7 - Respiratory Emergencies and Thoracic Trauma.pdf

of 112
-
Upload
rere-angelica -
Category
Documents
-
view
75 -
download
1
Transcript of 7 - Respiratory Emergencies and Thoracic Trauma.pdf
-
Respiratory
Emergencies
and Thoracic
Trauma
Michael D. Gooch
RN, MSN, ACNP, FNP, CFRN, CEN, EMT-P
1
-
Objectives
Discuss priorities of the primary and
secondary assessment of patients
presenting to the emergency
department.
Describe basic principles of disaster
management.
Analyze the effectiveness of patient or
family education in a clinical scenario.
Discuss the basic principles of safe
interfacility transfer.
2
-
Objectives
Describe anticipated assessment findings of patients with selected respiratory, medical, cardiovascular, neurologic, toxicological, gastrointestinal, and genitourinary emergencies,
Plan and prioritize interventions of patients with selected respiratory, medical, cardiovascular, neurologic, toxicological, orthopedic, psychiatric or gastrointestinal emergencies.
3
-
Objectives
Select appropriate triage
categories for patients in clinical
scenarios.
Differentiate cardiogenic,
hypovolemic, and distributive
shock with regards to
assessment and management.
4
-
Things to Review
ABG interpretation
Basic life support
COPD/Emphysema
ARDS
Childhood respiratory emergencies
Chest trauma
Indications/contraindications of
common drugs used in respiratory
conditions
5
-
Basic Respiratory/Airway
Concepts
Assessment of work of
breathing & adventitious breath
sounds
Laryngeal Mask Airway (LMA)
Used for blind intubation
Confirmation of ETT placement
Measurement for pediatric ETT
placement
6
-
Basic Respiratory/Airway
Concepts
Rapid Sequence Intubation (RSI)
Pre-med (to prevent bradycardia, dry secretions, suppress cough reflex, decrease ICP & muscle fasciculations)
Anesthetize / Sedate
Paralyze
Sellick maneuver for intubation
Cric or needle cricothyroidomy (jet insufflation)
For emergency airway 7
-
Basic Respiratory/Airway
Concepts
Continuous positive airway pressure
CPAP delivers pressurized air during inspiration & expiration via mask
Bi-level positive airway pressure
Bi-PAP alters pressure, increasing during inspiration
Positive End Expiratory Pressure (PEEP)
Increases alveolar gas exchange
May cause atelectasis
8
-
Basic Intervention
Aside from administration of oxygen, an essential item of equipment for preserving airway integrity once the airway is established is:
A. An accurate flow meter.
B. A suction catheter.
C. An ET tube.
D. A laryngoscope.
9
-
Device flow and concentrations
Device Gas Flow FiO2Nasal cannula 1 6 L/min 24 % - 44%
Simple face mask 8 10 L/min 40% 60%
Venturi mask Varies by dial 24%, 28%, 35%, 40%
Non re-breathing
mask
8 15 L/min 60% 100%
10
-
Basic Intervention
A mother comes into the ED carrying her 12-month-old child, who has stridor and is cyanotic. The mother states that the child was eating a hotdog before her symptoms began. Initial intervention would include:
A. Opening the airway and try to remove the food.
B. Delivering five back blows and five chest thrusts.
C. Grabbing the child by the legs and turning her upside down.
D. Performing a needle cricothyrotomy with a 14-gauge needle.
Holleran, 2001
11
-
Physiology of Ventilation
Control of Ventilation
Lung Volumes and Capacities
Compliance
Ventilation and Perfusion Ratios
Breath Sounds
12
-
Physiology of Ventilation
Ventilation
Movement of air in and out of the lungs
Occurs in two phases
Inspiration (Active)
Expiration (Passive)
13
-
Physiology of Ventilation
Controls of Ventilation
Voluntary
Involuntary
Medulla sets basic pattern of
breathing (brainstem)
Located in Brainstem
Rhythmic stimulation of
intercostal muscles & diaphragm
14
-
Lung Volumes and
Capacities
Tidal volume Normal is 5-8ml/kg
Residual volume
Minute volume Normal 5-7L/min
Vital capacity Normal 4500-5000ml
Functional residual capacity Normal 2200-2400ml
Alveolar ventilation Volume that reaches alveoli and participates in gas exchange
Anatomic dead space Volume remaining in conducting airways
15
-
Factors Affecting
Ventilation
Elasticity
Ability of the lungs to collapse and
recoil
Compliance
Ease with which the lungs expand
Surfactant
Reduces alveolar surface tension
16
-
Factors Affecting
Ventilation
Airway Resistance
Force that must be overcome for air to move in and out
Increased with Cystic Fibrosis, Asthma Attack
Work of Breathing
Amount of oxygen consumed to move air
Decreased compliance with Pulmonary Edema
Increased airway resistance, Increased RR
17
-
Physiology of Perfusion
Normal Gas Exchange
Depends on:
Adequate Ventilation
Adequate Perfusion
Adequate Diffusion
HIGHER concentration to LOWER
concentration
V/Q Matching18
-
Breath Sounds
19
-
Non-invasive Ventilation
Methods
Continuous positive airway pressure
CPAP delivers pressurized air during inspiration & expiration via mask
Bi-level positive airway pressure
Bi-PAP alters pressure, increasing during inspiration
Positive End Expiratory Pressure (PEEP)
Pressure continues through the end of the patients exhalation
Increases alveolar gas exchange
May cause atelectasis
20
-
End Tidal CO2
Pulse oximetry reflects
oxygenation, End Tidal CO2reflects ventilation.
21
-
Asthma
Chronic reversible, obstructive disorder Airway inflammation
Increased airway responsiveness
Multiple immunologic and non-immunologic triggers
Onset typically occurs before age 10 > 30% diagnosed in childhood will have it as an adult
> 4000 deaths each year
22
-
Pathophysiology
Immune system releases
various chemical mediators in
response to a
trigger/precipitating factor
Mediators cause smooth
muscle contraction,
vasodilation, mucosal edema,
and increased mucus secretion
23
-
AsthmaAcute Clinical Manifestations
Dyspnea at rest
Diffuse wheezing
Both insp. & exp.
Prolonged expiration phase
Diminished breath sounds
Cough
Reduced peak flow
Increased work of breathing
Tachycardia
Hyperresonance
Diaphoresis
Restlessness
Low Sats
Hypoxemia on ABGs
24
-
25
-
AsthmaManagement
Supplemental oxygen
Provide humidification
IV access and fluids
Bronchodilators
Corticosteroids
Heliox and/or
Magnessium
Secretion clearance
Anticipate
ventilatory support
Pt/family education
26
-
P.Z. a 44-year-old asthmatic measures her
peak flow rate. Peak expiratory flow rate
should be
A. greater than 80% of predicted or personal best
B. less than 50% of predicted or personal best
C. about 20-30%
D. half of predicted or personal best
-
Question????
Measurement of peak expiratory flow rate is a useful tool in
the management of asthma because:
A. Rising values can indicate and impending
exacerbation of asthma
B. It helps clear airway passages of mucus plugs
C. Measurement does not rely on patient effort
D. In can document reversibility of airway narrowing
ENA, CEN Review Manual, 2001 28
-
Question????
A patient experiencing an acute asthma exacerbation
states that his routine medication includes the use of a
cromolyn (Intal) inhaler. This medication is given to
A. Relieve acute bronchospasm on an as-
needed basis
B. Block the release of chemical mediators
from mast cells
C. Inhibit cough receptors in the bronchial
lining
D. Block the uptake of calcium in the bronchial
smooth muscle
ENA, CEN Review Manual, 2001 29
-
Question????
When you are teaching an asthma patient how to avoid
potential triggers of the disease, which of the following
should you be sure to discuss?
A. Avoidance of spicy foods can help to reduce
asthma attacks
B. Exacerbation of asthma can be reduced by
decreasing physical activity
C. Chronic postnasal drip can contribute to
recurrent asthma attacks
D. Most triggers of asthma can be avoided
ENA, CEN Review Manual, 2001
30
-
Question????
