3- Pneumonia 1435
33
Pneumonia Dr. Layla Borham
-
Upload
maram-abdullah -
Category
Documents
-
view
18 -
download
2
description
3- Pneumonia 1435.pd
Transcript of 3- Pneumonia 1435
Pneumonia
Dr. Layla Borham

Objectives
By the end of the lecture you are able to:
• Define pneumonia.
• Know classification of pneumonia.
• Describe the different antimicrobial regimens
used for treatment of pneumonia.
Dr. Layla Borham

Clinical Case • A 15 year old female with a history of hay fever develops fever,
headache and malaise for 4 days followed by a nonproductive cough
and scratchy throat.
• On examination, her temperature is 28.5°C, pulse 90 beats/min, BP
110/70, respiratory rate 20 beats/min.
• Physical examination is unremarkable except for scattered rales over
the left lower lung. Chest X ray reveals a patchy left lower lobe
infiltrate. Diagnosis was pneumonia. Erythromycin was prescribed.
• What is erythromycin? what other antimicrobials used in pneumonia?
• If she is taking antihistamines, what drug interaction might occur?
Dr. Layla Borham

4 Dr. Layla Borham
• Infection of the alveoli, distal airways, and
interstitium.
Classification
• Community-acquired pneumonia (CAP)
• Healthcare-acquired pneumonia (HCAP)
1. Hospital-acquired pneumonia (HAP)
2. Ventilator-associated pneumonia (VAP)

Pneumonia • Treatment of pneumonia depends largely on the empiric use of
antibiotic regimens directed against potential pathogens.
• Direct the use of antibiotic agents in bacterial pneumonia based on
laboratory data as well as clinical response.
• The possibility of Legionella infection should always be considered
when evaluating CAP, because delayed treatment significantly
increases mortality.
• The most prevalent causative organism is Streptococcus
pneumoniae, regardless of the host or the setting; empiric therapy
must be selected with this consideration in mind. Dr. Layla Borham

Drugs used in the treatment of Pneumonia
Dr. Layla Borham
Pneumonia
• A prudent course of action for empiric outpatient
therapy is to include:
(1) One of the macrolide agents plus a second- or third-
generation cephalosporin or amoxicillin and
clavulanate or
(2) Trimethoprim and sulfamethoxazole (TMP-SMZ) as a
single agent.
Dr. Layla Borham

Pneumonia
• Patients who have moderate clinical impairment or co-
morbidity are best treated with parenteral agents:
(1) Macrolide plus a second-generation or third-
generation cephalosporin, (as single agents) or
(2) Ampicillin and sulbactam (Unasyn), or
(3) Piperacillin and tazobactam (Zosyn), or
(4) Ticarcillin and clavulanate (Timentin).
Dr. Layla Borham

I. Macrolides
Azithromycin, Clarithromycin, Erythromycin
• Macrolide acts by inhibition of protein synthesis to arrest
bacterial growth.
• Macrolides provide the best coverage for the most likely
organisms in community-acquired bacterial pneumonia (CAP).
• It is the initial drug of choice, as they have effective coverage
for gram-positive, Legionella, and Mycoplasma organisms.
• Newer macrolides Azithromycin has better action against H
influenzae compared with erythromycin, and offers improved
compliance because of reduced dosing frequency and less GIT
adverse effects. Dr. Layla Borham

II. Cephalosporins • Second-generation cephalosporins (Cefprozil, Cefaclor, and
Cefuroxime) provide adequate activity against Gm +ve organisms.
• Third-generation cephalosporins (Cefotaxime, Ceftazidime,
Ceftriaxone) have wider activity against most gram-negative
bacteria, including beta-lactamase–producing strains and may be
effective against ampicillin-resistant S pneumoniae.
• IV cephalosporins may be combined with a macrolides. They
broaden the gram-negative coverage, and in the case of third-
generation agents, they may be effective against resistant S
pneumoniae. Dr. Layla Borham

