63 duodenal diseases on computed tomography
20
63 Duodenal Diseases on Computed Tomography
-
Upload
muhammad-bin-zulfiqar -
Category
Education
-
view
96 -
download
2
Transcript of 63 duodenal diseases on computed tomography

63 Duodenal Diseases on Computed Tomography

CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
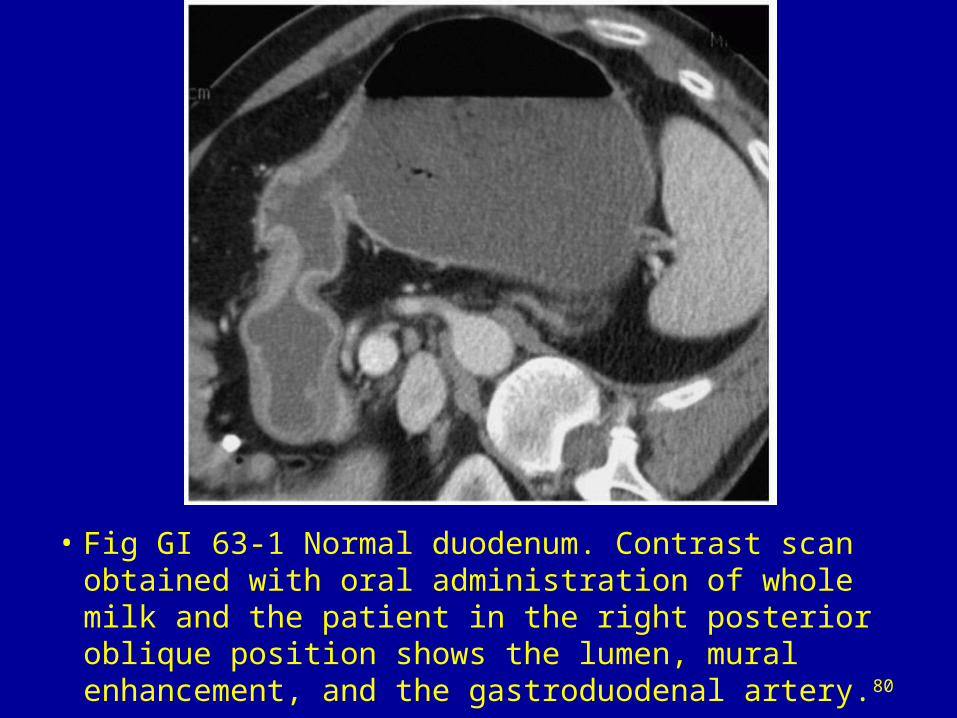
• Fig GI 63-1 Normal duodenum. Contrast scan obtained with oral administration of whole milk and the patient in the right posterior oblique position shows the lumen, mural enhancement, and the gastroduodenal artery.80

• Fig GI 63-2 Diverticulum. Contrast scan shows two “duodenal lumina,” with the true lumen lateral to the diverticulum (straight arrow). The diverticulum contains an air-fluid level and causes medial displacement of the pancreatic head (curved arrow).80

• Fig GI 63-3 Duplication. Scan without oral contrast shows two fluid-attenuation structures in the second portion of the duodenum. The duplicated segment (curved arrow) is medial to the true lumen and contains debris. The true lumen is narrowed (straight arrow).80
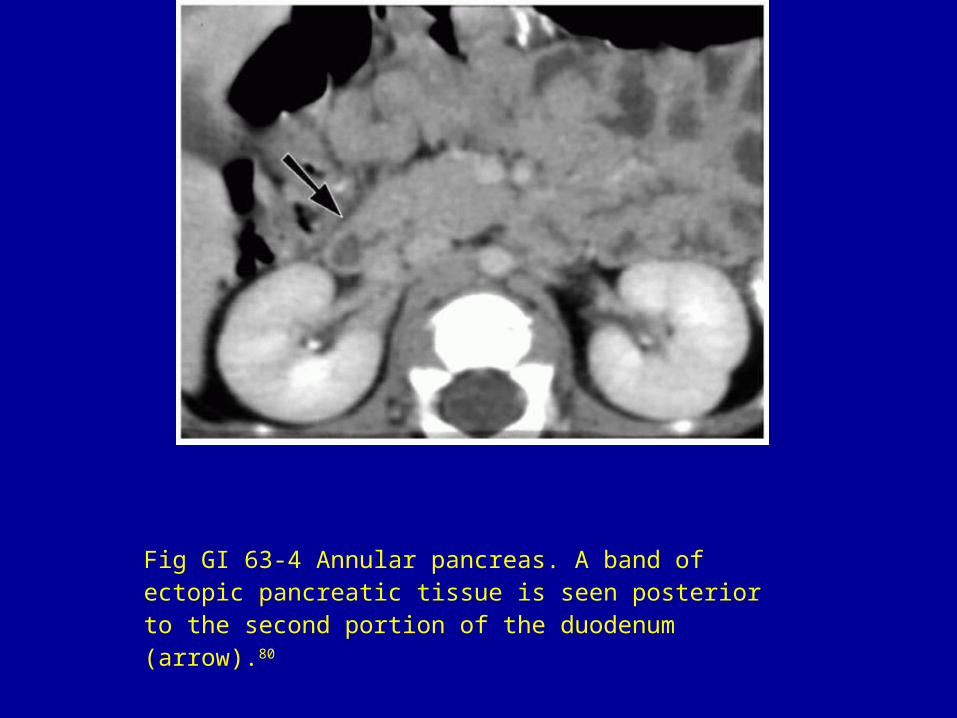
Fig GI 63-4 Annular pancreas. A band of ectopic pancreatic tissue is seen posterior to the second portion of the duodenum (arrow).80

