3 Assembly Functional JohnsonAbaciSullivan FINALc.ymcdn.com/sites/ Symptoms prevent me from walking...
26
10/10/17 1 Interdisciplinary Functional Restoration for Chronic Pain Peter Abaci, M.D., Mark Johnson, P.H.D., & Michael Sullivan, M.P.T. Interdisciplinary Functional Restoration for Chronic Pain Peter Abaci, M.D. Disclosures uNothing to disclose.
Transcript of 3 Assembly Functional JohnsonAbaciSullivan FINALc.ymcdn.com/sites/ Symptoms prevent me from walking...

10/10/17
1
Interdisciplinary Functional Restoration for Chronic Pain Peter Abaci, M.D., Mark Johnson, P.H.D., & Michael Sullivan, M.P.T.
Interdisciplinary Functional Restoration for Chronic Pain
Peter Abaci, M.D.
Disclosures
u Nothing to disclose.
10/10/17
2
Why are you here? u In order to carry a positive action, we must
develop here a positive vision ~Dalai Lama u You want something great for your patients u I tell you, we are here on Earth to fart
around, and don't let anybody tell you different ~Kurt Vonnegut
Entering the world of King Midas with good intentions
Why an FRP? u Turning spine
surgery lemons into lemonade
u The call of the like-minded
u Pain Pill Paradox

10/10/17
3
Physician Role in the FRP u Symptom Manager v. Healer u What hats to wear u No babysitting!
Possible Roles for the Physician u Business Owner u Manager u Content Creator u Clinical Team Leader u Medical Provider
Harlem Globetrotters
(2012, retrieved from https://www.youtube.com/watch?v=xKkxnWFq9T4)
10/10/17
4
Ingredients for Success
u Same page u Same message u Empathy u Facility u Culture
Ingredients for Success u Address Opioids u Manage Attitudes u Aftercare and follow-up u Team building u Success breeds success
5 Key Clinical Elements
u Mobility u Interaction u Independence u Validation u Love

10/10/17
5
Interdisciplinary Functional Restoration for Chronic Pain
Michael Sullivan, M.P.T.
Disclosures
u Nothing to disclose.
Learning Objectives

10/10/17
6
Interdisciplinary Pain Management: Physical Therapy
Goals: Reduce fear of movement and increase function through educating patients to better understand a chronic pain model accompanied by active treatment that emphasizes the development of transferable skills for pain management and includes home exercises and functional activities to address limitations.
California Dept of Workers Compensation Medical Treatment Utilization Schedule (MTUS) July 2009. ‘As is the case with all chronic medical conditions, chronic pain must be managed, not cured. In the medical model, responsibility resides primarily with the physician. The self-management approach places primary responsibility on the person with chronic pain. Currently, self-management strategies can significantly improve a patient’s function and quality of life, while reducing subjective experiences of pain. It is important to educate patients on this distinction, to avoid persistent and unrealistic expectations for an elusive cure, where none exists. This unrealistic curative view, often unwittingly fostered by healthcare providers or others, predictably leads to repeated failures, delayed recovery, and unnecessary disability and costs.’
(California Dept of Workers Compensation Medical Treatment Utilization Schedule (MTUS) July 2009).
Self-assessment on an 86-point scale of activities listed below including functional components required to engage in activities (grasping, lifting, carrying, pushing/pulling) and how these are impacted by pain Observation of functional components via a functional screening measure in which patients are asked to demonstrate their safe maximum ability and perceived reason for limitation: strength, pain, fear of pain in the future or endurance. Assessment, balance, ambulation, transfers, lifting floor to waist/waist to shoulder/shoulder to overhead, push/pull, grip, fine motor and gross motor skills.
ADL Assessment:

10/10/17
7
ADL Assessment
Basic ADLs u Dressing u Eating u Ambulating u Transfers u Toileting
u Hygiene
Instrumental ADLs u Shopping u Housekeeping u Food Preparation u Recreational Activities u Transportation u Travel u Social Activities
Work u Is there a job to return
to? u What is the physical
demand level of full duty work?
u Is the patient motivated to return to work?
u Are there adverse work relationships that affect return to work?
NAME DATE
Questions Concerning Activities of Daily Living (ADL)
1. How well can you perform personal self care activities including washing, dressing, using the bathroom, etc?
q I can look after myself normally without extra discomfort q I can look after myself normally but have extra discomfort q Self care activities are uncomfortable and are done slowly q I manage most of my personal self care with some help q I need a lot of help daily in most aspects of my self care q I cannot perform self care activities
2. How well can you lift and carry?
q I can lift and carry heavy objects without extra discomfort q I can lift and carry heavy objects but I get extra discomfort q I can lift and carry heavy objects q I can only lift and carry light to medium objects q I can only lift very light objects q I cannot lift or carry anything at all
3. How well can you walk (you may check more than one box)?
q There is no change from before my injury q Symptoms prevent me from walking more than 1 mile q Symptoms prevent me from walking more than 1/2 mile q Symptoms prevent me from walking more than 1/4 mile q I walk only short distances q I use a cane, crutches or walker q I am limited to use of a wheelchair
4. What is the most strenuous level of activity that you can do
for at least 2 minutes? q Very heavy activity q Heavy activity q Moderate activity q Light activity q Very light activity q Extremely light to no activity
5. How well can you climb one flight of stairs?
q No difficulty (and you can easily perform the activity) q Some difficulty (but you can still perform the activity) q A lot of difficulty (but you can still perform the activity) q Cannot climb one flight of stairs
6. How well can you sit for a period of time (even with some pain
or discomfort) before you absolutely have to stand, walk or lay down?
q I can sit without any time limitations q I can only sit between 1 hour to 2 hours at a time q I can only sit between 30 and 60 minutes at a time q I can only sit between 15 and 30 minutes at a time q I can only sit for less than 15 minutes at a time q I can not sit at all
7. How well can you stand or walk for a period of time (even with
some pain or discomfort) before you absolutely have to sit or lay down?
q I can stand/walk without any time limitations q I can only stand/walk between 1 hour to 2 hours at a time q I can only stand/walk between 30 and 60 minutes at a time q I can only stand/walk between 15 and 30 minutes at a time q I can only stand/walk for less than 15 minutes at a time q I cannot stand or walk at all
8. How well can you reach and grasp something off a shelf at chest level?
q No difficulty (and you can easily perform the activity) q Some difficulty (but you can still perform the activity) q A lot of difficulty (but you can still do the activity) q Unable (you cannot do this activity)
9. How well can you reach and grasp something off a shelf
overhead? q No difficulty (and you can easily perform the activity) q Some difficulty (but you can still perform the activity) q A lot of difficulty (but you can still do the activity) q Unable (you cannot do this activity)
10. How well can you push or pull (even with some pain or
discomfort)? q I can push or pull very heavy objects q I can push or pull heavy objects q I can push or pull light objects q I can push or pull very light objects q I can not push or pull anything
11. Do you have any difficulty with gripping, grasping, holding and
manipulating objects with your hands? q No difficulty (and you can easily perform the activity) q Some difficulty (but you can still perform the activity) q A lot of difficulty (but you can still do the activity) q Unable (you cannot do this activity)
12. Do you have any difficulty with repetitive motions such as
typing on a computer? q No difficulty (and you can easily perform the activity) q Some difficulty (but you can still perform the activity) q A lot of difficulty (but you can still do the activity) q Unable (you cannot do this activity)
13. Do you have any difficulty with forceful activities with your
arms and hands? q No difficulty (and you can easily perform the activity) q Some difficulty (but you can still perform the activity) q A lot of difficulty (but you can still do the activity) q Unable (you cannot do this activity)
14. Do you have any difficulty with kneeling, bending or
squatting? q No difficulty (and you can easily perform the activity) q Some difficulty (but you can still perform the activity) q A lot of difficulty (but you can still do the activity) q Unable (you cannot do this activity)
15. Do you have any difficulty with sleeping?
q I have no trouble sleeping because of my injury q My sleep is slightly disturbed (less than 1 hour sleepless) q My sleep is mildly disturbed (1-2 hours sleepless) q My sleep is moderately disturbed (2-3 hours sleepless) q My sleep is greatly disturbed (3-5 hours sleepless) q My sleep is completely disturbed (5-7 hours sleepless)
1. In regards to sexual function (orgasm, ejaculation, lubrication, erection) changes since and because of your injury:
q There has not been a change because of my injury q There has been a slight change because of my injury q There has been a moderate change because of my injury q There has been a major change because of my injury q No sexual functioning because of my injury
2. In regards to your pain at the moment:
q I have no pain at the moment q My pain is mild at the moment q My pain is moderate at the moment q My pain is severe at the moment q My pain is the worst imaginable at the moment
3. In regards to your pain most of the time:
25. Has there been any change in your ability to communicate (writing, typing, seeing, hearing, speaking) since and because of you injury?
No
Change Mild
Change Moderate Change
Severe Change
Writing Typing Seeing Hearing speaking
26. If 0 indicates "no pain" and 10 indicates "pain as bad as it can
be," on a scale of 0 to 10, what is your level of pain for the following questions?
q I have no pain most of the time q My pain is very mild most of the time q My pain is moderate most of the time q My pain is fairly severe most of the time q My pain is the worst imaginable most of the time
19. How much do your injury and/or pain interfere with your ability to travel?
q None q Some or a little of the time q A lot or most of the time q All of the time – I can’t travel
20. How much difficulty do you have with cooking, laundry,
housekeeping or shopping? q None q Some or a little of the time q A lot or most of the time q All of the time – I can’t do these things
21. How much do your injury and/or pain interfere with your ability
to engage in social activities? q None q Some or a little of the time q Most of the time q All of the time – I can’t engage in social activities
22. How much do your injury and/or pain interfere with your ability
to engage in recreational activities? q None q Some or a little of the time q A lot or most of the time q All of the time – I can’t engage in recreational activities
23. How much do your injury and/or pain interfere with
concentrating and thinking? q None q Some or a little of the time q A lot or most of the time q All of the time – I can’t concentrate or think very clearly
24. How much has your injury and/or pain caused emotional
distress with depression or anxiety? q None q Some or a little of the time (mild depression or anxiety) q A lot or most of the time (moderate depression or anxiety) q All of the time (severe depression or anxiety)
What was your pain level on average during the past week (circle the appropriate number)?
No Pain 0 1 2 3 4 5 6 7 8 9 10 Pain as bad as it can be
What was your pain level at its worst during the past week (circle the appropriate number)?
No Pain 0 1 2 3 4 5 6 7 8 9 10 Pain as bad as it can be

