51. Steal Phenomenon in Nerve Transfer: An … · Parry Romberg's Disease is an enigmatic...
31
ASRM SCIENTIFIC PAPER PRESENTATIONS: BASIC SCIENCE & OUTCOME STUDIES IN RESEARCH Monday, January 16, 2017, 7:30am – 9:15am 51. Steal Phenomenon in Nerve Transfer: An Experimental Rat Study Chang Gung Memorial Hospital, Kweishan, 256, Taiwan Johnny Chuieng - Yi Lu, M.D. 1 ; Aleksandra McGrath, M.D., P.H.D. 2 ; Frank Fang, MD 1 ; Tommy Nai-Jen Chang, M.D. 1 ; David Chwei-Chin Chuang, MD 1 ; (1)Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, Chang Gung Medical College and Chang Gung University, Taoyuan, Taiwan, (2)Chang Gung Memorial Hospital, Kweishan, Taiwan Background: In total root avulsion injuries of the brachial plexus, where donor nerves are scarce, using one donor nerve to simultaneously neurotize multiple targets can be common. Clinically we noticed that one donor nerve (CC7T = contralateral C7 transfer) to multiple targets (median and musculocutaneous nerves) shows poorer results than when one donor to one target individually. We suspect that steal phenomenon exists in nerve transfers and have designed an experimental rat model for study. Material and Methods: Fourty Sprague-Dawley rats, weighing 250 to 300 g were operated where the rat's left brachial plexus was used as the experimental site. The rats were divided into three groups based on the different methods of nerve transfers. The donor neurotizer was the ulnar nerve (UN), and the two targets intended for transfer include musculocutaneous nerve (MCN) and median nerve (MN). (Figure 1) Control MCN and MN untouched Group A UN transfer to MCN (one target) Group B UN transfer to MN (one target) Group C UN transfer to MCN and MN (two targets) The muscle weight, muscle action potential and tetanic contraction forces are measured, while the final axon counts of the involved nerves are also included. Results: When comparing the results of coapting to one target or two targets, there are no significant differences in target muscle potential or contraction force (Figure 2 and 3). However, there is a significant drop in muscle weight for both the biceps and flexor muscles (Figure 4). These findings show that one source coapting to two targets can still work, but the significant drop in muscle weight proves there is “subclinical difference”. In addition, coapting to two target
Transcript of 51. Steal Phenomenon in Nerve Transfer: An … · Parry Romberg's Disease is an enigmatic...

ASRM SCIENTIFIC PAPER PRESENTATIONS: BASIC SCIENCE & OUTCOME STUDIES IN RESEARCH
Monday, January 16, 2017, 7:30am – 9:15am
51. Steal Phenomenon in Nerve Transfer: An Experimental Rat Study Chang Gung Memorial Hospital, Kweishan, 256, Taiwan Johnny Chuieng - Yi Lu, M.D.1; Aleksandra McGrath, M.D., P.H.D.2; Frank Fang, MD1; Tommy Nai-Jen Chang, M.D.1; David Chwei-Chin Chuang, MD1; (1)Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, Chang Gung Medical College and Chang Gung University, Taoyuan, Taiwan, (2)Chang Gung Memorial Hospital, Kweishan, Taiwan Background: In total root avulsion injuries of the brachial plexus, where donor nerves are scarce, using one donor nerve to simultaneously neurotize multiple targets can be common. Clinically we noticed that one donor nerve (CC7T = contralateral C7 transfer) to multiple targets (median and musculocutaneous nerves) shows poorer results than when one donor to one target individually. We suspect that steal phenomenon exists in nerve transfers and have designed an experimental rat model for study. Material and Methods: Fourty Sprague-Dawley rats, weighing 250 to 300 g were operated where the rat's left brachial plexus was used as the experimental site. The rats were divided into three groups based on the different methods of nerve transfers. The donor neurotizer was the ulnar nerve (UN), and the two targets intended for transfer include musculocutaneous nerve (MCN) and median nerve (MN). (Figure 1) Control MCN and MN untouched Group A UN transfer to MCN (one target) Group B UN transfer to MN (one target) Group C UN transfer to MCN and MN (two targets) The muscle weight, muscle action potential and tetanic contraction forces are measured, while the final axon counts of the involved nerves are also included. Results: When comparing the results of coapting to one target or two targets, there are no significant differences in target muscle potential or contraction force (Figure 2 and 3). However, there is a significant drop in muscle weight for both the biceps and flexor muscles (Figure 4). These findings show that one source coapting to two targets can still work, but the significant drop in muscle weight proves there is “subclinical difference”. In addition, coapting to two target

nerves has a more detrimental effect on the distal muscles function, while the proximal muscles attracted less axons (Figure 5 and 6). Conclusions: The results of this study indicate that steal phenomenon does occur in nerve transfer, and when one source nerve coapts to two target nerves simultaneously, there is a more detrimental effect on the distal muscle group than the proximal muscle group. In summary, it is better to have one source nerve innervate one target nerve in nerve transfer even in total root avulsion injuries, where it is more important to have one much improved function than have poorer results for two functions.
Figure 1
Figure 2