• Cefepime is the best beta-lactam for IM administration.
This agent is a fourth-generation cephalosporin that has
gram-negative coverage comparable to ceftazidime but
with better gram-positive coverage (comparable to
ceftriaxone).
• Ceftaroline fifth-generation cephalosporins indicated
for community-acquired bacterial pneumonia.
• Activity against aerobic and anaerobic gram-positive
and aerobic gram-negative bacteria.
Dr. Layla Borham

III. Aztreonam (Azactam) • It is a monobactam, not a beta-lactam, antibiotic that
inhibits cell wall synthesis during bacterial growth.
• This agent has activity against gram-negative bacilli
but very limited gram-positive activity, and it is not
useful for anaerobes.
• It may be used in patients allergic to penicillins or
cephalosporins.
• As with all antibiotics eliminated by the kidneys, obtain
estimates of the CrCl, and make appropriate dosage
modifications. Dr. Layla Borham

IV. Fluoroquinolone: Ciprofloxacin • Fluoroquinolone that inhibits bacterial DNA synthesis
and, consequently, growth, by inhibiting DNA gyrase
and topoisomerases.
• Quinolones have broad activity against gram-positive
and gram-negative aerobic organisms but no activity
against anaerobes.
• Continue ciprofloxacin treatment for at least 2 days (7-
14 d typical) after the patient's signs and symptoms have
disappeared.
Dr. Layla Borham
V. Clindamycin
• Lincosamide semisynthetic antibiotic inhibits bacterial
growth, possibly by blocking protein synthesis.
• Clindamycin is also effective against aerobic and
anaerobic streptococci (except enterococci).
• Clindamycin is available in parenteral and oral form.
Dr. Layla Borham
VI. Carbapenem Ertapenem, Imipenem and cilastatin
• Carbapenem antibiotics that has bactericidal activity
resulting from inhibition of cell wall.
• Ertapenem is indicated for community-acquired
pneumonia due to S pneumoniae (penicillin-susceptible
isolates only).
• Imipenem and cilastatin used for treatment of multiple
organism infections. Use this agent with caution in the
presence of renal insufficiency. Dr. Layla Borham

Meropenem • It is indicated for community-acquired pneumonia,
including multi–drug-resistant S pneumoniae.
• A bactericidal broad-spectrum carbapenem antibiotic
that inhibits cell wall synthesis.
• It is effective against most gram-positive and gram-
negative bacteria and has slightly increased activity
against gram-negatives and slightly decreased activity
against staphylococci and streptococci compared with
imipenem. Dr. Layla Borham

VII. Sulfamethoxazole and trimethoprim
• This agent inhibits bacterial synthesis of dihydrofolic acid by
competing with paraaminobenzoic acid, thereby inhibiting
folic acid synthesis and resulting in inhibition of bacterial
growth.
VIII. Amoxicillin and clavulanate
• Alternative agent for patients who are allergic or intolerant
to macrolides.
• Amoxicillin inhibits bacterial cell wall synthesis. The
addition of clavulanate inhibits beta-lactamase producing
bacteria. Dr. Layla Borham
Ampicillin and sulbactam
• It is a combination of beta-lactamase inhibitor with
ampicillin that is used as an alternative to amoxicillin.
Piperacillin and tazobactam
Ticracillin and clavulanate
• Antipseudomonal penicillin plus beta-lactamase
inhibitor. Good coverage against most gram-positive,
most gram-negative, and most anaerobic bacteria
• Monitor liver and kidney functions and do CBC.
Dr. Layla Borham