A patient presents to the ED with a chief complaint
of sore throat, stuffy nose, and a nonproductive
cough that keeps him awake at night. A workup
has been complete and his CXR is negative. You
suspect that this patient has:
A. COPD
B. Asthma
C. Acute bronchitis
D. Pneumonia
ENA, CEN Review Manual, 2001 31
-
Acute Bronchitis
Assessment
Recent URI
Dry, hacky, cough
Nonproductive initially
Normal RR
Use of accessory muscles
Prolonged expiratory phase
Rhonchi, wet lung bases
Normal CXR32
-
Acute Bronchitis
Management
Rest
Humidification of air or supplemental
O2
Remove irritants
Increase PO fluid intake
Bronchodilators
Cough medications
33
-
Bronchiolitis
Assessment
Profuse secretions
Low-grade fever
Rhinorrhea
Cough
Poor feeding
Tachypnea
Tachycardia
Decreased sats
Signs of respiratory distress
Lethargy
34
-
Bronchiolitis
Management
Maintain ABCs
Pay close attention to infants
RSV culture
Oxygen therapy
Nebulizers for wheezing
Ribavirin for RSV
35
-
Question????
A 5-yr-old girl is brought to the ED by her family.
Her parents state that she has been febrile,
lethargic, and unable to lie down and has been
drooling. During the initial assessment of this
patient, the emergency nurse should do all of the
following except:
A. Assess the childs level of consciousness
B. Look down the childs throat
C. Assess the childs respiratory status
D. Assess the childs circulatory status
Holleran, 2001
36
-
Question????
A 21-year-old woman comes to the ED with a
chief complaint of persistent sore throat, high
fever, and inability to swallow. She is positioned
in the tripod position and appears anxious. You
suspect:
A. Croup
B. Epiglottitis
C. A foreign body aspiration
D. Pneumothorax
JEN, 28:2, 200237
-
Epiglottis
The initial care for a child who is suffering respiratory
distress from acute epiglottitis would include:
A. Administration of chloramphenicol
B. Administration of racemic epinephrine
C. Obtaining x-ray films of the childs neck
D. Preparing the child for intubation
Holleran, 2001 38
-
Epiglottitis
Holleran, 2001
The most common cause of epiglottitis is:
A. Streptococcus
B. Haemophilus influenzae
C. Staphylococcus
D. Pneumococcus
39
-
Epiglottitis
Causes
H. Influenzae
Staph
Strep
Laryngospasm possible upon visualization of epiglottis
Potential life-threatening condition characterized by edema of the epiglottis and epiglottic folds not extending below the vocal cords
40
-
Clinical Findings
Drooling
Acute/severe sore throat
Tripod or sniffing position
Dysphagia, dysphonia or aphonia
Inspiratory stridor, expiratory snore
Substernal or supraclavicular
retractions
Tenderness on palpation of the
anterior neck and hyoid bone
41
-
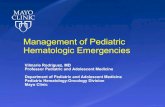
Thumb
Sign
Knoop, Stack, 2002 Atlas of Emergency Medicine42
-
Management
Decrease stress
Cool humidified oxygen
Have emergency surgical airway
equipment in room with patient
Antibiotics
Delay any diagnostic procedures
except lateral neck x-ray until
epiglottitis is ruled out or airway is
secured
43
-
Question????
A 4-yr-old child presents to the ED with a
barky cough, stridor, retractions, and
hypoxia. This child is most likely to have
A. Asthma
B. Croup
C. Pneumonia
D. Epiglottitis
ENA, CEN Review Manual, 200144
-
Croup????
Upon assessment, the nurse would expect to
note which early signs of hypoxemia in this
patient?