10/10/17
8
Tampa Scale of Kinesiophobia A 1- question test, the TSK uses a 68 point scale to
assess fear of movement. Scores of 37 or greater indicate fear of movement as a barrier to rehabilitation. u Originally developed to measure fear of movement
related to chronic low back pain u Validated to include other conditions u Fear-Avoidance model
Fear-avoidance and its Consequences in Chronic Musculoskeletal Pain:
A State of the Art
u Pain-related fear is associated with escape/avoidance of physical activities
u There is considerable evidence that pain-related fear not only leads to poor physical performance as measured in the laboratory, but that these effects also generalize to activities of daily life including activities at the workplace.
Vlaeyen, JWS, Linton, SJ. Pain 85 (2000) 317-332
Fear-avoidance and its Consequences in Chronic Musculoskeletal Pain:
A State of the Art (cont.)
u ‘physical performance and self reported disability levels
u The TSK appears to be sufficiently reliable and valid... with modest but significant correlations with the impact of pain on daily life activities’. (Citing Vlaeyen et.al.; 1995)
u ‘A large number of mainly cross-sectional studies have shown that pain related fear is indeed one of the most potent predictors of observable

10/10/17
9
Treatment for Chronic Pain
u Pain Science Education including how acute and chronic pain differ
u Restoring the building blocks of function u Functional activity exposure u Stress transferable skills to improve self
management
Medical Treatment Utilization Schedule (MTUS): Chronic Pain Treatment Guidelines (CA DWC 2009) Endorses the use of active treatment modalities (e.g., exercise, education, activity modification) instead of passive treatments noting this is associated with substantially better clinical outcomes. In a large case study of patients with low back pain treated by physical therapists, those adhering to guidelines for active rather than passive treatments incurred fewer treatment visits, cost less, and had less pain and less disability. The overall success rates were 64.7% among those adhering to the active treatment recommendations versus 36.5% for passive treatment. (Fritz, 2007)
Pain Science Education
Goals: u Reduce fear of movement and increase function through
educating patients to better understand a chronic pain model u Eliminate the perception of pain as a sensation and replace
this with recognition of pain as an experience u Understand that Pain ≠ Tissue Damage u Recognize movement as essential for health of the body and
mind u Create the conditions under which healing becomes possible

