3D Emergency Medicine -BE...1 EMERGENCY MEDICINE PHYSICIAN E & M, CRITICAL CARE AND OBSERVATION &...
48
1 EMERGENCY MEDICINE PHYSICIAN E & M, CRITICAL CARE AND OBSERVATION & PROCEDURE CODING Medical Account Services, Inc. Presented By: Lynne Severn MBA, CPC, CPMA 351 Ballenger Center Drive, Ste. 250 Frederick, MD 21701 240-529-1456 [email protected] “All rights reserved” TH BASICS THE BASICS 2
Transcript of 3D Emergency Medicine -BE...1 EMERGENCY MEDICINE PHYSICIAN E & M, CRITICAL CARE AND OBSERVATION &...
1
EMERGENCY MEDICINEPHYSICIAN E & M, CRITICAL CARE ANDOBSERVATION & PROCEDURE CODING
Medical Account Services, Inc.
Presented By:Lynne Severn MBA, CPC, CPMA
351 Ballenger Center Drive, Ste. 250
Frederick, MD 21701
240-529-1456
“All rights reserved”g
TH BASICSTHE BASICS2
2
CHECK YOUR RECORDS FOR THE FOLLOWING:
The medical record should be complete and legible
The patient’s name and the date of service should appear on every page of the record
Date of Service on the record should match the date of service on the claim
The medical record should clearly indicate the identity and professional credentials of all the people who contributed to the service
Information in the record should support all diagnosis reported on the claim
All procedures should be clearly documented
E & M Documentation should include HPI ROS PFSH Exam and MDM E & M Documentation should include HPI, ROS, PFSH, Exam and MDM
Health risk factors should be identified
Patient’s progress, response to and changes in treatment, and diagnosis revisions should be documented
Any condition that prevents you from collecting basic information should be noted
3
PROVIDER SIGNATURES
Documents must have a legible full signature Legible first initial & last name
If the signature is not legible then over or under the illegible signature you must : Type or print the provider’s name
Requirements are not considered to be met if: Initials only There is an unsigned typed note with providers typed name There is an unsigned handwritten noteg Statement - “signature on file” Illegible full or partial signature Stamp signatures
CMS Signature Requirements -CMS MLNMM6698 - March 16, 2010
4
3
ICD-9 SIGNS AND SYMPTOMS VS. FINAL DIAGNOSIS
ICD-9s are reported on all bills. The ICD-9 rules were not designed for billing purposes. Unfortunately, payers are now using the ICD 9s to establish medical necessity for claims Payers canthe ICD-9s to establish medical necessity for claims. Payers can use the diagnosis to deny line items/claims. Claims processing problems arise when the services provided are not supported by the primary diagnosis.
Conclusion – Be aware of the need to establish medical necessity
Use pain and injury codes where appropriate
Incorporate signs and symptoms as appropriate
5
ICD-9 codes should explain the reason for the visit in the medical record and support the necessity for the treatment of an illness and are important in submitting a claim cleanly the first time.
SHAR D VISIT R LSHARED VISIT RULES
6
4
SPLIT/SHARED VISIT RULES
Qualified Non Physician Providers (NPPs) who are permitted to assist a physician during a shared visit are:
Nurse practitioners Physician assistants Clinical nurse specialists Certified nurse midwife
Medicare reimburses services provided by an NPP alone at 85% of the rate it reimburses physicians. However, CMS reimburses visits shared between the physician and the NPP at 100% of the allowed amount to the physician.
To obtain the full reimbursement allowed, the physician must document his or her participation in the care of the patient along with the NPP’s documentation of his or her portion of the care. If the documentation does not support the physician’s presence and the portion of work the physician performed, the NPP should report the care alone. 7
REPORTING SPLIT/SHARED VISITS TO MEDICARE
The split/shared visit rules state that both the NPP and the physician must have a face-to-face encounter with the patient on the day the facility or practice reports the service. (The Handshake Rule)
Both the physician and the NPP should document their own participation in the medical record.
The physician practice employs the NPP. Warning - do not report a shared visit when a hospital facility or other entity employs the NPP.
The physician cannot simply co-sign the chart and state “reviewed and agree” in the record without seeing the patient personally.
The physician must perform and document at least some of the three key components of E/M services (i.e., the history, the exam, and the medical decision-making)
https://www.cms.gov/transmittals/downloads/R178CP.pdf8
5
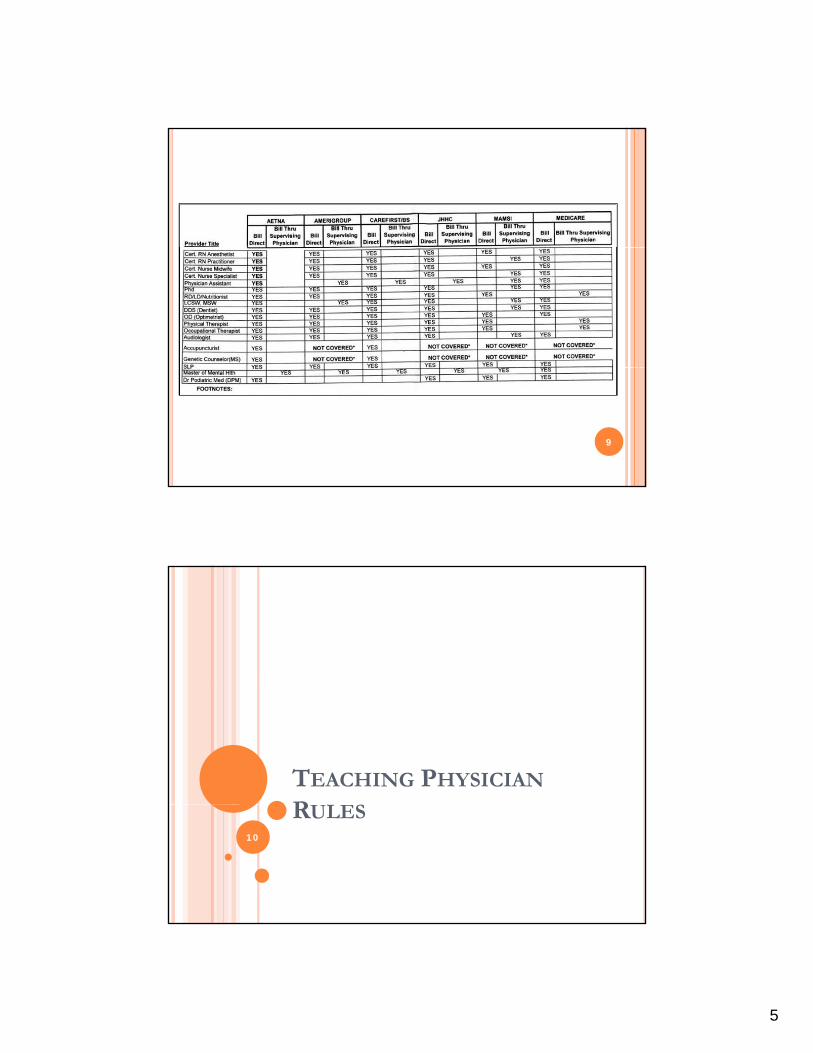
9
TEACHING PHYSICIAN
R L SRULES10
6
Why Do We Need to Know the Teaching Physician Rules?
The PATH audits led to the creation of compliance programs at major teaching institutions across the United States, often because those institutions were forced to pay settlements to the federal government due to abuses found when teaching physicians either did not meet the physical presence requirements when residents or fellows performed services or did not properly document their role in the billing of those services.
11
HIM professionals must understand the guidelines to accurately code and bill medical services properly and handle PATH audits.
BECAUSE….
Resident services are paid directly to hospitals via the Accreditation Council for Graduate Medical Education (ACGME). Teaching physicians are paid for h i i l i h f i f i hitheir involvement in the care of patients, not for time spent teaching.
According to the Medicare Part B Reference Manual:
In the teaching setting, physician services provided to individual patients are considered to be the payment responsibility of the Part B carrier. Conversely, physician services that are furnished for the general benefit of patients (i.e., supervising and teaching of residents) are considered to be services to the hospital and are therefore the payment responsibility of the Part A intermediary.4
In other words, teaching physicians who intend to bill for their services must
document their involvement in the specific care of the patient.
12
7
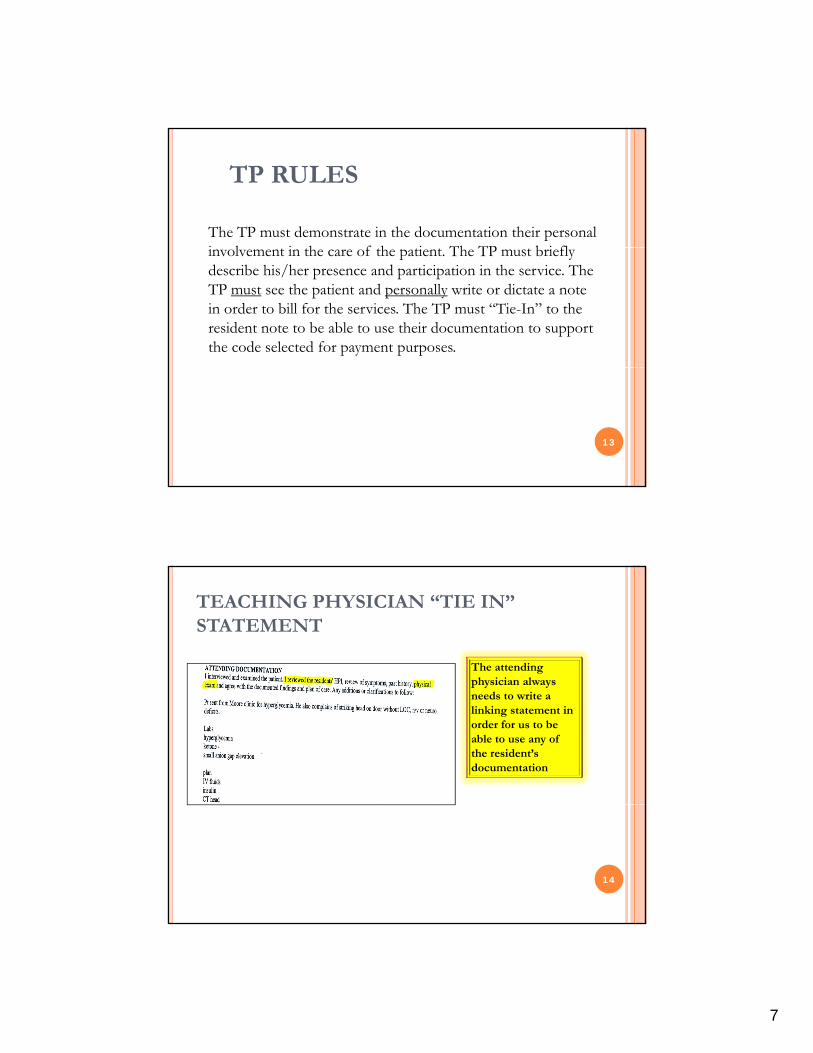
TP RULES
The TP must demonstrate in the documentation their personal i l i h f h i Th TP b i flinvolvement in the care of the patient. The TP must briefly describe his/her presence and participation in the service. The TP must see the patient and personally write or dictate a note in order to bill for the services. The TP must “Tie-In” to the resident note to be able to use their documentation to support the code selected for payment purposes.
