
6 bubbly lesions of bone
33
6 Bubbly Lesions of Bone
-
Upload
muhammad-bin-zulfiqar -
Category
Education
-
view
93 -
download
1
Transcript of 6 bubbly lesions of bone

6 Bubbly Lesions of Bone

CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL

• Fig B 6-1 Fibrous dysplasia. Views of (A) the humerus and (B) the ischium in two different patients show expansile lesions containing irregular bands of sclerosis, giving them a multilocular appearance.

• Fig B 6-2 Giant cell tumor of the distal femur. Typical eccentric lucent lesion in the metaphysis extends to the immediate subarticular cortex. The surrounding cortex, though thinned, remains intact.

• Fig B 6-3 Malignant giant cell tumor. The tumor has caused cortical disruption, extends outside the host bone, and has an ill-defined margin.

• Fig B 6-4 Fibrous cortical defect. Multilocular, eccentric lucency in the distal tibia. Note the thin, scalloped rim of sclerosis.

• Fig B 6-5 Nonossifying fibroma. Multilocular, eccentric lucency with a sclerotic rim in the distal femur.

• Fig B 6-6 Simple bone cyst in the proximal humerus. The cyst has an oval configuration, with its long axis parallel to that of the host bone. Note the thin septa that produce a multiloculated appearance.
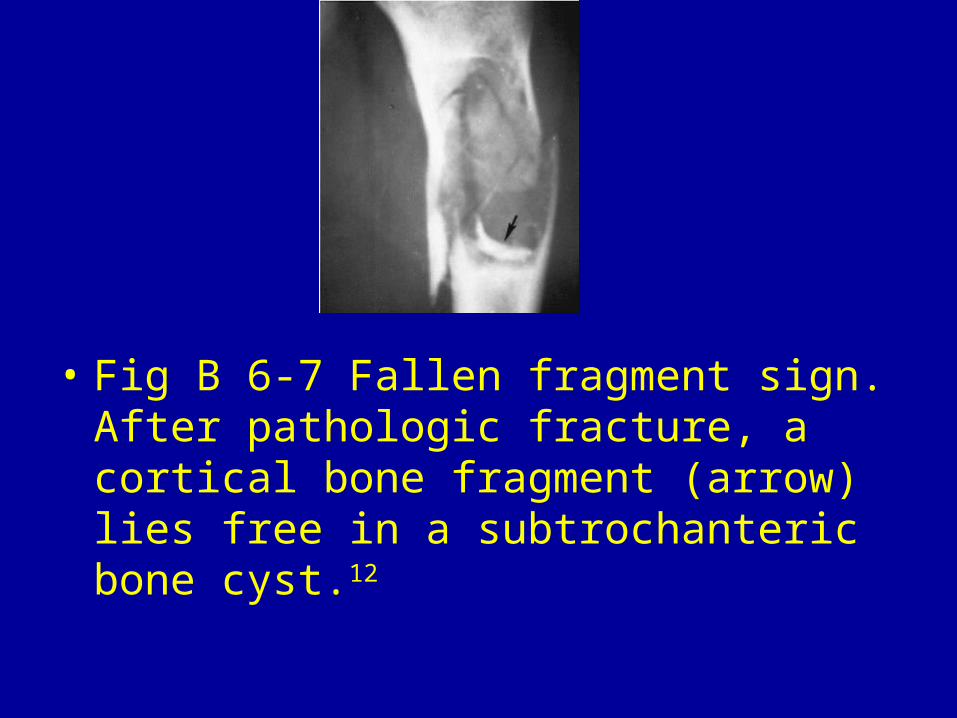
• Fig B 6-7 Fallen fragment sign. After pathologic fracture, a cortical bone fragment (arrow) lies free in a subtrochanteric bone cyst.12
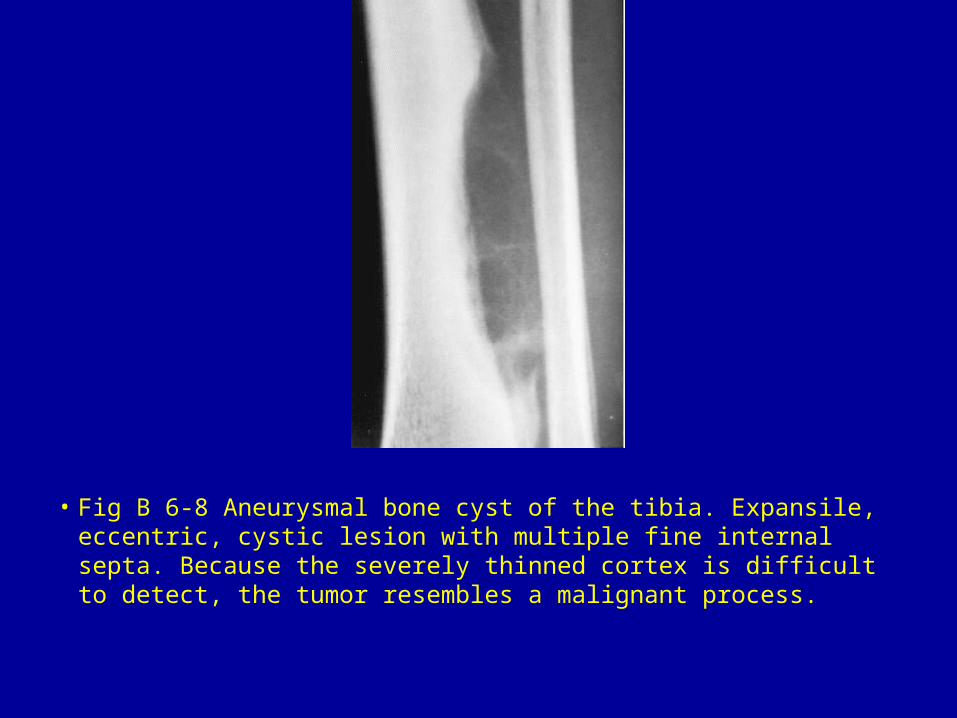
• Fig B 6-8 Aneurysmal bone cyst of the tibia. Expansile, eccentric, cystic lesion with multiple fine internal septa. Because the severely thinned cortex is difficult to detect, the tumor resembles a malignant process.