Figure 3

Figure 4
Figure 5

Figure 6

52. Microsurgical Reanastomosis of Utero-Ovarian Vessels Providing Sole Vascular Supply of Baboon Uterine Angiosome with Retention of Fertility Cleveland Clinic Florida, Weston, 199, USA Benjamin D Beran, M.D.1; Katrin Arnolds, M.D.1; Marie Shockley, M.D.1; Miguel Medina III, M.D.1; Krishna Rivas, D.V.M.2; Michael L. Sprague, M.D.1; Pedro Escobar, M.D.3; Andreas Tzakis, M.D.1; Tommaso Falcone, M.D.4; Stephen Zimberg, M.D.1; (1)Cleveland Clinic Florida, Weston, FL, (2)Mannheimer Foundation, Homestead, FL, (3)University of Texas MD Anderson Cancer Center, Houston, TX, (4)Cleveland Clinic, Cleveland, OH OBJECTIVE: To determine uterine and ovarian viability, while retaining spontaneous fertility potential, following alteration of the uterine angiosome in a baboon model. Our model received vascular supply only via utero-ovarian vessels with microsurgical anastomosis. DESIGN: Prospective observational trial of uterine and ovarian viability and resultant fertility in Papio hamadryas baboons with surgically-altered uterine perfusion. This data represents the third step of a step-wise protocol. The initial step involved ligation of bilateral uterine veins and the second step involved ligation of bilateral uterine arteries and veins while monitoring similar outcomes. METHODS: Three naïve female baboons underwent laparotomy to alter uterine perfusion. Bilateral uterine arteries and veins were surgically ligated. A circumferential colpotomy was made and repaired with absorbable barbed suture. Ipsilateral utero-ovarian artery and vein were identified, divided, and then re-anastomosed end-to-end using microsurgery. The same technique was then performed on the opposite side. The fallopian tubes were not altered. Intra-operative perfusion of the uterus was documented with near-infrared perfusion angiography. Resumption of menstrual blood flow, presence of uterus on transabdominal sonogram, and cervical biopsies performed 6-10 weeks post-laparotomy determined viability of the uterus. Cyclical changes of the sex skin demonstrated continued ovarian function. The females were released to the breeding colony and daily monitoring of sex skin turgescence was continued. Cessation of cycling suggested pregnancy and pregnancies were confirmed by transabdominal sonography. RESULTS: All surgeries occurred without incident, and near-infrared perfusion angiography confirmed intra-operative uterine perfusion after completion of microvascular anastomoses. One baboon acquired cellulitis of the skin incision which resolved with antibiotics. Trans-abdominal ultrasound confirmed presence of uterus in all animals 6-10 weeks after surgery, and simultaneous cervical biopsies verified normal cervical tissue. Within the first 60 days post-laparotomy, all animals demonstrated at least one menstrual bleed, and cyclical pattern of sex-skin changes in accordance with normal baboon physiology. Within 3-6 months of surgery, during routine semi-annual colony assessment, two of the three baboons had ongoing viable pregnancies, while the third demonstrated normal menstrual cycling and breeding behaviors.

CONCLUSIONS: Surgical alteration of the uterine angiosome with bilateral microsurgical anastomoses of the utero-ovarian vessels, in the absence of the uterine arteries and veins and cervico-vaginal vessel branches, sufficiently perfused the uterus and ovaries for viability and spontaneous fertility. This technique shows promise for application in future human uterine transplantation, which currently involves meticulous uterine artery and vein dissection without microsurgical re-anastomosis.

53. Validation and Comparison of Perfusion Diagnostics in a Tissue-like Flow Phantom, Using Laser Speckle Contrast Imaging, Sidestream Darkfield Microscopy and Optical Coherence Tomography. Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands Sanne M. Jansen, MD, PhD; Daniel Martijn de Bruin, PhD; Simon D. Strackee, MD, PhD; Ton G. van Leeuwen, Professor; Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands Free flap necrosis has a frequent occurrence and results in high morbidity, reoperation and high costs in health care. There is a development of new technologies to image, measure or monitor perfusion in patients. To implement these new techniques, it is of great importance that their measurements are validated. Because of the lack of a gold standard in perfusion diagnostics, validation remains a challenge. We hypothesize that a phantom model could be used to objectively validate and compare perfusion diagnostics. In this study we validated Laser Speckle Contrast Imaging (LSCI), Optical Coherence Tomography (OCT) and Sidestream Darkfield Microscopy in a tissue-like flow phantom. A silicon phantom with the optical properties and microvasculature of 400, 100 and 50 micrometer in diameter was created. Perfusion was mimicked by whole blood of a healthy volunteer, which was pumped through the phantom with a stable pump (Harvard Apparatus 2000) at different velocities (0-20 mm/sec). LSCI (n=150), OCT (n=50) and SDF (n=45) images were obtained of the different vessels at 5 velocity settings. Perfusion parameters in terms of vessel diameter and velocity were obtained. LSCI was not feasible to image vessels of 50 and 100 micrometer in diameter at a depth of 100 micrometer. The 400 micrometer vessel was visible at a depth of 800 micrometer. LSCI measured perfusion in Perfusion Units (arbitrary unit), which increased with the induced perfusion in the phantom. However, this increase was not linear. OCT was able to image all vessels and measure the vessel diameter precisely (SD of 10%). Moreover, perfusion could be measured and increased linear with the induced pump velocity. SDF was able to image all vessels, although the 400 micrometer vessel was less visible because of the imaging depth of 800 micrometer. Vessel diameters could be measured really precisely (SD 5%). We can conclude that LSCI, OCT and SDF are feasible to image blood flow at different velocities (0-20mm/s). LSCI is not able to measure vessel diameter, or image perfusion in single vessels smaller than 100 micrometer. OCT and SDF have a high accuracy and reliability for vessel diameter. OCT has a high accuracy in measurements of perfusion (0-20 mm/sec), however development is needed to relate the used parameter to mL/min/gram tissue. SDF has a high accuracy and reliability for slow flow rates of 1 mm/s and smaller. This tissue-like flow phantom was able to validate perfusion diagnostics of LSCI, OCT and SDF.

54. Changes in Cutaneous Gene Expression by DNA Microarray and Collagen Content is Associated with Clinical Improvement after Microvascular free tissue transfer in Parry Romberg's Disease University of Wisconsin Madison, Madison, 238, USA Tzujane Jenny Chen, MD1; Corinne Voukon, PhD2; Brian Eisinger, PhD2; Samuel O. Poore, MD, PhD3; Kevin Eliceiri, PhD2; John W. Siebert, MD1; (1)Division of Plastic and Reconstructive Surgery, University of Wisconsin, Madison, WI, (2)University of Wisconsin, Madison, WI, (3)Plastic and Reconstructive Surgery, Division of Plastic and Reconstructive Surgery, University of Wisconsin, Madison, WI Purpose: Parry Romberg's Disease is an enigmatic craniofacial disorder characterized by progressive facial atrophy. Standard reconstructive treatment allows the disease to "burn out" with 2 years of no change prior to intervention. In contrast, we have found that early intervention in active disease with a microvascular free flap (MVFF) is beneficial and results in stable clinical improvement without progression of disease, and early intervention in children may avoid the detrimental disease effects on facial growth. The pathogenesis and molecular mechanisms governing Parry Romberg's Disease have never before been described. The purpose of our current study was two fold; 1) to begin to elucidate the pathophysiology of this disease using imaging modalities and gene expression in the skin of patients with Parry Romberg Disease and 2) evaluate the effect of surgical treatment on gene expression and basic collagen characteristics. Methods: Patients with Parry Romberg Disease underwent MVFF to the face to address contour deformity. At the time of the initial surgery, tissue samples were collected for analysis. When each patient returned at 6 months for a scheduled revision surgery, another tissue sample was taken for analysis. Patients presenting for rhytidectomy had tissue samples taken as control tissue. Gene expression and collagen content were evaluated in all patients. Collagen content was analyzed using second harmonic generation (SHG) imaging. Collagen fiber quantification was done using the software package CT-FIRE. For gene expression, cDNA libraries were generated and sequenced. Patients with disease were compared to control samples. The effect of surgery on this measure was assessed with a paired t-test. Differential gene expression was calculated using a linear regression model. Results: Fifteen subjects were evaluated. (Four control and eleven Parry Romberg patients) All patients with Parry Romberg Disease underwent MVFF to the face. Seven patients underwent scheduled six month revision surgery. Significant changes in gene expression were seen after surgical intervention in Parry Romberg Disease. Postoperative patient samples were more similar to healthy control samples, unlike preoperative patient samples. 518 genes were upregulated including 13 genes involved with collagen and 43 genes involved with skeletal development, while 433 genes were downregulated postoperatively. Conclusions: We describe for the first time molecular signatures and collagen content in Parry Romberg Disease. Molecular signatures in skin became more similar to healthy controls and

