3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 53 … · 2018-08-07 · scan with the Voluson...
7
Sonography of the Fetal Cochlea in the Early Second Trimester of Pregnancy search of all National Center for Biotechnology Information resources focused on sonography of the fetal middle or inner ear retrieved no results. Prenatal sonographic visual- ization of the fetal middle and inner ear is hampered by acoustic shadowing of the temporal bones and, probably, for this reason has not previously been reported. Contrary to sonography, the contri- bution of magnetic resonance imaging (MRI) in the prenatal diag- nosis of middle and inner ear abnormalities has been investigated in recent years. 1 Zvi Leibovitz, MD, Sandro Egenburg, MD, Ayala Arad, MD, Simon Degani, MD, Hasan Bakry, MD, Israel Shapiro, MD, Gonen Ohel, MD Received May 29, 2012, from the Departments of Obstetrics and Gynecology (Z.L., S.D., H.B., I.S., G.O.) and Pathology (S.E., A.A.), Bnai Zion Medical Center, Haifa, Israel. Revision requested June 20, 2012. Revised manuscript accepted for publication June 26, 2012. We thank Catherine Garel, MD, for contri- butions in preparing the manuscript. Address correspondence to Zvi Leibovitz, MD, Department of Obstetrics and Gynecology, Bnai Zion Medical Center, PO Box 4940, 31048 Haifa, Israel. E-mail: [email protected] Abbreviations MRI, magnetic resonance imaging; 3D, 3- dimensional; 2D, 2-dimensional A ©2013 by the American Institute of Ultrasound in Medicine | J Ultrasound Med 2013; 32:53–59 | 0278-4297 | www.aium.org ORIGINAL RESEARCH Objectives—To examine the feasibility of imaging the fetal cochlea in the early second trimester. Methods—This study included 42 healthy fetuses of low-risk pregnancies between 14 and 16 weeks. The coronal head sections via sagittal and lateral acoustic windows were used for cochlear visualization. The coronal plane was directed across the thalamus, oriented to the petrous part of the temporal bones. All fetuses were examined by 2-dimensional (2D) transvaginal sonography. Transabdominal scans were added in 11 fetuses at 16 weeks. Three-dimensional (3D) multiplanar reconstruction was used for coronal plane refor- matting in cases with inappropriate head positioning for 2D scanning. Results—Because of temporal bone hypomineralization in the early second trimester, sonographic depiction of the cochlear labyrinth was possible. On coronal imaging, the cochleas showed ringlike echogenic borders containing hypoechoic liquid content. The cochlear modiolus appeared as a central echogenic round spot (“cochlear target sign”). The cochleas were observed caudad to the temporal lobes, separated by the clivus. Shifting of the coronal plane showed progressive coiling of the basal cochlear turn toward the second turn (“cochlear whirlpool sign”). Two-dimensional transvagi- nal scanning showed at least 1 cochlea in 79% (33 of 42) of the cases. Adding 3D mul- tiplanar reconstruction, at least 1 cochlear target sign was observed in 83% (35 of 42). The cochlear whirlpool sign on at least one side was shown in 57% (24 of 42). The max- imal cochlear diameter was measured in fetuses with clear cochlear margin visualiza- tion. In this subgroup, the mean gestational age ± SD was 15.8 ± 0.5 weeks, and the mean maximal cochlear diameter was 6.4 ± 0.8 mm. Conclusions—Prenatal sonographic inner ear depiction was previously considered impossible. Using a unique time window in the early second trimester, we achieved fea- sible fetal cochlear imaging. Key Words—cochlear target sign; cochlear whirlpool sign; fetal cochlea; sonography Videos online at jultrasoundmed.org
Transcript of 3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 53 … · 2018-08-07 · scan with the Voluson...

