3 Biomechanical Aspects of Spinal Deformities in ... 3-AS.pdf · Ankylosing Spondylitis CHAPTER 3...
10
3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis Jwalant S. Mehta, Vijay K. Goel, and Gautam Zaveri Overview of the Normal Sagittal Spinal and Global Parameters • Cervical lordosis: C2–C7 lordosis is measured by Cobb’s method from the lower endplate of C2 to the lower endplate of C7 (Fig. 3.1a). • T1 slope: The angle subtended between the horizontal plane and a line parallel to the superior endplate of T1 (Fig. 3.1b). With increasing deformity in ankylosing spondylitis (AS), the T1 slope increases. The goal of spinal realignment procedures is reduction in the T1 slope, thereby restoring horizontal gaze. • C7 sagittal vertical axis (SVA): The distance from the posterosuperior corner of the upper S1 endplate (lumbosacral pivot point) to a vertical plumb line dropped from the center of the C7 vertebral body, measured in millimeters (Fig. 3.2). Fig. 3.1 (a) Cervical lordosis as measured from inferior endplate of C2 to superior endplate of C7 by Cobb’s method. (b) T1 slope as measured between the horizontal plane and a line parallel to the superior endplate of T1. Fig. 3.2 C7 sagittal vertical axis (SVA): Full spine erect radiograph of a 67-year-old man with a long- standing ankylosing spondylitis demonstrating an ankylosed osteopenic spinal column with a reduced lumbar lordosis, increased thoracic kyphosis, and an increased SVA. Note T1 slope = 70 degrees. b a • Chin brow vertical angle (CBVA): The angle subtended between a vertical line and a line drawn from the patients chin to the brow. It is measured on a lateral full- body radiograph or a side-profile clinical photograph with the patient standing with the hips and knees extended and the neck in a neutral position (Fig. 3.3). • Thoracic kyphosis: Cobb’s angle from the upper endplate of T4 to the lower endplate of T12 using Cobb’s method. The normal range of thoracic kyphosis is 10 to 40 degrees (Fig. 3.4a).
Transcript of 3 Biomechanical Aspects of Spinal Deformities in ... 3-AS.pdf · Ankylosing Spondylitis CHAPTER 3...
Ankylosing Spondylitis
3 Biomechanical Aspects of Spinal Deformities in Ankylosing SpondylitisJwalant S. Mehta, Vijay K. Goel, and Gautam Zaveri
Overview of the Normal Sagittal Spinal and Global Parameters
•• Cervical lordosis: C2–C7 lordosis is measured by Cobb’s method from the lower endplate of C2 to the lower endplate of C7 (Fig. 3.1a).
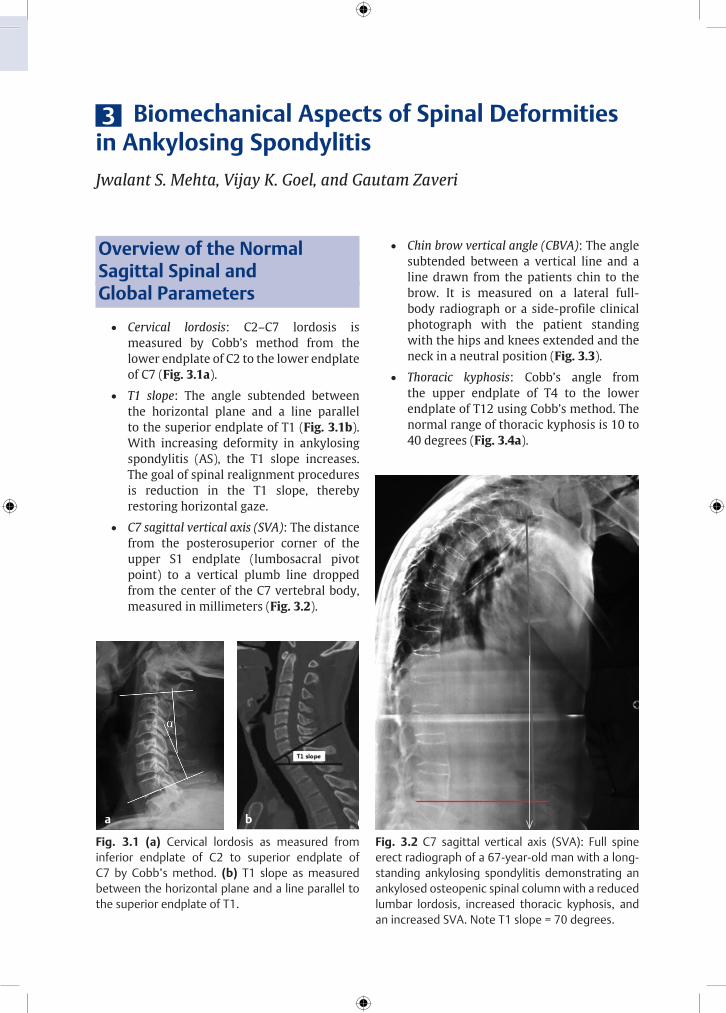
•• T1 slope: The angle subtended between the horizontal plane and a line parallel to the superior endplate of T1 (Fig. 3.1b). With increasing deformity in ankylosing spondylitis (AS), the T1 slope increases. The goal of spinal realignment procedures is reduction in the T1 slope, thereby restoring horizontal gaze.
•• C7 sagittal vertical axis (SVA): The distance from the posterosuperior corner of the upper S1 endplate (lumbosacral pivot point) to a vertical plumb line dropped from the center of the C7 vertebral body, measured in millimeters (Fig. 3.2).
Fig. 3.1 (a) Cervical lordosis as measured from inferior endplate of C2 to superior endplate of C7 by Cobb’s method. (b) T1 slope as measured between the horizontal plane and a line parallel to the superior endplate of T1.