were associated with clinical improvement after surgical intervention in Parry Romberg Disease. Microvascular free tissue transfer may have a physiologic impact on this enigmatic disease.

55. Early Markers of Angiogenesis and Ischemia During Bowel Conduit Neovascularization China Medical University Hospital, Taichung, 256, Taiwan Oscar J. Manrique, MD1,2; Pedro Ciudad, MD, PhD3; Alex K. Wong, MD4; Suresh K Agarwal, M.D.5; Federico Lo Torto, M.D.3; Hsu-Tang Cheng, MD6; Hung-Chi Chen, MD, PhD, FACS7; (1)Division of Plastic and Reconstructive Surgery, China Medical University Hospital, Taichung, Taiwan, (2)Mayo Clinic, Rochester, MN, (3)China Medical University Hospital, Taichung, Taiwan, (4)Division of Plastic Surgery, University of Southern California Keck School of Medicine, Los Angeles, CA, (5)University of Wisconsin, Madison, WI, (6)Department fo Plastic and Reconstructive Surgery, China Medical University Hospital, Taichung City, Taiwan, (7)Department of Plastic Surgery, China Medical University Hospital, Taichung, Taiwan Background: Jejunal and ileocolon flaps have been described as good and reliable method to restore the continuity of the aerodigestive tract after trauma or cancer resection. Radiation, infection or depleted recipient vessels, might place at risk these flaps during ischemic events. Based on several decades of experience and clinical observation, we have noticed that these flaps have a different physiologic response during ischemic events. One possible explanation is the lack of serosa in the posterior wall of the ileocolon flap as compared with a complete serosal coverage in the jejunal flap. Using an ischemia/reperfusion murine model, the purpose of this study is to evaluate the function of the serosal layer during the bowel conduit neovascularization phase after it has been transferred into a new recipient site. Materials and Methods: 2 groups of rats were compared: a control group (jejunal-conduit with serosa), and a target group (jejunal-conduit without serosa). These conduits were harvested out of the peritoneal cavity and transferred into a subcutaneous pocket. 72-hours after transfer and pedicle-ligation, histologic changes related to ischemia/reperfusion were assessed. In addition, tissue markers of angiogenesis (CD34), ischemia (LDH) and inflammation (IL1-b and IL-6) were analyzed. All statistical tests were two-sided with a significance level of 0.05. Results: 20 Sprague-Dawley male rats were compared: (10 with and 10 without serosa). Histologic analysis showed intact jejunal mucosa in the target group. The control group showed decreased number of mucin, globet cells, decreased height and fragmentation of villi with absence of intestinal glands (Figure-1). Markers of angiogenesis (CD34) were higher in the target group (Figure-2). In addition, markers of ischemia (LDH) (p=0.0045) and inflammation (IL-1b, p=0.0008, and IL-6, p=0.0008) were significantly lower in the target group as compared with control (Figure-3). Conclusions: During ischemic events the serosa plays an essential role in delaying the neovascularization and angiogenesis phase of the transferred bowel flaps. In circumstances when the recipient site does not offer an adequate and healthy bed or a vascular insult occurs, the use of bowel flaps with less amount of serosa may have a faster neovascularization phase increasing its chances of survival.

Figure 1. Histologic Analysis. A. Control group: fragmentation of villi with absence of intestinal glands. B. Target Group: intact jejunal mucosa.
Figure 2. A. Control group: decreased amount of CD34 stains. Target group: increased amount of CD34 stains (black triangles)
Figure 2. Serosa vs. No-Serosa group: (LDH: p=0.0045; IL-1b: p=0.0008; IL-6: p=0.0008).

56. Macrophages are Recruited to the Neuromuscular Junction After Nerve Injury Washington University School of Medicine, Saint Louis, 215, USA Alexandra Marie Keane, B.A.; Katherine Bernadette Santosa, M.D.; Albina Jablonka-Shariff, Ph.D.; Alison Kay Snyder-Warwick, M.D.; Washington University, Saint Louis, MO Background: The neuromuscular junction (NMJ) is the interface between a motor nerve and its target muscle. One important resident cell of the NMJ is the terminal Schwann cell (tSC). tSCs are active after nerve injury, extending long processes that guide axons for NMJ reinnervation. The mechanisms underlying tSC response to injury are unknown. We hypothesize that after nerve injury, the NMJ becomes hypoxic, leading to macrophage recruitment and macrophage-induced angiogenesis, allowing for tSCs to extend processes along the scaffold of newly formed blood vessels. In this study, we sought to determine if nerve injury induced macrophage recruitment to the NMJ, and at which time point after nerve injury macrophage recruitment was the greatest. Methods: Twenty one (n=3 per time point) adult S100-GFP mice underwent right peroneal nerve transection without repair. At a specified time point after nerve injury (1, 2, 3, 4, 5, 6, or 7 days), the animal was sacrificed, and the extensor digitorum longus (EDL) muscles from the right injured and left uninjured sides were harvested for immunostaining and confocal analysis. Immunocytochemical staining was performed with CD68 for monocytes/macrophages and DAPI for nuclear staining. Results: Preliminary results demonstrate significantly more CD68+ cells in denervated EDL muscles than in uninjured controls on postoperative days (POD) 4-7. We observed the highest number of macrophages recruited to the NMJ and muscle on POD5 after nerve injury. Interestingly, there were no differences in the number of CD68+ cells between the denervated EDL muscle and uninjured controls on POD1-3. The CD68+ cells were also morphologically distinct at different time points after nerve injury. The majority of CD68+ cells present in the denervated muscles at POD1-3 were small and round with scant cytoplasm while those present at POD4-7 were larger in size, irregularly shaped, granular and more phagocytic in appearance. Conclusions: After nerve injury, macrophages are recruited to the NMJ and muscle, with the most significant recruitment occurring at POD5. Additionally, macrophage morphology was notably different across different time points, which could represent a transition from M1 to M2 macrophage phenotypes. Drawing from these data, future studies will determine the importance of macrophage recruitment on NMJ reinnervation after nerve injury.