IX. Linezolid • Oxazolidinone antibiotic that prevents protein synthesis.
• It is used as an alternative drug in patients allergic to vancomycin
and for treatment of vancomycin-resistant enterococci. It is also
effective against MRSA and penicillin-susceptible S pneumoniae
infections.
• Linezolid is bacteriostatic against enterococci and staphylococci
and bactericidal against most strains of streptococci.
• Linezolid may increase serotonin CNS levels as a result of MAO-
A inhibition, increasing the risk of serotonin syndrome.
Dr. Layla Borham
X. Vancomycin
• It inhibits cell wall synthesis
• It has excellent gram-positive coverage, including
methicillin-resistant S aureus (MRSA).
• Use CrCl to adjust the dose in patients diagnosed with
renal impairment.
Dr. Layla Borham
XI. Doxycycline
• It inhibits protein synthesis and, thus, bacterial growth.
• A broad-spectrum, synthetically derived bacteriostatic
antibiotic in the tetracycline class.
• Doxycycline is an alternative agent for patients who
cannot tolerate macrolides or penicillins.
Dr. Layla Borham
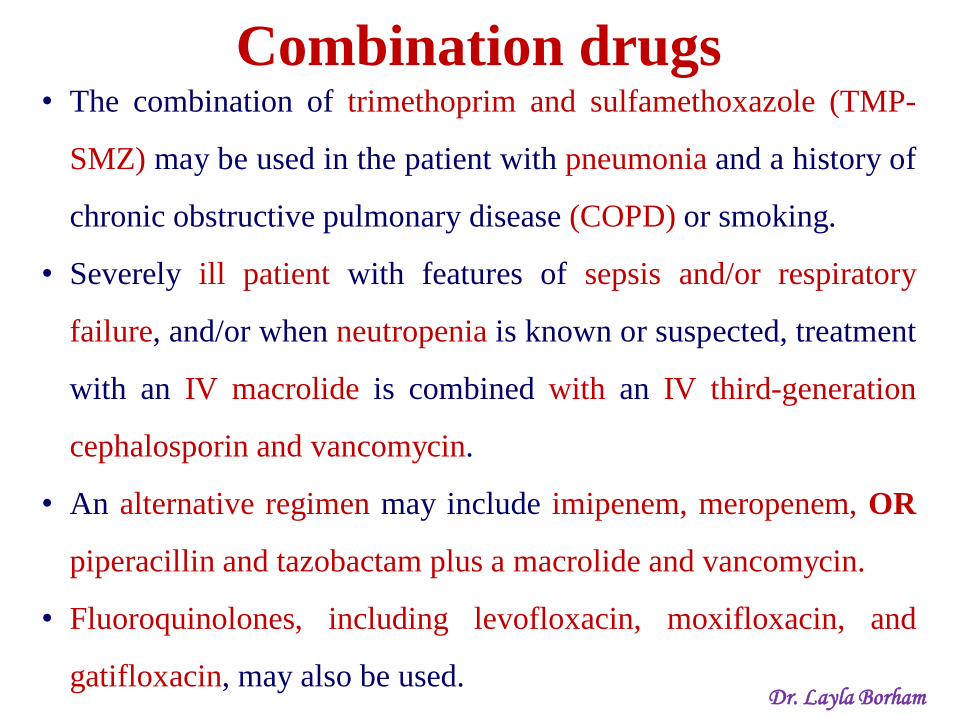
Combination drugs • The combination of trimethoprim and sulfamethoxazole (TMP-
SMZ) may be used in the patient with pneumonia and a history of
chronic obstructive pulmonary disease (COPD) or smoking.
