
2nd CUTEHeart Workshop Constantine Gatsosis Presentation
70
The link of diagnostic tests and patient outcomes: methodologic challenges April 2016 CUTEheart Workshop Constantine Gatsonis Department of Biostatistics and Center for Statistical Sciences Brown University School of Public Health
Transcript of 2nd CUTEHeart Workshop Constantine Gatsosis Presentation

The link of diagnostic tests and patient outcomes: methodologic challenges
April 2016 CUTEheart Workshop
Constantine GatsonisDepartment of Biostatistics and Center for Statistical SciencesBrown University School of Public Health

Outline 1. The problem: Broadly shared concern about the
effectiveness of modalities for diagnosis and prediction
2. The solutions, classical and new:
a. Randomized studies
b. Observational studies:
– Large databases: EMR, Health Insurance Claims
– Large registries: The National Oncology PET Registry studies
– Combining registries with administrative and insurance databases
3. Evaluation of effectiveness of diagnostics revisited
April 2016 CUTEheart Workshop

April 2016 CUTEheart Workshop
Diagnostic testing is receiving much attention and skepticism
1 ‐ Specificity
0.0 0.2 0.4 0.6 0.8 1.0
0.0
0.2
0.4
0.6
0.8
1.0
Sensitivity

April 2016 CUTEheart Workshop
CMS to Trim Spending on Diagnostic Lab TestsThe Centers for Medicare and Medicaid Services appear to be executing a two‐step strategy to shrink the $8 billion annual price tag of clinical diagnostic laboratory tests.On Sept. 25, CMS released a final payment determination for the Clinical Laboratory Fee Schedule that cuts payment by over 90 percent for some tests
October 2, 2015
The Health Care Value Transparency Movement and Its Implications for Radiology Daniel J. Durand, MD et al, JACR 2015 ….radiology, along with other “ancillary services,” has been a major focus of early efforts to enhance consumer price transparency. By contrast, radiology as a field remains in the “middle of the pack” with regard to quality transparency.
Addressing Overutilization in Medical Imaging Hendee et al, Radiology 2010Key forces influencing overutilization .. include payment mechanisms and financial incentives; the practice behavior of referring physicians; self‐referral, including referral for additional radiologic examinations; defensive medicine; missed educational opportunities when inappropriate procedures are requested; patient expectations; and duplicate imaging studies.

Tests and therapeutic interventions
Fundamentally tests provide information for use in selecting course of care. Both long‐ and short‐term effects of tests materialize in context of available health care options, including therapeutic interventions.Not possible to define and measure test effects outside the particular health care context in which the test will be used. However, oftentimes diagnosis may be ahead of therapy: e.g. DCIS in breast cancer, Amyloid plaque testing in Alzheimer’s
April 2016 CUTEheart Workshop

Main questions in test evaluation
April 2016 CUTEheart Workshop
Accurate? • Accuracy in detection• Accuracy in prediction
Affects Care ?
Affects Outcome?
Process of care:• Dx thinking/decision making• Tx thinking/decision making
Patient outcomes:• Quality of life, satisfaction, cost• Mortality, morbidity

The challenge for diagnosis and prediction
Dx informationOutcomes
How can we illuminate the complex path
The main pathway goes through therapyApril 2016 CUTEheart Workshop
THERAPY

CUTEheart WorkshopApril 2016
A heuristic argumenthighlighting key constraints

R
Test A
Test B
Tx1
Tx1
Tx2
Tx2
Outcome
Outcome
Outcome
Outcome
+
+
‐
‐
Simple randomized design, comparing two tests
April 2016 CUTEheart Workshop

Difference in success rates between two arms:D=(r1-r2)xpx(SensA – SensB)
r1 and r2 = success rates for therapeutic interventions Tx1 and Tx2, when performed on cases that have the clinical condition (irrespectively of which test detected them).
p = prevalence of the clinical conditionSens= test sensitivity (Specificities are assumed equal above).
Typically, overall effect D between arms will be much smaller than difference in efficacies of therapies r1-r2
If r1-r2 = 0 (therapy not effective) or SensA = SensBthen overall effect of test D=0. April 2016 CUTEheart Workshop
Key observations:

R
CT, 3 annual screens
WorkupTherapy
No further intervention
Lung Ca. Mortality+
+
‐
‐
Example: Lung Cancer Screening Trial
CUTEheart WorkshopApril 2016
X‐ray , 3 annual screens No further
intervention
Lung Ca. Mortality
Lung Ca. Mortality
Lung Ca. Mortality
N=53546

