39 pasko pcrrt drug dosing
47
Drug Dosing in Drug Dosing in PCRRT PCRRT Deb Pasko, Pharm.D Deb Pasko, Pharm.D Pharmacy Clinical Specialist, Pharmacy Clinical Specialist, PICU PICU University of Michigan Health University of Michigan Health System System
-
Upload
dang-thanh-tuan -
Category
Health & Medicine
-
view
1.924 -
download
1
Transcript of 39 pasko pcrrt drug dosing

Drug Dosing in Drug Dosing in PCRRTPCRRT
Deb Pasko, Pharm.DDeb Pasko, Pharm.D
Pharmacy Clinical Specialist, PICUPharmacy Clinical Specialist, PICU
University of Michigan Health SystemUniversity of Michigan Health System

CRRT Solute RemovalCRRT Solute Removal
Lots of things Lots of things removed by CRRT!removed by CRRT!
Drugs, nutrients… Drugs, nutrients… FD&C Blue dye #1…FD&C Blue dye #1…
Crit Care Med, Mar Crit Care Med, Mar 20022002

Dialysate is used (lactated Ringers, PD solution, Dialysate is used (lactated Ringers, PD solution, etc)etc)
Good for small solute removal (<500 Da)Good for small solute removal (<500 Da) diffusion rate inversely proportional to MWdiffusion rate inversely proportional to MW
Efficiency of solute removal dependent onEfficiency of solute removal dependent on Blood flowBlood flow Dialysate flow Dialysate flow Filter typeFilter type Solute molecular weightSolute molecular weight
Less good for larger solutes (MM, Less good for larger solutes (MM, Vancomycin?)Vancomycin?)
Diffusive TherapiesDiffusive Therapies

Joy MS, Matzke GR, Frye Joy MS, Matzke GR, Frye RF, Palevsky PM. AJKD RF, Palevsky PM. AJKD
1998;31:1019-271998;31:1019-27..

RRT Drug Removal MechanismsRRT Drug Removal Mechanisms
DiffusionDiffusion ConvectionConvection AdsorptionAdsorption
May be important for May be important for 2 Microglobulin removal2 Microglobulin removal Especially for PMMA membranesEspecially for PMMA membranes
Rarely important for drugsRarely important for drugs

Vancomycin overdoseVancomycin overdose
16 day old full-term infant presented to OSH 16 day old full-term infant presented to OSH hypothermia, bradycardia, and hypovolemia. hypothermia, bradycardia, and hypovolemia. Progressed to develop cardiac arrest, transferred Progressed to develop cardiac arrest, transferred to U of M. Dry wt. 2kg.to U of M. Dry wt. 2kg.
Received 3 doses of vancomycin 100mg/kgReceived 3 doses of vancomycin 100mg/kg Initial vancomycin serum concentration was Initial vancomycin serum concentration was
195.5 mg/L (desired peak conc ~35mg/L)195.5 mg/L (desired peak conc ~35mg/L)

Vancomycin overdose caseVancomycin overdose case

Hemodialyzer differences: Are they Hemodialyzer differences: Are they important in CVVHD?important in CVVHD?
Most published drug dosing guidelines assume Most published drug dosing guidelines assume they are all equal in terms of drug removalthey are all equal in terms of drug removal most hemofilters are high-permeability with large most hemofilters are high-permeability with large
porespores frequently high flux hemodialyzers were used for frequently high flux hemodialyzers were used for
CRRTCRRT Vancomycin CVVHD clearance differences Vancomycin CVVHD clearance differences
between different hemodialyzersbetween different hemodialyzers Joy MS, et al. Am J Kidney Dis 1998 Jun;31(6):1019-27Joy MS, et al. Am J Kidney Dis 1998 Jun;31(6):1019-27

No dialysate, removes plasma water as it seeps No dialysate, removes plasma water as it seeps through membranethrough membrane
Removes small and large molecules easilyRemoves small and large molecules easily as long as they can fit through membraneas long as they can fit through membrane Protein binding important determinant – sieving coefficientProtein binding important determinant – sieving coefficient <15,000 Da has potential to be removed substantially<15,000 Da has potential to be removed substantially
Drug removal easy to calculateDrug removal easy to calculate based on sieving coefficient – usually a function of PPBbased on sieving coefficient – usually a function of PPB ultrafiltrate concentration/plasma concentrationultrafiltrate concentration/plasma concentration
Convective TherapiesConvective Therapies (Hemofiltration)(Hemofiltration)