10/10/17
10
International Association for the Study of Pain (IASP)
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage
Acute nociceptive pain is coupled to the presence, intensity, or duration of noxious peripheral stimuli. This type of pain is crucial for survival. Chronic Pain: IASP “pain without apparent biological value that has persisted beyond the normal tissue healing time usually taken to be 3 months”.
IASP (cont.)
Normal sensory inputs cause abnormal sensing and responses to painful and other stimuli Induced by prolonged input into the dorsal horn, increases in membrane excitability (NMDA) and synaptic efficacy coupled with reduced inhibition lead to a form of neuroplasticity that creates states of facilitation and amplification. Increased action potential output is observed. Central windup: activity in the dorsal horn is uncoupled from the presence, intensity or duration of noxious peripheral stimulation. Increased release of glutamate and substance P is present.
Central Sensitization: Crucial to the Pathogenesis of Chronic Pain
10/10/17
11
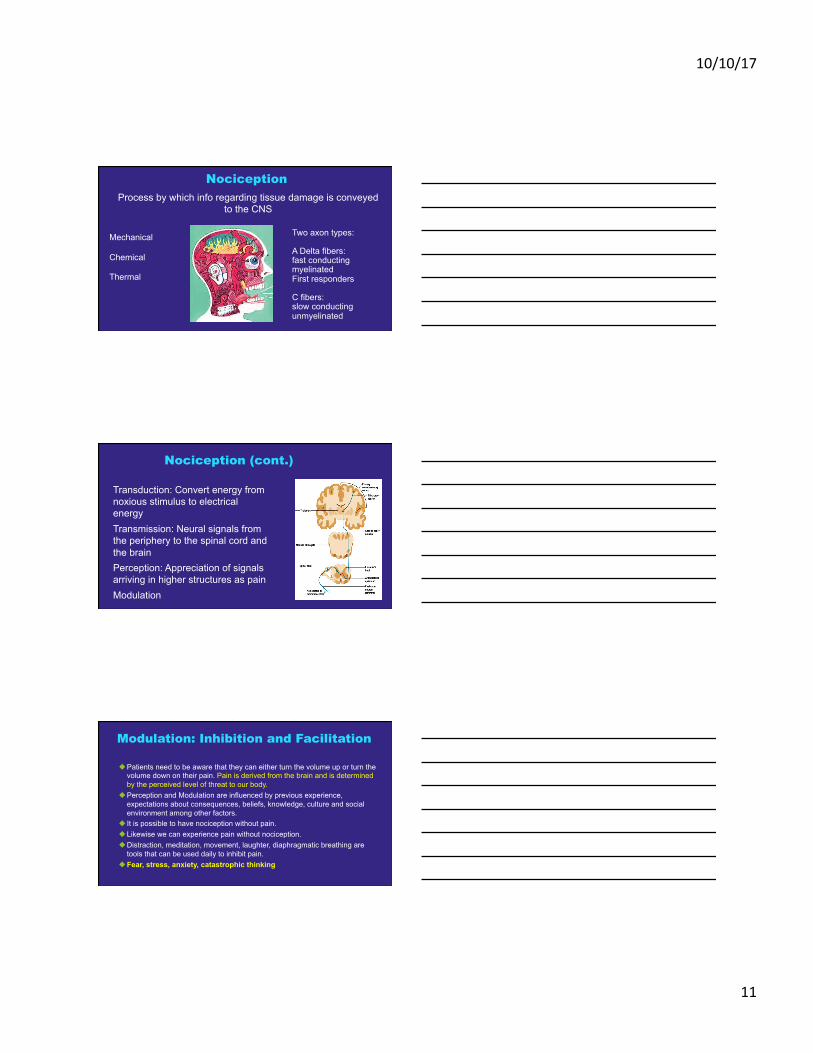
Nociception
Mechanical Chemical Thermal
Two axon types: A Delta fibers: fast conducting myelinated First responders C fibers: slow conducting unmyelinated
Process by which info regarding tissue damage is conveyed to the CNS
Transduction: Convert energy from noxious stimulus to electrical energy Transmission: Neural signals from the periphery to the spinal cord and the brain Perception: Appreciation of signals arriving in higher structures as pain Modulation
Nociception (cont.)
u Patients need to be aware that they can either turn the volume up or turn the volume down on their pain. Pain is derived from the brain and is determined by the perceived level of threat to our body.
u Perception and Modulation are influenced by previous experience, expectations about consequences, beliefs, knowledge, culture and social environment among other factors.
u It is possible to have nociception without pain. u Likewise we can experience pain without nociception. u Distraction, meditation, movement, laughter, diaphragmatic breathing are
tools that can be used daily to inhibit pain. u Fear, stress, anxiety, catastrophic thinking
u
Modulation: Inhibition and Facilitation
10/10/17
12
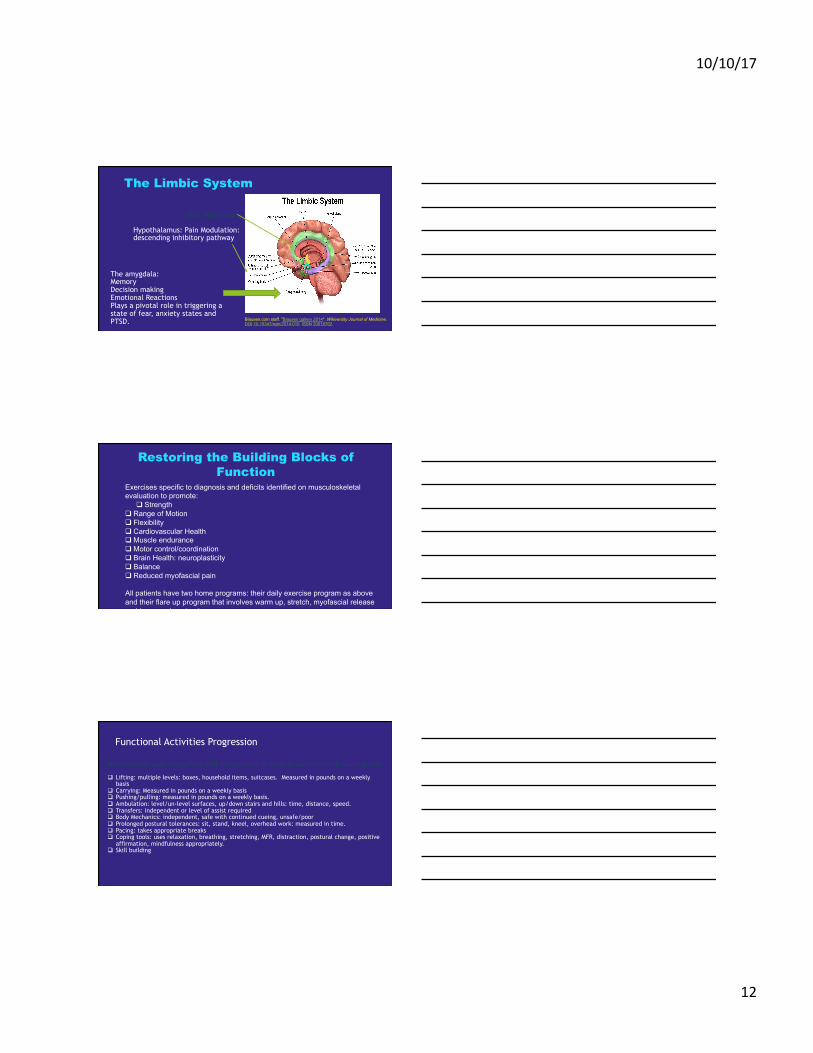
The amygdala: Memory Decision making Emotional Reactions Plays a pivotal role in triggering a state of fear, anxiety states and PTSD.
ACG: Motivation
The Limbic System
Blausen.com staff. "Blausen gallery 2014". Wikiversity Journal of Medicine. DOI:10.15347/wjm/2014.010. ISSN 20018762.
Hypothalamus: Pain Modulation: descending inhibitory pathway
Exercises specific to diagnosis and deficits identified on musculoskeletal evaluation to promote:
q Strength q Range of Motion q Flexibility q Cardiovascular Health q Muscle endurance q Motor control/coordination q Brain Health: neuroplasticity q Balance q Reduced myofascial pain
All patients have two home programs: their daily exercise program as above and their flare up program that involves warm up, stretch, myofascial release and increased postural awareness
Restoring the Building Blocks of Function
Functional Activities Progression
Patient specific goals ranging from BADL independence to return to work with a high work capacity. q Lifting: multiple levels: boxes, household items, suitcases. Measured in pounds on a weekly
basis q Carrying: Measured in pounds on a weekly basis q Pushing/pulling: measured in pounds on a weekly basis. q Ambulation: level/un-level surfaces, up/down stairs and hills: time, distance, speed. q Transfers: independent or level of assist required q Body Mechanics: independent, safe with continued cueing, unsafe/poor q Prolonged postural tolerances: sit, stand, kneel, overhead work: measured in time. q Pacing: takes appropriate breaks q Coping tools: uses relaxation, breathing, stretching, MFR, distraction, postural change, positive
affirmation, mindfulness appropriately. q Skill building

