4.Fluid and Electrolytes
23
47 FLUID ELECTROLYTE MANAGEMENT IN A NEONATE PHYSIOLOGY:The aim of fluid and electrolyte therapy is to ensure a smooth transition from the aquatic in-utero environment to the dry ex-utero environment. The amount of total body water (TBW) decreases markedly from intrauterine life to adulthood: water contribu tes to 90% of body weight in the 24 weeks old fetus, 75% in term infants, and 50% in adults Total body water is divided into two compartments: intracellular fluid (ICF) and extracellular fluid (ECF).Potassium (K+) is the major ion of the ICF while The major ion of ECF is sodium (Na). ECF decreases during growth.ECF is subdivided into intravascular and extra vascular components e.g ‘‘third space’’ which characterizes free fluid in preformed body compartments under physiologic al (like urine in the bladder, cerebrospinal fluid, etc) and pathological conditions (like ascites, or pleural effusions). After birth, there is efflux of fluid from the intracellular fluid (ICF) to the extracellular fluid (ECF) compartment. This increase in the ECF compartment floods the neonatal kidneys eventually resulting in a salt and water diuresis by 48 -72 hours. Loss of this excess ECW results in physiological weight loss in the first week of life. Since the ECW compartment is larger in more preterm neonates, the weight loss is greater in preterm neonates. Term infants are expected to loose up to 10% of their birth weight as compared upto 15% weight loss in premature neonates. Failure to loose this ECF may be associated with morbidities like patent ductus arteriosus (PDA)necrotizing enterocolitis (NEC) and chronic lung disease(CLD) in preterm neonates.
-
Upload
manju-kumari -
Category
Documents
-
view
229 -
download
0
Transcript of 4.Fluid and Electrolytes
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 1/23
47
FLUID ELECTROLYTE
MANAGEMENT IN A NEONATE
PHYSIOLOGY:The aim of fluid and electrolyte therapy is to ensure a smooth
transition from the aquatic in-utero environment to the dry ex-utero environment.
The amount of total body water (TBW) decreases markedly from intrauterine life to
adulthood: water contributes to 90% of body weight in the 24 weeks old fetus, 75% in
term infants, and 50% in adults
Total body water is divided into two compartments: intracellular fluid (ICF) and
extracellular fluid (ECF).Potassium (K+) is the major ion of the ICF while The major ion of
ECF is sodium (Na).
ECF decreases during growth.ECF is subdivided into intravascular and extra vascular
components e.g ‘‘third space’’ which characterizes free fluid in preformed body
compartments under physiological (like urine in the bladder, cerebrospinal fluid, etc)
and pathological conditions (like ascites, or pleural effusions).
After birth, there is efflux of fluid from the intracellular fluid (ICF) to the extracellular
fluid (ECF) compartment. This increase in the ECF compartment floods the neonatal
kidneys eventually resulting in a salt and water diuresis by 48-72 hours. Loss of this
excess ECW results in physiological weight loss in the first week of life.
Since the ECW compartment is larger in more preterm neonates, the weight loss is
greater in preterm neonates.
Term infants are expected to loose up to 10% of their birth weight as compared upto
15% weight loss in premature neonates.
Failure to loose this ECF may be associated with morbidities like patent ductus
arteriosus (PDA)necrotizing enterocolitis (NEC) and chronic lung disease(CLD) in preterm
neonates.