Doses Derived Via Sieving Doses Derived Via Sieving CoefficientCoefficient
Sieving Coefficient (SC) known for many drugsSieving Coefficient (SC) known for many drugs SC= UF/ASC= UF/A
Comes from CAVH or CVVH dataComes from CAVH or CVVH data Assumption often made that SC can be used Assumption often made that SC can be used
CVVHD when dialysate rate is low.CVVHD when dialysate rate is low. Saturation coefficient (Sa) more properly used in Saturation coefficient (Sa) more properly used in
CVVHDCVVHD SC related to protein binding of drugsSC related to protein binding of drugs
Protein binding may differ in critically ill vs. normalsProtein binding may differ in critically ill vs. normals

Sieving Coefficient & Protein Sieving Coefficient & Protein BindingBinding
DrugDrug Reported SCReported SC Free FractionFree FractionAmikacinAmikacin 0.930.93 0.950.95
ImipenemImipenem 0.780.78 0.800.80
MetronidazoleMetronidazole 0.840.84 0.800.80
PenicillinPenicillin 0.680.68 0.500.50
RanitidineRanitidine 0.780.78 0.850.85
VancomycinVancomycin 0.800.80 0.900.90
Valproic AcidValproic Acid 0.220.22 0.100.10

Drug Dosing recommendations Drug Dosing recommendations based on Sieving Coefficient (SC)based on Sieving Coefficient (SC) ClearanceClearance total total = Cl = ClCRRTCRRT + Cl + Cl residual renalresidual renal + +
Cl Cl non-renalnon-renal
SC equations only account for ClSC equations only account for ClCRRTCRRT
What about other clearances?What about other clearances? Cl Cl residual renal residual renal usually not an issue in usually not an issue in
CRRT patientsCRRT patients Cl Cl non-rena lnon-rena l not always available for not always available for
drugsdrugs

Non-renal clearance Non-renal clearance rates of selected drugs rates of selected drugs in patients with normal in patients with normal renal function and ESRDrenal function and ESRDDRUG NORMAL RENAL FX
(ML/MIN/70 KG)ESRD % DECLINE IN CL
Acyclovir 65 29 55
Aztreonam 40 27 33
Cefotaxime 217 130 40
Imipenem 128 54 56
Procainamide 257 102 60
Vancomycin 40 6 85

CRRT Challenges: Drug DosingCRRT Challenges: Drug Dosing Does CVVH removal = CVVHDF = CVVHD???Does CVVH removal = CVVHDF = CVVHD???
Molecular weight determines whether solute diffuses wellMolecular weight determines whether solute diffuses well Vancomycin (MW 1450 Da)Vancomycin (MW 1450 Da) Aminoglycosides (MW ~450 Da)Aminoglycosides (MW ~450 Da)
High dialysate flow rates don’t allow sufficient time for High dialysate flow rates don’t allow sufficient time for diffusiondiffusion
Probably not an issue when flow = ~1000ml/1.73m2/hrProbably not an issue when flow = ~1000ml/1.73m2/hr Does Sieving Coefficient (CVVH) = Saturation Does Sieving Coefficient (CVVH) = Saturation
Coefficient (CVVHD)???Coefficient (CVVHD)???

CRRT Challenges: Drug DosingCRRT Challenges: Drug Dosing
NO PEDIATRIC DOSINGNO PEDIATRIC DOSING!!!!!!!!!!!!!! Most CRRT dosing guidelines based on CVVH Most CRRT dosing guidelines based on CVVH
@ UFR of 1000 mL/hr@ UFR of 1000 mL/hr Trend is for higher UFR and HD flowsTrend is for higher UFR and HD flows UM uses 2L/1.73m2/hr UM uses 2L/1.73m2/hr Higher flow rates now achievable with new Higher flow rates now achievable with new
machinesmachines solute removal (H, HD, HDF) mechanismssolute removal (H, HD, HDF) mechanisms


Pediatric CrClPediatric CrCl
CLCLCRCR = K x L/S = K x L/SCRCR
Where ClWhere ClCRCR = creatinine clearance in = creatinine clearance in
ml/min/1.73m2 ml/min/1.73m2
K = constant of proportionality age specificK = constant of proportionality age specific
AgeAge KK
LBW ≤ 1yo 0.33
Full-term ≤ 1yo 0.45
2-12 0.55
13-21 female 0.55
13-21 male 0.70