• Severely ill patient with features of sepsis and/or respiratory
failure, and/or when neutropenia is known or suspected, treatment
with an IV macrolide is combined with an IV third-generation
cephalosporin and vancomycin.
• An alternative regimen may include imipenem, meropenem, OR
piperacillin and tazobactam plus a macrolide and vancomycin.
• Fluoroquinolones, including levofloxacin, moxifloxacin, and
gatifloxacin, may also be used. Dr. Layla Borham
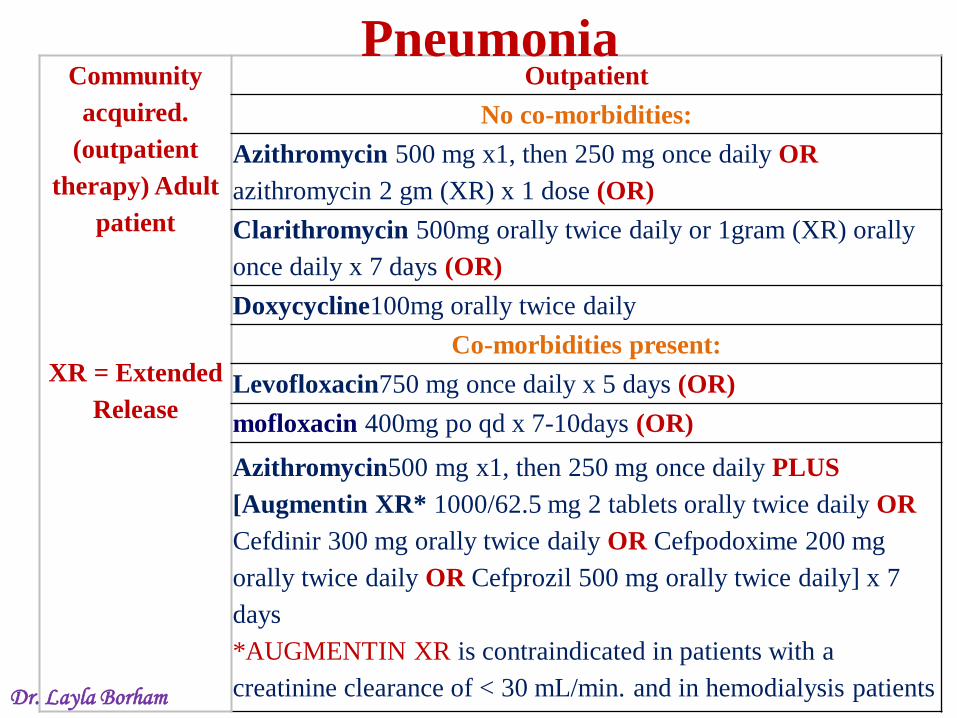
Community
acquired.
(outpatient
therapy) Adult
patient
XR = Extended
Release
Outpatient
No co-morbidities:
Azithromycin 500 mg x1, then 250 mg once daily OR
azithromycin 2 gm (XR) x 1 dose (OR)
Clarithromycin 500mg orally twice daily or 1gram (XR) orally
once daily x 7 days (OR)
Doxycycline100mg orally twice daily
Co-morbidities present:
Levofloxacin750 mg once daily x 5 days (OR)
mofloxacin 400mg po qd x 7-10days (OR)
Azithromycin500 mg x1, then 250 mg once daily PLUS
[Augmentin XR* 1000/62.5 mg 2 tablets orally twice daily OR
Cefdinir 300 mg orally twice daily OR Cefpodoxime 200 mg
orally twice daily OR Cefprozil 500 mg orally twice daily] x 7
days
*AUGMENTIN XR is contraindicated in patients with a
creatinine clearance of < 30 mL/min. and in hemodialysis patients Dr. Layla Borham
Pneumonia