• Fig GI 63-5 Ruptured duodenum (motor vehicle accident). There is fluid in the duodenum and leakage of fluid into the right anterior pararenal space (arrow).80

Fig GI 63-6 Duodenal perforation (endoscopy). Thick-walled, contracted duodenum with gas in the adjacent retroperitoneum (arrow).80
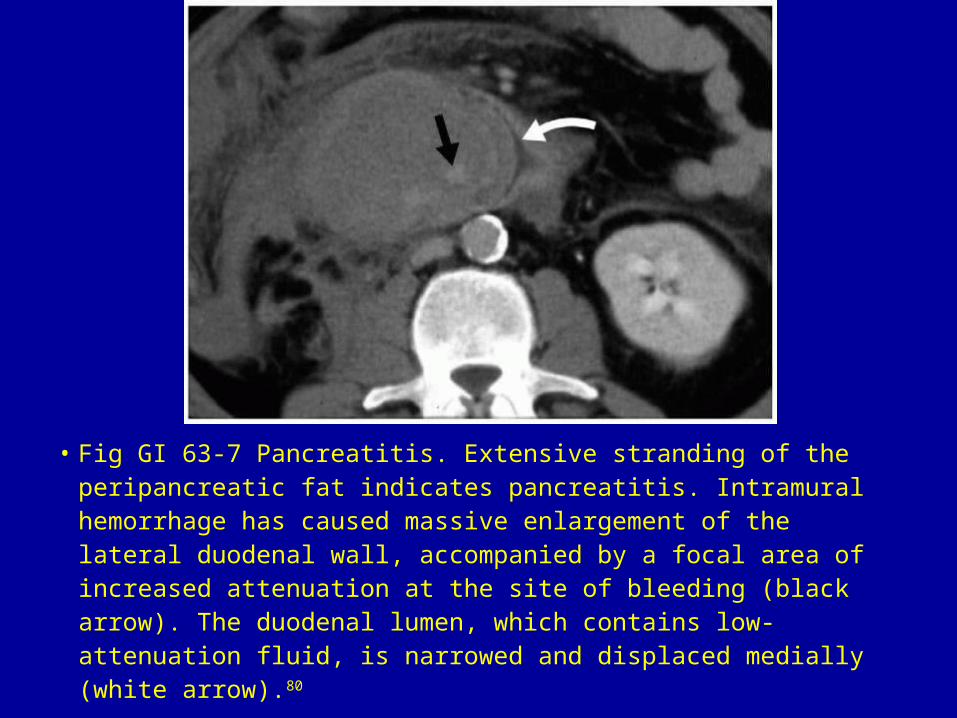
• Fig GI 63-7 Pancreatitis. Extensive stranding of the peripancreatic fat indicates pancreatitis. Intramural hemorrhage has caused massive enlargement of the lateral duodenal wall, accompanied by a focal area of increased attenuation at the site of bleeding (black arrow). The duodenal lumen, which contains low-attenuation fluid, is narrowed and displaced medially (white arrow).80

• Fig GI 63-8 Perforated ulcer. Intraperitoneal extravasation of oral contrast material from the lateral portion of the duodenum (white arrow) and leakage of contrast around the liver (black arrow).