Fig. 3.2 C7 sagittal vertical axis (SVA): Full spine erect radiograph of a 67-year-old man with a long-standing ankylosing spondylitis demonstrating an ankylosed osteopenic spinal column with a reduced lumbar lordosis, increased thoracic kyphosis, and an increased SVA. Note T1 slope = 70 degrees.
ba
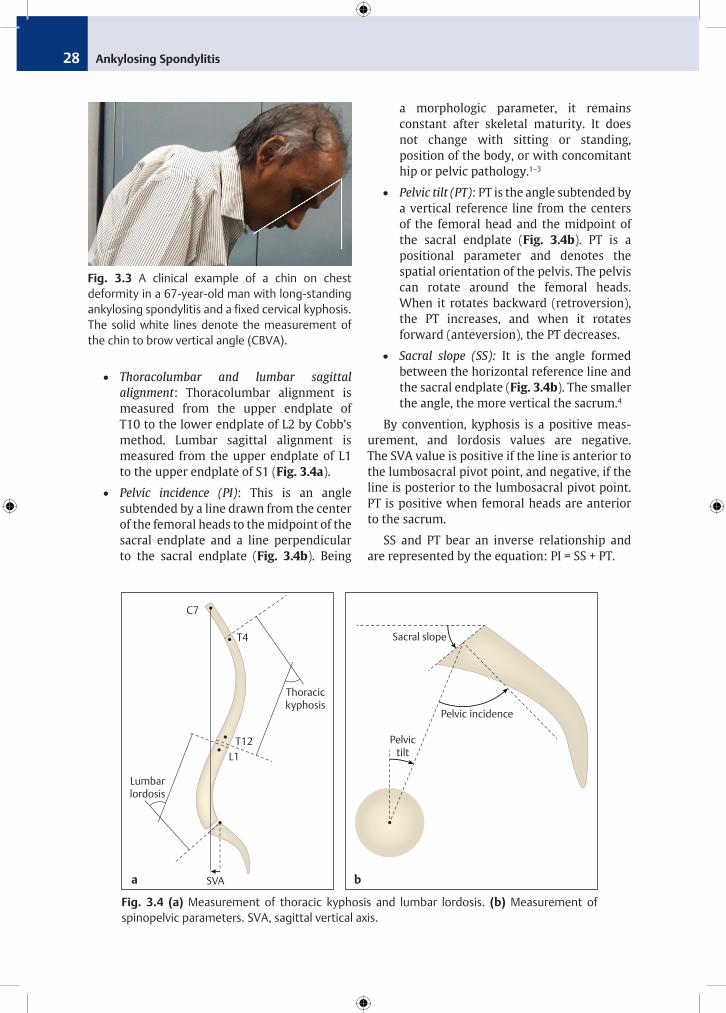
•• Chin brow vertical angle (CBVA): The angle subtended between a vertical line and a line drawn from the patients chin to the brow. It is measured on a lateral full-body radiograph or a side-profile clinical photograph with the patient standing with the hips and knees extended and the neck in a neutral position (Fig. 3.3).
•• Thoracic kyphosis: Cobb’s angle from the upper endplate of T4 to the lower endplate of T12 using Cobb’s method. The normal range of thoracic kyphosis is 10 to 40 degrees (Fig. 3.4a).
Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis28
•• Thoracolumbar and lumbar sagittal alignment: Thoracolumbar alignment is measured from the upper endplate of T10 to the lower endplate of L2 by Cobb’s method. Lumbar sagittal alignment is measured from the upper endplate of L1 to the upper endplate of S1 (Fig. 3.4a).
•• Pelvic incidence (PI): This is an angle subtended by a line drawn from the center of the femoral heads to the midpoint of the sacral endplate and a line perpendicular to the sacral endplate (Fig. 3.4b). Being
a morphologic parameter, it remains constant after skeletal maturity. It does not change with sitting or standing, position of the body, or with concomitant hip or pelvic pathology.1–3
•• Pelvic tilt (PT): PT is the angle subtended by a vertical reference line from the centers of the femoral head and the midpoint of the sacral endplate (Fig. 3.4b). PT is a positional parameter and denotes the spatial orientation of the pelvis. The pelvis can rotate around the femoral heads. When it rotates backward (retroversion), the PT increases, and when it rotates forward (anteversion), the PT decreases.
•• Sacral slope (SS): It is the angle formed between the horizontal reference line and the sacral endplate (Fig. 3.4b). The smaller the angle, the more vertical the sacrum.4
By convention, kyphosis is a positive meas-ure ment, and lordosis values are negative. The SVA value is positive if the line is anterior to the lumbo sacral pivot point, and negative, if the line is posterior to the lumbosacral pivot point. PT is positive when femoral heads are anterior to the sacrum.
SS and PT bear an inverse relationship and are represented by the equation: PI = SS + PT.
C7
T4
T12L1
Thoracickyphosis
Lumbarlordosis
SVA
Pelvic incidence
Sacral slope
Pelvictilt
Fig. 3.4 (a) Measurement of thoracic kyphosis and lumbar lordosis. (b) Measurement of spinopelvic parameters. SVA, sagittal vertical axis.
ba
Fig. 3.3 A clinical example of a chin on chest deformity in a 67-year-old man with long-standing ankylosing spondylitis and a fixed cervical kyphosis. The solid white lines denote the measurement of the chin to brow vertical angle (CBVA).
Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis 29
Pathology of Ankylosing Spondylitis
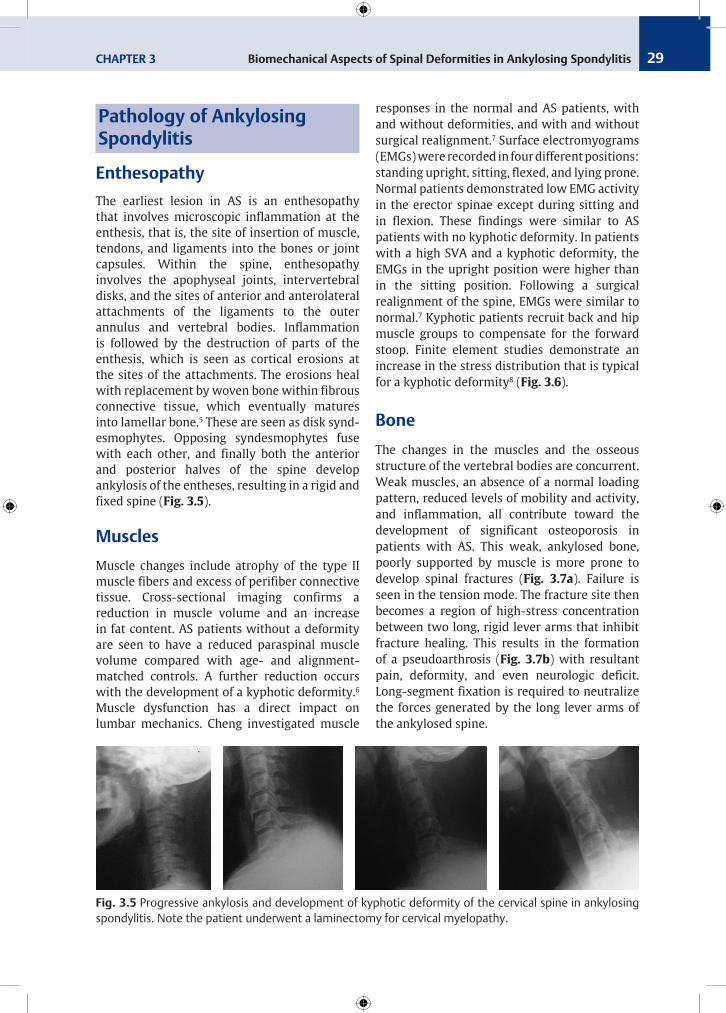
EnthesopathyThe earliest lesion in AS is an enthesopathy that involves microscopic inflammation at the enthesis, that is, the site of insertion of muscle, tendons, and ligaments into the bones or joint capsules. Within the spine, enthesopathy involves the apophyseal joints, intervertebral disks, and the sites of anterior and anterolateral attachments of the ligaments to the outer annulus and vertebral bodies. Inflammation is followed by the destruction of parts of the enthesis, which is seen as cortical erosions at the sites of the attachments. The erosions heal with replacement by woven bone within fibrous connective tissue, which eventually matures into lamellar bone.5 These are seen as disk synd-esmophytes. Opposing syndesmophytes fuse with each other, and finally both the anterior and posterior halves of the spine develop ankylosis of the entheses, resulting in a rigid and fixed spine (Fig. 3.5).
MusclesMuscle changes include atrophy of the type II muscle fibers and excess of perifiber connective tissue. Cross-sectional imaging confirms a reduction in muscle volume and an increase in fat content. AS patients without a deformity are seen to have a reduced paraspinal muscle volume compared with age- and alignment-matched controls. A further reduction occurs with the development of a kyphotic deformity.6 Muscle dysfunction has a direct impact on lumbar mechanics. Cheng investigated muscle
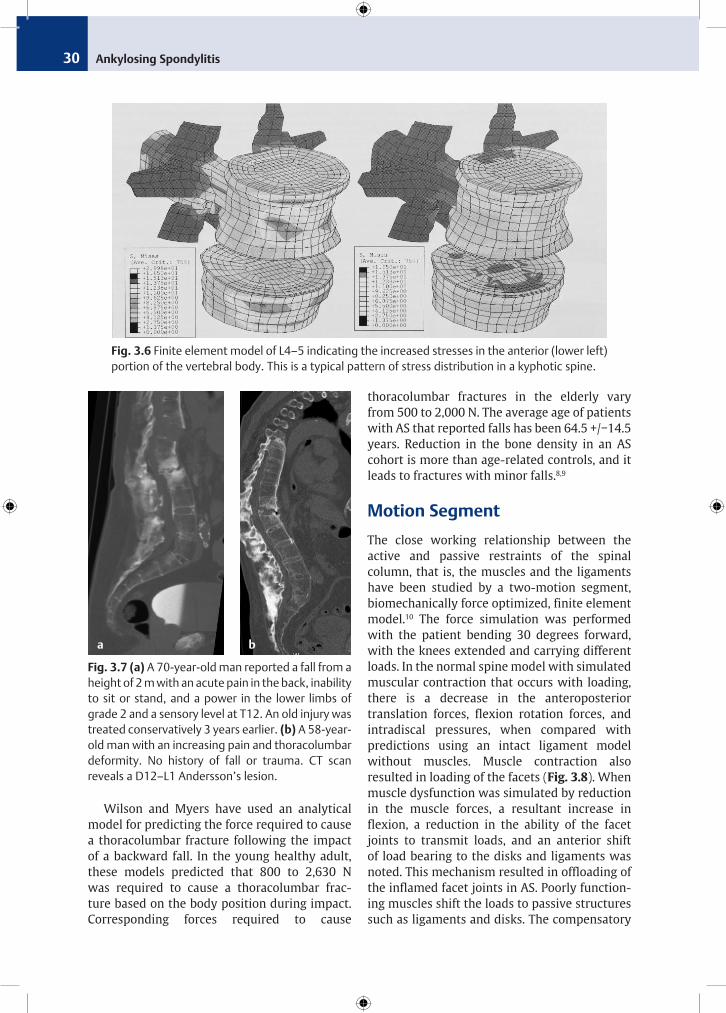
responses in the normal and AS patients, with and without deformities, and with and without surgical realignment.7 Surface electromyograms (EMGs) were recorded in four different positions: standing upright, sitting, flexed, and lying prone. Normal patients demonstrated low EMG activity in the erector spinae except during sitting and in flexion. These findings were similar to AS patients with no kyphotic deformity. In patients with a high SVA and a kyphotic deformity, the EMGs in the upright position were higher than in the sitting position. Following a surgical realignment of the spine, EMGs were similar to normal.7 Kyphotic patients recruit back and hip muscle groups to compensate for the forward stoop. Finite element studies demonstrate an increase in the stress distribution that is typical for a kyphotic deformity8 (Fig. 3.6).