Community
acquired
Pneumonia
- Adult (any
age)
Hospitalized patient:
Azithromycin 500mg IV once daily PLUS Ceftriaxone1 gram q24h
(OR)
Azithromycin500mg IV once daily PLUS Ertapenem 1 gram q24h
(OR)
Monotherapy:
Levofloxacin750 mg IV/PO once daily (OR)
Moxifloxacin 400mg IV qd.
ICU patient (CAP):
Ceftriaxone1-2 grams IV q24h OR
Ampicillin-sulbactam(Unasyn) 1.5-3.0 grams ivpb q6h] PLUS
[Azithromycin500mg IV once daily OR Levofloxacin750 mg IV/PO
once daily
(OR)
Moxifloxacin 400mg IV qd.] PLUS Vancomycin - (patient-specific
regimen - trough goal 15-20 mcg/ml) Dr. Layla Borham

Hospital-
acquired
Pneumonia
(HAP)
(nosocomial)
Multi-drug resistance unlikely
Ceftriaxone1-2 grams IV q24h OR
Ampicillin-sulbactam(Unasyn) 3.0 grams ivpb q6h OR
Levofloxacin750 mg IV/PO once daily
Multi-drug resistance LIKELY
Piperacillin-tazobactam3.375g ivpb q6h OR
Cefepime2 grams IV every 12 hours OR
Meropenem 1 gm IV q8h OR
Doripenem 500 mg IV q8h
PLUS (If MRSA suspected)
Vancomycin - (patient-specific regimen - trough goal 15-20
mcg/ml)
Dr. Layla Borham
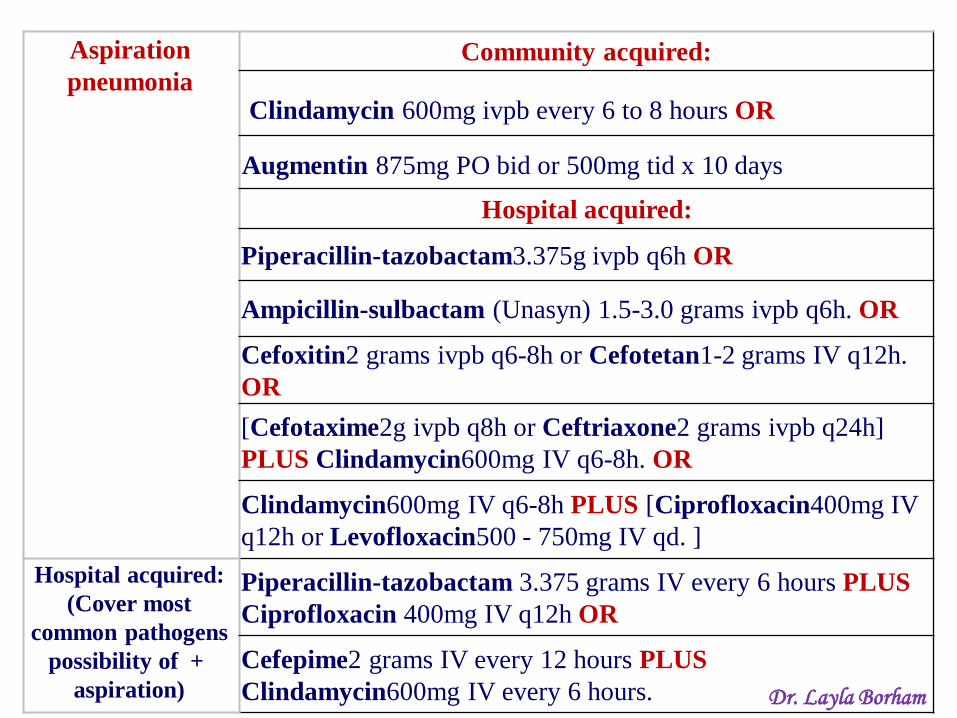
Aspiration
pneumonia
Community acquired:
Clindamycin 600mg ivpb every 6 to 8 hours OR
Augmentin 875mg PO bid or 500mg tid x 10 days
Hospital acquired:
Piperacillin-tazobactam3.375g ivpb q6h OR