13
TEACHING PHYSICIAN “TIE IN” STATEMENT
The attending physician always p ys c ysneeds to write a linking statement in order for us to be able to use any of the resident’s documentation
14
8
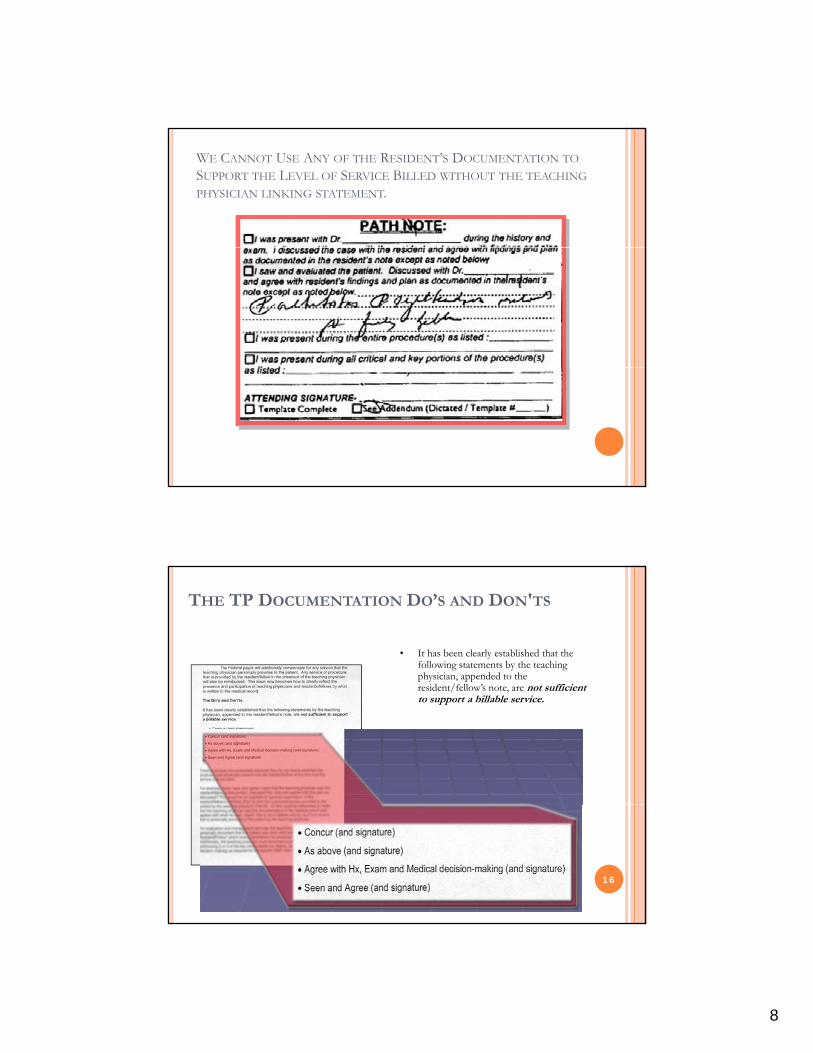
WE CANNOT USE ANY OF THE RESIDENT’S DOCUMENTATION TO
SUPPORT THE LEVEL OF SERVICE BILLED WITHOUT THE TEACHING
PHYSICIAN LINKING STATEMENT.
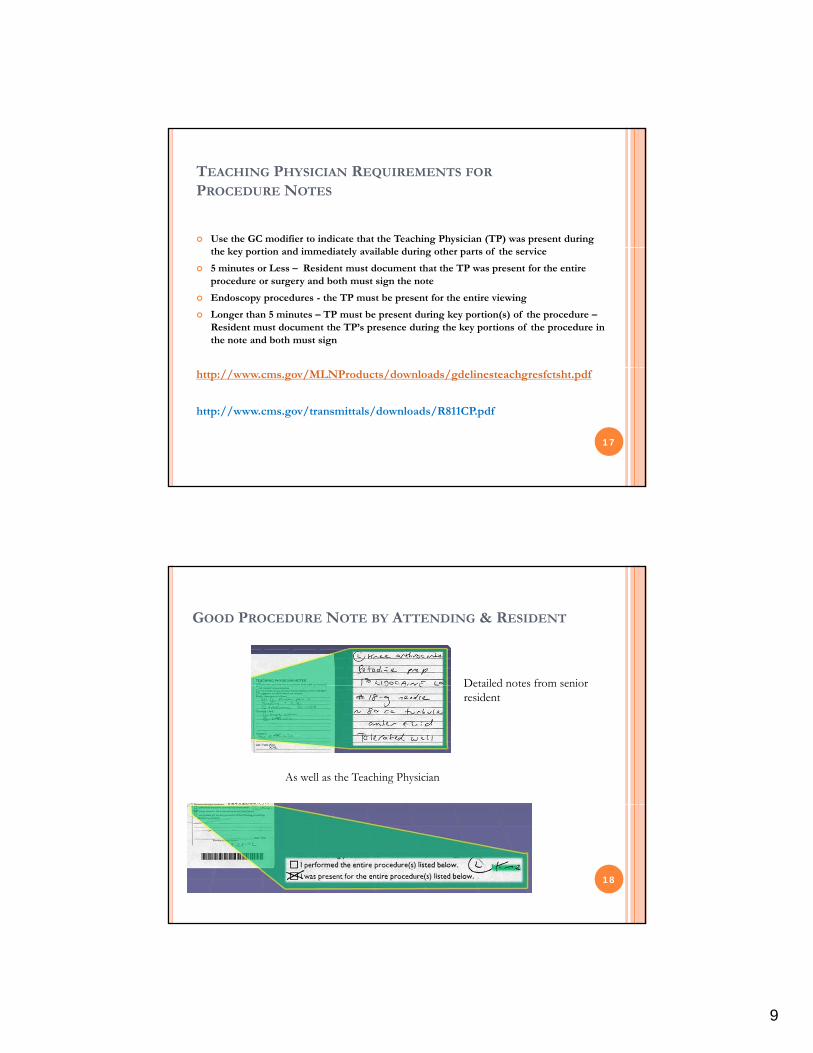
THE TP DOCUMENTATION DO’S AND DON'TS
• It has been clearly established that the following statements by the teaching physician, appended to the
id /f ll ’ ffi iresident/fellow’s note, are not sufficient to support a billable service.
16
9
TEACHING PHYSICIAN REQUIREMENTS FOR
PROCEDURE NOTES
Use the GC modifier to indicate that the Teaching Physician (TP) was present during the key portion and immediately available during other parts of the service
5 minutes or Less – Resident must document that the TP was present for the entire procedure or surgery and both must sign the note
Endoscopy procedures - the TP must be present for the entire viewing
Longer than 5 minutes – TP must be present during key portion(s) of the procedure –Resident must document the TP’s presence during the key portions of the procedure in the note and both must sign
http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf
http://www.cms.gov/transmittals/downloads/R811CP.pdf
17
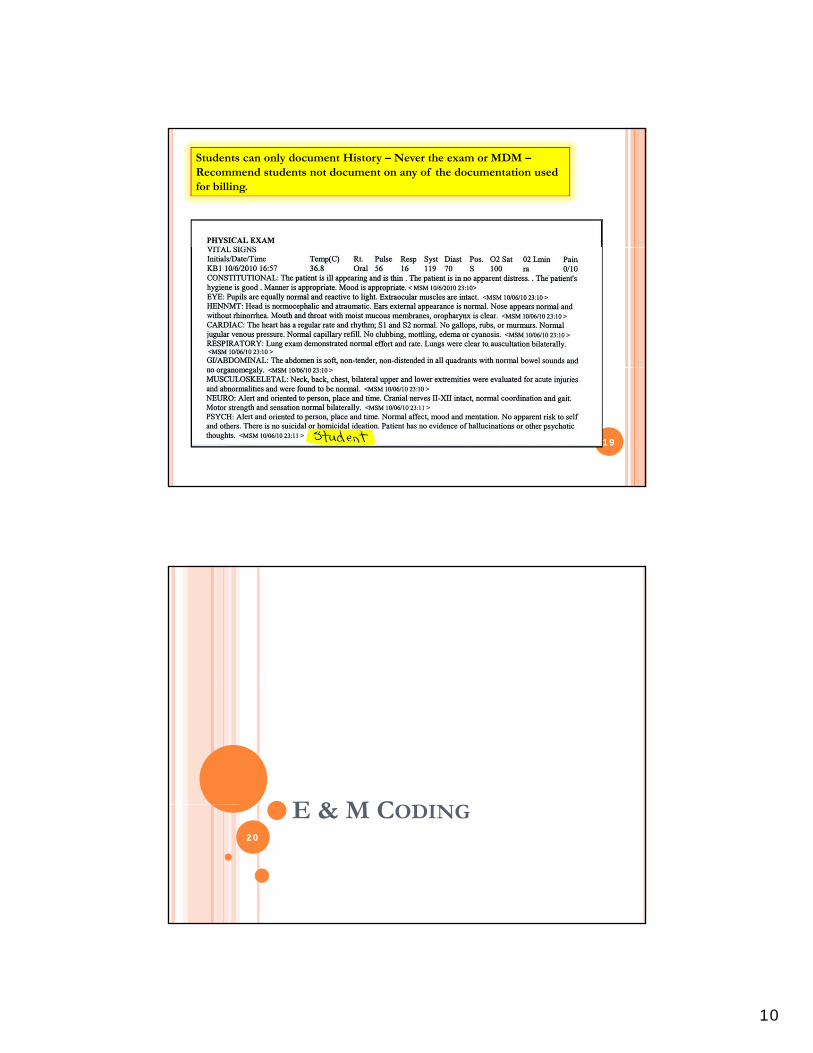
GOOD PROCEDURE NOTE BY ATTENDING & RESIDENT
Detailed notes from seniorDetailed notes from senior resident
As well as the Teaching Physician
18
10
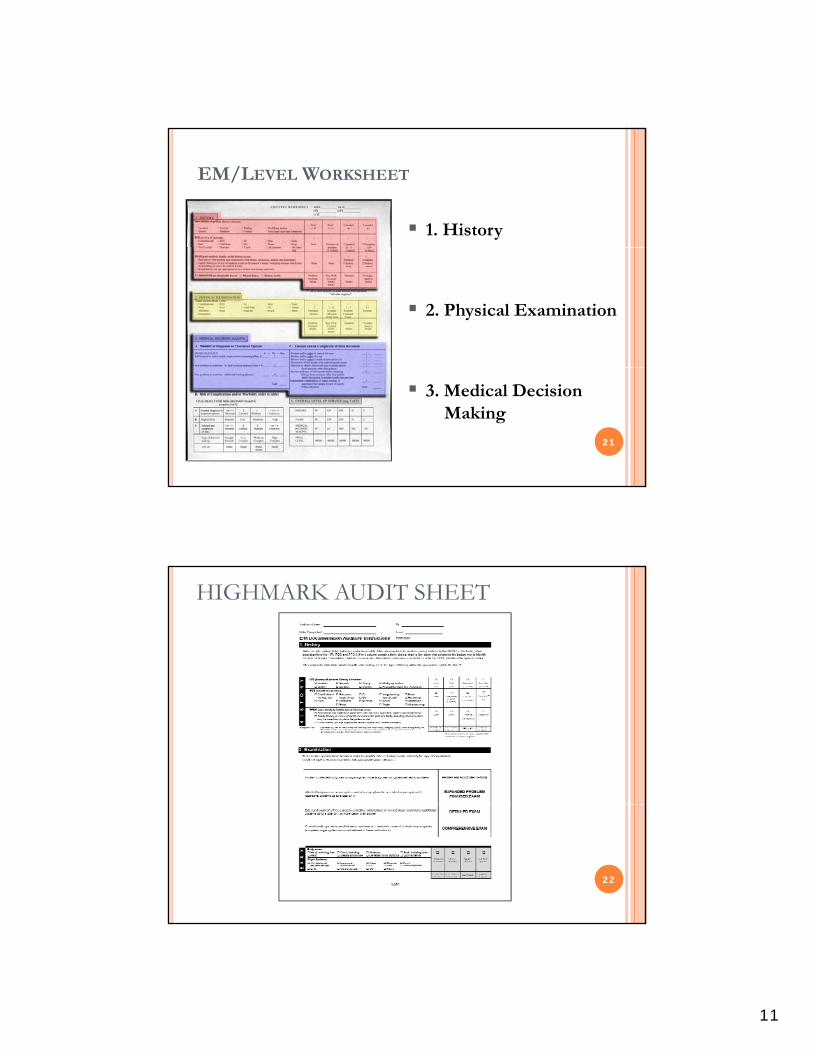
Students can only document History – Never the exam or MDM –Recommend students not document on any of the documentation used for billing.