Sonography of the Fetal Cochlea in theEarly Second Trimester of Pregnancy
search of all National Center for Biotechnology Informationresources focused on sonography of the fetal middle orinner ear retrieved no results. Prenatal sonographic visual-
ization of the fetal middle and inner ear is hampered by acousticshadowing of the temporal bones and, probably, for this reason hasnot previously been reported. Contrary to sonography, the contri-bution of magnetic resonance imaging (MRI) in the prenatal diag-nosis of middle and inner ear abnormalities has been investigated inrecent years.1
Zvi Leibovitz, MD, Sandro Egenburg, MD, Ayala Arad, MD, Simon Degani, MD, Hasan Bakry, MD, Israel Shapiro, MD, Gonen Ohel, MD
Received May 29, 2012, from the Departments ofObstetrics and Gynecology (Z.L., S.D., H.B., I.S.,G.O.) and Pathology (S.E., A.A.), Bnai ZionMedical Center, Haifa, Israel. Revision requestedJune 20, 2012. Revised manuscript accepted forpublication June 26, 2012.
We thank Catherine Garel, MD, for contri-butions in preparing the manuscript.
Address correspondence to Zvi Leibovitz,MD, Department of Obstetrics and Gynecology,Bnai Zion Medical Center, PO Box 4940, 31048Haifa, Israel.
E-mail: [email protected]
AbbreviationsMRI, magnetic resonance imaging; 3D, 3-dimensional; 2D, 2-dimensional
A
©2013 by the American Institute of Ultrasound in Medicine | J Ultrasound Med 2013; 32:53–59 | 0278-4297 | www.aium.org
ORIGINAL RESEARCH
Objectives—To examine the feasibility of imaging the fetal cochlea in the early secondtrimester.
Methods—This study included 42 healthy fetuses of low-risk pregnancies between 14 and16 weeks. The coronal head sections via sagittal and lateral acoustic windows were used forcochlear visualization. The coronal plane was directed across the thalamus, oriented tothe petrous part of the temporal bones. All fetuses were examined by 2-dimensional (2D)transvaginal sonography. Transabdominal scans were added in 11 fetuses at 16 weeks.Three-dimensional (3D) multiplanar reconstruction was used for coronal plane refor-matting in cases with inappropriate head positioning for 2D scanning.
Results—Because of temporal bone hypomineralization in the early second trimester,sonographic depiction of the cochlear labyrinth was possible. On coronal imaging,the cochleas showed ringlike echogenic borders containing hypoechoic liquid content.The cochlear modiolus appeared as a central echogenic round spot (“cochlear targetsign”). The cochleas were observed caudad to the temporal lobes, separated by theclivus. Shifting of the coronal plane showed progressive coiling of the basal cochlearturn toward the second turn (“cochlear whirlpool sign”). Two-dimensional transvagi-nal scanning showed at least 1 cochlea in 79% (33 of 42) of the cases. Adding 3D mul-tiplanar reconstruction, at least 1 cochlear target sign was observed in 83% (35 of 42).The cochlear whirlpool sign on at least one side was shown in 57% (24 of 42). The max-imal cochlear diameter was measured in fetuses with clear cochlear margin visualiza-tion. In this subgroup, the mean gestational age ± SD was 15.8 ± 0.5 weeks, and themean maximal cochlear diameter was 6.4 ± 0.8 mm.
Conclusions—Prenatal sonographic inner ear depiction was previously consideredimpossible. Using a unique time window in the early second trimester, we achieved fea-sible fetal cochlear imaging.
Key Words—cochlear target sign; cochlear whirlpool sign; fetal cochlea; sonography
Videos online at jultrasoundmed.org
3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 53

We present a study aimed at showing the fetal cochleaon prenatal sonography, which to our knowledge has notbeen reported previously. It was assumed that incompleteossification of the temporal bones in the early secondtrimester will enable sufficient ultrasound penetration toachieve sonographic imaging of the fetal cochlea.