A. Use of accessory muscles
and development of a resonant cough
B. Expiratory stridor and cyanosis
C. Lethargy and tachypnea
D. Restlessness and a rapidly increasing
heart rate
Vonfrolio, 1998
45
-
CroupManagement
The nurse knows that management of a child with
croup is primarily directed toward:
A. Maintaining the patients airway and
adequate respiratory exchange
B. Maintaining acid-base balance
C. Increasing the humidification of inspired
air
D. Liquefying respiratory secretions
Vonfrolio, 1998 46
-
CroupLaryngotracheobronchitis
Affects children 6 months - 4
years
Viral illness with slow onset (few
days)
Barky cough stridor low fever
Aerosolized (racemic)
epinephrine steroids cool air
mist
Must rule out epiglottitis
47
-
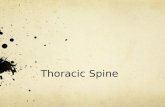
Normal X-Ray Steeple Sign
48
-
Pertussis
(Whooping Cough)
Acute, highly contagious bacterial infection
Bordetella pertussis ( gram negative cocci)
Infants & children up to 4 years
Peak incidence late summer & fall
7-10 day incubation (up to 21 days)
Airbornespread by coughing & sneezing 49
-
50
-
Pertussis
(Whooping Cough)
Severe, paroxysmal explosive coughing
Catarrhal stage: URI symptoms
Paroxysmal stage (2 4 weeks)
Apnea may occur in infants
Convalescent stage
Isolation
Erythromycin & palliative treatment
Patient education
51
-
Pneumonia
Acute infection of lung parenchyma
Impairs gas exchange
Pathogens may be bacterial, viral,
fungal, protozoan or others
Majority are viral
Bacterial cause majority of deaths
52
-
Pneumonia
Assessment
Dyspnea
Productive cough
Pleuritic chest pain
Fever/chills
Tachypnea
Dullness on percussion
Coarse crackles
Bronchial breath sounds
over affected lobe
Tachycardia53
-
Pneumonia
Management CXR
Sputum gram stain & C&S
Blood cultures
Position to facilitate breathing
Humidified oxygen
Secretion removal
Administer abx
Prepare for ventilatory support
Monitor for dysrhythmias 54
-
Indications for
Hospitalization
PaO2 < 65mmHg, SaO2 < 92%,
PaCO2 > 40mmHg
Patients unable to take
adequate fluids
Patients in a debilitated state,
exhaustion
Significant effusion on CXR
Suspicion of PCP
55
-
Question????
An obese 36-yr-old female present to your ED with sudden
onset of left-sided chest pain and shortness of breath. She
is diaphoretic, pale and in acute respiratory distress. She
denies any trauma, fever, n/v. Past medical history is
unremarkable except that she was placed on BCP 6 months
ago. Initial vital signs are BP 100/60, HR 120, RR 36/min,
and O2 saturations 92%. Based on your assessment, you
suspect the patient has:
A. Pericarditis
B. Acute coronary syndrome
C. Pulmonary embolus
D. Viral pneumonia56
-
Pulmonary Embolus
Risk factors
Virchows triad Hypercoagulability
Vessel injury
Venous stasis
Immobilization
Smoker
Oral BCP
Lung Bone Fractures
57
-
Pulmonary Embolus
Manifestations
Tachypnea
Tachycardia
Dyspnea
Anxiety
Chest pain
Cough
Right sided S2
Hemodynamic
instability
Hypotension
Shock
Signs of Rt
ventricular
failure
58
-
Hypoxic vasoconstriction
Decreased surfactant
Release of neurohumural mediators
Pulmonary edema
Atelectasis
Venous Stasis
Vessel Injury
Hypercoagulability
Thrombus Formation
Dislodgement of portion of thrombus
Tachypnea, Dyspnea, Hypoxemia,
Dead space, V/Q imbalances, Shock
Occlusion of part of pulmonary circulation
59
-
Pulmonary Embolus
Dx and Management
ABGs
Decreased PaO2, SaO2,
and SvO2
Respiratory alkalosis
D-dimers
Atrial dysrhythmias
New RBBB
CXRleast beneficial
V/Q scan
Angiography
Prevent embolus formation
ABCs