19
E & M CODI GE & M CODING20
11
EM/LEVEL WORKSHEET
1. History
2. Physical Examination
21
3. Medical Decision Making
HIGHMARK AUDIT SHEET
22
12
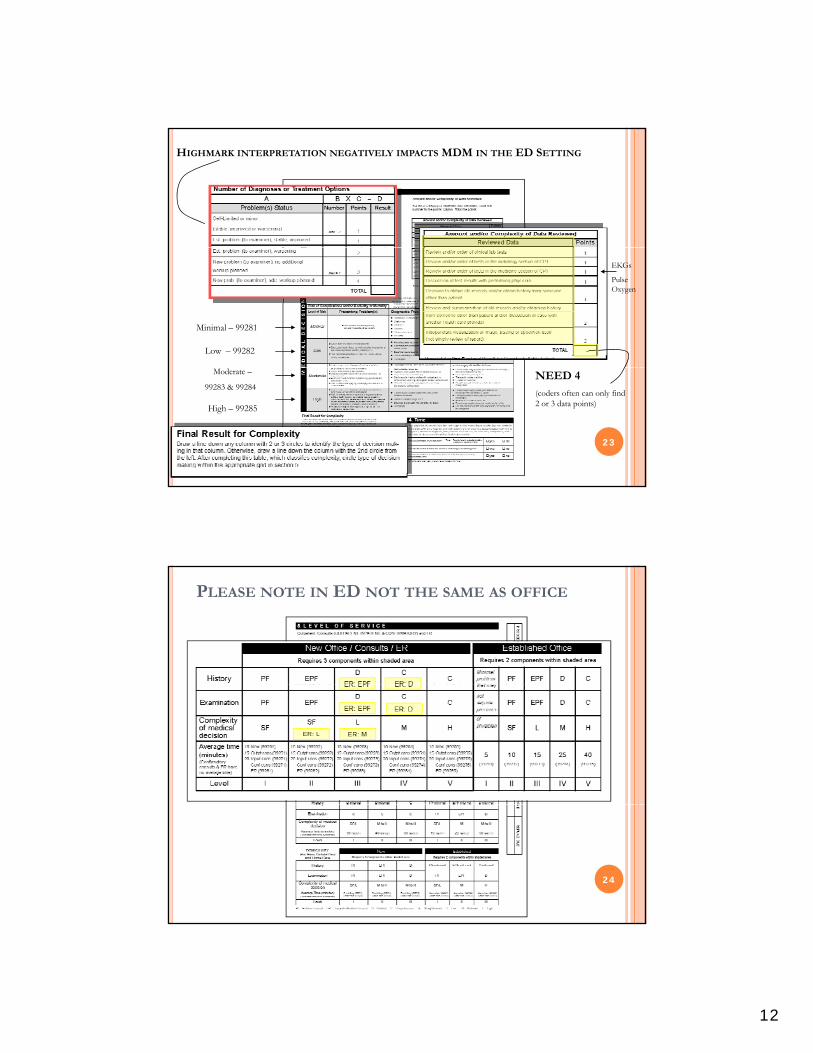
HIGHMARK INTERPRETATION NEGATIVELY IMPACTS MDM IN THE ED SETTING
Minimal – 99281
Low – 99282
EKGs
Pulse Oxygen
23
Moderate –
99283 & 99284
High – 99285
NEED 4
(coders often can only find 2 or 3 data points)
PLEASE NOTE IN ED NOT THE SAME AS OFFICE
24
13
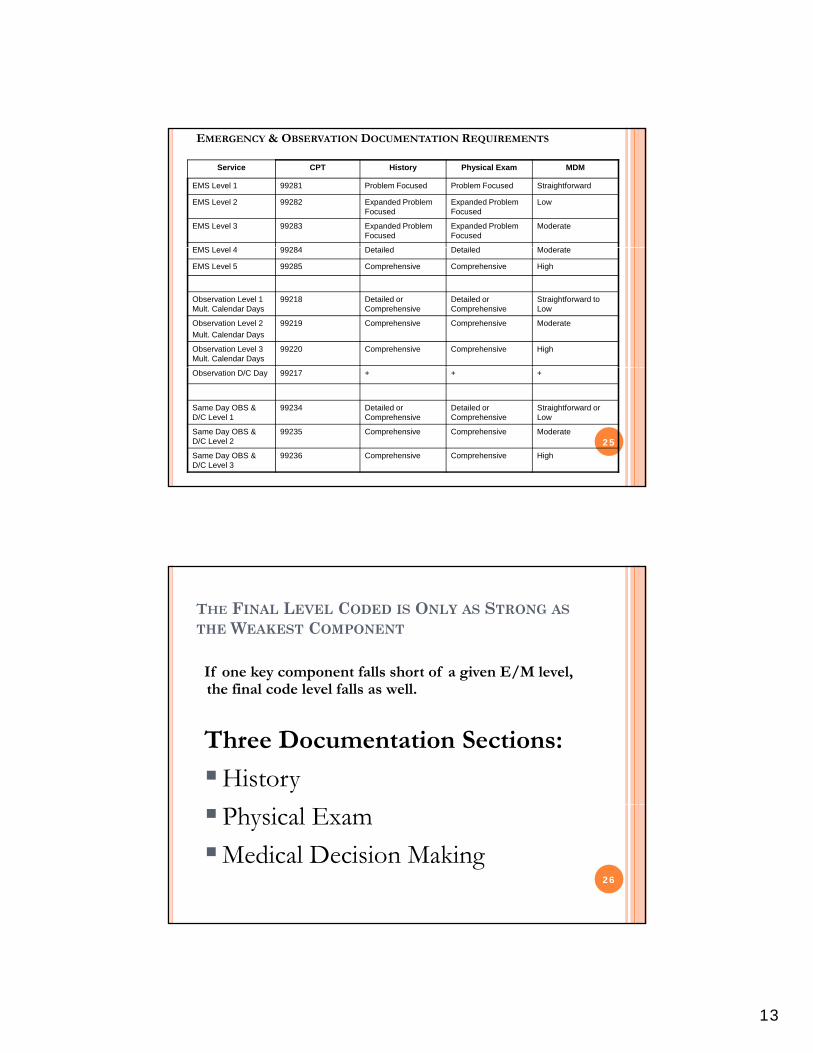
EMERGENCY & OBSERVATION DOCUMENTATION REQUIREMENTS
Service CPT History Physical Exam MDM
EMS Level 1 99281 Problem Focused Problem Focused Straightforward
EMS Level 2 99282 Expanded Problem Focused
Expanded Problem Focused
Low
EMS Level 3 99283 Expanded Problem Focused
Expanded Problem Focused
Moderate
EMS L l 4 99284 D t il d D t il d M d tEMS Level 4 99284 Detailed Detailed Moderate
EMS Level 5 99285 Comprehensive Comprehensive High
Observation Level 1 Mult. Calendar Days
99218 Detailed or Comprehensive
Detailed or Comprehensive
Straightforward to Low
Observation Level 2
Mult. Calendar Days
99219 Comprehensive Comprehensive Moderate
Observation Level 3 Mult. Calendar Days
99220 Comprehensive Comprehensive High
25
Observation D/C Day 99217 + + +
Same Day OBS & D/C Level 1
99234 Detailed or Comprehensive
Detailed or Comprehensive
Straightforward or Low
Same Day OBS & D/C Level 2
99235 Comprehensive Comprehensive Moderate
Same Day OBS & D/C Level 3
99236 Comprehensive Comprehensive High
THE FINAL LEVEL CODED IS ONLY AS STRONG AS
THE WEAKEST COMPONENT
If one key component falls short of a given E/M level, h fi l d l l f ll llthe final code level falls as well.
Three Documentation Sections:
History
26
Physical Exam
Medical Decision Making
14
CHIEF COMPLAINT
Required for all visit and levelsRequired for all visit and levels of service. This must be noted for every patient seen in the Emergency Department
27
HPI – ALWAYS TRY TO LIST FOUR OF THE FOLLOWING
ELEMENTS THIS ALLOWS THE CODERS TO POTENTIALLY
MEET A LEVEL 99285
Modifying Factors
Quality
Severity
Timing
Context
Location
Duration
Associated Signs
28
Timing Associated Signs & Symptoms
15
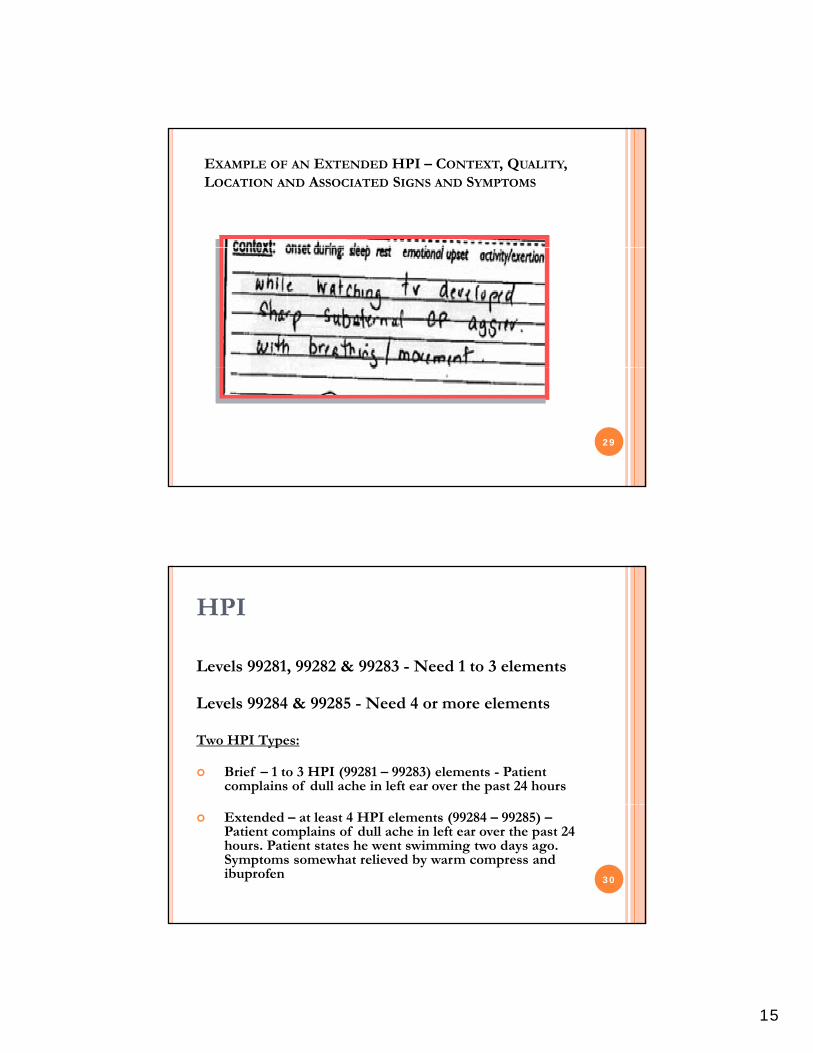
EXAMPLE OF AN EXTENDED HPI – CONTEXT, QUALITY, LOCATION AND ASSOCIATED SIGNS AND SYMPTOMS
29
HPI
Levels 99281, 99282 & 99283 - Need 1 to 3 elements
Levels 99284 & 99285 - Need 4 or more elements
Two HPI Types:
Brief – 1 to 3 HPI (99281 – 99283) elements - Patient complains of dull ache in left ear over the past 24 hours
Extended – at least 4 HPI elements (99284 – 99285) –Patient complains of dull ache in left ear over the past 24 hours. Patient states he went swimming two days ago. Symptoms somewhat relieved by warm compress and ibuprofen 30
16
REVIEW OF SYSTEMS
Levels 99281, 99282 and 99283 require one system
Level 99284 requires 2 to 9 systems
Level 99285 requires 10 systems or more unless you note that all systems were negative except as marked or you note that the history collection was limited due to the patient’s altered mental status or patient acuity
31
THIRD DOCUMENTATION REQUIREMENT – REVIEW OF
SYSTEMS
Constitutional
Eyes
Ears, Nose, Mouth, Throat
1. Complete ROS consists of at least 10 organ systems
2. The ROS can be documented by listing the system followed by negative or normal
3. The ROS can also be documented by listing
Cardiovascular
Respiratory
Gastrointestinal
Genitourinary
Musculoskeletal
Integumentary
N l i l
