4 Holley - UAB
15
1/16/2015 1 Rb tL H ll MS MD FPMRS Rb tL H ll MS MD FPMRS Robert L. Holley, MSc, MD, FPMRS Robert L. Holley, MSc, MD, FPMRS Professor of Obstetrics and Gynecology Professor of Obstetrics and Gynecology Division of Urogynecology and Pelvic Reconstructive Surgery Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology Department of Obstetrics and Gynecology University of Alabama at Birmingham School of Medicine University of Alabama at Birmingham School of Medicine Disclosures Disclosures I have no conflicts of interest pertinent to this lecture. I have no conflicts of interest pertinent to this lecture. Objectives Objectives Appreciate the history associated with the Appreciate the history associated with the development of the development of the cystoscope cystoscope Review indications for diagnostic Review indications for diagnostic cystourethroscopy cystourethroscopy Become familiar with instrumentation for Become familiar with instrumentation for diagnostic and operative cystoscopy diagnostic and operative cystoscopy Become familiar with normal bladder/urethral Become familiar with normal bladder/urethral anatomy and identify abnormal anatomy and identify abnormal cystoscopic cystoscopic findings findings
Transcript of 4 Holley - UAB

1/16/2015
1
R b t L H ll MS MD FPMRSR b t L H ll MS MD FPMRSRobert L. Holley, MSc, MD, FPMRSRobert L. Holley, MSc, MD, FPMRS
Professor of Obstetrics and GynecologyProfessor of Obstetrics and Gynecology
Division of Urogynecology and Pelvic Reconstructive SurgeryDivision of Urogynecology and Pelvic Reconstructive Surgery
Department of Obstetrics and GynecologyDepartment of Obstetrics and Gynecology
University of Alabama at Birmingham School of MedicineUniversity of Alabama at Birmingham School of Medicine
DisclosuresDisclosures
I have no conflicts of interest pertinent to this lecture.I have no conflicts of interest pertinent to this lecture.
ObjectivesObjectives
Appreciate the history associated with the Appreciate the history associated with the development of the development of the cystoscopecystoscope
Review indications for diagnostic Review indications for diagnostic cystourethroscopycystourethroscopy
Become familiar with instrumentation for Become familiar with instrumentation for diagnostic and operative cystoscopydiagnostic and operative cystoscopy
Become familiar with normal bladder/urethral Become familiar with normal bladder/urethral anatomy and identify abnormal anatomy and identify abnormal cystoscopiccystoscopicfindingsfindings

1/16/2015
2
Howard KellyHoward Kelly
Bladder distensionBladder distension
Scope introduced using an Scope introduced using an obturator, with obturator, with ptpt in kneein knee--chest chest positionposition
Negative intraNegative intra--abdominal abdominal pressure allowed air to distend pressure allowed air to distend bladderbladder
Head mirror to reflect lightHead mirror to reflect light
Greatly improved visualizationGreatly improved visualization
20th Century and Today20th Century and Today
Hopkins/Kopany 1954Hopkins/Kopany 1954
FiberFiber--optic scopeoptic scope
Rod lens system Rod lens system
Angled scopesAngled scopes
Complex instrumentationComplex instrumentation
Flexible cystoscopeFlexible cystoscope
General surgeons developed Urology subspecialtyGeneral surgeons developed Urology subspecialty
Ob/Gyn combined program decreased cystoscopy Ob/Gyn combined program decreased cystoscopy training by gynecologiststraining by gynecologists
Granting Of Privileges For Granting Of Privileges For CystourethroscopyCystourethroscopy
“Should be based on training, experience and “Should be based on training, experience and demonstrated competence”demonstrated competence”
“Implies that the physician has knowledge and “Implies that the physician has knowledge and competency in the instrumentation and surgical competency in the instrumentation and surgical co pete cy t e st u e tat o a d su g caco pete cy t e st u e tat o a d su g catechnique; can recognize normal and abnormal technique; can recognize normal and abnormal bladder and urethral findings: and has knowledge bladder and urethral findings: and has knowledge of pathology, diagnosis and treatment of specific of pathology, diagnosis and treatment of specific diseases of the lower urinary tract”diseases of the lower urinary tract”
ACOG Committee Opinion Number 372 July 2007, Reaffirmed 2010

