545 Pembroke Street W. Pembroke, ON Canada Child Care and ... · an Individual Program Plan in...
7
INTEGRATION SERVICES REFERRAL AND INTAKE PROCESS The County of Renfrew Child Care and Early Years Integration Services offers support to child care agencies for children who have displayed difficulties in one or more developmental areas (such as cognitive. physical, behavioural, social/emotional etc.). Once referred, the child will be placed on the caseload of an Integration Coordinator, who will hold a Team Meeting with the parent/guardians, child care staff and any other individuals involved, to discuss the child’s strengths, needs, and to develop goals within the program. The Integration Coordinator will then complete routine visits and consultations with staff to provide recommendations based on the goals developed at the Team Meeting, as well as the needs observed within the program. The Integration Coordinator will complete an Individual Program Plan in conjunction with the Consulting Psychologist to outline specific methodology in order to achieve the goals set by the family and child care staff. Additional supports provided by Integration Services may be in the form of an environmental assessment, providing resource materials, providing enhanced staffing to the program, or training/workshops for staff. These supports will be determined by the Integration Coordinator based on observations, needs assessments, data collection, and other supporting documentation once the child is in attendance at the Child Care Program. Referral Process: 1. Discuss concerns with the child’s parent/guardian. 2. Discuss the services provided through Integration Services with the parent/guardian. 3. Complete Integration Services Referral & Intake Package with the parent/guardian. Consent to Disclose and Verify Information is required to share information with outside agencies including the Child Care Program. The Referral and Intake Package must be completed and reviewed with the parent/guardian to ensure accuracy and that they are fully aware of all information documented and shared. Please do not send this package home with the parent/guardian to complete. 4. Fax or mail the completed consent and referral form to: Integration Services County of Renfrew Child Care and Early Years Division 545 Pembroke Street West Pembroke ON K8A 5P2 Fax: 613-732-4437 The Integration Coordinator assigned to the file will review the referral form to ensure that all necessary information is completed prior to being placed on Integration Service’s caseload. The Integration Coordinator will then contact the family, Child Care Centre, and outside agencies in order to obtain additional information and to schedule a Team Meeting. Department of Social Services Child Care and Early Years Division 545 Pembroke Street W. Pembroke, ON Canada K8A 5P2 Phone: 613-732-4100 Fax: 613-732-4437 www.countyofrenfrew.on.ca
Transcript of 545 Pembroke Street W. Pembroke, ON Canada Child Care and ... · an Individual Program Plan in...

INTEGRATION SERVICES REFERRAL AND INTAKE PROCESS
The County of Renfrew Child Care and Early Years Integration Services offers support to child care agencies for children who have displayed difficulties in one or more developmental areas (such as cognitive. physical, behavioural, social/emotional etc.).
Once referred, the child will be placed on the caseload of an Integration Coordinator, who will hold a Team Meeting with the parent/guardians, child care staff and any other individuals involved, to discuss the child’s strengths, needs, and to develop goals within the program. The Integration Coordinator will then complete routine visits and consultations with staff to provide recommendations based on the goals developed at the Team Meeting, as well as the needs observed within the program. The Integration Coordinator will complete an Individual Program Plan in conjunction with the Consulting Psychologist to outline specific methodology in order to achieve the goals set by the family and child care staff.
Additional supports provided by Integration Services may be in the form of an environmental assessment, providing resource materials, providing enhanced staffing to the program, or training/workshops for staff. These supports will be determined by the Integration Coordinator based on observations, needs assessments, data collection, and other supporting documentation once the child is in attendance at the Child Care Program.
Referral Process: 1. Discuss concerns with the child’s parent/guardian.2. Discuss the services provided through Integration Services with the parent/guardian.3. Complete Integration Services Referral & Intake Package with the parent/guardian.
Consent to Disclose and Verify Information is required to share information with outsideagencies including the Child Care Program.
The Referral and Intake Package must be completed and reviewed with the parent/guardianto ensure accuracy and that they are fully aware of all information documented and shared.Please do not send this package home with the parent/guardian to complete.