• Fig B 6-9 Enchondroma. (A) Well-demarcated tumor (arrow) expands the bone and thins the cortex. (B) Pathologic fracture (arrow).

• Fig B 6-10 Multiple enchondromatosis. View of both hands demonstrates multiple globular and expansile lucent filling defects involving all the metacarpals and the proximal and middle phalanges.

• Fig B 6-11 Central chondrosarcoma. Irregular and ill-defined lytic lesion of the lower ilium.

• Fig B 6-12 Brown tumors. Multiple lytic lesions (A) in the pelvis and (B) about the knee.

• Fig B 6-13 Solitary plasmacytoma of the ilium (arrows). Some residual streaks of bone remain in this osteolytic lesion, producing a soap-bubble appearance.

• Fig B 6-14 Solitary plasmacytoma. Highly destructive tumor that has obliterated virtually all of the left half of the pelvis.

• Fig B 6-15 Renal cell carcinoma metastatic to bone. Typical expansile bubbly lesion (arrows) in the proximal shaft of the radius.
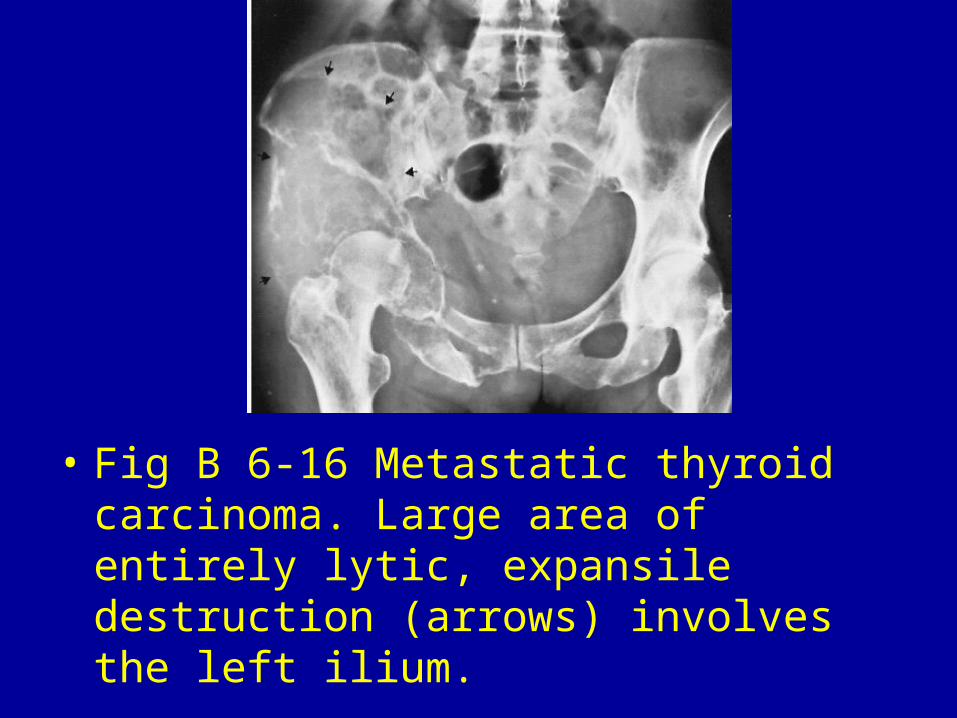
• Fig B 6-16 Metastatic thyroid carcinoma. Large area of entirely lytic, expansile destruction (arrows) involves the left ilium.

