36. Lateral Thigh Perforator Flap for Breast ... · augment venous drainage by an additional...
26
ASRM Scientific Paper Presentations: Breast & Microsurgical Practice Sunday, January 15, 2017, 1:30pm – 3:00pm 36. Lateral Thigh Perforator Flap for Breast Reconstruction: Computed Tomographic Angiography Analysis and Clinical Cases University of Pittsburgh, Pittsburgh, PA, USA Marco Maricevich, MD 1 ; Michael Bykowski, MD 1 ; Mark Asher Schusterman II, MD 2 ; Evan Katzel, MD 1 ; Michael Gimbel, MD 1 ; (1)University of Pittsburgh, Pittsburgh, PA, (2)University of Pittsburgh Medical Center, Pittsburgh, PA PURPOSE While abdominally based flaps remain first choice for autologous breast reconstruction, alternative donor sites are necessary when the abdomen is unavailable. We propose the lateral thigh region as a suitable donor site for select patients. METHODS The lateral thigh perforator flap (LTP) anatomy was studied in 100 CT angiograms (DIEP protocol) at our institution (200 thighs). Collected data included lateral circumflex femoral artery (LCFA) origin, number/type/course of lateral thigh perforators, pedicle characteristics, and reference point measurements. A clinical LTP breast reconstruction series is presented. RESULTS LCFA originated from the profunda femoral artery in 83% of patients. Perforators analyzed originated from the ascending branch of the LCFA (4.6mm average diameter), averaging 2.6 perforators/thigh. Mean estimated pedicle length was 7.7cm (+/- 0.7cm). Septocutaneous perforators were present in 97% (1.8 perforators/thigh), emerging mainly through the TFL- gluteus medius septum. Musculocutaneous perforators were present in 64% (0.9 perforators/thigh). Septocutaneous perforators were always larger than musculocutaneous. The mean distance between ASIS and perforator was 9.9cm (+/- 1.5cm). Perforators were located 0.13cm (+/- 1.1cm) below the pubic symphysis level. Our LTP clinical series featured dissection in the supine position and primary donor site closure (5 patients, 8 LTP flaps). Our surgical technique and planning evolved with lessons learned from each case. CONCLUSIONS Lateral thigh perforators are consistent and dependable on CTA analysis and in clinical practice. Preoperative imaging and flap planning with reliable landmarks are important for successful LTP
Transcript of 36. Lateral Thigh Perforator Flap for Breast ... · augment venous drainage by an additional...

ASRM Scientific Paper Presentations: Breast & Microsurgical Practice
Sunday, January 15, 2017, 1:30pm – 3:00pm
36. Lateral Thigh Perforator Flap for Breast Reconstruction: Computed Tomographic Angiography Analysis and Clinical Cases University of Pittsburgh, Pittsburgh, PA, USA Marco Maricevich, MD1; Michael Bykowski, MD1; Mark Asher Schusterman II, MD2; Evan Katzel, MD1; Michael Gimbel, MD1; (1)University of Pittsburgh, Pittsburgh, PA, (2)University of Pittsburgh Medical Center, Pittsburgh, PA PURPOSE While abdominally based flaps remain first choice for autologous breast reconstruction, alternative donor sites are necessary when the abdomen is unavailable. We propose the lateral thigh region as a suitable donor site for select patients. METHODS The lateral thigh perforator flap (LTP) anatomy was studied in 100 CT angiograms (DIEP protocol) at our institution (200 thighs). Collected data included lateral circumflex femoral artery (LCFA) origin, number/type/course of lateral thigh perforators, pedicle characteristics, and reference point measurements. A clinical LTP breast reconstruction series is presented. RESULTS LCFA originated from the profunda femoral artery in 83% of patients. Perforators analyzed originated from the ascending branch of the LCFA (4.6mm average diameter), averaging 2.6 perforators/thigh. Mean estimated pedicle length was 7.7cm (+/- 0.7cm). Septocutaneous perforators were present in 97% (1.8 perforators/thigh), emerging mainly through the TFL-gluteus medius septum. Musculocutaneous perforators were present in 64% (0.9 perforators/thigh). Septocutaneous perforators were always larger than musculocutaneous. The mean distance between ASIS and perforator was 9.9cm (+/- 1.5cm). Perforators were located 0.13cm (+/- 1.1cm) below the pubic symphysis level. Our LTP clinical series featured dissection in the supine position and primary donor site closure (5 patients, 8 LTP flaps). Our surgical technique and planning evolved with lessons learned from each case. CONCLUSIONS Lateral thigh perforators are consistent and dependable on CTA analysis and in clinical practice. Preoperative imaging and flap planning with reliable landmarks are important for successful LTP

harvest. We believe the LTP represents a reasonable alternative for select patients undergoing autologous breast reconstruction.


