cost of care almost double in their remaining lifetime!
For someone 60 at age of purchase, with cost of care compounding at 5% the costs in the future will approximately quadruple in their remaining life time.
Buying a policy without inflation protection provides a false sense of security and fails to protect the assets it was purchased to protect.
Under the DRA Policies Must Meet the Following Inflation Provisions
Age Type of Inflation Protection Required by DRA
60 or Younger Compound
61 – 75 Compound or Simple
75 or older Not required
NOTE: The DRA did not specify the percentage of inflation protection required or whether Future Purchase Options would be deemed as meeting the inflation protection requirement.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 224
Since most people will not access benefits under their policy for many years. Inflation protection is important so that the value of the benefit remains meaningful when the benefit is needed. Remember the asset protection will grow along with the benefit amount since the assets protected are the same amount as the benefits paid out.
Policies sold to individuals who are 60 or younger must provide compound annual inflation protection
Policies sold to individuals 61-75 must provide some level of inflation protection o Compound – no % specified o Simple – no % specified o Future Purchase Option (may or may not be allowed)
Policies sold to individuals 76 or older do not require inflation protection, however companies may still offer it
Case Studies Regarding Buy-Up vs. Automatic Inflation Protection
One 65 year old purchases a daily benefit of $100 with 5% compound inflation protection at an annual premium of $1,101 which remains level throughout the lifetime of the policy.
Another 65 year old purchases a policy with a FPO rider with will also increase at 5% compounded, for an annual premium of $629 per year.
The third 65 year old purchases a policy with $200 per day benefit and no inflation protection for a premium of $1,139 per year.
At this point the Future Purchase Option seems like the best choice with the lowest premium, but—
Let’s see how they compare at the end of 10 years:
The first person with prefunded inflation guard has a daily benefit of $163 per day and the premium is still $1,101.
The man with the FPO policy also has a benefit of $163 per day, but his premium is now $1,185 per year.
The third man, with no inflation protection still has $200 per day in benefit and his premium is still $1,139.
Even at the 10 year mark, the premiums are not that far off and the FPO policy still looks like a good deal but—
At the end of 20 years:
The first person now has a daily benefit of $265 and premium of $1,101 per year. The second person’s benefit is also $265 but his premium has soared to $3,925 per
year! And the third person still has $200 per day with a premium of $1,139.
Since coverage won’t be needed for 14 years or more, automatic inflation protection comes out ahead.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 225
Since one of the primary reasons for purchasing the coverage is to protect assets, an insured with inadequate limits will end up spending the assets they sought to protect to pay the difference between what the policy covers and the cost of their long term care. This is especially true in states that require the complete exhaustion of benefits before Medicaid will pay.
The differences are not nearly as dramatic in the first 10 years as they are in twenty. This is a good example of why most states require that agents use charts and examples showing at least 20 years when describing the effects of inflation on coverage and premium.
Buy-up Options (Future Purchase Options) on LTC are similar to Term Life Insurance. You get a lot of current protection for a small initial premium. This works well for covering a specific short-term obligation (such as a mortgage). However, using either to cover an event that is 20-30 years or more in the future is risky since by the time people actually need the coverage it can be so expensive that it has lapsed or has not kept up with inflation.
Compound vs. Simple vs. No Inflation Protection
Case Study about Inflation Protection
James and Robert are both 65-years-old and in good health. They both buy long-term care insurance policies on the same day in 2006.
James buys a Partnership policy that includes inflation protection that increases benefits by 5 percent a year, compounded.
Robert buys non-partnership long-term care policy without built-in inflation protection.
Both of their policies have a total benefit limit of $138,700 ($190 daily benefit), which in 2006 is enough to pay for about two years of nursing home care. If they were to need long-term care within a few months, their policies would pay for $138,700 in long-term care.