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 2/23
48
Renal function Kidneys in the neonate have a limited capacity to excrete
both concentrated and dilute urine.
The physiological range for urine osmolality in neonates varies from a lowerlimit of 50
mmol/L to an upper limit of 600 mmol/L in preterms and 800 mmol/L in term infants.
An acceptable osmolality range of 300-400 mmol/L would correspond to a daily urine
output of 2-3 kg/hr.
Sodium supplementation should be started after ensuring initial diuresis,(Generally
within 48-72 hrs) a decrease in serum sodium or at least 5-6%weight loss. Also, failure to
supplement sodium after the first week of life would result in low body stores of
sodium.
Preterm neonates have a limited tubular capacity to reabsorb sodium and hence have
increased urinary losses. Sodium requirements ranges from 3-5 mEq/kg/day in preterm
neonates after the first week of life.
Failure to provide this amount of sodium may be associated with poor weight gain. Very
low birth weight infants on exclusive breast-feeding may need sodium supplementation
in addition to breast milk until32-34 weeks corrected age.
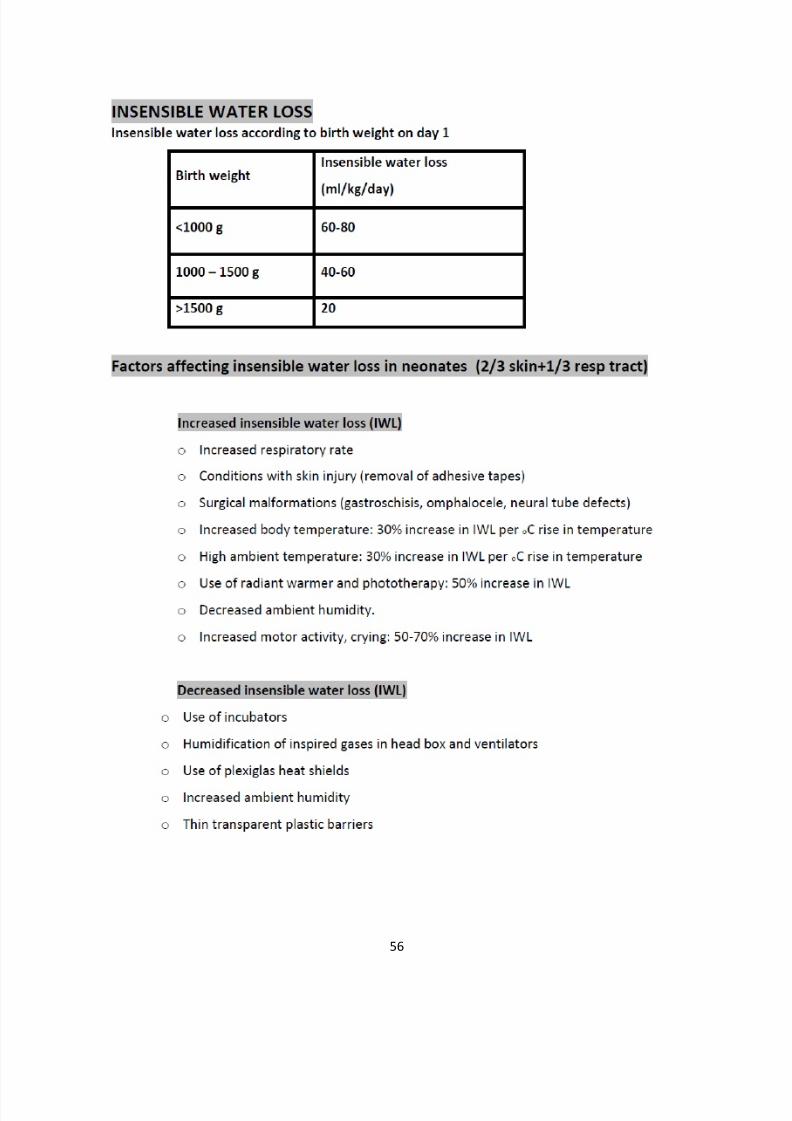
Fluid losses and insensible water loss: In
addition to mandatory water loss by the kidneys and gastro-intestinal system (termed as
sensible loss), additional water losses occur due to evaporation from the skin and respiratory
tract. This water loss is termed as insensible water loss (IWL).
Insensible water losses tend to be higher in preterm infants Evaporation loss through
the skin usually contributes to 70% of IWL. The remaining 30% is contributed through
losses from the respiratory tract.

