Describing the causes of Near-Miss Maternal Morbidity and ...

Queensland Maternal and Perinatal Quality Council
20
0
10
20
30
40
NSW Vic Qld WA SA Tas ACT NT
State
Per
cent
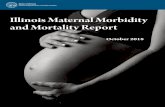
7. Maternal morbidity Tables 5 and 6 describe six standard ACHS/RANZCOG obstetric clinical indicator outcomes for Queensland for 2002 and 2003. They are presented by size of facility of birth for public and private facilities separately. Private facilities, compared with public facilities, consistently demonstrated higher intervention rates (caesarean section, induction of labour, perineal surgical repair) and lower rates for successful vaginal birth after previous caesarean section. National comparative data is presented on three related obstetric quality indicators: Induction of labour rates in low risk parturients (aged 25-29, nulliparous, vertex presenting, 37-41 weeks gestation) (Figure 7), caesarean section rates for low risk parturients (Figure 8), and length of hospital stay for uncomplicated vaginal and caesarean births (Figure 9). Of particular note is that, in 2003, Queensland fell in the mid range (30%) for induction of labour rates for low risk women, and it had the highest caesarean section rate in Australia (24%) for this low risk group (see Figures 7 and 8). Such data need careful interpretation by the managers of maternity services in Queensland and these services are encouraged to review these data as part of their quality improvement processes. Length of stay in hospital following birth is used as a proxy measure for service efficiency. Queensland, in the 2002/2003 fiscal period, had the lowest lengths of stay for both uncomplicated vaginal births (2.4 days) and caesarean births (3.9 days) (see Figure 9). Such efficiencies must be assessed alongside maternal and neonatal morbidity figures to ensure there is not a trade off between service efficiency and quality. Further discussion on other clinical quality indicators is provided in section 10. Figure 7. Inductions for selected nulliparae, public hospitals, 2003
Source: SCRGSP (2005) Note: 2003 data for the AT and NT are not available. Data for Queensland are preliminary and subject to revision.

Queensland Maternal and Perinatal Quality Council
21
Table 5. ACHS/RANZCOG Obstetric and Gynaecology Clinical Indicators by size of facility of birth, Public and Private Facilities, Queensland, 2002 Clinical indicators by size of facility (births per year) More than 2,000 1000-1999 500-999 Less than 500 Total (b) Type of accommodation of mother Public Private Public Private Public Private Public Private Public Private Total (c) MOTHERS 1. Induction of labour other than for defined indications (d)
Mothers who had an induction of labour other than for defined indications (No.)
776
927
707
563
247
753
258
419
1,988
2,662
4,650
1.1 As a proportion of all mothers who had an induction (%)
26.2
60.4
23.1
59.3
28.2
57.9
34.0
51.2
26.0
57.8
37.9
1.2 As a proportion of all mothers (%)
6.5
15.9
5.9
14.6
7.2
17.0
6.3
15.1
6.3
15.7
9.6 2. The rate of vaginal delivery following primary Caesarean section
Mothers who had a vaginal delivery following primary Caesarean section (No.)
224
66
202
52
72
76
49
33
547
227
774
2.1 As a proportion of all mothers who had a previous primary Caesarean section (%)
22.8
7.4
28.3
8.7
26.4
14.8
19.0
11.3
24.6
9.9
17.1 3. Primary Caesarean section for failure to progress (e) Mothers who had a primary Caesarean section for failure to progress after a period of labour with cervical dilatation of 3cm or less (No.)
93
101
77
78
36
90
32
33
238
302
540
3.1 As a proportion of all mothers who had a primary Caesarean section for specified reasons (f) (%)
4.7
7.8
5.1
8.6
8.1
11.1
9.2
7.3
5.6
8.7
7.0 Mothers who had a primary Caesarean section for failure to progress after a period of labour with cervical dilation of more than 3cm (No.)
413
148
330
163
101
177
103
91
947
579
1,526
3.2 As a proportion of all mothers who had a primary Caesarean section for specified reasons (f) (%)
21.0
11.4
21.9
18.1
22.7
21.9
29.7
20.3
22.2
16.8
19.8 4. Primary Caesarean section for fetal distress (e) (g)
Mothers who had a primary Caesarean section for fetal distress after a period of labour (No.)
453
163
334
119
108
102
59
43
954
427
1,381
4.1 As a proportion of all mothers (%)
3.8
2.8
2.8
3.1
3.2
2.3
1.4
1.5
3.0
2.5
2.9
4.2 As a proportion of all mothers who had a primary Caesarean section (%)
21.7
9.7
20.1
10.7
23.3
10.9
16.4
8.3
20.9
10.1
15.7 5. Incidence of an intact lower genital tract in primiparous mothers delivering vaginally
Primiparous mothers delivering vaginally not requiring surgical repair of the lower genital tract (h) (No.)
1,190
251
1,401
97
376
251
464
114
3,431
713
4,144
5.1 As a proportion of all primiparous mothers delivering vaginally (%)
33.7
18.2
41.4
12.8
42.9
20.6
44.1
16.1
38.8
17.5
32.1 Number of mothers 11,902 5,837 11,908 3,858 3,417 4,442 4,118 2,780 31,345 16,917 48,262 LIVEBIRTHS 6. Apgar Score (i)
Liveborn babies with an Apgar score of 4 or below at 5 minutes post delivery (No.)
70
28
54
9
16
12
14
9
154
58
212
6.1 As a proportion of live births (%)
0.6
0.5
0.5
0.2
0.5
0.3
0.3
0.3
0.5
0.3
0.4
Number of livebirths 12,038 6,053
11,951 3,909 3,434 4,503 4,115 2,803 31,538 17,268 48,806 (a) The Australian Council on Healthcare Standards/The Royal Australian College of Obstetricians and Gynaecologists - Obstetric and Gynaecology Indicators - Version 3. (b) Excludes homebirths and births at an unknown facility. (c) Includes not stated accommodation type of mother. (d) Defined indications include: Diabetes, premature rupture of membranes, hypertensive disorders (including chronic renal disease), IUGR, isoimmunisation, fetal distress, IUFD, chorioamnionitis, and prolonged pregnancy (41 completed weeks, or more). (e) Where condition was reported as a labour and delivery complication. (f) For the purpose of this report, Caesarean sections for specified reasons are those where elective, repeat elective and social are not reported as the reason for Caesarean section. (g) May include some cases where meconium liquor was reported as a labour and delivery complication but not necessarily as an indicator of fetal distress. (h) This indicator uses the need for surgical repair as a measure of degree of severity of genital tract trauma. Therefore mothers with minor trauma not requiring repair are included. (i) Apgar score at 10 minutes post delivery is not collected by the Data Services Unit.
Source: PDCU

