59-291 Section 3, Lecture 7 Drugs for...
16
1 Drugs for Hyperlipidemia • Lipids are necessary for human life • Cholesterol – Essential component of cell membrane – Precursor to the sterol and steroid compounds • Triglycerides (TG) – Composed of 3 fatty acids and glycerol – Main storage form of fuel, generate high-energy compound such as ATP, that provides energy for muscle contraction and metabolic reactions 59-291 Section 3, Lecture 7
Transcript of 59-291 Section 3, Lecture 7 Drugs for...
1
Drugs for Hyperlipidemia
• Lipids are necessary for human life• Cholesterol
– Essential component of cell membrane– Precursor to the sterol and steroid compounds
• Triglycerides (TG)– Composed of 3 fatty acids and glycerol– Main storage form of fuel, generate high-energy
compound such as ATP, that provides energyfor muscle contraction and metabolic reactions
59-291 Section 3, Lecture 7
2
HyperlipidemiaHyperlipoproteinemia
• Increases concentrations of lipids andlipoproteins
• Hypercholesterolemia; high concentrationof cholesterol– Atherosclerosis and coronary artery disease
• Hypertriglyceridemia; high concentration oftriglyceride– Pancreatitis– Development of atherosclerosis and heart
disease
3
Coronary Heart Disease (CHD)• The main cause of premature death in
industrialized countries• Modifiable risk factors
– Hypertension– Cigarette smoking– Low high density lipoprotein (HDL) <40 mg/dl
• Unmodifiable risk factors– Male gender– Family history of premature CHD; CHD in
first-degree male relative <55, female <65– Advance age; Men>45, Women >55

4
Progression of CHD Damage toendothelium andinvasion ofmacrophages
Smooth musclemigration