4. Fax or mail the completed consent and referral form to:Integration ServicesCounty of Renfrew Child Care and Early Years Division545 Pembroke Street WestPembroke ON K8A 5P2Fax: 613-732-4437
The Integration Coordinator assigned to the file will review the referral form to ensure that all necessary information is completed prior to being placed on Integration Service’s caseload. The Integration Coordinator will then contact the family, Child Care Centre, and outside agencies in order to obtain additional information and to schedule a Team Meeting.
Department of Social Services Child Care and Early Years
Division
545 Pembroke Street W. Pembroke, ON Canada
K8A 5P2 Phone: 613-732-4100
Fax: 613-732-4437 www.countyofrenfrew.on.ca

Integration Services Consent to Disclose and Verify Information
1. I/We,
Full name of applicant / recipient Name of spouse / same-sex partner Name of child Date of Birth
consent to the collection of information by, and the release of information to, an authorized representative of the Corporation of the County of Renfrew Child Care and Early Years Division for the purpose of planning for the integration of my/our dependent child or child in my/our care who I/we am/are the legal guardian of, in a licensed Child Care or Nursery School Program.
2. I/We consent to the information being exchanged with agencies checked off in the following list in order
to verify information for the purpose of determining or verifying my/our initial and ongoing eligibility for services provided by the County of Renfrew Child Care and Early Years Integration Services.
Renfrew County & District Health Unit Family & Children’s Services Renfrew County Developmental Services Community Care Access Centre Preschool Speech and Language The Phoenix Centre Ottawa Children’s Treatment Centre
Infant Hearing Program Blind Low-Vision Program Renfrew County District School Board Renfrew County Roman Catholic School Board French Public School Board French Catholic School Board
Licensed Day Care / Nursery School Program: Other Professional – i.e. speech pathologist, doctor: 3. I understand that Integration Services and Fee Subsidy are programs offered through the Child Care and Early Years Division and information is shared between these programs when necessary. (Initial) ________ 4. I/We further consent to the use of the following email address __________________________________________
for the purpose of communication regarding my child, newsletters and/or other pertinent information. (Initial) ______ I have read or had read to me and understand the consent set out above. Signature / mark of applicant/recipient or person applying Date on behalf of applicant/recipient I have read or had read to me and understand the consent set out above and I join in this consent. Signature / mark of applicant/recipient or person applying Date on behalf of applicant/recipient
545 Pembroke Street W.
Pembroke, ON Canada K8A 5P2
Phone: 613-732-4100
Fax: 613-732-4437 www.countyofrenfrew.on.ca
Department of Social Services Child Care and Early Years
Division
This consent will be in effect from the date of signature until the applicant/recipient is released from the program or County of Renfrew Child Care and Early Years Integration Services has received written notice from the applicant/recipient or person applying on behalf of the applicant/recipient.

Integration Services Referral Form
Note: as per Ministry Guidelines the child must be diagnosed with a physical, emotional or cognitive impairment that is likely to continue for a prolonged period of time as verified by
objective psychological or medical findings.
Child’s Name: Child’s Date of Birth:(dd/mmm/yyyy)
Diagnosis:
Parent/Guardian Name:
Complete Mailing Address: Postal Code:
Phone Number (home): Phone Number (work): Other:
Email:
Agency Referring:
Agency Contact (name, address and phone):
Child Care Program:
Group (e.g. Toddler, Preschool):
Currently attending
Waiting for vacancy
Attendance: Days: M T W T F # Hours / week:
Agencies presently involved or on wait list for services:
Agency Name Contact Name Involved Waitlist
Date of Referral: Signature of Referring Agency Contact:
Date: Signature of Parent/Guardian:
545 PEMBROKE STREET W. PEMBROKE, ON CANADA
K8A 5P2 PHONE: 613-732-4100
FAX: 613-732-4437 WWW.COUNTYOFRENFREW.ON.CA
Department of Social Services Child Care and Early Years
Division

Please fill out the following information as accurately as possible. It is extremely important and necessary to be used as documentation of potential areas of concern. Once you have completed this form and returned it to Child Care and Early Years Integration Services, the Integration Coordinator can continue with the next step in the process of supporting you and the Program in the appropriate manner.