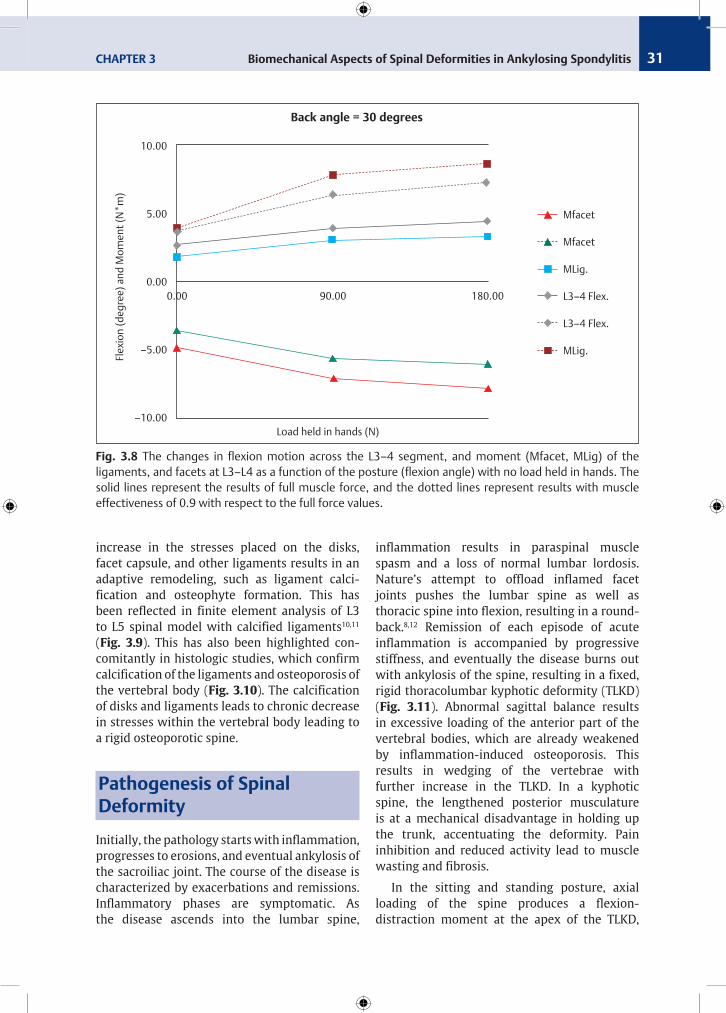
BoneThe changes in the muscles and the osseous structure of the vertebral bodies are concurrent. Weak muscles, an absence of a normal loading pattern, reduced levels of mobility and activity, and inflammation, all contribute toward the develop ment of significant osteoporosis in patients with AS. This weak, ankylosed bone, poorly supported by muscle is more prone to develop spinal fractures (Fig. 3.7a). Failure is seen in the tension mode. The fracture site then becomes a region of high-stress concentration between two long, rigid lever arms that inhibit fracture healing. This results in the formation of a pseudoarthrosis (Fig. 3.7b) with resultant pain, deformity, and even neurologic deficit. Long-segment fixation is required to neutralize the forces generated by the long lever arms of the ankylosed spine.
Fig. 3.5 Progressive ankylosis and development of kyphotic deformity of the cervical spine in ankylosing spondylitis. Note the patient underwent a laminectomy for cervical myelopathy.
Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis30
Wilson and Myers have used an analytical model for predicting the force required to cause a thoracolumbar fracture following the impact of a backward fall. In the young healthy adult, these models predicted that 800 to 2,630 N was required to cause a thoracolumbar frac-ture based on the body position during impact. Corresponding forces required to cause
thora columbar fractures in the elderly vary from 500 to 2,000 N. The average age of patients with AS that reported falls has been 64.5 +/−14.5 years. Reduction in the bone density in an AS cohort is more than age-related controls, and it leads to fractures with minor falls.8,9
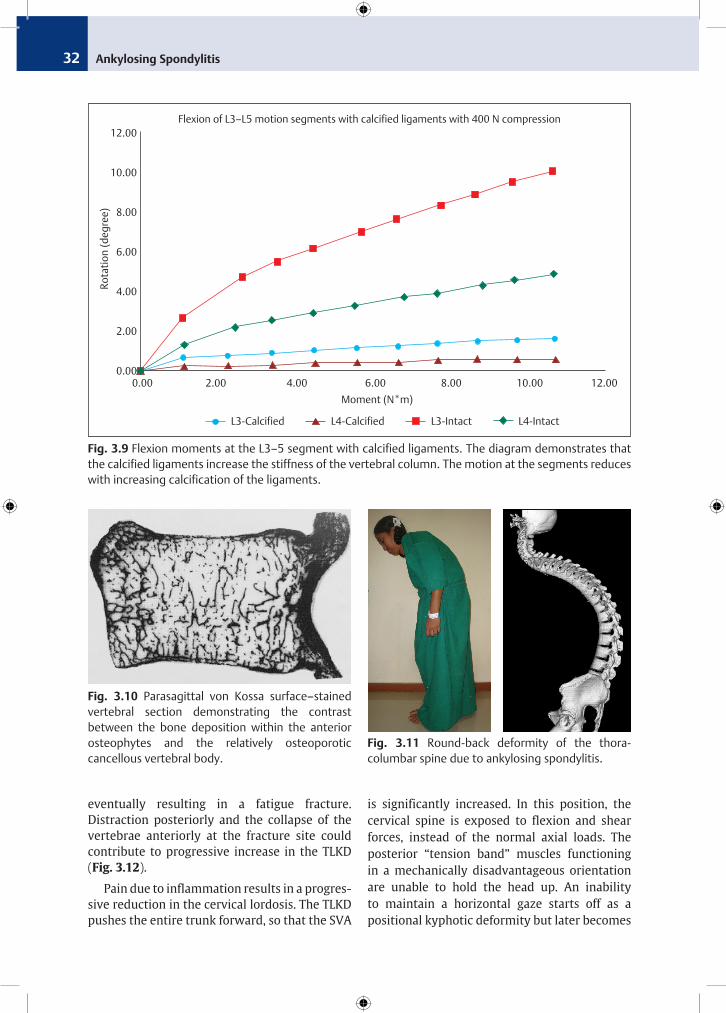
Motion SegmentThe close working relationship between the active and passive restraints of the spinal column, that is, the muscles and the ligaments have been studied by a two-motion segment, bio mechanically force optimized, finite element model.10 The force simulation was performed with the patient bending 30 degrees forward, with the knees extended and carrying different loads. In the normal spine model with simulated muscular contraction that occurs with loading, there is a decrease in the anteroposterior trans lation forces, flexion rotation forces, and intra discal pres sures, when compared with predic tions using an intact ligament model without muscles. Muscle contraction also resulted in loading of the facets (Fig. 3.8). When muscle dys function was simulated by reduction in the muscle forces, a resultant increase in flexion, a reduction in the ability of the facet joints to transmit loads, and an anterior shift of load bearing to the disks and ligaments was noted. This mechanism resulted in offloading of the inflamed facet joints in AS. Poorly function-ing muscles shift the loads to passive structures such as ligaments and disks. The compensatory
Fig. 3.6 Finite element model of L4–5 indicat ing the increased stresses in the anterior (lower left) portion of the vertebral body. This is a typical pattern of stress distribution in a kyphotic spine.
Fig. 3.7 (a) A 70-year-old man reported a fall from a height of 2 m with an acute pain in the back, inability to sit or stand, and a power in the lower limbs of grade 2 and a sensory level at T12. An old injury was treated conservatively 3 years earlier. (b) A 58-year-old man with an increasing pain and thoracolumbar deformity. No history of fall or trauma. CT scan reveals a D12–L1 Andersson’s lesion.