Calculating Total ClearanceCalculating Total Clearance
Example:Example: 2yo, 15kg, L = 60cm, S2yo, 15kg, L = 60cm, SCRCR = 1.0 mg/dL, K = 0.55 = 1.0 mg/dL, K = 0.55 CrCl = 0.55 x 60/1 = 33ml/min/1.73m2CrCl = 0.55 x 60/1 = 33ml/min/1.73m2 However, if anuric renal clearance = zeroHowever, if anuric renal clearance = zero PCRRT = CVVHD of 2L/1.73m2/hr, BSA of 0.5PCRRT = CVVHD of 2L/1.73m2/hr, BSA of 0.5
Qd = ~578ml/hr Qd = ~578ml/hr (38.5ml/kg, or 9.6ml/min/0.5 BSA, or (38.5ml/kg, or 9.6ml/min/0.5 BSA, or
33.2ml/min/1.73ml/min)33.2ml/min/1.73ml/min) If this patient was not anuric and had renal fxn as above = If this patient was not anuric and had renal fxn as above =
66ml/min/1.73m2, and we need to adjust accordingly66ml/min/1.73m2, and we need to adjust accordingly

Adjusting doses based on ClAdjusting doses based on Cl
Using the previous example for vancomycin:Using the previous example for vancomycin: >50ml/min/1.73m2 = q6-8h dosing>50ml/min/1.73m2 = q6-8h dosing 30-50ml/min/1.73m2 = q12h dosing30-50ml/min/1.73m2 = q12h dosing
It is easy to under-dose or possibly overdose using It is easy to under-dose or possibly overdose using this method, need to be carefulthis method, need to be careful
Is CrCl the most reliable method for children?Is CrCl the most reliable method for children?

What drugs do we care about?What drugs do we care about?
Drugs are “Drugs are “dialyzable” ifdialyzable” if:: Small MWSmall MW Small volume of distributionSmall volume of distribution Not highly protein boundNot highly protein bound Water solubleWater soluble

CaseCase
10mof, ALL s/p chemo & BMT x60days, now admitted to 10mof, ALL s/p chemo & BMT x60days, now admitted to unit for increased O2 needs requiring vent support, GVHD unit for increased O2 needs requiring vent support, GVHD gut/liver stage IV and in septic shock.gut/liver stage IV and in septic shock.
PE: T 39.1, HR 180, BP 60/30, wt. 8.5kg, Ht 60cmPE: T 39.1, HR 180, BP 60/30, wt. 8.5kg, Ht 60cm I/O: 900/50 over past 24hrs (0.24cc/kg/hr)I/O: 900/50 over past 24hrs (0.24cc/kg/hr) Baseline Scr = 0.3mg/dL, now 0.6mg/dLBaseline Scr = 0.3mg/dL, now 0.6mg/dL Meds: Dopamine, Cefepime, Gentamicin, Linezolid, Meds: Dopamine, Cefepime, Gentamicin, Linezolid,
Voriconazole, Pentamidine, Hydrocortisone, Protonix, Voriconazole, Pentamidine, Hydrocortisone, Protonix, TPN/lipids, Dilaudid/Ativan, PhenobarbTPN/lipids, Dilaudid/Ativan, Phenobarb

Case con’tCase con’t
AM BC shows Pseudomonas aer. and VREAM BC shows Pseudomonas aer. and VRE Order written to start CVVH @ 2L/1.73m2/hr,Order written to start CVVH @ 2L/1.73m2/hr,
Calc. clearance: BSA = 0.38m2 (7.24ml/min, or Calc. clearance: BSA = 0.38m2 (7.24ml/min, or 33ml/min/1.73m2)33ml/min/1.73m2)
What drugs do we care about?What drugs do we care about? If you can titrate we don’t necessarily careIf you can titrate we don’t necessarily care For this patient antibiotics are going to save her For this patient antibiotics are going to save her
lifelife

So what drugs need adjustment?So what drugs need adjustment?
Dopamine?Dopamine? Cefepime?Cefepime? Gentamicin?Gentamicin? Linezolid?Linezolid? Voriconazole?Voriconazole? Pentamidine?Pentamidine?
Hydrocortsione?Hydrocortsione? Protonix?Protonix? TPN?TPN? Dilaudid?Dilaudid? Ativan?Ativan?