• Fig GI 63-9 Gastric outlet obstruction (duodenal ulcer). Dilated stomach and thickened wall of the duodenal bulb, associated with stranding of the periduodenal fat (arrow).80
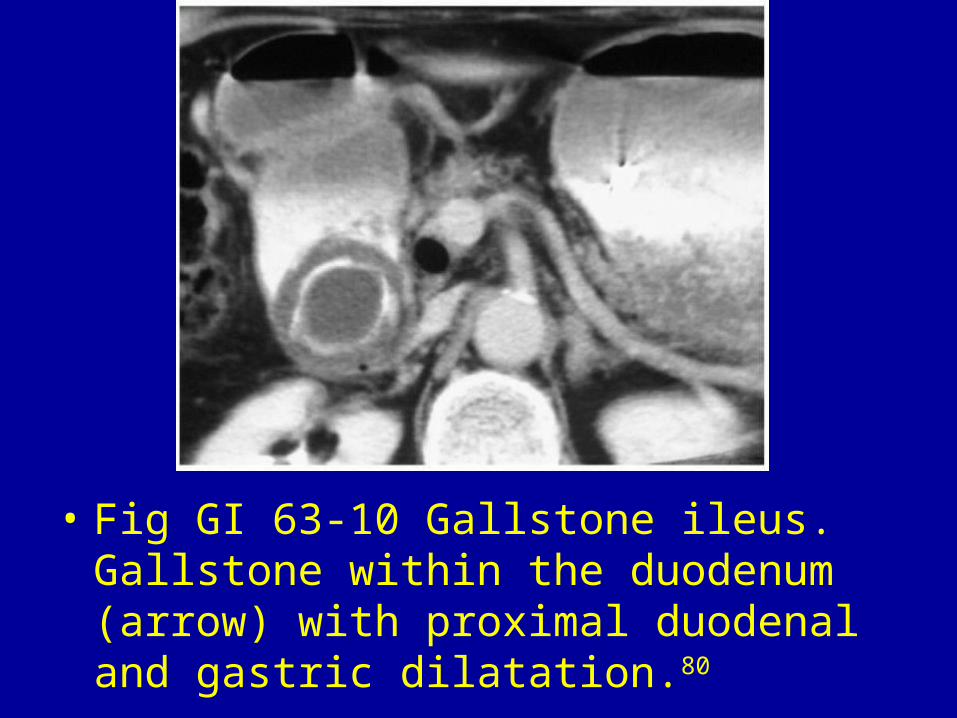
• Fig GI 63-10 Gallstone ileus. Gallstone within the duodenum (arrow) with proximal duodenal and gastric dilatation.80

• Fig GI 63-11 Henoch-Schonlein purpura. Marked thickening of the second and fourth portions of the duodenal wall (arrows). The lumen was narrowed, but there was no obstruction of the gastric outlet.80

• Fig GI 63-12 Lipoma. Low-attenuation lesion with well-circumscribed margins (arrow).80

• Fig GI 63-13 Villous adenoma. Soft-tissue mass (white arrow) arising from the medial wall of the duodenum. The duodenal lumen is narrowed (black arrow).80

• Fig GI 63-14 Peutz-Jeghers syndrome. Soft-tissue filling defect in the duodenal lumen (arrow), outlined by water. There were several polyps in the proximal small bowel.80

• Fig GI 63-15 Adenocarcinoma. A solid intraluminal soft-tissue mass (arrow) without transmural invasion or retroperitoneal adenopathy.80
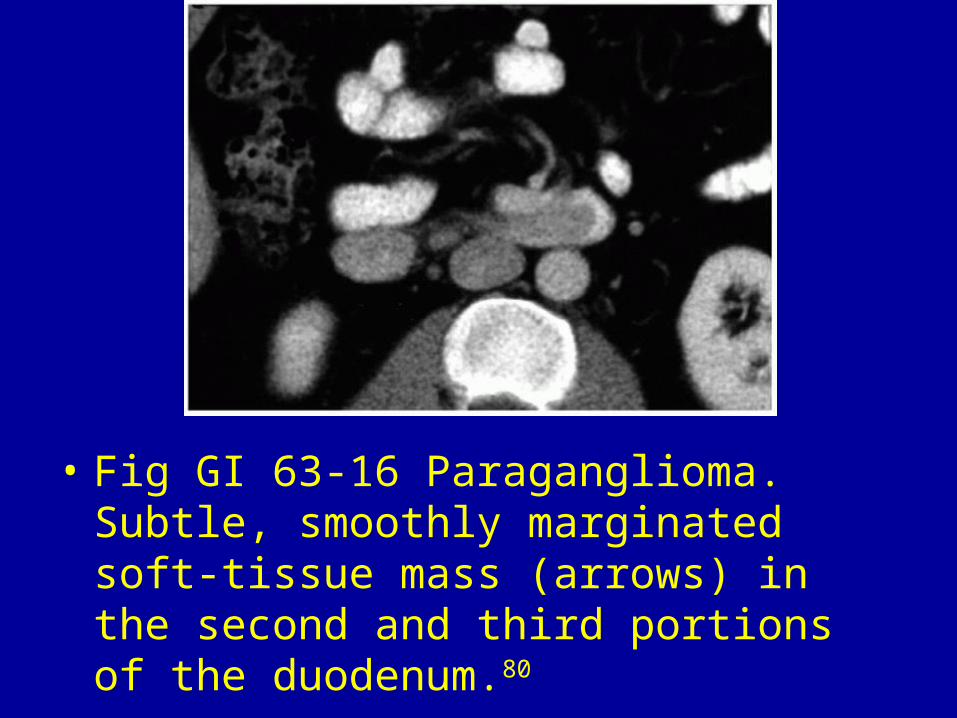
• Fig GI 63-16 Paraganglioma. Subtle, smoothly marginated soft-tissue mass (arrows) in the second and third portions of the duodenum.80

• Fig GI 63-17 Metastasis (colon cancer). Mass of soft-tissue attenuation that causes lateral displacement of the duodenum (arrow). The lesion mimics a mass arising in the duodenum or pancreatic head.80