10/10/17
13
Pain is a biopsychosocial phenomena and needs to be treated as such
Dr. Melzack: The Neuromatrix
• Sensory: Intensity, location, quality, duration
• Emotional: Unpleasantness
• Cognitive: Appraisal, distraction, power of thoughts
Time to Update our Definition of Pain?
Pain is an unpleasant sensory, emotional and cognitive experience associated with actual or potential tissue damage, or described in terms of such damage.
Interdisciplinary Functional Restoration for Chronic Pain
Mark Johnson, Ph.D.
10/10/17
14
Disclosures
u Nothing to disclose.
u Most effective treatment: Integrated interdisciplinary pain rehabilitation program
u Emphasis is placed on educating patients in active self-management techniques that stress maximizing function and integrating treatment modalities
u Compared to other approaches, “CPPs offer the most efficacious and cost-effective, evidence-based treatment for persons with chronic pain”
u This model of treatment outperformed other approaches based on a number of parameters including pain levels, function, health care utilization, cost-effectiveness, medication use, and return to work rates.
Goals of Interdisciplinary Treatment
u Decrease pain intensity u Decrease reliance on pain meds u Reduce use of health care services / Increase self-
management of pain u Increase physical activity and activities of daily living u Improve psychosocial functioning u Return to work, school, and previous leisure pursuits/
interests
(Stanos & Houle, 2006; Sanders, Harden & Vicente, 2005)
10/10/17
15
Effectiveness of Interdisciplinary Programs on Psychological Measures
Improvements in: u Health-related quality of life u Pain intensity and pain interference u Pain behaviors u Depression u Anxiety
(Hoffman, Chatkoff, Papas & Kerns, 2007), (Dysvik, Kvaloy, Stokkeland & Natvig, 2010; Stanos & Houle, 2006)
Our Psychological Assessment Measures
u Patient Health Questionnaire u PHQ-9 (Depression) u GAD-7 (Anxiety)
u Brief Pain Inventory u Intensity u Interference
u Chronic Pain Coping Inventory (CPCI) u Wellness-Focused vs. Illness-Focused Coping Behaviors
Psychosocial Evaluation
u Reason for Referral u Psychosocial History and Current
Functioning u Pre-morbid versus post-injury functioning
u Substance Use History and Current Functioning
u Mental Health History and Current Functioning

10/10/17
16
Psychosocial Evaluation (cont).
u Mental Status Examination u Psychological Testing Results u Summary and Recommendations
u Appropriateness and Initial Treatment Goals u Includes Provider Recommendations and Patient’s
Goals u Personal functional goal achievement = greatest
satisfaction (Hazard, et al., 2012)
Psychosocial Assessment
Emotional state relates to pain intensity u General Anxiety can increase pain
u Pain-related anxiety/fear is more predictive of disability
u Depression can lead to increased disability (cause/effect?) u Anger and hostility play a role in outcomes u Pain and suffering u Overt pain behaviors; Secondary gain
Psychosocial Assessment (cont.)
u Active coping strategies u Social support (can buffer the effects of daily
pain on mood) u Cognitive aspects: Catastrophizing, perceived
control, self-efficacy u Personal functional goal achievement =
greatest satisfaction (Hazard, et al., 2012) u (Eccleston, 2001)