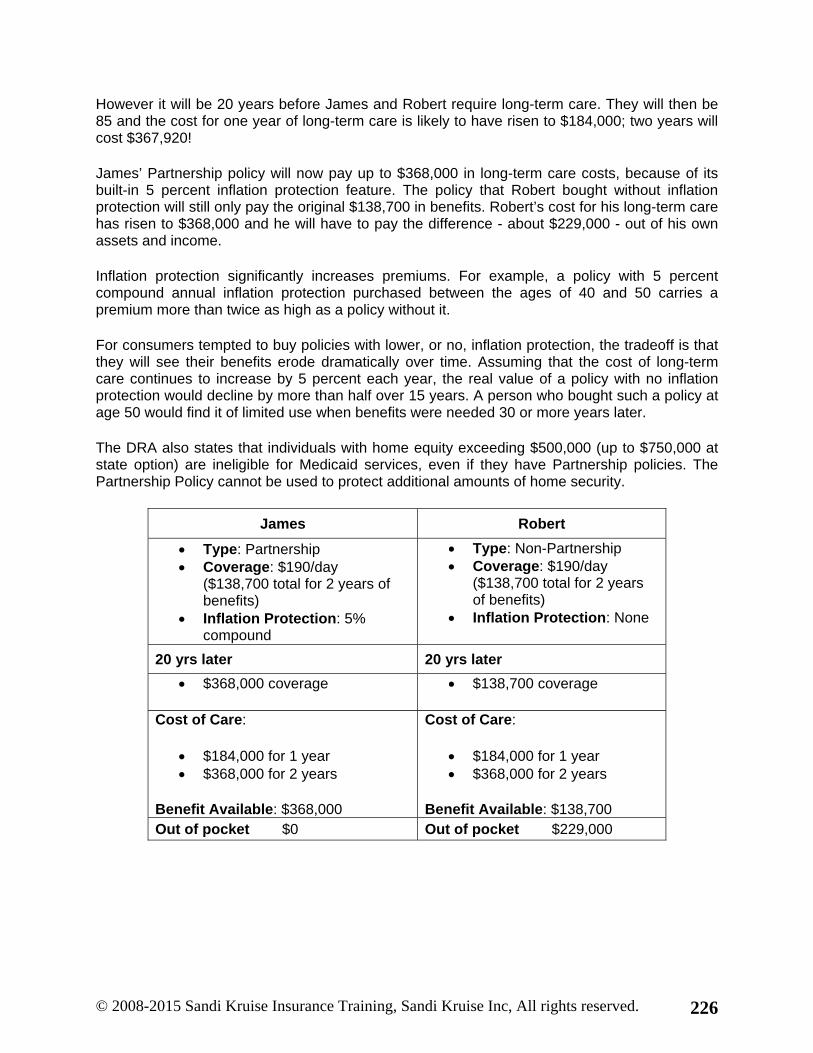
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 226
However it will be 20 years before James and Robert require long-term care. They will then be 85 and the cost for one year of long-term care is likely to have risen to $184,000; two years will cost $367,920!
James’ Partnership policy will now pay up to $368,000 in long-term care costs, because of its built-in 5 percent inflation protection feature. The policy that Robert bought without inflation protection will still only pay the original $138,700 in benefits. Robert’s cost for his long-term care has risen to $368,000 and he will have to pay the difference - about $229,000 - out of his own assets and income.
Inflation protection significantly increases premiums. For example, a policy with 5 percent compound annual inflation protection purchased between the ages of 40 and 50 carries a premium more than twice as high as a policy without it.
For consumers tempted to buy policies with lower, or no, inflation protection, the tradeoff is that they will see their benefits erode dramatically over time. Assuming that the cost of long-term care continues to increase by 5 percent each year, the real value of a policy with no inflation protection would decline by more than half over 15 years. A person who bought such a policy at age 50 would find it of limited use when benefits were needed 30 or more years later.
The DRA also states that individuals with home equity exceeding $500,000 (up to $750,000 at state option) are ineligible for Medicaid services, even if they have Partnership policies. The Partnership Policy cannot be used to protect additional amounts of home security.