Antibiotic Guidelines UMAntibiotic Guidelines UM

Linezolid Clearance During CVVHDF Linezolid Clearance During CVVHDF
85 yo 90 kg anuric male in the SICU with 85 yo 90 kg anuric male in the SICU with documented abdominal VRE infectiondocumented abdominal VRE infection
Linezolid 600 mg IV q12Linezolid 600 mg IV q12 No published literature on CRRT removalNo published literature on CRRT removal CVVHDF regimen:CVVHDF regimen:
dialysate flow rate 2000 mL/hrdialysate flow rate 2000 mL/hr mean ultrafiltrate production rate of 775 mL/hrmean ultrafiltrate production rate of 775 mL/hr

Linezolid CalculationsLinezolid Calculations
Half-life, elimination rate, and volume of distributionHalf-life, elimination rate, and volume of distribution Sieving coefficient (SC) was calculated:Sieving coefficient (SC) was calculated:
SC= CE / Cp, Cp = (CA + CV) / 2SC= CE / Cp, Cp = (CA + CV) / 2
The clearance from CRRT (Cl CRRT) calculated as: The clearance from CRRT (Cl CRRT) calculated as: Cl CRRT = (QD + QF) x SCCl CRRT = (QD + QF) x SC
CE = the concentration in the effluentCE = the concentration in the effluent Cp is the linezolid concentration in the plasmaCp is the linezolid concentration in the plasma CA is the linezolid concentration in the plasma drawn from CA is the linezolid concentration in the plasma drawn from
the pre-filter sampling portthe pre-filter sampling port CV is the linezolid concentration in the plasma drawn from CV is the linezolid concentration in the plasma drawn from
the post-filter sampling port.the post-filter sampling port.

Linezolid ResultsLinezolid Results Vd = 60L (normal 40-60L)Vd = 60L (normal 40-60L) TT1/21/2 = 7.5-9 hrs during CVVHDF (8hrs) = 7.5-9 hrs during CVVHDF (8hrs) SC = 0.77– 0.81 (PPB 30%)SC = 0.77– 0.81 (PPB 30%) ClClCRRTCRRT = 36.5 mL/min with mean effluent flow rate = 36.5 mL/min with mean effluent flow rate
of 46.2 mL/min of 46.2 mL/min (normal Cl(normal ClRR 40mL/min) 40mL/min)
No dosage change necessaryNo dosage change necessary First measured linezolid CRRT reportFirst measured linezolid CRRT report Kraft MK, Pasko DA, DePestel DD, Ellis JJ, Peloquin CA, Mueller Kraft MK, Pasko DA, DePestel DD, Ellis JJ, Peloquin CA, Mueller
BA. Linezolid clearance during continuous venovenous BA. Linezolid clearance during continuous venovenous hemodiafiltration: A case report. Pharmacotherapy. 2003 hemodiafiltration: A case report. Pharmacotherapy. 2003 Aug;23(8):1071-5Aug;23(8):1071-5..

So what drugs need adjustment?So what drugs need adjustment?
Dopamine?Dopamine? Cefepime?Cefepime? Gentamicin?Gentamicin? Linezolid?Linezolid? Voriconazole?Voriconazole? Pentamidine?Pentamidine?
Hydrocortsione?Hydrocortsione? Protonix?Protonix? TPN?TPN? Dilaudid?Dilaudid? Ativan?Ativan?

Gentamicin pharmacokineticsGentamicin pharmacokinetics
This patient weighing 8.5kg receives a gent This patient weighing 8.5kg receives a gent dose of 21mg (2.5mg/kg)dose of 21mg (2.5mg/kg)
What peak concentration (mg/L) can be What peak concentration (mg/L) can be expected?expected?
Volume of distribution of gent is 0.2-0.4L/kgVolume of distribution of gent is 0.2-0.4L/kg 0.25L/kg is normal, but in fluid overloaded 0.25L/kg is normal, but in fluid overloaded
patients, expect higher values. If 0.3L/kg = patients, expect higher values. If 0.3L/kg = 2.55 Liters = Vd2.55 Liters = Vd 21mg/2.55L = 8.2 mg/L assuming no drug removal21mg/2.55L = 8.2 mg/L assuming no drug removal

Gent kinetics con’tGent kinetics con’t
30 min after the 21mg dose is done a peak is 30 min after the 21mg dose is done a peak is done = 4.0mg/Ldone = 4.0mg/L
What is the patients actual volume of What is the patients actual volume of distribution?distribution? 5.1 Liters = 0.6L/kg (actually double!!!!)5.1 Liters = 0.6L/kg (actually double!!!!)

