
63F with RA and is taking prednisone and methotrexate. She has a failed R hip arthroplasty and tells...
17
63F with RA and is taking prednisone 63F with RA and is taking prednisone and methotrexate. She has a failed R and methotrexate. She has a failed R hip arthroplasty and tells you her hip arthroplasty and tells you her surgeon is interested in doing a surgeon is interested in doing a revision. On exam, she has weakness of revision. On exam, she has weakness of R grip, generalized hyperreflexia and R grip, generalized hyperreflexia and hypertonia, and synovitis. hypertonia, and synovitis. What is the next step? What is the next step? A. Obtain ANA, anti-DNA, and anti-Sm ab A. Obtain ANA, anti-DNA, and anti-Sm ab B. Test for cryoglobulins B. Test for cryoglobulins C. Add tumor necrosis factor alpha C. Add tumor necrosis factor alpha inhibitor inhibitor D. Obtain images of cervical spine D. Obtain images of cervical spine
-
date post
19-Dec-2015 -
Category
Documents
-
view
214 -
download
0
Transcript of 63F with RA and is taking prednisone and methotrexate. She has a failed R hip arthroplasty and tells...

63F with RA and is taking prednisone and 63F with RA and is taking prednisone and methotrexate. She has a failed R hip methotrexate. She has a failed R hip arthroplasty and tells you her surgeon is arthroplasty and tells you her surgeon is interested in doing a revision. On exam, interested in doing a revision. On exam, she has weakness of R grip, generalized she has weakness of R grip, generalized hyperreflexia and hypertonia, and hyperreflexia and hypertonia, and synovitis.synovitis.
What is the next step?What is the next step?A. Obtain ANA, anti-DNA, and anti-Sm abA. Obtain ANA, anti-DNA, and anti-Sm abB. Test for cryoglobulinsB. Test for cryoglobulinsC. Add tumor necrosis factor alpha inhibitorC. Add tumor necrosis factor alpha inhibitorD. Obtain images of cervical spineD. Obtain images of cervical spine
35F on OCPs for 10 y develops a PE 35F on OCPs for 10 y develops a PE and is found to be heterozygous for and is found to be heterozygous for prothrombin g20210A mutation. She prothrombin g20210A mutation. She was anticoagulated for 6 months. was anticoagulated for 6 months.
How should she be counseled?How should she be counseled?
A.A. Take a daily aspirinTake a daily aspirin
B.B. Continue life-long anticoagulationContinue life-long anticoagulation
C.C. Offer genetic counseling for family Offer genetic counseling for family membersmembers
D.D. Do nothing furtherDo nothing further

You are told that test X has a You are told that test X has a sensitivity of 85% and a specificity of sensitivity of 85% and a specificity of 70%.70%.
Calculate the positive likelihood ratio.Calculate the positive likelihood ratio. Is this a good test?Is this a good test?


26F marathon runner present to clinic 26F marathon runner present to clinic with fatigue and mild dyspnea with with fatigue and mild dyspnea with exertion. You check a hgb and find exertion. You check a hgb and find that it is 7.8 g/dl.that it is 7.8 g/dl.
All the following might explain her All the following might explain her anemia except:anemia except:
A. Dilutional pseudoanemiaA. Dilutional pseudoanemia
B. Intravascular hemolysisB. Intravascular hemolysis
C. Iron deficiency anemiaC. Iron deficiency anemia
D. Splenic sequestrationD. Splenic sequestration

Match sensitivity reaction with typeMatch sensitivity reaction with type
Type IType I Type IIType II Type IIIType III Type IVType IV
A.A. mast cell-mast cell-mediated reactionmediated reaction
B.B. Immune complex Immune complex mediatedmediated
C.C. T-cell mediatedT-cell mediated
D.D. Antibody-mediated Antibody-mediated reactionreaction

Match cancer and bone lesionMatch cancer and bone lesion
A.A. BreastBreast
B.B. ProstateProstate
C.C. LungLung
D.D. KidneyKidney
E.E. MyelomaMyeloma
F.F. ThyroidThyroid
G.G. MelanomaMelanoma
BlasticBlastic LyticLytic Blastic and LyticBlastic and Lytic