High-flow oxygen
Cardiopulmonary support
Baseline clotting profiles
Thrombolytic therapy
Heparin
LMWH
Oral anticoagulation
60
-
Pulmonary Embolus
When the nurse dorsiflexes the patients foot, the
patient complains of calf pain. The nurse correctly
interprets this response as an indication of a positive:
A. Trousseaus sign
B. Homans sign
C. Kehrs sign
D. Babinskis reflex
Vonfrolio, 1998
61
-
Atelectasis
When assessing breath sounds in a patient with
atelectasis, the nurse would expect to hear bronchial
breath sounds over the:
A. Carina
B. Middle of the right lung lobe
C. Right main-stem bronchus
D. Left main-stem bronchus
Vonfrolio, 199862
-
Pleural Effusion
Physical examination of a patient diagnosed
with a pleural effusion will reveal:
a) Increased tactile fremitus
b) Resonance upon percussion
c) Tracheal deviation toward the affected
side
d) Decreased or absent breath sounds
(JEN, 31:3, 2005)
63
-
Pleural Effusion
Fluid collection in the pleural space
Blood - hemothorax
Chyle - chylothorax
Serous serous effusion
Purulent empyema
64
-
S/S
Cough
Dyspnea
Use of accessory muscles
Fever
Increased fremitus above effusion, absent fremitus over effusion
Dullness to percussion
Lethargy/malaise
Treatment
Thorocentesis
Chest tube
Oxygen
Possible antibiotics
65
-
Cor Pulmonale
Alteration in the structure and
function of the right ventricle due to
a primary disorder of the respiratory
system
Pulmonary vasoconstriction
Primary lung disorders that
compromise the pulmonary
vascular bed (i.e. emphysema,
pulmonary embolism)
Idiopathic primary pulmonary
hypertension 66
-
Clinical Manifestations
Split 2nd heart sound
Right ventricular
failure
Distended neck veins
Right ventricular 3rd
heart sound
Peripheral edema
Treatment
Treat underlying
disorder
Avoid Fluid loading
Vasopressors
Oxygen
Vasodilators
67
-
Question????
A 52-yr-old male presents to the ED with complaints of
shortness of breath. He is unable to speak in complete
sentences. He reports a chronic cough with thick sputum.
He has smoked 1 packs of cigarettes for over 25 years.
On physical exam, he has scattered rhonchi and expiratory
wheezes, peripheral edema, and distended neck veins. The
history and clinical findings are consistent with a diagnosis
of:
A. Pneumonia C. Chronic bronchitis
B. Pulmonary edema D. Asthma
68
-
Emphysema
Disorder of impeded expiration
caused by:
Permanent over-distention of
alveoli
Loss of elastic recoil of the lungs
(compliance)
Increased dead space and
decreased functional lung tissue
69
-
Chronic Bronchitis
Inflammation of bronchi
Increased mucus production
Chronic cough
Chronic irritation
Loss of cilia
Peripheral mucus plugging
Airway collapse with air trapping
Chronic hypoxemia with hypercapnia
70
-
Clinical Presentation
Dyspnea on exertion progressing to
dyspnea at rest
Crackles, rhonchi, expiratory wheezes
Inability to speak in complete sentences
Pulsus paradoxus
Hypoxemia and hypercarbia on ABGs
Barrel chest appearance
Labs polycythemia, increased WBC,
eosinophilia, decreased alpha-antitrypsin
enzyme is indicative of emphysema
71
-
Chronic Bronchitis Management
72
-
Discharge Teaching
Exercise
Cough and deep breathing
Adequate hydration
Medication education
Pursed lip breathing or
diaphragmatic breathing
Immunizations
73
-
Emphysema
Patient teaching for a patient with emphysema should
include:
A. The importance of being vaccinated each year
against pneumococcal disease.
B. the need for prophylactic antibiotic therapy
when a family member is ill.