1/16/2015
3
Indications for Diagnostic Cystoscopy Indications for Diagnostic Cystoscopy
Identify intraoperative urinary tract injury:Identify intraoperative urinary tract injury:
--Bladder perforation during TVTBladder perforation during TVT
--Ureteral patency after vault suspensionUreteral patency after vault suspension
Recurrent UTIs Recurrent UTIs
Irritative voiding symptoms in the absence of UTI, Irritative voiding symptoms in the absence of UTI, esp following prior mesh procedure:esp following prior mesh procedure:
--Bladder stonesBladder stones
--Foreign body in bladder and/or urethraForeign body in bladder and/or urethra
Diagnosis and/or treatment of interstitial cystitisDiagnosis and/or treatment of interstitial cystitis
Indications for Diagnostic Cystoscopy.... Indications for Diagnostic Cystoscopy....
VesicovaginalVesicovaginal fistulafistula
Bladder/urethral diverticulumBladder/urethral diverticulum
HematuriaHematuria
Evaluate for spread of gynecologic malignancyEvaluate for spread of gynecologic malignancy Evaluate for spread of gynecologic malignancyEvaluate for spread of gynecologic malignancy
Operative Operative cystocysto in in GynGyn::
BiopsyBiopsy
Foreign body removal (stone, mesh)Foreign body removal (stone, mesh)
IntradetrusorIntradetrusor Botox injectionsBotox injections
Urethral bulking agentsUrethral bulking agents
When to do cystoscopy?When to do cystoscopy?
When the risk of lower urinary tract injury exceeds When the risk of lower urinary tract injury exceeds 1.5%, the routine use of diagnostic cystoscopy is 1.5%, the routine use of diagnostic cystoscopy is warrantedwarranted
Procedures whose risk exceeds this rate include:Procedures whose risk exceeds this rate include:
Laparoscopic and robotic h sterectomLaparoscopic and robotic h sterectom Laparoscopic and robotic hysterectomyLaparoscopic and robotic hysterectomy
AntiAnti--incontinence procedures incontinence procedures
Majority of procedures for correcting pelvic organ Majority of procedures for correcting pelvic organ prolapseprolapse
The safety profile for intraThe safety profile for intra--operative diagnostic operative diagnostic cystoscopy is excellentcystoscopy is excellent

1/16/2015
4
Intraoperative cystoscopy....Intraoperative cystoscopy....Who needs it? Who needs it?
ACOG recommendation: all ACOG recommendation: all pt’spt’s undergoing undergoing prolapse and/or incontinence proceduresprolapse and/or incontinence procedures
Hysterectomy: depends on routeHysterectomy: depends on route
Rate of injury diagnosed with routine cystoscopy:Rate of injury diagnosed with routine cystoscopy:
Route Bladder Ureter
Abdominal 2.2-2.5% 1.7-2.2%
Vaginal 4-6% 1.4-2.6%
LSC 2-3% 0-1.5%
Gilmour, ObGyn ‘06Ibeanu, ObGyn ‘09Vakili, AJOG ‘05
Intraoperative cystoscopy....Intraoperative cystoscopy....Who needs it? Who needs it?
Other surgical/patient factors that increase risk of Other surgical/patient factors that increase risk of urinary tract injuryurinary tract injury
Prior C/S or laparotomyPrior C/S or laparotomy
EndometriosisEndometriosis EndometriosisEndometriosis
ObesityObesity
Large pelvic massLarge pelvic mass
History of pelvic radiationHistory of pelvic radiation
Instrumentation: Rigid CystoscopyInstrumentation: Rigid Cystoscopy
TelescopeTelescope
0, 12, 30 or 700, 12, 30 or 70°°
BridgeBridge
Connector for scope and sheathConnector for scope and sheath
Operative portsOperative ports
Sheath (17Sheath (17--28 French)28 French)
Vehicle for introducing scope, distending media and Vehicle for introducing scope, distending media and instruments into bladderinstruments into bladder
ObturatorObturator
Allows for atraumatic placement of larger caliber sheathsAllows for atraumatic placement of larger caliber sheaths

1/16/2015
5
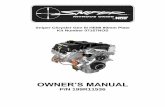
Rigid Rigid CystoscopeCystoscope
Components of a rigid cystoscope
A: Telescopes. 70-degree lateral angled-view telescope (above) and a 30-degree forward-oblique telescope (below).
B: Bridges. Single-port bridge (below) and dual-port deflecting bridge (above).
C: Sheath, 22-French operating.
D: Assembled cystoscope with a diagnostic 17-French sheath.
Rigid CystoscopyRigid Cystoscopy
TelescopesTelescopes
Degree of scope Advantages Disadvantages
70- Good visualization of entire bladder wall (esp for
- Urethroscopy difficult- Diagnostic only
TVT trocar placement)- Diagnostic only
30Visualize all quadrantsOperative cysto
- None (pt discomfort if awake)
0, 12- Urethroscopy- Operative cysto (biopsy, stents, bulking)
- Poor visualization of dome, anterolateral walls
Flexible CystoscopyFlexible Cystoscopy
Useful for office diagnostic cystoscopyUseful for office diagnostic cystoscopy
All 3 parts (scope, bridge, sheath) in oneAll 3 parts (scope, bridge, sheath) in one
1515--FrenchFrench
Learning curveLearning curveea g cu eea g cu e

