
5pediatrics2.1 Neuro Exam Uerm2015b
6
MACASAET, MERCADO, NARANJA, NG UERM2015B 1 of 6 5.2.1 NEURO EXAM Jan 14, 2014 Dr. Panlilio Legend: Nelson’s/DelMundo/Adams Italic - Recording PPT/ 2015B Pedia I Trans NOTE: No trans from previous batch. This was discussed in passing and was given as a reading assignment. THE NEUROLOGIC EXAM History Taking A. History - most important component of child evaluation - Children > 3-4 years old can already contribute to their history - Obtain a comprehensive review of the function and interaction of the organ systems o CNS abnormalities may first present with symptoms of other systems B. Chief complaint - concise and should be within the developmental context. - a parent may complain that the child cannot talk yet. The seriousness of this problem depends on the child’s age, parent-child interaction, full auditory system, and intellectual level of the child. C. History of Present Illness D. Birth history – includes: - review of pregnancy, labor, delivery, and congenital disorders seen - Mother’s smoking and alcohol consumption, toxin exposure, and drug use as well. - Fetal activity in utero - Mother’s postpartum health - Birth weight, length, head circumference o Among the three, the most important reference neurologically is the head circumference - APGAR score - Sleep patterns, nature of cry and suck, general well-being E. Developmental milestones (see Appendix) - Most important component of neurologic history . Pediatric history will have a different important component. So in the quiz/exam, neurologic is changed to pediatric, developmental milestones. - Tells you whether there is a global developmental delay vs. an isolated motor delay, slow or delayed vs. loss of skill or regression. - Patterns of developmental abnormality: o Abnormality from birth – intrauterine or perinatal cause. o Abnormality of the nervous system – slow rate of skill acquisition in infancy or childhood o Degenerative disease of the CNS – loss of already acquired skills (regression) F. Family History – includes ages and well-being of all close relatives, neuro diseases (epilepsy, migraine, stroke, developmental delay), other heredofamilial disorders. - sex and age of death of miscarriages or live born siblings - postmortem examinations of dead siblings - consanguineous marriage of parents G. Social History - School performance - Personality - Social relationships Neurologic Exam Proper Observe patient: o when interacting with parents, playing, or by him/herself. o Facies, posture, gait disturbance, hemiparesis. o Attention disorders, lethargy, lack of environmental awareness Setting must be neutral and enjoyable for the child. Cooperation is essential. Assess: mental status, cognitive function, alertness, muscles power and tone, hearing, Newborn alertness: o Level depends on time of last feeding, room temperature, and the gestational age. o < 28 wks old – do not consistently demonstrate periods of alertness o Older infant –gentle physical stimulation can be applied, which will result to a brief period of alertness. o Term babies have more developed waking and sleeping patterns. A. HEAD o Size and shape Tower head/ oxycephalic - premature suture closure and is associated with various inherited craniosynostosis Broad forehead – hydrocephalus Square/box shaped skull – fluid in subdural spaces causing middle fossa enlargement -> chronic subdural hematoma Macrocephaly - o Venous pattern Marked venous distention may be due to increased ICP and/or thrombosis of the superior sagittal sinus o Fontanels – normally slightly depressed and pulsatile. Best evaluated when infant is upright. Posterior - closes at 6-8wks. - Persistence suggests underlying hydrocephalus or congenital hypothyroidism. Anterior - 2 x 2cm - Closes at 9-18months
Transcript of 5pediatrics2.1 Neuro Exam Uerm2015b
-
MACASAET, MERCADO, NARANJA, NG UERM2015B 1 of 6
5.2.1 NEURO EXAM
Jan 14, 2014 Dr. Panlilio
Legend: Nelsons/DelMundo/Adams Italic - Recording PPT/ 2015B Pedia I Trans
NOTE: No trans from previous batch. This was discussed in passing and was given as a reading assignment.
THE NEUROLOGIC EXAM
History Taking
A. History - most important component of child evaluation
- Children > 3-4 years old can already contribute to their history
- Obtain a comprehensive review of the function and interaction of the organ systems
o CNS abnormalities may first present with symptoms of other systems
B. Chief complaint - concise and should be within the developmental context.
- a parent may complain that the child cannot talk yet. The seriousness of this problem depends on the childs age, parent-child interaction, full auditory system, and intellectual level of the child.
C. History of Present Illness D. Birth history includes:
- review of pregnancy, labor, delivery, and congenital disorders seen
- Mothers smoking and alcohol consumption, toxin exposure, and drug use as well.
- Fetal activity in utero - Mothers postpartum health - Birth weight, length, head circumference
o Among the three, the most important reference neurologically is the head circumference
- APGAR score - Sleep patterns, nature of cry and suck,
general well-being E. Developmental milestones (see Appendix)
- Most important component of neurologic history. Pediatric history will have a different important component. So in the quiz/exam, neurologic is changed to pediatric, developmental milestones.
- Tells you whether there is a global developmental delay vs. an isolated motor delay, slow or delayed vs. loss of skill or regression.