y gthe signs or symptoms that the patient has denied
4. Documenting “review of systems negative or normal” does not meet any numerical requirement and is not considered a ROS. Always indicate a “negative” or “positive” statement for each system
5. Documenting any pertinent positives and negative combined with the statement “all
32
Neurological
Psychiatric
Endocrine
Hematologic/Lymphatic
Allergic/immunologic
negative combined with the statement all other systems negative” will be considered a complete ROS. However, “all other systems negative” indicates that the physician has reviewed all 14 systems
17
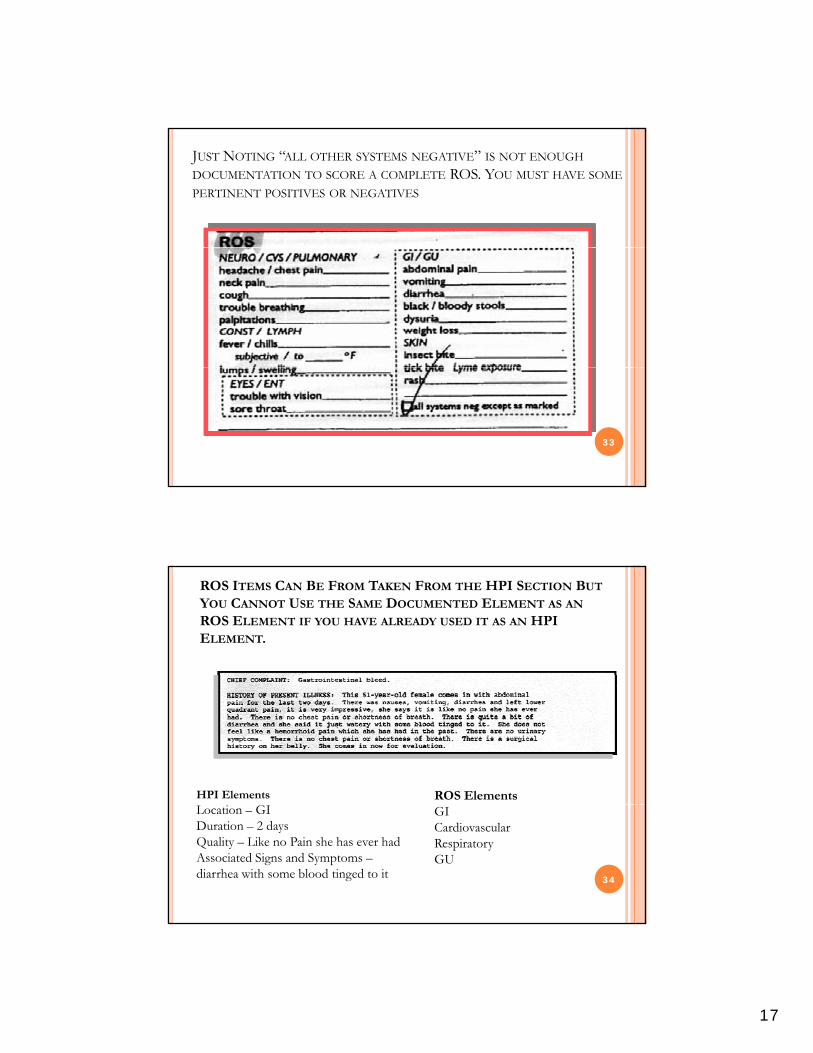
JUST NOTING “ALL OTHER SYSTEMS NEGATIVE” IS NOT ENOUGH
DOCUMENTATION TO SCORE A COMPLETE ROS. YOU MUST HAVE SOME
PERTINENT POSITIVES OR NEGATIVES
33
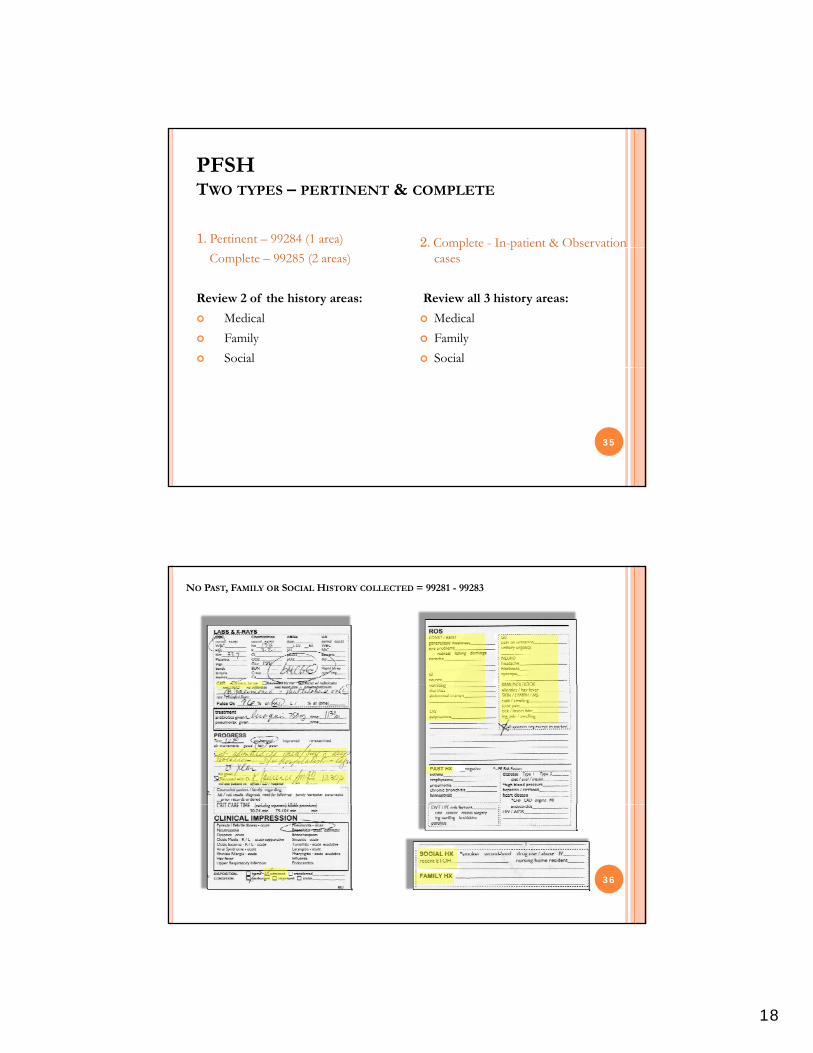
ROS ITEMS CAN BE FROM TAKEN FROM THE HPI SECTION BUT
YOU CANNOT USE THE SAME DOCUMENTED ELEMENT AS AN
ROS ELEMENT IF YOU HAVE ALREADY USED IT AS AN HPI ELEMENT.
HPI Elements ROS Elements
34
Location – GIDuration – 2 daysQuality – Like no Pain she has ever hadAssociated Signs and Symptoms –diarrhea with some blood tinged to it
GICardiovascularRespiratoryGU
18
PFSHTWO TYPES – PERTINENT & COMPLETE
1. Pertinent – 99284 (1 area) 2. Complete - In-patient & Observation Complete – 99285 (2 areas)
Review 2 of the history areas:
Medical
Family
Social
p pcases
Review all 3 history areas:
Medical
Family
Social
35
NO PAST, FAMILY OR SOCIAL HISTORY COLLECTED = 99281 - 99283
36
19
E/M DOCUMENTATION INSTRUCTIONS
*Complete PFSH:
2 hx areas: a) Estab pts, office (outpt) care; domiciliary care; home care
37
2 hx areas: a) Estab pts, office (outpt) care; domiciliary care; home care b) Emergency Dept c) Subseq nursing facility care
3 hx areas: a) New pts, office (outpt) care; domiciliary care; home care b) Consultations c) Initial hospital care d) Hospital Observatione) Comprehensive nursing facility assessments
THE EMERGENCY MEDICINE CAVEAT
“If the physician is unable to obtain history from the patient or other source the record should describe thepatient or other source, the record should describe the patient’s medical condition/other circumstance, which precludes obtaining a history.” CMS 1995 Guidelines
Urgent/emergency conditions
P i ’ i bili i
38
Patient’s inability to communicate
Patient at a very high level of risk
Immediate action necessary
20
You must state the reason the history is not obtained and
THE EMERGENCY MEDICINE CAVEAT
history is not obtained and documented on the record.
Must act quickly to prevent deterioration of patient status
39
p s s
Patient too ill to speak, uncooperative, unconscious
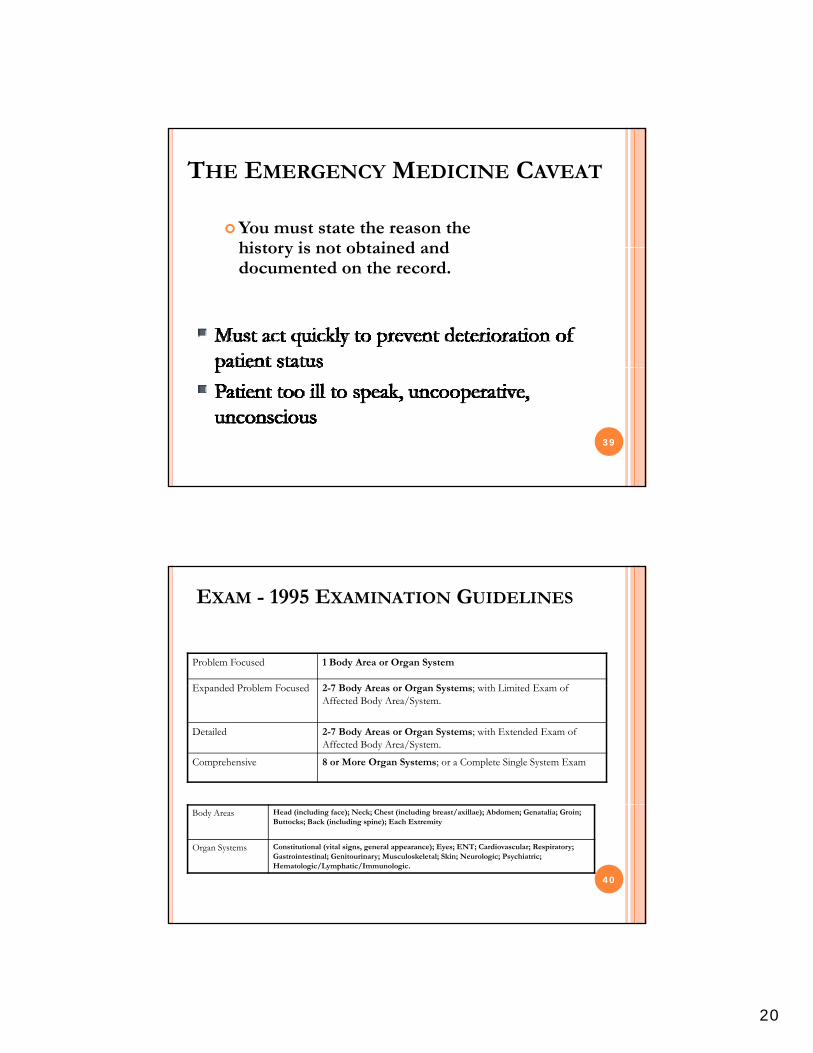
EXAM - 1995 EXAMINATION GUIDELINES
Problem Focused 1 Body Area or Organ System
E d d P bl F d 2 7 B d A O S i h Li i d E fExpanded Problem Focused 2-7 Body Areas or Organ Systems; with Limited Exam of Affected Body Area/System.
Detailed 2-7 Body Areas or Organ Systems; with Extended Exam of Affected Body Area/System.
Comprehensive 8 or More Organ Systems; or a Complete Single System Exam
40
Body Areas Head (including face); Neck; Chest (including breast/axillae); Abdomen; Genatalia; Groin; Buttocks; Back (including spine); Each Extremity
Organ Systems Constitutional (vital signs, general appearance); Eyes; ENT; Cardiovascular; Respiratory; Gastrointestinal; Genitourinary; Musculoskeletal; Skin; Neurologic; Psychiatric; Hematologic/Lymphatic/Immunologic.