35M presents with Hep C with cirrhosis 35M presents with Hep C with cirrhosis presents with general malaise for last presents with general malaise for last week. On exam, he has an open skin week. On exam, he has an open skin lesion on R arm, no hepatosplenomegaly lesion on R arm, no hepatosplenomegaly or signs of decompensated liver failure. or signs of decompensated liver failure. Blood cultures are drawn and grow out a Blood cultures are drawn and grow out a gram negative rod. You suspect he gram negative rod. You suspect he became infected through close contact became infected through close contact with his dogs.with his dogs.
What is the best next step?What is the best next step?A.A. Start a fluoroquinoloneStart a fluoroquinoloneB.B. Start a penicillinStart a penicillinC.C. Start a tetracyclineStart a tetracyclineD.D. Initiate contact isolationInitiate contact isolation
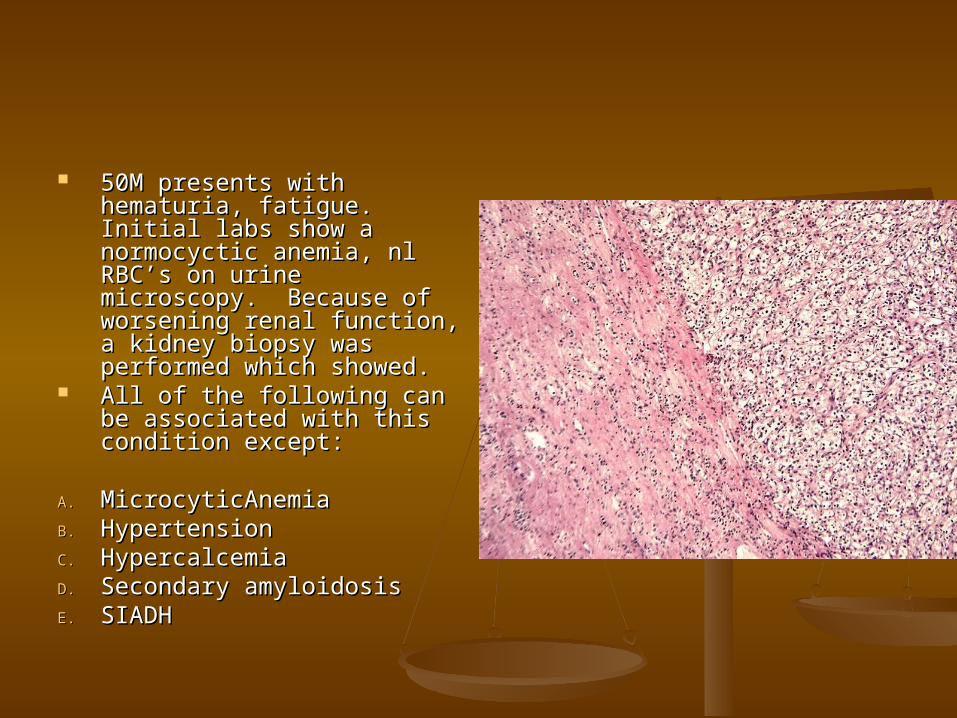
50M presents with 50M presents with hematuria, fatigue. Initial hematuria, fatigue. Initial labs show a normocyctic labs show a normocyctic anemia, nl RBC’s on urine anemia, nl RBC’s on urine microscopy. Because of microscopy. Because of worsening renal function, worsening renal function, a kidney biopsy was a kidney biopsy was performed which showed.performed which showed.
All of the following can be All of the following can be associated with this associated with this condition except:condition except:
A.A. MicrocyticAnemiaMicrocyticAnemiaB.B. HypertensionHypertensionC.C. HypercalcemiaHypercalcemiaD.D. Secondary amyloidosisSecondary amyloidosisE.E. SIADH SIADH

55F with CKD on HD 55F with CKD on HD presents with progressive presents with progressive pain in RUE. Also with pain in RUE. Also with itching, burning. No itching, burning. No trauma to this region. Ca x trauma to this region. Ca x Phos is 35. Picture is Phos is 35. Picture is shown on R.shown on R.
What is the most like cause of What is the most like cause of her condition?her condition?
A.A. CalciphylaxisCalciphylaxisB.B. Nephrogenic systemic Nephrogenic systemic
fibrosisfibrosisC.C. Stevens-Johnson’s Stevens-Johnson’s
syndromesyndromeD.D. Secondary amyloidosis due Secondary amyloidosis due
to HDto HD