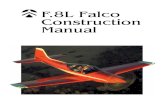
Fetal cochleas develop in a unique early acceleratedpattern. These internal auditory organs look dispropor-tionally large in a fetal head dissection at the end of firsttrimester (Figure 1). Jeffery and Spoor2 investigated fetalcochlear size by postmortem high-resolution MRI. Theyfound that the prenatal labyrinth attains an adult-equivalentsize between 17 and 19 weeks’ gestation. Nemzek et al3
measured the basal cochlear turn diameter in fetal speci-mens by postmortem computed tomography and MRI.The basal cochlear turn diameter ranged from 5 mm at 14weeks to 9 mm at 24 weeks. It appears that the fetal cochleain the early second trimester is large enough for measurementby sonography.
Anatomically, the cochlear labyrinth is located in themedioanterior area of the petrous part of the temporalbone, and the vestibular apparatus occupies its posteriorregion. The cochlear modiolus axis is directed anteriorly
with the basal cochlear turn in its posterior end. This spa-tial orientation of the cochleas results in their typical coiledappearance on a coronal section through the fetal head(Figure 2B).
Most inner ear malformations arise when formationof the membranous labyrinth is interrupted during the firsttrimester of pregnancy. The arrested transformation of theotic vesicle into the normal cochlea and vestibule may beeither a result of an inborn genetic error or a consequenceof teratogenic exposure during the weeks of inner earorganogenesis.4
Materials and Methods
This research was conducted as an observational cohortstudy. Approval for the study was given by the InstitutionalReview Board (Helsinki Committee protocol), includingacquisition of informed consent for sonographic examina-tions from all patients.
Intending to show the fetal cochlea, we performed42 sequential fetal scans at 14 to 16 gestational weeks.All patients had singleton low-risk pregnancies with normalfetal anatomy and growth. The examinations were performedwith a Voluson 730 Expert ultrasound machine (GE Health-care, Milwaukee, WI) using RIC 5-9H/OB endovaginaland RAB 4-8L/OB abdominal probes. Based on thecochlear orientation within the petrous part of the tempo-ral bone (Figures 1 and 2B), coronal insonation planeswere applied for cochlear imaging.
In the sonographic coronal plane, as in the pathologicdissection, the cochleas were shown in their typical coiledshape (Figure 2A). On the sonogram, the cochlearlabyrinth showed ringlike echogenic borders containinghypoechoic liquid content. The cochlear modiolus appearedas a central echogenic round spot. The term proposed forthis sonographic appearance was the “cochlear target sign.”The cochleas were observed caudad to the temporal lobes,separated by the clivus in the midline (Figure 2).
For depiction of the cochlear target sign via the ante-rior fontanel or sagittal suture, the coronal plane wasdirected across the thalamus, oriented to the petrous partof the temporal bones. On coronal scanning through themastoid fontanel or the posterior part of the squamoussuture, the cochlea enters the plane just posterior to theauricular edge (Figure 3). To minimize temporal boneshadowing, the insonation plane was oriented perpendi-cular to the mastoid fontanel and posterior part of thesquamous suture.
All fetuses were scanned by 2-dimensional (2D) coro-nal head planes using the endovaginal probe. In addition,
Leibovitz et al—Sonography of the Fetal Cochlea in the Early Second Trimester
J Ultrasound Med 2013; 32:53–5954
Figure 1. Coronal head dissection of a 13-week abortus. The cochleas(co) are cross-sected at the level of their basal turns (bt). The modiolus(mo) is indicated in the center of the cochlear labyrinth. The labyrinthsappear within soft hypo-ossified tissue of the temporal bones. The cochlear basal turn diameter (btd) was 5 mm in this specimen, andthe skull biparietal diameter (bpd) was 21 mm, with a basal turndiameter/biparietal diameter ratio of 0.24. See the measurements fromthe 16-week fetus in Figure 2 for comparison.