ba
Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis 31
Fig. 3.8 The changes in flexion motion across the L3–4 segment, and moment (Mfacet, MLig) of the ligaments, and facets at L3–L4 as a function of the posture (flexion angle) with no load held in hands. The solid lines represent the results of full muscle force, and the dotted lines represent results with muscle effectiveness of 0.9 with respect to the full force values.
Mfacet
Mfacet
MLig.
L3–4 Flex.
L3–4 Flex.
MLig.
10.00
5.00
0.00
–5.00
–10.00
Flex
ion
(deg
ree)
and
Mom
ent (
N*m
)
0.00 90.00 180.00
Load held in hands (N)
Back angle = 30 degrees
increase in the stresses placed on the disks, facet capsule, and other ligaments results in an adaptive remodeling, such as ligament calci-fication and osteophyte formation. This has been reflected in finite element analysis of L3 to L5 spinal model with calcified ligaments10,11 (Fig. 3.9). This has also been highlighted con-comitantly in histologic studies, which confirm calcification of the ligaments and osteoporosis of the vertebral body (Fig. 3.10). The calcification of disks and ligaments leads to chronic decrease in stresses within the vertebral body leading to a rigid osteoporotic spine.
Pathogenesis of Spinal Deformity
Initially, the pathology starts with inflammation, progresses to erosions, and eventual ankylosis of the sacroiliac joint. The course of the disease is characterized by exacerbations and remissions. Inflammatory phases are symptomatic. As the disease ascends into the lumbar spine,
inflam mation results in paraspinal muscle spasm and a loss of normal lumbar lordosis. Nature’s attempt to offload inflamed facet joints pushes the lumbar spine as well as thoracic spine into flexion, resulting in a round-back.8,12 Remission of each episode of acute inflammation is accompanied by pro gressive stiffness, and eventually the disease burns out with ankylosis of the spine, result ing in a fixed, rigid thoracolumbar kyp hotic deformity (TLKD) (Fig. 3.11). Abnormal sagittal balance results in excessive loading of the anterior part of the vertebral bodies, which are already weakened by inflammation-induced osteoporosis. This results in wedging of the vertebrae with further increase in the TLKD. In a kyphotic spine, the lengthened posterior musculature is at a mechanical disadvantage in holding up the trunk, accentuating the deformity. Pain inhibition and reduced activity lead to muscle wasting and fibrosis.
In the sitting and standing posture, axial loading of the spine produces a flexion- distraction moment at the apex of the TLKD,
Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis32
Fig. 3.10 Parasagittal von Kossa surface–stained vertebral section demonstrating the contrast between the bone deposition within the anterior osteophytes and the relatively osteoporotic cancellous vertebral body.
Fig. 3.11 Round-back deformity of the thora-columbar spine due to ankylosing spondylitis.
Fig. 3.9 Flexion moments at the L3–5 segment with calcified ligaments. The diagram demonstrates that the calcified ligaments increase the stiffness of the vertebral column. The motion at the segments reduces with increasing calcification of the ligaments.
