6.Buhling and Davids Patofis
13
Summary Hyperemesis gravidarum is a multifactorial illness that f re q u e ntly deve lops pre g n a n c y . I t is import a nt t h at p at i e nt s undergo multimodal therapy, taking approaches into con - sideration, after diverse underlying illnesses has been the thyroid gland . Patient counse ling should take place in a setting that is suited ps ychoso cial aspects o f the illness. This article also deals with the results of aims to provide physicians with an evidence-based step-by-step guide. Introduction Almost all p regnant women report experiencing char acte- ristic attacks of nausea during the first trimester of preg- nancy. Although this nausea is characteristically described as “morning sicknes s” , these nauseous attacks are restrict- ed tothe morning hours in just 17 % of all p regnant women (Ismail and Kenny 200 7); in most pregnant women,attacks can occur throu g hou t the day. Gene ra ll y, naus ea and vo m i t - ing in (early) pr egnancy are mild and self-limiting, usually ending be fore the 14 th week of pregnancy (Sheehan 2007). In 1-3 % of the patien ts affec ted, sympto ms are so se vere that hyperemesis gravida rum is diagnosed. However , data on the frequency of such attacks also depend on the diag- nostic criteria used to define hyperemesis gravidarum (HG) (Eliakim et al. 2000; ACOG 20 04).The followin g factors a re usually used f or defining the illness: unrelievable vomiting where there is no ot her cause , the inabili ty to take in f ood, the presence of catabolic metabolism (severe ketonuria), loss of weight and severely impaired general well-being. When a patient with HG presents with such criteria, she is normall y admitte d to hos pital, as outp atient treatmen t is no longer possible due to the subjectively and objectively gre atly we a kened nutrit ional and ge n eral co n dit i on . H y pe r- emesis is ther efore not only one of the most frequen t indi- cation s for hospita l admittance during the first trimester of pregn ancy , but is by all means , a major c ost factor in the German h ealth sy stem. In 2005,for example, 17 574 p reg- nant women were admitted to hospital with this diagnosis (Information System of Federal Health Monitoring, 2007). The yearly cost of hospital admittances alone w as about 28 million euros per year, based on an average cost of 1 590 euros per case (300 euros per day , for 5.3 days).The cost of lo st working hours and outpa tient treatmen t is n ot even incl uded in this amount. Apart from these econo mic aspects, a specific medical problem should be pointed out: m o r ta lities due to HG are rare , unlike dur ing the period prior to the introd uction of intr avenous ther apy , (in the UK, in the “pre-infus ion era” the mortality rate of women w ith HG was 1. 6 women p er 10000 births; Ve rberg et al. 2005). However,a curren t study of US American coh orts showed that hyperemesis patients with a weight -increase of less than 7 kg during pregnancy run an increased risk of a range of unfavo rable obstetric constellations (Dodds et al.2006) (T ab.1). Table 1: Perinatal out come p aramet ers for hy p eremesi s patients with a we i g ht increase o f less than 7 kg du ring pregna ncy (a cco rding to Dodd s e t a l . 2 0 0 6 ) Etiology and Pathogenesis Etiology , pathogene sis, and to a certa in extent the resu lt- ing ther apeu tic mana gement of HG, are the subject of a debate that has continued for decades,in which very con - flicting views are e xpressed on the causes of the illness (Soltan i and T aylor 2003 ). It is interes ting that until the middle of the 1 9 th century“excessive or unrelievable vomi- ting”was largely unknown in the field obstetrics (Meyer 1914).Today , it is repe atedly emp hasize d that the symp- toms of HG are on ly observed in humans,almost exclu- sively in pregnant women who live in W estern societies (Simpson et al. 2001).The illness is more frequen tly found in female immigr ants (David et al. 2002) in comparison with native inhabitants.There are various theories on the pathogen esis of HG (Fig. 1). Bühling K . J. Nausea... Gynakol Geburtsmed Gynakol Endokrinol 2008;4(1):36–48 publiziert 31.03.08 www .akademos.de/gyn © akademos Wissenschaftsverlag 2008 ISSN 1614-8533 Nausea and Hyperemesis Gravidarum Kai J. Bühling 1,2 ,Matthias David 3 1 Hormone C onsultation,Department of Gynec ology,University Medical Center Hamburg-E ppendorf 2 Practice for Gynecology,Endocrinology and Reproductive Medicine, Hamburg 3 Charité – Medica l Center Berlin,Department of Gynecology and Obstetrics,Berlin Reviewe r: Dolores Foth,Köln and Pete r Rott, Berlin Perinatal Outcome Parameter 5-minute Apgar score< 7 Premature birth < 37/0 SSW Birth weight< 2500 g Gestational diabetes Induced delivery Delivery by cesarean section Relative Risk 5,0 3,0 2,8 1,4 1,4 1,4 D o w n l o a d e d f r o m c m e . a k a d e m o s . d e o n T u e s d a y , N o v e m b e r 1 9 , 2 0 1 3 D o w n l o a d e d f r o m c m e . a k a d e m o s . d e o n T u e s d a y , N o v e m b e r 1 9 , 2 0 1 3 C o p y r i g h t © 2 0 1 3 a k a d e m o s W i s s e n s c h a f t s v e r l a g . A l l r i g h t s r e s e r v e d C o p y r i g h t © 2 0 1 3 a k a d e m o s W i s s e n s c h a f t s v e r l a g . A l l r i g h t s r e s e r v e d
-
Upload
truly-graceva -
Category
Documents
-
view
224 -
download
0
Transcript of 6.Buhling and Davids Patofis

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 1/13
Summary
Hyperemesis gravidarum is a multifactorial illness thatf re q u e ntly develops pre g n a n c y. I t is import a nt t h at p at i e nt sundergo multimodal therapy,taking approaches into con-sideration, after diverse underlying illnesses has been thethyroid gland. Patient counseling should take place in asetting that is suited psychosocial aspects of the illness.This article also deals with the results of aims to providephysicians with an evidence-based step-by-step guide.
Introduction
Almost all pregnant women report experiencing characte-ristic attacks of nausea during the first trimester of preg-nancy.Although this nausea is characteristically describedas “morning sickness”, these nauseous attacks are restrict-ed to the morning hours in just 17 % of all pregnant women
(Ismail and Kenny 2007); in most pregnant women,attackscan occur t h ro u g h o u t the day. G e n e ra l l y, nausea and vo m i t-ing in (early) pregnancy are mild and self-limiting, usuallyending before the 14th week of pregnancy (Sheehan 2007).In 1-3% of the patients affected, symptoms are so severethat hyperemesis gravidarum is diagnosed.However, dataon the frequency of such attacks also depend on the diag-nostic criteria used to define hyperemesis gravidarum (HG)(Eliakim et al. 2000;ACOG 2004).The following factors areusually used for defining the illness: unrelievable vomitingwhere there is no other cause, the inability to take in food,the presence of catabolic metabolism (severe ketonuria),
loss of weight and severely impaired general well-being.When a patient with HG presents with such criteria,she isnormally admitted to hospital,as outpatient treatment isno longer possible due to the subjectively and objectivelyg re atly we a kened nutritional and ge n e ral co n d i t i o n . H y p e r-emesis is therefore not only one of the most frequent indi-cations for hospital admittance during the first trimesterof pregnancy, but is by all means, a major cost factor in theGerman health system. In 2005,for example,17574 preg-nant women were admitted to hospital with this diagnosis(Information System of Federal Health Monitoring, 2007).The yearly cost of hospital admittances alone was about28 million euros per year,based on an average cost of
1 590 euros per case (300 euros per day, for 5.3 days).Thecost of lost working hours and outpatient treatment is noteven included in this amount. Apart from these economicaspects, a specific medical problem should be pointed out:m o rtalities due to HG are ra re , u n l i ke during the period priorto the introduction of intravenous therapy, (in the UK, inthe “pre-infusion era”the mortality rate of women with HG
was 1.6 women per 10000 births;Verberg et al. 2005).However,a current study of US American cohorts showedthat hyperemesis patients with a weight-increase of lessthan 7 kg during pregnancy run an increased risk of a rangeof unfavorable obstetric constellations (Dodds et al. 2006)(Tab.1).
