7585 081 8
38
Swedish health care from an international perspective INTERNATIONAL COMPARISON 2015 Swedish Association of Local Authorities and Regions Swedish health care from an international perspective 2015 2016
-
Upload
sveriges-kommuner-och-landsting -
Category
Documents
-
view
243 -
download
0
description
http://webbutik.skl.se/bilder/artiklar/pdf/7585-081-8.pdf
Transcript of 7585 081 8

Swedish health care from an international perspectiveINTERNATIONAL COMPARISON 2015
Swedish
Association
ofLocalAuthorities
andRegions
Swedish
healthcarefrom
aninternationalperspective2015
2016


Swedish health care from aninternational perspectiveINTERNATIONAL COMPARISON 2015

Contact
Mattias Lundbäck tfn +46-8-452 76 86Roger Molin tfn +46-8-452 7726
Previous issues
Swedish health care in an international context (2005), isbn 91-7164-049-5
The Swedish Health Care System (2008), isbn 978-91-7164-450-3
Sveriges Kommuner och Countrysting118 82 Stockholm Visitors Hornsgatan 20
Phone +46-8-452 70 00 Fax +46-8-452 70 50
www.skl.se
© Sveriges Kommuner och Landsting1st edition, april 2016
Graphic form and production Elisabet JonssonDiagrammes Elisabet JonssonFonts Chronicle och Whitney.
isbn 978-91-7585-081-8
2 Swedish health care from an international perspective – international comparison 2015

Swedish health care from an international perspective – international comparison 2015 3
Foreword
Health care in Sweden is mainly financed jointly from taxes and is universal.Almost a tenth of society’s total resources go to health care. This is why it iscrucial that health care resources are used well and produce good health out-comes.
To get an idea about the efficiency and quality of health care in Sweden, the-re has to be something to compare it with. This report compares the perfor-mance of health care in Sweden with that of health care in other countries.Sweden is compared with the eu-15 excluding Greece, plus Norway and theus. In everyday terms, the issue is whether health care in Sweden gives valuefor money, when compared with health care in other countries.
The Swedish Association of Local Authorities and Regions (salar) uses anumber of different methods to continually follow the quality and efficiencyof health care in Sweden. International comparisons were published in 2005and 2008 using the same format as this report. An international comparisonof waiting times in more than 20 countries was published in 2011.
Since 2006 salar has been carrying out Open comparisons of the qualityand efficiency of health care along with the National Board of Health and Wel-fare. These studies compare the county councils in Sweden with one another.There are also separate Open comparisons of different parts of health care,such as cancer care and pharmaceuticals.
salar is aiming to make all parts of health care open and transparent.This report has been written by Mattias Lundbäck and Roger Molin at the
Economy and Governance Division of salar.
Stockholm i juni 2015
Håkan SörmanDirector General, Swedish Association of Local Authorities and Regions

Contents
5 1. Swedish health care is strong6 Measuring the quality of health care is a challenge
9 2. A comparison of quality and efficiency in 16 countries9 Summary10 Focus on health care outcomes11 Sweden tops quality index12 Public health factors decisive for some countries13 The USA uses most – Luxembourg least in relation to GDP14 Health care in Sweden is efficient compared with health care in other countries
17 3. International comparisons that include Sweden18 Health Consumer Powerhouse19 The Conference Board of Canada22 The Commonwealth Fund23 Comparisons with a patient perspective give poorer results for Sweden
25 Annex: Indicators in the quality index26 Mortality in acute heart attacks26 Mortality in stroke27 Hip fracture surgery initiated within 2 days27 Breast cancer five-year survival28 Colorectal cancer five-year survival29 Amputations on account of diabetes30 Infant mortality31 Vaccination32 Potential years of life lost (PYLL)33 Blood pressure and blood sugar34 Consumption of antibiotics
4 Swedish health care from an international perspective – international comparison 2015

Swedish health care is strongThis report compares how Swedish health care stands up incomparison with health care in other countries: the EU-15 ex-cluding Greece, plus Norway and the United States. They are allrich countries in a position to provide high class health care. Ouranalysis shows that health care in Sweden does excellently in acomparison with health care in these countries. It tops both theindexes we have used, for quality and for efficiency.
salar’s first international comparison, published in 2005, also concludedthat Swedish health care performed well compared with health care in othercountries. This applied both to access to health care and to quality and results.At the same time, the costs of health care were moderate compared with ot-her countries, and this was expressed by saying that Swedish health care gavegood value for money. This conclusion was based both on an in-house indica-tor-based study and on comparisons made in 2003–2004 by institutions andresearchers in Canada, the Netherlands, the uk and France.
In 2008 salar carried out a new international comparison. That time italso included two summary indexes, of quality and efficiency. The conclusionfrom 2005 still stood in 2008: health care in Sweden performed well in inter-national terms. The index for quality ranked Sweden first of the 17 countriescompared. The index regarding efficiency put Sweden in third place, withFinland coming first and Spain second.
The 2008 study also reported three international comparisons that inclu-ded Sweden. They had been carried out in 2005–2007, one by a Swedish com-pany and two by different Canadian institutions.
They also gave Sweden a high ranking, as second out of 27 countries (be-hind Australia), as third out of 17 countries (behind Switzerland and Japan)and as sixth out of 29 countries (behind Austria, the Netherlands, France,Switzerland and Germany).
The countries selected varied between the different comparisons; in all,more than 30 countries were included. The method for comparisons also va-ried, as did the measures of quality and efficiency used.
The comparison in 2015 again comes the conclusion that Sweden holds astrong position in international comparisons that focus on health care out-
Swedish health care from an international perspective – international comparison 2015 5
CHAPTER1