57. A Novel Graft Targeted Immunosuppression Strategy Promotes Survival and Neuroregeneration in Porcine Heterotopic Flap and Orthotopic Forelimb VCA United States Army Institute for Surgical Research, San Antonio, TX Sharon D Lawson, MD1; Charles Anton Fries, MA, MB, BChir, MRCS2; Lin Wang, MD2; Nitin Joshi, PhD3; Praveen Kumar Vemula, MD, PhD4; Jeffrey Karp, MD, PhD3; Vijay Gorantla, MD, FACS5; Michael R. Davis, MD, FACS2; (1)United States Army Institute for Surgical Research, San Antonio, TX, (2)Reconstructive Surgery, United States Army Institute of Surgical Research, San Antonio, TX, (3)Brigham and Womens Hospital, Boston, MA, (4)Institute for Stem Cell Biology and Regenerative Medicine, National Centre for Biological Sciences, Bangalore, India, (5)University of Pittsburgh, Pittsburgh, PA Aims: Vascularized Composite Allotransplantation (VCA), as exemplified by hand and face transplantation, can restore form, function and quality of life in unreconstructable combat or civilian trauma. To date two amputee service members have received hand transplants. However the life enhancing utility of VCA is restricted by the lifelong risks of systemic immunosuppression, To justify such risks, and to support VCA options over conventional reconstruction or prostheses, we need to accomplish graft survival consistent with functional neuroregeneration. Our goal was to establish efficacy and feasibility of a tacrolimus eluting graft embedded system to prevent acute rejection (AR) and promote neuroregeneration after VCA. Methods: A tacrolimus eluting inflammation/AR responsive hydrogel platform was developed and evaluated in two robust pre-clinical porcine VCA models. First, gracilis myocutaneous flaps were transplanted heterotopically into recipient necks. Group 1 (controls, n=8) received no additional intervention. In group 2 (experimental, n=10), 28mg of an enzyme responsive tacrolimus-eluting hydrogel was injected into the subcutaneous space of the donor flap. The second experiment employed a true orthotopic forelimb transplant. Group 3 (controls, n=2) received no additional intervention. Group 4 (experimental, n=9) received the enzyme responsive tacrolimus-eluting hydrogel injected into the subcutaneous space of the donor forelimb. Tacrolimus levels in VCA tissues and systemic troughs were serially monitored along with clinicopathologic signs of AR. Nerve regeneration was longitudinally assessed by nerve conduction studies. Results: Control VCA in both models underwent Banff Grade 4 acute rejection (AR) by post operative day six. The embedded gels delayed grade 4 rejection in the gracilis flaps beyond 14 days. The forelimb with embedded gels had not undergone acute rejection after four weeks with two animals surviving to the end point of the study at 100 days. Nerve regeneration studies in the forelimb model showed positive results from day 57 with nerve conduction velocities of approximately 20 m/s. Conclusions: Graft embedded macrophage responsive hydrogels successfully achieved high tacrolimus levels in VCA tissues with negligible / undetectable systemic levels with successful prevention of AR, prolongation of VCA survival and electrophysiologic evidence of nerve regeneration. Future studies will investigate repeated delivery of drug gels once monthly to further prolong graft survival for longer-term evaluation of immune and functional neuroregeneration outcomes.

58. Simplifying Arterial Coupling - A Preclinical Assessment of an Everter Device to Aid with Arterial Anastomosis University of Michigan, Ann Arbor, 212, USA Ian C. Sando, MD1; Jeffrey S. Plott, MME2; Brendan M. McCracken, BS2; Mohamad H. Tiba, MD2; Kevin R. Ward, MD2; Jeffrey H. Kozlow, MD, MS3; Paul S. Cederna, MD3; Adeyiza O. Momoh, MD1; (1)Department of Surgery, Section of Plastic Surgery, University of Michigan, Ann Arbor, MI, (2)University of Michigan, Ann Arbor, MI, (3)Section of Plastic Surgery, University of Michigan, Ann Arbor, MI INTRODUCTION: Microvascular arterial anastomosis using coupling devices is less time-consuming and technically demanding than manual suturing; however, the limited ability to stretch the thick, muscular wall of arteries over the rings of coupler devices often precludes their use. We designed a tool to make arterial coupling simple and efficient. The device consists of a silicone dilator that fits into the cut end of an artery to circumferentially evert its thick, muscular wall and engage coupler pins simultaneously (Fig. 1). The aim of this study was to 1) evaluate the device's effectiveness in engaging vessel walls on coupler pins, and 2) evaluate efficiency and patency with arterial anastomoses performed with the everter and coupler in comparison to hand sewn anastomoses using a live porcine model. METHODS: The bilateral femoral arteries of five male swine (30-40 kg) were exposed and sharply divided. Arteries were randomized to undergo anastomosis using either interrupted sutures (Control, n=5) or the everter device with the Synovis GEM Microvascular Anastomotic COUPLER System (Experimental Group, n=5). We evaluated the percent of pins that engaged the arterial wall, the time to perform the anastomosis, and vessel patency immediately afterwards and at one-week post-anastomosis. RESULTS: All animals tolerated the procedures well with no major complications. Arteries were coupled using 2.5 mm coupler rings. On average, 73% of coupler pins engaged the vessel walls after a single pass of the everter. On average, time to perform anastomosis was significantly less when using the everter/coupler compared to manual suturing (6.2 min vs. 20.9 min, p < 0.001). At the end of the surgical procedures, we observed 100% patency with flow through the anastomoses in both groups of vessels (5 of 5 respectively) by hand held Doppler assessment. At one week post-op, 3 of 4 coupled arteries and 4 of 4 hand sewn arteries were patent; the fifth subject is pending evaluation. CONCLUSIONS: Successfully completing arterial anastomoses was easier and significantly more time-efficient when using the everter/coupler compared to a standard hand sewn technique. The everter device has the potential to streamline the arterial microvascular anastomotic procedure, obviate the need for a skilled assistant, and minimize surgeon fatigue during long, complex operative procedures. Decreased one-week patency rates in the everter/coupler group were likely due to excessive tension across coupled anastomoses in our model, and larger studies with tension-free anastomoses are needed to confirm long-term safety and efficacy.