Cholesterolaccumulatesaroundmacrophage andmuscle cells
Collagen andelastic fibersform a matrixaround thecholesterol,macrophagesand musclecells
5
Lipoproteins and Lipid transport• Lipids are insoluble in plasma and must be
transported• Lipoproteins are distinguished according
to their buoyant density, lipid and proteincomposition, role in lipid transport andassociation with apoproteins
• Chylomicrons• Very Low-Density Lipoproteins (VLDL)• Low- Density Lipoproteins (LDL)• High Density Lipoproteins (HDL)
6
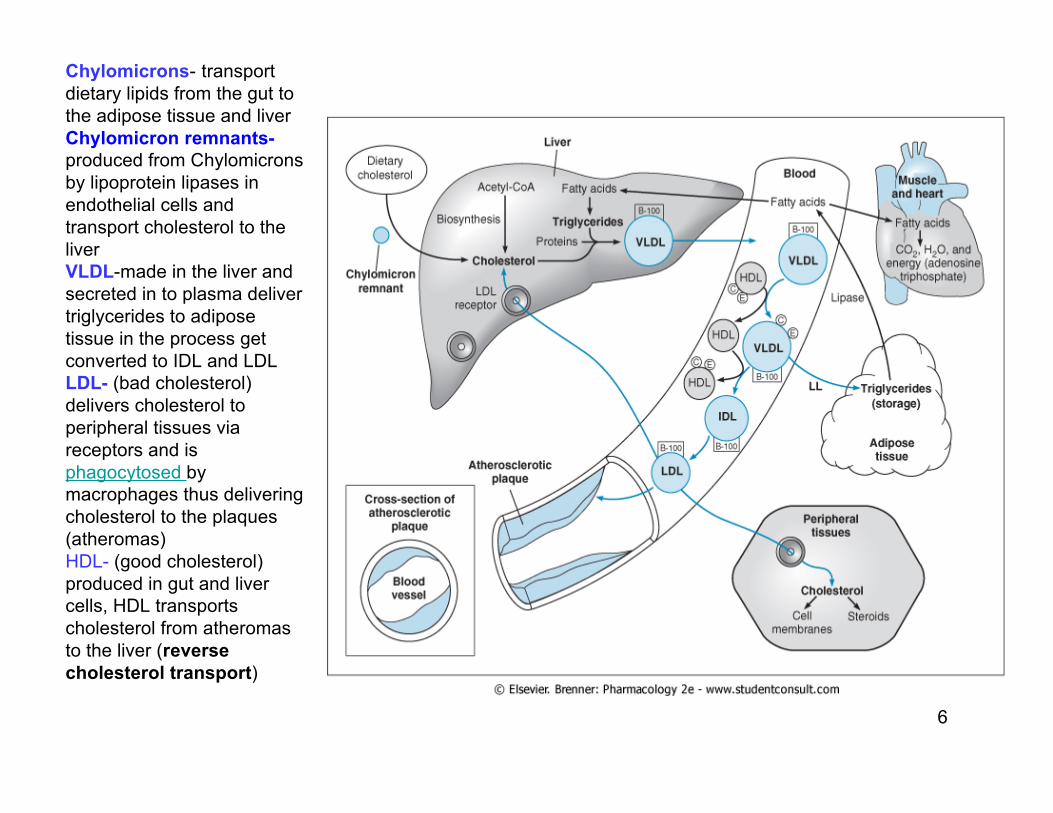
Chylomicrons- transportdietary lipids from the gut tothe adipose tissue and liverChylomicron remnants-produced from Chylomicronsby lipoprotein lipases inendothelial cells andtransport cholesterol to theliverVLDL-made in the liver andsecreted in to plasma delivertriglycerides to adiposetissue in the process getconverted to IDL and LDLLDL- (bad cholesterol)delivers cholesterol toperipheral tissues viareceptors and isphagocytosed bymacrophages thus deliveringcholesterol to the plaques(atheromas)HDL- (good cholesterol)produced in gut and livercells, HDL transportscholesterol from atheromasto the liver (reversecholesterol transport)
7
Causes and Types ofHyperlipoproteinemia
• Genetics and environmental factors• Increase the formation or reduce the
clearance of LP from circulation• Factors
– Biochemical defects in LP metabolism– Excessive dietary intake of lipids– Endocrine abnormality– Use of drugs that perturb LP formation or
catabolism
8
Primary Hyperlipoproteinemia• Caused by a monogenic defect (a specific
defect at a single gene)• LDL cholesterol levels are severely high