37. Stacked Microsurgical Autologous Flap Breast Reconstruction is an Ideal Option after Unilateral Nipple-Sparing Mastectomy NYU Langone Medical Center, New York, NE, USA Jordan D. Frey, MD; Michael Alperovich, MD; Christina Y Ahn, MD; Robert J Allen, MD; NYU Langone Medical Center, New York, NY Introduction: Nipple-sparing mastectomy (NSM) allows for complete preservation of the nipple-areola complex and is increasing in popularity. Autologous options in NSM provide an aesthetic reconstruction in a single stage, however donor tissue may be scarce in these patients. Stacked microsurgical breast reconstruction, especially in unilateral cases, is an attractive alternative in NSM that is yet to be described. Methods: Patients undergoing NSM with stacked autologous flap reconstruction were identified with demographics, intraoperative variables, and outcomes analyzed. Results: Six patients who underwent unilateral NSM with stacked autologous free flaps were identified. The average patient age and BMI were 50.17 years and 21.67, respectively. Average follow-up was 28.62 months. Five patients (83.3%) underwent unilateral NSM and reconstruction for a therapeutic indication. The average mastectomy weight was 235.67 grams. All patients were reconstructed with stacked DIEP flaps. Four patients (66.7%) had NSM performed through a vertical radial incision while two utilized a lateral radial incision (33.3%). The average total flap weight was 397.33 grams. Anastomoses in five stacked flaps (83.3%) were performed in an anterograde and retrograde fashion to the internal mammary (IMA) vessels. In one stacked flap (16.7%), the two flaps were anastomosed in series to the IMA. Three flaps (50%) were neurotized. All flaps were monitored with a skin paddle while one flap also utilized an implantable Doppler device. There were no major complications and 3 incidences of minor complications. Minor complications included one instance of minor mastectomy flap necrosis (16.7%) managed with local wound care only and 2 instances of fat necrosis (33.3%), one of which was excised in the operating room and one of which was treated with liposuction. There were no incidences of partial or complete flap loss. The average number of secondary procedures was 0.83 per patient. The most common secondary procedures performed were fat grafting (5 patients), skin paddle excision (3 patients), breast mound revision (2 patients), and mastopexy (1 patient). Conclusions: Stacked microsurgical autologous breast flaps provide an optimal reconstruction after NSM and may be considered the reconstruction of choice in patients undergoing unilateral NSM with inadequate donor site tissue for single flap reconstruction.


38. A Novel Strategy to Supercharge a Deep Inferior Epigastric Artery Perforator (DIEP) Flap after Port-a-Cath Removal Chad Teven, Chicago, IL, USA Chad M Teven, M.D.; The University of Chicago Medical Center, Chicago, IL; Adrian SH Ooi, MBBS, MMed, MRCS; University of Chicago Medical Center, Chicago, IL; David W. Chang, MD, FACS; Plastic Surgery Deparment, University of Chicago Medical Center, Chicago, IL; David H. Song, MD, MBA; Section of Plastic and Reconstructive Surgery, Department of Surgery, University of Chicago Medical Center, Chicago, IL Purpose Autologous breast reconstruction using the deep inferior epigastric artery perforator (DIEP) flap has become increasingly popular due to its unique advantages. However, compared to some other forms of abdominal-based autologous reconstruction, DIEP flaps are associated with an increased risk of venous congestion. Many techniques – or lifeboats - have been introduced to diagnose and treat this potentially devastating complication. In this case report we describe a novel strategy to augment venous drainage when venous congestion is encountered. Methods A patient presented requesting autologous reconstruction and removal of a venous access catheter that had been used for chemotherapy administration. Results We performed left delayed breast reconstruction using a single-perforator DIEP flap from the right hemi-abdomen. The superficial inferior epigastric vein (SIEV) to this flap was preserved. This flap was based on a single medial row perforator. After anastomosis to the internal mammary vessels, the SIEV became moderately engorged. A decision was made to augment venous drainage by an additional anastomosis of the SIEV, which was noted to be in close proximity to the Port-a-Cath. After removal of the Port-a-Cath from the left chest, we anastomosed the SIEV to the fibrous capsular sheath that had formed around the indwelling catheter in order to allow additional venous drainage. Flow through this conduit was confirmed using Doppler ultrasound. There were no flap-related complications and the patient was discharged in good condition. Conclusion We report for the first time the use of the fibrous capsular sheath that formed around an indwelling venous catheter to augment venous drainage in DIEP flap reconstruction. Further research is necessary to characterize the indications and limitations of this novel technique.

39. The Effect of BMI on Patient Reported and Surgical Outcomes in Autologous Breast Reconstruction: A Multicenter Prospective Mastectomy Reconstruction Outcomes Consortium (MROC) Study University of Michigan, Ann Arbor, 212, USA Dhivya R Srinivasa, MD1; Edwin G. Wilkins, MD2; Jennifer B Hamill, MPH1; Ji Qi, MS1; Hyungjin M Kim, ScD1; Andrea L. Pusic, MD, MHS3; Mark W. Clemens, MD4; Patrick B. Garvey, MD4; (1)University of Michigan, Ann Arbor, MI, (2)Department of Surgery, Section of Plastic Surgery, University of Michigan, Ann Arbor, MI, (3)Division of Plastic and Reconstructive Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, (4)Department of Plastic Surgery, MD Anderson Cancer Center, Houston, TX BACKGROUND Despite the rising incidence of obesity among patients seeking post-mastectomy reconstruction, there are few multicenter, prospective studies evaluating the impact of body mass index (BMI) on risks and patient-reported outcomes (PROs) in these procedures. Our aim was to evaluate the effects of BMI on surgical complications and PROs in abdominal-based, microsurgical breast reconstruction. METHODS Patients undergoing immediate or delayed abdominal-based, free flap breast reconstruction were enrolled in the 11-center Mastectomy Reconstruction Outcomes Consortium Study. In addition to demographic and clinical variables, PROs (using the BREAST-Q) were assessed preoperatively and at one year postoperatively. Surgical complications, including major complications requiring re-operation or readmission, were evaluated at one year. The BMI cohorts were defined by World Health Organization criteria as underweight/normal (<25.0 kg/m2), overweight (25.0-29.9 kg/m2), Class I obesity (30.0-34.9 kg/m2), and Class II/III obesity (≥35.0 kg/m2). Adjusting for baseline demographic and clinical differences, mixed-effects regression models analyzed BMI effects on complications and PROs. RESULTS We evaluated 589 patients (107 free TRAM, 415 DIEP, and 67 SIEA). Compared with underweight/normal BMI, Class II/III obesity was associated with significantly greater risks for any complication and for major complications (OR 3.75, p<0.0001, and OR 2.26, p=0.017, respectively). While overweight and Class I obese BMIs were not associated with higher risks for major complications, the effect of Class I obesity on risk for any complication approached significance (OR 1.66 p=0.06). Regression analyses of PROs showed no significant BMI effects on psychosocial or physical well-being at one year following reconstruction. For sexual well-being, overweight BMI was associated with significantly higher scores, compared with underweight/normal BMI (OR 5.49, p=0.045). Regression analysis found no significant BMI effects on patient satisfaction with the reconstructed breast. In univariate analyses, satisfaction with breasts improved significantly over time for all patients (p=0.001), with gains noted in all BMI categories between the preoperative and one-year postoperative time periods.