1/16/2015
6
Cystourethroscopy SetupCystourethroscopy Setup
Lithotomy position (high or low)Lithotomy position (high or low)
Must have:Must have:
CystoscopeCystoscope
Light sourceLight source
Can fill bladder through catheter and look through Can fill bladder through catheter and look through eyepiece on scopeeyepiece on scope
Helpful, but not necessary:Helpful, but not necessary:
Bag of cysto fluid/tubing (80cm above bladder)Bag of cysto fluid/tubing (80cm above bladder)
CameraCamera
Cystourethroscopy SetupCystourethroscopy Setup
Distension mediumDistension medium
Normal salineNormal saline
Sterile water Sterile water –– safe for electrocauterysafe for electrocautery
Antibiotic prophylaxisAntibiotic prophylaxis
Not indicated for diagnostic cysto unless urine Not indicated for diagnostic cysto unless urine dip/culture are positive (ACOG, AUA)dip/culture are positive (ACOG, AUA)
No endocarditis prophylaxis (AHA)No endocarditis prophylaxis (AHA)
Indicated for operative cysto (biopsy, etc)Indicated for operative cysto (biopsy, etc)
Single dose of Cipro 500mg or Bactrim DSSingle dose of Cipro 500mg or Bactrim DS
Operative CystoscopyOperative Cystoscopy
Numerous instruments availableNumerous instruments available
Most pertinent to Gynecologic proceduresMost pertinent to Gynecologic procedures
Grasping forcepsGrasping forceps
Biopsy forcepsBiopsy forceps
ScissorsScissors
Needle/syringe for Botox/bulking agentsNeedle/syringe for Botox/bulking agents
BugbeeBugbee monopolarmonopolar ball electrodeball electrode

1/16/2015
7
Diagnostic Cystoscopy TechniqueDiagnostic Cystoscopy Technique
3030°°/ 70/ 70°° scope w/ 17scope w/ 17--French sheathFrench sheath
2% lidocaine jelly2% lidocaine jelly
Identify air bubble for orientationIdentify air bubble for orientation
InIn--andand--out technique for 12 sweeps, out technique for 12 sweeps, a da d ou ec que o s eeps,ou ec que o s eeps,corresponding to numbers on a clockcorresponding to numbers on a clock
If If ptpt has cystocele, vaginal finger can aid in has cystocele, vaginal finger can aid in visualization of visualization of trigonetrigone/UOs/UOs
Key point: be systematic and thorough, same way Key point: be systematic and thorough, same way every time, documentationevery time, documentation
Normal Bladder MucosaNormal Bladder Mucosa
Smooth surfaceSmooth surface
Pale Pale pink/glistening whitepink/glistening white
Fine vasculatureFine vasculature Fine vasculatureFine vasculature

1/16/2015
8
TrigoneTrigone
Formed by ureteral orifices Formed by ureteral orifices and UVJand UVJ
Thicker, more granular Thicker, more granular texture than dometexture than dometexture than dometexture than dome
InteruretericInterureteric ridgeridge
UO’s usually circular/UO’s usually circular/slitlikeslitlikeopeningsopenings
Trigonal MetaplasiaTrigonal Metaplasia
Squamous metaplasia on Squamous metaplasia on histologyhistology
Thickened white membrane Thickened white membrane with villous contourwith villous contour
Common finding atCommon finding at trigonetrigone Common finding at Common finding at trigonetrigone(>50% reproductive age (>50% reproductive age women)women)
Response to irritative or Response to irritative or infectious process (chronic infectious process (chronic UTI, catheter, UTI, catheter, etcetc))
AKA AKA trigonitistrigonitis
Urethrovesical JunctionUrethrovesical Junction
Usually round or inverted Usually round or inverted horseshoe in shapehorseshoe in shape
Should be closed at rest until Should be closed at rest until cystocysto fluid opens the lumenfluid opens the lumencystocysto u d ope s t e u eu d ope s t e u e
Should close with hold/stress Should close with hold/stress maneuversmaneuvers