35M with HIV presents 35M with HIV presents with severe HA and with severe HA and vomiting x 2 days. vomiting x 2 days. Fevers at home and in Fevers at home and in ED. No complaints on ED. No complaints on mental status changes. mental status changes. You are worried about You are worried about a meningitis, so you a meningitis, so you perform a lumbar perform a lumbar puncture. OP 35 mmhg. puncture. OP 35 mmhg. CSF stain shown. CSF stain shown.
What is the next best What is the next best step?step?
A. Start vancomycin, A. Start vancomycin, ampicillin, ceftriaxoneampicillin, ceftriaxone
B. Start antifungalsB. Start antifungalsC. Start dexamethasoneC. Start dexamethasoneD. Consult neurosurgeryD. Consult neurosurgery

45F life-long nonsmoker 45F life-long nonsmoker presents to clinic with presents to clinic with progressive DOE and RUQ progressive DOE and RUQ pain. She works in an pain. She works in an office setting, no recent office setting, no recent travels. On exam, she has travels. On exam, she has decreased B sounds at decreased B sounds at her bases, panniculitis of her bases, panniculitis of her abdomen. She is not her abdomen. She is not anemic. Because of anemic. Because of suspicious lesions on CXR, suspicious lesions on CXR, a CT chest was done and a CT chest was done and is shown.is shown.
What is the next best step?What is the next best step?A.A. Consult pulm for Consult pulm for
bronchoscopy and biopsybronchoscopy and biopsyB.B. Consult CT surgery for Consult CT surgery for
open lung biopsyopen lung biopsyC.C. Start bronchodilators, Start bronchodilators,
steroids, oxygensteroids, oxygenD.D. Put patient on airborn Put patient on airborn
precautions and check precautions and check AFB’s in sputumAFB’s in sputum

80M with NICM, EF 30% presents with 80M with NICM, EF 30% presents with increasing of SOB. Has been taking increasing of SOB. Has been taking diuretics as prescribed and has adhered to diuretics as prescribed and has adhered to dietary restrictions. On exam, he has JVD to dietary restrictions. On exam, he has JVD to his ear at 30 degrees, crackles to mid-lung, his ear at 30 degrees, crackles to mid-lung, and B LE edema- symmetric. His labs: serum and B LE edema- symmetric. His labs: serum Na 127, Cr 1.1, Urine Na 5, U P/C ratio 0.1. Na 127, Cr 1.1, Urine Na 5, U P/C ratio 0.1.
What is the most likely cause of his What is the most likely cause of his hyponatremia?hyponatremia?
A.A. CHF exacerbationCHF exacerbation
B.B. Renal salt wastingRenal salt wasting
C.C. SIADHSIADH
D.D. Nephrotic syndromeNephrotic syndrome
78M presents with ataxia for 2 weeks. He 78M presents with ataxia for 2 weeks. He reports one episode of urinary incontinence 3 reports one episode of urinary incontinence 3 days ago. His family brings him in to clinic days ago. His family brings him in to clinic saying, “He is becoming more forgetful.” saying, “He is becoming more forgetful.” You obtain a CT head and await the results. You obtain a CT head and await the results.
What is the next best step?What is the next best step?
A.A. Lumbar punctureLumbar puncture
B.B. Consult neurology for concerns of evolving Consult neurology for concerns of evolving CVACVA
C.C. Start antibioticsStart antibiotics
D.D. Obtain a CTLS MRI and start dexamethasoneObtain a CTLS MRI and start dexamethasone

35M with CKD stage V on 35M with CKD stage V on HD presents with HD presents with severe HA. In the ED, severe HA. In the ED, his BP is 230/120. He his BP is 230/120. He has a seizure and a has a seizure and a brain MRI is obtained brain MRI is obtained and shown. Blood and shown. Blood cultures drawn and cultures drawn and were negative. were negative.
What is the most likely What is the most likely diagnosis?diagnosis?
A.A. Septic emboliSeptic emboliB.B. Hypertensive Hypertensive
encephalopathyencephalopathyC.C. ToxoplasmosisToxoplasmosisD.D. Nocardia infectionNocardia infection

You are preparing for EBM and come You are preparing for EBM and come across an RCT with a power calculation. across an RCT with a power calculation. You find out that the trial did not enroll You find out that the trial did not enroll enough people to reach power.enough people to reach power.
What is the major concern with this trial?What is the major concern with this trial?
A.A. There is a chance of missing a true There is a chance of missing a true difference.difference.
B.B. There is a chance that the results show There is a chance that the results show that the treatment is effective when it is that the treatment is effective when it is not.not.
C.C. We will not be able to calculate the We will not be able to calculate the number needed to treat.number needed to treat.


