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 3/23
49
Various environmental and neonatalfactors have been implicated in excessive insensible
waterlosses through the skin and respiratory tract .
The emphasis in fluid and electrolyte therapy should be on prevention of excessive IWL
rather than replacement of increased IWL.
Transparent plastic barriers reduce IWL in preterm infants. Thin, transparent plastic
barriers (e.g., cling-wrap) may be used to increase the local humidity and limit air
movement. These transparent plastic films may be fixed to the supporting walls of the
radiant warmer in order to create a micro-environment around the baby. These plastic
barriers are effective in reducing IWL without interfering with the thermal regulation of
the warmer.They have been found to reduce the IWL by 50-70% for preterm infants
under the radiant warmer.
FLUID :HOW MUCH TO GIVE:
(a) Term babies and babies with birth weight > 1500 grams. A
full term infant on intravenous fluids would need to excrete a solute load of about
15 mosm/kg/day in the urine. To excrete this solute load at a urine osmolarity of
300 mosm/kg/day, the infant would have to pass a minimum of 50 ml/kg/day.
Allowing for an additional IWL of 20 ml/kg, the initial fluids should be 60-70
ml/kg/day. The initial fluids should be 10% dextrose with no electrolytes in order
to maintain a glucose infusion rate of 4-6 mg/kg/min. Hence total fluid therapy
on day would be 60 ml/kg/day. It is provided as 10% dextrose. As the infant
grows and receives enteral milk feeds, the solute load presented to the kidneys
increases and the infant requires more fluid to excrete the solute load. Water is also
required for fecal losses and for growth purposes. The fluid requirements
increase by 15-20 ml/kg/day until a maximum of 150 ml/kg/day . Sodium
and potassium should be added after 48 h of age and glucose infusion should
be maintained at 4-6 mg/kg/min. On day 7 Fluids should be given at 150-160
ml/kg/day .

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 4/23
50
(b) Preterm baby with birth weight 1000-1500 gram The urine output
in a preterm baby would be similar to a term baby. However, the fluid requirement will
be higher due to increased IWL and increased weight loss (extracellular fluid loss).
Liberal use of caps, socks and plastic barriers to reduce the IWL under the radiant
warmer is recommended. Using this method it has been found out that 80-
100ml/kg/day of 10% dextrose to be adequate on day 1 of life. As the skin matures in a
preterm baby, the IWL progressively decreases and becomes similar to a term baby by
the end of the first week. Hence, the fluid requirement in a preterm baby, initially
higher due to increased IWL, would become similar to a term baby by the end of the
first week . Plastic barriers, caps and socks are used throughout the first week in
order to reduce IWL from the immature skin. Fluids need to be increased at 10-15
ml/kg/day until a maximum of 150ml/kg/day. Sodium and potassium should be added
after 48 hours and glucose infusion should be maintained @4-6 mg/kg/min. Fluids
should be given at 150-160 ml/kg/day and sodium supplementation at 3-5 mEq/kg
should continue till 32-34 weeks corrected gestational age. Depending on the
condition of the baby and if IWL is not prevented adequately fluids can be increased
to 170-180 ml/kg/day in these newborns.
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 5/23
51
MONITORING FLUID AND ELECTROLYTE
STATUS: this is done with help of several indices.
1. Body weight : Serial weight measurements can be used as a guide to
estimate the fluid deficit in newborns.
Term neonates loose 1-3% of their birth weight daily with acumulative loss of 5-
10% in the first week of life.
Preterm neonates loose 2-3% of their birth weight daily with a cumulative loss
of 15-20% in the first week of life. Failure to lose weight in the first week of life
should be an indicator for fluid restriction.
excessive weight loss in the first 7 days or later would be non-physiological and
would merit correction with fluid therapy.
2. Clinical examination: The usual physical signs of dehydration are
unreliable in neonates.
Tachycardia indicates CCF or hypovolemia.
Capillary refill time > 3 sec indicates decreased cardiac output.
Blood pressure changes are late.
Reduced skin turgor, dry mucous membranes, reduced urine output, depressed AF
indicate under hydration.
Edema (genital, periorbital, peripheral) and Hepatomegaly may indicate CCF.
Normal urine output is 1-3 ml/kg/hr. Less than 0.5 ml/kg/hr is significant oliguria .
Infants with 10% (100 ml/kg) dehydration may have sunken eyes and fontanel, cold
and clammy skin, poor skin turgor and oliguria.
Infants with 15% (150ml/kg) or moredehydration would have signs of shock
(hypotension,tachycardia and weak pulses) in addition to the above features.
Dehydration would merit correction of fluid andelectrolyte status gradually over
the next 24 hours.