CONCLUSION Although obese patients undergoing abdominal-based free-flap breast reconstruction appeared to experience more postoperative complications, these women reported significant psychosocial and body image benefits that were equivalent to or better than those reported by underweight/normal weight patients. In light of these significant quality of life benefits, surgeons should discuss the advantages and risks of free flap breast reconstruction with their higher BMI patients.

40. Prior Radiation in Nipple-Sparing Mastectomy Does Not Increase Risk in Implant-Based Breast Reconstruction but Comparatively Increases Risk in Autologous Reconstruction NYU Langone Medical Center, New York, 221, USA Jordan D. Frey, MD1; Michael Alperovich, MD1; Jamie P. Levine, MD2; Mihye Choi, MD1; Nolan S. Karp, MD1; (1)NYU Langone Medical Center, New York, NY, (2)Institute of Reconstructive Plastic Surgery, NYU Langone Medical Center, New York, NY Background: Breast reconstruction in patients undergoing nipple-sparing mastectomy (NSM) with prior radiation is generally considered a higher risk procedure. However, as the technique has evolved, more patients with advanced disease and neoadjuvant therapy are undergoing NSM with both implant-based and autologous reconstruction. Methods: All patients undergoing NSM with implant-based and autologous reconstructions from 2006 to 2015 were identified. Results were compared for implant-based reconstructions with and without pre-operative radiation. Results were then compared for patients with prior radiation who underwent implant-based versus autologous NSM reconstruction. Results: NSMs undergoing implant-based reconstruction with prior radiation were significantly more likely to have diabetes (p=0.0480), a therapeutic mastectomy (p=0.0037), and to undergo neoadjuvant chemotherapy (p=0.0003). Those with prior radiation also had a significantly shorter follow-up period (p=0.0331). Notably, those with and without prior radiation had similar rates of tissue expander (76.0% versus 73.8%) and immediate, permanent implant (24.0% versus 26.2%) reconstruction (p=0.8025). Age (p=0.0917), BMI (p=0.8257), and cancer stage (p=0.8784), among other variables, were similar. Reconstructive outcomes were then compared. Rates of major (p=0.5359) and minor (p=0.5835) mastectomy flap necrosis, complete (p=0.4533) and partial (p=0.2722) nipple necrosis, as well as infection (major, p=0.3737; minor, p=0.8770) were equivalent between those with and without prior radiation. Rates of explantation (p=0.7431) and implant failure (p=0.2721), among other outcomes, were likewise equivalent. Next, reconstructive outcomes for implant-based and autologous reconstructions with prior radiation were compared. There was no significant difference in BMI between these two groups (24.60 to 23.86 kg/m2, p=0.600). Those with autologous reconstructions had significantly more major mastectomy flap (p=0.0495) and complete nipple necrosis (p<0.0001) than implant-based reconstructions; other outcomes were equivalent. Conclusions: Patients undergoing NSM with implant-based breast reconstruction after radiation do not appear to be at higher risk for complications. Those with prior radiation who underwent autologous NSM reconstruction had significantly more mastectomy flap and nipple necrosis compared to those with implant-based reconstruction despite similar BMIs. Possible

explanations are that autologous reconstructions place the breast envelope under greater immediate stress than implant-based reconstructions, the majority of which were tissue expander-based reconstructions and that retraction on the mastectomy flaps to expose the internal mammary vessels and perform microsurgery may predispose to mastectomy flap ischemia
Figures:
Table 1: Demographics of Implant-Based NSM Reconstructions with and without Prior Radiation
Table 2: Reconstructive Outcomes of Implant-Based NSM Reconstructions with and without Prior Radiation

Table 3: Reconstructive Outcomes of Implant-Based and Autologous NSM Reconstructions with Prior Radiation