Moment (N*m)
Rota
tion
(deg
ree)
12.00
10.00
8.00
6.00
4.00
2.00
0.00
L3-Calcified L4-Calcified L3-Intact L4-Intact
0.00 2.00 4.00 6.00 8.00 10.00 12.00
Flexion of L3–L5 motion segments with calcified ligaments with 400 N compression
eventually resulting in a fatigue fracture. Distraction posteriorly and the collapse of the vertebrae anteriorly at the fracture site could contribute to progressive increase in the TLKD (Fig. 3.12).
Pain due to inflammation results in a progres-sive reduction in the cervical lordosis. The TLKD pushes the entire trunk forward, so that the SVA
is significantly increased. In this position, the cervical spine is exposed to flexion and shear forces, instead of the normal axial loads. The posterior “tension band” muscles functioning in a mechanically disadvantageous orientation are unable to hold the head up. An inability to maintain a horizontal gaze starts off as a positional kyphotic deformity but later becomes

Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis 33
fixed. The endpoint of a very severe deformity of the cervical spine in AS is known as “chin on chest” deformity (see Fig. 3.3).
Compensatory Mechanisms in the Upright Position
The basis for a normal posture is the ability to maintain a forward gaze while the trunk is positioned in the “zone of economy.” Any increase in SVA takes the trunk forward and away
from this comfort zone. Sagittal malalignments cause pain, deformity, and disability. A loss of horizontal forward gaze, besides being disabling, can also affect social interactions.
Nature attempts to balance the spine in fixed TLKD and restore forward gaze by compensating above in the cervical spine or below in the pelvis and lower extremities.13,14 Because the cervical spine in AS is frequently fused, its ability to com-pensate for the TLKD is limited. Hence the pelvic and lower extremity muscles are recruited to maintain an upright position.
In the normal spine, the pelvic orientation coupled with the lumbar lordosis and hip exten-sion facilitates the upright stance with minimal expense of energy. A reduction in lumbar lordosis can be compensated by pelvic retro-version. The higher the PI, the better the adapt-ability of the pelvis to a loss of lumbar lordosis. The retroversion is a compensatory mechan-ism and can be measured radiogra phically as PT (Fig. 3.13). Once the maximum pelvic com-pensation is achieved, further compensation is possible through the lower extremities. In AS the hip movements are often impaired, leading to a loss of this modality for compensation. Flexion of the knees provides a transitory, posterior translation of the SVA in an attempt for truncal
C7
PT
HA
Cobb T1–S1 (–)
A
PT
SVA
HA
C7
B
Cobb T1–S1
PT
SVA
C
HA
C7
Cobb T1–S1
SVA
D
PT
HA
Cobb T1–S1
C7
Fig. 3.13 Loss of normal lumbar lordosis and increasing thoracic kyphosis cause progressive anterior translation of SVA. Initially the pelvic retroversion with reduction in sacral slope attempts to pull the SVA back to maintain sagittal balance. HA, Head of femur; PT, pelvic tilt; SVA, sagittal vertical axis.
Fig. 3.12 X-ray and MRI of a 67-year-old man with Andersson’s lesion.
Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis34
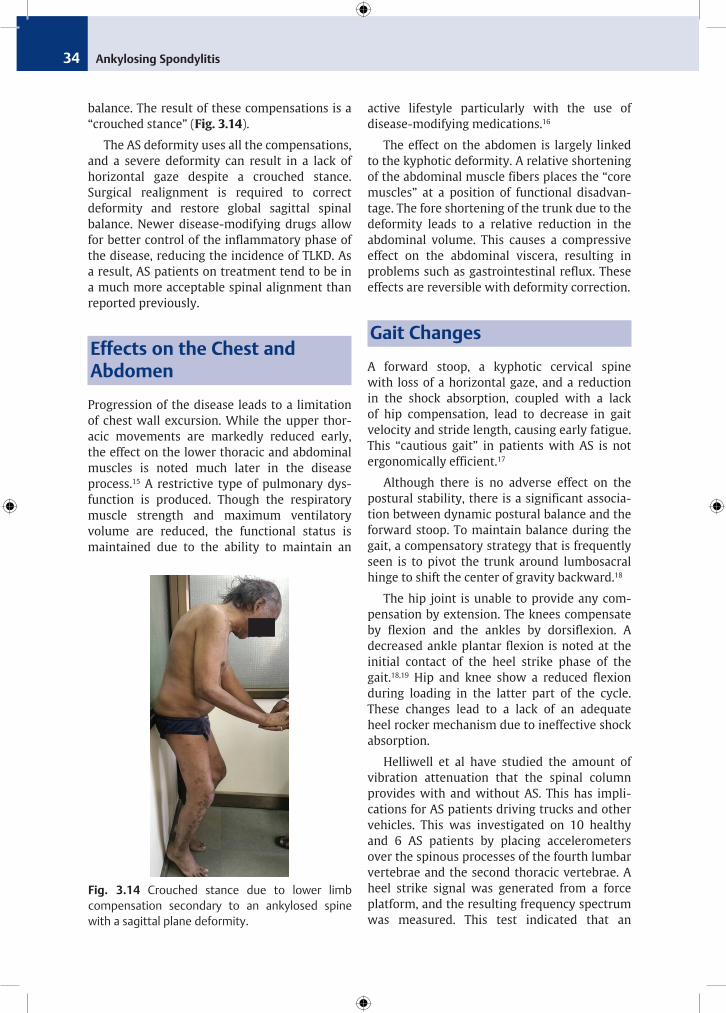
balance. The result of these compensations is a “crouched stance” (Fig. 3.14).
The AS deformity uses all the compensations, and a severe deformity can result in a lack of horizontal gaze despite a crouched stance. Surgical realignment is required to correct deformity and restore global sagittal spinal balance. Newer disease-modifying drugs allow for better control of the inflammatory phase of the disease, reducing the incidence of TLKD. As a result, AS patients on treatment tend to be in a much more acceptable spinal alignment than reported previously.