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 6/23
52
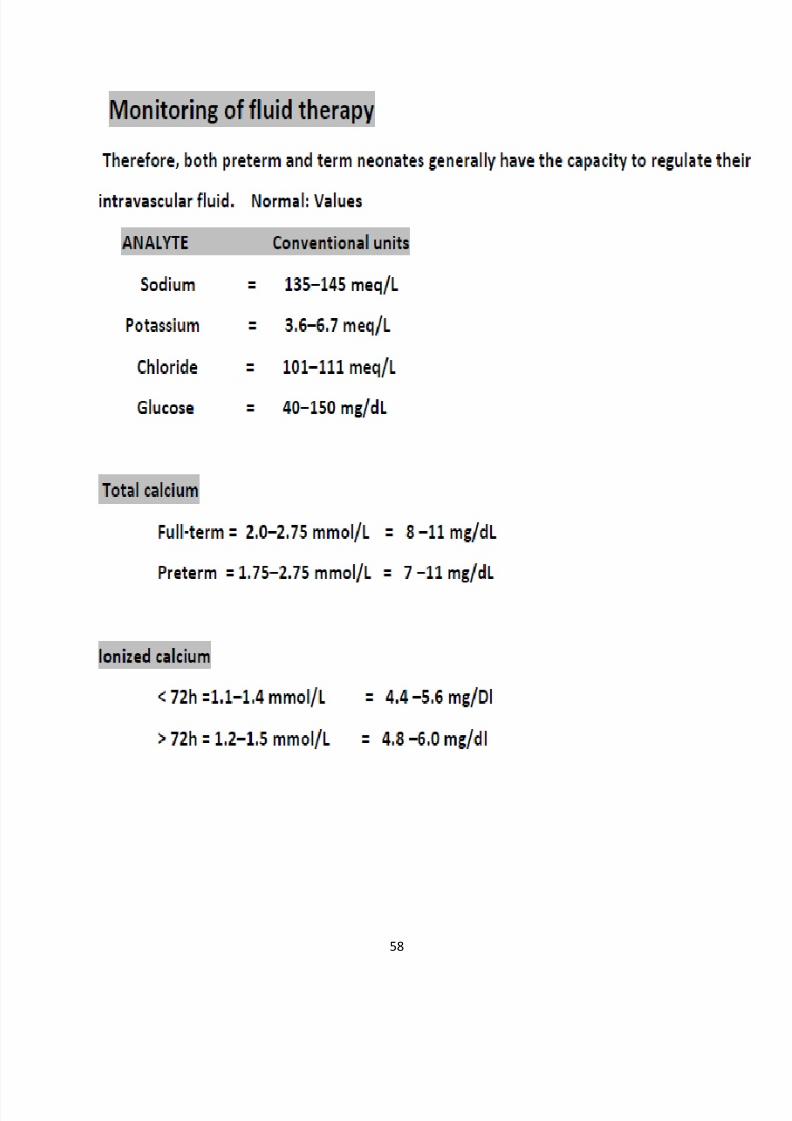
3. Serum biochemistry: Serum sodium and plasma osmolarity would be
helpful in the assessment of the hydration status in an infant. Serum sodium values
should be maintained between 135-145 meq/L.
Hyponatremia with weight loss suggests sodium depletion and would merit sodium
replacement.
Hyponatremia with weight gain suggests water excess andnecessitate fluid restriction.
Hyponatrremia with no edema,and decreased urinec output asociated with urine
osm>serum osmolarity would suggest SIADH.Treatment is to decrease fluids to 2/3.
Hypernatremia with weight loss suggests dehydration and would require fluid
correction over 48 hours.
Hypernatremia with weight gain suggests salt and water load and would be an
indication of fluid and sodium restriction.
4. Urine output, specific gravity (SG) and
osmolarity: The capacity of the newborn kidney to either concentrate or
dilute urine is limited and estimation of urine SG would be useful to guide fluid therapy.
The acceptable range for urine output would be 1-3 ml/kg/hr, for
specific gravity between 1.005 to 1.012 and for osmolarity between100-400 mosm/L.
Specific gravity can be checked by dipstick or by a handheld
refractometer . Osmolarity is estimated by freezing point
osmometer.
5. Serum blood urea nitrogen (BUN), creatinine:
Serum creatinine is a useful indicator of renal function. There is an exponential fall in
serum creatinine levels in the first week of life as maternally derived creatinine is
excreted. Failure to observe this normal decline in serial samples is a better indicator of
renal failure as compared to a single value of creatinine in the first week of life.