Table 1: Pe r i n atal outcome parameters for hy p e remesis pat i e nts with
a we i g ht i n c rease of less than 7 kg during pregnancy (a cco rding to
Dodds et a l . 2 0 0 6 )
Etiology and Pathogenesis
Etiology, pathogenesis,and to a certain extent the result-
ing therapeutic management of HG,are the subject of adebate that has continued for decades, in which very con-flicting views are expressed on the causes of the illness(Soltani and Taylor 2003). It is interesting that until themiddle of the 19th century“excessive or unrelievable vomi-ting”was largely unknown in the field obstetrics (Meyer1914).Today, it is repeatedly emphasized that the symp-toms of HG are only observed in humans,almost exclu-sively in pregnant women who live in Western societies(Simpson et al. 2001).The illness is more frequently foundin female immigrants (David et al. 2002) in comparisonwith native inhabitants.There are various theories on the
pathogenesis of HG (Fig. 1).
Bühling K. J. Nausea... Gynakol Geburtsmed Gynakol Endokrinol 2008;4(1):36–48 publiziert 31.03.08 www.akademos.de/gyn © akademos Wissenschaftsverlag 2008 ISSN 1614-8533
Nausea and HyperemesisGravidarum
Kai J. Bühling1,2,Matthias David3
1 Hormone Consultation,Department of Gynecology,University
Medical Center Hamburg-Eppendorf 2 Practice for Gynecology,Endocrinology and Reproductive Medicine,
Hamburg3 Charité – Medical Center Berlin,Department of Gynecology and
Obstetrics,Berlin
Reviewer: Dolores Foth,Kölnand Peter Rott, Berlin
Perinatal Outcome Parameter
5-minute Apgar score <7
Premature birth <37/0 SSW
Birth weight <2500 g
Gestational diabetes
Induced delivery
Delivery by cesarean section
Relative Risk
5,0
3,0
2,8
1,4
1,4
1,4

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 2/13
Figure 1:Pathogenetic mechanisms involved in the development of
nausea/hyperemesis gravidarum (modified according to Verberg et
al.2005)
Currently, the most-favored explanation of the causes of HG is the so-called “hormone theory”– many studies haveshown a connection between raised HCG values and the
occurrence of pathological vomiting. Numerous othersomatic causes are also under discussion, but they havenot been confirmed by any studies (Verberg et al. 2005).A study providing an overview of the 15 prospective studiespublished between 1990 und 2005 that examined therelationship between HCG and hyperemesis, summarizesthe results. Significantly raised HCG values were found(Verberg et al. 2005) in 11 studies.This suggests that HCGpossibly causes hyperemesis gravidarum via a stimulatoryeffect on the secretory processes of the gastrointestinaltract,or, as HCG is structurally similar to TSH (both!-armsare identical), the TSH receptor is stimulated (Ismail andKenny 2007).
In early pregnancy, the physiological stimulation of thethyroid gland sometimes leads to a transient “gestationalthyreotoxicosis”.This occurs about twice or three times
more frequently in women with hyperemesis gravidarum(Goodwin 1992). Eleven of the 15 prospective studies thatcompared the T4 values of hyperemesis patients withasymptomatic pregnant women found significantly in-creased values in the women with hyperemesis,and thiswas also the case with regard to TSH values (Verberg etal.2005).
A current publication evaluated all studies carried out be-tween 1966 and 2007 on the subject of“HG and helicobac-
ter pylori infection”.Ten of these 14 case-control studiesfound a significant relationship between HG and helico-
bacter pylori infection.The odds-ratio ranged from 0.55 to
Ovar/corpus luteum
Placenta
Hypothalamus/
adrenal cortex
Thyroid gland
Cortisol/ACTH
TSH/thyroxine
Hypothesis I on the patho-
genesis of HG: endocrine
factors cause HG
Hypothesis II on the
pathogenesis of HG:
nonendocrine factors
cause HG
Estrogen/progesterone
Prolactin
Leptin
overactive immunesystem
H.pylori infection
overactive hypothala-mic-pituitary-adrenal
axis
pregnancy-induced
transitory thyretoxi-
cosis
alterations in the
gastrointestinal tract
vitamin deficit/traceelement deficit
raised liver enzymes
psychological causes
gastrointestinal tract
immunologic causes
infectious causes
anatomic causes
»nerval causes«
HCG

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 3/13
Diagnostics
The definition of HG is not clear-cut.Severe nausea andvomiting,and electrolyte metabolism,are typical charac-teristics,as well as digestion,which result in a physicallyweakened condition and psychological ultimately a diag-nosis of exclusion, i.e. before a patient is diagnosed re-commended, numerous differential diagnostics must be
considered, gastrointestinal,metabolic,and neurologicalcauses (Tab. 2).
Table 2: Hyperemesis gravidarum – differential diagnostics
(according to Ismail and Kenny 2007)
Some laborato ry para m e t e r s, in particular the hemato c r i tva l u e s, e l e ct ro l yt e s, t ra n s a m i n a s e s, b i l i r u b i n ,and above all,TSH and free t hy roid hormones, p l ay a significant role ind i a g n o s i s .With re ga rd to HG, sys t e m atic endocrine diag-nostics are carried out, depending on the severity of t h esy m p to m s .P re g ravida parameters should be co n s u l t e d , i f on hand. In cases with no previous findings,basic labora-to ry diagnostics should be performed at l e a s t o n ce. As func-tional diagnostics, the TSH (TSH may be phys i o l o g i c a l l y
s u p p ressed by the cross re a ction of HCG in the first t r i m e s-t e r,b u t p ro n o u n ced suppression may also be an indicat i o nof malfunct i o n ) , f T 3, and fT4 values should be determined.Free t hy roid hormones dire ctly re f l e ctthe endocrine func-tion of the t hy roid gland, while TSH values provide info r m a-tion on the re q u i red degree of t hy roid gland stimulat i o n .With a co n s t e l l ation of suppressed TSH (due to a cross re a c-tion with HCG) and normal fT3/fT4 va l u e s, no further t re at-m e nt is nece s s a ry.If findings are abnormal, the t hy roid an-tibody TPO-Ab and the TS H - re ce p to r-Ab in part i c u l a r,s h o u l dbe determined. The benefits of t hy re o s t atic t re at m e nt of l at e nt hy p e rt hy reosis (suppressed TS H , fT3 incre a s e d ; fT4in the upper ra n ge) must be co n s i d e red in each individual
109.33 and only three times was it under 1,which is the sig-n i f i c a n cera n ge.The authors t h e re fo re concluded t h at t h e s every heterogenous results were,overall, only of limited sig-n i f i c a n ce(G o l b e rg et a l . 2 0 0 7 ) . As biological-somat i c appro-aches were not able to supply any satisfactory explanation,or because it was not possible to identify the underlyingpathophysiological mechanism of HG,the original psycho-
genetic model (based on psychoanalytic theory) foundmany supporters (Munch 2002).The postulated psycholo-gical causes of HG can be divided into four main categories(Verberg et al.2005):1. HG is an expression of conflicts, such as rejection of
the pregnancy, conflict caused by ambivalence towardsmotherhood, or of an immature personality, strongdependency on the mother,fear of pregnancy,
2. HG is an expression of sexual dysfunction(s),3. HG is a conversion symptom,an expression of a hyste-
rical,neurotic,or depressive dysfunction,4. HG results from psychosocial stress,experienced
violence,and/or conflict in the relationship with thepartner.