comes. Sweden takes first place both in the quality index that summarises dif-ferent quality indicators and in the efficiency index that relates quality to re-source use. As in several other comparisons, the Nordic countries also havehigh rankings, with Norway, Finland and Denmark, in that order, taking third,fourth and fifth place. The Netherlands comes second.
The three comparisons carried out by other organisations that are includedin the 2015 report place Sweden as number 3 out of 11 countries (Com-monwealth Fund), 6 out of 17 countries (Conference Board of Canada) and 13out of 30 countries (Health Consumer Powerhouse).
So, in these three comparisons, which also take account of other aspects ofhealth care than health outcomes, the picture is more fragmented. Swedenalso takes a strong position in these studies, as long as the comparisons rela-te to the results of health care. But when the comparisons also cover otheraspects, such as patient involvement, information and waiting times, Swedencomes, as can be seen, lower down in the overall ranking.
Measuring the quality of health care is a challenge
Good health is a high priority for most people. Our health is the result of acomplex interplay between our genes, the environment we live in, the socie-ty we are a part of and our lifestyles. But health care also plays an importantrole for health in various situations. So it is important that health care in Swe-den functions as well as it possibly can.
To assess the performance of health care in Sweden, there has to be so-mething to compare it with. Other countries are asking the same questionabout their own health systems. This shows why international comparisonshave become more and more common and why they are encouraged by, forexample, the World Health Organisation (who), the Organisation for Eco-nomic Cooperation and Development (oecd) and the European Union (eu).Comparisons are a way of getting guidance about the quality and efficiency ofa country’s health system.
A further reason for making comparisons is bound up with the fact that, aspart of a decentralised system of county councils and municipalities, healthcare in Sweden is mainly financed by taxes, and accounts for approaching 10per cent of the total resources of society. Making good use of these resourcesis important for the legitimacy of this way of financing and organising healthcare.
The scale and complexity of health care presents a challenge to measure-ments of the overall quality and efficiency of a whole health system. And weare aware that there are severe limitations on international comparisons ofwhole health systems. At the same time, no other approach is open to anyonewho wants to form a view about the state of health care in Sweden comparedwith health care in other countries. This is also why large numbers of inter-national comparisons are carried out and why organisations like the who,oecd and eu provide statistics as input for audits.
The health systems of different countries have different forms of financing,different allocations of resources between different parts of health care anddifferent forms of employment for health care professionals. But it is difficultto assess different ways of organising and financing health care in analyticalterms and to then go on to establish what is a good health system. This is whythere is a predominance of comparisons that look at different dimensions ofoutcomes. These then deal with different aspects of health in the population,
6 Swedish health care from an international perspective – international comparison 2015
1. Swedish health care is strong

such as life expectancy, remaining life expectancy at various ages, avoidablemortality, infant mortality and mortality in various widespread diseases.
Efficiency is another central theme of international comparisons. It is ge-nerally measured by considering various aspects of outcomes in relation tothe costs of health care. This acts as a rough estimate of what you get for yourmoney in various health systems.
One problem in making comparisons has long been access to data. But formore than a decade the oecd has been providing a set of quality indicatorsthat have become the standard. The purpose is to provide data for internatio-nal comparisons as guidance in various countries’ reforms of their healthsystems.
Our assessment is that the approach that dominates international compa-risons, focusing on the outcomes of health care, is also the most appropriateone. We make the assessment that, for most patients, the ultimate test of thequality of health care is whether health care saves lives and creates the con-ditions for continued independent living.
However, the quality of health care is not solely about whether or not the fi-nal result is good. It is also about the ability of health care to create securityduring the health care process by responding to patient expectations regar-ding service, involvement and treatment. The ability to make matters easierfor patients by not having long waiting times is also significant. But it is dif-ficult to find international comparisons of waiting times. There are no inter-nationally agreed measurement points, and there are great differences betwe-en measurements of waiting times in different countries.
The intention was to include the whole of the eu-15, but we were forced toexclude Greece on account of a lack of data.
Swedish health care from an international perspective – international comparison 2015 7
1. Swedish health care is strong

8 Swedish health care from an international perspective – international comparison 2015
1. Swedish health care is strong

A comparison of quality andefficiency in 16 countriesWe have compared how Swedish healthcare stands up in relationto health care in other countries: the EU-15 excluding Greece,plus Norway and the United States. These countries are all rela-tively rich, and are in a good position to provide high class healthcare. Our analysis shows that health care in Sweden stands upexcellently in a comparison. It tops both the indexes we use, forquality and for efficiency.
Summary
Our assessment is that the approach that dominates international compari-sons, focusing on the outcomes of health care, is also the most appropriateone. We make the assessment that, for most patients, the ultimate test of thequality of health care is whether health care manages to save their lives whenthey are ill or have been injured.
The first piece of good news for patients in Swedish is that health care inSweden is at its best in the areas that are concerned with survival. Swedentops the quality index we use, which includes 13 different quality indicators.The index includes survival after a heart attack, stroke, breast cancer and rec-tal cancer as well as infant mortality. We have aimed to give a broad picture ofresults and to reflect many areas of health care.
The second piece of good news is that health care in Sweden makes gooduse of its resources. Sweden also takes first place in the efficiency index, inwhich overall quality in health care is related to the costs of achieving this qu-ality.
To sum up, health care in Sweden holds a strong position when it is com-pared with health care in other countries.
However, health care is not only about whether or not the final result isgood. It is also about the ability of health care to create security during the he-alth care process by responding to patient expectations regarding service, in-volvement and good treatment. The ability to make matters easier for pati-ents by not having long waiting times is also significant. But it is difficult to
Swedish health care from an international perspective – international comparison 2015 9
CHAPTER2

find international comparisons of waiting times. There are no internationallyagreed measurement points, and there are great differences between measu-rements of waiting times in different countries,
One problem in comparisons has long been access to data. But for morethan a decade the oecd has been providing a set of quality indicators thathave become the standard. The purpose is to provide data for internationalcomparisons as guidance in various countries’ reforms of their healthsystems.
Focus on health care outcomes
What do people mean when they talk in everyday terms about “quality ofcare”. Presumably the term can refer to just curing diseases, for example sur-vival in cancer or the ability to walk after a hip operation. But it can probablyalso cover treatment in health care, how secure you feel during the health careprocess and how long you need to wait.
What we compare in this report is not patients’ experience of health care.This is a tricky area to measure, but, above all, it is difficult to assess what ex-pectations patients have in each country.
Nor do we compare waiting times or the occurrence of queues for healthcare. This is not because the differences are small – there is quite substantialvariation between different countries. But it is difficult to compare waiting ti-mes since there are cross-country differences in ways of measuring and re-porting waiting times. Even though the majority of the countries included inour comparison follow waiting times, there is no uniformity at all in how wai-ting times are measured and reported.
We have selected 13 indicators of health care results from oecd HealthData 2014, the who and the eu. The indicators have been selected so as to re-flect different parts of health care in the broadest possible way. For example,we use thirty-day survival after a stroke to reflect the results of stroke careand thirty-day survival after a heart attack to reflect the results of heart healthcare.
The choice of data depends both on the availability of data and on the pre-valence of the conditions in society. Cancer and cardiovascular diseases eachhave two indicators. Child and maternity care has three indicators. Diabetesand diabetes-related complaints have two indicators. The care of older peo-ple with multiple illnesses has two indicators and preventive care has two in-dicators. We have also chosen to include pyll – potential years of life lostbecause individuals die before the age of 70 years.
Unfortunately, we have not been able to find a good indicator of the quali-ty of mental health care, even though suicide is picked up to some extent bypyll – at any rate to the extent it occurs before the age of 70.
It is important to emphasise that in every comparison there will be factorsthat are not picked up by various key ratios showing what proportion of pati-ents get well again. In our case they can concern quality in palliative care orin care of severely ill older people, where a return to health is not a realistic al-ternative. But such factors can still be of great importance for patients’ qua-lity of life. Similarly, it is important to bear in mind that a country with medi-ocre results on average may very well have diagnoses or geographical areaswhere their results are good. So a low ranking when oecd data are compareddoes not mean that a country does not have any good examples.
Unfortunately we have also been forced to exclude Greece from the com-parison since that country does not have values for several of the indicators
10 Swedish health care from an international perspective – international comparison 2015
2. A comparison of quality and efficiency in 16 countries