21
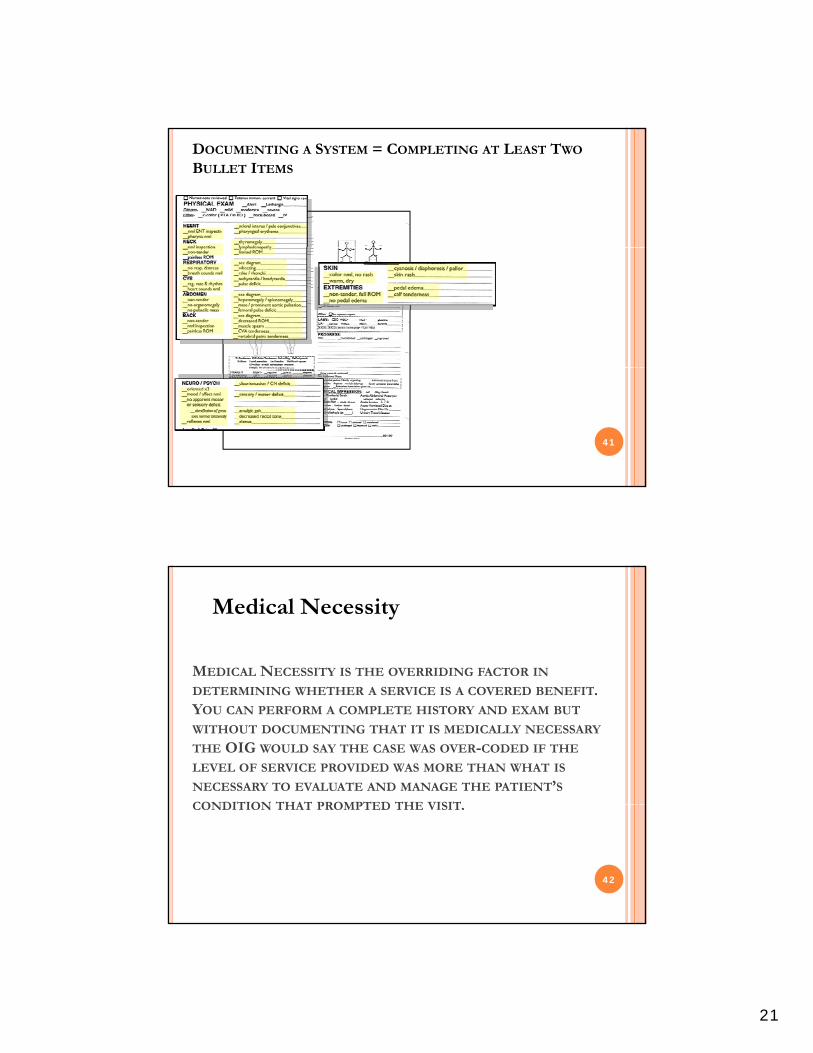
DOCUMENTING A SYSTEM = COMPLETING AT LEAST TWO
BULLET ITEMS
41
MEDICAL NECESSITY IS THE OVERRIDING FACTOR IN
Medical Necessity
DETERMINING WHETHER A SERVICE IS A COVERED BENEFIT. YOU CAN PERFORM A COMPLETE HISTORY AND EXAM BUT
WITHOUT DOCUMENTING THAT IT IS MEDICALLY NECESSARY
THE OIG WOULD SAY THE CASE WAS OVER-CODED IF THE
LEVEL OF SERVICE PROVIDED WAS MORE THAN WHAT IS
NECESSARY TO EVALUATE AND MANAGE THE PATIENT’SCONDITION THAT PROMPTED THE VISITCONDITION THAT PROMPTED THE VISIT.
42

22
MEDICAL DECISION MAKING
Number of Dx or Treatment Options
Almost all ED patients qualify as a new problem to the examiner. They only differ based on whether or not any additional work-up is planned.
43
p p
NUMBER OF DIAGNOSIS OR TREATMENT
OPTIONS - CONTROVERSY
Method 1 - Counting any diagnostic work-up that occurs in the ED as additional work-up planned tends to cause many encounters to score to a higher MDM and E&M level than
h b d b d h f i bl F li i lwhat may be warranted based on the nature of presenting problem. From a clinical perspective it is hard to make the argument that a patient that presents with a sore throat and has a strep test done should be scored as Extensive with regards to the number of diagnoses or management options. This can lead to scoring low risk cases as 99284s simply because of the MDM scoring system.
Method 2 - For ED E&M services reserve the additional work-up planned for those patients who will receive additional work-up after the ED encounter. This will help your coders more clearly differentiate between 99283, 99284 and 99285 within your practice.
The 2 common interpretations are described above, however, Medicare carrier Highmark’s interpretation is an extension of #2. The state that the additional work-up must be after the current encounter and has to be performed by the same MD. Their position is that the ED MD would never be given credit for additional work-up planned.
44
23
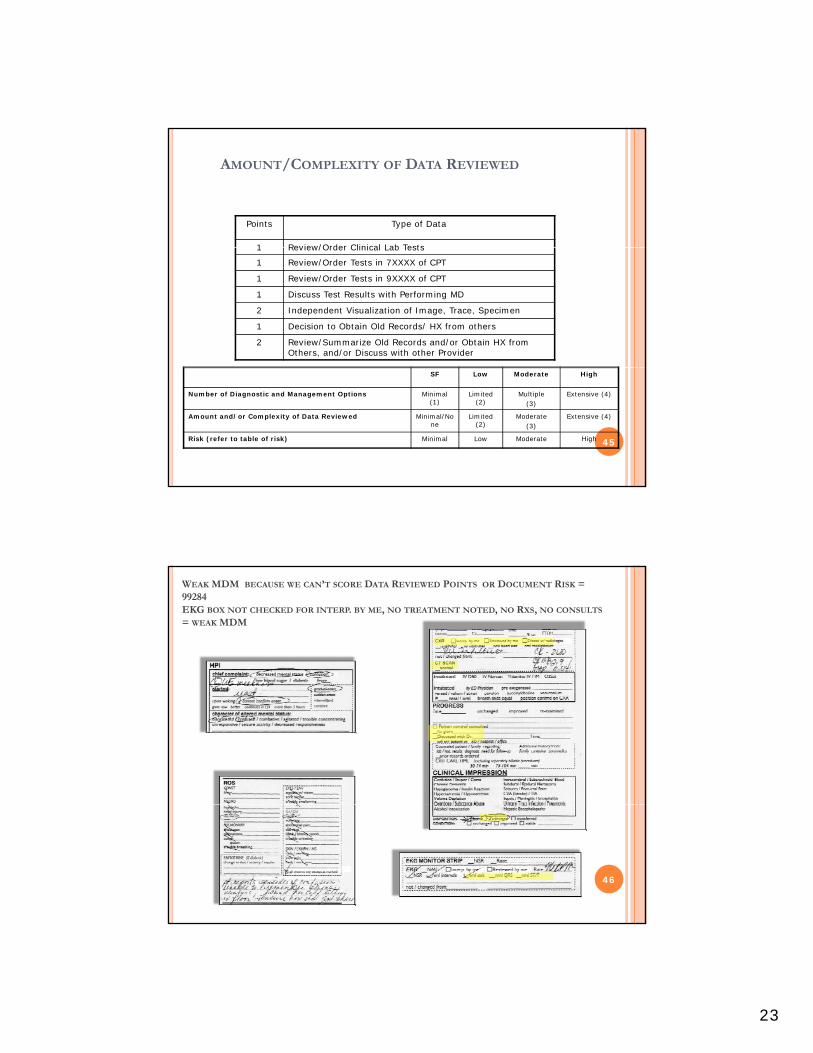
AMOUNT/COMPLEXITY OF DATA REVIEWED
Points Type of Data
1 Review/Order Clinical Lab Tests1 Review/Order Clinical Lab Tests
1 Review/Order Tests in 7XXXX of CPT
1 Review/Order Tests in 9XXXX of CPT
1 Discuss Test Results with Performing MD
2 Independent Visualization of Image, Trace, Specimen
1 Decision to Obtain Old Records/ HX from others
2 Review/Summarize Old Records and/or Obtain HX from Others, and/or Discuss with other Provider
45
SF Low Moderate High
Number of Diagnostic and Management Options Minimal (1)
Limited (2)
Multiple (3)
Extensive (4)
Amount and/or Complexity of Data Reviewed Minimal/None
Limited (2)
Moderate (3)
Extensive (4)
Risk (refer to table of risk) Minimal Low Moderate High
WEAK MDM BECAUSE WE CAN’T SCORE DATA REVIEWED POINTS OR DOCUMENT RISK = 99284EKG BOX NOT CHECKED FOR INTERP. BY ME, NO TREATMENT NOTED, NO RXS, NO CONSULTS
= WEAK MDM
46
24
Speaking with another healthSpeaking with another health care provider from another
practice or service = 2 MDM points – you must be specific and identify who you spoke
with.
47
Deciding to collect the history from the parents or others = 1 point
Summarizing and collecting the history from the parents = 2 points
48
25
Ordering an EKG = 1 MDM point
Doing the interpretation = 2 MDM points but you must indicate it was “my interpretation”