41. Evolution in the Monitoring of Free Flap Autologous Breast Reconstruction in Nipple-Sparing Mastectomy: The NYU Experience NYU Langone Medical Center, New York, 221, USA John T. Stranix, MD1; Jordan D. Frey, MD1; Michael V Chiodo, MD1; Michael Alperovich, MD1; Christina Y Ahn, MD1; Robert J Allen, MD1; Mihye Choi, MD1; Nolan S. Karp, MD1; Jamie P. Levine, MD2; (1)NYU Langone Medical Center, New York, NY, (2)Institute of Reconstructive Plastic Surgery, NYU Langone Medical Center, New York, NY Background: Nipple-sparing mastectomy (NSM) is the latest advancement in the treatment of breast cancer. Autologous free flap reconstruction provides excellent aesthetic outcomes in NSM. However, the question remains of how to best monitor these reconstructions in the acute post-operative period. We therefore examined outcomes in NSM with buried free flap reconstruction versus free flap reconstruction incorporating a skin paddle for monitoring. Methods: All autologous free flap reconstructions with NSM performed from 2006 to 2015 were identified. Free flaps were divided into those that were completely buried and those with a skin paddle for monitoring. Demographics and operative results were analyzed and compared for each group. Results: 221 free flaps for breast reconstruction in NSM were identified: 50 buried flaps and 171 flaps incorporating a skin paddle. Most common flaps used were deep inferior epigastric perforator (DIEP) (64%), profunda artery perforator (PAP) (12.1%), and muscle-sparing transverse rectus abdominis myocutaneous (MS-TRAM) flaps (10.4%). Patients undergoing NSM free flap reconstruction with a skin paddle had significantly greater BMI (p=0.006) and greater smoking history (p=0.058). Mastectomy weight (p = 0.017) and flap weight (p<0.0001) was significantly greater in flaps incorporating a skin paddle. Flaps incorporating a skin paddle were also more likely to utilize MS-TRAM flaps and less likely to utilize a non-abdominally based free flap (p=0.003). The majority (86.0%) of buried flaps were monitored using an internal Cook Doppler system (p<0.0001). Other demographics including age (p=0.614) and laterality of NSM (p=0.999) were equivalent between the groups. Comparing outcomes between buried flaps versus flaps incorporating skin paddle, there were no significant differences in flap failure (2.0% vs. 2.3%, p=1.000) or percentage of flaps requiring return to the operating room (6.0% vs. 4.7%, p=0.715). The buried flap group had an absolute greater mean number of revisions per NSM (0.82) compared to the skin paddle group (0.44), however revision rates per NSM were statistically equivalent between the groups (p=0.296). Conclusions: While buried free flap reconstruction in NSM has been shown to be a safe and effective option, our technique has evolved to favor incorporating a skin paddle. This is advantageous as it allows for reliable visual monitoring. Additionally, regardless of monitoring technique utilized, many patients with free flap reconstruction in NSM opt for a secondary revision at which time the skin paddle may easily be removed.

Figures:

42. Perforator Numbers and Complications in DIEP Flap Breast Reconstruction: Is There a Correlation? University of Texas Southwestern Medical Center, Dallas, 232, USA Shuhao Zhang, MD; Andrew A. Gassman, MD; Samar Kayfan, BA; Jenny Wang, BS; Michael Zhou, BA; Nicholas T. Haddock, MD; Sumeet S. Teotia, MD; University of Texas Southwestern Medical Center, Dallas, TX Background: Single perforator flaps in breast reconstruction have been reported to have increased fat necrosis.1-2 We were motivated to evaluate our experience and the effect of number of perforators on DIEP flap complications and donor site morbidity. Methods: 199 patients underwent 328 DIEP flaps by two surgeons from 2010 to 2016 at a university hospital. Perforator selection was guided by CT imaging and clinical observation. First, perforator average size was compared among flaps with 1 perforator (n= 110 flaps), 2 perforators (n= 136 flaps), and 3 perforators (n= 82 flaps). Next, rates of fat necrosis, flap failure, and abdominal bulging were analyzed among the same three perforator groups. In addition, rates of postoperative abdominal bulge requiring surgical intervention was compared to the presence of a nerve-preserving type flap harvest. Results: Average perforator size significantly decreased as the number of perforators increased (1 perforator = 2.11mm, 2 perforators = 1.80mm, 3 perforators = 1.65mm, p-value = 0.02 and 0.01 for 1 versus 2 perforator flaps and 1 versus 3 perforator flaps, respectively). However, no significant differences were noted in fat necrosis, flap failure, and abdominal bulging rates across perforator groups. Additionally, flap weights were not significantly different across the three groups (Average: 1 perforator-774 grams, 2 perforators-797 grams, and 3 perforators-749 grams). Neither perforator number nor nerve preserving techniques were found to result in significant decreases in abdominal bulge rates. Conclusion: Contrary to other studies, we found that the number of perforators harvested in DIEP flap breast reconstruction was not associated with increase or decrease in flap survival or fat necrosis. This occurrence could be attributed to the surgeons’ choosing to proceed with single perforator flaps only when perforator size was adequately large, maintaining consistent blood supply. There was no association among perforator number, utilization of nerve sparing procedures, and abdominal bulge that required subsequent surgical intervention. Despite this, we still cautiously advocate nerve-preserving techniques that may have a subclinical effect.