included. If the country had been included in the comparison anyway, thiscould have led to incorrect conclusions about the quality and efficiency of thishealth system.
We have chosen the indicators that, in our view, best reflect the results ofhealth care. But we have not made our own assessment of the reliability of theindicators, in the sense of how reliably they have been collected. We have ta-ken the fact that they are indicators in the oecd’s and the who’s library of in-dicators as a sufficient mark of quality.
Sweden tops quality index
All indicators used in the report are rescaled so that the best country scoresone and the worst county scores zero for each index. The other countries arethen given a value between zero and one that is calculated using linear inter-polation. This means, in more everyday terms, that their relative positionbetween zero and one is determined by which limit value (0 or 1) they are clo-sest to.
Then, when we calculate the total index for quality for countries, we justsum each country’s sub-indexes. So the sub-indexes all have the same weightin the total index. We do not weight for resource utilisation in the quality in-dex; instead we construct a separate index of efficiency in which the qualityachieved is related to resource utilisation by countries.
As mentioned above, the quality index has been built up from thirteen dif-ferent quality indicators, most of which have been taken from oecd HealthStatistics 2014. These data are available to the public on the oecd website. Inaddition, we have used two indicators from the who and one indicator of an-tibiotics consumption from the eu.
The indicators are as follows:
By itself, the above table shows that Sweden has very good results. The largestlead seems to be in cardiovascular care and in preventive care, including vac-cinations.
Swedish health care from an international perspective – international comparison 2015 11
2. A comparison of quality and efficiency in 16 countries
Table 1 • IndicatorsPer cent unless otherwise stated
Indicator Average Swedishvalue value
1. Thirty-day mortality for heart attack 6.68 4.52. Thirty-day mortality for ischemic stroke 7.49 6.43. Hip fracture surgery initiated within 2 days (share of patients) 75.1 93.44. Five-year survival rate for breast cancer 84.6 84.75. Five-year survival rate for colorectal cancer 61.4 63.96. Lower extremity amputation on account of complications in
diabetes per 100,000 9.92 3.37. Neonatal mortality, percentage of live births 2.25 1.78. DTP vaccination, percentage of children vaccinated 96.1 989. Measles vaccination, percentage of children vaccinated 93.1 9710. Number of potential years of life lost per 100,000 before the age of 70 3,011 2,42111. Percentage with raised blood sugar 7.55 7.112. Percentage with raised blood pressure (untreated) 24.1 24.513. Consumption of antibiotics (DDD per 100,000, ATC J01) 21.3 14.1
Sources: OECD, WHO and EU.

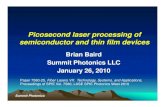
The figure shows that, on average, Sweden achieves better results than any ot-her country in the comparison. We can also note that, in general, the Nordiccountries get good results.
Public health factors decisive for some countries
When comparing the health outcome in different countries it can be difficultto separate public health factors from the contribution made by health care.We have therefore also looked at how three variables that characterise popu-lation lifestyles affect country placings. We have chosen to correct for smo-king rates, obesity rates and high rates of alcohol consumption.
This correction should only be seen as an example of how outcomes can beadjusted for factors wholly or partly outside the control of health care. Someother factors that can be difficult to capture are the large socioeconomic va-riations found in countries like Italy and Spain. An in-depth analysis couldtherefore also weigh in education levels and much else besides. But that iscomplicated and falls outside the framework of this short report.
All these factors have the expected sign in the regression, i.e. a high preva-lence has a negative impact on the outcome. However, overconsumption of al-cohol is not a significant indicator when the two other risk factors are inclu-ded.
If the variation in the quality index that is explained by these three publichealth factors is removed, there is still an unexplained part. The unexplainedpart could be interpreted as the residual effect of the health system.
It turns out that public health affects the placing of some countries, but thatSweden still takes first place in the quality index. See table 2.
The uk and the us climb a few places. This can be interpreted as showingthat these countries achieve better results than should be expected given theunhealthy lifestyle there. In contrast, Norway falls sharply, which can be in-terpreted as showing that Norway ought to be able to achieve better results –given the healthy lifestyle of Norwegians.
12 Swedish health care from an international perspective – international comparison 2015
2. A comparison of quality and efficiency in 16 countries
Figure 1 • Quality indexIndex
Inde
x
Portugal
Spain
Great B
ritain
German
y
Irelan
d
France
Austria
USA
Belgium
Italy
Denmark
Luxe
mbourg
Finlan
d
Norway
Netherl
ands
Sweden
0.0
0.2
0.4
0.6
0.8
1.0
Index based on 13 quality indicators.
Sources: OECD, WHO and EU.

The US uses most – Luxembourg least in relation to GDP
To make an assessment of the efficiency of these countries’ health systems,quality needs to be related to resource utilisation. In this report we have cho-sen the simple measure of health care expenditure per inhabitant as a pro-portion of gdp to measure resource utilisation in each health system. Wehave done so since the major part of health care costs can be attributed to staffcosts. Working with summary indexes that are weighted in various ways doesnot make much of a contribution to the discussion when, as here, compari-sons are being made between countries at about the same level of develop-ment.
However, three countries differ from the others to some extent; they areLuxembourg, Norway and Portugal. Portugal has a relatively low per capitagdp and its resource utilisation may therefore be overestimated slightly. Cor-respondingly, Norway and Luxembourg have a very high per capita gdp andthis means that their resource utilisation may be underestimated. The chiefdifference is that health care in Norway and Luxembourg can buy conside-rably more advanced medical equipment and pharmaceuticals for a givenproportion of gdp. In the case of Luxembourg it is also possible to buy healthcare from countries were production is much cheaper.
This can be worth bearing in mind when we compare the efficiency of he-alth systems. One general reservation is that it is, in any case, possible to esti-mate resource utilisation in many different ways since health systems are or-ganised in different ways and responsibility for services like health and el-derly care can be defined in varying ways in different countries.
The expenditure share of health care in the different countries is set out intable 3 on page 14.
It is the us, in particular, that deviates upwards regarding resource utilisa-tion. One important reason can be that the pay levels of some groups in healthcare are higher there than in the other countries. Another reason may be thatthe insurance system and an insufficient ability to set priorities are driving upcosts.
Swedish health care from an international perspective – international comparison 2015 13
2. A comparison of quality and efficiency in 16 countries
Table 2 • Country placings in the quality indexIndex
Sweden 0.14Netherlands 0.08Finland 0.07UK 0.03Austria 0.03France 0.02Luxembourg 0.01Ireland 0.01USA –0.02Germany –0.03Belgium –0.03Norway –0.05Denmark –0.05Spain –0.05Italy –0.05Portugal –0.12
Sources: OECD, WHO and EU.
The quality index after the effect of threepublic health indicators has been remo-ved. The indicator is the residual in a mul-tiple regression in which the quality indexis the dependent variable and the obesityrate, alcohol consumption and smokingare independent variables.