49
NO EXTRA MDM DATA POINTS SCORED
50
26
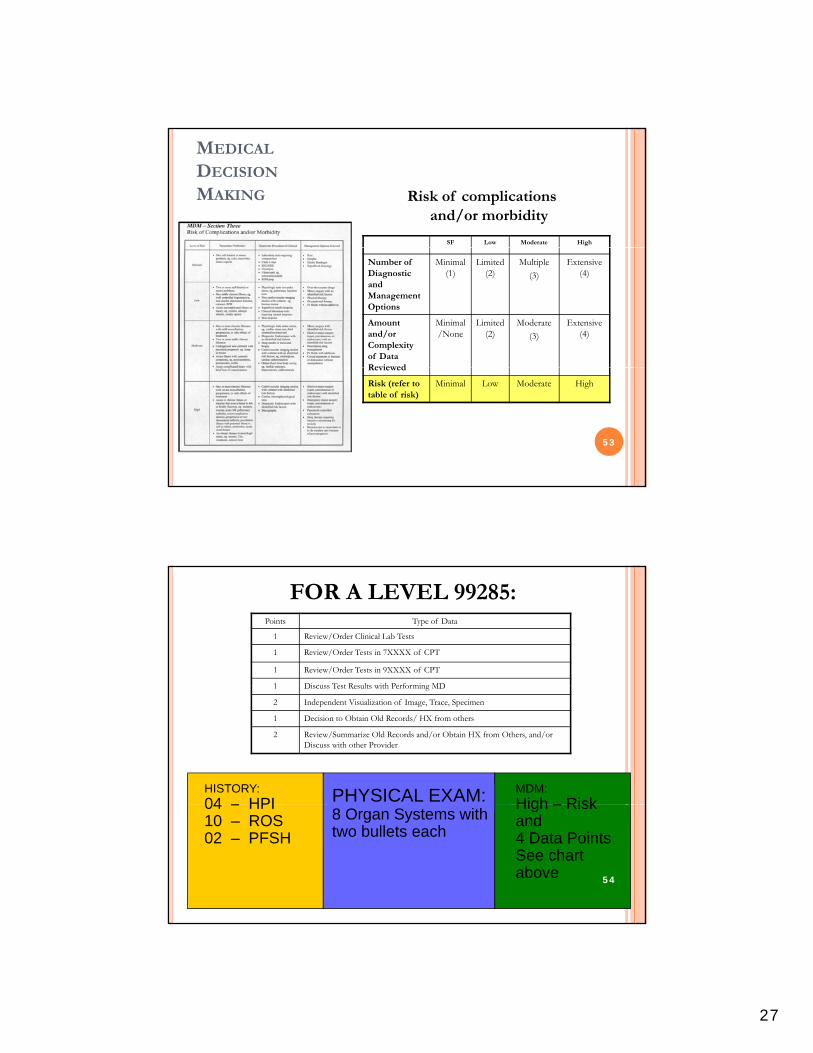
EXAMPLES OF T-SYSTEM BOXES THAT SCORE
MDM DATA POINTS
1. Hx – Exam Limited
3. X-Rays
51
2. ROS Box
4. Wound Description / Repair
MORE MDM DOCUMENTATION BOXES
5. Prior Records Reviewed & Counseled Patient etc.
6. Treatment / Intubated
527. EKG, Lab, X-Rays 8. Procedures
27
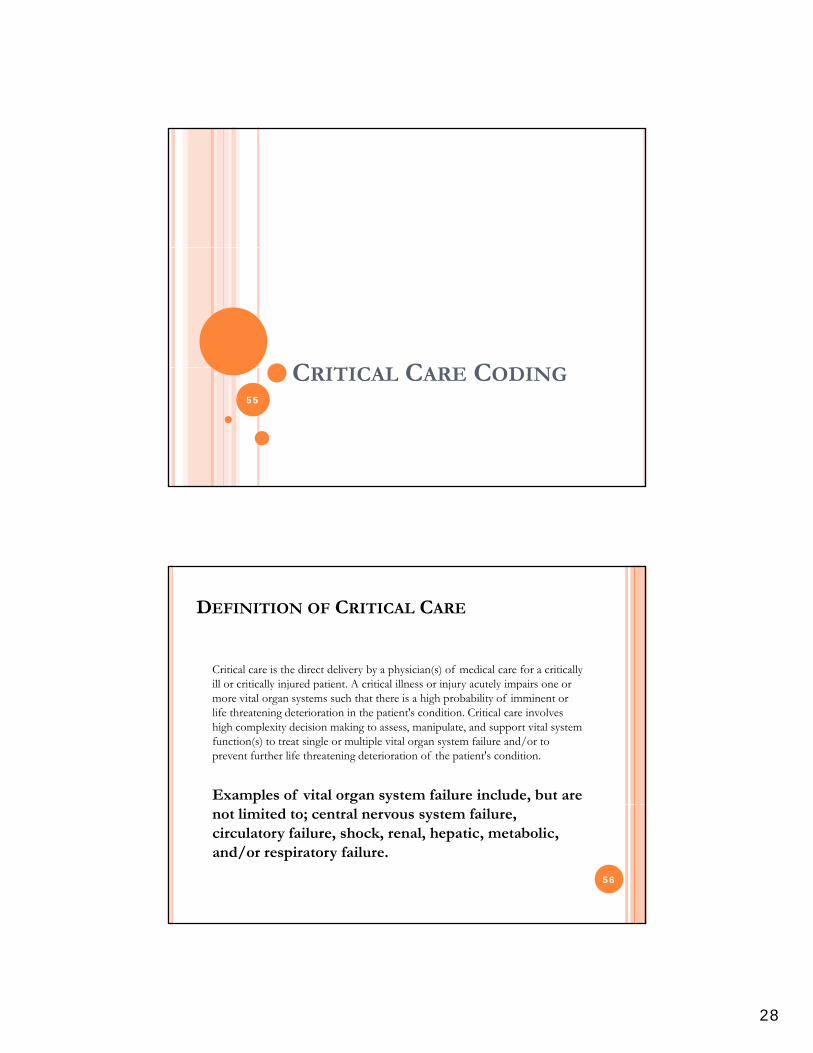
MEDICAL
DECISION
MAKING Risk of complications and/or morbidity
SF Low Moderate High
Number of Diagnostic and Management Options
Minimal (1)
Limited (2)
Multiple
(3)
Extensive (4)
Amount and/or Complexity of Data Reviewed
Minimal/None
Limited (2)
Moderate
(3)
Extensive (4)
Reviewed
Risk (refer to table of risk)
Minimal Low Moderate High
53
FOR A LEVEL 99285:Points Type of Data
1 Review/Order Clinical Lab Tests
1 Review/Order Tests in 7XXXX of CPT
1 Review/Order Tests in 9XXXX of CPT
1 Disc ss Test Res lts ith Performing MD
HISTORY:04 – HPI PHYSICAL EXAM: MDM:
High – Risk
1 Discuss Test Results with Performing MD
2 Independent Visualization of Image, Trace, Specimen
1 Decision to Obtain Old Records/ HX from others
2 Review/Summarize Old Records and/or Obtain HX from Others, and/or Discuss with other Provider
04 – HPI10 – ROS02 – PFSH
8 Organ Systems with two bullets each
High – Risk and4 Data PointsSee chart above 54
28
CRITICAL CARE CODINGCRITICAL CARE CODING55
DEFINITION OF CRITICAL CARE
Critical care is the direct delivery by a physician(s) of medical care for a critically ill or critically injured patient A critical illness or injury acutely impairs one orill or critically injured patient. A critical illness or injury acutely impairs one or more vital organ systems such that there is a high probability of imminent or life threatening deterioration in the patient's condition. Critical care involves high complexity decision making to assess, manipulate, and support vital system function(s) to treat single or multiple vital organ system failure and/or to prevent further life threatening deterioration of the patient's condition.
Examples of vital organ system failure include, but are not limited to; central nervous system failure, circulatory failure, shock, renal, hepatic, metabolic, and/or respiratory failure.
56
29
MEDICARE POLICY FOR CRITICAL CARE
Before coding critical care ask and answer the following questions:
1. Does the record demonstrate work preformed during the encounter is more intensive than the work of other E/M codes of the same time duration?
2. Does the record demonstrate the patient has acute impairment of one or more vital organ systems and has a high probability of imminent or life-threatening deterioration?
3. Does your documentation demonstrate; direct personal involvement, frequent assessments, a high-complexity of MDM and urgent interventions?
4. Is the time spent specifically recorded?
57
ACTIVITIES QUALIFYING FOR CRITICAL CARE
Time spent w/patient
Reviewing test results
Discussing patient’s care w/medical staff
Documenting critical care services in medical services record
Discussing patient’s condition with family (but onlyquestions regarding treatment)questions regarding treatment)
58
30
OTHER CODING REQUIREMENTS
Only one physician may bill for critical care services during any one single period of time even if more than one physician is providing care to a critically ill/injured patient. Both of the following medical review criteria must be met in addition to the CPT definitions:
Clinical Condition Criterion
There is a high probability of sudden, clinically significant, or life threatening deterioration in the patient’s condition which requires the highest level of physician preparedness to intervene urgently.
Treatment Criterion
Critical care services require direct personal management by the physician. They are life and organ supporting interventions that require frequent personal assessmentlife and organ supporting interventions that require frequent, personal assessment and manipulation by the physician. Withdrawal of, or failure to initiate these interventions on an urgent basis would likely result in sudden, clinically significant or life threatening deterioration in the patient’s condition.
Providing medical care to a critically ill patient should not be automatically determined to be a critical care service for the sole reason that the patient is critically ill. The physician service must be medically necessary and meet the definition of critical care services as described previously in order to be considered covered. 59
A split/shared E/M service performed by a physician and a qualified NPP of the same group
No Shared Visits When Billing for Critical Care
practice (or employed by the same employer) cannot be reported as a critical care service. Critical care services are reflective of the care and management of a critically ill or critically injured patient by an individual physician or qualified NPP for the specified reportable period of time and shall n t b r pr nt ti f mbin d r i
60
not be representative of a combined service between a physician and a qualified NPP.
31
TP CRITICAL CARE RULES
Time spent teaching may not be counted towards critical care time.
Ti t b th id t i th b f th T hi Time spent by the resident in the absence of the Teaching Physician is not counted toward critical care time.
The Teaching Physician must be present for all critical care time billed.
Only time spent by the resident and Teaching Physician together with the patient, or time spent by the Teaching Physician alone with the patient, may be counted towards critical care time.
The TP must document their PERSONAL time involved. 61
Since critical care is a time-based code, the physician’s progress note must contain documentation of the total time involved providing critical care services.
Time involved performing procedures that are not bundled into critical care (i.e., billed separately) may not be included and counted toward critical care time. The physician’s progress note must document that time involved in
Medical Review Guidelines regarding “Full Attention”
d d d d w d p y p g d v v dthe performance of separately billable procedures was not counted toward critical care time.
Time involved with family members or other surrogate decision makers, whether to obtain a history or to discuss treatment options may be counted toward critical care time only when the patient is unable or incompetent to participate in giving a history and/or making treatment decisions and the discussion is absolutely necessary for treatment decisions under consideration that day, and all of the following are documented in the physician’s progress note for that day:
• the reason the patient was unable or incompetent to participate in giving history and/or making treatment decisions
• the necessity of the discussion (e g no other source was available to obtain a history” or “because
62
• the necessity of the discussion (e.g., no other source was available to obtain a history or because the patient was deteriorating so rapidly needed to discuss treatment options with family immediately”)
• the treatment decisions for which the discussion was needed• a summary of the discussion as related to the treatment decision.
The physician’s progress note must link the family discussion to a specific treatment issue and explain why the discussion was necessary on that day. All other family discussions, no matter how lengthy, may not be counted towards critical care time.
32
CRITICAL CARE
99291: Code used to report the 1st hour ( up to 74 i ) i d f iminutes) on a given date of service.
99292: Code used for each 30 minutes beyond the 1st
hour.
Critical care of less than 30 minutes may not be d lreported separately
63
BUNDLED SERVICES
Interpretation of cardiac output measurements
Chest x-rays
Blood gases
Blood draw from specimen
Analysis of information data stored in computers
Gastric intubation
Pulse oximetry
Temporary transcutaneous pacing
Ventilator Management Ventilator Management
Vascular access procedures
Family psychotherapy
64
33
OBSERVATION CODINGOBSERVATION CODING65
OBSERVATION CARE DEFINED
“Observation care is a well-defined set of specific, clinically appropriate services, which include ongoing short term treatment, assessment, and reassessment, that are furnished while a decision is being made regarding whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital.” – Highmark/CMS
66
34
IT IS IMPORTANT TO DOCUMENT OBSERVATION
CORRECTLY BECAUSE:
OIG
CERT findings of inappropriate admits
RAC findings – lack of medical necessity for short stays
Coding and Billing rules are confusing
Hospital and Physician billing both depend on time line being establishedline being established
67
OBSERVATION REQUIREMENTS
Intended for short stays of 24 – 48 hours
Out-patient locations 22 or 23 Out patient locations 22 or 23
A written order to begin observation services is required
Start time must be documented
End time must be documented
Services provided must be consistent with the order
68
35
OBSERVATION DOCUMENTATION
Medical record must demonstrate:
Consistency between the practitioner intent and services provided
Medical necessity of services
Medical appropriateness of the observation stay
**Include a dated and timed order for observation, interval progress notes and a discharge note**
69
OBSERVATION SERVICES
99217 –Observation care discharge
99218–99220 Initial Observation care
99224-99226-Subsequent Observation care
99234–99236 Observation or Inpatient Care Services (Including Admission and Discharge Services)(Including Admission and Discharge Services)
70
36
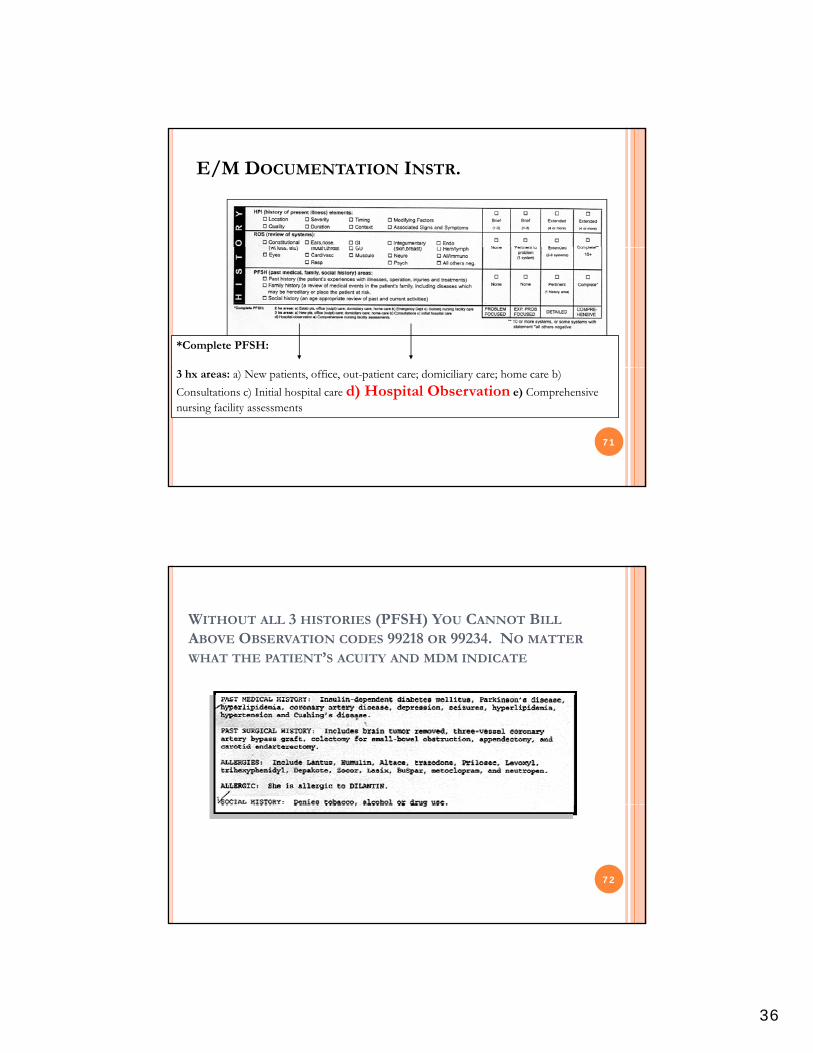
E/M DOCUMENTATION INSTR.