43. Revisiting the Caudal Anastomosis to the Internal Mammary System in Free Flap Breast Reconstruction: A Call for Caution University of Texas Southwestern Medical Center, Dallas, 232, USA Sumeet S. Teotia, MD; Kyle Sanniec, MD; Andrew A. Gassman, MD; Samar Kayfan, BA; Jenny Wang, BS; Michael Zhou, BA; Nicholas T. Haddock, MD; University of Texas Southwestern Medical Center, Dallas, TX Introduction: As breast reconstructive microsurgeons increase their armamentarium of flaps with experience, the need for stacked and multiple flaps may generate an improved aesthetic outcome. Bi-pedicled and stacked flaps have been performed by microsurgeons using the cranial and caudal internal mammary system. We present our experience utilizing this system for flap reliability. Method: 736 flaps for breast reconstruction were performed from 2010-2016 (DIEP/SIEA and PAP flaps) by 2 senior surgeons at a university hospital. 220 (30%) of those flaps were either: Stacked PAP flaps, 4-flap (Bilateral PAP+DIEP flap), or Double-pedicle DIEP/SIEA flaps. Specific data regarding number, type, and locality of anastomosis was analyzed. Results: 454 anastomosis were performed in 87 patients who underwent 220 flaps (Double-pedicle flaps, 4-Flap, Stacked PAP,). Out of 454 anastomosis, 167 were to Caudal IMA/V (37%), 171 were to Cranial IMA/V (38%), and 116 were intra-flap (25%). There were 0 flap losses in Double-pedicle DIEP group (58-patients, 116-flaps), 3 flap losses in 4-Flap group (23-patients, 92-flaps), and 0 in Stacked-PAP group (6-patients, 12-flaps). In the 3 flap losses of 4-Flap group, 2 flaps were to Caudal IMA/V (1 arterial thrombosis, 1 venous thrombosis), and 1 cranial IMA/V (venous thrombosis). Also, in the 4-Flap group, 3 flaps were salvaged by converting to intra-flap anastomosis (6 anastomosis) due to intraoperative thrombosis of Caudal IMA/V (all 3 had arterial thrombosis related to caudal IMA). In the Stacked-PAP group, there were 2 flaps salvaged, 1 by converting to intra-flap artery from caudal IMA, and other was venous congestion from caudal IMV pedicle kink seen POD#1. In the Double-pedicle DIEP group, 1 flap was salvaged by converting 1 arterial anastomosis from caudal IMA to intra-flap. Total flap loss rate in entire group was 1.4%. Flap loss avoidance (or net increase in flap success) by either conversion to intra-flap anastomosis or early suspicion of caudal system compromise was 2.7% (6 flaps prevented out of 220). Conclusion: Caudal IMA/V system remains a viable and safe option for anastomosis in multiple flap procedures. However, based on our large experience with stacked and multiple flaps, we add caution utilizing the caudal system, particularly in patients with radiation, anastomosis mismatch and intraoperative spasm. The enthusiasm towards usage of caudal IMA/V system should be appropriately attenuated in certain circumstances with preference towards intra-flap anastomosis. We propose and present various methods to prevent such complications, with intra-operative algorithm geared towards technique modification and alternatives for microsurgeons.

44. Effects of Radiation Therapy on Internal Mammary Arteries and Early Complications in Microvascular Breast Reconstruction Division of Plastic Surgery, Washington University in St. Louis School of Medicine, Saint Louis, MO Elizabeth B Odom, MD1; Ali A Qureshi, MD2; Aaron Mull, MD3; Caroline B. Min, BS2; Daniel Hunter, RA4; Terence M. Myckatyn, MD5; (1)Box 3238, St. Louis, MO, (2)Washington University School of Medicine, St. Louis, MO, (3)Division of Plastic and Reconstructive Surgery, Washington University School of Medicine, St. Louis, MO, (4)Division of Plastic and Reconstructive Surgery, 660 S. Euclid, NT NW Tower, Ste 1150, St. Louis, MO, (5)Division of Plastic Surgery, Washington University in St. Louis School of Medicine, Saint Louis, MO Background: Many surgeons delay breast reconstruction for 6 months following radiation therapy due to documented adverse effects on tissues and blood vessels. However, vascular compromise appears to be progressive, taking several weeks to manifest. Therefore, microvascular breast reconstruction within a few weeks of radiation therapy may in fact be ideal. There is a paucity of data evaluating the early versus late effects of radiation on the internal mammary artery (IMA). The goal of this study is to histologically evaluate IMAs and anastomotic complications in patients <6 weeks and >6 months post-radiation to delineate the best time-frame in which to perform these autologous breast reconstruction. Methods: After approval from the Institutional Review Board, prospective data were obtained for all women ages 20-60 undergoing microvascular breast reconstruction between July 2015 and April 2016. Patients were separated into no radiation, early (<6 weeks from radiation therapy) or late (>6 months from radiation therapy) groups. A 3-4mm IMA biopsy was taken at the time of surgery. Samples were stained for macrophages (CD68), smooth muscle actin, elastin, and with Gomori trichrome and were analyzed by a single investigator. For the purpose of this abstract IMAs with contralateral radiation were considered to be radiated. Results: 36 IMAs in 22 patients were analyzed. 6 IMAs had no radiation, 12 had radiation <6 weeks (average 38.33 days), and 18 had radiation >6 months (average 1211 days) prior to surgery. There were no differences in demographics, surgical variables, or cardiovascular comorbidities between groups. Number of treatments and total cGy did not differ. Histologically, only arterial intimal thickness differed between early and late groups (18.69±6.05μm vs 27.99±8.92μm, p=0.007). There was a trend toward an increased macrophage count in the late group when compared to the early group (29.03 vs 20.53 per 100,000μm2,
p=0.07). Patients with any radiation had more macrophages (p=0.03), less smooth muscle actin (p=0.04), and a thicker tunica intima (p<0.001) than those who did not. Two patients, one without radiation and one in the late group, had early anastomotic complications. Only one patient, in the no radiation group had total flap loss. Conclusions: Patients < 6 weeks from radiation therapy have less intimal thickening and fewer macrophages in the IMA wall than those >6 months from radiation. This suggests more inflammation in the IMA with delayed reconstruction. There were too few patients to draw conclusions about vascular outcomes. We suggest a larger study to strengthen these findings.