The fact that the incidence of HG is usually low during warand postwar periods has been t a ken as pro of of the psyc h o-genesis of this complaint. It should,however,be taken intoconsideration that during periods of adversity and hungerother problems are much more strainful than morningsickness, and therefore the symptoms of HG are possiblypaid less attention at such times.
Apart from the psychoanalysis-based conversion dysfunc-tion,Buckwalter and Simpson (2002) particularly empha-
size“stress factors”such as fear, lack of information onpregnancy,bad communication,amongst others,as possi-ble triggers of increased nausea or HG.Studies on the sub-
ject have produced various results; some studies confirmedthe connection between social factors and increased vo-miting and others could establish no connection.It woulddefinitely appear that the relationship between the part-ners plays a very important role in the woman’s ability todeal with the negative physical and psychological effectsof stress.
Finally,HG can be an expression of an immature coping
mechanism.Vomiting could be an adopted unconsciousmethod of evading situations that are difficult to tolerateor that are stressful (Buckwalter and Simpson 2002).
According to current knowledge,HG is a classical exampleof the interaction of biological-somatic,psychological,andsocial factors.
Bühling K. J. Nausea... Gynakol Geburtsmed Gynakol Endokrinol 2008;4(1):36–48 publiziert 31.03.08 www.akademos.de/gyn © akademos Wissenschaftsverlag 2008 ISSN 1614-8533
Gastrointestinal illnesses
Endocrine dysfunctions
Drug-induced vomiting
Neurovestibular dysfunction
Psychiatric illnesses
gastritis
reflux esophagitis
intestinal infections
peptic ulcer
(sub-) ileus
hepatitis
diabetes
hyperthyroidism
Addison’s disease
hypercalcemia
antibiotics
iron substitution
other drugs

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 4/13
Figure 2: Algorithm on an evidence-based five-step regimen for
nausea and (hyper-)emesis gravidarum.
Conservative Treatment Strategies
Acupuncture
In various studies, a c u p u n ct u re or acupre s s u re at the P6p o i nt (“inner gate”) improved sy m p to m s . Bands we realso used to apply pressure (Roscoe 2002),achieving goodresults. These acupre s s u re bands are little known in Ger-m a ny,b u t t h ey proved ve ry effe ct i ve in some ra n d o m , p l a-ce b o -co nt rolled studies, t h at is to say, the sy m p toms we rea l l ev i ated significantly (e. g. www. a ku p re s s u r- b a n d . d e ) .Pat i e nts t h e m s e l ves should also at t e m p t to apply acupre s-s u re to P6 eve ry four hours (see Fi g. 3 ) ; in a ra n d o m i ze d ,p l a ce b o -co nt rolled study, this also bro u g ht good re s u l t s( Ro s coe 2002).The significance of acupre s s u re and acu-p u n ct u re in t re at m e nt of HG is, h oweve r,co nt rove r s i a l .
This is shown by the ve ry va rying results of the studies onh a n d . One study by Knight and cowo r kers showed t h at“ real acupunct u re is” n o t m o re effe ct i ve than “mock acu-p u n ct u re ”( w i t h o u t p u n cturing the skin) (Knight 2 0 0 1 ) .T h e re is t h e re fo re no pro of t h at this type of t re at m e nt i sm o re effe ct i ve than mock- a c u p re s s u re or acupunct u re ,a l t e rations in eating habits, or counseling on changes inl i fe style (J ewell and Young 2006).
3
Step 1
Exclusion of a manifest dysfunction o f the thyroid gland by clinical
and laboratory tests, evaluation of psychosomatic components, and
if necessary, suggestions on possibilities of improving the situation
Step 2
Alteration o f daily habits: nutritional adjustment, smaller meals,taking the first meal (crisp bread, for instance) in the morning
before getting up; acupressure if required (manual or with an
acupressure band)
Step 3
Ginger tea, raw ginger, ginger capsules (e.g . Zintona® 4 x1 capsule)
Step 4
Vitamin B6, 10 mg 3 x daily (e.g . 3 x1 tab. Nausan®)
Step 5
Meclozine (12.5 mg max. 4x daily), metoclopramide
(10 mg max. 4x daily or promethazine (12.5 mg max. 4x daily)
c a s e ; h oweve r, the benefits of t hy re o s t atic t re at m e nt a p-pear to be slight in comparison with the risks. In pro-nounced sy m p to m atic hy p e rt hy reosis during pre g n a n c y,which can be diffe re nt i ated from M. B a s e d ow(ra re duringp regnancy) by determining the t hy re o t ropine re ce p to ra u to a ntibody (TRA K ) , l ow-dose t hy re o s t atic t re at m e ntshould be co m m e n ced (2.5-5.0 mg t h i a m a zol or 50-100 mg
p ro py l t h i o u racil [PTU]) (Bohnet, 1 9 9 5 ) . I t should alays bere m e m b e red t h at H CG is slightly physiologically raised inmultiple pre g n a n c i e s, which is why HG is more fre q u e nt i nsuch cases (Grun et a l . 1 9 97 ) . In order to assess the seve r i t yof the illness, and as a criterion for hospital admittance ,i tis import a nt to determine the ke tone bodies in the urine.During initial exa m i n ation or on admittance , u l t ra s o u n dshould always be performed on HG pat i e nts (e. g. to deter-mine int a ct g rav i d i t y,multiple birt h , p l a ce nta struct u re , o rto exclude a hyd at i d i form mole).
The physician should discuss the psychosocial co m p o n e nt swith the pat i e ntin an appro p r i ate manner; for exa m p l e ,the re l ationship with the partner (the part n e r ’s re a ction tothe pre g n a n c y,the part n e r ’s re a ction to HG), the social cir-c u m s t a n ces (pre s s u re due to other children or members of the fa m i l y, the living co n d i t i o n s, and the work situat i o n ) ,the possibility, and the need of help. These topics are , h ow-eve r,n o t usually subjects for discussion during the initialmeeting (in an acute situat i o n , for instance , or on admit-t a n ce to the clinic) but should be approached during t h es e cond or t h i rd meeting.