Health care in Sweden is efficient compared with healthcare in other countriesOne common way of comparing efficiency is to use non-parametric methods.The technique is based on identifying which units – in this case countries –strictly dominate others. In doing so, either a constant return to scale or a vari-able return to scale can be assumed.
In both cases the result – the quality index – is set against resource utilisa-tion. The countries that manage to achieve most for a given utilisation of re-sources are assessed as having maximum efficiency.
The reason why you may wish to use one or other of these methods is thatwe cannot be sure that spending on health care gives as good a return irre-spective of how much resources are already used for health care. In a countrythat spends two per cent of gdp on health care, an additional one percentagepoint will be of much greater importance than in a country that already usesten per cent. When the differences between countries are large, it can be ap-propriate to open up the possibility that the return is diminishing. A variablereturn to scale can therefore be assumed.
If we impose the restriction that the return to scale has to be constant, Swe-den comes first since Sweden has the highest ratio between the quality indexand health care expenditure/gdp. This does not change substantially if wethen permit variable return to scale.
14 Swedish health care from an international perspective – international comparison 2015
2. A comparison of quality and efficiency in 16 countries
Table 3 • Countries’ health care expenditure as a proportion of GDPPer cent
Country Expenditure/GDP
Belgium 10.61Denmark 10.87Finland 8.95France 11.52Ireland 8.71Italy 9.25Luxembourg 7.29Netherlands 12.10Norway 9.28Portugal 10.23Spain 9.44UK 9.23Sweden 9.49Germany 11.25US 17.02Austria 10.87
Source: OECD Health Statistics 2014.
Total health care expenditure as a propor-tion of countries’ GDP. Most recent figu-res available.

Swedish health care from an international perspective – international comparison 2015 15
2. A comparison of quality and efficiency in 16 countries
Diagram 2 • Efficiency indexIndex
0.0
0.2
0.4
0.6
0.8
1.0
Inde
x
USA
Portugal
Austria
France
Spain
German
y
Belgium
Denmark
Great B
ritain
Irelan
d
Netherl
ands
Italy
Norway
Finlan
d
Luxe
mbourg
Sweden This index is based on quality in relation
to expenditure (ratio) assuming a con-stant return to scale.
Sources: OECD, WHO and EU.

16 Swedish health care from an international perspective – international comparison 2015
2. A comparison of quality and efficiency in 16 countries

International comparisonsthat include SwedenThis section describes the results of three international compa-risons carried out by other organisations that include Sweden.The countries selected vary between these studies, as do thefocus areas and methods. But they are three broad comparisonsthat assess different aspects of quality in the health systems ofthe countries covered. In all these cases Sweden gets a high ran-king, but its placing depends on what quality aspects are inclu-ded and what aspects are given most weight.
Two of these three studies were also included in the salar report from 2008:the Health Consumer Powerhouse and the Conference Board of Canada. The2008 report also contained a comparison from the Fraser Institute, but thatstudy has not been updated and therefore it is not included here. However,Sweden has been included in an international comparison conducted by theCommonwealth Fund and it is therefore reported here.
We assess these three studies as being among the most tone-setting and asrepresenting attempts to rank quality in different health systems. The dataused and the indicators selected differ between these studies and this can giveus a picture of how the choice of indicators affects Sweden’s placing.
It is necessary to be clear, from the outset, that different things can bemeant by quality of care. Patients who get healthy as a result of health care canstill be dissatisfied with the health care process. And patients that health caredoes not manage to cure may very well be satisfied with how they have beentreated and other aspects.
It is important to absorb the insight that patient satisfaction is somethingcompletely different from treatment outcomes. Many aspects of health careare best measured by questionnaires or other subjective metrics. But there isno guarantee that a country that has a large proportion of satisfied patientsalso has good treatment outcomes.
Swedish health care from an international perspective – international comparison 2015 17
CHAPTER3

Health Consumer Powerhouse
The Health Consumer Powerhouse (hcp), which was originally a Swedishcompany, started its activities by comparing Swedish county councils interms of a number of quality indicators in 2004.
In 2005 hcp published its first international comparison covering a dozencountries and 2o indicators. Since then its comparisons have been expandedgradually and the 2014 index covers 30 countries: the 28 eu member countri-es, and Norway and Switzerland. The number of variables is now 48 spreadover six sub-disciplines:1. Patient rights and information2. Accessibility3. Outcomes4. Range and reach of services provided5. Prevention6. Pharmaceuticals
hcp emphasises that its ranking is carried out from a health consumer per-spective. So it is not a pure assessment of quality of care, for example heart at-tack survival rates, even though outcome indicators also form part of the in-dex.
The total index composed from the various sub-disciplines gives them theweights shown in table 4.
18 Swedish health care from an international perspective – international comparison 2015
3. International comparisons that include Sweden
The indicators included in each sub-discipline are listed below.• Patient rights and information: 12 indicators. Healthcare law based on patients’ rights:
patient organisation involvement; no-fault malpractice insurance; right to second opini-on; access to own medical record; registry of bona fide doctors; web or 24/7 telephoneHC info; cross-border care seeking freely allowed; provider catalogue with quality ran-king; EPR [electronic patient record] penetration; on-line booking of appointments; e-prescriptions.
• Accessibility: 5 indicators. Family doctor same day access; direct access to specialist; ma-jor elective surgery <90 days; cancer therapy < 21 days; CT scan < 7 days; A&E waiting ti-mes.
• Outcomes: 8 indicators. Decrease of CVD deaths; decrease of stroke deaths; infant deat-hs; cancer survival; preventable years of life lost; MRSA infections; abortion rates; de-pression.
• Range and reach of services provided: 8 indicators. Equity of healthcare systems; cata-ract operations per 100,000 age 65+; kidney transplants per million pop.; dental care in-cluded in public healthcare; informal payments to doctors; long term care for the elder-ly; % of dialysis done outside of clinic; caesarean sections.
• Prevention: 7 indicators. Infant 8-disease vaccination; blood pressure; smoking preven-tion; alcohol; physical activity; HPV vaccination; traffic deaths.
• Pharmaceuticals: 7 indicators. Rx (i.e. prescription drugs) subsidy; layman-adaptedpharmacopoeia; novel cancer drugs deployment rate; access to new drugs (time to subsi-dy); arthritis drugs; metformin use; Antibiotics/capita (less is better).
For each of the 48 indicators points are given on a three-point scale: Three points: Goodoutcome. Two points: Intermediary outcome. One point: Not-so-good outcome.
HCP’s Indicators