45. Morbidity and Quality of Life Outcomes of Breast Reconstruction for Unilateral Mastectomy vs. Additional Contralateral Prophylactic Mastectomy: a Cohort Study of 211 Breast Reconstruction Patients Department of Plastic and Reconstructive Surgery, Johns Hopkins University, Baltimore, MD, Mohamad E. Sebai, MBBS1; Ricardo J Bello, MD, MPH2; Eric L. Wan, BS3; Charalampos Siotos, MD4; Jeff Aston, BS4; David Cui, NA4; Julie Lee, N/A4; Sethly Davis, N/A4; Justin M Sacks, MD, MBA5; Michele A. Manahan, MD1; Carisa M. Cooney, MPH6; Gedge D. Rosson, MD6; (1)Department of Plastic and Reconstructive Surgery, Johns Hopkins University, Baltimore, MD, (2)Plastic and Reconstructive Surgery, John's Hopkins University, Baltimore, MD, (3)Johns Hopkins University School of Medicine, Baltimore, MD, (4)Johns Hopkins University, Baltimore, MD, (5)Plastic and Reconstructive Surgery, The Johns Hopkins Hospital, Baltimore, MD, (6)Department of Plastic and Reconstructive Surgery, Johns Hopkins University School of Medicine, Baltimore, MD Background: The rates of contralateral prophylactic mastectomy at the time of therapeutic mastectomy for unilateral breast cancer have more than tripled in the past decade, reaching 12.7% of cases. This is despite the lack of evidence for survival benefit associated with these procedures. Indeed, there is a lack of published data on postoperative outcomes for cases of contralateral prophylactic mastectomy followed by bilateral breast reconstruction (CBR) compared to unilateral mastectomy and breast reconstruction (UR). We performed the current study to investigate potential differences in morbidity and patient-reported quality of life (QoL) outcomes between these two groups. Methods: Using our IRB-approved, prospectively collected breast reconstruction patient registry, we queried pre- and post-operative data from patients who underwent CBR or UR at our institution. Data included patient demographics, comorbidities, surgical history, cancer treatment, pre-operative and 12-month post-final reconstruction Breast-Q© scores, breast reconstruction treatment, and post-operative complications. We used simple and multiple linear regression to compare morbidity and QoL changes between the study groups (CBR vs. UR). Satisfaction with abdomen domain was not included in the analyses due to the heterogeneity of reconstruction types, however, type of reconstruction was adjusted for in the adjusted analysis. Results: Between 2010 and 2015, 211 patients underwent CBR (n=86, 40.8%) or UR (n=125, 59.2%). While the unadjusted surgical morbidity was significantly higher for the BR group at 60 days post-tissue expander placement (p<0.001), it was not significantly different between groups immediately before final reconstruction, at 60 days post-final reconstruction, or at 1 year post-final reconstruction. After adjusting for age, BMI, type of reconstruction, timing of reconstruction, chemotherapy, radiotherapy, and previous breast surgery, CBR patients did not have a statistically significant difference in pre- to post-reconstruction changes of QoL when compared to UR in the domains of Satisfaction with Breast (p=0.62), Psychosocial Well-being (p=0.71), Sexual Well-being (p=0.85), and Chest Physical Well Being (p=0.09). Conclusion: Our findings suggest that performing a contralateral prophylactic mastectomy at the time of therapeutic mastectomy and bilateral breast reconstruction for unilateral breast cancer is not associated with higher QoL compared to unilateral mastectomy and breast reconstruction. While there was no increased morbidity at 1 year post-final breast reconstruction, there was a

higher rate of short-term (60-day) complications for staged breast reconstruction following tissue expander placement for the CBR group. These results would help in counseling patients interested in undergoing contralateral prophylactic mastectomy and bilateral breast reconstruction for unilateral breast cancer.

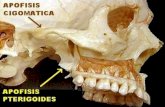
127. Surgeon-Based 3-D Printing for Vascularized Bone Transfers Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, 211, USA Erin M Taylor, MD; Division of Plastic Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA; Matthew L Iorio, MD; Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA Background: Three-dimensional (3-D) printing is a revolutionary technology with the capacity to design accurate physical models in preoperative planning. We present our experience in surgeon-based design of 3-D models using home 3-D software and printing technology for use as an adjunct in vascularized bone transfer. Methods: Home 3-D printing techniques were used in the design and execution of vascularized bone flap transfers to the upper extremity. MeshLab 3-D imaging software was used to convert preoperative 3-D computed-tomography scans to home 3-D printing data. A 3-D printer (M3D) created physical models of the anatomical defect requiring reconstruction, which were sterilized for use in the operating room. Vascularized bone flaps were designed intraoperatively based on the 3-D printed models. Results: Three-dimensional models were created for intraoperative use in vascularized bone flaps including 1) medial femoral trochlea (MFT) flap for scaphoid avascular necrosis and non-union (Figure 1), 2) MFT flap for lunate avascular necrosis and non-union, 3) medial femoral condyle (MFC) flap for wrist arthrodesis, and 4) free fibula osteocutaneous flap for distal radius non-union. Templates based on the 3-D models allowed for the precise and rapid contouring of well-vascularized bone flaps. All patients had successful osseous union and functional improvement following vascularized bone flap reconstruction. Conclusion: Surgeon-based 3-D-printing is a feasible, innovative technology that allows for the precise and rapid contouring of well-vascularized bone flaps. The technology is easy to use and convenient for the creation of models as compared to traditional send-out manufacturing. Surgeon-based 3-D printing has the potential of becoming a workhorse technology in vascularized bone transfer.
Figure 1: A) Proximal pole scaphoid avascular necrosis and fracture in 3-D imaging software and B) scaphoid 3-D printed to-scale with accurate proximal pole disruption.