*Complete PFSH:
71
3 hx areas: a) New patients, office, out-patient care; domiciliary care; home care b)
Consultations c) Initial hospital care d) Hospital Observation e) Comprehensive nursing facility assessments
WITHOUT ALL 3 HISTORIES (PFSH) YOU CANNOT BILL
ABOVE OBSERVATION CODES 99218 OR 99234. NO MATTER
WHAT THE PATIENT’S ACUITY AND MDM INDICATE
72
37
PROCEDURE NOTESPROCEDURE NOTES73
INTUBATION- NEED TO KNOW; SIZE OF THE TUBE, HOW IT WAS
PLACED, CONFIRM CORRECT PLACEMENT, POST PROCEDURE PATIENT
STATUS
The patient was positioned appropriately and a # 4endotracheal tube was placed under direct laryngoscopy. p y g pyCorrect placement was confirmed by presence of bilateral breath sounds without air sounds in the abdomen on auscultation. A CO2 monitor was also used to confirm tracheal placement of the ET tube.
A chest x-ray was ordered to assess for pneumothorax and verify endotracheal tube placement.y p
The patient tolerated the procedure well and there were no complications.
74
38
LUMBAR PUNCTURE – NEED TO KNOW; ANESTHESIA TYPE, PREPPED AND
DRAPED, SIZE OF NEEDLE, WHERE IT WAS INSERTED, HOW MUCH FLUID WAS REMOVED, TESTS ORDERED, AND PATIENT’S POST PROCEDURE STATUS
Procedure - Lumbar Puncture
Indication meningitisIndication – meningitis
Anesthesia - local 1% lidocaine w/ epi. Informed consent was obtained from the patient's mother. The area was prepped and draped in the usual sterile fashion. Using landmarks, a 22 gauge spinal needle was inserted in the L4-L5
Th t l t d d th ispace. The stylet was removed and the opening pressure was measured at 18 cm of water. 4cc of clear fluid was collected and sent for routine studies. CSF was also sent for HSV and EBV PCR. The patient tolerated the procedure well. There was no blood loss or hematoma. 75
DOCUMENTING THE INTERPRETATION OF A
12 LEAD EKG
Document at least 3 of the following 6 elements:
Rh h d Rhythm and rate
Axis
Intervals
ST segment change
Comparison to prior EKG
Diagnosis (i.e. “acute inferior MI”)
U l i di h h i i d b Use personal pronouns to indicate that the interpretation was done by the ED physician – “My interpretation follows”
76
39
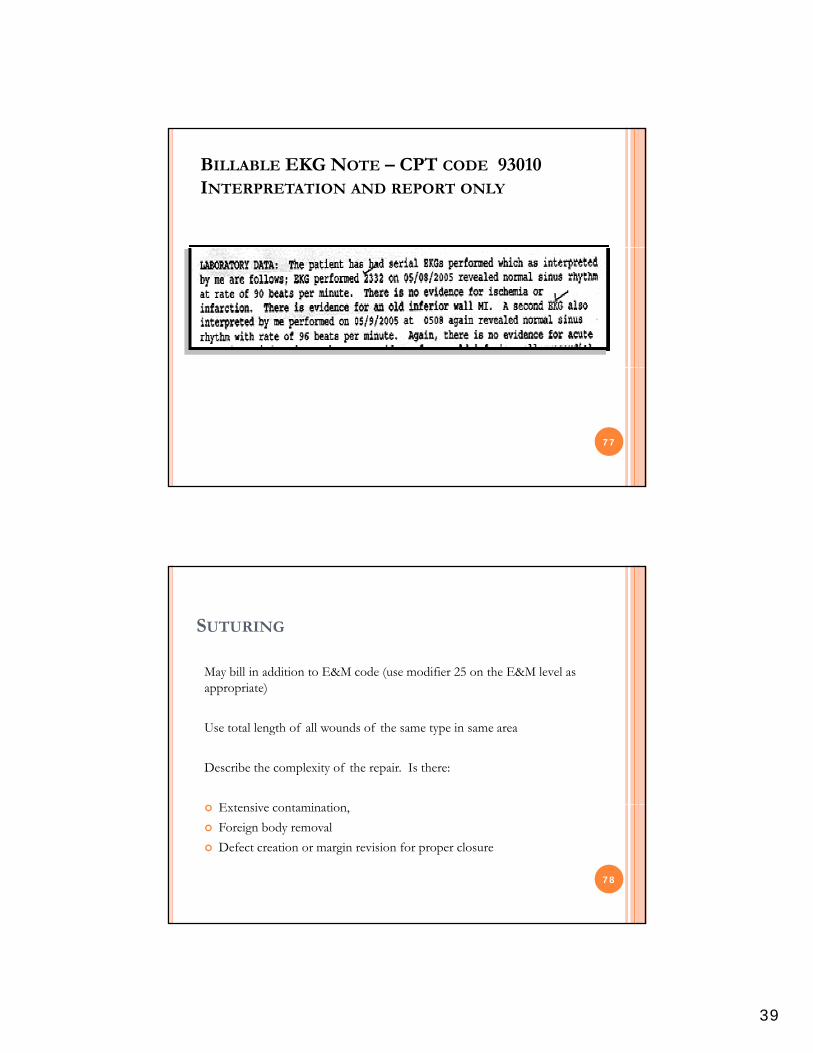
BILLABLE EKG NOTE – CPT CODE 93010 INTERPRETATION AND REPORT ONLY
77
SUTURING
May bill in addition to E&M code (use modifier 25 on the E&M level as i )appropriate)
Use total length of all wounds of the same type in same area
Describe the complexity of the repair. Is there:
E i i i Extensive contamination,
Foreign body removal
Defect creation or margin revision for proper closure
78
40
FAST EXAMS(FOCUSED ASSESSMENT BY SONOGRAPHY FOR TRAUMA)
a First look for fluid around the heart by performing a limited
Clinical approach- There is no fast exam specific code
a. First look for fluid around the heart by performing a limited trans thoracic echocardiography.
b. Then look for free fluid in the abdomen by performing a limited abdominal ultrasound.
Dual Service – 2 separate CPT codes.
93308 26 E h rdi r ph r l tim
79
93308-26 – Echocardiography real time
76705-26 – Ultrasound abdominal real time
*Remember you are required to retain the actual image in your documentation as well as your separately identifiable interpretive report.
FAST EXAM DOCUMENTATION
93308-26 – Looks for heart activity & pericardial fluid. It is directed to a single diagnostic problem.g g p
NOTE: Identify the presence or absence of pericardial fluid.
76705-26 – Looks for free fluid in the abdomen or hemoperitoneum.
80
NOTE: Identify the presence or absence of pericardial or intraperitoneal fluid.
41
OTHER BILLABLE ULTRASOUNDS
Abdominal Aortic Aneurysm – 76775-26 Echography abdominal B scan and/or realEchography, abdominal, B-scan and/or real time with image documentation limited (single organ, quadrant, follow-up)
Pericardial Fluid – 93308-26 Echocardiography, transthoracic real time with image
81
transthoracic, real-time with image documentation; limited
BILLABLE NOTE FOR 93308-26
82
42
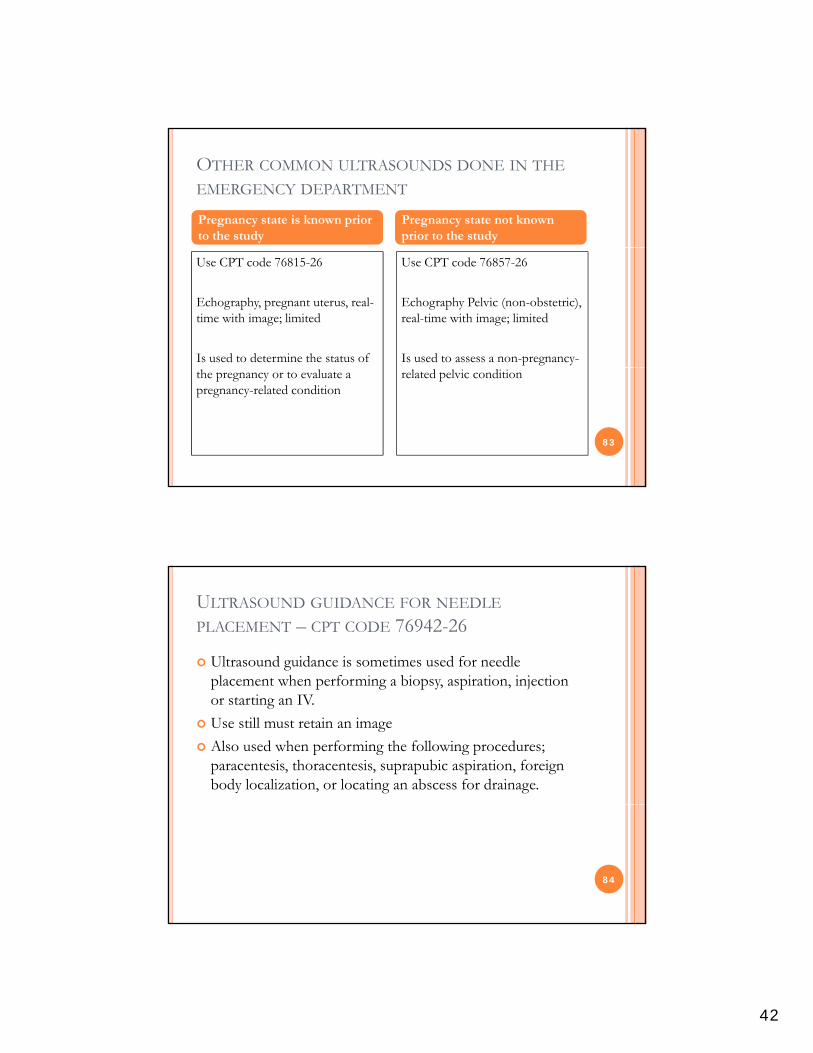
OTHER COMMON ULTRASOUNDS DONE IN THE
EMERGENCY DEPARTMENT
Pregnancy state is known prior to the study
Pregnancy state not known prior to the study
Use CPT code 76815-26
Echography, pregnant uterus, real-time with image; limited
Is used to determine the status of
Use CPT code 76857-26
Echography Pelvic (non-obstetric), real-time with image; limited
Is used to assess a non-pregnancy-
83
the pregnancy or to evaluate a pregnancy-related condition
related pelvic condition
ULTRASOUND GUIDANCE FOR NEEDLE
PLACEMENT – CPT CODE 76942-26
Ultrasound guidance is sometimes used for needle placement when performing a biopsy, aspiration, injectionplacement when performing a biopsy, aspiration, injection or starting an IV.
Use still must retain an image
Also used when performing the following procedures; paracentesis, thoracentesis, suprapubic aspiration, foreign body localization, or locating an abscess for drainage.
84
43
CONSCIOUS SEDATION = MODERATE SEDATION
Documentation Rules
Tell us who performs the procedure requiring sedation Tell us who provides the moderate sedation servicesp Tell us the patient’s age Tell us who is helping you to monitor the patient if you are also
performing the procedure Tell us about monitoring the patient’s cardiorespiratory functions
(pulse-oximetry, cardiorespiratory monitor, and blood pressure) for the duration of the procedure
Tell us when you start and stop the procedure
85
If the same person is performing the procedure and providing the moderate sedation then we need you to note that there was an independent trained observer assisting in the monitoring of the patients level of consciousness and physiological status – if the answer is yes we can bill for
the procedure and the conscious sedation – This is good news!
REMEMBER
Moderate Sedation begins with the administration of the sedating agent, requires continuous face-to-face attendance, and ends at the conclusion of personal contact by theand ends at the conclusion of personal contact by the physician providing the sedation.
99143 under 5 years - same physician performing the procedure
99148 under 5 years - different physician performing the procedure
99144 over 5 years - same physician performing the procedure
99149 over 5 years – different physician performing the procedure
86
In addition to 99143 & 99144 you can report 99145 for each additional 15 minutes beyond the first 30 minutes
In addition to 99148 & 99149 you can report 99150 for each additional 15 minutes beyond the first 30 minutes
44
CORRECT ORTHO CODES FOR FRACTURE/DISLOCATION
CARE DEPEND ON EXTENT OF TREATMENT
Coders apply orthopedic codes for theCoders apply orthopedic codes for the treatment of fractures, sprains and other orthopedic injuries only when the ED delivers definitive care, sometimes also called restorative care. Definitive care aims to repair, rather than simply stabilize the injury Along with casting, definitive careinjury. Along with casting, definitive care may also include splinting, strapping and/or pain management.