Treatment
Pat i e nts with nausea gravidarum or less seve re cases of hy p e remesis gravidarum can be t re ated as outpat i e nt s .An exa ct anamnesis should first be carried out when nau-s e a/HG deve l o p s . Eating early in the morning often leadsto improve m e ntif the illness is strictly “morning sickness”.Lo n ger periods of fasting should be avoided (Newman eta l . 1 9 9 3 ) , as well as possible t r i gger fa ctors (odors, fo o d s)(Bühling and Bohnet 2 0 0 6 ) .Water and elect ro l yte metabo-lisms t h at a re still balance d ,good co m p l i a n ce of the pre g-n a nt wo m a n ,and the possibility of psyc h o s o m at i c - o r i e nt e dbasic care are pre conditions for t re ating pat i e nts with re g-ular vomiting as outpat i e nt s . Besides the import a nt p syc h o-
socially orient e d , emotionally support i ve discussions withthe pat i e nt , t h e rapeutic emphasis should be placed on nu-tritional advice ,with the aim of bringing about a changein life style during pre g n a n c y.The scheme favo red by t h eauthors is shown in Fi g u re 2.

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 5/13
Figure 3:Acupressure at P6 every 4 hours, either manually or using
an acupressure band
GingerGinger is a classical remedy used throughout Asia to treatnausea and vomiting during pregnancy. Several currentstudies have compared the effectiveness of ginger to thatof a placebo in the treatment of nausea or vomiting inpregnancy. Several studies have proved that ginger (at adose of about 1 g/day) reduces nausea,thus providing anaturopathic therapeutic approach (Fischer-Rasmussen et
al.1990; Vutyavanich et al.2001; Niebyl 2002; Ismail 2007).
Balanced SupplementsAs early as the beginning of the 1990s,Czeizel and cowor-kers showed that administration of multivitamin sup-plements, which,apart from containing lower doses of vitamin B6 (2.6 mg),also contained 4.0 µg vitamin B12,statistically reduces HG by 50%.This result was based ona study in which the multivitamin supplement was ad-ministered to 500 pregnant women,and 500 pregnantwomen in the control group were given a placebo con-taining only vitamin C. Interviews carried out during the
first trimester showed that the incidence of pregnancyaccompanied by nausea was substantially higher in theplacebo group (6.6% vs. 3 % at the end of the first trimes-ter).The authors presumed this to be the result of a latentvitamin deficiency that normalized due to substitution,thus leading to a distinct i m p rove m e nt in the clinical sy m p-toms (Czeizel et al. 1992). Virtually at the same time, twocontrolled randomized studies were published which exa-mined the effe cts of vitamin B6 substitution as a mono-t h e ra py on HG (Sahakian et a l . 1 9 9 1 ;Vu t yavanich et a l . 1 9 9 5 ) .In 1991,Sahakian and coworkers reported on the results of a study performed on 59 pregnant women with HG, whowere randomly allocated to two study branches.31 test
persons received 25 mg of vitamin B6 3 x daily; the other28 test persons received a placebo.The parameters of bothgroups were comparable at the start of the study. After athree-day treatment, the severe cases of nausea decreasedsignificantly (median difference 4.3 ± 2.1 vs.1.8 ± 2.2;p < 0.1).The number of pregnant women with vomiting also de-creased from 15 to 8/31 in this branch of the study;in the
placebo group,on the other hand, the rate increased from10 to 15/28. The authors hereby confirmed, in a randomizeddouble-blind study, the results of a study performed byWillis and colleagues in 1942.
In 1995, the results of a further randomized,double-blindstudy by Vutyavanich and coworkers from Thailand werepublished:169 pregnant women were administered 30 mgof vitamin B6 daily (divided into three separate doses);167 pregnant women received a placebo applied in thesame manner (Vutyavanich et al. 1995).The results wereevaluated by way of a score.The decrease in symptoms
was more statistically significant in the group receivingvitamin B6 than in the placebo group, particularly duringthe first three days.The authors therefore recommendvitamin B6 as the substance of choice for treatment of HG.
Another vitamin with possible antiemetic effects, vitaminB12, is also under discussion.There is,however, little data onthis subject. A study performed by Conklin and coworkersin 1958 was not able to show any significant e ffe cts (Co n k l i nand Nesbitt 1958). In the studies available,the laboratoryparameters of pregnant women with and without symp-toms were unfortunately,not compared, but they did uni-formly show the positive effects of vitamin substitution.
Bühling K. J. Nausea... Gynakol Geburtsmed Gynakol Endokrinol 2008;4(1):36–48 publiziert 31.03.08 www.akademos.de/gyn © akademos Wissenschaftsverlag 2008 ISSN 1614-8533
P6
7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 6/13
In view of the effectiveness of vitamin B6 on the symptomsof hyperemesis gravidarum, it must be assumed that hypo-vitaminosis of this vitamin (at least latent) is a further pa-thogenetic factor.
In Germany, Nausan®,an approved supplement that makesuse of the antiemetic characteristics of high doses of vita-
min B6, has been available for the treatment of nausea/-hy p e remesis gravidarum since 2007. I t also co ntains a smallamount of vitamin B12.Nausan® should be taken from atleast 3 times,up to a maximum of 6 times daily.
Another illness should be taken into consideration withinthe fra m ework of HG t h e ra py. Re ce nt l y, C h i o s s i’s wo r kg ro u ppointed out that world literature describes 49 cases of afirst manifestation of Wernicke’s encephalopathy duringpregnancy.Wernicke’s encephalopathy is caused by a lackof vitamin B1 (lack of thiamine).The authors concludedthat patients with HG, who also suffer from neurologicalsymptoms (e.g. impaired vision,confusion, and ataxia),could suffer from this illness,and high-dose thiamine sub-stitution should be commenced immediately (Chiossi et al.2006). Robinson and colleagues made a similar recommen-dation when reporting on the case of a pregnant womanwith HG and diathesis. A lack of vitamin K proved to bethe cause in this case, whereby,the symptoms improvedquickly after suitable substitution (Robinson et al. 1998).
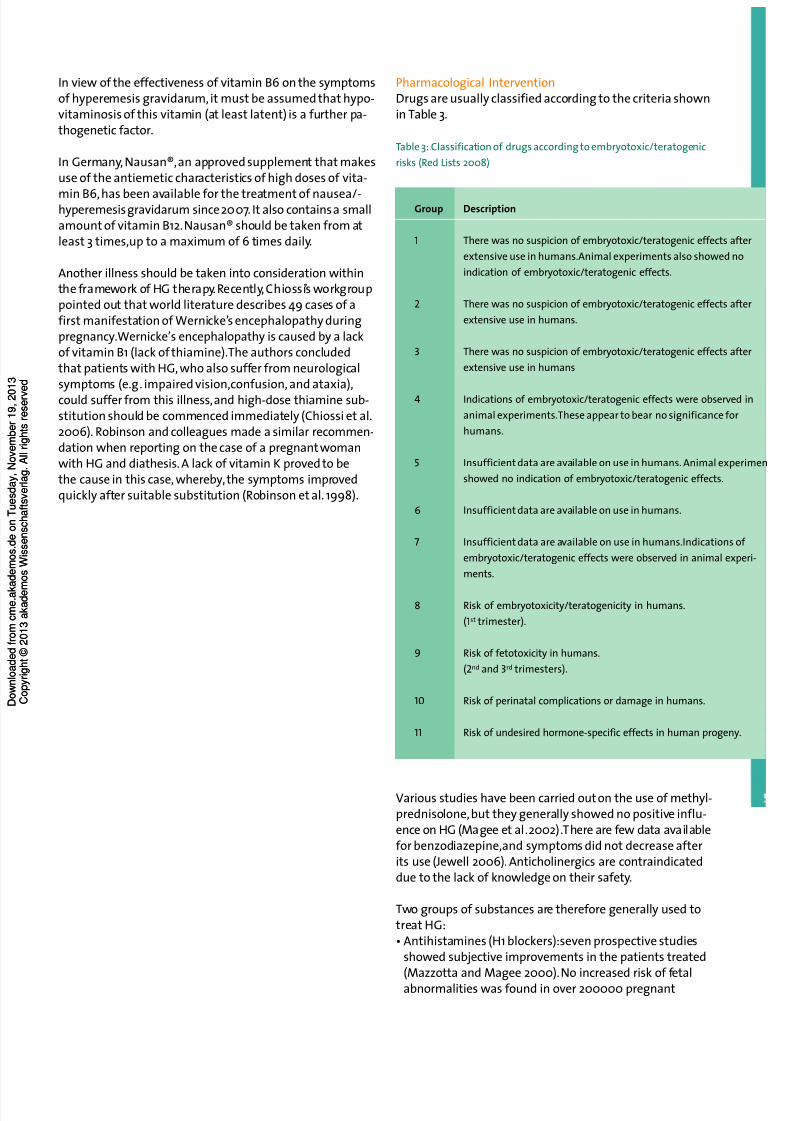
Pharmacological InterventionDrugs are usually classified according to the criteria shownin Table 3.