Ampicillin-sulbactam (Unasyn) 1.5-3.0 grams ivpb q6h. OR
Cefoxitin2 grams ivpb q6-8h or Cefotetan1-2 grams IV q12h.
OR
[Cefotaxime2g ivpb q8h or Ceftriaxone2 grams ivpb q24h]
PLUS Clindamycin600mg IV q6-8h. OR
Clindamycin600mg IV q6-8h PLUS [Ciprofloxacin400mg IV
q12h or Levofloxacin500 - 750mg IV qd. ]
Hospital acquired:
(Cover most
common pathogens
+ possibility of
aspiration)
Piperacillin-tazobactam 3.375 grams IV every 6 hours PLUS
Ciprofloxacin 400mg IV q12h OR
Cefepime2 grams IV every 12 hours PLUS
Clindamycin600mg IV every 6 hours. Dr. Layla Borham
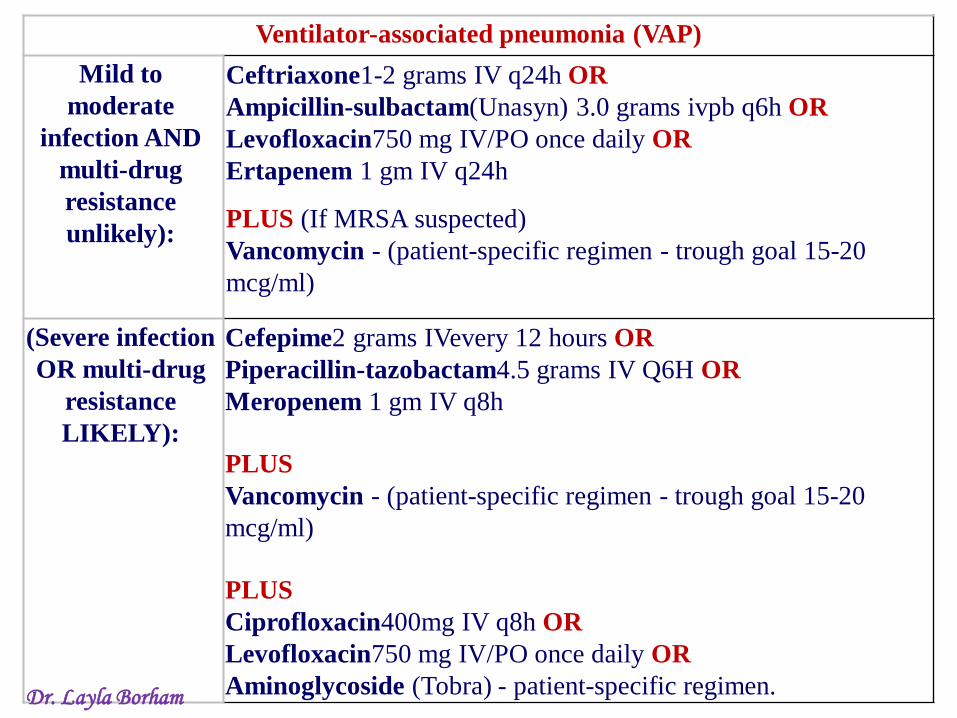
Ventilator-associated pneumonia (VAP)
Mild to
moderate
infection AND
multi-drug
resistance
unlikely):
Ceftriaxone1-2 grams IV q24h OR
Ampicillin-sulbactam(Unasyn) 3.0 grams ivpb q6h OR
Levofloxacin750 mg IV/PO once daily OR
Ertapenem 1 gm IV q24h
PLUS (If MRSA suspected)
Vancomycin - (patient-specific regimen - trough goal 15-20
mcg/ml)
(Severe infection
OR multi-drug
resistance
LIKELY):
Cefepime2 grams IVevery 12 hours OR
Piperacillin-tazobactam4.5 grams IV Q6H OR
Meropenem 1 gm IV q8h
PLUS
Vancomycin - (patient-specific regimen - trough goal 15-20
mcg/ml)
PLUS
Ciprofloxacin400mg IV q8h OR
Levofloxacin750 mg IV/PO once daily OR
Aminoglycoside (Tobra) - patient-specific regimen. Dr. Layla Borham