Sweden gets the highest score in two categories: range and reach of services pro-vided and prevention. Sweden is also among the best regarding outcomes, aswell as with respect to the use of pharmaceuticals. As regards patient rights andinformation Sweden scores just above the average. In contrast Sweden gets avery low score in the category of accessibility.
In the overall index Sweden come in thirteenth place out of the thirtycountries. This is slightly worse than in last year’s report where Sweden tooktwelfth place and in the 2012 report where Sweden came in sixth.
The outcomes category, where Sweden has previously obtained the highestscore, has been changed in the past two years. For the two largest groups of di-seases hcp has chosen the rate of decrease for deaths on account of strokeand cardiovascular diseases. This is a relative measure that does not take ac-count of results already achieved. Previously indicators that reflected the ab-solute level were used.
But the fact that Sweden does not get the highest possible score for outco-mes is mainly due to Sweden’s high abortion rate. Without this indicator, whi-ch can be discussed, Sweden would take the top position. It is undoubtedlypossible to influence the abortion rate through better sex education inschools and contraceptive advice. But it does not seem likely that these ac-tions are working badly in Sweden in comparison with countries like Sloveniaand Montenegro that get top results thanks to a low abortion rate. The statis-tics are probably steered by completely different factors – outside the controlof the health system.
The hcp produces an extensive index with many different dimensions. Butit is not solely an index of the quality of health care. The hcp points out thatthe index measures how good health care is from the perspective of healthconsumers. And then the actual results of health care, for instance in terms ofsurvival, are not the only or even the most important factor.
The Conference Board of Canada
The Conference Board of Canada (cbc) is an independent non-profit-orga-nisation, which performs work for both the public and the private sector. Thecbc wants to produce more knowledge about economic trends, policy deve-lopment in various areas and organisational development.
In 2004 the cbc published a comparison ranking health care in 24 countri-es on the basis of 24 indicators. It ranked Switzerland first and Sweden se-cond. Three years later Sweden had fallen to third place while the number ofcountries had decreased to 17.
In the comparisons made for last year (2014) Sweden coms sixth overall,with a “B” grade. In the first two reports Sweden had an “A” grade. The lowestgrade is ”D”. The report again covers 17 countries this time. The indicators
Swedish health care from an international perspective – international comparison 2015 19
3. International comparisons that include Sweden
Table 4 • Sub-disciplines and relative weightsPer cent
Discipline Relative weight
Patient rights and information 15Accessibility 22.5Outcomes 25Range and reach of services provided 15Prevention 12.5Pharmaceuticals 10
Source: Health Consumer Powerhouse.

have been changed by no longer dividing up life expectancy into men’s andwomen’s life expectancy. Instead the indicator “Self-reported health status”has been added.
Sweden’s results on the various sub-indicators are shown below. “A” is bestand “D” is worst.
20 Swedish health care from an international perspective – international comparison 2015
3. International comparisons that include Sweden
Table 5 • Report card of health indicatorsGrades A–D
Life Self- Pre- Mor- Mor- Mor- Mor- Mor-expect- reported mature tality tality tality tality tality
ancy health mor- due to due to due to due to due tostatus tality cancer circulatory respiratory dia- musculo-
diseases diseases betes skeletalsystem
diseases
Australia B A A A A A B CBelgium C A B B C D A BCanada B A A C A B C CDenmark D A B D C C B DFinland C B B A D A A BFrance B B B B A A A CGermany C B A B D A B AIreland C A B C D D B DItaly A B A B B A C BJapan A D A A A C A ANetherlands B A A D B C B CNorwat B A A B B C A BSwitzerland A A A A B A A CUK C A B C C D A DSweden B A A A C A B BUSA D A D B C C C CAustria C A B B D A D A
Table 6 • Sweden’s grades for health indicatorsGrades A–D
Indicator Sweden’s grade (A–D)
Life expectancy BSelf-reported health status APremature mortality AMortality due to cancer AMortality due to circulatory diseases CMortality due to diabetes BMortality due to respiratory diseases AMortality due to musculo-skeletal system diseases BMortality due to mental disorders CInfant mortality AMortality due to medical misadventures C
Source: Conference Board of Canada, 2014.
The Conference Board grades the countri-es.

Swedish health care from an international perspective – international comparison 2015 21
3. International comparisons that include Sweden
The Conference Board of Canada has followed the various countries compa-red over time and in its most recent report it publishes a graph showing de-velopments from the 1960s to the present. Finland, Norway and Sweden areall in category B. Both Norway and Sweden have been in category A previous-ly, but are now in category B. Finland has gone in the opposite direction, fromD to C and then to B. Denmark has fallen from B to C and now, in the latestranking, to D.
Table 7 • Different countries’ placings from the 1960sGrades A–D
1960s 1970s 1980s 1990s 2000s
Australia C C C B BBelgium D D D D CCanada B B B B BDenmark B B C D DFinland D D C C BFrance D C C C BGermany D D C C BIreland C D D D CItaly C B C C BJapan C B A A ANetherlands B A B C CNorway A A B B BSwitzerland C B B B AUK C C D D DSweden A A A A BUS C C C D DAustria D D C C C
Source: Conference Board of Canada, 2014.

The Commonwealth Fund
The Commonwealth Fund is a private foundation in the us whose purpose isto improve health care. It makes running comparisons of different us states,but also presents international perspectives. Sweden was not one of thecountries covered originally, but has been included in the 2014 comparison.
Overall, Sweden was ranked third of the 11 countries covered. As regardsquality of care, Sweden got the second lowest score of all the countries. In con-trast, as regards access Sweden comes in fourth place.
Table 8 • Different countries’ placings in five different dimensionsRanking
Cana- Fran- Ger- Nether- New Nor- Swe- Switz- UK USA Aus-da ce many lands Zealand way den erland tria
Overall ranking 10 9 5 5 7 7 3 2 1 11 4Quality care 9 8 7 5 4 11 10 3 1 5 2Effective care 7 9 6 5 2 11 10 8 1 3 4Safe care 10 2 6 7 9 11 5 4 1 7 3Coordinatedcare 8 9 10 5 2 7 11 3 1 6 4Patient-centredcare 8 10 7 3 6 11 9 2 1 4 5
Access 9 11 2 4 7 6 4 2 1 9 8Cost-relatedproblem 5 10 4 8 6 3 1 7 1 11 9Timeliness 11 10 4 2 7 8 9 1 3 5 6
Efficiency 10 8 9 7 3 4 2 6 1 11 4Equity 9 7 4 8 10 6 1 2 2 11 5Healthy lives 8 1 7 5 9 6 2 3 10 11 4
Source: The Commonwealth Fund, 2014.
The report covers 80 indicators grouped in five different dimensions: quality,access, efficiency, equity and healthy lives (public health). The indicators havemostly been taken from the Commonwealth Fund’s questionnaires aimed atpatients with multiple illnesses, doctors in primary care and the populationin general. In addition, indicators from the who and oecd are used regar-ding outcomes and costs.
The Commonwealth Fund uses country rankings to combine the indica-tors. This is similar to the methodology we use in this report, with the diffe-rence that we also take account of the differences in the values of the indica-tors. If country A has a heart attack mortality of 5 per cent, country B 4.5 percent and country C 3.5 per cent, the countries will get the following scores inthe Commonwealth Fund’s report: A=3, B=2 and C=1. In this report the cor-responding figures would instead be A=0, B=0.33, C=1, as we also give weightto how much the countries differ from one another in absolute numbers. Onaverage both methods ought to give roughly the same results, but in the op-posite order.
All the indicators apart from healthy lives are based on questionnaires andtherefore on the subjective experiences of patients, health care professionalsor the population. On this point the Commonwealth Fund’s study differs fromthe others. Using subjective views as the basis for estimating objective facts istricky. It is difficult to capture patients’ expectations and the replies givenalso depend, of course, on what people in the country expect.
22 Swedish health care from an international perspective – international comparison 2015
3. International comparisons that include Sweden