Queensland Maternal and Perinatal Quality Council
22
Table 6. ACHS/RANZCOG Obstetric and Gynaecology Clinical Indicators by size of facility of birth, Public and private facilities, Queensland, 2003
Clinical indicators by size of facility (births per year) More than 2,000 1000-1999 500-999 Less than 500 Total (b) Type of accommodation of mother Public Private Public Private Public Private Public Private Public Private Total (c) MOTHERS 1. Induction of labour other than for defined indications(d)
Mothers who had an induction of labour other than for defined indications (No.)
769
976
695
648
331
743
213
428
2,008
2,795
4,803
1.1 As a proportion of all mothers who had an induction (%)
23.6
57.7
26.3
62.2
33.5
57.6
30.0
53.9
26.4
58.0
38.7
1.2 As a proportion of all mothers (%)
5.4
16.3
6.7
17.5
8.9
16.3
5.0
16.3
6.2
16.5
9.7 2. The rate of vaginal delivery following primary Caesarean section
Mothers who had a vaginal delivery following primary Caesarean section (No.)
259
91
175
48
60
60
38
41
532
240
772
2.1 As a proportion of all mothers who had a previous primary Caesarean section (%)
20.3
9.2
24.9
7.9
22.5
9.9
14.1
12.4
21.2
9.5
15.3 3. Primary Caesarean section for failure to progress (e)
Mothers who had a primary Caesarean section for failure to progress after a period of labour with cervical dilatation of 3cm or less (No.) 74
71
93
92
56
86
25
39
248
288
536
3.1 As a proportion of all mothers who had a primary Caesarean section for specified reasons (f) (%) 3.0
5.6
6.8
11.5
10.2
10.8
7.0
8.6
5.3
8.6
6.7
Mothers who had a primary Caesarean section for failure to progress after a period of labour with cervical dilation of more than 3cm (No.) 549
173
358
121
126
162
123
90
1,156
546
1,702
3.2 As a proportion of all mothers who had a primary Caesarean section for specified reasons (f) (%) 22.6
13.6
26.2
15.1
23.0
20.3
34.6
19.9
24.6
16.4
21.2
4. Primary Caesarean section for fetal distress (e) (g)
Mothers who had a primary Caesarean section for fetal distress after a period of labour (No.)
497
196
298
114
125
125
54
61
974
496
1,470
4.1 As a proportion of all mothers (%)
3.5
3.3
2.9
3.1
3.4
2.7
1.3
2.3
3.0
2.9
3.0
4.2 As a proportion of all mothers who had a primary Caesarean section (%)
19.4
11.6
19.6
11.1
21.7
13.2
14.1
11.3
19.3
11.8
15.9 5. Incidence of an intact lower genital tract in primiparous mothers delivering vaginally
Primiparous mothers delivering vaginally not requiring surgical repair of the lower genital tract (h) (No.)
1,498
283
1,259
91
406
260
478
112
3,641
746
4,387
5.1 As a proportion of all primiparous mothers delivering vaginally (%)
35.8
20.0
40.2
11.9
41.7
21.5
44.9
16.3
38.9
18.3
32.7 Number of mothers 14,225 6,003 10,321 3,707 3,708 4,556 4,294 2,629 32,548 16,895 49,443 LIVEBIRTHS 6. Apgar Score (i)
Liveborn babies with an Apgar score of 4 or below at 5 minutes post delivery (No.)
85
20
37
4
11
11
17
5
150
40
190
6.1 As a proportion of live births (%)
0.6
0.3
0.4
0.1
0.3
0.2
0.4
0.2
0.5
0.2
0.4 Number of livebirths 14,373 6,174 10,374 3,758 3,741 4,613 4,296 2,663 32,784 17,208 49,992 (a) The Australian Council on Healthcare Standards/The Royal Australian College of Obstetricians and Gynaecologists - Obstetric and Gynaecology Indicators - Version 3. (b) Excludes homebirths and births at an unknown facility. (c) Includes not stated accommodation type of mother. (d) Defined indications include: Diabetes, premature rupture of membranes, hypertensive disorders (including chronic renal disease), IUGR, isoimmunisation, fetal distress, IUFD, chorioamnionitis, and prolonged pregnancy (41 completed weeks, or more). (e) Where condition was reported as a labour and delivery complication. (f) For the purpose of this report, Caesarean sections for specified reasons are those where elective, repeat elective and social are not reported as the reason for Caesarean section. (g) May include some cases where meconium liquor was reported as a labour and delivery complication but not necessarily as an indicator of fetal distress. (h) This indicator uses the need for surgical repair as a measure of degree of severity of genital tract trauma. Therefore mothers with minor trauma not requiring repair are included. (i) Apgar score at 10 minutes post delivery is not collected by the Data Services Unit.
Source: PDCU

Queensland Maternal and Perinatal Quality Council
23
0
5
10
15
20
25
30
NSW Vic Qld WA SA Tas ACT NT
State
Per
cent
Figure 8. Caesarean sections for selected nulliparae, public hospitals, 2003
Source: SCRGSP (2005) Note: 2003 data for the ACT and NT are not available. Data for Queensland are preliminary and subject to revision. Figure 9. Average length of stay for selected maternity-related AN-DRGs, public hospitals,
fiscal year 2002/03
0
2
4
6
NSW Vic Qld WA SA Tas ACT NT Aust
State
Day
s/se
para
tion
O01D caesarean delivery O60D vaginal delivery
Source: SCRGSP (2005)
Note: Includes AN-DRG O01D caesarean delivery without complicating diagnosis and AN-DRG O60D vaginal delivery without complicating diagnosis;

Queensland Maternal and Perinatal Quality Council
24
8. Perinatal mortality 8.1 Modus operandi All perinatal deaths in Queensland are subject to a systematic review process. Perinatal mortality data have been obtained from the Perinatal Data Collection Unit (PDCU, Queensland Health), the Registrar General for Births Deaths and Marriages and case summaries from hospital and regional perinatal mortality committees in Queensland. During 2002 and 2003, a number of local mortality committees collaborated with the Council in the perinatal mortality review process. Local committees classified 68.77% of the 2002 mortality cases and 65.42% of the 2003 mortality cases. In 2003 the working party of the Perinatal Morbidity and Mortality sub-committee received 55 (17.4%) case summaries and cause of death classifications assigned by these local committees to be quality checked. Of these cases, 83.6% of the classifications (n=46) were found to be correct, while 16.4% of the classifications (n=9) were changed. The terms of reference for the Perinatal Morbidity and Mortality sub-committee are: ♦ Review and report on patterns and trends of perinatal morbidity and mortality. ♦ Support and guide clinicians in clinical audit activities, including classification of perinatal
deaths and important perinatal morbidity. ♦ Determine and report on preventable factors. ♦ Liaise with appropriate local and national bodies in the identification of clinical indicators. ♦ Identify evidence-based health care interventions which may reduce morbidity and
mortality. ♦ Identify strategies for dissemination of information to clinicians. ♦ Identify research priorities into perinatal morbidity and mortality. The terms of reference for the Perinatal Mortality working party are: • Monitor the quality of classifications by undertaking quality assurance activities in
relation to ANZACPM and ANZNDC classifications • Provide support and feedback to local committees undertaking classifications • Maintain the Maternal and Perinatal Mortality Audit Guidelines in collaboration with
Maternal Mortality and Morbidity sub-committee • Make preliminary reports to the Perinatal Morbidity and Mortality sub-committee on
classified data • Participate in interpretation of data for the annual report • Meet annually with the relevant mortality sub-committee of Queensland Paediatric
Quality Council • Liaise with the national classification group Australian and New Zealand Mortality
Classification Special Interest Group