.47. The Free Flap Fast-Track: Decreasing the Cost of Free Flaps by Minimizing Hourly Monitoring and Expediting Transfer out of the ICU Postoperatively Beth Israel Deaconess Medical Center, Boston, 211, USA Joseph A. Ricci, MD; Christina R Vargas, MD; Bernard T. Lee, MD, MBA; Division of Plastic and Reconstructive Surgery, Beth Isreal Deaconess Medical Center / Harvard Medical School, Boston, MA Introduction: Historically, identifying failing free flaps has required intense postoperative monitoring for more than 24 hours in a Post-Anesthesia Care Unit (PACU) or Intensive Care Unit (ICU) with hourly flap checks and one-to-one nursing; at a cost of thousands of dollars. Recently, the use of transcutaneous oxygen sensors (Vioptix; Freemont, CA) has resulted in the earlier detection of free flap issues, decreased flap loss and improved flap salvage rates. With routine continuous flap monitoring on all patients using Vioptix sensors, this study aims to identify whether the postoperative paradigm can safely be changed to permit the earlier transfer of patients from the PACU or ICU, to a standard inpatient units; with the goal of substantial cost savings without jeopardizing flaps. Materials and Methods: All consecutive Deep Inferior Epigastric Perforator (DIEP) Flaps performed at a single institution were reviewed and cases requiring a takeback to the operating room for flap related complications were collected. Data evaluated included patient demographics, the time course of the complication relative to the end of the initial procedure and outcomes like flap loss and salvage. Hourly costs for patient care in the ICU, PACU and surgical inpatient unit were obtained from the hospital financial office. A cost benefit analysis was performed with the Incremental Cost Effectiveness Ratio. Results: Over an 11 year span, 1128 DIEP flaps were performed with 56 takebacks occurring. A return to the operating room within 24 hours of the original procedure occurred with 20 flaps. At 14 hours postoperatively, the majority (15/20; 75%) of failing free flaps had been identified and brought back to the OR, with only six other flaps encountering problems between 15 and 24 hours postoperatively. Cost analysis revealed that after 14 hours of intensive monitoring, the cost of identifying each individual subsequent failing free flap exceeded the cost of one further hour of intensive monitoring. Conclusions: The paradigm for postoperative monitoring of free flaps has historically been intensive and costly. New monitoring techniques have improved flap success rates and less stringent monitoring algorithms are required in an effort to decrease healthcare expenditures. We propose a fast-track pathway for free flaps, reducing the amount of time spent in the intensive monitoring setting down to 14 hours, as patients can be safely monitored on standard surgical units with Vioptix monitoring at a significant cost savings and minimal risk of missing a failing free flap.

48. Bridge Over Troubled Waters: A Quantitative and Qualitative Data Study Analyzing Free Flaps using Near Infrared Spectroscopy The University of Chicago Medical Center, Chicago, 203, USA Amir Inbal, MD1; Adrian SH Ooi, MBBS, MMed, MRCS1; Benjamin T Lemelman, MD2; Chad Teven, MD1; Zach Collier, BA3; David H. Song, MD, MBA4; (1)University of Chicago Medical Center, Chicago, IL, (2)University of Chicago Medicine, Chicago, IL, (3)University of Chicago, Chicago, IL, (4)Section of Plastic and Reconstructive Surgery, Department of Surgery, University of Chicago Medical Center, Chicago, IL Background and objectives: With the advent of novel technologies, early detection of vascular compromise in free flap surgery is becoming an important aspect for perfecting outcomes. Recently, the tissue oximetry near infrared spectroscopy, ViOptix¨ has been shown to have the greatest impact in the post-operative period with decreased re-operations and increased salvage rates. While showing promise, there is a substantial learning curve that must be overcome in order to optimally employ the tissue oximetry technology. In order to facilitate rapid progression through the learning curve with the aim of mastering ViOptix¨ interpretation, we quantitatively and qualitatively characterized the different ViOptix¨ waveforms for arterial and venous compromise. Patients and Methods: We retrospectively reviewed all patients that underwent re-operation and exploration of their free flap due to a faulty ViOptix¨ reading between 2013 and 2016. The vascular etiology for flap compromise was collected and linked to each ViOptix¨ reading (figure 1-2). Quantitatively and qualitatively assessment of the waveforms was performed by calculations of the slopes and area-under-the-curve (AUC). Information on patient and flap characteristics as well as outcomes was analyzed. Results: Between 2013 and 2016, 14 free flaps had abnormal ViOptix¨ readings, which prompted flap re-exploration for vascular compromise. The waveforms of seven DIEP flaps, three SIEA flaps, one RFF flap, one SCIP flap, one FFF flap and one free LD flap were analyzed. At surgery, ten flaps were found to have a venous compromise etiology and four flaps had an arterial one. Venous compromise was associated with a sharper drop in tissue oximetry percentage reading over time (slope = 1.2% decrease per minute) compared to the arterial reading (slope = 0.9% decrease per minute), although not statistically significant at 95% confidence (p = 0.06). Following time interval standardization of the ViOptix¨ readings, using Area Under the Curve (AUC) calculations, determined that venous compromise group exhibited significantly greater AUC (2096 ± 637 units) than the arterial group (1410 ± 187 units, p = 0.01), which corroborates the finding that the venous group has a steeper slope (figure3-4). The vascular etiology for flap compromise was found to have a characteristic and consistent waveform. Conclusions: By quantitatively and qualitatively characterizing the different ViOptix¨ waveforms the etiology for vascular compromise can be detected in real time and the learning effect duration accelerated. This potentially allows the surgeon or anyone, anywhere for early detection and a specific response to the vascular compromise etiology.