– Deficiency of LDL receptors– Defect in the structure of apoprotien B
• LDL receptors do not recognize LDL, LDL remainsin circulation
• VLDL and TG levels are severely high– Lipoprotein lipase deficiency
• Prevents delivery of TG to adipose tissue
9
• Polygenic-environmental hyperlipidemia– Milder forms of hyperlipidemia– Influence of several genes– Excessive of dietary intake– More common than primary form– Responsible for most cases of accelerated
atherosclerosis• Secondary hyperlipidemia
– Alcoholism– Diabetes melitus– Uremia– Drugs; β blockers, oral contraceptives, thiazide
diuretics– Diseases: hypothyroidism, nephrotic syndrome,
obstructive liver disease
10
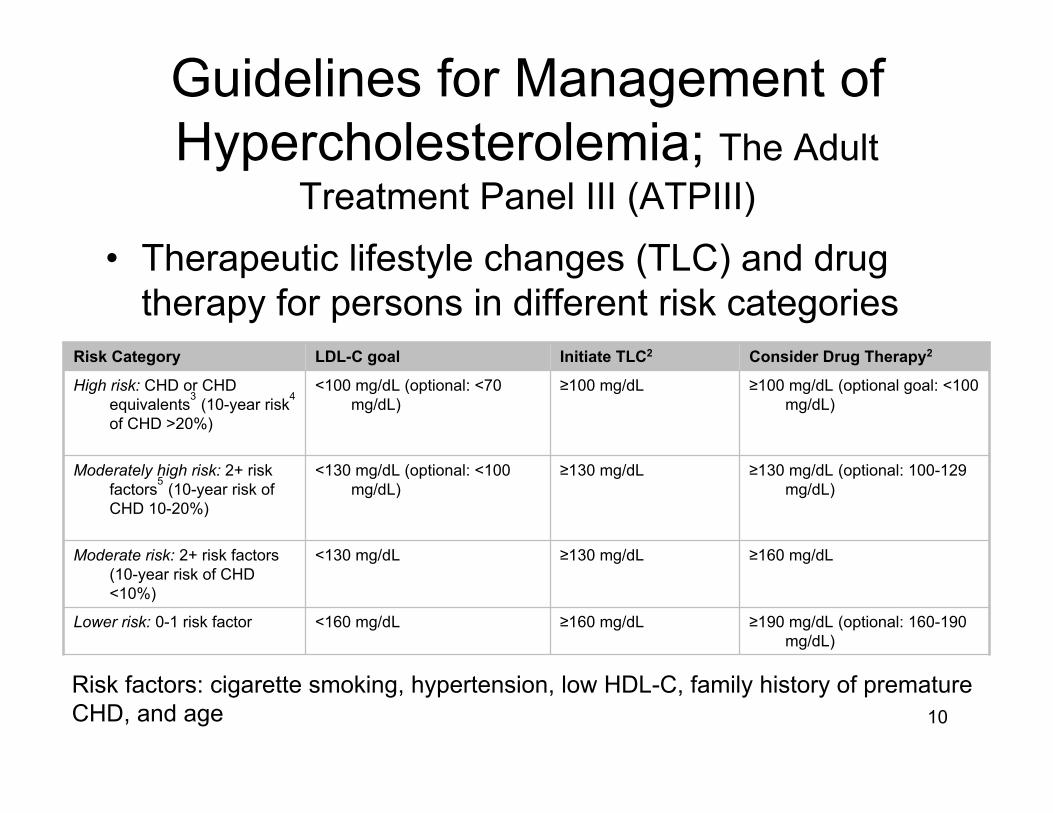
Guidelines for Management ofHypercholesterolemia; The Adult
Treatment Panel III (ATPIII)• Therapeutic lifestyle changes (TLC) and drug
therapy for persons in different risk categories
≥190 mg/dL (optional: 160-190mg/dL)
≥160 mg/dL<160 mg/dLLower risk: 0-1 risk factor
≥160 mg/dL≥130 mg/dL<130 mg/dLModerate risk: 2+ risk factors(10-year risk of CHD<10%)
≥130 mg/dL (optional: 100-129mg/dL)
≥130 mg/dL<130 mg/dL (optional: <100mg/dL)
Moderately high risk: 2+ riskfactors5 (10-year risk ofCHD 10-20%)
≥100 mg/dL (optional goal: <100mg/dL)
≥100 mg/dL<100 mg/dL (optional: <70mg/dL)
High risk: CHD or CHDequivalents3 (10-year risk4
of CHD >20%)
Consider Drug Therapy2Initiate TLC2LDL-C goalRisk Category
Risk factors: cigarette smoking, hypertension, low HDL-C, family history of prematureCHD, and age
11
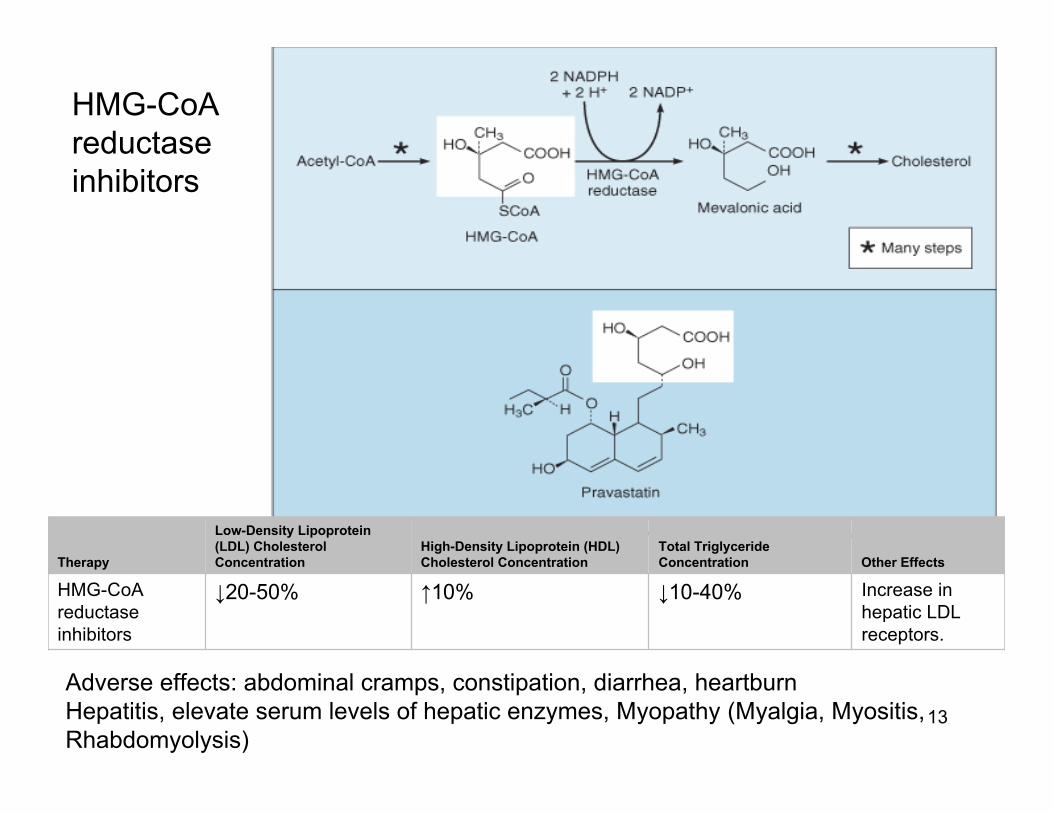
• Drugs for hypercholesterolemia– 3-hydroxy-3- methyglutaryl Co A (HMG-CoA)