Queensland Maternal and Perinatal Quality Council
25
8.2 Clinical classification All perinatal deaths in the year 2002 and 2003 were classified according to the Australian and New Zealand Antecedent Classification of Perinatal Mortality (ANZACPM), and the Australian and New Zealand Neonatal Death Classification (ANZNDC). The purpose of classifying deaths according to the ANZACPM and ANZNDC systems is to focus on aetiology and to enable consideration of preventable factors associated with perinatal deaths through the systematic application of clinically relevant categories to large populations. (Further information about the classification systems is to be found in Appendices 12.2 and 12.3). The Council acknowledges and sincerely thanks clinicians who have participated in local mortality review and classification and those who have provided data to assist in review of perinatal deaths by the Council. 8.3 Data Collection Perinatal mortality data have been obtained from the Perinatal Data Collection Unit (PDCU) within Queensland Health, the Registrar General of Births Deaths and Marriages and from hospital and regional perinatal mortality committees in Queensland. The major data sources are the Perinatal Data Collection Forms (MR63d), the Medical Certificate of Cause of Perinatal Death, the Council’s Confidential Perinatal Mortality Case Summary Form, the hospital discharge summary and autopsy and placental pathology reports when available. All registered perinatal deaths in Queensland are documented by the Registrar General for Births, Deaths and Marriages. This information is then collected by the Perinatal Data Collection Unit (PDCU). For each death, hospitals provide the PDCU with information concerning the post mortem, placenta pathology and histology, neonatal discharge summary, the death certificate, and the perinatal data collection form (MR63-D). Copies of this information are obtained by the Clinical Quality Unit. Any further information needed to classify cause of death is requested through the Chief Health Officer. The Perinatal Mortality working party then reviews and classifies all mortality cases. 8.4 Perinatal mortality rates and trends
8.4.1 Multiple pregnancy
In 2002 and 2003 there were 3405 births from multiple pregnancies, contributing to 3.42% of all births (Table 7). Of these births, the percentage of non-Indigenous multiple births was 3.47% and the percentage of Indigenous multiple births was 2.50%. Looking at Queensland, the perinatal mortality rate for twins was 4.8 times the mortality rate for singletons. The mortality rate for triplets or higher was 3.2 times the mortality rate for singletons. The stillbirth rate for twins was three times the stillbirth rate for singletons, while the neonatal mortality rate for twins was 8.6 times the neonatal mortality rate for singletons.

Queensland Maternal and Perinatal Quality Council
26
Table 7. Births and perinatal mortality by plurality for all Queensland births and by Indigenous status of mother, Queensland, 2002 and 2003
Stillbirths Neonatal deaths
Perinatal deaths
Total births
Live births
n rate1 n rate2 n rate1 All Queensland Singleton 96158 95587 571 5.94 275 2.88 846 8.80 Twins 3262 3202 60 18.39 79 24.67 139 42.61 Triplets or higher 143 141 2 13.99 2 14.18 4 27.97 Total multiples 3405 3343 62 18.21 81 24.23 143 42.00 Total births 99563 98930 633 6.36 356 3.60 989 9.93 non-Indigenous Singleton 90634 90118 516 5.69 240 2.66 756 8.39 Twins 3122 3065 57 18.26 73 23.82 130 42.41 Triplets or higher 140 138 2 14.29 2 14.49 4 28.99 Total multiples 3262 3203 59 18.09 75 23.42 134 41.84 Total births 93896 93321 575 6.12 315 3.38 890 9.54 Indigenous Singleton 5524 5469 55 9.96 35 6.40 90 16.46 Twins 140 137 3 21.43 6 43.80 9 65.69 Triplets or higher 3 3 0 0.00 0 0.00 0 0.00 Total multiples 143 140 3 20.98 6 42.86 9 64.29 Total births 5667 5609 58 10.23 41 7.31 99 17.65
1 rate per 1,000 total births within the respective category 2 rate per 1,000 live births within the respective category 3 includes sixteen unknown Indigenous status 4 includes four unknowns Indigenous status 5 includes 20 unknown Indigenous status 6 Indigenous status of mother: Australian Aboriginal, Torres Strait Islander, or Australian Aboriginal and Torres
Strait Islander Table 8 presents the frequencies and mortality rates for singleton and multiple births classified using the ANZACPM cause of death. Among singletons, the most common causes of death were classified as ‘Congenital abnormality’ (rate of 2.11) and ‘Unexplained antepartum death’ (rate of 2.23). In contrast, the most common causes of death among multiples were classified as ‘Spontaneous preterm’ (rate of 18.80) and ‘Specific perinatal conditions’ (rate of 10.28). Multiple births were 18.30 more likely to die from ‘Specific perinatal conditions’, 11.81 more likely to die from ‘Spontaneous preterm’ and 8.07 more likely to die from ‘Fetal growth restriction’ than singletons.

Queensland Maternal and Perinatal Quality Council
27
Table 8. Perinatal mortality by ANZACPM cause of death and plurality, Queensland, 2002 and 2003
95%n % rate1 n % rate2 CI
1 Congenital abnormality 203 24 2.11 11 8 3.23 1.53 0.75-2.802 Perinatal infection 23 3 0.24 1 1 0.29 1.23 0.03-7.563 Hypertension 21 2 0.22 2 1 0.59 2.69 0.31-11.004 Antepartum haemorrhage 68 8 0.71 7 5 2.06 2.91 1.13-6.325 Maternal conditions 37 4 0.38 1 1 0.29 0.76 0.02-4.526 Specific perinatal conditions 54 6 0.56 35 24 10.28 18.30 11.61-28.527 Hypoxic peripartum death 24 3 0.25 1 1 0.29 1.18 0.03-7.228 Fetal growth restriction 28 3 0.29 8 6 2.35 8.07 3.18-18.179 Spontaneous preterm 153 18 1.59 64 45 18.80 11.81 8.68-15.91
10 Unexplained antepartum death 214 25 2.23 12 8 3.52 1.58 0.81-2.8211 No obstetric antecedent 21 2 0.22 1 1 0.29 1.34 0.03-8.36
846 100 8.80 143 100 42.00 4.77 3.97-5.71
Multiple Relative Risk
Total
ANZACPM cause of deathSingleton
1 rate per 1,000 singleton births : n=96,158 2 rate per 1,000 multiple births : n=3,405 3 risk for multiple birth Note: 95% CI calculated as per Ulm (1990)
8.4.2 Perinatal mortality rates using the Register of Births, Deaths and Marriages definition
Using the stillbirth definition of at least 20 weeks gestation or 400 grams weight at birth, the perinatal mortality rate in Queensland for the year 2002 was 10.27 per 1,000 total births, with a somewhat lower rate of 9.57 per 1,000 total births in 2003 (Table 9). The stillbirth rate in 2002 was 6.63 per 1,000 total births and the neonatal mortality rate was 3.66 per 1,000 live births. In comparison, in 2003 the stillbirth rate was 6.08 per 1,000 total births and the neonatal mortality rate was 3.52 per 1,000 live births. In 2002 the Indigenous perinatal mortality rate per 1,000 total births (19.22) was almost twice the non-Indigenous rate (9.73). This differential was slightly smaller in 2003 where the Indigenous perinatal mortality rate was 15.81 compared with the non-Indigenous perinatal mortality rate of 9.19. As seen in Table 9, over the period 2000 to 2003, the relative risk for Indigenous perinatal mortality, when compared with non-Indigenous perinatal mortality, has slightly decreased (1.97 to 1.72), largely due to the relative reduction in stillbirths (1.83 to 1.51).