1/16/2015
9
Normal UrethraNormal Urethra
Pink, lush epithelium in Pink, lush epithelium in folds (estrogenfolds (estrogen--dependent)dependent)
Urethral crest may be seen Urethral crest may be seen as a posterior longitudinal as a posterior longitudinal ridgeridgeridgeridge
Walls of UVJ and urethra Walls of UVJ and urethra may not may not coaptcoapt in in pt’spt’s with with intrinsic sphincter intrinsic sphincter deficiencydeficiency
Ureteral PatencyUreteral Patency
Free flow of urine from ureteral orifice confirms Free flow of urine from ureteral orifice confirms patencypatency
Cystoscopy cannot diagnose ureteral injury just its Cystoscopy cannot diagnose ureteral injury just its absenceabsence

1/16/2015
10
Acute CystitisAcute Cystitis
Reddened and edematous mucosa obscures Reddened and edematous mucosa obscures vasculaturevasculature
May have hemorrhagesMay have hemorrhages
Known bacterial cystitis contraindication to Known bacterial cystitis contraindication to cystoscopycystoscopy
NonNon--infectious causes:infectious causes:
RadiationRadiation
HemorrhagicHemorrhagic
Catheter reactionCatheter reaction
Interstitial cystitisInterstitial cystitis
TrabeculationTrabeculation
Hypertrophied detrusor musculatureHypertrophied detrusor musculature
Associated with detrusor Associated with detrusor overactivityoveractivity and obstructionand obstruction
Enlargement of intervening Enlargement of intervening sacculessaccules can lead to can lead to diverticuladiverticula

1/16/2015
11
Chronic inflammation leads to Chronic inflammation leads to fibrosis in bladder wallfibrosis in bladder wall
Present with pain, urgency, Present with pain, urgency, frequencyfrequency
HydrodistensionHydrodistension to max to max capacity under general capacity under general anesthesiaanesthesia
Punctate hemorrhages (A) and Punctate hemorrhages (A) and glomerulationsglomerulations (B) are (B) are pathognomonicpathognomonic
Interstitial CystitisInterstitial Cystitis
Hunner’sHunner’s ulcerulcer
Uncommon finding seen in severe, longUncommon finding seen in severe, long--standing ICstanding IC
Surface epithelium destroyed by inflammationSurface epithelium destroyed by inflammation
Appear as velvety red patches or linear cracksAppear as velvety red patches or linear cracks
May crack and bleed with May crack and bleed with hydrodistensionhydrodistension
Cystitis CysticaCystitis Cystica
Benign 1Benign 1-- to 2to 2--mm clear mucosal cysts at the bladder mm clear mucosal cysts at the bladder basebase
Formed by single layers of Formed by single layers of subepithelialsubepithelial transitional transitional cellscells
Associated with chronic irritation and commonly Associated with chronic irritation and commonly surrounded by inflammationsurrounded by inflammation

1/16/2015
12
Bladder PolypBladder Polyp
Benign growth covered by epitheliumBenign growth covered by epithelium
Variable in appearanceVariable in appearance
Usually asymptomaticUsually asymptomatic
5 5 –– 10% may progress to cancer, so should be 10% may progress to cancer, so should be biopsiedbiopsied
Bladder CancerBladder Cancer
Transitional cell carcinomaTransitional cell carcinoma
Most common followed by adenoMost common followed by adeno-- and squamous celland squamous cell
Typical raised lesion with villous or papillary Typical raised lesion with villous or papillary appearance and surrounding inflammationappearance and surrounding inflammation
May be associated with CIS, which can mimic the May be associated with CIS, which can mimic the appearance of infectious cystitisappearance of infectious cystitis
VesicovaginalVesicovaginal FistulaFistula
Vast majority are postVast majority are post--hysterectomyhysterectomy
Usual location is bladder base, superior to Usual location is bladder base, superior to interuretericinterureteric ridge in area of vaginal cuffridge in area of vaginal cuff
Fistula may be large with obvious opening into vagina Fistula may be large with obvious opening into vagina or small with scarring being the only mucosal or small with scarring being the only mucosal abnormalityabnormality