reductase inhibitor– Bile acid-binding resin– Ezetimibe
• Drugs for reducing elevated TG and toraise HDL-C levels– Fibric acid derivatives– niacin
12
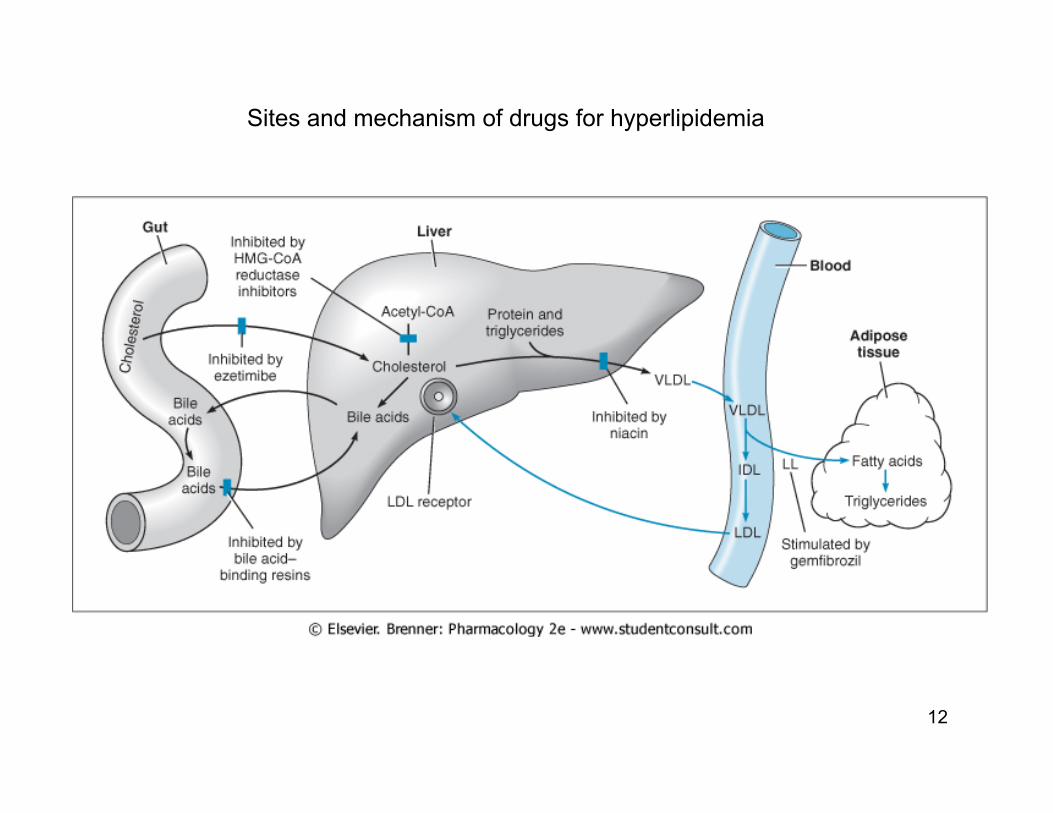
Sites and mechanism of drugs for hyperlipidemia
13
Other EffectsTotal TriglycerideConcentration
High-Density Lipoprotein (HDL)Cholesterol Concentration
Low-Density Lipoprotein(LDL) CholesterolConcentrationTherapy
Increase inhepatic LDLreceptors.
↓10-40%↑10%↓20-50%HMG-CoAreductaseinhibitors
Adverse effects: abdominal cramps, constipation, diarrhea, heartburnHepatitis, elevate serum levels of hepatic enzymes, Myopathy (Myalgia, Myositis,Rhabdomyolysis)
HMG-CoAreductaseinhibitors
14
Bile Acid-Binding Resins• Moderately effective with excellent safety record• Large MW polymers containing Cl-• Resin binds to bile acids and the acid-resin
complex is excreted– prevents enterohepatic cycling of bile acids– obligates the liver to synthesize replacement bile
acids from cholesterol• The liver increases the number of LDL receptors
to obtain more cholesterol• The levels of LDL-C in the serum are reduced as
more cholesterol is delivered to the liver• Little effect on levels of HDL-C and TG• Excellent choice for people that cannot tolerate
other types of drugs
15
Adverse effects
• GI side effects, constipation and fecalimpaction, which can be prevented byincreased water consumption, analirritation and skin rash
• Bind to digoxin, varfarin, thyroxin; takeresins 2 h before or after taking othermedicines
16
Practice Questions
• List 4 risk factors associated with CHD• Cigarette smoking• Low HDL-C• Hypertension• Family history of premature CHD• Age