Queensland Maternal and Perinatal Quality Council
28
0
5
10
15
20
25
30
1999 2000 2001 2002 2003
Year
Rat
e (p
er 1
000
birth
s)
non-Indigenous Stillbirth non-Indigenous Neonatalnon-Indigenous Perinatal Indigenous StillbirthIndigenous Neonatal Indigenous Perinatal
Table 9. Perinatal mortality by Indigenous status of mother, Queensland, 1999 to 2003
n rate1 95% CI n rate2 95% CI n rate1 95% CI
1999 48747 48400 347 7.12 6.40-7.12 170 3.51 3.01-4.06 517 10.61 9.72-11.542000 49318 48960 358 7.26 6.54-8.03 182 3.72 3.21-4.28 540 10.95 10.06-11.892001 49690 49327 363 7.31 6.59-8.08 199 4.03 3.50-4.61 562 11.31 10.37-12.462002 49195 48869 326 6.63 5.94-7.37 179 3.66 3.15-4.22 505 10.27 9.40-11.182003 50367 50061 306 6.08 5.43-6.78 176 3.52 3.03-4.06 482 9.57 8.74-10.44non-Indigenous
3
1999 45853 45534 319 6.96 6.23-7.74 152 3.34 2.84-3.89 471 10.27 9.34-11.202000 46471 46159 312 6.71 6.00-7.48 160 3.47 2.96-4.03 472 10.16 9.24-11.082001 46958 46629 329 7.01 6.28-7.79 174 3.73 3.21-4.30 503 10.71 9.80-11.672002 46437 46143 294 6.33 5.64-7.07 158 3.42 2.92-3.97 452 9.73 8.86-10.652003 47458 47178 280 5.90 5.24-6.61 156 3.31 2.82-3.85 436 9.19 8.36-10.07Indigenous4
1999 2894 2866 28 9.68 6.57-13.58 18 6.28 3.86-9.50 46 15.89 11.78-20.802000 2847 2801 46 16.16 11.98-21.15 22 7.85 5.06-11.45 68 23.88 18.70-29.882001 2732 2698 34 12.45 8.77-16.97 25 9.27 6.15-13.24 59 21.60 16.60-27.452002 2758 2726 32 11.60 8.08-15.95 21 7.70 4.91-11.33 53 19.22 14.55-24.732003 2909 2883 26 8.94 5.98-12.69 20 6.94 4.37-10.30 46 15.81 11.72-20.70Relative Risk for Indigenous
4
1999 0.91-2.05 1.08-3.07 1.12-2.102000 1.73-3.29 1.37-3.52 1.80-3.042001 1.21-2.53 1.55-3.77 1.51-2.642002 1.23-2.64 1.35-3.54 1.46-2.632003 0.97-2.27 1.24-3.34 1.24-2.341.51 2.10 1.72
Stillbirths Neonatal Deaths Perinatal Deaths
1.78 2.48 2.021.83 2.25 1.97
1.39 1.88 1.552.41 2.27 2.35
All Queensland
YearTotal
BirthsLive
Births
1 For all births of at least 400 grams weight or 20 weeks gestation 2 rate per 1,000 total births 3 rate per 1,000 live births 4 numbers include births where Indigenous status was not stated: 1 in 1999; 9 in 2000; 8 in 2001; 10 in 2002 and
8 in 2003 5 Indigenous status of mother: Australian Aboriginal, Torres Strait Islander, or Australian Aboriginal and Torres
Strait Islander 6 Indigenous vs non-Indigenous Figure 10 presents the rates of stillbirths, neonatal mortality and perinatal mortality by the Indigenous status of mother. As can be seen in the Figure, the Indigenous mortality rates have been consistently higher than the non-Indigenous mortality rates. Figure 10. Rates of perinatal mortality for non-Indigenous and Indigenous births,
Queensland, from 1999 to 2003. Note: Indigenous status of mother: Australian Aboriginal, Torres Strait Islander, or Australian Aboriginal and Torres Strait Islander

Queensland Maternal and Perinatal Quality Council
29
0
2
4
6
8
10
12
14
16
1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
Rat
e (p
er 1
000
birt
hs)
Stillbirth Neonatal Perinatal Stillbirth: all TOPs
Perinatal: all TOP Stillbirth: TOP no CA Perinatal: TOP no CA
8.4.2.1. Late terminations of pregnancy
Data on late terminations of pregnancy (>20 weeks gestation), as a result of voluntary interruption of pregnancy, have been reported in Queensland since 1995. No data are available for terminations less than 20 weeks gestation. Pregnancies may be terminated due to detected congenital anomalies (CA), for social/psychological reasons or for maternal medical or pregnancy complications (e.g., fulminating pre-eclampsia). In 2001 there were 54 terminations of pregnancy, of which 24 were due to congenital anomalies; in 2002 there were 28 terminations of pregnancies, of which 21 were due to congenital anomalies; while in 2003 of the 24 terminations of pregnancies, 23 were due to congenital anomalies. Figure 11 presents the stillbirth, neonatal mortality and perinatal mortality rates corrected for all terminations of pregnancies (all TOP) and corrected only due to social/psychological reasons (TOP no CA). After adjusting for termination of pregnancy, the increase in the stillbirth death rate is no longer apparent. The contribution to the stillbirth death rate of terminations for maternal social/psychologic indications has reduced over this period to the point where, for the years 2002 and 2003, the very small number of cases did not affect the unadjusted rate. Figure 11. Stillbirth, neonatal mortality and perinatal mortality rates in Queensland, 1999 to
2003, corrected for all late terminations (all TOP) and for late terminations not due to congenital anomalies (TOP no CA)
Note: Data includes three terminations at 19 weeks: one each in 2000, 2002, and 2003.
As seen in Table 10, the perinatal mortality rate generally decreased as birth weight increased. The exception to this pattern was the high mortality rate for babies weighing 4500 or more grams at birth. The perinatal mortality rate for babies weighing less than 500 grams was almost 100% (989.83 deaths per 1,000 total births).

Queensland Maternal and Perinatal Quality Council
30
Table 10. Perinatal mortality by birth weight, Queensland, 2002 and 2003
Stillbirths Neonatal deaths Perinatal deaths Birth weight (grams)
Total births
Live births n rate1 n rate2 n rate1
<500 295 70 225 762.71 67 957.14 292 989.83 500-749 279 193 86 308.24 96 497.41 182 652.33 750-999 241 208 33 136.93 32 153.85 65 269.71 1000-1499 711 663 48 67.51 25 37.71 73 102.67 1500-1999 1418 1378 40 28.21 25 18.14 65 45.84 2000-2499 4076 4034 42 10.30 19 4.71 61 14.97 2500-2999 14476 14418 58 4.01 36 2.50 94 6.49 3000-3499 34345 34297 48 1.40 32 0.93 80 2.33 3500-3999 31042 31010 32 1.03 16 0.52 48 1.55 4000-4499 10755 10746 9 0.84 3 0.28 12 1.12 4500+ 1925 1913 12 6.23 5 2.61 17 8.83 Total 99563 98930 633 6.36 356 3.60 989 9.93
1 rate per 1,000 total births within that birth weight 2 rate per 1,000 live births within that birth weight As gestational age increased, the perinatal mortality rate decreased (Table 11). This trend occurred for both stillbirths and neonatal mortality. Of note, there was a slight increase in the rate of mortality at 42 weeks or greater gestational age. The perinatal mortality rate for less than 24 weeks gestational age was close to 100% (977.90 per 1000 total births), and this can be accounted for by the high rate of neonatal deaths. Table 11. Perinatal mortality by gestational age at birth, Queensland, 2002 and 2003
Stillbirths Neonatal deaths Perinatal deaths Gestational Age
(weeks)
Total births
Live births n rate1 n rate2 n rate1
<24 362 115 247 682.32 107 930.43 354 977.90 24-27 428 359 69 161.21 93 259.05 162 378.50 28-31 969 904 65 67.08 28 30.97 93 95.98 32-36 6724 6617 107 15.91 47 7.10 154 22.90 37-41 89964 89822 142 1.58 80 0.89 222 2.47 42+ 1116 1113 3 2.69 1 0.90 4 3.58
Total 99563 98930 633 6.36 356 3.60 989 9.93 1 rate per 1,000 total births within the gestation age 2 rate per 1,000 live births within the gestation age