10/10/17
17
Functional Restoration Program (FRP) Daily Schedule
Monday Tuesday Wednesday Thursday Friday*
9:00-10:00 Functional Functional Functional Functional Functional
10:00 - 10:50 Mindfulness Lecture PT Special Lecture MD Lecture Nutrition Psychology Lecture
10:50 - 11:00 Break Break Break Break Break
11:00 - 12:00 Gym Gym Gym Gym Gym
12:00 - 1:00 Lunch Lunch Lunch Lunch Wellness
1:00 - 2:00 Wellness Wellness Wellness Wellness Lunch
2:00 - 2:50 Psychology Psychology Psychology Psychology Psychology
2:50 - 3:00 Break Break Break Break Break
3:00 - 4:00 Affective Expression Affective Expression Affective Expression Affective Expression Graduation
Functional Restoration Program (FRP) Weekly Schedule
Education As The Cornerstone Of Treating Chronic Pain u Week 1: Acute vs. Chronic Pain u Week 2: Chronic Pain and Mood u Week 3: Cognitive Processes and Pain u Week 4: Interpersonal Functioning and Pain u Week 5: Stress and Pain u Week 6: Preventing and Managing Pain Flare-ups
Acute versus Chronic Pain (Week 1)
u Acute vs. Chronic Pain Model u Distinguishing between hurt and harm
u Fear Avoidance (Kinesiophobia) u Biomedical vs. Biopsychosocial Model
u Gate Control Theory (Melzack & Casey, 1968; u Melzack & Wall, 1965) u Neuromatrix Model (Melzack, 1999)
u Medical vs. Self-Management Model u Passive vs. Active Strategies
(Neraz, 2012, retrieved from https://sensethesenses.wordpress.com/2012/10/16/gate-control-theory/)
Gate Control Theory of Pain
(MTUS. Medical Treatment Utilization Schedule: Chronic Pain Medical Treatment Guidelines, 2009; Eccleston, 2001)
10/10/17
18
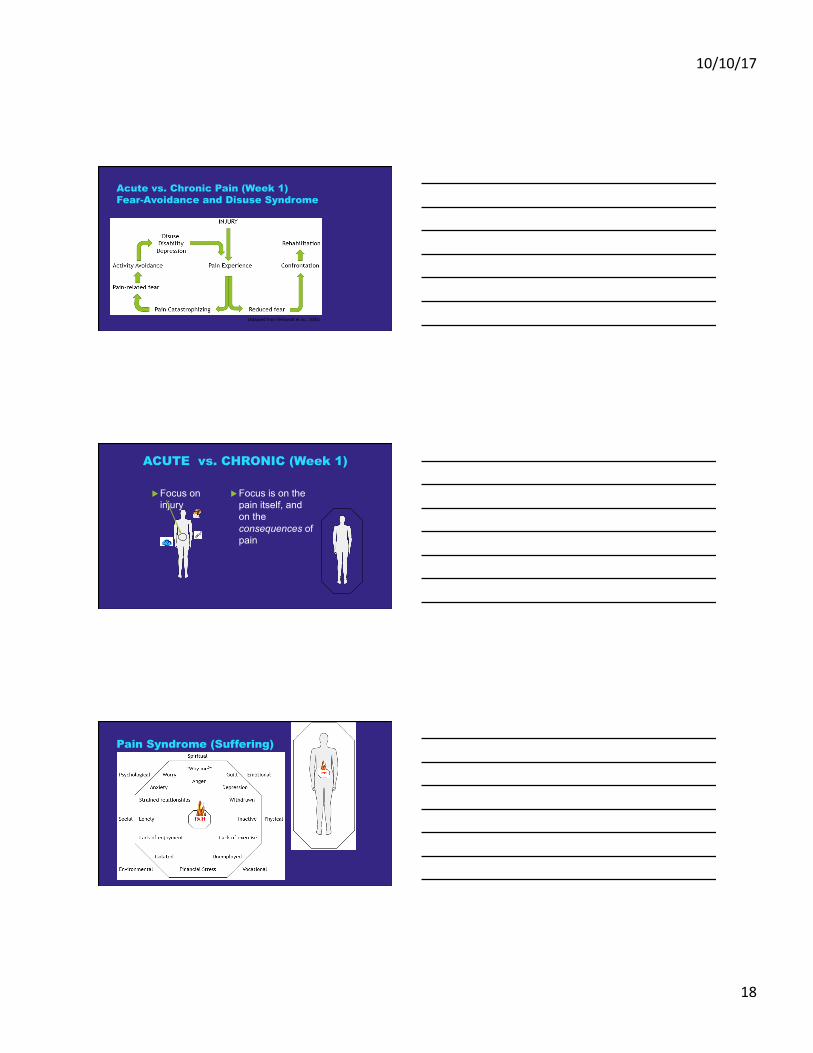
Acute vs. Chronic Pain (Week 1) Fear-Avoidance and Disuse Syndrome
(Adapted from Verbundt et al., 2003)
ACUTE vs. CHRONIC (Week 1)
u Focus on injury
u Focus is on the pain itself, and on the consequences of pain
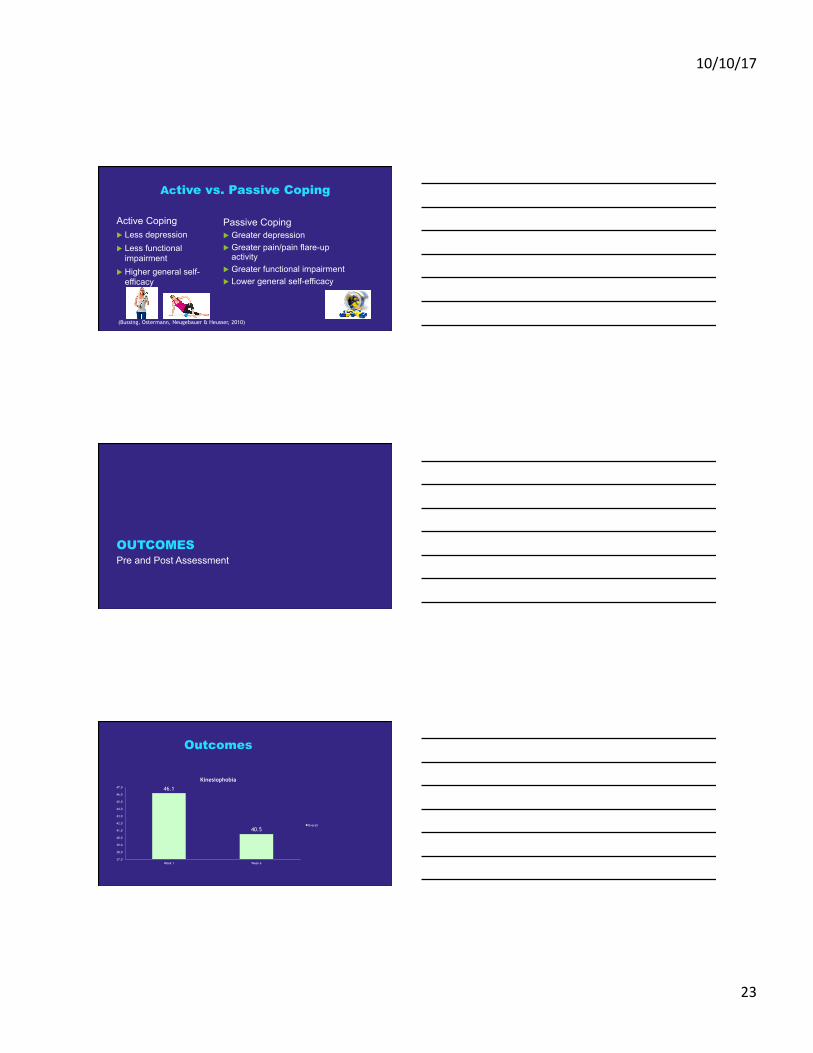
Pain Syndrome (Suffering)