James Robert
Type: Partnership Coverage: $190/day
($138,700 total for 2 years of benefits)
Inflation Protection: 5% compound
Type: Non-Partnership Coverage: $190/day
($138,700 total for 2 years of benefits)
Inflation Protection: None
20 yrs later 20 yrs later
$368,000 coverage $138,700 coverage
Cost of Care:
$184,000 for 1 year $368,000 for 2 years
Benefit Available: $368,000
Cost of Care:
$184,000 for 1 year $368,000 for 2 years
Benefit Available: $138,700 Out of pocket $0 Out of pocket $229,000

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 227
Has the Partnership Program Fulfilled Its Promise?
Some experts believe that the Partnership program has made progress toward meeting its goals. For example, the original four states have been modestly successful in promoting higher quality insurance products with inflation protection. As of mid-2006, about 240,000 Partnership policies had been sold, and about 194,000 were in force.
Service Utilization
As of June 30, 2006, the breakdown of the major types of services cumulatively accessed by the policyholders includes:
10% - Skilled Nursing Facility 25% - Assisted Living Facility/RCF 13% - Home Health Aide 22% - Attendant/Personal Care 1% - Homemaker/Chore Services >1% - Adult Day Care
Source: CPLTC Quarterly Report, 2nd qtr 2006
Partnership policies are providing LTC options and choices for middle-income persons that they might not otherwise have had.
Only 10% of benefits have been used for Skilled Nursing Facilities whereas 24% of benefits have been paid for assisted living and over half of all benefits have been paid for home and community care which is not covered adequately by any other type of insurance or government program. This shows that people prefer to get care in the home and community, if they have the funds to pay.
Partnership Experience
The Long-Term Care Partnership Program seems to be succeeding in eliminating participants’ need to access Medicaid. Less than 1% of partnership policyholders are currently accessing their LTC insurance benefits.
Since the programs began, only 251 policyholders in all four states have exhausted their long-term care insurance benefits. More policyholders have died while receiving long-term care insurance benefits (899 policyholders) than have exhausted their long-term care insurance benefits (251 policyholders). Of those only 175 have accessed Medicaid.
Source: http://www.rwjf.org/index.jsp

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 228
Long-Term Care Partnerships—Experience from Implementation to 2006
But although sales increased initially each year when the programs were launched, they later leveled off. (In California, growth was significantly higher and peaked later, in 2003). These Partnership policies represented a small fraction of the total number of long-term care policies sold in the four states.
Another goal of the Partnership program is to attract moderate-income purchasers, those most in danger of exhausting their savings and other assets in order to qualify for Medicaid. Here, too, the record in the four states shows mixed results.
Although some purchasers have modest incomes, the policies appear to have attracted wealthier buyers. In the three states that have surveyed a sample of Partnership policyholders—California, Connecticut and Indiana—the majority reported their total assets were greater than $350,000. Roughly half of the policyholders in each of these three states also reported average monthly household incomes of greater than $5,000.
Although most Partnership applicants have been able to purchase insurance, 16 percent of individuals who applied were denied coverage during the medical underwriting process, during which private companies assess the health and future risk, or “insurability,” of individual applicants.
With regard to the cost impact on Medicaid, it is still difficult to assess whether the Partnerships will make much of a dent. The typical lag between when a policy is purchased and benefits are exhausted can be decades. Through 2006, fewer than 4,000 Partnership policyholders had claimed benefits, and only 175 had accessed Medicaid after exhausting their Partnership benefits.
Partnership directors, however, assert that their programs have already produced savings for Medicaid and, indeed, some factors point in this direction. Policyholders who access their private insurance benefits, for example, do not tend to exhaust them (they are more likely to die while receiving the private benefit than to access Medicaid).
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 229
Will States Seek to Make Further Improvements?
Consumers purchasing Partnership policies or any other type of long-term care insurance policy face complex decisions. They need to understand the scope and flexibility of covered benefits, minimum daily benefit amounts, elimination periods (sometimes called waiting periods or deductibles), inflation protection and whether to include non-forfeiture features (which pay out benefits even if the policy lapses).
Unfortunately, some of the key terminology in policies varies from company to company. This creates extra challenges for consumers, who may not clearly understand the consequences of their choices. Moreover, many purchasers are likely to rely on the advice of agents, who have their own interests and may not be particularly well informed about how long-term care insurance relates to Medicaid. This is the reason why the DRA requires all agents who market or sell LTC insurance to obtain education on long-term care in general and Partnership LTC in particular.