Queensland Maternal and Perinatal Quality Council
31
0
200
400
600
800
1000
19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42
Gestational age (weeks)
Rat
e (p
er 1
000
birth
s)
Stillbirths Neonatal deaths
Figure 12 shows there was a sharp drop in the perinatal mortality rate as gestational age increased. Figure 12. Perinatal mortality rates for individual gestational ages, Queensland, 2002 and
2003. As shown in Table 12, births to older women had the highest perinatal mortality rate. In particular the highest perinatal mortality rate occurred for births to women age 45 years or more, and this can be accounted for by the high rates of stillbirths and neonatal mortality. High perinatal mortality rates also occurred for births to women aged 40 to 44 years, which can also be accounted for by the high rate of stillbirths. Table 12. Perinatal mortality by age of mother, Queensland, 2002 and 2003
Stillbirths Neonatal deaths Perinatal deaths Age of Woman (years)
Total births
Live births n rate1 n rate2 n rate1
<20 6158 6108 50 8.12 32 5.24 82 13.32 20-24 17477 17360 117 6.69 79 4.55 196 11.21 25-29 28872 28728 144 4.99 92 3.20 235 8.14 30-34 31097 30910 187 6.01 96 3.11 284 9.13 35-39 13279 13183 96 7.23 42 3.19 138 10.39 40-44 2583 2546 37 14.32 12 4.71 49 18.97 45+ 97 95 2 20.62 3 31.58 5 51.55
Total 99563 98930 633 6.36 356 3.60 989 9.93 1 rate per 1,000 total births within the age group 2 rate per 1,000 live births within the age group
8.4.3 Perinatal mortality rates using World Health Organisation (WHO) definitions
The World Health Organisation (WHO) uses different definitions for fetal and neonatal deaths. To enable meaningful comparison, mortality rates using WHO definitions are provided here.

Queensland Maternal and Perinatal Quality Council
32
Using WHO definitions, a late fetal death is defined as a stillborn of not less than 28 weeks gestation or of not less than 1000 grams weight at delivery. A neonatal death is classified using the same parameters, in addition to being under seven days of age. Using these definitions, the crude perinatal mortality rate for Queensland was 4.85 per 1,000 total births for 2002 and 4.92 per 1,000 total births for 2003 (Table 13). Examining the 95% confidence intervals, there has been no significant differences in the rates of perinatal deaths from 1999 to 2003. Table 13. Perinatal mortality using the WHO International definition, Queensland, 1999 to
2003 Perinatal Deaths Year
Total Births
Live Births
n rate1 95% CI 1999 48554 48400 228 4.70 4.12-5.33 2000 49124 48960 251 5.11 4.51-5.76 2001 49500 49327 261 5.27 4.66-5.93 2002 49029 48869 238 4.85 4.26-5.49 2003 50225 50061 247 4.92 4.33-5.55
1 rate per 1,000 total births 8.5 Causes of specific perinatal mortality
8.5.1 ANZACPM causes of perinatal mortality
The main causes of death using the Australian and New Zealand Antecedent Classification of Perinatal Mortality (ANZACPM) clinical classification system are presented in Table 14. As seen in Table 14, using the ANZACPM cause of death, the most common causes of perinatal mortality were classified as ‘Unexplained antepartum deaths’ (rate of 2.27), ‘Spontaneous preterm’ (rate of 2.18), and ‘Congenital abnormality’ (rate of 2.15). The most common causes of stillbirths were classified as ‘Unexplained antepartum deaths’ (rate of 2.27) and ‘Congenital abnormality’ (rate of 1.17). ‘Spontaneous preterm’ (rate of 1.33) and ‘Congenital abnormality’ (rate of 0.99) accounted for the most common causes of neonatal mortality. Table 14. Perinatal mortality by ANZACPM cause of death, Queensland, 2002 and 2003
n % rate1 n % rate2 n % rate1
1 Congenital abnormality 116 18.33 1.17 98 27.53 0.99 214 21.64 2.152 Perinatal infection 14 2.21 0.14 10 2.81 0.10 24 2.43 0.243 Hypertension 13 2.05 0.13 10 2.81 0.10 23 2.33 0.234 Antepartum haemorrhage 41 6.48 0.41 34 9.55 0.34 75 7.58 0.755 Maternal conditions 30 4.74 0.30 8 2.25 0.08 38 3.84 0.386 Specific perinatal conditions 64 10.11 0.64 25 7.02 0.25 89 9.00 0.897 Hypoxic peripartum death 11 1.74 0.11 14 3.93 0.14 25 2.53 0.258 Fetal growth restriction 31 4.90 0.31 5 1.40 0.05 36 3.64 0.369 Spontaneous preterm 85 13.43 0.85 132 37.08 1.33 217 21.94 2.18
10 Unexplained antepartum death 226 35.70 2.27 0 0.00 0.00 226 22.85 2.2711 No obstetric antecedent 2 0.32 0.02 20 5.62 0.20 22 2.22 0.22
633 100 6.36 356 100 3.60 989 100 9.93
Perinatal DeathsANZACPM cause of death
Total
Stillbirths Neonatal Deaths
1 rate per 1,000 total births : n = 99,563 2 rate per 1,000 live births: n = 98,930

Queensland Maternal and Perinatal Quality Council
33
Congenital abnormality18%
Perinatal infection2%
Hypertension2%
Antepartum haemorrhage
6%
Maternal conditions5%
No obstetric antecedent0%
Unexplained antepartum death37%
Spontaneous preterm13%
Fetal growth restriction5%
Hypoxic peripartum death
2%
Specific perinatal conditions
10%
Congenital abnormality28%
Perinatal infection3%
Hypertension3%
Antepartum haemorrhage
10%
Maternal conditions2%
No obstetric antecedent6%
Spontaneous preterm36%
Fetal growth restriction1%
Hypoxic peripartum death
4%
Specific perinatal conditions
7%
The percentage of stillbirths within each ANZACPM classification is presented in Figure 13 and the percentages of neonatal deaths is presented in Figure 14. Of concern is the high percentage of stillbirths classified as ‘Unexplained antepartum death’ (37%). ‘Spontaneous preterm’ (36%) accounted for the most common cause of neonatal deaths. Figure 13. Stillbirths by ANZACPM cause of death, Queensland, 2002 and 2003
Figure 14. Neonatal mortality by ANZACPM cause of death, Queensland, 2002 and 2003

Queensland Maternal and Perinatal Quality Council
34
Table 15 shows that the most common causes of Indigenous perinatal mortality were classified as ‘Spontaneous preterm’ and ‘Unexplained antepartum’. Of note, cause of death classified as ‘Spontaneous preterm’ (rate of 5.70) was over one-and-a-half times the next highest cause of death which was classified as ‘Unexplained antepartum deaths’ (rate of 3.39). Compared with non-Indigenous mortality rates, the Indigenous mortality rates were 5.58 times higher for cause of death classified as ‘Perinatal infection’, 3.78 higher for cause of death classified as ‘Maternal conditions’, and over two-and-a-half times higher for cause of death classified as ‘Spontaneous preterm’, ‘Antepartum haemorrhage’, and ‘Hypertension’. Table 15. Perinatal mortality by ANZACPM cause of death and Indigenous status of
mother, Queensland, 2002 and 2003
n % rate1 n % rate2
1 Congenital abnormality 204 22.92 2.17 10 10.10 1.78 0.82 0.38-1.522 Perinatal infection 18 2.02 0.19 6 6.06 1.07 5.58 1.79-14.523 Hypertension 20 2.25 0.21 3 3.03 0.53 2.51 0.47-8.38
4 Antepartum haemorrhage 65 7.30 0.69 10 10.10 1.78 2.57 1.17-4.995 Maternal conditions 31 3.48 0.33 7 7.07 1.25 3.78 1.39-8.666 Specific perinatal conditions 81 9.10 0.86 8 8.08 1.43 1.65 0.68-3.38
7 Hypoxic peripartum death 25 2.81 0.27 0 0.00 0.00 0.00 0-2.638 Fetal growth restriction 33 3.71 0.35 3 3.03 0.53 1.52 0.30-4.80
9 Spontaneous preterm 185 20.79 1.97 32 32.32 5.70 2.89 1.90-4.1910 Unexplained antepartum death 207 23.26 2.20 19 19.19 3.39 1.54 0.90-2.4411 No obstetric antecedent 21 2.36 0.22 1 1.01 0.18 0.80 0.02-4.91
890 100 9.48 99 100 17.65 1.86 1.48-2.27
95% CI
Total
Relative RiskANZACPM cause of death
non-Indigenous Indigenous
1 rate per 1,000 total births: n=93,896 non-Indigenous , n=5667 Indigenous 2 risk for Indigenous vs non-Indigenous 3 Indigenous status of mother: Australian Aboriginal, Torres Strait Islander, or Australian Aboriginal and Torres
Strait Islander.
8.5.2 ANZACPM causes of perinatal mortality by birth weight and gestational age
Table 16 presents the ANZACPM causes of death by birth weight. ‘Spontaneous preterm’ accounted for the most common cause of death for birth weights of less than 1000 grams, while ‘Unexplained antepartum deaths’ accounted for the most common cause of death among birth weights of 1000 to 1499 grams. For birth weights between 1500 to 2499 grams and 2500 to 3999 grams the most common causes of death were classified as ‘Unexplained antepartum deaths’ and ‘Congenital abnormality’. Of note, caution must be used when interpreting the percentages within some of the birth weight groups due to the small number of deaths.