- Patterns of developmental abnormality:
o Abnormality from birth intrauterine or perinatal cause.
o Abnormality of the nervous system slow rate of skill acquisition in infancy or childhood
o Degenerative disease of the CNS loss of already acquired skills (regression)
F. Family History includes ages and well-being of all close relatives, neuro diseases (epilepsy, migraine, stroke, developmental delay), other heredofamilial disorders.
- sex and age of death of miscarriages or live born siblings
- postmortem examinations of dead siblings
- consanguineous marriage of parents G. Social History
- School performance - Personality - Social relationships
Neurologic Exam Proper Observe patient:
o when interacting with parents, playing, or by him/herself.
o Facies, posture, gait disturbance, hemiparesis. o Attention disorders, lethargy, lack of
environmental awareness Setting must be neutral and enjoyable for the child.
Cooperation is essential. Assess: mental status, cognitive function, alertness,
muscles power and tone, hearing, Newborn alertness:
o Level depends on time of last feeding, room temperature, and the gestational age.
o < 28 wks old do not consistently demonstrate periods of alertness
o Older infant gentle physical stimulation can be applied, which will result to a brief period of alertness.
o Term babies have more developed waking and sleeping patterns.
A. HEAD
o Size and shape Tower head/ oxycephalic -
premature suture closure and is associated with various inherited craniosynostosis
Broad forehead hydrocephalus Square/box shaped skull fluid in
subdural spaces causing middle fossa enlargement -> chronic subdural hematoma
Macrocephaly - o Venous pattern
Marked venous distention may be due to increased ICP and/or thrombosis of the superior sagittal sinus
o Fontanels normally slightly depressed and pulsatile. Best evaluated when infant is upright.
Posterior - closes at 6-8wks. - Persistence suggests
underlying hydrocephalus or congenital hypothyroidism.
Anterior - 2 x 2cm - Closes at 9-18months
-
MACASAET, MERCADO, NARANJA, NG UERM2015B 2 of 6
- Small/absent = premature fusion = microcephaly
- Bulging = increased ICP o Sutures and skull bones
Assessed through palpation Marked overriding = underlying
brain abnormality Craniotabes softening of the
parietal bone; associated with prematurity.
o Cranial bruit Assessed through auscultation
using stethoscope diaphragm Auscultate over temporal and carotid
areas Prominent over anterior fontanel,
temporal region, orbits Normal bruit soft, symmetric,
-
MACASAET, MERCADO, NARANJA, NG UERM2015B 3 of 6
3. note deviation of eyes during turn towards the direction of rotation and on stopping quick phase nystagmus backwards (optokinetic nystagmus)
o CALORIC TEST may also be used to evaluate vestibular function. Abnormality suggests impaired brainstem function: valuable in perinatal asphyxia
VII. GLOSSOPHARYNGEAL & VAGUS (CN IX & X)
Position of uvula at rest, quality of voice, palatal movements during phonation
Gag reflex absent in 1/3 of healthy individuals; may be absent in normal babies
Swallowing and drooling Taste sensation (posterior 1/3 of tongue) An isolated lesion of CN IX is RARE
VIII. SPINAL ACCESSORY (CN XI)
Note movements of head side-to-side, shrugging and symmetry of shoulders in young children
Strength of muscles (through palpation) and against resistance in older children
Motor neuron disease, myotonic dystrophy, and myasthenia gravis are the most common conditions producing weakness and atrophy of these muscles
IX. HYPOGLOSSAL (CN XII)
Assess motility, size, shape, and presence of atrophy/fasciculations of the tongue
Bilateral injury - no tongue protrusion, + dysphagia Werdnig-Hoffmann disease - infantile spinal
muscular atrophy, or SMA type 1; presents as a floppy infant
D. MOTOR EXAM
Observe childs posture, movements when walking and running
HYPOTONIA most common abnormality of tone in neurologically compromised patients
o Slipping through armpit on vertical suspension
o Head lag on pull-to-sit (NO traction response) HYPERTONIA
o Notable resistance to passive movements on joints
o Varying degrees of posture (e.g. opisthotonus) o Fisting; buried or cortical thumbs
I. POWER/ STRENGTH Pronator sign: sensitive test for weakness; hypotonic
hand hyperpronates MUSCLE POWER
0 no muscle contraction 1 flicker or trace of contraction 2 active movement, gravity eliminated 3 active movement against gravity 4 active movement against gravity and resistance 5 normal power
Muscle power in infants and small children relies on age appropriate gross and fine motor milestones
Symmetries of movement Distal power: can be tested by evaluating the palmar
grasp Gowers sign Include muscles of respiration - observe the action of
the intercostal muscles and diaphragmatic movement
II. TONE Degree of joint/muscle resistance. Remember that it is
different from strength Muscle tone increases with age Scarf sign: when the upper extremity of a normal
term infant is pulled gently across the chest, the elbow normally does not quite reach the midsternum
o Elbow of a hypotonic infant extends beyond the midline with ease
Pull-to-sit / head control test: for infants > 4months old.