10/10/17
19
Pain Syndrome Alleviated (Week 1)
Chronic Pain and Mood (Week 2)
Grief and Loss u Death u Divorce/break-up u Loss of job u Loss of Finances u Loss of youth u Loss of Health u Opportunities u Loss of dreams u Loss of identity u Loss of role
u Loss of safety, trust u Loss of functioning (i.e. –
Amputation) u Terminal Illness Diagnosis u Vision/Hearing Loss u Major Move (Loss of space) u Retirement u Miscarriage
(Furnes & Dysvik, 2010)
Managing Anger
Anger
Primary Emotions: Hurt Sad Scared Lonely Frustrated Disrespected
Unmet Emotional Needs: e.g.- Safety, Control, Companionship
Good Actions Bad Actions e.g. – Assertive Communication e.g. - Push people away (aggression)
Chronic Pain and Mood (Week 2)
10/10/17
20
Chronic Pain and Mood (Week 2) u Anger –
Suppression may aggravate pain (Burns et al., 2008) u Depression – u CBT/Behavioral Activation (Adapted for Chronic Pain)(Kim,
Crouch & Olatunji, 2017) u Anxiety –
Repression may interfere with FRP process and outcomes (Burns, 2000)
u Sleep – u (Insomnia secondary to chronic pain) CBT/Behavioral Sleep
Medicine (Currie & Wilson, 2000) (Eccleston, 2001)
Cognitive Processes and Pain (Week 3)
u Cognitive Behavioral Therapy (CBT) u To address maladaptive thoughts and beliefs about pain the pain experience to change behaviors
related to it (Mathews & Davin, 2014)
u Examples: Catastrophizing (greater pain; worse adjustment) u All-or-none thinking (Psychic Prison)
u Acceptance – Cure-focused to coping-focused (predicts greater adjustment to pain and less disability) (McCracken, 1998)
u Reappraisal (meaning, values, change of life course) u Changing Locus of Control
u Maladaptive vs. Adaptive Coping / Passive vs. Active
(Coughlin, Badura, Fleischer & Guck, 2000; Bussing, Ostermann, Neugebauer & Heusser, 2010)
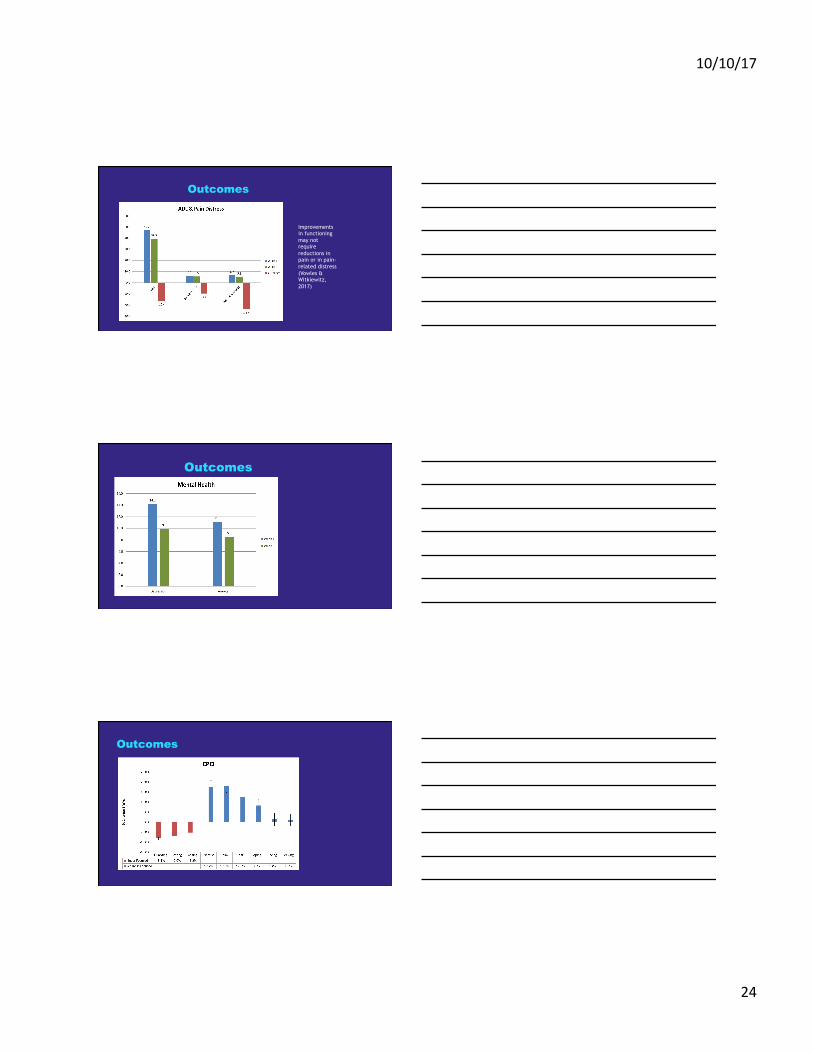
Cognitive Processes and Pain (Week 3)
Func
tion
Time
Acute Injury Normal Healing
Downward shift to chronic
Adaptive Healing