Table 3: Classification of drugs according to embryotoxic/teratogenic
risks (Red Lists 2008)
Various studies have been carried out on the use of methyl-prednisolone,but they generally showed no positive influ-e n ce on HG (Magee et a l .2 0 0 2 ) .T h e re are few data ava i l a b l efor benzodiazepine,and symptoms did not decrease afterits use (Jewell 2006). Anticholinergics are contraindicateddue to the lack of knowledge on their safety.
Two groups of substances are therefore generally used totreat HG:• Antihistamines (H1 blockers):seven prospective studies
showed subjective improvements in the patients treated(Mazzotta and Magee 2000).No increased risk of fetalabnormalities was found in over 200000 pregnant
Group
1
2
3
4
5
6
7
8
9
10
11
Description
There was no suspicion of embryotoxic/teratogenic effects after
extensive use in humans.Animal experiments also showed no
indication of embryotoxic/teratogenic effects.
There was no suspicion of embryotoxic/teratogenic effects after
extensive use in humans.
There was no suspicion of embryotoxic/teratogenic effects after
extensive use in humans
Indications of embryotoxic/teratogenic effects were observed in
animal experiments.These appear to bear no significance for
humans.
Insufficient data are available on use in humans. Animal experimen
showed no indication of embryotoxic/teratogenic effects.
Insufficient data are available on use in humans.
Insufficient data are available on use in humans.Indications of
embryotoxic/teratogenic effects were observed in animal experi-
ments.
Risk of embryotoxicity/teratogenicity in humans.
(1st trimester).
Risk of fetotoxicity in humans.
(2nd and 3rd trimesters).
Risk of perinatal complications or damage in humans.
Risk of undesired hormone-specific effects in human progeny.

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 7/13
women who took H1 blockers in early gravidity.A meta-analysis even showed a slightly reduced risk of fetal mal-formation (Seto et al. 1997). If the above-mentionedmeasures are unsuccessful,the H1 antihistamine meclo-zine (Peremesin®) can be administered (12.5 mg max. 4 xdaily). Although the substance was shown to be embryo-toxic in animal experiments, similar effects were not
found in humans; the substance is therefore classified inGroup 3 of the classification of drug safety in pregnancy(see Tab.3). In 1979, the very strict American FDA evenreapproved the drug for use during pregnancy (Schaeferand Spielmann 2001;Magee et al. 2002).The soporificdoxylamine (Hoggar N®; 12.5 mg up to 3x daily),which isoften used in the USA,is a further option.Some studiesshow that the H1 antagonist doxylamine is effective intreating nausea/HG. Doxylamine is classified as a Group 4drug with regard to its use during pregnancy (see Tab. 3)(Schaefer and Spielmann 2001;Magee et al. 2002).
• Dopamine antagonists:within this context, metoclopra-mide (MCP) is probably the most widely used drug. Sur-prisingly enough, there are no randomized studies on thisdrug. It is unlikely that the drug has teratogenic effects,based on the data available (corresponding to Group 4 of the classification of drugs for use during pregnancy, seeTab.3), but only a limited number of studies have beencarried out on the drug. In spite of this,MCP is one of most frequently used drugs in Germany for treating HG;the dosage is 10 mg (max. 4 x daily). Evidence is available,however, that promethazine, which belongs to the samegroup of substances, reduces emesis (Atosil®;12.5 mg,max. 4 x daily). Promethazine is also classified in the drugsafety Group 4 (Schaefer and Spielmann 2001; Magee et
a l .2 0 0 2 ) . D i m e n hyd r i n ate (Vo m ex A® ) , which also belongsto this group of active ingredients, was also shown tohave positive effects (Cartwright 1951). Although no teratogenic effects were found in animal experiments, the-manufacturers have stated that the extent of the experi-ments was not sufficient to exclude such characteristics.T h e re fo re ,if the use of a dopamine ant a go n i s t is indicat e d ,promethazine is the preferred drug. At least one study on800 mother-child pairs has been published on the safetyof this drug.
Patients should be informed that all the above-mentioned
active ingredients reduce the capability to react (Red Lists2007).Experience has shown,however, that there is a muchhigher acceptance of drugs that are indicated for treatingvomiting than drugs prescribed as “sleeping pills”or “psy-chotropic”drugs.
In rare therapy-resistant cases,after the appropriate risk-benefit analysis,the possibility of administering the anti-emetic antidepressive mirtazapine (Remergil®) or the anti-emetic ondansetrone (Zof ran®) remains (Rohde et a l . 2 0 0 3 ) .In a ve ry small study,i t was found t h at the latter is not m o reeffective than promethazine,even if clinical practice provi-des a different impression (Sullivan 1995).The products are
summarized in Table 4. It should be mentioned that in theUSA, in Bendectin® (in the United Kingdom Debendox®,inCanada Diclectin®) a pro d u ct i s, or was ava i l a b l e ,which co n-tains a co m b i n ation of 10 mg of vitamin B6 and 10 mg dox y-lamine.At the time of the Contergan® scandal, a study waspublished in which the authors pointed out a slightly in-creased risk of lip-jaw-palate cleft associated with the use
of Bendectin® (Golding et al. 1983).This led the manufac-turers to recall the drug, but although the results of somehigh-quality studies co nt ra d i cted these findings, the manu-facturers did not re-release the drug onto the market. InCanada,where health authorities are as strict as those inGermany, Diclectin® is still on the market (Mitchell et al.1981;Mitchell et al. 1983; Elbourne et al. 1985).