Queensland Maternal and Perinatal Quality Council
35
Table 16. Perinatal mortality by ANZACPM cause of death and birth weight (grams), Queensland, 2002 and 2003
Birth Weight (grams)
<1000 1000-1499 1500-2499 2500-3999 4000+ ANZACPM cause of death
n % n % n % n % n %
1 Congenital abnormality 103 19.11 16 21.92 39 30.95 53 23.87 3 10.34
2 Perinatal infection 11 2.04 0 0.00 1 0.79 11 4.95 1 3.45
3 Hypertension 11 2.04 2 2.74 9 7.14 1 0.45 0 0.00
4 Antepartum haemorrhage 49 9.09 8 10.96 10 7.94 8 3.60 0 0.00
5 Maternal conditions 17 3.15 3 4.11 4 3.17 7 3.15 7 24.14
6 Specific perinatal conditions 52 9.65 5 6.85 14 11.11 16 7.21 2 6.90
7 Hypoxic peripartum death 1 0.19 1 1.37 3 2.38 16 7.21 4 13.79
8 Fetal growth restriction 22 4.08 5 6.85 6 4.76 2 0.90 1 3.45
9 Spontaneous preterm 203 37.66 10 13.70 3 2.38 1 0.45 0 0.00
10 Unexplained antepartum death 70 12.99 23 31.51 35 27.78 90 40.54 8 27.59
11 No obstetric antecedent 0 0.00 0 0.00 2 1.59 17 7.66 3 10.34
Total 539 100.00 73 100.00 126 100.00 222 100.00 29 100.00 ‘Congenital abnormality’, ‘Spontaneous preterm’, and ‘Unexplained antepartum deaths’ accounted for the most common causes of death across the different gestational age groups (Table 17). In particular, for babies up to and including 27 weeks gestational age the most common cause of death was classified as ‘Spontaneous preterm’. In contrast, the most common cause of death for babies between 28 and 41 weeks gestational age was classified as ‘Unexplained antepartum deaths’. There were too few deaths for babies of 42 weeks and more gestational age to comment on cause of death. Of note, ‘Congenital abnormality’ was the second most commonly classified cause of death among babies less than 24 weeks gestational age.

Queensland Maternal and Perinatal Quality Council
36
Table 17. Perinatal mortality by ANZACPM cause of death and gestational age (weeks), Queensland, 2002 and 2003 Gestational Age
< 24 24 - 27 28 - 31 32 - 36 37 - 41 42+ Total ANZACPM cause of death
n % n % n % n % n % n % n % 1 Congenital abnormality 87 24.58 15 9.26 20 21.51 46 29.87 46 20.72 0 0.00 214 21.64 2 Perinatal infection 6 1.69 4 2.47 2 2.15 3 1.95 9 4.05 0 0.00 24 2.43 3 Hypertension 0 0.00 10 6.17 4 4.30 8 5.19 1 0.45 0 0.00 23 2.33 4 Antepartum haemorrhage 35 9.89 15 9.26 10 10.75 9 5.84 6 2.70 0 0.00 75 7.58 5 Maternal conditions 11 3.11 6 3.70 4 4.30 6 3.90 10 4.50 1 25.00 38 3.84 6 Specific perinatal conditions 34 9.60 20 12.35 5 5.38 14 9.09 16 7.21 0 0.00 89 9.00 7 Hypoxic peripartum death 0 0.00 1 0.62 1 1.08 3 1.95 19 8.56 1 25.00 25 2.53 8 Fetal growth restriction 5 1.41 6 3.70 9 9.68 10 6.49 6 2.70 0 0.00 36 3.64 9 Spontaneous preterm 146 41.24 61 37.65 8 8.60 2 1.30 0 0.00 0 0.00 217 21.94
10 Unexplained antepartum death 30 8.47 24 14.81 30 32.26 52 33.77 89 40.09 1 25.00 226 22.85 11 No obstetric antecedent 0 0.00 0 0.00 0 0.00 1 0.65 20 9.01 1 25.00 22 2.22 Total 354 100.00 162 100.00 93 100.00 154 100.00 222 100.00 4 100.00 989 100.00

Queensland Maternal and Perinatal Quality Council
37
Figure 15 presents the ANZACPM cause of death for stillbirths 28 weeks or more gestational age. The percentage of stillbirths 28 weeks or more gestational age classified as ‘Unexplained antepartum deaths’ (40.9%) is higher than the percentage of stillbirths at all gestational ages classified as ‘Unexplained antepartum deaths’ (22.85%) (see Figure 13). Figure 15. Stillbirths at 28 weeks or more gestational age by ANZACPM cause of death,
Queensland, 2002 and 2003.
Antepartum haemorrhage
7.0%
Specific perinatal
conditions10.3%
Maternal conditions
5.1%
Hypoxic peripartum death
2.3%Fetal growth restriction
5.1%
Spontaneous preterm10.1%
Unexplained antepartum
death40.9%
Hypertension2.3%
Perinatal infection
2.1%
Congenital abnormality
14.6%
No obstetric antecedent
0.4%