Gent kinetics con’tGent kinetics con’t
Peak was 4.0 mg/LPeak was 4.0 mg/L 12 hours later a random level was done 12 hours later a random level was done
1.0 mg/L1.0 mg/L What is the half-life (tWhat is the half-life (t1/21/2) of gentamicin?) of gentamicin? 4.0mg/L 4.0mg/L → 2.0mg/L → 1.0mg/L in 12 hours→ 2.0mg/L → 1.0mg/L in 12 hours 6 hour half-life6 hour half-life Ln 4 – ln 1Ln 4 – ln 1 = kel = 0.115 = kel = 0.115
12hrs12hrs

Gent kinetics FINALGent kinetics FINAL
Half-life = 0.693 / 0.115 = 6 hoursHalf-life = 0.693 / 0.115 = 6 hours

So what drugs need adjustment?So what drugs need adjustment?
Dopamine?Dopamine? Cefepime?Cefepime? Gentamicin?Gentamicin? Linezolid?Linezolid? Voriconazole?Voriconazole? Pentamidine?Pentamidine?
Hydrocortsione?Hydrocortsione? Protonix?Protonix? TPN?TPN? Dilaudid?Dilaudid? Ativan?Ativan?

Phenobarbital casePhenobarbital case
2 wof transferred to UM w/ severe CHF w/ AV valve 2 wof transferred to UM w/ severe CHF w/ AV valve regurgitation and seizure dxregurgitation and seizure dx
1/20 had cleft AV valve repair w/ PDA ligation, went 1/20 had cleft AV valve repair w/ PDA ligation, went on VA ECMO, developed ARFon VA ECMO, developed ARF
1/24 went on CVVHD in-line w/ECMO circuit1/24 went on CVVHD in-line w/ECMO circuit Wt 3.45kg (dry), Ht 47cm, BSA 0.21m2Wt 3.45kg (dry), Ht 47cm, BSA 0.21m2 Qd set at 300ml/hr (~2400ml/1.73m2/hr)Qd set at 300ml/hr (~2400ml/1.73m2/hr) Quf at 69ml/hr (drips + no net loss)Quf at 69ml/hr (drips + no net loss) Hemodiafilter = Mini-Plus, 0.08m2Hemodiafilter = Mini-Plus, 0.08m2

Phenobarbital casePhenobarbital case
Phenobarbital dose pre dialysis initiation = Phenobarbital dose pre dialysis initiation = 25mg q24h = 7.2mg/kg = 35.5mg/L serum 25mg q24h = 7.2mg/kg = 35.5mg/L serum concentrationconcentration
CVVHD started 1/24CVVHD started 1/24 1/25 Pb = 14.2 mg/L1/25 Pb = 14.2 mg/L 1/26 Pb = 9.6 1/26 Pb = 9.6 1/28 Pb = 13.9 @ 07001/28 Pb = 13.9 @ 0700 1/28 1400 sequential levels done1/28 1400 sequential levels done

Phenobarbital casePhenobarbital caseSiteSite Concentration (mg/L)Concentration (mg/L)
Pre-oxygenatorPre-oxygenator 26.526.5
Post-oxygenatorPost-oxygenator 24.724.7
Pre-hemodiafilterPre-hemodiafilter 26.226.2
Post-hemodiafilterPost-hemodiafilter 25.925.9
EffluentEffluent 11.411.4

Drug dosing problems in Drug dosing problems in high volume hemofiltrationhigh volume hemofiltration
Most drugs have Most drugs have >> 2 compartments (pools) 2 compartments (pools) like urea measurements during HDlike urea measurements during HD high volume hemofiltration removes drug from high volume hemofiltration removes drug from
peripheral compartment rapidlyperipheral compartment rapidly how fast can drug transfer from deeper how fast can drug transfer from deeper
compartment?compartment? Many drugs rapidly stripped from first poolMany drugs rapidly stripped from first pool