The National Association of Insurance Commissioners calls for insurers to offer “meaningful” inflation protection—e.g., through policies featuring 5 percent compound annual inflation. However, the DRA allows states to determine the type and amount of inflation protection required.
Responsibilities, Suitability & Ethical Concerns
Agent Responsibilities
To Understand and Explain to Clients: o The difference between Partnership and non-Partnership policies o How the product interacts with Medicaid o The various benefit choices o The various inflation protection choices o Disclosure documents o The suitability and affordability of purchase
Maintain required continuing education
NAIC Model Suitability Standards Apply
Policy summary Suitability Guidelines Suitability Worksheet No unnecessary replacements Affordability Individual plan to suit clients LTC
goals
Disclosure Materials
Outline of Coverage Inflation Protection Buyers Guide(s) Medicaid Eligibility Disclosure Replacement Disclosure (if
applicable) Partnership or non-Partnership
Disclosures Other Materials required by each
state

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 230
Each state will specify what types of disclosures must be made to applicants, what form the notice must use, and at what time during the sales cycle they must be provided.
Most states will require the agent to deliver a copy of a shopper’s guide to the proposed insured, which may be the one published by the NAIC or one that is state specific, or possibly both. States and companies may require additional brochures and notices.
Agents will also usually be required to provide the insured with an outline of coverage, as well as charts and information regarding inflation protection.
Affordability and Suitability
Asset protection makes Partnership Policies more affordable. In the past the only way to get lifetime asset protection was to buy a lifetime policy. This was too expensive for most people. With the partnership the consumer can buy a shorter, more affordable policy and still get lifetime asset protection. The protection offered by the Partnership provides an especially strong incentive for those most at risk of depleting their resources when the need for care arises.
Middle-income elderly generally have fewer assets to protect and are less able to afford lengthy benefit periods of four years or more. They are also the most likely candidates to spend down to the poverty level to qualify for Medicaid. In fact, 20 to 25 percent of all those who enter nursing homes today as private payers, end up on Medicaid. The extra protection offered by the Partnership program makes purchasing protection more meaningful and more affordable to these persons.
The Partnership provides relatively affordable life long protection with the purchase of shorter-term policies. After that, Medicaid will be available to pay for the remainder of their LTC expenses.
For policies with built in automatic inflation protection, premiums are level and once purchased will remain at the purchase age for the remainder of the life of the policy. Level premiums can still be increased for an entire class of policy holders.
Reasons People Buy LTC Insurance
Asset protection To maintain their independence and dignity Not to become a burden on their spouse or loved ones Access to the types of care and the care settings of their choice
With a Partnership policy even people with moderate levels of assets and income can attain these important goals.
Partnership Features Focus on the Reasons People Purchase LTC
With a Partnership policy in place, together with a loving and caring support system, seniors have a much better chance of getting the care they need, while preserving their dignity and freedom of choice.
© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 231
Remember, LTC insurance is just one part of their overall plan.
It doesn’t replace family caregivers It makes it easier for their family to care for them longer at home
Partnership Plan Design
Factors to Consider When Designing an Appropriate Plan with the Partnership:
The amount of assets the client wishes to protect An adequate benefit per day for care
The benefit period will be determined by dividing the amount of assets by the daily nursing facility benefit amount then rounding to the closest number of years of coverage available.
Asset Protection & Plan Design
Clients can purchase coverage equal to all their assets, or only some of their assets. The amount they buy is up to them. Remember, if clients buy less coverage than the assets they currently have, the inflation protection feature of the policy will increase their asset protection each year. If the value of their assets is also increasing the coverage might not keep up.
After they own the policy for approximately 14 years, the amount of asset protection they bought will have approximately doubled. They will have twice as much asset protection as they purchased originally.
If, however, the value of their assets at the time of application for Medicaid or their death exceeds the asset protection of their Partnership policy, the additional amount will be subject to spend down before eligibility or estate recovery at the time of their death.