C. The need for adequate hydration to reduce
mucus tenacity
D. The importance of smoking cessation to
reverse structural damage caused by the
disease
ENA, CEN Review Manual, 2001
74
-
Rib/Sternal Fractures
Associated with blunt trauma
Results in decreased minute
ventilation
splinting from pain
pulmonary shunting from atelectasis
and hypoxia
Must consider concomitant injuries
1st rib fractures seen with injuries to
subclavian artery and aortic rupture
Lower rib fractures associated with
spleen or liver injuries75
-
Rib/Sternal Fractures
Assessment
Chest wall pain
Aggravated with deep breathing &
coughing
Point tenderness
Subcutaneous emphysema
Hypoventilation
Shallow respirations
76
-
Rib/Sternal Fractures
Management
Monitor respiratory status
Analgesics
Cough & deep breathe
Incentive spirometry
Complications
Pneumothorax
Hemothorax77
-
Flail Chest
Fracture of two or more ribs in two
or more places
Costochondral separation
Sternal fracture
Results in free-floating segment
and paradoxical chest wall
movement
78
-
Flail Chest Assessment
Rapid labored breathing
Hyperventilation (early)
Paradoxical chest wall movement
Crepitus of chest wall
Diaphoresis
Pain
Dyspnea
Hypoxia
Diminished breath sounds
Respiratory failure
79
-
Flail Chest Management
ABCs
May require intubation
High flow O2 Stabilize chest wall
Turn on affected side
IV access/fluid resuscitation
Pain management
Monitor ABGs
Anticipate need for thorcostomy
Continuous monitoring of respiratory status 80
-
Pneumothorax
A 30-yr-old man has attempted suicide by shooting
himself in the left upper chest. On arrival to the ED,
the patient is alert, complaining of shortness of
breath, and is pale and diaphoretic. His vital signs
are BP 80/palpation, HR 140, RR 32/min. The
emergency nurse needs to assess quickly for the
presence of:
A. Breath sounds
B. Peripheral edema
C. Capillary refill
D. Altered mental statusHolleran, 2001 81
-
Pneumothorax Accumulation of air in pleural space
creating loss or collapse of the lung
Loss of intrapulmonary/intrapleural
subatmospheric pressure
Elastic recoil leads to collapse
Decreased area for
ventilation/perfusion
Hypoxemia
82
-
Pneumothorax
Results from blunt or penetrating trauma May be spontaneous
May be closed, open and can become tension ptx
Clinical manifestations Dyspnea, tachypnea, tachycardia,
Decreased or absent breath sounds on affected side
Subcutaneous emphysema +/-
Management Chest Tube
83
-
Pneumothorax
No breath sounds are auscultated on the left side.
The patients respiratory distress increases and he
becomes agitated. Until a physician is available, a
critical intervention the emergency nurse may
perform is
A. Obtain central line access
B. Perform a needle thorocotomy
C. Place the patient on a pulse oximeter
D. Obtain an emergent chest radiograph
Holleran, 2001
84
-
Question????
The correct location to perform a needle
thoracentesis is:
A. Unaffected side, third intercostal space at
the midclavicular line
B. Affected side, fifth intercostal space, at
the anterior axillary line
C. Unaffected side, second intercostal
space, midclavicular line
D. Affected side, second intercostal space,
midclavicular line 85
-
Pneumothorax
After the emergency nurse performs the needle
thorocostomy, evaluation of the effectiveness of this
procedure would include all of the following except:
A. A rush of air after insertion of the needle
B. Improvement in the patients blood pressure
C. A dramatic increase in the patients
shortness of breath
D. Decrease in the patients shortness of
breathHolleran, 2001 86
-
Chest Tube Management
A chest tube is inserted into the patients chest by the emergency
physician. The tube is connected to a water-seal bottle that has
a moderate air and fluid leak seen on expiration. When the
patient is taken to the radiology department, the bottle is
accidentally broken. Which nursing action should be taken?
A. Remove the chest tube immediately to prevent
aspiration of glass particles
B. Apply a clamp to the chest tube near the insertion site
and instruct the patient to exhale deeply
C. Pinch the chest tube, place the end of the tube in a
bottle of sterile saline or water and encourage
the patient to cough and breathe deeply
D. Use the phone in radiology to order a new bottle an
and do not manipulate the chest tube 87
-
Hemothorax
Clinical Manifestations
Dyspnea, chest pain
Dullness on percussion
Decreased or absent BS
Hypoxia
Respiratory distress
Signs of shock
Management
Chest tube insertion
Autotransfusion
Thoracotomy
Fluid resuscitation
Blood product transfusion
88
-
Question????
An unrestrained female driver is brought to the ED by
EMS. Paramedics report she was driving an old car
without airbags and that the steering wheel was bent. The
patient is awake and alert. She is pale and anxious with
labored respirations. She states that another driver cut
her off at an intersection. You note paradoxical chest wall
movement and suspect a flail chest. Which of the
following would be your primary concern for this patient?