Bühling K. J. Nausea... Gynakol Geburtsmed Gynakol Endokrinol 2008;4(1):36–48 publiziert 31.03.08 www.akademos.de/gyn © akademos Wissenschaftsverlag 2008 ISSN 1614-8533
7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 8/13
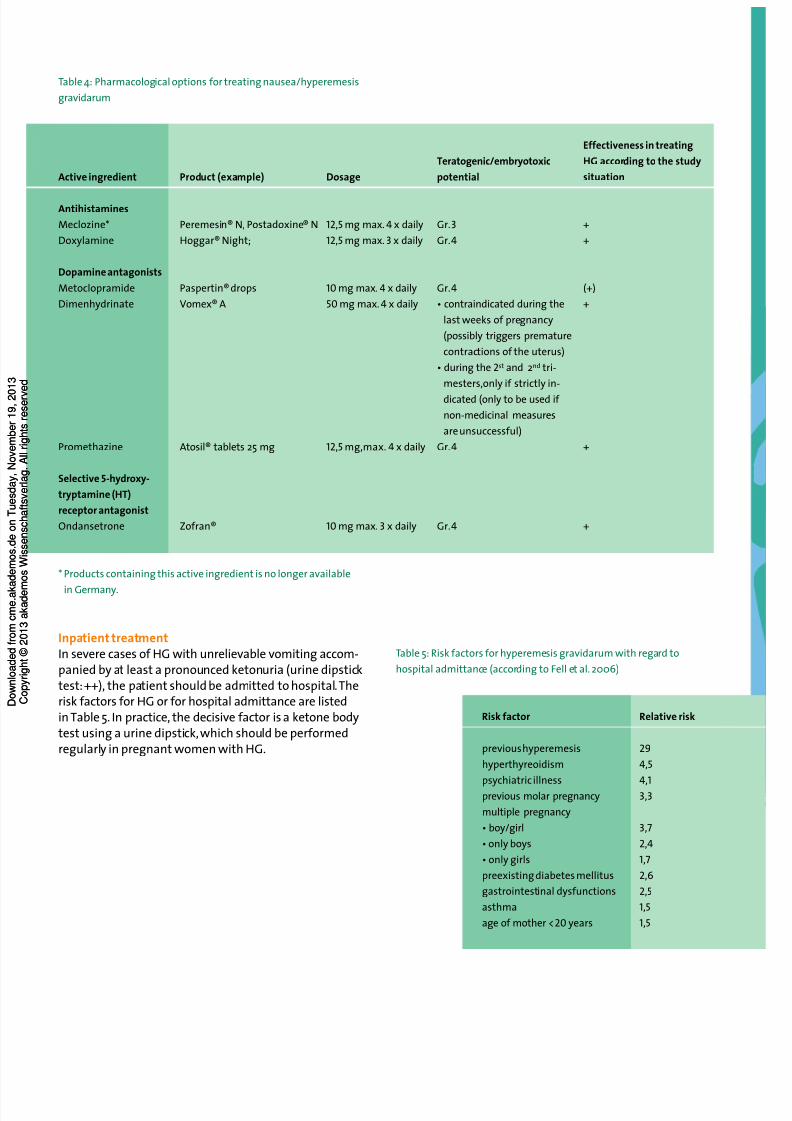
Table 4: Pharmacological options for treating nausea/hyperemesis
gravidarum
* Products containing this active ingredient is no longer available
in Germany.
Inpatient treatmentIn severe cases of HG with unrelievable vomiting accom-panied by at least a pronounced ketonuria (urine dipsticktest:++), the patient should be admitted to hospital.Therisk factors for HG or for hospital admittance are listedin Table 5. In practice, the decisive factor is a ketone bodytest using a urine dipstick,which should be performedregularly in pregnant women with HG.
Table 5: Risk factors for hyperemesis gravidarum with regard to
hospital admittance (according to Fell et al. 2006)
Active ingredient
Antihistamines
Meclozine*
Doxylamine
Dopamine antagonists
Metoclopramide
Dimenhydrinate
Promethazine
Selective 5-hydroxy-
tryptamine (HT)
receptor antagonist
Ondansetrone
Product (example)
Peremesin® N, Postadoxine® N
Hoggar® Night;
Paspertin® drops
Vomex® A
Atosil® tablets 25 mg
Zofran®
Dosage
12,5mg max.4 x daily
12,5mg max.3 x daily
10mg max.4 x daily
50 mg max.4 x daily
12,5mg,max. 4 x daily
10mg max.3 x daily
Teratogenic/embryotoxic
potential
Gr.3
Gr.4
Gr.4
• contraindicated during the
last weeks of pregnancy
(possibly triggers premature
contractions of the uterus)
• during the 2st and 2nd tri-
mesters,only if strictly in-
dicated (only to be used if
non-medicinal measures
are unsuccessful)
Gr.4
Gr.4
Effectiveness in treating
HG according to the study
situation
+
+
(+)
+
+
+
Risk factor
previous hyperemesis
hyperthyreoidism
psychiatric illnessprevious molar pregnancy
multiple pregnancy
• boy/girl
• only boys
• only girls
preexisting diabetes mellitus
gastrointestinal dysfunctions
asthma
age of mother <20 years
Relative risk
29
4,5
4,1
3,3
3,7
2,4
1,7
2,6
2,5
1,5
1,5

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 9/13
“Somatic”treatment consists of abstention from food,volume and electrolyte substitution,vitamin intake andadministration of antiemetics,as shown above.Food intakeshould not be built up until there has been a significantdecrease in vomiting.The patient cannot be dischargeduntil the ketone bodies in the urine are negative, the nutri-tional condition has stabilize d , and t h e re has been improve-
ment in the overall condition of the patient. It is also im-portant that the above-mentioned laboratory tests areperformed and that the patient’s body-weight is monito-red.Admittance to hospital,for instance,is a form of“psy-chosomatic intervention”, as the patient is thus removedfrom stressful domestic surroundings. In addition, psycho-somatic-oriented treatment (psychodynamic intervention,behavioral therapy) may be necessary.This should be dis-cussed with the patient.The pregnant woman should betaken seriously;labeling the patient a “hysterical psycho-logical case”is just as inappropriate, as treatment that islimited to antiemetic therapy and electrolyte balance.
CME Prakt Fortbild Gynakol Geburtsmed GynakolEndokrinol 2008; 4(1): 36–48
KeywordsHyperemesis gravidarum,Nausea gravidarum, vitaminsupplementation,pregnancy
ReferencesACOG Practice Bul l e t inNo 52. Clinical Manage m e ntG u i d-lines for Obstetrician-Gynecologists. Nausea and Vomitingof Pregnancy. Obstet Gynecol 2004;103: 803–815.Bohnet HG. Schilddrüsenfunktionsstörungen. In:Wulf K-H,Schmidt-Matthiesen H.Endokrinologie und Reproduktions-medizin I. 3. Auflage.München,Wien, Baltimore: Urban &
Schwarzenberg 1995.Buckwalter JG, Simpson SW. Psychological factors in theetiology and treatment of severe nausea and vomiting inpregnancy. Am J Obstet Gynecol 2002;186: S210–214.Bühling KJ,Bohnet HG. Ursachen und Therapie derSchwangerschaftsübelkeit. Frauenarzt 2006; 47:1110–1113.Cartwright EW. Dramamine in nausea and vomiting of pregnancy.West J Surg 1951; 59: 216–34.Chiossi G,Neri I,Cavazzuti M,Basso G,Facchinetti F.