1. Birth History
Full Term Premature Were there any concerns with the baby’s health after birth? No Yes, please explain: __________________________________________________________________________________________
________________________________________________________________________________________
Additional Comments: __________________________________________________________________________________________
__________________________________________________________________________________________
_______________________________________________________________________________________
2. Medical History
Family Doctor: _____________________________ Paediatrician______________________________ Specialist(s): _______________________________ Other Practitioners (ie: naturopath): _______________________________ _________________________________________ _______________________________ _________________________________________ Does your child have asthma? No Yes, Please describe: _______________________________________ Does your child have allergies? No Yes, Please describe: _______________________________________ Has your child’s vision been tested? No Yes, Child’s age at exam: ________________________________ Has your child’s hearing been tested since birth? No Yes, Child’s age at exam: ______________________ Has your child had recurring ear infections? No Yes, Please describe: _____________________________ Has your child seen an Ear, Nose and Throat doctor? No Yes Does your child have tubes in his/her ears? No Yes Does your child have a history of feeding difficulties (ie. Difficulty breast/bottle feeding, growth/weight concerns, transitioning to solids, managing textures, gagging, choking, overstuffing mouth, feeding equipment) No Yes, Please describe: __________________________________________________________________________________________
________________________________________________________________________________________
Does your child have a history of sleeping difficulties? (ie: falling asleep, waking often, apnea, snoring) No Yes, Please describe: __________________________________________________________________________________________
________________________________________________________________________________________
Has your child been hospitalized or had any surgeries since birth? No Yes, Please describe:
__________________________________________________________________________________________
________________________________________________________________________________________
Does your child require ongoing medication? No Yes, Please describe: ____________________________
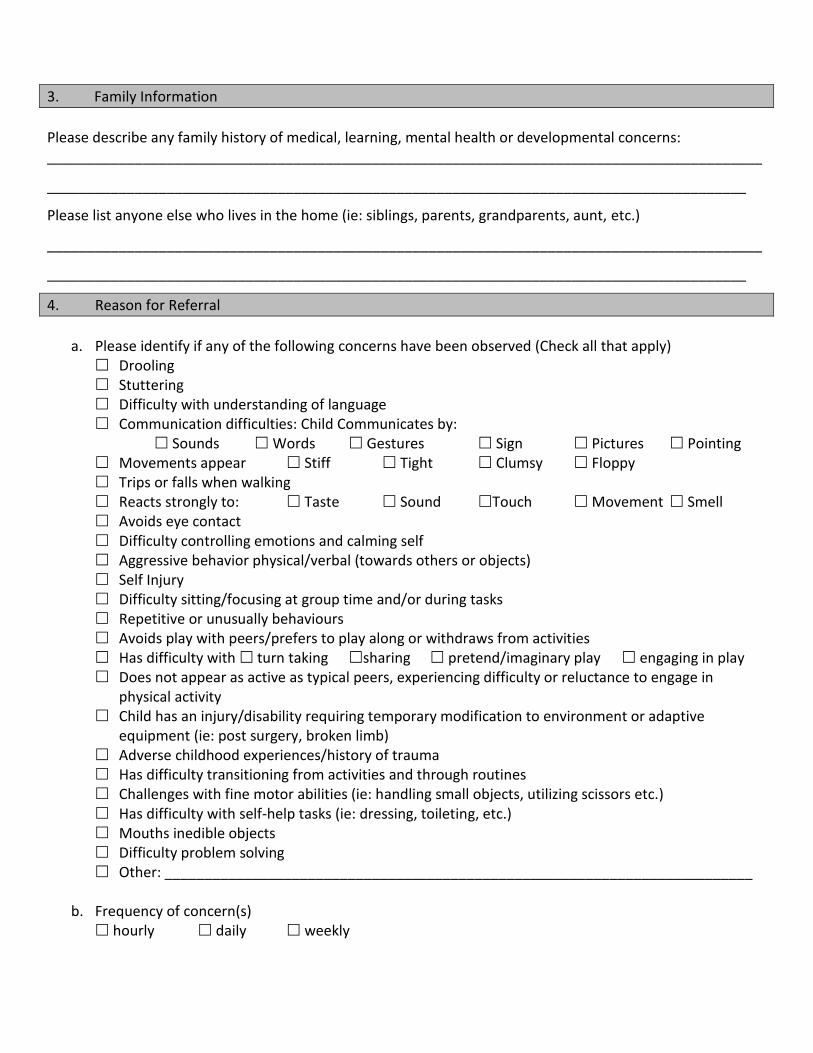
3. Family Information
Please describe any family history of medical, learning, mental health or developmental concerns: __________________________________________________________________________________________
________________________________________________________________________________________
Please list anyone else who lives in the home (ie: siblings, parents, grandparents, aunt, etc.)