Pneumonia
• Duration of treatment:
1. Community acquired-mild: 7-10days.
2. Gram negative (usually nosocomial): 3 to 6
weeks.
3. Staphylococcal: 3 to 4 weeks
4. Legionella, mycoplasma, chlamydia: 14 to 21
days.
5. Lung abscess: 4 to 6 weeks.

Basic Pharmacodynamics of Antimicrobial Drugs
Mechanism of
Action Toxicity
Aminoglycosides
Protein
synthesis, Cell
membrane leak
Nephrotoxic, NMJ block,
Ototoxic, Vestibular
Cephalosporins Cell Wall
Synthesis
Hypersensitivity, Immune
reactions, Drug Fevers
Fluoroquinolones DNA Gyrase
Cartilage damage (juveniles),
Skin rash, Stevens-Johnson
syndrome
Macrolides Protein
synthesis
GI intolerance, NMJ block,
Myocardial depression,
thrombophlebitis and
cholestatic hepatitis Dr. Layla Borham
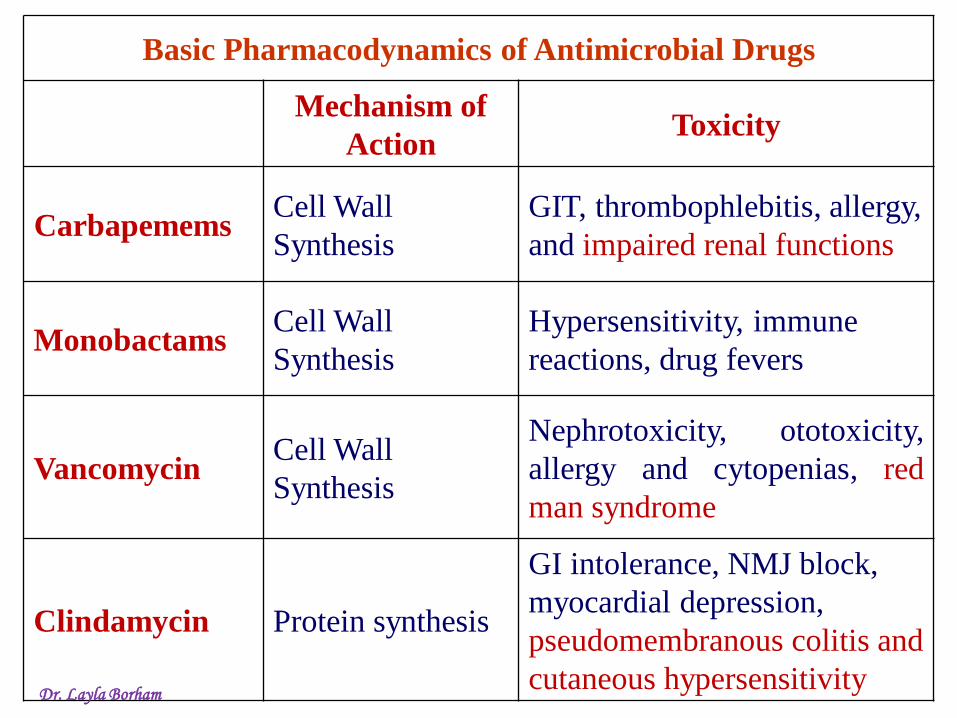
Basic Pharmacodynamics of Antimicrobial Drugs
Mechanism of
Action Toxicity
Carbapemems Cell Wall
Synthesis
GIT, thrombophlebitis, allergy,
and impaired renal functions
Monobactams Cell Wall
Synthesis
Hypersensitivity, immune
reactions, drug fevers
Vancomycin Cell Wall
Synthesis
Nephrotoxicity, ototoxicity,
allergy and cytopenias, red
man syndrome
Clindamycin Protein synthesis
GI intolerance, NMJ block,
myocardial depression,
pseudomembranous colitis and
cutaneous hypersensitivity Dr. Layla Borham

Basic Pharmacodynamics of Antimicrobial Drugs
Mechanism of
Action Toxicity
Penicillins Cell Wall Synthesis Hypersensitivity
Sulfonamides Folic Acid Synthesis
Immune, Nephrotoxic,
Hemolytic anemia,
depression anemia
Tetracyclines Protein synthesis
Nephrotoxic, GI
irritation, Hepatotoxic,
Phototoxic, Dental/Bone
(juveniles)

Infectious
Diseases Society
of America
(IDSA)
guidelines for
treatment of
patients with
community-
acquired
pneumonia.

![ﻡ 2013 ـﻫ 1435 islamic nation1427@yahoo€¦ · ﻡ 2013 - ـﻫ 1435 islamic_nation1427@yahoo.com ‹ËÜ”÷]](https://static.fdocuments.in/doc/165x107/606289f32474f209fa138569/i-2013-i-1435-islamic-nation1427yahoo-i-2013-i-1435-islamicnation1427yahoocom.jpg)