49. Work-Related Physical Discomfort in ASRM Members: a Survey Mayo Clinic Arizona, Phoenix, 192, USA Ashley L. Howarth, MD; Mayo Clinic, Phoenix, AZ; Susan Hallbeck, PhD; Mayo Clinic, Rochester, MN; Raman C. Mahabir, MD; Plastic Surgery, Mayo Clinic, Phoenix, AZ; Valerie Lemaine, MD; Division of Plastic Surgery, Mayo Clinic, Rochester, MN; Gregory R. D. Evans, MD, FACS; Aesthetic and Plastic Surgey Institute, University of California at Irvine, Orange, CA; Shelley S. Noland, MD; Department of Orthopaedics and Sports Medicine, Mayo Clinic, Phoenix, AZ INTRODUCTION The risks of physical discomfort and injury are high in microsurgeons, who typically perform long surgeries under loupe magnification and with microscopes. The inherent ergonomic difficulties increase cervical strain and negatively affect posture. Identifying the prevalence and impact of work-related physical discomfort and injury will guide preventive strategies to prolong personal well-being, job satisfaction, and career duration. METHODS After Institutional Review Board approval, a 29 question survey was designed to evaluate microsurgeons and their risk of occupational injury and current levels of physical discomfort. The survey was sent to the membership of the American Society for Reconstructive Microsurgery. It was administered and responses were collected via the Mayo Clinic Survey Center. RESULTS There were 118 respondents, 79% male, 71% aged 31-50 years old. The practice profiles were primarily academic (68%) and private practice (26%). On a scale of 0-10 (0 no pain, 10 worst pain imaginable), work-related physical discomfort had a median of 3 for standard surgery (no loupes/microscope), 5 for surgery with loupes, and 6 for surgery with a microscope. The most common location of pain during, immediately after, and day after surgery was the neck (median 4, 4, 2.5) followed by the shoulder, upper back, and lower back. Within one week of the survey, 82% had nonzero pain, median of 4. Pain was reported within the first four hours of surgery in half of respondents. Over half (57%) feel that pain will influence their ability to perform surgery in the future. Operating time was often more than eight hours per day (46%) and more than three days per week (32%). Surgeon discomfort affects posture (71%), stamina (36%), sleep (28%), relations with others (25%), concentration (23%), and surgical speed (19%). Tremor caused by work-related physical discomfort was present in 9%. Medical treatment for discomfort was sought by 73%. Time off work for treatment or rehabilitation occurred in 8%. CONCLUSION Work-related physical discomfort is a critical and urgent issue amongst microsurgeons. Nearly all microsurgeons surveyed experience physical discomfort on a regular basis. This negatively impacts many spheres of life and often requires medical treatment. More than half of the respondents felt that their physical discomfort would limit their future careers, perhaps the most concerning finding. It is imperative that microsurgeons employ preventive strategies to combat work-related physical discomfort.

50. A Prospective Trial of Rapid Point of Care Coagulation Testing in Free Tissue Transfer: Applications for Personalized Microsurgical Care University of California, San Francisco, San Francisco, 194, USA Eric D Wang, MD1; Alvin Wong, MD1; Jeffrey Go, MS, BA1; Benedict Del Buono, BA1; Helen Park, BA1; Sarosh Zafar, MD2; Michael J. Terry, MD3; Jason H. Pomerantz, MD4; William Y. Hoffman, MD4; Scott L. Hansen, MD3; Mitchell J Cohen, MD1; Hani Sbitany, MD3; Esther A. Kim, MD3; (1)University of California San Francisco, San Francisco, CA, (2)University of California, San Francisco, San Francisco, CA, (3)Plastic and Reconstructive Surgery, University of California, San Francisco, San Francisco, CA, (4)Department of Surgery, DIvision of Plastic and Reconstructive Surgery, University of California, San Francisco, San Francisco, CA Introduction: Imbalances in hemostatic factors can result in devastating microsurgical complications. Novel point of care tests, such as rotational thromboelastometry (RoTEM) and platelet impedance aggregometry (IA) have been adopted in other disciplines for measuring dynamic changes in coagulation. We investigated microsurgical applications of these tests for quantifying overall thrombotic potential and specific risk factors preoperatively. Methods: With institutional approval, consecutive patients undergoing microsurgical free tissue transfer were enrolled in our prospective observational study. Serial phlebotomy was performed pre- and postoperatively, after standardized administration of aspirin and subcutaneous heparin. We analyzed blood samples using RoTEM (TEM USA, Durham, NC) and Multiplate IA (Roche USA, South San Francisco, CA) in addition to conventional complete blood count and coagulation parameters (PT/aPTT). RoTEM measures mechanical properties of evolving clot, whereas Multiplate IA measures changes in electrical impedance caused by platelet aggregation. Both investigational techniques utilize whole blood across multiple parallel channels, allowing isolation of specific pathways with the addition of agonists and inhibitors. Our primary outcome was unexplained intraoperative or postoperative anastomotic thrombosis requiring revision or reoperation. Data were analyzed using Fisher’s exact, Student’s t-test and logistic regression, with statistical significance defined at an alpha < 0.05. Results: Over an initial 10-month study period, 52 patients met criteria and had complete serial data sets for analysis. Fifteen patients (28.8%) experienced the primary outcome of unexplained flap thrombosis, but a majority of these (14/15, 93%) were successfully salvaged. The thrombosis cohort was significantly younger and less likely to have an active oncologic diagnosis. Multiplate IA demonstated that the thrombotic cohort had approximately half the relative response to standardized postoperative aspirin dosing compared to controls (31.6 vs 62.1%, p=0.005). RoTEM detected a preoperative hypercoagulable phenotype among this cohort, with shorter clot formation times and stronger clot firmness compared to controls. In multivariate logistic modeling, these factors were found to be independent predictors of thrombosis, with OR 1.06 (95%CI 1.02-1.11) and OR 1.44 (95%CI 1.17-1.79), respectively. Receiver operating characteristic analysis found our preoperative model to be a robust discriminator of hypercoagulability (AUC = 0.859). Conclusions: In our prospective observational study, RoTEM and Multiplate IA can preoperatively identify a hypercoagulable phenotype. Our ongoing prospective study will further validate our predictive

model and develop criteria for their application in microsurgery. This technology could allow for preoperative risk stratification and the selection of alternative reconstructive methods or timing for patients with abnormal coagulation.