A. Pulmonary contusion
B. Deep vein thrombosis
C. Facial lacerations
D. Concurrent thoracic vertebral fracture89
-
Pulmonary Contusion
Bruising to the lung parenchyma
resulting in hemorrhage into eh alveoli
and small airways
Airway collapse, loss of ventilation
and pulmonary shunting
Classic symptom is progressive
dyspnea and hypoxemia
Treat with supplemental O2,
supportive ventilatory management,
and pain management for frequently
associated rib fractures 90
-
Question????
A victim of a stab wound to the epigastric area
presents to the ED. Upon evaluation, he suddenly
develops shortness of breath, chest pain and
decreased breath sounds. You suspect:
A. Diaphragmatic tear
B. Myocardial contusion
C. Flail chest
D. Rib fractures
ENA, CEN Review manual, 2001
91
-
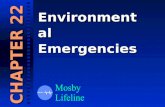
Pathophysiology of ARDS
Smeltzer, Bare, Hinkle & Cheever. 2008. Brunner & Suddarths Textbook of Medical-Surgical Nursing 11th edition
92
-
ARDS
Clinical Manifestations
Rapid shallow breathing
Dyspnea
Respiratory alkalosis
Decreased lung compliance
Refractory hypoxemia
Progressive metabolic acidosis
Diffuse alveolar infiltrates on CXR 93
-
Management
Ventilatory support
Mechanical ventilation
PEEP
Increases FRC and decreases dead space (recruits alveoli)
Sedation
Careful Fluid Management
Proning/Rotation Therapy94
-
ABGs
Condition pH PCO2 HCO3
Respiratory
Acidosis
normal
Respiratory
Alkalosis
normal
Metabolic Acidosis normal
Metabolic Alkalosis normal
95
-
ABGs Normal Values
Variable Normal Value
pH 7.35-7.45
PaO2 80-100
PaCO2 35-45
HCO3 22-26
BE + 2 -2
96
-
ABG Interpretation
pH 7.35 (< acidosis) 7.45 (> alkalosis)
CO2 35 (< alkalosis) 45 (> acidosis)
HCO3 22 ( alkalosis)
Compensation is based on the pH:
If the pH is 7.35-7.45 and the other
values are abnormal, then the patient is
considered compensated
97
-
Steps to Determine
Step One: Look at the pH
If the pH is > 7.45 go to step 2 (pt is
alkaloid)
If the pH is < 7.35 go to step 3 (pt is
acidosis)
Step Twowhen the pH is elevated
pCO2 < 40mmHg alkalosis is
respiratory origin
pCO2 > 40mmHg or normal, alkalosis is
metabolic origin, go to step 4
98
-
Steps to Determine
Step Threewhen the pH is decreased
pCO2 > 40mmHg, acidosis is
respiratory
pCO2 < 40mmHg or normal, acidosis is
metabolic, go to step 4
Step Four
pH and bicarbonate are both
decreased= metabolic acidosis
pH and bicarbonate are both elevated=
metabolic alkalosis
99
-
Question????
A 78-yr-old male is brought to the ED from home with
complaints of fever, tachycardia and tachypnea.
His ABGs reveal pH 7.01; PO2 125mmHg; PCO242mmHg; HCO3 10mEq/liter.
The correct interpretation of these ABGs is:
A. Metabolic acidosis
B. Metabolic alkalosis
C. Respiratory acidosis
D. Respiratory alkalosis100
-
Question????
A patient has been in cardiopulmonary arrest for
approximately 15 minutes with ongoing resuscitative
efforts. His ABGs reveal:
pH 7.15; PO2, 50mmHg; PCO2, 68mmHg;
HCO3, 18mEq/liter
You interpret this as:
A. Fully compensated respiratory acidosis
B. Fully compensated metabolic acidosis
C. Partially compensated respiratory alkalosis
D. Mixed metabolic and respiratory acidosis101
-
Question????
Interpret the following ABGs:
pH 7.60; PO2 , 140mmHg; PCO2, 15mmHg;
HCO3, 22mEq/liter
A. Metabolic acidosis
B. Metabolic alkalosis
C. Respiratory acidosis
D. Respiratory alkalosis
102
-
Question????