Effects on the Chest and Abdomen
Progression of the disease leads to a limitation of chest wall excursion. While the upper thor-acic movements are markedly reduced early, the effect on the lower thoracic and abdominal muscles is noted much later in the disease process.15 A restrictive type of pulmonary dys-function is pro duced. Though the respiratory muscle strength and maximum ventilatory volume are reduced, the functional status is main tained due to the ability to maintain an
active lifestyle particularly with the use of disease-modifying medications.16
The effect on the abdomen is largely linked to the kyphotic deformity. A relative shortening of the abdominal muscle fibers places the “core muscles” at a position of functional disadvan-tage. The fore shortening of the trunk due to the deformity leads to a relative reduction in the abdominal volume. This causes a compressive effect on the abdominal viscera, resulting in problems such as gastrointestinal reflux. These effects are reversible with deformity correction.
Gait Changes
A forward stoop, a kyphotic cervical spine with loss of a horizontal gaze, and a reduction in the shock absorption, coupled with a lack of hip compensation, lead to decrease in gait velocity and stride length, causing early fatigue. This “cautious gait” in patients with AS is not ergonomically efficient.17
Although there is no adverse effect on the postural stability, there is a significant associa-tion between dynamic postural balance and the forward stoop. To maintain balance during the gait, a compensatory strategy that is frequently seen is to pivot the trunk around lumbosacral hinge to shift the center of gravity backward.18
The hip joint is unable to provide any com-pensation by extension. The knees compensate by flexion and the ankles by dorsiflexion. A decreased ankle plantar flexion is noted at the initial contact of the heel strike phase of the gait.18,19 Hip and knee show a reduced flexion during loading in the latter part of the cycle. These changes lead to a lack of an adequate heel rocker mechanism due to ineffective shock absorption.
Helliwell et al have studied the amount of vibration attenuation that the spinal column provides with and without AS. This has impli-cations for AS patients driving trucks and other vehicles. This was investigated on 10 healthy and 6 AS patients by placing accelerometers over the spinous processes of the fourth lumbar vertebrae and the second thoracic vertebrae. A heel strike signal was generated from a force platform, and the resulting frequency spectrum was measured. This test indicated that an
Fig. 3.14 Crouched stance due to lower limb compensation secondary to an ankylosed spine with a sagittal plane deformity.
Ankylosing Spondylitis CHAPTER 3 Biomechanical Aspects of Spinal Deformities in Ankylosing Spondylitis 35
ankylosed spine loses its ability to attenuate the frequencies created during normal walking and running between 15 and 40 Hz.17 This may also increase the risk of spinal fracture in advanced cases of AS. Surgical correction of the truncal alignment improves the spine function, parameters of gait, and reduces the energy expenditure during ambulation.20
Effect of Surgical Realignment
The biomechanical effects of the AS deformity are not reversible, though surgical re-alignment can improve the mechanics, gait, and the effi-ciency of energy expenditure with activities of daily living. The compensatory realignment changes between segments are closely linked. Reciprocal effects are seen following surgical reconstruction. Correcting thoracic hyper-kyphosis leads to a reduction in the lordosis of the unfused lumbar segments. A lumbar osteotomy can increase the lumbar lordosis with a concomitant increase in the thoracic kyphosis. Such a change can ironically increase the SVA or produce an inefficient forward gaze, if the compensation is inadequate. Hence, the compensatory effects should be borne in mind when performing a spinal realignment.
The compensation provided by the cervical spine needs a special mention. Progression of the disease is marked by an increase in the C2–C7 SVA and the T1 slope, with a reduction in the C2–C7 lordosis and is closely linked to increased pain and a reduced QoL (quality of life). Among these, C2–C7 SVA is the most significant predictor of QoL.21 A CBVA between −10 and +10 degrees provides an optimal horizontal gaze, though at the expense of a poor downward gaze, with resultant functional difficulties.22 Therefore, a CBVA of 10 to 20 degrees (a slight under correction) achieves a better patient satisfaction.
Cervical alignment has an effect on the thoracic alignment. The T1 slope is an important intermediary parameter that helps capture the reciprocal differences. A more proximal level of the corrective osteotomy influences the CBVA, whereas a more distal level improves the sagittal alignment. Careful planning of the osteotomy would permit addressing the disability.23–25
Summary
AS is a progressive inflammatory enthesopathy that leads to the formation of bridging synd-esmophytes between the adjacent vertebrae. The fusion of the disks and facet joints, with calcification of the supporting ligaments, results in a rigid immobile spine. Patients who have a more aggressive form of the disease tend to develop a significant “round-back” kyphotic deformity. The cervical spine may also develop a significant kyphosis and a chin-on-chest deformity resulting in loss of horizontal gaze.
Compensation for the rigid deformity comes from retroversion of the pelvis, extension of the hips, flexion of the knees, and dorsiflexion at the ankles. Because the movements at the hip are often restricted, the patient attempts to translate the SVA posteriorly by flexion of the knees.
The goal of corrective osteotomies is to restore spinal balance by restoring the SVA close to normal. Realignment reduces the load on the compensatory mechanisms, so that the PT reduces, the knee flexion diminishes, and the forward vision is restored.
Key Points
•• The deformity in AS is the end result of changes involving the entheses, bones, muscles, and ligaments.
•• The classic deformity in AS is a round-back kyphosis, resulting in a positive sagittal imbalance, as measured by the SVA.
•• Compensation for the sagittal imbalance comes from retroversion of the pelvis, extension of the hips, flexion of the knees, and dorsiflexion at the ankle (crouched lower limb posture).
•• Although the cervical spine is also frequ-ently in kyphosis, a severe chin-on-chest deformity resulting in loss of horizontal vision is uncommon.