Hyperemesis gravidarum complicated by Wernicke ence-phalopathy:background, case report,and review of theliterature.Obstet Gynecol Surv 2006;61: 255–68.Conklin FJ, Nesbitt REL. Buclizine hydrochloride for nauseaand vomiting of pregnancy. Obstet Gynecol 1958;11: 214–9.Cz ei z el AE, D udas I, F r itz G, Tecsoi A, Hanck A, Kun ovits G.
The effect of periconceptional multivitamin-mineralsupplementation on vertigo, nausea and vomiting in thefirst trimester of pregnancy. Arch Gynecol Obstet 1992;251:181–5.David M,Borde T,Kentenich H. Die psychische Belastungvon Migrantinnen im Vergleich zu einheimischen Frauen –der Einfluß von Ethnizität, Migrationsstatus und Akkultura-tionsgrad.Geburtsh Frauenheilk 2002;62(S1):37–44.Dodds L,Fell DB,Joseph KS, AllenVM, Butler B.Outcomeof pregnancies complicated by hyperemesis gravidarum.
Obstet Gynecol 2006;107:285–292.Elbourne D, Mutch L, Dauncey M, Campbell H,
Samphier M. Debendox revisited. Br J Obstet Gynaecol1985;92(8):780–5.Eliakim R,Abulafia O, Sherer DM. Hyperemesis gravida-rum: a current review. Am J Perinatol 2000;17: 207–218.Fell DB, Dodds L, Joseph KS,Allen VM, Butler B. Risk fac-tors for hyperemesis gravidarum requiring hospital admis-sion during pregnancy. Obstet Gynecol 2006;107: 277–284.Fischer-RasmussenW, Kjaer SK, Dahl C, Asping U. Gingert re at m e nt of hy p e remesis grav i d a r u m . Eur J Obstet G y n e co lReprod Biol 1991;38: 19–24.
GBE Gesundheitsberichterstattung des Bundes.(http://www.gbebund.de/gbe10/pkg_isgbe5.prc_isgbe?p_uid=gast&p_aid=47015335&p_sprache=D).GodwinTM, Montoro M, Mestman JH. Transient hyper-thyroidism and hyperemesis gravidarum: clinical aspects.Am J Obstet Gynecol 1992; 167:648–652.Golberg D, Szilagyi A, Graves L. Hyperemesis gravidarumand Helicobacter pylori infection: a systematic review.Obstet Gynecol 2007;110:695–703.Golding J,Vivian S,Baldwin JA.Maternal anti-nauseantsand clefts of lip and palate. Hum Toxicol 1983; 2(1):63–73.Goodwin TM.Nausea and vomiting of pregnancy: An ob-stetric sy n d ro m e.Am J Obstet G y n e col 2002; 1 8 6:S 1 8 4– S 1 8 9 .
Bühling K. J. Nausea... Gynakol Geburtsmed Gynakol Endokrinol 2008;4(1):36–48 publiziert 31.03.08 www.akademos.de/gyn © akademos Wissenschaftsverlag 2008 ISSN 1614-8533

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 10/13
Grun JP, Meuris S,De Nayer P, Glinoer D.The thyrotrophicrole of human chorionic gonadotrophin (hCG) in the earlystages of twin (versus single) pregnancies. Clin Endocrinol(Oxf) 1997;46:719–25.Ismail SK, Kenny L.Review on hyperemesis gravidarum.Best Pract Res Clin Gastroenterol 2007; 21:755–69.Jewell D,Young G. Interventions for nausea and vomiting
in early pregnancy. Cochrane Database Syst Rev 2006;4.Knight B, Mudge C,Openshaw S,White A,Hart A. Effectof acupuncture on nausea of pregnancy: a randomized,controlled trial. Obstet Gynecol 2001;97: 184–188.Koren G,Levichek Z. The teratogenicity of drugs for nau-sea and vomiting of pregnancy: Perceived versus true risk.Am J Obstet Gynecol 2002;186: S248–S252.Magee LA, Mazzotta P, Koren G. Evidence-based view of safety and effectiveness of pharmacologic therapy for nau-sea and vomitino of pregnancy (NVP).Am J Obstet Gynecol2002;186:S256–S261.Mar Melero-Montes M, Jick H. Hyperemesis gravidarumand the sex of the offs p r i n g. E p i d e m i o l o gy 2000; 1 2: 1 2 3–1 2 4.Mazzotta P, Magee LA. A risk-benefit assessment of phar-macological and nonpharmacological treatments for nau-sea and vomiting of pregnancy. Drugs 2000;59: 781–800.Meyer J. Geschichte der Hyperemesis gravidarum und ihrerTheorien.Straßburg:Inauguraldiss 1914.Miller F. Nausea and vomiting in pregnancy:The problemof perception – Is it really a disease? Am J Obstet Gynecol2002;186:S182–S183.Mitchell AA, Rosenberg L, Shapiro S, Slone D. Birth de-fects related to bendectin use in pregnancy. I. Oral cleftsand cardiac defects. JAMA 1981;245(22):2311–4.Mitchell AA, Schwingl PJ, Rosenberg L, Louik C,
Shapiro S. Birth defects in relation to Bendectin use inpregnancy. II. Pyloric stenosis.Am J Obstet Gynecol 1983;147(7):737–42.Munch S. Chicken or the egg? The biological-psychologicalcontroversy surrounding hyperemesis gravidarum. Soc SciMed 2002;55: 1267–1278.Newman V, Fullerton JT, Anderson PO. Clinical advancesin the management of severe nausea and vomiting duringpregnancy. J Obstet Gynecol Neonatal Nurs 1993;22:483–90.Niebyl JR, Goodwin TM.Overview of nausea and vomitingof pregnancy with an emphasis on vitamins and ginger.
Am J Obstet Gynecol 2002;186: S253–S255.Robinson JN, Banerjee R,Thiet MP. Coagulopathy secon-dary to vitamin K deficiency in hyperemesis gravidarum.Obstet Gynecol 1998; 92: 673–5.Rohde A, Dembinski J, Dorn C. Mirtazapin (Remergil) fortreatment resistant hyperemesis gravidarum:rescue of atwin pregnancy. Arch Gynecol Obstet 2003;268: 219–221.Roscoe JA, Matteson SE. Acupressure and acustimulationbands for control of nausea: A brief review. Am J ObstetGynecol 2002;186: S244–S247.Rote Liste® 2007. Frankfurt a.M.:Rote Liste® ServiceGmbH 2007.Rote Liste® 2008. Frankfurt a.M.:Rote Liste® Service
GmbH 2008.
Sahakian V, Rouse D, Sipes S, Rose N, Niebyl J. Vitamin B6is effective therapy for nausea and vomiting of pregnancy:a randomized,double-blind placebo-controlled study.Obstet Gynecol 1991; 78: 33–6.Schaefer Ch,Spielmann H.Arzneiverordnungen in derSchwangerschaft und Stillzeit. 6. Auflage.München, Jena:Urban & Fischer 2001.