Phenobarb case finalPhenobarb case final
SC = 0.44SC = 0.44 ClClCRRTCRRT = =
2.7ml/0.21m2/min or 22.3ml/1.73m2/min (40)2.7ml/0.21m2/min or 22.3ml/1.73m2/min (40) Vd = 3.24L/kg (0.9L/kg, normal 0.6)Vd = 3.24L/kg (0.9L/kg, normal 0.6) New maintenance dose to maintain level of New maintenance dose to maintain level of
25mg/L = 25mg/L = 32.4mg (~10mg/kg) IV q8hrs32.4mg (~10mg/kg) IV q8hrs Original maintenance dose 25mg q24hrsOriginal maintenance dose 25mg q24hrs

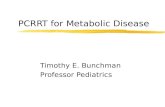
Deep/CentralCompartment
Pool 2???Liters
Dialysate
UF Soln
Qb
Qb
UF Soln
SpentDialysate &/orUF
Dialysate
Pool 16L?
k12
k21
k32k23
Deeper compartment(s)?
Pool 3???Liters
Solute K inetics during CRRT
Peripheralcompartment
PatientCRRT
Mueller BA, Pasko DA. Artif Organs 2003;27:808-14.

Drug is infused into compartment being Drug is infused into compartment being filtered/dialyzedfiltered/dialyzed reduced ability to distribute into tissues (kreduced ability to distribute into tissues (k1212)) serum concentrations during infusion higher than serum concentrations during infusion higher than
usual “therapeutic” serum concentrationusual “therapeutic” serum concentration 6L/hr = 1L/10 min = entire plasma 6L/hr = 1L/10 min = entire plasma
volume/hrvolume/hr Qb 150 ml/min Quf/hd 33 mL/min = Qb 150 ml/min Quf/hd 33 mL/min =
22% of volume removed22% of volume removed ““first-pass” effectfirst-pass” effect
IV drug administration: Drug IV drug administration: Drug removed as it is infusedremoved as it is infused

Drug Prescribing in Renal Drug Prescribing in Renal FailureFailure
edited by George Aronoff et aledited by George Aronoff et al Commonly carried text by Commonly carried text by
pharmacistspharmacists http://www.kdp-baptist.louisville.ehttp://www.kdp-baptist.louisville.e
du/renalbook/du/renalbook/ New edition to come out soonNew edition to come out soon Recommendations for new drugsRecommendations for new drugs IHD and CRRT recommendationsIHD and CRRT recommendations Pediatric recommendationsPediatric recommendations

Strength of EvidenceStrength of Evidence
A.A. Controlled studies in humans or Controlled studies in humans or large case series experience large case series experience
B.B. Small Case Series or Human Small Case Series or Human Uncontrolled TrialsUncontrolled Trials
C.C. Animal or In Vitro DataAnimal or In Vitro Data
D.D. Known Drug Characteristics Known Drug Characteristics A.A. Vast majority are of this typeVast majority are of this type
58 drugs are A->C

D. “Known drug characteristics“D. “Known drug characteristics“
These recommendations made by These recommendations made by panel of nephrologists and panel of nephrologists and pharmacistspharmacists
Based on:Based on: Protein Binding InformationProtein Binding Information Volume of DistributionVolume of Distribution Molecular WeightMolecular Weight

When in doubt, start here…When in doubt, start here… Blood flow, filter type are not very important.Blood flow, filter type are not very important. Find outFind out
In CVVHD: Dialysate flow rate (ml/hr)In CVVHD: Dialysate flow rate (ml/hr) Usually 2 L/1.73m2/hr (33 mL/1.73m2/min)Usually 2 L/1.73m2/hr (33 mL/1.73m2/min)
In CVVH: Substitution Fluid rate (ml/hr)In CVVH: Substitution Fluid rate (ml/hr) Usually 2L/1.73m2/hr (33 mL/1.73m2/min)Usually 2L/1.73m2/hr (33 mL/1.73m2/min)
Add this to patient’s native Cr Cl Add this to patient’s native Cr Cl (ml/1.73m2/min)(ml/1.73m2/min)
This is patient’s new Cr Cl This is patient’s new Cr Cl dose accordingly dose accordingly Works in most cases…is good enough for initial Works in most cases…is good enough for initial
estimates. Follow up with drug level monitoring.estimates. Follow up with drug level monitoring.

PCRRT & Roller pumpPCRRT & Roller pump

Future research neededFuture research needed
ECMO/PCRRTECMO/PCRRT MARSMARS RADRAD

CRRT Dosing should not be CRRT Dosing should not be confusing!confusing!