59. Cuff Anastomosis Technique in Supermicrosurgery: A Prospective, Randomized, Comparative Animal Study The Curtis National Hand Center, Baltimore , 210, USA Derek Fletcher, MD1; Ryan D Katz, MD2; Sione Fanua, MS1; James Higgins, MD3; Kenneth R Means Jr, MD1; Ebrahim Paryavi, MD, MPH4; (1)Union Memorial Hospital, Baltimore, MD, (2)Curtis Hand Center, Union Memorial Hospital, Baltimore, MD, (3)Curtis National Hand Center, Union Memorial Hospital, Baltimore, MD, (4)Hand Surgery, Union Memorial Hospital, Baltimore, MD Abstract: Cuff Anastomosis Technique in Supermicrosurgery: A Prospective, Randomized, Comparative Animal Study. Hypothesis: Cuff microsurgical anastomosis technique is faster than traditional suture anastomosis technique with equal flap survival rates. A prospective, randomized, comparative animal study using the rat superficial inferior epigastric artery (SIEA) free flap model was used to test the hypothesis. Methods: Bilateral SIEA free flaps were performed on seventeen, six to eight-week-old male, Charles River rats. Laterality of anastomosis technique was randomized, right versus left, for cuff versus suture microsurgical technique. Average arterial and venous vessel diameters were 0.3-0.4mm and 0.5-0.8mm, respectively. Appropriately sized, sterile polymide tubes (Rivertech Medical) were chosen for each anastomosis based on vessel external diameter. The tubes were hand cut to produce the cuff. Cuff technique was performed by pulling the recipient vessel through the lumen of the cuff, everting the vessel edge over the edge of the cuff opening and securing it with a 10-0 nylon suture loop. The everted recipient vessel/cuff -construct was then intussuscepted into the lumen of the flap vessel and secured with a second 10-0 nylon suture loop and a simple interrupted suture. Procedural time for each anastomosis was recorded and flap survival was monitored for seven days. Statistical analysis for differences in anastomotic time and flap survival over seven days was performed using the Wilcoxon rank sum test and the Wilcoxon sign rank test, respectively. Results: The median procedure time for arterial and venous anastomoses was significantly faster for cuff versus suture technique: arterial anastomosis times were 7.68 minutes versus 9.18 minutes (p<0.04) and venous anastomosis times were 4.75 minutes versus 17.2 minutes (p<0.001). Flap survival rates for cuff and suture technique were 80% and 70%, respectively. The difference in flap survival rate was not statistically significant (p=1.0). Conclusion: Cuff microsurgical anastomosis technique was faster than suture anastomosis technique with equal vessel patency and flap survival rates in the rat SIEA free flap model. Cuff technique is well suited for use in rat vessels less than one millimeter in diameter and may have broader applications in the field of clinical microsurgery.

60. Lymph Node Transfer Decreases Swelling and Restores Immune Function in A Transgenic Model of Lymphedema Memorial Sloan Kettering Cancer Center , New York , 221, USA Jung-Ju Huang, MD1; Jason Gardenier, MD2; Geoffrey E. Hespe, B.S.3; Gabriela Garcia Nores, MD4; Raghu P. Kataru, PhD4; Jessie Z. Yu, MD5; Joseph H Dayan, MD4; Babak J. Mehrara, MD6; (1)Division and Reconstructive Microsurgery, Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, Linkou Me, Taoyuan, Taiwan, (2)Department of Surgery, Weill Cornell Medical College, New York, NY, (3)Memorial Slaon-Kettering Cancer Center, New York, NY, (4)Memorial Sloan Kettering Cancer Center, New York, NY, (5)memorial Sloan Kettering Cancer Center, New York, NY, (6)Division of Plastic and Reconstructive Surgery, Memorial Sloan Kettering Cancer Center, New York, NY Purpose: Lymphedema is a morbid disease and lymph node transfer (LNT) is considered the most promising treatment. The mechanism of LNT remains unclear and its effectiveness in restoring immune function is not well explored. The purpose of this study was therefore to analyze lymphatic and immune function after LNT. Methods: Hindlimb lymphedema was induced in a transgenic mouse model by ablating the lymphatic system using diphtheria toxin following with popliteal lymph node dissection. Two weeks later, experimental animals underwent popliteal LNT while controls were treated with popliteal incision alone. Limb swelling, pathological change of the tissue, immune cell trafficking, and immune responses were then analyzed 10 weeks later. Results: LNT animals had a marked reduction in foot swelling from 30.8% to 4.8%, giving the reduction rate as 84.4% ; in contrast, control animals had no improvement in swelling from 31.3% preoperatively to 31.1 % over this period of time. These measurements were confirmed with histological studies demonstrating a 47.6% reduction in adipose deposition and a 31.9% reduction of collagen type I deposition after LNT in comparison to control. In addition, animals treated with LNT had decreased infiltration of T cells and marked lymphatic regeneration with connection to the transferred lymph node. Less sclerosis of the collecting lymphatic vessels was identified. Moreover, animals treated with LNT were able to traffic dendritic cells to their lymph nodes and had significant increases in antibody responses as compared with controls. In response to DNFB, systemic immune responses were restored in LNT group. Conclusions: LNT markedly induces lymphangiogenesis and improves lymphatic function in a mouse model of lymphedema. Transplanted lymph nodes maintain immunologic function and can support migration of antigen presenting cells.
61. RHAMM is a Novel Target For Promoting Subcutaneous Adipogenesis London Regional Cancer Program, London, 251, Canada S. Bahram Bahrami, PhD1; Cornelia Tolg, PhD2; Caitlin J Symonette, MD, MSc3; Veiseh Mandana, PhD4; David Holdsworth, PhD5; Mina Bissell, PhD6; Arjang Yazdani, MD3; Eva Turley, PhD7; (1)Biological Systems and Engineering Division, Biosciences Area, Berkeley, CA, (2)Cancer Research Laboratories, London, ON, Canada, (3)University of Western Ontario, Hand and Upper Limb Centre, London, ON, Canada, (4)Palo Alto Research Centre (PARC, a Xerox Company), Palo Alto, CA, (5)Preclinical Imaging Research Centre, London, ON, Canada, (6)University of Minnesota, Minneapolis, MN, (7)London Health Sciences Centre, London, ON, Canada Background: The Receptor for Hyaluronan-Mediated Motility (RHAMM) is a key regulator of stem cell differentiation and its functional loss results in an increased ratio of adipocytes to myofibroblasts (Tolg et al., 2006 J Cell Biol. 175, 1017). We developed RHAMM functionblocking peptides to promote subcutaneous adipogenesis as an alternative to autologous fat transfer for volume restoration and skin rejuvenation. Methods: Subcutaneous fat content of adult female wild type vs. RHAMM-/- mice were quantified using micro-CT imaging and histology. RHAMM function blocking peptides were screened for the ability to promote adipogenesis of mesenchymal stem cells and preadipocytes using Oil red O. Peptides were assessed for adipogenic potential in skin and mammary fat pads.Peptides were formulated in collagen I or Orthovisc gels to retain peptides at injection site. Skin and mammary fat pads were quantified using micro-CT and image analyses. Results: Micro-CT showed increased adipogenesis in female RHAMM-/- mice. Histological andimmunohistochemical analysis of RHAMM-/- tissue confirmed an increased subcutaneous fat layer (p < 0.05) in RHAMM-/- versus wild-type mice. Injection of RHAMM function blocking peptides that promote adipogenesis in culture increased dorsal back subcutaneous fat pad area (208.3 � 10.4 mm2 versus control 84.11 � 4.2 mm2; p < 0.05) and mammary fat pad size (45 ± 11mg above control background, p=0.002) in female rats. Conclusion: Blocking RHAMM function by peptide injection is a novel and minimally invasive method for promoting subcutaneous adipogenesis and it represents an alternative or complementary tool to subcutaneous fat augmentation techniques.