Short & Fat Partnership vs. Long & Lean Non-Partnership
Some clients and agents feel that the best type of coverage is a policy with the largest benefit period – even if they need to reduce the daily benefit to afford it. In reality, the daily benefit amount will be the determining factor as to the type of coverage and facility or provider they have access to.
With the Partnership, when coverage runs out, the beneficiary can apply to Medicaid to cover additional LTC needs. Someone with longer but skimpy benefits will either spend their assets to provide care or will have to settle for less expensive care options.
Example:
Two 68 year olds purchase long-term care policies with a $100 per day benefit and a 30-day elimination period. They both pay the same premium for their policies.
One purchases a one-year Partnership policy with 5% inflation protection and the other purchases a two-year non-partnership policy without inflation protection.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 232
At age 82, both suffer a stroke requiring one year of care in a nursing home. Which one comes out ahead?
The coverage on the non-Partnership policy remained the same, $100 per day; however, the coverage on the Partnership policy has doubled to $200 per day.
Assuming that nursing home cost has also risen at the rate of 5% compounded, the purchaser with the non-Partnership policyholder would have to make up the difference of $100 per day ($36,500 total for the year) out of pocket while the purchaser of the Partnership policy would have his/her needs covered in full.
But what if they needed to stay longer! Which policy would be better then?
The Partnership policy covers only one year. If the purchasers disabilities required them to stay 4 years instead of only 1, the Partnership policyholder would be eligible for Medicaid after his/her policy benefits ran out and would be able to protect $73,000 worth of non-exempt assets plus $2,000.
The purchaser of the 2 year non-Partnership policy would also be eligible for Medicaid after their policy ran out, but not until they “spent down” all of their assets to the Medicaid level of $2,000. Remember also, that by the end of the two years of coverage, he would have already paid $73,000 or more in co-payments ($36,500 per year). Now both men are on Medicaid but one has only $2,000 and the other one has $73,000 plus $2,000.
1 year Partnership with 5% compound inflation protection
2 year Non-Partnership with no inflation protection
Care Costs: $200/day Benefits: $200 per day Out of Pocket: $0
Care Costs: $200/day Benefits: $100 per day Out of pocket: $100 per day
After one year After two years Transfers to Medicaid Out of Pocket: $0 Retained assets: $73,000
Transfers to Medicaid Out of pocket: $73,000 Retained assets: $2,000
After 4 years After 4 years Receiving care on Medicaid Out of pocket: $0 Retained assets: $73,000
Receiving care on Medicaid Out of pocket: $0 Retained assets: $2,000
As you can see, the Partnership policyholder still comes out far ahead.
This shows that a shorter, more affordable Partnership policy will probably be all the coverage that most people will need. Most people will not exhaust a 2-3 year policy. However, if they do end up needing additional coverage, they can get help paying for it from Medicaid and still retain their protected assets.

© 2008-2015 Sandi Kruise Insurance Training, Sandi Kruise Inc, All rights reserved. 233
SUMMARY
Hopefully you have learned a number of things from this course that will help you with your clients as well as in your life. The population of elders in the United States will continue to swell and to grow older than any previous generation. The government programs are not keeping pace with this surge of seniors now, and it will get worse in the future.
It is important that consumers know the facts about long-term care and what type of programs are available to assist them in receiving adequate care without wiping out a lifetime of savings to do so.
It is important for us as Americans to honor our parents and other older persons who have worked hard and grown old working to make this world a better place for their children. At the same time, children are our future and we can’t shortchange them with substandard education, childcare or medical care in order to cover the massive expenses of the elderly.
The Partnership program is a wonderful example of how the public and private sectors of our nation can come together to help fund expenses that are extremely difficult for either to fund separately. It is up to insurance agents to make this program a success. As you meet with your clients, please take a little extra time to explain how the benefits of the Partnership policies can meet their needs. It may make the difference between being able to plan ahead for many middle income clients across the nation and they, and their children and grandchildren, will thank you for it.


