S e to A, E inarson T,Ko r en G. P regnancy outcome fo l l ow i n gfirst trimester exposure to antihistamines: meta-analysis.Am J Perinatol 1997;14:119–24.Sheehan P. Hyperemesis gravidarum.Assesment andmanagement.Aust Fam Phys 2007; 36: 698–701.Simpson SW, Goodwin TM,Robins SB,Rizzo AA,
Howes RA, Buckwalter DK. Psychological factors andhyperemesis gravidarum. J Womens Health Gend BasedMed 2001;1:471–477.Soltani H,Taylor GM. Changing attitudes and perceptionsto hyperemesis gravidarum.Midwives 2003;6: 520–524.Sullivan CA,Johnson CA,Roach H,Martin RW,
Stewart DK, Morrison JC. A prospective, randomized,double-blind comparison of the serotonin antagonistondansetron to a standardized regimen of promethazinefor hyperemesis gravidarum. A preliminary investigation.Am J Obstet Gynecol 1995;172:299.Tan JYL,Loh KC, Yeo GSH, Chee YC. Transient hyperthyroi-dism of hy p e remesis grav i d a r u m . BJ OG 2002; 1 0 9: 6 8 3–6 8 8 .Verberg MFG, Gillott DJ, Al-Fardan N,Grudzinskas JG.
Hyperemesis gravidarum, a literature review.Hum ReprodUpdate 2005;11:527–539.Vutyavanich T, Kraisarin T,Ruangsri R. Ginger for nauseaand vomiting in pregnancy: randomized,double-masked,placebo-controlled trial.Obstet Gynecol 2001;97: 577–82.
Vutyavanich T, Wongtrangan S,Ruangsri R. Pyridoxinefor nausea and vomiting of pregnancy: a randomized,double-blind, placebo-controlled trial. Am J Obstet Gynecol1995;173:881–4.

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 11/13
Associate Professor Dr. med. Kai J.Bühling
Hormone ConsultationDepartment of GynecologyUniversity Medical Center Hamburg-Eppendorf Martinistr. 5220246 HamburgGermany
Associate Professor (PD) Dr.med. Kai J.Bühling commencedhis training as a specialist in Hamburg at the General Hos-pital,Altona (Prof. V. Lehmann) after completing his studiesin Hamburg and Berlin and gaining his doctorate in Berlin.In 1997, Dr.Bühling returned to Berlin and finished his spe-cialist training at the Department of Obstetrics (Director:Prof. J.W. Dudenhausen) and Department of Gynecology(Director: Prof. Dr.W.Lichtenegger). In 2004, he received hisqualification as a university lecturer at the Berlin Charité,after completion of his thesis on the subject of gestationaldiabetes.From 2004 to 2005,Dr.Bühling carried out clinicaland scientific work, focussing on gynecological endocrino-logy, for Prof. H. Lübbert,and continued this work aftermoving to Hamburg and joining the group practice Bohnet,
Knuth and Graf.Since 2007,he has his own practice and isconsultant and director of Hormone Consulting at the Uni-versity Medical Ce nter Hamburg - E p p e n d o rf, w h e re he isalso qualified to teach.Dr.Bühling has specialist qualifica-tions in obstetrics and perinatal medicine, gy n e co l o g i c a le n d o c r i n ology and reproductive medicine, as well as beingan approved diabetologist. Apart from his work on diabe-tes, diseases of the t hy roid gland, and on nutrition duringp re g n a n c y,his scientific work focuses on the diagnosticsand treatment of gynecological-endocrinological disease.
Conflict of interest
The author Kai J.Bühling declares that this article waswritten without the influence of any industrial interests.He also states that he has received material or financialsupport from the company Steripharm for an expertise.The gratuity has no influence on the co nt e nts of this art i c l e.
The author Matthias David declares that there is noconflict of interest as defined by the guidelines of theInternational Committee of Medical Journal Editors(ICMJE;www.icmje.org).
Manuscript informationSubmitted on: 08.03.2008
Accepted on:20.03.2008
Bühling K. J. Nausea... Gynakol Geburtsmed Gynakol Endokrinol 2008;4(1):36–48 publiziert 31.03.08 www.akademos.de/gyn © akademos Wissenschaftsverlag 2008 ISSN 1614-8533

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 12/13
CME-Continuing MedicalEducation
Nausea and hyperemesis gravidarum
Question 1Nausea gravidaruma. is a very rare illness,b. only affects women with a low standard of
education,c. is a very frequent illness,d. cannot be treated,e. must be treated by psychotherapy.
Question 2Nausea gravidarum develops ina. 0,1 % of all pregnant women,b. 0,5 % of all pregnant women,c. 1 % of all pregnant women,d. 10% of all pregnant women,e. > 50% of all pregnant women.
Question 3Which stat e m e nt is inco r re ctwith re ga rd to possiblecauses of hyperemesis gravidarum (HG)?a. HG is an expression of conflicts,such as rejection
of pregnancy, conflict caused by ambivalencetoward motherhood,an immature personality,dependency on the mother,fear of pregnancy.
b. HG is an expression of sexual dysfunction(s).
c. HG occurs in connection with exaggeratedsolicitousness on behalf of the partner.
d. HG is a conversion symptom,as an expression of a hysterical,neurotic,or depressive dysfunction.
e. HG is the result of psychosocial stress, violence,and/or conflict in the relationship between thepartners.
Question 4Which of the following illnesses must be excludedin patients with hyperemesis gravidarum in earlypregnancy?
a. Restless legs syndrome (RLS).b. Hyperthyreosis.c. Fibromyalgia.d. Preeclampsia.e. Coronary heart disease.
Question 5The pregnancy hormone HCGa. stimulates the function of the thyroid gland,b. inhibits the function of the thyroid gland,c. does not influence thyroid gland function,d. leads to a decrease in SHBG,e. is generated in the pituitary gland.
Question 6If TSH is suppressed during pregnancy,a. thyreostatic treatment should be commenced
immediately,b. no further measures are necessary,c. it is a primarily physiological process,d. low doses of L-thyroxine should be administered,e. it is a symptom of latent hypothyreosis.
Question 7A psychosocial component in the development of hyperemesis gravidaruma. can be excluded if the patient denies that such a
component exists during her first conversationwith the physician,
b. is a precondition for inpatient treatment,c. is an indication for psychotherapy,d. is improbable if the patient has just separated
from her partner,e. can often be elicited in a second conversation
with the patient.
Question 8The most significant therapeutic life-style altera-tions in patients with nausea gravidarum are:a. to eat three large meals,b. to eat a small meal (crisp bread) before getting
up in the morning, particularly in the case of morning sickness
c. to avoid eating proteins,d. to drink two liters of fruit juice a day,e. to continue a fast that has possibly already
begun.
Question 9Which of the following options are effective intreating hyperemesis gravidarum, according toevidence-based criteria?1. Acupressure.2. Prescription of preparations containing ginger.3. Removing the patient from the domestic
surroundings by admittance to hospital.4. High-dosage vitamin B6 supplementation
(e.g.Nausan®)5. Administration of promethazine (e. g. Atosil®)
a. All answers are correct.b. Only answers 1, 2 and 3 are correct.c. Only answers 1, 2, 4 and 5 are correct.d. Only answer 5 is correct.e. None of the answers are correct.

7/23/2019 6.Buhling and Davids Patofis
http://slidepdf.com/reader/full/6buhling-and-davids-patofis 13/13
Question 10In which of the following instances, in connection
with hyperemesis gravidarum, should hospitaladmittance be considered?1. Ketonuria (++).2. Exsiccosis.3. A stressful domestic situation.4. A weakened general condition.5. Uterine bleeding.
a. All answers are correct.b. Only answer 1 is correct.c. Only answers 1 and 5 are correct.d. Only answers 3 and 4 are correct.e. None of the answers are correct.