__________________________________________________________________________________________
________________________________________________________________________________________
4. Reason for Referral
a. Please identify if any of the following concerns have been observed (Check all that apply) Drooling Stuttering Difficulty with understanding of language Communication difficulties: Child Communicates by:
Sounds Words Gestures Sign Pictures Pointing Movements appear Stiff Tight Clumsy Floppy Trips or falls when walking Reacts strongly to: Taste Sound Touch Movement Smell Avoids eye contact Difficulty controlling emotions and calming self Aggressive behavior physical/verbal (towards others or objects) Self Injury Difficulty sitting/focusing at group time and/or during tasks Repetitive or unusually behaviours Avoids play with peers/prefers to play along or withdraws from activities Has difficulty with turn taking sharing pretend/imaginary play engaging in play Does not appear as active as typical peers, experiencing difficulty or reluctance to engage in
physical activity Child has an injury/disability requiring temporary modification to environment or adaptive
equipment (ie: post surgery, broken limb) Adverse childhood experiences/history of trauma Has difficulty transitioning from activities and through routines Challenges with fine motor abilities (ie: handling small objects, utilizing scissors etc.) Has difficulty with self-help tasks (ie: dressing, toileting, etc.) Mouths inedible objects Difficulty problem solving Other: __________________________________________________________________________
b. Frequency of concern(s) hourly daily weekly

c. Environment: Where does the concern occur? circle snack/meal small group large group outdoors transition nap/rest time craft time play time other (please explain) ____________________________________________________________________________________
__________________________________________________________________________________
d. What strategies or adaptations have you made or tried? physical space structures equipment communication material sensory materials program transitions routine Please explain in detail:________________________________________________________________
___________________________________________________________________________________
5. Additional Information
Has your child has a private assessment for: Speech Physiotherapy Occupational Therapy Other: ___________________________
Name of therapist and date of assessment:______________________________________________________ (Please attach a copy of any assessments/reports completed to date.) Additional comments/concerns (to be completed by the parent/guardian) _________________________________________________________________________________________
_________________________________________________________________________________________
Additional comments/concerns (to be completed by the referral source) _________________________________________________________________________________________
_________________________________________________________________________________________
Have you received a signed Consent to Disclose and Verify Information for involvement of Child Care Integration Services? (If you require a blank copy, please inquire with the Integration Coordinator) Yes No I have read or had read to me and understand the consent set out above. ________________________________________________ ___________________________________ Signature/mark of applicant/recipient or person applying Date on behalf of applicant/recipient I have read or had read to me and understand the consent set out above and I join in this consent. ________________________________________________ ___________________________________ Signature/mark of applicant/recipient or person applying Date on behalf of applicant/recipient

Please fax or mail this form to:
Integration Services County of Renfrew Child Care and Early Years Division
545 Pembroke Street West Pembroke Ontario K8A5P2
Fax: 613-732-4437
Questions can be directed to: Integration Services 613-732-4100
Toll free: 1-866-561-7679 Email: [email protected]