• Fig B 6-17 Lymphoma. There is a focal lytic defect with endosteal scalloping of the cortex.

• Fig B 6-18 Langerhans cell histiocytosis. Bubbly osteolytic lesion in the femur, with scalloping of the endosteal margins and a thin layer of periosteal response.
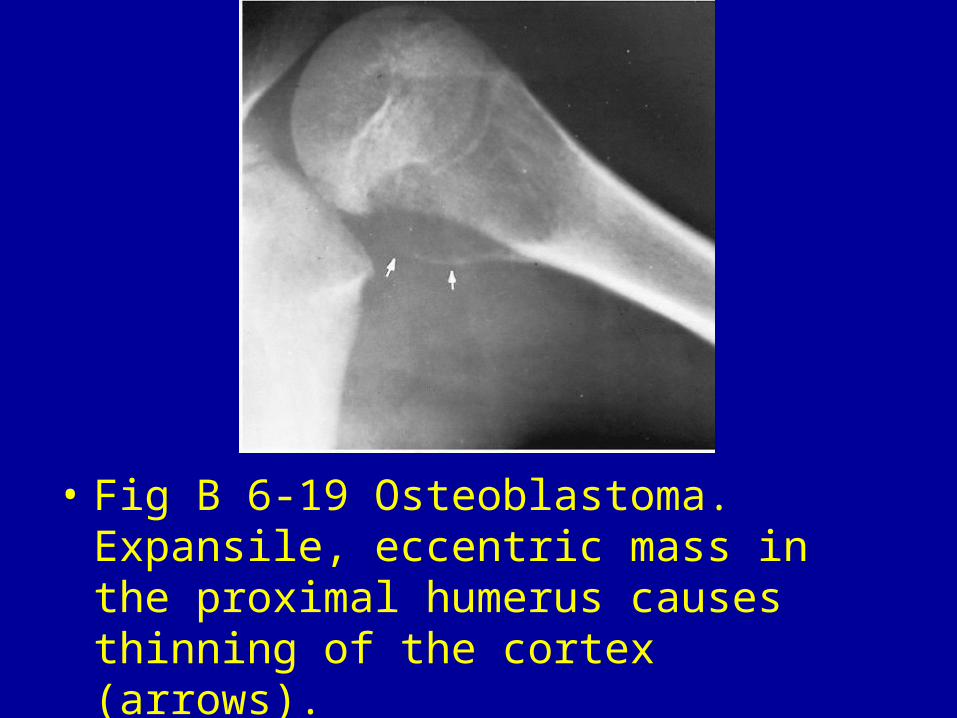
• Fig B 6-19 Osteoblastoma. Expansile, eccentric mass in the proximal humerus causes thinning of the cortex (arrows).

Fig B 6-20 Chondroblastoma. Osteolytic lesion containing calcification (arrows) in the epiphysis. Note the open epiphyseal line.13

• Fig B 6-21 Chondromyxoid fibroma. Ovoid, eccentric metaphyseal lucency with thinning of the overlying cortex and a sclerotic inner margin.