63. Multi-disciplinary Evaluation Methods for Facial Paralysis Patients Who Has Received Functioning Free Muscle Transplantation Chang Gung Memorial Hospital, Taoyuan, 256, Taiwan Tsung-Kai Lin, MD1; Johnny Chuieng - Yi Lu, M.D.2; David Chwei-Chin Chaung, MD2; (1)Chang Gung University and Medical College, Taoyuan, Taiwan, (2)Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, Chang Gung Medical College and Chang Gung University, Taoyuan, Taiwan Abstract Background: Treatments for facial paralysis patients include static and dynamic procedures. Functioning free muscle transplantation (FFMT) has now become a standard procedure in providing active facial reanimation. Multiple methods have been used to evaluate the pre- and post- operative results, but none of which holds as the benchmark for proper evaluation. Aims and Objectives: Facial paralysis patients who show good functional results are not always satisfied, especially congenital facial paralysis patients like Möbius syndrome. The aims of this article are to use multidisciplinary methods to gain further insights subjectively and objectively for patient outcomes evaluation. Materials and Methods: From January 1986 to January 2010, a total of 26 facial paralysis patients (both unilateral and bilateral) received Spinal accessory nerve (XI) innervated muscle for smile reconstruction. The evaluation methods used were composed of a Smile Excursion Score (from 0 to 4) to evaluate muscle excursion, a staging system (from Stage I to V) to determine the Cortical Adaptation Stage of the functioning muscle, and a questionnaire to assess the satisfaction of the patients (from 1 to 5). Results: A total of 32 functioning free muscle transplantations were performed on 26 patients. The mean Smile Excursion Score improved from 0.5 to 3.4 postoperatively. 84% of the patients showed independent smile, while 90% of patients showed at least a satisfaction score of 3 or more out of 5. Majority of the patients (50%) were more concerned with the aesthetic look rather than the functional status. Conclusion: The aforementioned evaluation methods provide not only objective results but also subjective outcomes that allow surgeons to better understand the postoperative presentations. Subjective feedbacks directly from the patients can allow surgeons to gain further insights and enlighten surgeons on possible revisions to improve the final outcomes. Keywords: facial paralysis, XI-innervated free muscle, outcome evaluation

Figures


64. Here Comes More Sun Shine: Industry's Payments to Plastic Surgeons Duke University Medical Center, Durham , 222, USA Rizwan Ahmed, MD1; Joseph Lopez, MD MBA2; Kate Buretta, MD1; Sunjae Bae, MD MPH3; Justin Sacks, MD4; Dorry L. Segev, MD PHD5; Alexander Allori, MD MPH1; Jeffrey Marcus, MD6; (1)Duke University, Durham, NC, (2)Johns Hopkins University School of Medicine, Baltimore, MD, (3)Johns Hopkins University, Baltimore, MD, (4)Department of Plastic and Reconstructive Surgery, The Johns Hopkins School of Medicine, Baltimore, MD, (5)Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, MD, (6)Division of Plastic Surgery, Duke University, Durham, NC Background:The Physician Payment Sunshine Act (PPSA) is a government initiative requiring all biomedical companies to publicly disclose payments to physicians. We previously published the initial release of payment data made to plastic surgeons. With help from plastic surgeons the biomedical device industry has engineered products to improve outcomes in Reconstructive Microsurgery. However, there continues to be a lack of awareness and misinterpretation among plastic-surgeons, the public, and the media regarding these financial transactions. The goal of this study is to evaluate the most current PPSA data and explore the context of these payments. Methods:Using PPSA data (Jan-Dec 2014), we studied the distribution of non-research industry payments made to plastic and craniofacial surgeons nationally. Results: During the 2014 fiscal year, industry paid $28,876,097 to 6,487 plastic-surgeons. Plastic-surgeons received a median (IQR) of $232($91-$624); mean $44,451. Amongst all plastic-surgeons, 26.9% received <$100, 55.2% received between $100 and $999, 14.4% received between $1,000 and $9,999, 3.1% received between $10,000- $99,999, and 0.4% received in excess of $100,000. The four highest paid plastic-surgeons received $8,286,882, $4,750,139, $1,633,432, and $393,557. The four largest payment categories were: royalty or licensing fees ($14,408,952) to 27 individuals; speaker fees ($5,307,153) to 272 individuals; consulting fees ($3,481,382) to 361 individuals; and meals ($2,203,663) to 6,366 individuals. The four highest paying companies contributed to 74.3% of total payments. These were: Allergan Inc. ($16,283,184); LifeCell Corporation ($1,970,173); Valeant Pharmaceuticals North America ($1,938,119); and Mentor Worldwide LLC ($1,287,643). The four highest paid states were: California ($10,488,318); Tennessee ($4,939,012); Illinois ($2,240,886); and New York ($1,252,135). Conclusion: More than 80% of all plastic surgeons received payments <$1,000 during a 12 month period. Royalty and licensing fees contributed to almost half of total payments, but these were paid to <0.005% of plastic surgeons. Awareness of the PPSA and continued surveillance of its data are critical for plastic-surgeons as it provides a means to prevent public misconceptions about industry payments within the specialty.