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 7/23
53
6. Blood gas: Blood gases are not needed routinely for fluid management.
However, they are useful in the acid base management of patients with poor tissue
perfusion and shock. Hypo-perfusion is associated with metabolic acidosis.
LABORATORY GUIDELINES FOR FLUID AND
ELECTROLYTE THERAPYIntravenous fluids should be increased in the presence of (a) Increased weight loss (>3%/day or a cumulative loss >20%)
(b) Increased serum sodium (Na>145 mEq/L)
(c)Increased urine specific gravity (>1.020) or
urine osmolality (>400mosm/L)(d) Decreased urine output(<1 ml/kg/hr).
Similarly, fluids should be restricted in the presence of (a) Decreased weight loss (<1%/day or a cumulative loss <5%),
(b) Decreased serum sodium in the presence of weight gain (Na<130 mEq/L)
(c) Decreased urine specific gravity (<1.005) or urine osmolality
(<100mosm/L)
(d) Increased urine output (>3 ml/kg/hr)
GUIDELINES FOR STARTING
ELECTROLYTES: Sodium and potassium should be started in the IV fluids after 48 hours, each in a dose
of 2-3 meq/kg/day.
Calcium may be used in a dose of 4 ml/kg/day (40 mg/kg/day) of calcium gluconate for
the first 3 days in certain high risk situations .
Dextrose infusion should be maintained at 4-6 mg/kg/min.
10% dextrose may be used in babies >1250 grams and 5% in those below 1250 gm.

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 8/23
54
CORRECTION OF DEHYDRATION:
Moderate (10%) to severe (15%) dehydration fluid deficits are corrected gradually over
24 hours. For infants in shock, 10-20 ml/kg of normal saline is given immediately over 1-2 hours followed by half correction over 8 hours. The remaining deficit is administered
over 16 hours.
Assuming equal losses of fluid from the ECW and ICW, the replacement fluid after
correction of shock, should consist of N/2 composition. This fluid and electrolyte
solution should be administered in addition to the maintenance fluid therapy. Assuming
a deficit of 10% isotonic dehydration in a 3 kg child on day 4, the fluid calculation would
be as follows
(a) Dehydration replacement: 300 ml of N/2 saline over 24 hours (150 ml over 8 hours
and 150 ml over 16 hours) (b) Maintenance fluids: 300 ml (100 ml/kg/day on day 4) of
N/5 in 10% dextrose over 24 hrs.