An anxious, panic-stricken patient arrives in the ED
with a chief complaint of dyspnea, rapid respiration and
periorbital edema. All serious causes for this breathing
pattern are eliminated and the patient is diagnosed with
hyperventilation. Which of the following findings do you
anticipate?
A. Respiratory Alkalosis
B. Dehydration
C. Stroke
D. Metabolic acidosisENA, CEN Review Manual, 2001
103
-
Question????
Factors that may limit the usefulness of a pulse
oximeter include:
A. Limited ambient light
B. Carbon monoxide poisoning
C. Normovolemia
D. Limited patient movement
104
-
Question????
Respiratory syncytial virus (RSV) not transmitted
by:
A. Large droplet aerosols
B. Sneezing
C. Visitors
D. Hand washing
105
-
Question????
A 67-yr-old female is brought to the ED in respiratory
distress. She is given supplemental oxygen via NRB.
Her vital signs are BP 158/84, HR 108, RR 28 and
labored. A stat CXR is performed and the physician
orders nitroglycerin and lasix. The goal of this therapy
is to:
A. Increase preload and increase afterload
B. Decrease preload and increase afterload
C. Increase preload and decrease afterload
D. Decrease preload and decrease afterload
106
-
107
-
References
Buttaro, T. M., Trybulski, J., Bailey, P. P., & Sandberg-Cook, J. (2008). Primary care a collaborative approach (3rd ed.). St. Louis: Mosby Elsevier.
Crain, E. F., & Gershel, J. C. (2003). Clinical manual of emergency pediatrics(4th ed.). New York: McGraw-Hill.
Dains, J. E., Baumann, L. C., & Scheibel, P. (2003). Advanced health assessment and clinical diagnosis (2nd ed.). St. Louis: Mosby.
Danis, D. M. , Blansfield, J. S., & Gervasini, A. A. (2007). Handbook of clinical trauma care: the first hour (4th ed.). St. Louis: Mosby Elsevier.
108
-
References Diaz, S. E. (2006). The little black book of emergency medicine (2nd
ed.). Boston: Jones and Bartlett.
Edmunds, M. W. & Mayhew, M. S. (2004). Pharmacology for the primary care provider (2nd ed.). St Louis: Elsevier Mosby.
Field, J. M. (2006). Advanced cardiac life support. Dallas: American Heart Association.
Guyton, A. C. & Hall, J. E. (2000). Textbook of medical physiology(10th ed.). Philadelphia: W. B. Saunders. 109
-
References
Hawkins, H. S. (2004). Emergency nursing
pediatric course (3rd ed.). Des Plaines, IL:
Emergency Nursing Association.
Hay, W. W., Levin, M. J., Sondheimer, J. M.,
& Deterding, R. R. (2003). Current diagnosis
and treatment in pediatrics (18th ed.). New
York: McGraw Hill.
Hazinski, M. F. (2006). Basic life support for
healthcare provider. Dallas: American Heart
Association.
Holleran, R. S. (2005). Emergency and
transport nursing examination review (4th
ed.). St. Louis: Elsevier Mosby.110
-
References
Howard, P. K. & Steinman, R. A. (2010). Sheehys Emergency Nursing Principles and Practice (6th ed.). St. Louis: Mosby.
Hoyt, K. S. & Selfridge-Thomas, J. (2007). Emergency nursing core curriculum (6th ed.). St. Louis: Saunders Elsevier.
Karch, A. M. (2003). Nursing drug guide. Philadelphia: Lippincott.
Ma, O. J., Cline, D. M., Tintinalli, J. E., Kelen, G. D., & Stapczynski, J. S. (2004). Emergency medicine manual (6th ed.). New York: McGraw-Hill.
111
-
References
McCance, K. L., & Huether, S. E. (2006). Pathophysiology: The biologic basis for disease in adults and children (5th ed.). St. Louis: Mosby.
Trott, A. T. (2005). Wounds and lacerations (3rd ed.). St. Louis: Elsevier Mosby.
Pagana, K. D. & Pagana, T. J. (2009). Diagnostic and laboratory test reference (9th ed.). St. Louis: Mosby.
Ralston, Mark. (2006). Pediatric advanced life support. Dallas: American Heart Association.
112