Queensland Maternal and Perinatal Quality Council
38
8.6 ANZNDC causes of neonatal mortality The main causes of death using the Australian and New Zealand Neonatal Death Classification (ANZNDC) system are presented in Table 18 by Indigenous status of mother. As seen in the Table, the Indigenous neonatal mortality rate was over three times the non-Indigenous neonatal mortality rate for deaths classified as ‘Extreme Prematurity’ and ‘Infection’. Table 18. Neonatal mortality by ANZNDC cause of death and Indigenous status of mother,
Queensland, 2002 and 2003 Relative
n rate2 n rate3 Risk4 95% CI1 Congenital abnormality 91 0.97 7 1.24 1.27 0.50-2.732 Extreme Prematurity 93 0.99 18 3.18 3.21 1.82-5.353 Cardio-Respiratory disorders 52 0.55 5 0.88 1.59 0.50-3.964 Infection 29 0.31 6 1.06 3.43 1.16-8.405 Neurological 26 0.28 2 0.35 1.27 0.15-5.096 Gastrointestinal 8 0.09 2 0.35 4.14 0.43-20.767 Other 16 0.17 1 0.18 1.04 0.02-6.67
315 3.35 41 7.23 2.16 1.52-2.99
ANZNDC cause of death
Total
Non-Indigenous Indigenous1
1 Indigenous status of mother: Australian Aboriginal, Torres Strait Islander, or Australian Aboriginal and Torres
Strait Islander 2 Rate per 1000 live births, N=93,896 3 Rate per 1000 live births, N=5,667 4 Relative risk: Indigenous vs non-Indigenous When examining the percentages of deaths classified by the ANZNDC causes of death by birth weight, caution must be used due to the small number of deaths within some of the birth weight groups (Table 19). Among babies weighing less than 1000 grams, the most common cause of death was classified as ‘Extreme prematurity’. Of these deaths, 82.4% were not resuscitated. ‘Congenital abnormality’ accounted for the most common cause of death among babies weighing greater than 1000 grams. Table 19. Neonatal mortality by ANZNDC cause of death and birth weight (grams),
Queensland, 2002 and 2003
n % n % n % n % n %1 Congenital abnormality 11 5.64 8 32.00 29 65.91 49 58.33 1 12.502 Extreme Prematurity 108 55.38 0 0.00 2 4.55 0 0.00 1 12.50
(not resuscitated) (89) (45.64) 0 (0) (0) 0 (0) (0) (1) (12.50) (unsuccessful resuscitation) (19) (9.76) 0 (0) (2) (4.55) (0) (0) (0) 0
3 Cardio-Respiratory disorders 44 22.56 6 24.00 2 4.55 4 4.76 1 12.504 Infection 19 9.74 4 16.00 1 2.27 10 11.90 1 12.505 Neurological 4 2.05 4 16.00 6 13.64 12 14.29 2 25.006 Gastrointestinal 6 3.08 2 8.00 2 4.55 0 0.00 0 0.007 Other 3 1.54 1 4.00 2 4.55 9 10.71 2 25.00
195 100.00 25 100.00 44 100.00 84 100.00 8 100.00Total
Birth Weight (grams)
ANZNDC cause of death<1000 1000-1499 1500-2499 2500-3999 4000+
Table 20 presents the percentages of deaths classified by the ANZNDC causes of death by gestational age (in weeks). For babies less than 24 weeks gestational age, the most common cause of death was classified as ‘Extreme Prematurity’. Of these babies, 91.30% were not resuscitated. For babies 24 to 27 weeks gestational age, the most common cause of death was classified as ‘Cardio-Respiratory disorders’. ‘Congenital abnormality’ accounted for the most common cause of death among babies 28 to 41 weeks gestational age.

Queensland Maternal and Perinatal Quality Council
39
Table 20. Neonatal mortality by ANZNDC cause of death and gestational age (weeks), Queensland, 2002 and 2003
n % n % n % n % n % n %1 Congenital abnormality 6 5.61 5 5.38 11 39.29 32 68.09 44 55.00 0 0.002 Extreme Prematurity 92 85.98 16 17.20 2 7.14 1 2.13 0 0.00 0 0.00
(not resuscitated) (84) (78.51) (6) (6.52) (0) (0) (1) (2.13) (0) (0) (0) (0) (unsuccessful resuscitation) (8) (7.47) (10) (10.68) (2) (7.14) (0) (0) (0) (0) (0) (0)
3 Cardio-Respiratory disorders 5 4.67 41 44.09 5 17.86 1 2.13 5 6.25 0 0.004 Infection 3 2.80 16 17.20 5 17.86 3 6.38 8 10.00 0 0.005 Neurological 0 0.00 7 7.53 2 7.14 6 12.77 13 16.25 0 0.006 Gastrointestinal 0 0.00 6 6.45 2 7.14 2 4.26 0 0.00 0 0.007 Other 1 0.93 2 2.15 1 3.57 2 4.26 10 12.50 1 100.00
107 100.00 93 100.00 28 100.00 47 100.00 80 100.00 1 100.00
32-36 37-41 42+
Total
24-27 28-31ANZNDC cause of death < 24Gestational Age (weeks)

Queensland Maternal and Perinatal Quality Council
40
10
20
30
40
50
1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
Per
cent
Stillbirths Neonatal Deaths
8.7 Perinatal autopsy The percentage of autopsies performed on stillbirths and on neonatal deaths from 1995 to 2003 is presented in Figure 16. Of concern is the decrease in the rate of autopsies being performed for both stillbirths and neonatal deaths. Autopsies have been performed on less than 30% of stillbirths since 2002 and on less than 30% of neonatal deaths since 2000. Figure 16. Rates of perinatal autopsy, Queensland, 1995 to 2003 Table 21 presents the number of perinatal deaths classified by ANZACPM cause of death and the rate for which autopsies were performed within each ANZACPM cause of death. Overall, autopsies have been performed for only 23% of all perinatal deaths: 26.9% of stillbirths and 16% of neonatal deaths. These percentages are even lower when examining the percentages of autopsies performed within a classification of cause of death. Of note, autopsies were performed for over 60% of stillbirths classified as ‘Hypoxic peripartum deaths’ (7/11) and for 60% of neonatal deaths classified as ‘No obstetric antecedent’ (12/20). Of particular concern is the low stillbirth autopsy rate of 38.50 for deaths classified as ‘Unexplained antepartum death’. Table 21. Perinatal autopsy by ANZACPM cause of death, Queensland, 2002 and 2003
n rate2 n rate2 n rate2
1 Congenital abnormality 116 23 19.83 98 18 18.37 214 41 19.162 Perinatal infection 14 4 28.57 10 2 20.00 24 6 25.003 Hypertension 13 1 7.69 10 1 10.00 23 2 8.704 Antepartum haemorrhage 41 6 14.63 34 2 5.88 75 8 10.675 Maternal conditions 30 4 13.33 8 1 12.50 38 5 13.166 Specific perinatal conditions 64 14 21.88 25 3 12.00 89 17 19.107 Hypoxic peripartum death 11 7 63.64 14 5 35.71 25 12 48.008 Fetal growth restriction 31 12 38.71 5 1 20.00 36 13 36.119 Spontaneous preterm 85 12 14.12 132 12 9.09 217 24 11.06
10 Unexplained antepartum death 226 87 38.50 0 0 NA 226 87 38.5011 No obstetric antecedent 2 0 0.00 20 12 60.00 22 12 54.55
633 170 26.86 356 57 16.01 989 227 22.95Total
Perinatal DeathsWith autopsy With autopsy With autopsy
N1N1N1ANZACPM cause of death
Stillbirths Neonatal Deaths
1 total number of deaths by ANZACPM cause of death 2 rate per 100 deaths within the ANZACPM cause of death

Queensland Maternal and Perinatal Quality Council
41
9. Perinatal morbidity 9.1 Australian and New Zealand Neonatal Network (ANZNN) The ANZNN provides information on babies treated in Level III neonatal intensive care units (NICUs) in Australia and New Zealand. In Queensland there are three NICUs: The Townsville Hospital, The Royal Brisbane and Women’s Hospital and the Mater Mothers’ Hospital. Babies registered are those who are admitted to a Level III NICU at less than 28 days (during their first admission) who meet the following criteria: ♦ are <32 completed weeks gestation, OR ♦ are <1500 grams birth weight, OR ♦ receive assisted ventilation including continuous positive airway pressure (CPAP) for
four or more hours, OR ♦ undergo major surgery. In 2002, 7045 babies were registered across the ANZNN which is somewhat greater than the number of babies registered in 2001 (6805). There were slightly more male babies registered in Queensland than female babies, which is comparable across other states and New Zealand. Approximately half of the registered babies in Queensland were born at 32-43 weeks gestation, with a modal gestational age of 31 weeks. This pattern was similar to Australian registered babies. The distribution of birth weight for Queensland registered babies showed a modal weight of 1500-1999 grams, which was similar to Australian registered babies.
9.1.1 ANZNN clinical indicators
Information was obtained for five clinical indicators: cranial ultrasound, eye examination, chronic lung disease, use of exogenous surfactant for hyaline membrane disease (HMD) and acquired infection. Table 23 presents the clinical indicator, the indicator’s comparison population and the specific indicator associated with the clinical area. The expected rate of presentation for the specific indicator and the overall rate from the ANZNN data are provided in the Table to enable a comparison with the observed rate for Queensland Queensland indicator rates for each of the three cranial ultrasound indicators and the two eye examination indicators are better than the expected rates (Table 23). In comparison to the ANZNN rates, the Queensland rates are slightly better. Queensland indicator rates for the chronic lung disease indicator and the exogenous surfactant for HMD are equal to the expected rate and better than the ANZNN rate.