87
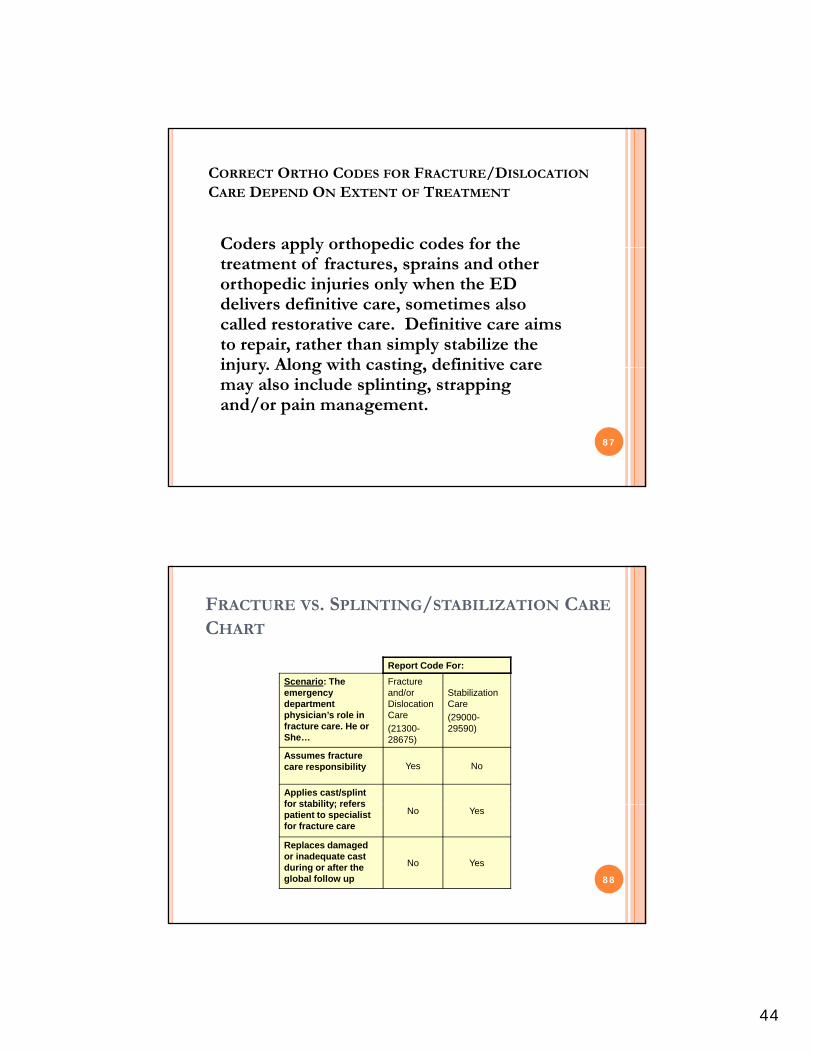
FRACTURE VS. SPLINTING/STABILIZATION CARE
CHART
Scenario: The Fracture
Report Code For:
emergency department physician’s role in fracture care. He or She…
and/or Dislocation Care
(21300-28675)
Stabilization Care
(29000-29590)
Assumes fracture care responsibility Yes No
Applies cast/splint for stability; refers
88
for stability; refers patient to specialist for fracture care
No Yes
Replaces damaged or inadequate cast during or after the global follow up
No Yes
45
BILLABLE NOTE FOR FRACTURE CARE
89
DEFINITIVE FRACTURE CARE IN THE ED
Many ED physicians provide definitive fracture care for fractures such as:fractures such as:
Finger Fractures 26720, 26750
Toes Fractures 28490, 28510
Clavicle Fractures 23500
Rib Fractures 21800
Nasal Fractures 21315
These are high RVU procedures and should not be overlooked. 90
46
SPLINTS
If a splint is applied and checked by the ED physician this level of care usually does not meet the requirement for y qdefinitive or restorative care but a splinting code can be billed for stabilizing the fracture.
Common splinting CPT codes include:
Finger 29130 g Short Arm 29125 Long Arm 29105 Short Leg 29515 Long Leg 29505 91
PQRS MEASURES IN THE
EDED92
47
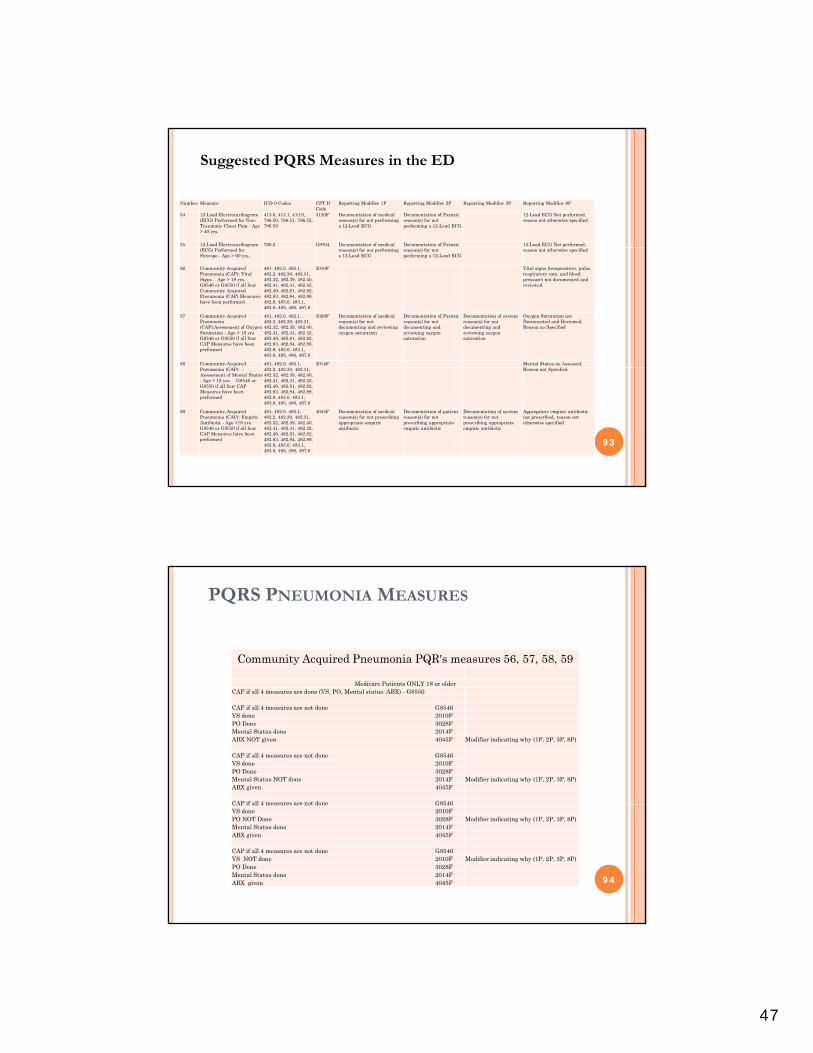
Number Measure ICD-9 Codes CPT II Code
Reporting Modifier 1P Reporting Modifier 2P Reporting Modifier 3P Reporting Modifier 8P
54 12-Lead Electrocardiogram (ECG) Performed for Non-Traumatic Chest Pain - Age > 40 yrs.
413.0, 413.1, 413.9, 786.50, 786.51, 786.52, 786.59
3120F Documentation of medical reason(s) for not performing a 12-Lead ECG
Documentation of Patient reason(s) for not performing a 12-Lead ECG
12-Lead ECG Not performed, reason not otherwise specified
55 12-Lead Electrocardiogram 780.2 G8704 Documentation of medical Documentation of Patient 12-Lead ECG Not performed,
Suggested PQRS Measures in the ED
(ECG) Performed for Syncope - Age > 60 yrs.
reason(s) for not performing a 12-Lead ECG
reason(s) for not performing a 12-Lead ECG
reason not otherwise specified
56 Community-Acquired Pneumonia (CAP): Vital Signs - Age > 18 yrs. G8546 or G8550 if all four Community Acquired Pneumonia (CAP) Measures have been performed
481, 482.0, 482.1, 482.2, 482.30, 482.31, 482.32, 482.39, 482.40, 482.41, 482.41, 482.42, 482.49, 482.81, 482.82, 482.83, 482.84, 482.89, 482.9, 483.0, 483.1, 483.8, 485, 486, 487.0
2010F Vital signs (temperature, pulse, respiratory rate, and blood pressure) not documented and reviewed
57 Community-Acquired Pneumonia (CAP):Assessment of Oxygen Saturation - Age > 18 yrs. G8546 or G8550 if all four CAP Measures have been performed
481, 482.0, 482.1, 482.2, 482.30, 482.31, 482.32, 482.39, 482.40, 482.41, 482.41, 482.42, 482.49, 482.81, 482.82, 482.83, 482.84, 482.89, 482.9, 483.0, 483.1, 483.8, 485, 486, 487.0
3028F Documentation of medical reason(s) for not documenting and reviewing oxygen saturation
Documentation of Patient reason(s) for not documenting and reviewing oxygen saturation
Documentation of system reason(s) for not documenting and reviewing oxygen saturation
Oxygen Saturation not Documented and Reviewed, Reason no Specified
58 Community-Acquired 481, 482.0, 482.1, 2014F Mental Status no Assessed,
93
Pneumonia (CAP): -Assessment of Mental Status - Age > 18 yrs. G8546 or G8550 if all four CAP Measures have been performed
482.2, 482.30, 482.31, 482.32, 482.39, 482.40, 482.41, 482.41, 482.42, 482.49, 482.81, 482.82, 482.83, 482.84, 482.89, 482.9, 483.0, 483.1, 483.8, 485, 486, 487.0
Reason not Specified
59 Community-Acquired Pneumonia (CAP): Empiric Antibiotic - Age >18 yrs. G8546 or G8550 if all four CAP Measures have been performed
481, 482.0, 482.1, 482.2, 482.30, 482.31, 482.32, 482.39, 482.40, 482.41, 482.41, 482.42, 482.49, 482.81, 482.82, 482.83, 482.84, 482.89, 482.9, 483.0, 483.1, 483.8, 485, 486, 487.0
4045F Documentation of medical reason(s) for not prescribing appropriate empiric antibiotic
Documentation of patient reason(s) for not prescribing appropriate empiric antibiotic
Documentation of system reason(s) for not prescribing appropriate empiric antibiotic
Appropriate empiric antibiotic not prescribed, reason not otherwise specified
PQRS PNEUMONIA MEASURES
Community Acquired Pneumonia PQR's measures 56, 57, 58, 59
Medicare Patients ONLY 18 or olderMedicare Patients ONLY 18 or olderCAP if all 4 measures are done (VS, PO, Mental status. ABX) - G8550
CAP if all 4 measures are not done G8546VS done 2010FPO Done 3028FMental Status done 2014FABX NOT given 4045F Modifier indicating why (1P, 2P, 3P, 8P)
CAP if all 4 measures are not done G8546VS done 2010FPO Done 3028FMental Status NOT done 2014F Modifier indicating why (1P, 2P, 3P, 8P)ABX given 4045F
CAP if all 4 measures are not done G8546
94
CAP if all 4 measures are not done G8546VS done 2010FPO NOT Done 3028F Modifier indicating why (1P, 2P, 3P, 8P)Mental Status done 2014FABX given 4045F
CAP if all 4 measures are not done G8546VS NOT done 2010F Modifier indicating why (1P, 2P, 3P, 8P)PO Done 3028FMental Status done 2014FABX given 4045F
48
REFERENCESREFERENCES95
REFERENCES
AMA CPT® Professional Edition ICD-9-CM For Physiciansy https://www.cms.gov/transmittals/downloads/R178CP.pdf http://www.cms.hhs.gov/Transmittals/Downloads/R1548CP.p
df http://www.cms.hhs.gov/MLNMattersArticles/downloads/M
M5993.pdf http://www.acep.org/
h // /Cli i l P i http://www.acep.org/Clinical---Practice-Management/Ultrasound/
http://www.acep.org/content.aspx?id=30428 http://www.cms.gov/ http://www.ahima.org/ 96