Comparisons with a patient perspective give poorer resultsfor Sweden
The Conference Board’s measurement is the narrowest one in the sense thatit only looks at outcomes – not at factors such as waiting times and equity. Butthere is also a subjective factor in this measurement: “self-reported healthstatus”. The Health Consumer Powerhouse applies an explicit health consu-mer perspective. This means that it takes account not only of how well healthcare manages to cure diseases but also of what rights patients have and howthey are treated as “customers” in the system. The Commonwealth Fund hasa purely subjective perspective.
The different studies measure different quality aspects and this affects theresults of the different comparisons. In the Health Consumer Powerhouse’smeasurement Sweden comes in thirteenth place out of 30 countries. In theConference Board’s measurement Sweden comes in sixth place out of 17countries. In the Commonwealth Fund’s study Sweden comes in third placeout of 11 countries included.
Swedish health care from an international perspective – international comparison 2015 23
3. International comparisons that include Sweden

24 Swedish health care from an international perspective – international comparison 2015
3. International comparisons that include Sweden

Annex: Indicators in the quality index
In every case the most recent year available is used. This can mean that thereis a difference of one, or at most, two years between the measurement points.Normally these differences ought not to be of any great importance for theranking.
The scores of the different countries within each indicator are shown in ta-ble 9. The figures are rounded.
Swedish health care from an international perspective – international comparison 2015 25
Table 9 • Different countries’ scores within each indicator*Index
Country 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13.Heart Stroke Hip Breast Colorectal Dia- Neonatal DTP Measles Years of Blood Blood Anti-attack fracture cancer cancer betes mortality vaccin. vaccin. life lost sugar pressure bio.
Belgium 0.38 0.49 0.66 0.55 0.98 0.20 0.67 0.73 1.00 0.51 0.52 0.63 0.00Denmark 1.00 1.00 0.98 0.18 0.10 0.00 0.41 0.59 0.69 0.75 0.61 0.61 0.72Finland 0.32 0.80 0.81 0.66 0.91 0.82 0.96 0.95 0.94 0.57 0.44 0.04 0.56France 0.46 0.33 0.66 0.50 0.68 0.74 0.59 0.59 1.00 0.56 0.89 0.49 0.00Ireland 0.36 0.12 0.80 0.00 0.40 0.94 0.56 0.77 0.81 0.72 0.67 0.12 0.37Italy 0.53 0.64 0.00 0.50 0.68 0.82 0.74 0.64 0.88 0.91 0.65 0.35 0.12Luxembourg 0.02 0.00 0.66 0.50 0.68 1.00 0.85 0.86 1.00 1.00 0.44 0.45 0.10Netherlands 0.36 0.48 1.00 0.66 0.82 0.35 0.52 0.91 0.88 0.85 1.00 0.45 1.00Norwat 0.75 0.82 0.66 0.68 0.82 0.64 1.00 0.77 0.69 0.91 0.30 0.11 0.70Portugal 0.08 0.03 0.17 0.26 0.37 0.39 0.67 1.00 0.94 0.58 0.74 0.00 0.39Spain 0.07 0.08 0.11 0.50 0.68 0.59 0.70 0.86 0.81 0.90 0.17 0.47 0.48UK 0.19 0.05 0.89 0.18 0.00 0.86 0.41 0.86 0.81 0.59 0.71 0.43 0.53Swedeb 0.75 0.65 0.97 0.84 0.92 0.97 0.85 0.95 0.94 0.96 0.66 0.36 0.85Germany 0.00 0.61 0.85 0.55 0.96 0.05 0.67 0.95 0.81 0.73 0.50 0.25 0.81USA 0.58 0.97 0.66 1.00 1.00 0.13 0.00 0.68 0.69 0.00 0.00 1.00 0.46Austria 0.20 0.71 0.66 0.44 0.86 0.57 0.63 0.00 0.00 0.74 0.87 0.37 0.86
*The indicators are presented in greater detail in table 1 on page 11.
Source: OECD, WHO and EU.

Mortality in acute heart attacks
This indicator represents a common disease and therefore a large number ofpatients. The indicator comes from oecd Health Statistics and refers to pa-tients aged 45 and older admitted to hospital. Denmark is the country that hasthe lowest mortality. Then come Norway and Sweden, which share secondplace.
Mortality in stroke
The indicator represents a common and serious illness that is a common cau-se of admission to hospital. The indicator comes from oecd Health Statisticsand refers to patients aged 45 and older admitted to hospital.
Sweden comes fifth after Denmark, Norway, Finland and Austria.
26 Swedish health care from an international perspective – international comparison 2015
Annex: Indicators in the quality index
Table 10 • Different countries’ indicator for mortality in acute heart attacksPer cent
Country 2010 2011
Denmark 3.3 3Finland 7.6 7France 6.2 ..Ireland 7.5 6.8Italy 5.8 5.8Luxembourg 6.9 8.8Netherlands 6.8 ..Norway 4.1 4.5Portugal .. 8.4Spain 8.8 8.5UK 8.4 7.8Sweden 4.8 4.5Germany 9.6 8.9USA 5.5 ..Austria 8.5 7.7
Source: OECD Health Statistics 2014.
The proportion of deaths in heart attacks(AMI, acute myocardial infarction) within30 days. Refers to patients admitted tohospital. The figures are age-standar -dised.
Table 11 • Different countries’ indicator for mortality in strokePer cent
Country 2010 2011
Denmark 3,9 4,1Finland 5,5 5,4France 8,5 ..Ireland 11,1 9,9Italy 6,5 6,5Luxembourg 10,1 10,7Netherlands 7,5 ..Norway 5,5 5,3Portugal .. 10,5Spain 10,5 10,2UK 11,7 10,4Sweden 6,6 6,4Germany 6,9 6,7USA 4,3 ..Austria 6,1 6
Source: OECD Health Statistics 2014.
Proportion of deaths within 30 days inischemic stroke. Refers to patients admit-ted to hospital. The figures are age-stan-dardised.