10/10/17
21
Social, Relational, Communication & Pain (Week 4)
u Illness Behavior Model, including secondary gain factors u Family (Rewarding pain behaviors,
overprotecting) u Sick Role u Verbal vs. Non-Verbal Communication u Effective Communication
u Passive / Aggressive / Passive-Aggressive – Assertive
(Retrieved from http://www.quickmeme.com/meme/3scxx1)
(Mathews & Davin, 2014)
Stress and Pain (Week 5) u Stress Management
u Includes education on CNS / Stress Response
u Maladaptive vs. Adaptive Coping u Relaxation Training
u PMR, Guided Imagery, Diaphragmatic Breathing, Biofeedback
u Address any PTSD issues (Sanders, Harden & Vicente, 2005) u Change Locus of Control (external to
internal) (Coughlin, Badura, Fleischer & Guck, 2000)
An Example of Maladaptive (Passive) Coping: “Now,
don’t talk about it, repress it, and deny it…”
(Lopez, 2016, retrieved from http://www.dailymotion.com/video/x50lqyl)

10/10/17
22
Preventing and Managing Pain Flare-ups
u Pain beliefs (i.e. – perceived activity as trigger) u Avoidance of activity as pathway in which flare-ups relate to disability
(Suri, Saunders & Von Korff, 2012) u Disuse vs. Exercise u Pacing, Time-based pacing, Activity-rest cycling u Proper body mechanics, healthy posture and ergonomics
u (Eccleston, 2011)
Flare-Up Prevention and Management
Systematic review: u Fear Avoidance + Passive Coping =
Independently predicts Greater Disability (Suri, Saunders & Von Korff, 2012;
Chou & Schekelle (2010)
Active vs. Passive Coping
Active Coping u Problem-solving u Information gathering u Refocusing/reappraisal u Self-regulation
Passive Coping u Reliance on others u Avoidance/Escape u Helplessness
(Bussing, Ostermann, Neugebauer & Heusser, 2010; Snow-Turek, Norris & Tan, 1995)
10/10/17
23
Active vs. Passive Coping
Active Coping u Less depression u Less functional
impairment u Higher general self-
efficacy
Passive Coping u Greater depression u Greater pain/pain flare-up
activity u Greater functional impairment u Lower general self-efficacy
(Bussing, Ostermann, Neugebauer & Heusser, 2010)
OUTCOMES Pre and Post Assessment
Outcomes
46.1
40.5
37.0
38.0
39.0
40.0
41.0
42.0
43.0
44.0
45.0
46.0
47.0
Week 1 Week 6
Kinesiophobia
Overall
10/10/17
24
Outcomes
Improvements in functioning may not require reductions in pain or in pain-related distress (Vowles & Witkiewitz, 2017)
Outcomes
Outcomes

10/10/17
25
Outcomes Effect Sizes
References u Burns, J. W. (2000). Repression predicts outcome following multidisciplinary treatment of chronic pain,
Health Psychology, 19(1), 75-84 u Burns, J. W., Quartana, P., Gilliam, W., Gray, E., Matsuura, J., Nappi, C. Wolf, B. & Lofland, K. (2008), 27(5),
645-652 u Bussing, Ostermann, Neugebauer & Heusser,Snow-Turek, Norris & Tan, (2010) JAMA, 303 (13),
1295-1302 u Coughlin, A.M., Badura, A.S., Fleischer, T.D. & Guck (2000) Multidisciplinary treatment of chronic pain
patients: its efficacy in changing patient locus of control, Archives of Physical Medicine Rehabilitation, 81 (6), 739-740
u Curry, S. R. & Wilson, K. G. (2000). Cognitive-behavioral treatment of insomnia secondary to chronic pain, Journal of Consulting and Clinical Psychology, 68(3), 407-416
u Dysvik, E., Kvaloy, J.T, Stokkeland, R & Natvig, G.K (2010) The effectiveness of a multidisciplinary pain management programme managing chronic pain on pain perceptions, health-related quality of life and stages of change--A non-randomized controlled study
u Eccleston, C. (2001). Role of psychology in pain management, British Journal of Anaesthesia, 87(1), 144-152 u Fleischer u Furnes & Dysvik (2010). Dealing with grief related to loss by death and chronic pain: an integrated theoretical
framework. Part 1. Patient Prefer Adherence, 4, 135-140.
References
u Gatchel, R. J. & Okifugi, A. (2006) Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain, Journal of Pain, 7, 11, 779-793
u Hazard RG, Spratt KF, McDonough CM, Carayannopoulos AG, Olson CM, Reeves V, Sperry ML, Ossen ES.
u Hoffman, Chatkoff, Papas & Kerns, (2007) Meta-analysis of psychological interventions for chronic low back pain, Health Psychology, 26 (1), 1-9
u Kim, E. H., Crouch, T. B. & Olatunji, B. O. (2017), Adaptation of behavioral activation in the treatment of chronic pain, Psychotherapy, 1-8
u Mathews & Davin, (2014) Chronic Pain Rehabilitation, Neurosurgery Clinics of North America, 25, (4), 799-802
u McCracken, L. M. (1998) Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain. Pain, 74 (1), 21-27
u MTUS. Medical Treatment Utilization Schedule: Chronic Pain Medical Treatment Guidelines, 2009 u Neubauer
10/10/17
26
References
u Sanders, S. H., Harden, R. N. and Vicente, P. J. (2005), Evidence-Based Clinical Practice Guidelines for Interdisciplinary Rehabilitation of Chronic Nonmalignant Pain Syndrome Patients. Pain Practice, 5: 303–315. doi:10.1111/j.1533-2500.2005.00033.x
u Stanos & Houle, Multidisciplinary and interdisciplinary management of chronic pain, Physical Medicine and Rehabilitation Clinics of North America, 17 (2), 435-50
u Suri, P., Saunders, K. W. & Von Korff, M. (2012) Prevalence and characteristics of flare-ups of chronic nonspecific back pain in primary care: a telephone survey, Clinical Journal of Pain, 28(7), 573-580