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 9/23
55
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 10/23
56

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 11/23
57
When to stop fluids?
If the baby is taking 2/3 of the demand orally and the baby is not very sick, has no significant
electrolyte abnormalities one may contemplate about stopping IV fluids.
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 12/23
58

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 13/23
59
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 14/23
60
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 15/23
61
HYPONATREMIA
Na < 130 meq/l ( to be concerned if < 125 meq/l)
May be associated with Normal / increased / decreased Total Body Sodium
Clinical classification of hyponatremia :
Hypertonic : Hyperglycemia
Isotonic: Hyperlipidemia, Hyperproteinemia
Hypotonic: True hyponatremias (Osm < 270)
HYPERTONIC HYPONATREMIA
Serum osmolality elevated
Causes :Hyperglycemia ,increased Urea, Mannitol
Each 100 mg/dl increase of Blood Glucose , Na drops by 1.6 mEq/l
T/t : Control of primary cause i.e treat hyperglycemia
ISOTONIC HYPONATREMIA / PSEUDOHYPONATREMIA
When solid component ↑,there is a decrease in serum Na
( Hyponatremia) despite a normal amount of Na .
Serum Osmolarity is normal despite hyponatremia
This is an artifact due to error in measurement of Na in conditions like like
hyperlipidemia and/or hyperproteinemia
This error could be avoided by the use of Ion Specific Electrode (ISE) which measures Na
in serum water .
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 16/23
62
TRUE/ HYPOTONIC HYPONATREMIA
Types
Euvolemic: SIADH, Excess IVF, Pain, stress
Hypovolemic: Diuretics, CAH, Renal, GI causes, third spacing, Tubular imbalance (
immaturity)
Hypervolemic: CHF
SITUATIONS
Hyponatremia with weight loss suggests sodium depletion and would
merit fluid and sodium replacement .
Hyponatremia with weight gain suggests water excess and
necessitate fluid restriction .
Hyponatremia with no edema,and decreased urine output asociated
with urine osm>serum osmolarity would suggest SIADH.
Treatment is to decrease fluids to 2/3.
If serum sodium is less than 120,then furosemide along with 3% Nacl
should be given.
Hypernatremia with weight loss suggests dehydration and would
require fluid correction over 48 hours .
Hypernatremia with weight gain suggests salt and water load and
would be an indication of fluid and sodium restriction.
If the cause of hyponatremia is ARF then fluid should restricted
to less than sum total of (IWL+urine output . Fluids must be
restricted to insensible water loss (IWL) along with urinary loss.
The urinary loss must be replaced volume for volume. The insensible
water loss in a term neonate is 25 mL/kg/day. In preterm neonates

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 17/23
63
this canvary widely depending on gestation, postnatal age, use of
radiant warmers, phototherapy. It can vary from 40-100mL/kg/day.
IWL can be assumed to be 40 mL/kg/day in preterm infants for
calculating fluids in neonates (adequate care must be taken to
reduce IWL by using caps, socks, cling wrap, oil especially for
preterm babiesunder radiant warmer). It is advisable to revise fluid
requirement every eight hourly basing on urine output.The fluid
should be electrolyte free, 10% dextrose.
MANAGEMENT ASYMPTOMATIC HYPONATREMIA :
Na requirement (along with maintenance) =
0.6 X BW X (desired serum Na - current serum Na) X 1/2(Half
correction in one day) +maintenance(3 meq/kg/day) Correct over 48 hrs
AIM: No more than 10 mEq/L/day .
SYMPTOMATIC HYPONATREMIA (NA<120 MG/DL)
Give 3% NaCl
Roughly equals 3% NS bolus 4-6ml/kg slow iv over 1-2 hrs.
AIM for correction in 4hrs