3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 54

J Ultrasound Med 2013; 32:53–59 55
Leibovitz et al—Sonography of the Fetal Cochlea in the Early Second Trimester
Figure 2. A, Coronal head sonogram of a 16-week fetus. This image was obtained by insonation through the anterior fontanel on a transabdominalscan with the Voluson 730 Expert machine and the RAB 4-8L/OB probe. The cochlear target sign (co) is indicated. B, Corresponding pathologicimage. The clivus is marked by the asterisk. In this fetus, the cochlear basal turn diameter was 7 mm, and the skull biparietal diameter was 36 mm, witha ratio of 0.18. See the measurements from the 13-week abortus in Figure 1 for comparison.
Figure 3. A–C, Sequential transvaginal coronal sonograms of the same fetus with 90° rotation. There is a progressive entrance of the cochlear struc-ture (co) into the image during the shift of the insonation plane behind the fetal auricle (asterisk). Cochlear insonation in this case was achievedthrough the mastoid fontanel. The maximal cochlear diameter is the distance between the arrowheads in C.
3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 55

in 11 of 42 cases, transabdominal scanning of the fetal headwas performed. For the probe facing the lateral fetal headaspect, scanning was performed through the squamoussuture and mastoid fontanel. For the probe facing thevertex, the scan was done via the anterior fontanel andsagittal suture.
In the cases with difficult coronal imaging by 2D scan-ning (usually due to inappropriate fetal head positioning),3-dimensional (3D) sonography was used to create aproper coronal plane for cochlear depiction. It wasachieved by a 3D multiplanar reconstruction display in the4D View application (GE Healthcare). With this applica-tion, the fetal head was orientated in 3 standard orthogo-nal planes: multiplanar reconstruction plane A for thecoronal section, multiplanar reconstruction plane B for themedian section, and multiplanar reconstruction plane C
for the axial section. In the median section, the fetal headwas upwardly positioned at an angle of 20° to 30° betweenthe clivus and vertical axis. This 3D multiplanar recon-struction display setup provides conventional identifica-tion of the left and right fetal head sides on axial andcoronal sections. Continuing to operate in the median sec-tion, the multiplanar reconstruction navigation point wasmoved to the clivus at the level of the lower vermian edge(Figure 4). This step resulted in depiction of the cochleartarget sign in the coronal section. For optimization of 3Dmultiplanar reconstruction cochlear imaging, the volumeacquisition plane was as close to the coronal plane as possible.Cochlea imaging by the 3D multiplanar reconstructiondisplay was also tested by activation of the static volumecontrast imaging mode using a minimal slice thickness(1–2 mm).
Leibovitz et al—Sonography of the Fetal Cochlea in the Early Second Trimester
J Ultrasound Med 2013; 32:53–5956
Figure 4. Three-dimensional approach to cochlear imaging in a 15-week fetus. A, The acoustic window of the mastoid fontanel and the squamoussuture is shown by the maximal-mode rendering algorithm in the initial acquisition. B, Three-dimensional multiplanar reconstruction display of thesame volume after standard head orientation (see “Materials and Methods”). The navigation point (red spot) is placed close to the clivus at the levelof the inferior vermian margin (yellow dashed line). In this navigation setup, the cochleas (co) are shown in the coronal section.
3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 56

Performing fine back-and-forth coronal plane shifting,we observed progressive coiling of the basal cochlear turntoward the second turn. We named this dynamic findingthe “cochlear whirlpool sign,” This impressive imagingeffect was achieved either by delicate probe movement ona 2D B-mode scan or by coronal slicing on the 3D multi-planar reconstruction display. Videos 1 and 2 show thecochlear whirlpool and target signs, respectively.
Our study parameters included the visualization ratefor the fetal cochlear target and whirlpool signs in vertexand lateral head approaches. An additional study parameterwas the maximal cochlear diameter. The method for meas-urement of the maximal diameter is shown in Figure 3C.The calipers were placed on the outer echogenic edges ofthe cochlear target sign. Its widest diameter correspondedto the size of the basal cochlear turn.