65. Cost Analysis of Enhanced Recovery after Surgery in Microvascular Breast Reconstruction Mayo Clinic, Rochester, 213, USA Christine Oh, MD1; James Moriarty, M.S.2; Bijan Borah, Ph.D2; Whitney Bergquist, Pharm. D., R.Ph2; Niles J. Batdorf, MD3; Kristin Mara, MS2; William Scott Harmsen, Ph.D2; Michel Saint-Cyr, MD4; Valerie Lemaine, MD5; (1)Department of Surgery, Division of Plastic Surgery, Mayo Clinic, Rochester, MN, (2)Mayo Clinic, Rochester, MN, (3)Plastic and Reconstructive Surgery, Mayo Clinic, Rochester, MN, (4)Baylor Scott & White Health, Temple, TX, (5)Division of Plastic Surgery, Mayo Clinic, Rochester, MN Background: Enhanced recovery after surgery (ERAS) pathways have been shown in multiple surgical specialties to decrease hospital length of stay (LOS) after surgery. ERAS in breast reconstruction has been found to decrease hospital length of stay and inpatient opioid use. ERAS protocols can facilitate patients' recovery and is a systemwide improvement that can potentially increase the quality of care while decreasing costs. Methods: A standardized ERAS pathway was developed through multidisciplinary collaboration. It addressed all phases of surgical care for patients undergoing free-flap breast reconstruction utilizing an abdominal donor site. In this retrospective cohort study, clinical variables associated with hospitalization costs for patients who underwent free-flap breast reconstruction with the ERAS pathway were compared with those of historical controls, termed traditional recovery after surgery (TRAS). All patients included in the study underwent surgery between September 2010 and September 2014. Predicted costs of the study groups were compared using a generalized linear model to account for the highly skewed nature of healthcare cost data. Results: A total of 200 patients were analyzed: 82 in the ERAS cohort and 118 in the TRAS cohort. Clinical variables found to have a statistically significant difference between groups included unilateral versus bilateral procedure (p=0.04) and need for post-operative blood transfusion (p=0.03). Statistically different variables were controlled for in regression analysis of cost variables. Adjusted mean costs of ERAS patients were found to be $4,576 less than the TRAS control group ($38,688 versus $43,264). Conclusions: Implementation of the ERAS pathway was associated with significantly decreased costs when compared to historical controls. There has been a healthcare focus towards resource allocation that requires plastic surgeons to recognize the need for an economic evaluation of clinical practice. The ERAS pathway can increase health care accountability by improving quality of care while decreasing costs associated with autologous microsurgical breast reconstruction.


66. Quality of Life and Health Outcomes after Genital Gender Confirming Surgery: A Systematic Review of the Global Experience The Johns Hopkins University School of Medicine, Baltimore, 210, USA Eric L. Wan, BS1; Charalampos Siotos, MD2; Andrea Lo, N/A2; Ricardo J. Bello, MD, MPH3; Stella M. Seal, MLS4; Jens U Berli, MD5; Carisa M. Cooney, MPH4; Damon S. Cooney, MD, PhD6; Gedge D. Rosson, MD4; Richard Redett, MD1; (1)Johns Hopkins University School of Medicine, Baltimore, MD, (2)Johns Hopkins University, Baltimore, MD, (3)Department of Plastic and Reconstructive Surgery, Johns Hopkins University, Baltimore, MD, (4)Department of Plastic and Reconstructive Surgery, Johns Hopkins University School of Medicine, Baltimore, MD, (5)Oregon Health & Science University, Portland, OR, (6)Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD Background: Nearly 1.4 Million Americans are transgender. The prevalence of gender confirming surgery (GCS) in the U.S. is at least 1 per 100,000 people and is expected to increase when a 33-year exclusion on coverage for transitional care was lifted in 2014. Recently, it was demonstrated that covering transgender surgery is cost-effective. We systematically reviewed whether quality of life and health outcomes improve after genital GCS. Methods: We searched the PubMed, Embase, Scopus, and Web of Science databases across all years for articles describing GCS. Two authors independently reviewed 1590 titles and abstracts based on inclusion and exclusion criteria. Studies were included if they reported health-related quality of life, mental health outcomes, sexual health outcomes, and/or the absolute number of complications. We excluded case studies and studies that performed surgery on subjects less than 18 years of age or that addressed failed reassignment or reversal surgery. Finally, we conducted a synthesis of the outcomes of genital gender confirming surgery with pooled estimates. Results: Thirty-eight studies were included and represented 3,117 transgender patients who underwent genital "sex-reassignment surgery" [2207 male-to-females (MtF), 910 female-to-males (FtM)]. The majority (26/38) were retrospective studies; only 4 were prospective. After surgery, protective sensation was present in 287/326 patients (81.3%, 95% CI: 72.9% to 89.6%) and erogenous sensation was present in 559/633 (71.8%, 95% CI: 40.7% to 100%). Orgasm with masturbation was achieved in 349/481 (76.3%, 95% CI: 67.2% to 85.4%). Tissue necrosis after either phalloplasty or vaginoplasty occurred in 80/1392 (6.9%, 95% CI: 4.1% to 9.6%) (Figure 1). Of the FtMs, 663/821 (79.7%, 95% CI: 62% to 97.3%) could stand while voiding, and fistula occurred in 44/418 (13.7%, 95% CI: 6.4% to 21%). For the MtFs, neovaginal stenosis occurred in 144/1322 (11%, 95% CI: 7.6% to 14.5%). Only 1 study for each of the health-related quality of life, mental health, and sexual health outcomes used a validated questionnaire. Conclusions: Most existing studies are of low levels of evidence, making it difficult to make robust conclusions regarding the effectiveness of genital GCS. One study suggests that GCS alleviates gender dysphoria and makes quality of life comparable to that of the general population. Here, we have described the rates of positive outcomes and complications following GCS. Reconstructive microsurgeons are uniquely poised to affect the transitional care of transgender individuals and advance the science of GCS.