Queensland Maternal and Perinatal Quality Council
42
Table 22. ANZNN clinical indicators, Queensland and ANZNN, 2002
Clinical Area Population Specific IndicatorExpected
Rate Qld Rate ANZNNa
Cranial Ultrasound (CU)
Babies born at < 31 weeks gestation or < 1250 grams birth weight and survive to day 3
Proportion of babies having at least one CU in first 10 days and survive to day 3
>95% 97% 97.00%
Proportion of babies with an intraventricular haemorrhage (IVH) of any grade
<45% 28% 27.10%
Proportion of babies with a Grade 3 or 4 IVH <10% 7.10% 6.30%
Eye examinations
Babies born at < 30 weeks gestation or < 1250 grams birth weight and survive to 36 weeks post menstrual age
Proportion of babies with at least one eye examination >90% 95% 87%
Proportion of babies with Stage 3 or 4 retinopathy of prematurity <8% 5.10% 7.30%
Chronic lung disease at 36 weeks gestation
Babies born at <32 weeks gestation and survive to 36 weeks post menstrual age
Proportion of babies having supplemental oxygen or respiratory support for their initial respiratory disease at 36 weeks post menstrual age
<20% 20% 23.50%
Exogenous surfactant for hyaline membrane disease (HMD)
Babies of any gestation with endotracheal ventilation for four or more hours for hyaline membrane disease
Proportion of use of at least one dose of exogenous surfactant
>90% 90% 87%
Late-onset septicaemia
Babies who survive to day 2 Proportion of babies with
late-onset septicaemia born at <28 weeks gestation or <1000 grams birth weight
<50% 31.65% 23.89%
Proportion of babies with late-onset septicaemia born at >27 weeks gestation of >999 grams birth weight
<10% 3.17% 5.97%
aExcludes Queensland data.

Queensland Maternal and Perinatal Quality Council
43
9.2 Congenital anomalies sub-committee Purpose This sub-committee was established in 2004 to provide advice and make recommendations to the Quality Councils on matters related to the incidence of birth anomalies in Queensland. Structure • The sub-committee has been established under the auspices of the Queensland
Maternal and Perinatal Quality Council (QMPQC). • Establishment of the sub-committee has been authorised by the Chief Health Officer. • Members of the sub-committee are bound by the quality assurance and confidentiality
provisions of the Health Services Act 1991. • Sub-committee membership is limited to the minimum number of participants to achieve
the required expertise and achieve the objectives of the sub-committee. Meetings/activities/reporting • The sub-committee meets 2-3 weeks before Council meetings. • All activities of the sub-committee must be endorsed by the QMPQC. • The sub-committee may function without the support of the secretariat and the sub-
committee chairman is responsible for recording and reporting activity. • The work of the sub-committee is to be included in the annual Council report. Objectives
1. Using routinely collected data, monitor the incidence of birth anomalies in Queensland.
2. Provide advice, through the Quality Councils, on data collection methodologies and strategies to improve reporting.
3. Analyse, interpret and assess the burden of birth anomalies in Queensland.
4. Provide advice, through the Quality Councils, on measures to reduce the incidence of preventable birth anomalies.
5. Investigate changes in the frequency of specific birth anomalies which may point to a possible cause.
6. Provide health professionals and the public with information about birth anomalies in Queensland.
7. Provide advice, through the Quality Councils, to assist in the development of policies and subsequent planning and delivery of health services for those with birth anomalies.
8. Monitor and evaluate the effectiveness of public health measures to reduce the incidence of birth anomalies.
9. Provide local statistics to assist health professionals counsel families about the chances of having a child with a birth anomaly.
10. Encourage screening and ante-natal detection of birth anomalies to assist with planning healthcare facilities.
11. To advocate for the development of an accurate database encompassing the entire spectrum of birth anomalies, including those terminated at <20 weeks gestation.
12. To assist the Health Information Services and the Perinatal Data Collection Unit with activities including driving analyses, providing clinical advice and informing change.

Queensland Maternal and Perinatal Quality Council
44
9.3 Early onset group B streptococcal disease (EOGBSD) An audit project is currently being undertaken of EOGBSD in Queensland. This aims to identify the rate of this condition, and examine factors related to the ‘Clinical Practice Guidelines for Prevention of Neonatal Early Onset Group B Streptococcal Disease’, to determine the adherence to these guidelines and to ascertain their usefulness or need for any revised recommendations. The audit will be both retrospective and prospective, with case ascertainment being from both public and private pathology laboratories. Staff in Queensland hospitals are urged to assist in this audit process by providing clinical data when requested.

Queensland Maternal and Perinatal Quality Council
45
10. Quality indicators
10.1 Quality indicators sub-committee This sub-committee, following the direction of the Chief Health Officer, has been established to broaden the Council’s role to greater than that of a mortality audit or sentinel event group. That is, the Council wishes to take a bigger role in the examination of Quality and Safety indicators in maternal and perinatal services in Queensland. It is important that this is done within a national framework and within the pragmatic confines of realistic reliable data collection. The frameworks being developed by the Core Maternity Indicated Project funded through the Australian Council for Safety and Quality in Health Care are critical to the work of this sub-committee and Council. It may be that a major role of this sub-committee initially is to work with other national or state groups which are developing similar reforms and quality measures. One of the sub-committee’s functions is to examine existing national and other state initiatives in this area and work with national and state groups to achieve a set of quality indicators for use in Queensland. The sub-committee draws on policy guidelines from organisations including the Australian Council on Healthcare Standards (ACHS), Australian Council for Safety and Quality in Health Care (ACSQHC), Perinatal Society of Australia and New Zealand (PSANZ), Women’s and Children’s Hospitals Australasia (WCHA), Department of Human Services Victoria, Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG), Australian College of Midwives (ACMI) and the National Perinatal Statistics Unit. The major challenge for this sub-committee and similar groups nationally is agreeing on a set of national indicators that are measurable in all jurisdictions. In addition to standard collection of data on indicators such as caesarean section rates, induction of labour rates and vaginal birth after caesarean section rates, up to 20 other possible indicators have been suggested or are collected variably by some organisations and some states. These include indicators such as term infants transferred or admitted to NNU or SCU for reasons other than birth defect, rate of administration of antenatal corticosteroids before 34 weeks, proportion of women offered interventions to stop smoking and neonatal surfactant use rates. 10.2 Future directions The sub-committee has undertaken two tasks for 2006:
a) Support the work of the Maternity Collaboration Quality Indicator Project in the establishment of core national indicators.
b) Collate data and analyse these three areas (where Queensland has reliable data): • 3rd and 4th degree perineal trauma • outcomes for standard primiparous women • SCC and NNU admission rate for other than congenital anomalies following
elective CS The sub-committee also agreed that it recommend research for other quality indicators such as breastfeeding rates at three and six months, referral rates to home visit programs and the rate of use of hand held records.