Results
Two-dimensional transvaginal coronal fetal head scanningshowed at least 1 cochlea in 79% (33 of 42) of all cases.In 6 fetuses, the proper insonation plane was not achievedbecause of inappropriate head positioning, and in 3 othercases, the resolution was suboptimal because of a deephead location in the scanning plane. When the 3D multi-planar reconstruction display was used for reformatting ofthe coronal plane, at least 1 cochlear target sign was observedin 83% (35 of 42) of all cases. The cochlear whirlpool sign onat least one side was shown in 57% (24 of 42) of all fetuses.It was possible only by the transvaginal imaging, applyingcoronal plane shifting along the cochlear axis, as describedin “Materials and Methods.”
When the probe faced the lateral fetal head aspect,cochlear scanning was performed through the mastoidfontanel and posterior part of the squamous suture. Thislateral head scanning was achieved in all 42 fetuses. By suchan approach, the proximal cochlea (close to the probe) wasvisualized in 83% (35 of 42) of all fetuses by combining the2D and 3D multiplanar reconstruction imaging modes.Both cochleas were observed in 40% (17 of 42) of all cases.Depiction of the distal cochlea (remote from the probe)was less clear compared to the proximal one.
When the probe was oriented toward the upper headaspect, scanning was performed via the anterior fontanel andsagittal suture. Such an approach was technically feasible dur-ing the scans of 31 fetuses. In this subgroup of fetuses, unilat-eral and bilateral cochlear depictions were achieved in 62%(19 of 31) and 77% (24 of 31) of these cases, respectively.Cochlear images through the anterior fontanel and sagittalsuture had lower quality compared to lateral head scanning.
Transabdominal cochlear imaging was less effectiveand had a lower resolution compared to transvaginal imag-ing. The cochlear target sign was shown in 54% (6 of 11)of the fetuses in abdominal scanning subgroup. Cochlearvisualization was bilateral in most of them (5 of 6).
No cases of cochlear depiction were added by activationof static volume contrast imaging. However, it was our sub-jective impression that thin-slice static volume contrast imag-ing provided a more clear perception of the cochlear edges.
Measurement of the maximal cochlear diameter wasapplied only when clear cochlear margins were visualized.It was feasible in the subgroup of 31 fetuses with clear depic-tion of the proximal cochlea by the transvaginal lateral headapproach (Figure 3C). In this subgroup of the fetuses, themean gestational age ± SD was 15.8 ± 0.5 weeks, and themean maximal cochlear diameter was 6.4 ± 0.8 mm.
Discussion
Bilateral severe congenital hearing loss in the human pop-ulation appears in about 1 per 1000 live births. It is esti-mated that about half of the affected infants or childrenhave hereditary deafness.5–8 Congenital membranous mal-formations of the cochlear duct are responsible for approx-imately 80% of the cases of congenital sensorineuralhearing loss.4 In these malformations, the bony architec-ture of the inner ear is usually normal on computed tomog-raphy and MRI. Bony inner ear malformations representthe remaining 20% of congenital sensorineural hearing losscases. In this group, the malformations can readily be diag-nosed by computed tomographic and MRI analysis.9,10
In 1987, Jackler et al4 proposed one of the most widelyaccepted classifications of inner ear malformations.According to this radiologic classification, there are severaldistinctive vestibulocochlear malformations: (1) completelabyrinthine aplasia, in which there is complete lack of innerear development (Michel aplasia); (2) cochlear aplasia,characterized by a complete lack of cochlear development;(3) common cavity malformation, in which the cochleaand vestibule form a common cavity without internalarchitecture; (4) cochlear hypoplasia, in which a smallcochlear bud contains a decreased number of turns; and(5) incomplete partition, characterized by a small cochleawith an incomplete or interscalar septum. The last two cat-egories are related to Mondini-Alexander dysplasia in anearlier classification scheme by Omerod.11 Park et al12
reported outcomes of 46 pediatric patients with congenitalinner ear malformations. Twenty percent of them had adiagnosis of absence of cochlear structures on radiologicstudies of the temporal bones.