Hip fracture surgery initiated within 2 days
The indicator is intended to give a picture of how well collaboration betweenelderly care and health care functions, as well as how well health care is ableto coordinate interventions involving several actors.
It is desirable to keep the waiting time to surgery as short as possible in or-der to be able to achieve good results. Sweden has the third best result, afterthe Netherlands and Denmark.
As can be seen there is very great cross-country variation.
Breast cancer five-year survival
The indicator is intended to give a picture of how well health care of one of themost common forms of cancer functions. Early discovery gives better resultsand the choice of five-year survival therefore reflects both the quality of pre-ventive work and the efficiency of health care as such.
The measure is age-standardised and refers to the 15–99 age group. The us
has the best result, followed by Sweden and Finland.
Swedish health care from an international perspective – international comparison 2015 27
Annex: Indicators in the quality index
Table 12 • Different countries’ indicator for hip fracture surgery initiated within 2 daysPer cent
Country 2010 2011
Denmark 93,3 94Finland 82,7 84,2Germany 85,6 86,2Ireland 81,6 83,2Italy 34,2 36,8Netherlands 95,1 ..Portugal .. 46,6Spain 41,8 43,2Sweden 91,2 93,4UK 86,4 88,4
Source: OECD Health Statistics 2014.
Proportion of patients with a hip fracturetreated surgically within 2 days after ad-mission to hospital. Patients aged 65 andolder. The figures are not age-standardi-sed.
Table 13 • Different countries’ indicator for breast cancer five-year survivalPer cent
Country 2004–2009 2005–2010 2006–2011 2007–2012
Belgium 84,8 85 .. ..Denmark 82 81,2 82 ..Finland 87,4 85,9 .. ..Ireland 80 80,5 .. ..Netherlands 84,4 85,8 85,9 ..Norway 86,5 86 86,1 ..Portugal 82,5 82,6 .. ..UK 80,8 81,9 80,7 82Sweden 86 85,9 86,3 87,4Germany 85 .. .. ..USA 88,7 .. .. ..Austria 80,9 82,7 84,5 84,1
Source: OECD Health Statistics 2014.
Breast cancer five-year survival rate. Re-fers to the 15–99 age group and only towomen. The figures are age-standardised.

Colorectal cancer five-year survival
The indicator is intended to give a picture of how well health care of one of themost common forms of cancer functions. Early discovery gives better resultsand the choice of five-year survival therefore reflects both the quality of pre-ventive work and the efficiency of health care as such.
The measure is age-standardised and refers to the 15–99 age group. Swedenis among the best countries – it is chiefly the uk, Denmark, Portugal and Ire-land that have poor results among countries reporting this indicator.
28 Swedish health care from an international perspective – international comparison 2015
Annex: Indicators in the quality index
Table 14 • Different countries’ indicator for colorectal cancer five-year survivalPer cent
Country 2004–2009 2005–2010 2006–2011 2007–2012
Belgium 63.5 64.5 .. ..Denmark 55.5 .. .. ..Finland 63.2 63.8 .. ..Ireland 57.1 58.6 .. ..Netherlands 60.9 62 62.9 ..Norway 63.1 62.3 62.9 ..Portugal 57.2 58.3 .. ..UK 53 53.2 54 54.5Sweden 60.7 61.7 63.1 63.9Germany 64.3 .. .. ..USA 64.7 .. .. ..Austria 62.8 62.1 62.6 63.3
Source: OECD Health Statistics 2014.
Colorectal cancer five-year survival Refersto the 15–99 age group. The figures areage-standardised.

Amputations on account of diabetes
With good out-patient care and continuous monitoring it should be possibleto keep a patient’s blood sugar level within acceptable limits. If leg ulcers stilldevelop on account of diabetes, there are now methods of avoiding gangrene.Needing to resort to amputation is therefore a failure for the preventive careof diabetes patients.
The measure applies to patients per 100,000 inhabitants aged 15 or over andis age-standardised. Here Sweden is in second place, just behind Luxem-bourg.
Swedish health care from an international perspective – international comparison 2015 29
Annex: Indicators in the quality index
Table 15 • Different countries’ indicator for amputations on account of diabetesPer cent
Country 2009 2010 2011
Belgium 15.9 .. ..Denmark 19.2 .. ..Finland 6.5 6.5 5.8France .. 7.4 7.1Ireland 4.9 5.2 3.8Italy 5.7 5.9 5.7Luxembourg 4.6 7.0 2.8Netherlands 11.6 13.5 ..Norway 9.3 7.8 8.7Portugal .. .. 12.8Spain 10.6 9.7 9.6UK 5.3 5.3 5.1Sweden 3.6 3.2 3.3Germany 20.6 .. 18.4USA .. 17.1 ..Austria 3.6 3.2 3.3
Source: OECD Health Statistics 2014.
Lower extremity amputations on accountof diabetes per 100,000 inhabitants Refersto the 15–99 age group. The figures areage-standardised.

30 Swedish health care from an international perspective – international comparison 2015
Annex: Indicators in the quality index
Infant mortality
This is a commonly used indicator. We have chosen the proportion of infantswho die within 28 days from birth. The indicator reflects the quality of ma-ternity care and of delivery.
Here Sweden takes a share of third place, behind Norway and Finland.
Table 16 • Different countries’ indicator for infant mortalityPer cent
Country 2010 2011 2012
Belgium 2.2 .. ..Denmark 2.6 2.8 2.9Finland 1.5 1.6 1.4France 2.5 2.3 2.4Greece 2.5 2.2 1.9Ireland 2.6 2.5 ..Italy 2.2 2 2Luxembourg 2.2 2.8 1.7Netherlands 2.8 2.7 2.6Norway 1.6 1.4 1.3Portugal 1.7 2.4 2.2Spain 2.1 2.1 2.1UK 2.9 3 2.9Sweden 1.6 1.4 1.7Germany 2.3 2.4 2.2USA 4.1 4 ..Austria 2.7 2.4 2.3
Source: OECD Health Statistics 2014.
Neonatal mortality. Deaths before the ageof 28 days per 1,000 live births.