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 18/23
64
HYPERNATREMIA(> 150 MEQ/L)
Causes:
Normal/ deficient ECF Volume: Usually seen in VLBW, due to inadequatefree water intake to compensate for very high IWL
Rx: Increase free water
ECF Volume excess: Excess administration of isotonic( I/V boluses) &
Hypertonic fluids( Soda bicarb admn.)
Rx: Restrict Na and Fluids
Effect of hypernatremia
1. Acute Hypernatremia : Hypertonic ECF leads to Cell shrinkage which can lead
to intracerebral bleed or cerebral venous thrombosis.
2. Chronic Hypernatremia : cells generate osmoprotective amino acids &
idiogenic osmoles stored-- hence no cell shrinkage and baby may be asymptomatic.
Clinical features
a) Irritability ,drowsiness alternating
with irritability
b) Excessive /high pitched crying
c) Hyperpnea
d) Doughy skin (>loss of 10% of wt)
e) Fever
f) Tremulousness
g) Seizures
h) Focal deficit and coma
Management
No fluid boluses unless child is in shock .IF In SHOCK ,give 20-30 ml/kg of NS OVER 20-30 min(ROBERTON)
Maximum correction possible is 12 meq/day….i.e 145-157 meq/l will reqire correction over 1
day, 157-169 meq/l will require correction over 2 days….
Typical fluid used is initially DNS, subsequently I/2 DNS … generally 1.25-1.5 times normal
luid in usion rate.
8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 19/23
65
Complications
Rapid correction of Chr hypernatremia leads to Extrapontine myelinolysis ( Presents
as seizures during correction)
Hyperglycemia ( inhibition of insulin secretion)-no need to give insulin
Hypocalcemia, hypokalemia
CSF Protein due to leakage from damaged Blood vessel

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 20/23
66
Potassium disturbance : Hyperkalemia and Hypokalemia
HYPERKALEMIA
Common causes :
Increase K release: Tissue destruction, hemolysis, bleeding, IVH, hypothermia, BA
,cephalhematoma
Decreased K Clearance: ARF, oliguria,hyponatremia, CAH
Misc: Blood/ exchange transfusion, dehydration, excess administration,VLBW
Commonest cause of cardiac arrthythmias and death if treatment is not initiated
promptly
Pseudohyperkalemia : Due to sampling error as in hemolysed sample
Avoid heel-prick samples
if injected into sample tube forcefully
increased K levels due to hemolysis
blood obtained by vessel pucture
SIGNS : brady or tachyarrhythmias, Cardiac instability or collapse
ECG : changes progress with increasing K levels
1) Peaked T waves
(increased repolarization)
2) Flattened P waves & increasing PR intervals
( suppression of atrial conductivity)
3) QRS widening & slurring
( conduction delay in ventricular & myocardium)

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 21/23
67
MANAGEMENT :
Stop K intake
Rule out spurious hyperkalemia - trauma , thrombocytosis ,hyperleucocytosis (TLC
>50,000 /mm3)
Repeat serum K , ECG to be repeated.
GOAL 1 : REMOVE ALL SOURCES OF EXOGENOUS POTASSIUM –
rehydrate & stabilize baby
GOAL 2 :STABILI ZATION OF CONDUCTING TISSUESCalcium gluconate (10%) given carefully under cardiac monitoring 1-2 ml/kg I/V as a slow
infusion.
If baby is also hyponatremic - Hypertonic Nacl infusion may also be used .
GOAL 3 : DILUTION & INTRACELLULAR SHIFTING OF POTASSIUM
1) Alkalemia : Na bicarbonate
2) Insulin: Bolus of insulin & glucose (0.05 units/kg of regular insulin with 2ml/kg of 10%dextrose - followed by continuous infusion of D10 at 2-4 ml/kg/hr and human insulin 10
units/100ml at rate of 1ml/kg/hr.)
3) Beta-2-adrenergic stimulation: enhances K uptake via stimulation of Na-K ATPase .
Salbutamol ,given as puffs if baby is on ventilator .
Less effective in preterms due to immaturity of the beta receptors
GOAL 4 : ENHANCED K EXCRETION
1) Exchange resins :
Cation exchange resins like Na or Ca polystrene sulfonate , or Kayexelate given rectally (
1gm/kg with 0.5 g/ml of DW/NS ) with a minimum retention time of 30 minutes
2) Furosemide : 1mg/kg iv may increase K excretion
3) Peritoneal dialysis & double-volume exchange transfusion with fresh whole blood.

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 22/23

8/3/2019 4.Fluid and Electrolytes
http://slidepdf.com/reader/full/4fluid-and-electrolytes 23/23
69