J Ultrasound Med 2013; 32:53–59 57
Leibovitz et al—Sonography of the Fetal Cochlea in the Early Second Trimester
3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 57

The distribution of causes of profound hearing loss ininfancy includes environmental etiologies in 50% (viralinfection by cytomegalovirus, rubella, measles, herpes sim-plex virus, neonatal jaundice, neonatal meningitis, prema-turity, and ototoxic drugs). The remaining 50% of cases areof genetic origin. Of them, 70% are nonsyndromic geneticdisorders (autosomal dominant deafness [DFNA] genes,autosomal recessive deafness [DFNB] genes, X-linked deaf-ness [DFN] genes, and rare cases of mitochondrial inher-itance).13 Abnormal connexin 26 protein is the mostcommon cause of nonsyndromic deafness. Connexin 26is a gap junction protein in the inner ear cells. Its functionis important in potassium concentration regulation.Abnormal connexin 26 causes an improper potassiumgradient. It results in the inability of hair cells to generatean action potential. Mutations in the gap junction beta 2(GBJ2) gene result in production of the nonfunctionalconnexin 26. It is related to about 50% of children withsevere to profound nonsyndromic autosomal recessivehearing loss.14 Syndromic etiologies of congenital hearingloss are responsible for about 30% of cases. There are morethan 400 forms of syndromic deafness, including Ushersyndrome, Pendred syndrome, Alport syndrome, Waar-denburg syndrome, Jervell and Lange-Neilsen syndrome,and branchio-oto-renal syndrome.13
Our study represents a new approach to prenatalimaging of the cochlear labyrinth. We used a unique oppor-tunity in the early second trimester when the hypominer-alized fetal temporal bone provided an acoustic windowfor sonography of the cochlea. Because of its rapid growthin the late first and early second trimesters, the fetal cochleaappears as an observable organ in the coronal transpetrosalplane of the fetal head.
We achieved a high feasibility rate of fetal cochleardepiction using coronal head scanning through the mas-toid fontanel or squamous suture. Interesting results wereretrieved from the subgroup of 31 fetal scans in which theheads were in the appropriate position for coronalinsonation and were located in the optimal focal zone ofthe sonographic plane. In these fetuses, the cochlear tar-get sign (at least on one side) was always observed. Thisobservation is very reassuring because nonvisualizationof the cochleas in our study was related to technical imag-ing obstacles. For this reason, repeated examinations andfetal head manipulation might improve the cochleardepiction rate. The most important limitation of sono-graphic fetal cochlear imaging is ossification of the tem-poral bones. It causes acoustic shadowing, which hidescochlear structures in fetal scans at more advanced gesta-tional ages.1
On the basis of our results, we hypothesize that earlysecond-trimester cochlear sonography may be of value inthe diagnosis of cochlear aplasia. This malformation mayappear as a familial autosomal dominant or familial auto-somal recessive disorder. It had also been reported withthe Klippel-Fiel anomaly, Wildervanck syndrome, thalido-mide embryopathy, and anencephaly. A complete lack ofinner ear development may be bilateral or unilateral. It maybe associated with other abnormalities caused by failure ofthe otic placode. These include middle ear anomalies,hypoplasia of the petrous bone, and abnormal courses ofthe transverse sinus and jugular veins.15
The much more complicated question is whether ourdata may be helpful in the diagnosis of the cochlearhypoplasia (Mondini-Alexander dysplasia). As mentionedin the classification of Jackler et al,4 cochlear hypoplasia ischaracterized by a small cochlear bud with a decreasednumber of turns. Normal human cochlear coiling consistsof 2.5 turns. In a pathologic dissection of the fetal inner ear,complete coiling is observed at 8 to 9 weeks’ gestation.16
Depiction of all cochlear turns was impossible in our study.In the subgroup of the 31 scans with optimal cochlear visu-alization, the cochlear whirlpool sign was observed in 77%(24 of 31) of the fetuses. However, we could not count morethan 2 cochlear turns, which means that incomplete cochlearrotation is an unreliable finding on cochlear sonography.