• Fig B 6-22 Intraosseous ganglion cyst. Lucent lesion with sclerotic margin (arrow) in the medial malleolus.14
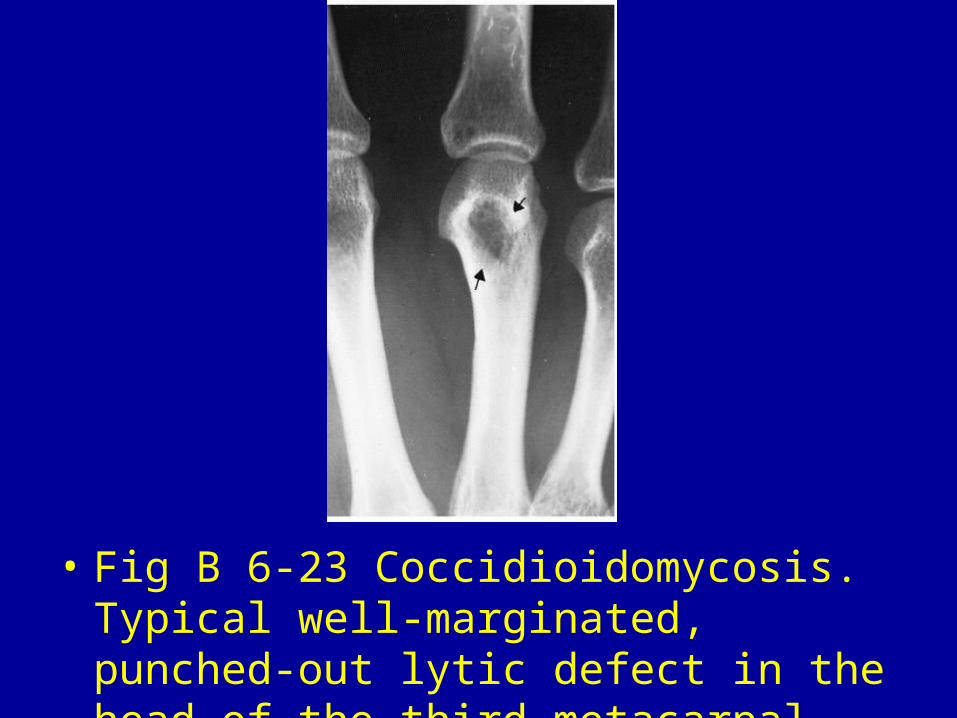
• Fig B 6-23 Coccidioidomycosis. Typical well-marginated, punched-out lytic defect in the head of the third metacarpal (arrows).15

• Fig B 6-24 Hemophilia. (A) Large subchondral cysts about the elbow. (B) Destructive, expansile lesion of the lower tibial shaft.16

• Fig B 6-25 Hemangioendothelioma. Expansile lucency containing delicate bony trabeculation.

• Fig B 6-26 Cystic angiomatosis. Lytic lesion in the proximal left humerus (arrow) with relatively well-defined lobular margins and minimal marginal sclerosis. Additional lytic lesions (arrowheads) are in the midhumeral diaphysis. Multiple lesions were seen elsewhere in the axial and proximal appendicular skeleton.17
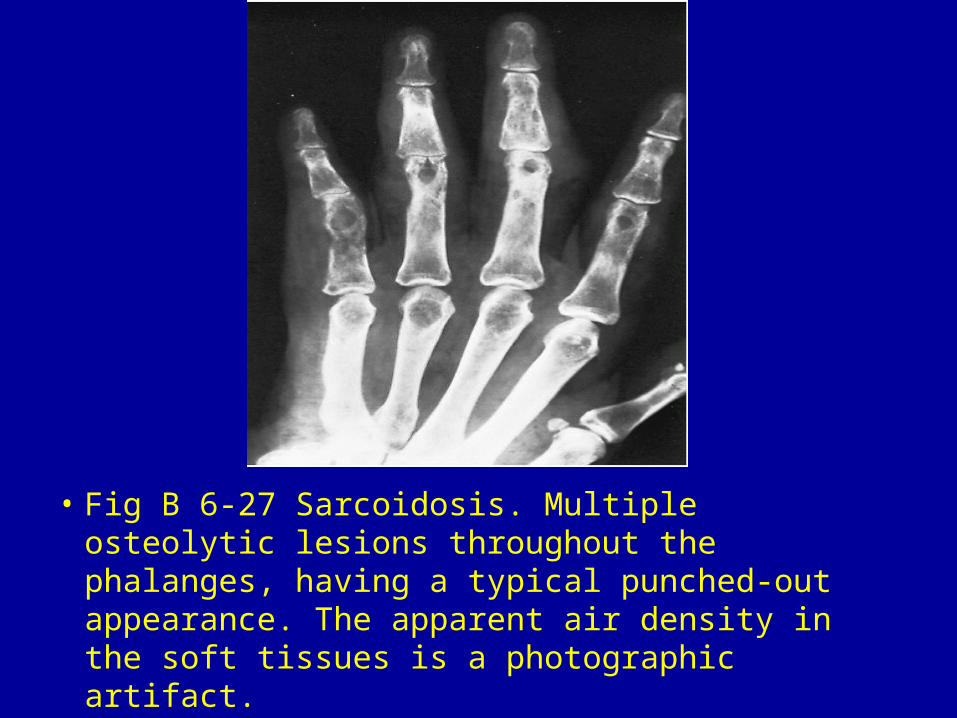
• Fig B 6-27 Sarcoidosis. Multiple osteolytic lesions throughout the phalanges, having a typical punched-out appearance. The apparent air density in the soft tissues is a photographic artifact.

• Fig B 6-28 PVNS. Large lucent lesion (arrowheads) in the proximal tibia extending to the articular surface, mimicking a giant cell tumor.14





