Vertical suspension (holding patient at armpits) Horizontal suspension (prone position, holding at
abdomen) 28 wks AOG extremities are still extended 32 wks AOG flexion is evident particularly in the
lower extremities First 3 months normal hypotonia 8-22 months decrease in flexor tone and increase in
extensor tone
Spasticity - Initial resistance to passive movement followed by sudden release (clasp knife phenomenon)
o Spastic lower extremities = drag legs while crawling or walking in tiptoe.
o Opisthotonos head and heels bent backward and body bent forward; evident in patients with marked spasticity.
Clonus sudden dorsiflexion of the foot with knee partially flexed.
o UMN lesion o Sustained clonus always abnormal o 5-10 beats normal clonus in newborns
unless asymmetric Rigidity constant resistance to passive movement of
both extensors and flexors o Cogwheel sensation o Does not give way unlike in spasticity o Decerebrate rigidity injury to the brainstem
at the level of the superior colliculi = marked extension of extremities
III. MOTILITY AND LOCOMOTION < 32 wks AOG random, slow, writhing movements
interspersed with rapid, myoclonic-like activity of the extremities.
> 32 wks AOG flexion is the primary motor activity Ataxia incoordination of movement/ balance.
o Truncal ataxia unsteadiness during sitting or standing; cerebellar vermis lesion
o Intention tremor cerebellar hemispheres
IV. REFLEXES Table 2. Primitive Reflexes
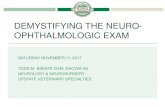
Normal Neurologic Development
Fig. 1. Development of dendrites. Upper row, left to right: 1 month premature
(8 months gestation); newborn at term; 1 month; 3 months; and 6 months.
Lower row, left to right: 15 months; 2 years; 4 years; 6 years. Full dendritic
development: 2-3 years.
-
MACASAET, MERCADO, NARANJA, NG UERM2015B 4 of 6
Myelogenetic chronology (please see Appendix) parallel index of development and maturation of the nervous system and is apparently related to the functional activity of the fiber systems.
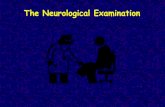
Fig. 2. Organ growth curves. From 0-2 years, brain development is at maximum then goes into plateau. The lymphoid organs peak between 5-10 years, thats why tonsillitis is most common at this time.
Soft Neurologic Signs Abnormal performance on a motor or sensory test that is
not age appropriate Persistence of these signs indicate close follow up of the
child Neurologic dysfunction presence and persistence of two
or more soft neurologic signs (attention deficit disorder, learning problem, or cerebral palsy)
Always correlate with age as there are, for example, some movements abnormal for a 7 y/o but normal for a 4 y/o.
Non-localizable and age-dependent Cut-off age for most is at 6 years Persistence is generally considered abnormal MOST COMMON are the following:
o Choreiform movements o Jerky ocular pursuit o Motor impersistence o Reflex asymmetry o Gross and fine motor incoordination o Right/left disorientation o Inability to distinguish double tactile
stimulation o Synkinesia (disappears by 9 years)
-
MACASAET, MERCADO, NARANJA, NG UERM2015B 5 of 6
APPENDIX
Screening Scheme for Developmental Delay: Upper Range
Guidelines with regard to the upper range of normal skills that are usually recalled by the parents and that, if not present, should alert the physician.
AGE
(months)
GROSS MOTOR FINE MOTOR SOCIAL SKILLS LANGUAGE
3 Supports weight on
forearms
Opens hands
spontaneously
Smiles appropriately Coos, laughs
6 Sits momentarily Transfers objects Shows likes/dislikes Babbles
9 Pulls to stand Pincer grasp Plays pat-a-cake, peek-
a-boo
Imitates sound
12 Walks with one hand
held
Releases an object on
command
Comes when called 1-2 meaningful
words
18 Walks upstairs with
assistance
Feeds from a spoon Mimics actions of
others
At least 6 words
24 Runs Builds tower of 6 blocks Plays with others 2-3 word sentences
MYELOGENETIC CHRONOLOGY
-
MACASAET, MERCADO, NARANJA, NG UERM2015B 6 of 6
SUMMARY OF DEVELOPMENTAL MILESTONES










![Neuro Assessment for Scalp the Non-Neuro Nurse … · Neuro Assessment for the Non-Neuro Nurse Terry M. Foster, RN, ... Microsoft PowerPoint - Neuro Grand Forks ND [Read-Only] Author:](https://static.fdocuments.in/doc/165x107/5b88746b7f8b9a301e8d8c76/neuro-assessment-for-scalp-the-non-neuro-nurse-neuro-assessment-for-the-non-neuro.jpg)




![2015 AOA Neuro-Imaging.ppt [Read-Only]OF NEURO-IMAGING Presented by Kelly A. Malloy, OD ... indicative of meningioma ... 84 year – old woman Previous Dx of ARMD OU EXAM RESULTS VA:](https://static.fdocuments.in/doc/165x107/5e3318a39e695f0df717c0d3/2015-aoa-neuro-read-only-of-neuro-imaging-presented-by-kelly-a-malloy-od-.jpg)