1/16/2015
13
Acute UrethritisAcute Urethritis
Reddened, edematous mucosa along the length of the Reddened, edematous mucosa along the length of the urethraurethra
Urethral PolypsUrethral Polyps
Inflammatory polyps and Inflammatory polyps and fronds found at or near the fronds found at or near the UVJUVJ
Response to chronic Response to chronic inflammationinflammation
Usually translucent with Usually translucent with villous appearancevillous appearance
Can become large enough to Can become large enough to fill the proximal urethral fill the proximal urethral lumenlumen
UrethrovaginalUrethrovaginal FistulaFistula
Opening seen along lateral or posterior surface of Opening seen along lateral or posterior surface of urethraurethra
Urethral diverticulum has similar appearance, but Urethral diverticulum has similar appearance, but may express an exudate with palpationmay express an exudate with palpation

1/16/2015
14
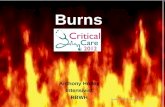
Mesh ErosionMesh Erosion
A: vaginal mesh erosion A: vaginal mesh erosion viewed with a viewed with a cystoscopecystoscope
B: mesh within the B: mesh within the urethral lumen during urethral lumen during urethroscopyurethroscopyurethroscopyurethroscopy
High index of suspicion in High index of suspicion in anyone with LUTS and anyone with LUTS and h/o sling or other mesh h/o sling or other mesh procedureprocedure
Surgical introduction of forgeign bodies into the bladder
This is the metallic This is the metallic tip of a tack used in tip of a tack used in sacrocolpopexy sacrocolpopexy protruding into theprotruding into theprotruding into the protruding into the bladder dome.bladder dome.
A Loop of Prolene A Loop of Prolene suture in the bladder.suture in the bladder.
Sling arm noted in Sling arm noted in the lateral bladder the lateral bladder wallwall
Complications Associated with CystoscopyComplications Associated with Cystoscopy
InfectionInfection
Asymptomatic Asymptomatic BacteriuriaBacteriuria 55--8%8%
Symptomatic UTI 2Symptomatic UTI 2--5%5%
Send urine cx on anyone with symptoms preSend urine cx on anyone with symptoms pre oror Send urine cx on anyone with symptoms preSend urine cx on anyone with symptoms pre-- or or postpost--opop
CystoscopicCystoscopic findings consistent with acute cystitis findings consistent with acute cystitis should be treatedshould be treated

1/16/2015
15
Cystoscopy ComplicationsCystoscopy Complications
Traumatic injury to bladder/urethraTraumatic injury to bladder/urethra
Incidence unknownIncidence unknown
Scope trauma to bladder wallScope trauma to bladder wall
Usually at bladder base above Usually at bladder base above trigonetrigone
Observe for bleeding;Observe for bleeding; electrocauteryelectrocautery if neededif needed Observe for bleeding; Observe for bleeding; electrocauteryelectrocautery if neededif needed
Bladder perforationBladder perforation
Control bleedingControl bleeding
Foley catheter drainageFoley catheter drainage
LSC/laparotomy only if concern for abdominal bleeding LSC/laparotomy only if concern for abdominal bleeding or extremely large defector extremely large defect
CaseCase
At the end of a TVH, uterosacral suspension and At the end of a TVH, uterosacral suspension and cystocele repair for stage 2 prolapse, you perform cystocele repair for stage 2 prolapse, you perform cystoscopy and ~2 minutes after indigo carmine is cystoscopy and ~2 minutes after indigo carmine is given, there is flow only from the right side. given, there is flow only from the right side. Management options…..Management options…..g pg p
Give it time… +/Give it time… +/-- IV Lasix 10IV Lasix 10--20mg20mg
Still no flow…Still no flow…
Confirm surgical history (nephrectomy, Confirm surgical history (nephrectomy, etcetc))
Cut uterosacral stitch on that side and look againCut uterosacral stitch on that side and look again
Attempt to pass stent/Urology consultAttempt to pass stent/Urology consult
IntraopIntraop or postor post--op renal ultrasound/retrogradeop renal ultrasound/retrograde
SummarySummary
Knowledge of the components of a Knowledge of the components of a cystoscopecystoscopeand how to use an angled lens are imperative and how to use an angled lens are imperative before attempting cystoscopy.before attempting cystoscopy.
Ability recognize bladder injury and document Ability recognize bladder injury and document ureteral patency during pelvic surgery will aid in ureteral patency during pelvic surgery will aid in prompt recognition and allow for early correction prompt recognition and allow for early correction of injuries common to gynecologic surgery.of injuries common to gynecologic surgery.
Knowledge of typical lesions is important for Knowledge of typical lesions is important for recognition of pathology and appropriate therapy.recognition of pathology and appropriate therapy.