Vaccination
We have chosen to include two measures of preventive health care via vacci-nation for serious diseases. These indicators are the vaccination rate for dip-htheria, tetanus, pertussis (dtp) and for measles.
These indicators reflect both information work and how well preventivehealth care reaches out to all parts of the population.
In both cases Sweden is among the countries with the highest vaccinationcoverage.
Swedish health care from an international perspective – international comparison 2015 31
Annex: Indicators in the quality index
Table 17 • Different countries’ indicator for vaccinationPer cent
Country DTP (2013) Measles (2013)
Belgium 99 92Denmark 94 89Finland 98 97France 99 89Greece 99 99Ireland 96 93Italy 97 90Luxembourg 99 95Netherlands 97 96Norway 94 93Portugal 98 98Spain 96 95UK 96 95Sweden 98 97Germany 96 97USA 94 91Austria 83 76
Source: OECD Health Statistics 2014.
Vaccination coverage. Percentage of child-ren immunised against measles andagainst diphtheria, tetanus and pertussis.

Potential years of life lost (PYLL)
pyll, Potential Years of Life Lost, is a general measure of how many years oflife are lost because of people dying prematurely (before the age of 70). It canbe difficult to distinguish between what is an effect of good health care andwhat is an effect of a healthy lifestyle.
We have nevertheless chosen to include this indicator that has been crea-ted to capture factors not covered by the other indicators. Sweden has the bestscore after Luxembourg (smallest number of years of life lost per 100,000).
32 Swedish health care from an international perspective – international comparison 2015
Annex: Indicators in the quality index
Table 18 • Different countries’ indicator for PYLLYears per 100,000 inhabitants
Country 2010 2011 2012
Belgium 3,445.9 .. ..Denmark 3,253.3 3,101.7 2,913.5Finland 3,556.6 3,394.8 3,307.2France 3,440.6 3,338.1 ..Greece 3,193.0 3,105.4 ..Ireland 2,977.7 .. ..Italy 2,526.5 .. ..Luxembourg 2,738.1 2,639.2 2,327.4Netherlands 2,737.6 2,687.0 2,676.1Norway 2,775.4 2,760.2 2,541.2Portugal 3,492.1 3,398.4 3,286.5Spain 2,716.4 2,668.2 2,556.5UK 3,261.8 .. ..Sweden 2,486.9 2,419.7 2,421.1Germany 3,128.8 3,069.8 2,941.8USA 4,628.9 .. ..Austria 3,219.7 3,068.2 2,935.2
Source: OECD Health Statistics 2014.
PYLL is calculated by summing, for alldeaths before 70 years, the years of lifelost until the deceased would have re-ached 70. The sum of years of life lost isthen divided by the population and is cal-culated per 100,000 inhabitants agedbetween 0 and 69.

Blood pressure and blood sugar
We include two indicators from the World Health Organisation that reflecthow well work to control blood pressure and blood sugar levels functions inthe different countries.
Sweden has average values for both these indicators.
Swedish health care from an international perspective – international comparison 2015 33
Annex: Indicators in the quality index
Table 19 • Different countries’ indicator for blood pressure and blood sugar, 2008
Per cent
Country Raised HBA1 Raised blood pressure
Belgium 7.85 20.7Denmark 7.35 21.05Finland 8.3 28.8France 5.75 22.65Greece 8.7 22.45Ireland 7.0 27.8Italy 7.1 24.6Luxembourg 8.3 23.2Netherlands 5.1 23.25Norway 9.15 27.95Portugal 6.6 29.4Spain 9.9 22.9UK 6.75 23.4Sweden 7.05 24.5Germany 7.95 25.9USA 10.85 15.6Austria 5.85 24.25
Source: World Health Statistics, 2014.
The figures refer to the estimate by theWorld Health Organisation (WHO) of theproportion of the population that has raised blood sugar (25 years and above)and raised blood pressure (25 years and above). The figures are age-standardised.The limit for high blood pressure is>140/>90 and that for blood sugar is>7.0
mmol/l.

Consumption of antibiotics
Antibiotics should only be prescribed when a bacterial infection has beenestablished. But since many antibiotics are cheap, doctors often tend to meetpatients’ wishes – even though this risks increasing antibiotic resistance. Norcan problems caused by viruses be attacked using antibiotics, which meansthat antibiotics are then consumed unnecessarily.
Sweden has the third lowest consumption, after the Netherlands and Au-stria.
34 Swedish health care from an international perspective – international comparison 2015
Annex: Indicators in the quality index
Table 20 • Different countries’ indicator for consumption of antibioticsDDD per 100,000 inhabitants and days
Country 2008 2009 2010 2011 2012 Average annual Statistiscalchange significance
2008–2012
Belgium 27.7 27.5 28.4 29.0 29.8 0.55 significantDenmark 16.0 16.0 16.5 17.4 16.4 0.35 n.s.Finland 18.3 18.0 18.5 20.1 19.5 0.55 n.s.France 28.0 29.6 28.2 28.7 29.7 0.24 n.s.Greece 45.2 38.6 39.4 35.1 31.9 n.a.Ireland 22.4 20.8 20.3 22.6 23.0 0.30 n.s.Italy 28.5 28.7 27.3 28.2 27.6 –0.22 n.s.Luxembourg 27.1 28.2 28.6 27.6 27.9 0.09 n.s.Netherlands 11.2 11.4 11.2 11.4 11.3 0.02 n.s.Norway 15.5 15.2 15.8 16.5 16.9 0.40 significantPortugal 22.6 22.9 22.4 23.2 22.7 0.02 n.s.Spain 19.7 19.7 20.3 20.9 20.9 0.34 significantUK 16.9 17.3 18.7 18.8 20.1 0.76 significantSweden 14.6 13.9 14.2 14.3 14.1 –0.09 n.s.Germany 14.5 14.9 14.5 14.1 14.9 –0.02 n.s.Austria 15.1 15.9 15.0 14.5 13.9 –0.34 significant
Source: EU.
Consumption of antibiotics group J01 forsystemic use. DDD per 100,000 inhabi-tants and day.


Swedish health care from an international perspective
International comparison 2015
The Swedish Association of Local Authorities and Regions (salar)regularly publishes data for assessing quality and efficiency insectors for which municipalities and county councils are respon-sible. This report compares health care in various countries. He-alth care in Sweden is compared with health care in Belgium,Denmark, Finland, France, Italy, Ireland, Luxembourg, the Neth -erlands, Norway, Portugal, Spain, the UK, Germany, the US andAustria.
The purpose is to see how health care in Sweden stands up incomparison with health care in these countries. This can serve asa basis for discussions about the strengths and weaknesses of healthcare in Sweden.
salar has published reports on health care in Sweden with in-ternational comparisons on two previous occasions: in 2005 and2008.
This report has been written by Mattias Lundbäck och RogerMolin, both at at the Economy and Governance Division of sa-
lar.
Health care in Sweden from an international perspective – inter-national comparison 2015 can be downloaded from our websitewww.skl.se.
Download at www.skl.se/English pages, Publications and reports.
Price Free.ISBN 978-91-7585-081-8
Post 118 82 Stockholm Besök Hornsgatan 20
Telefon 08-452 70 00
www.skl.se