•• The paraspinal muscles develop an atrophy of the type II muscle fibers with an increase in the amount of fibrous tissue. The forward stoop puts the posterior
Ankylosing Spondylitis36
musculature at a significant mechanical disadvantage.
•• The deformity, along with the fusion of the spine and sacroiliac joints, results in a slow, energy-inefficient gait, with a short stride length and easy fatiguability.
•• The end result following the chronic inflammation is a rigid osteopenic spinal column that is prone to fractures.
•• Surgical correction of the deformity leads to improved biomechanics and an energy-efficient gait.
References 1. Le Huec JC, Aunoble S, Philippe L, Nicolas P. Pelvic
parameters: origin and significance. Eur Spine J 2011;20(Suppl 5):564–571
2. Roussouly P, Pinheiro-Franco JL. Sagittal para-meters of the spine: biomechanical approach. Eur Spine J 2011;20(Suppl 5):578–585
3. Roussouly P, Nnadi C. Sagittal plane deformity: an overview of interpretation and management. Eur Spine J 2010;19(11):1824–1836
4. Mac-Thiong JM, Roussouly P, Berthonnand E, et al. Sagittal parameters of global spinal balance: normative values from a prospective cohort of 709 asymptomatic Caucasian adults. Spine 2010;35(22):E1193–E1198
5. Ball J. Enthesopathy of rheumatoid and anky losing spondylitis. Ann Rheum Dis 1971;30(3):213–223
6. Bok DH, Kim J, Kim TH. Comparison of MRI-defined back muscles volume between patients with ankylosing spondylitis and control patients with chronic back pain: age and spinopelvic alignment matched study. Eur Spine J 2017;26(2): 528–537
7. Cheng CK, Chen PQ, Tsuang YH, Lin SW, Lee WL. Muscular activities in ankylosing spondylitic patients. A surface EMG study. I Orthop Surg ROC 1994;11:321–326
8. Kuroki H, Holekamp S, Goel V, Panjabi M, Ebraheim N, Singer K. Biomechanics of spinal deformity in inflammatory disease. In: Govender S, Leong JCY, eds. Inflammatory Diseases of the Spine. Singapore: TIG Asia Media; 2004, 01–1 to 01–20
9. Myers ER, Wilson SE. Biomechanics of osteo-porosis and vertebral fractures. Spine 1997;22 (24 Suppl):5S- 31S
10. Goel VK, Kong W, Han JS, Weinstein JN, Gilbertson LG. A combined finite element and optimization investigation of lumbar spine mechanics with and without muscles. Spine 1993;18(11):1531–1541
11. Kong WZ, Goel VK, Gilbertson LG, Weinstein
JN. Effects of muscle dysfunction on lumbar spine mechanics. A finite element study based on a two motion segments model. Spine 1996; 21(19):2197–2206, discussion 2206–2207
12. Simkin PA, Downey DJ, Kilcoyne RF. Apophyseal arthritis limits lumbar motion in patients with ankylosing spondylitis. Arthritis Rheum 1988; 31(6):798–802
13. Lazennec JY, Brusson A, Rousseau M-A. Hip-spine relations and sagittal balance clinical conse-quences. Eur Spine J 2011;20(Suppl 5):686–698
14. Shin JK, Lee JS, Goh TS, Son SM. Correlation between clinical outcome and spinopelvic para-meters in ankylosing spondylitis. Eur Spine J 2014;23(1):242–247
15. Ragnarsdottir M, Geirsson AJ, Gudbjornsson B. Rib cage motion in ankylosing spondylitis patients: a pilot study. Spine J 2008;8(3):505–509
16. Sahin G, Calikoğlu M, Ozge C, et al. Respiratory muscle strength but not BASFI score relates to diminished chest expansion in ankylosing spondylitis. Clin Rheumatol 2004;23(3):199–202
17. Helliwell PS, Smeathers JE, Wright V. Shock absorption by the spinal column in normal and in ankylosing spondylitis. Proc Inst Mech Eng 1989;203(4):187–190
18. Del Din S, Carraro E, Sawacha Z, et al. Impaired gait in ankylosing spondylitis. Med Biol Eng Comput 2011;49(7):801–809
19. Bot SD, Caspers M, Van Royen BJ, Toussaint HM, Kingma I. Biomechanical analysis of posture in patients with spinal kyphosis due to ankylosing spondylitis: a pilot study. Rheumatology (Oxford) 1999;38(5):441–443
20. Haddas R, Belanger T. Clinical gait analysis on a patient undergoing surgical correction of kyphosis from severe ankylosing spondylitis. Int J Spine Surg 2017;11(3):18
21. Lee JS, Youn MS, Shin JK, Goh TS, Kang SS. Relationship between cervical sagittal alignment and quality of life in ankylosing spondylitis. Eur Spine J 2015;24(6):1199–1203
22. Song K, Su X, Zhang Y, et al. Optimal chin-brow vertical angle for sagittal visual fields in ankylosing spondylitis kyphosis. Eur Spine J 2016;25(8):2596–2604
23. Debarge R, Demey G, Roussouly P. Radiological analysis of ankylosing spondylitis patients with severe kyphosis before and after pedicle subtrac-tion osteotomy. Eur Spine J 2010;19(1): 65–70
24. Obeid I, Boniello A, Boissiere L, et al. Cervical spine alignment following lumbar pedicle subtraction osteotomy for sagittal imbalance. Eur Spine J 2015;24(6):1191–1198
25. Lee DH, Ha JK, Chung JH, Hwang CJ, Lee CS, Cho JH. A retrospective study to reveal the effect of surgical correction of cervical kyphosis on thoraco-lumbo-pelvic sagittal alignment. Eur Spine J 2016;25(7):2286–2293