The maximal cochlear diameter in our study was relatedto the size of the basal cochlear turn and showed good cor-relation with the results of Nemzek et al.3 However, ourmeasurements were not confirmed in a case-control studyincluding fetuses with cochlear hypoplasia. For this reason,the results for the maximal cochlear diameter have limitedvalue in the diagnosis of fetal cochlear hypoplasia.
Summarizing our findings, we can conclude that fetalcochlear imaging in the early second trimester is feasible ifhigh-resolution sonography is used and proper coronalfetal head scanning is performed.
References
1. Katorza E, Nahama-Allouche C, Castaigne V, et al. Prenatal evaluation ofthe middle ear and diagnosis of middle ear hypoplasia using MRI. PediatrRadiol 2011; 41:652–657.
2. Jeffery N, Spoor F. Prenatal growth and development of the modernhuman labyrinth. J Anat 2004; 204:71–92.
3. Nemzek WR, Brodie HA, Chong BW, et al. Imaging findings of the devel-oping temporal bone in fetal specimens. AJNR Am J Neuroradiol 1996;17:1467–1477.
4. Jackler RK, Luxford WM, House WF. Congenital malformations of theinner ear: a classification based on embryogenesis. Laryngoscope 1987;97:2–14.
Leibovitz et al—Sonography of the Fetal Cochlea in the Early Second Trimester
J Ultrasound Med 2013; 32:53–5958
3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 58

5. Morton NE. Genetic epidemiology of hearing impairment. Ann NY AcadSci 1991; 36:16–31.
6. Davis A, Wood S. The epidemiology of childhood hearing impairment:factors relevant to planning of services. Br J Audiol 1992; 26:77–90.
7. Martin JAM. Aetiological factors relating to childhood deafness in theEuropean community. Audiology 1982; 21:149–158.
8. Parving A. Hearing screening: aspects of epidemiology and identificationof hearing impaired children. Int J Pediatr Otorhinolaryngol 1999; 49(suppl1):S287–S292.
9. Antonelli PJ, Varela AE, Mancuso AA. Diagnostic yield of high resolutioncomputed tomography for pediatric sensorineural hearing loss. Laryngo-scope 1999; 109:1642–1647.
10. McClay JE, Tandy R, Grundfast K, et al. Major and minor temporal boneabnormalities in children with and without congenital sensorineural hear-ing loss. Arch Otolaryngol Head Neck Surg 2002; 128:664–671.
11. Omerod FC. The pathology of congenital deafness. J Laryngol Otol 1960;74:919–950.
12. Park AH, Kou B, Hotaling A, Azar-Kia B, Leonetti J, Papsin B. Clinicalcourse of pediatric inner ear malformation. Laryngoscope 2000; 110:1715–1719.
13. American College of Medical Genetics. Genetics evaluation guidelinesfor the etiologic diagnosis of congenital hearing loss. Genetic Evaluationof Congenital Hearing Loss Expert Panel. ACMG statement. Genet Med2002; 4:162–171.
14. Kemperman, MH, Hoefsloot LH, Cremers CW. Hearing loss and con-nexin 26. J R Soc Med 2002; 95:171–177.
15. Scott DA, Carey JC. Inner ear. In: Stevenson RE, Hall JG (eds). HumanMalformations and Related Anomalies. 2nd ed. New York NY: Oxford Uni-versity Press; 2006:366–371.
16. Pujol R, Lavigne-Rebillard M. Early stages of innervation and sensory celldifferentiation in the human organ of Corti. Acta Otolaryngol 1985;423:43–50.
J Ultrasound Med 2013; 32:53–59 59
Leibovitz et al—Sonography of the Fetal Cochlea in the Early Second Trimester
3201jumv-online.qxp:Layout 1 12/20/12 9:05 AM Page 59