Figure 1: Pooled Estimate of Tissue Necrosis Following Gender Confirming Surgery

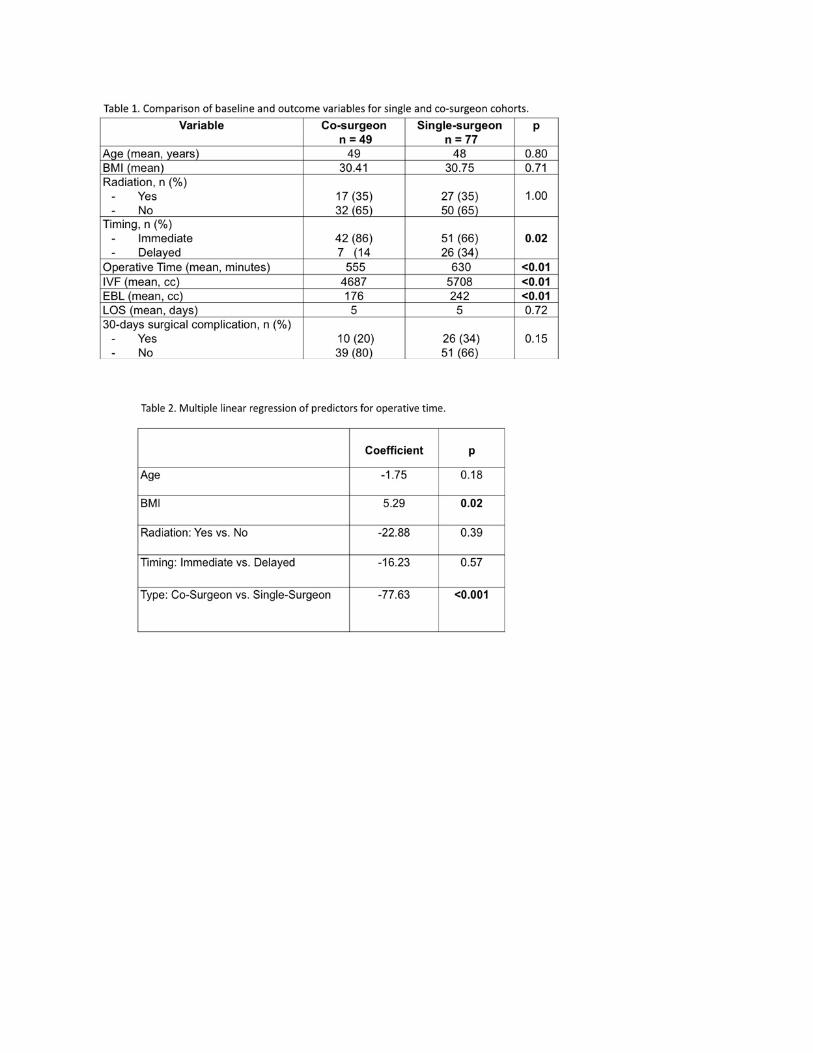
67. Outcomes Associated with Co-surgeons Versus Single-surgeon for Bilateral Autologous Free Flap Breast Reconstruction Memorial Sloan Kettering Cancer Center, New York, 221, USA Geoffrey E Hespe, BS; Shantanu N Razdan, MD, MSPH; Hinaben Panchal, MD; Robert J Allen, Jr., MD; Peter G Cordeiro, MD; Colleen M McCarthy, MD, MS; Andrea L Pusic, MD, MHS; Joseph H Dayan, MD; Joseph J Disa, MD; Babak J Mehrara, MD; Evan Matros, MD MPH; Memorial Sloan Kettering Cancer Center, New York, NY Background: Bilateral autologous free flap breast reconstructions are time and labor intensive procedures. In order to circumvent long operative times while ensuring patient safety, plastic surgeons have started working together on such cases. There is insufficient data in the literature about the benefits of co-surgeon operations. We hypothesized that use of co-surgeons would reduce operative time without increasing complication rates. Methods: A retrospective chart review was performed at Memorial Sloan Kettering Cancer Center from Feb 2014 through May 2016 of bilateral free flap autologous breast reconstructions. Cases were divided into two cohorts: single-surgeon (SS) and co-surgeons (CS). The same surgeons participated in both the SS and CS operations. Baseline demographic and clinical variables including age, BMI, smoking, comorbidities, radiation and timing of reconstruction were noted. Outcome variables included operative time, length of stay (LOS), intraoperative intravenous fluids (IVF), estimated blood loss (EBL), and complications. Continuous and categorical variables were compared using t-test and chi-square tests respectively. Multiple linear regression analysis was performed to evaluate predictors of operative time after adjustment for confounding. Results: A total of 126 patients underwent bilateral free flap breast reconstructions: 49 (39%) by CS and 77 (61%) by SS. There were no significant differences in baseline characteristic between the two groups except for the proportion of immediate reconstructions. Mean operative time, IVFs and EBL were significantly less in the CS than the SS group (Table 1, p<0.01). A trend towards lower 30-day complication rates was observed with CS operations. LOS was comparable between groups. After adjustment for confounders, regression analysis demonstrated co-surgeons were an independent predictor of decreased operative time compared to single surgeon (Table 2, p<0.001). Higher BMI was a predictor of increased OR time (p=0.02). Conclusions: Co-surgeon breast reconstructions were associated with a significant decrease in operative time and a trend toward lower complication rates. Additional studies are warranted to determine the overall impact of co-surgeon cases on medical spending.