April 2016 CUTEheart Workshop

A randomized study of strategies formanaging stable angina patients
CUTEheart Workshop
http://www.acrin.org/PROTOCOLSUMMARYTABLE/ACRIN4701RESCUE/tabid/747/Default.aspx
April 2016
April 2016 CUTEheart Workshop
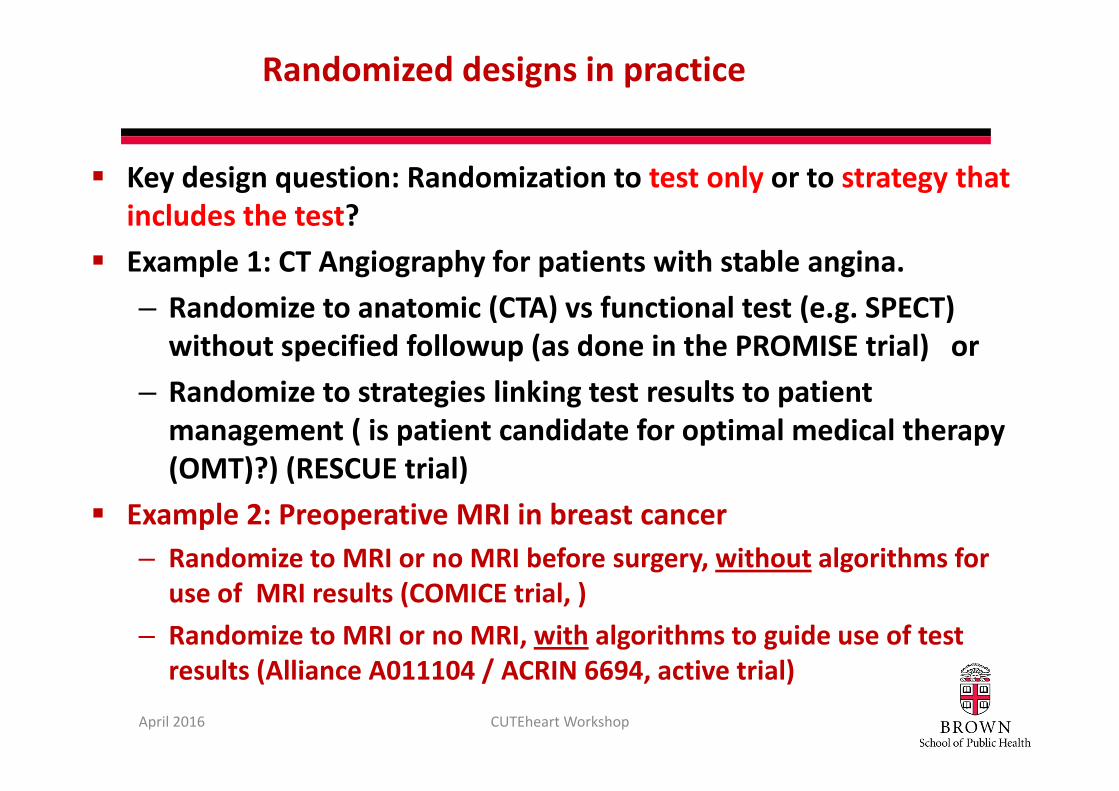
Randomized designs in practice
Key design question: Randomization to test only or to strategy that includes the test?Example 1: CT Angiography for patients with stable angina. – Randomize to anatomic (CTA) vs functional test (e.g. SPECT) without specified followup (as done in the PROMISE trial) or
– Randomize to strategies linking test results to patient management ( is patient candidate for optimal medical therapy (OMT)?) (RESCUE trial)
Example 2: Preoperative MRI in breast cancer– Randomize to MRI or no MRI before surgery, without algorithms for
use of MRI results (COMICE trial, )– Randomize to MRI or no MRI, with algorithms to guide use of test
results (Alliance A011104 / ACRIN 6694, active trial)

A more elaborate design-Paired tests-Randomized discordantpairs
April 2016 CUTEheart Workshop
Outcome
Tx2
Outcome
A B
+ + Tx1
Tx1
Tx2
Outcome
Outcome
Outcome
Tx1
- -
Tx2 Outcome
+ -
- +
R
R

April 2016 CUTEheart Workshop
Randomized designs in practice, cont.
Paired test designs– Efficient but rarely adopted. MINDACT trial is example.
– Ethical issues‐ can positive or negative test results be ignored?
– Implementation difficulties. Strong potential for non‐compliance.

Beyond clinical trials
• Observational studies– Registry studies – Electronic Medical Records– Claims datasets– Cohort studies
• Research synthesis– Systematic reviews and meta‐analysis– Modeling
April 2016 CUTEheart Workshop

Use of large databases (e.g. EMR, Claims)
General approach:– Construct longitudinal record including test and outcome information.
– Use methods for observational data to make comparisons.
Recent examples:– Coronary calcium study using Medicare claims.– Testing of ER patients with chest pain study using EMR data.
April 2016 CUTEheart Workshop

April 2016 CUTEheart Workshop
Outcomes After Coronary Artery Calcium and Other Cardiovascular Biomarker Testing Among Asymptomatic
Medicare BeneficiariesJacqueline Baras Shreibati, MD, MS; Laurence C. Baker, PhD; Michael V. McConnell, MD, MSEE; Mark A.
Hlatky, MD
Effectiveness of CAC and hs-CRP testing
Circ Cardiovasc Imaging.2014;7:655‐662.)
20% random sample of Medicare beneficiaries
without CVD claims in previous 6 mos.
Propensity score matching of patients receiving CAC and high sensitivity C-reactive protein testingCompared utilization and outcomes

Testing of ER patients with chest pain
>420K ER patients. Records from 2011 MarketscanPatients classified into 5 testing strategiesOutcomes compared using regression analysis
April 2016 CUTEheart Workshop
JAMA Intern Med. 2015;175(3):428‐436.

Limitations of Claims and EMR data
EMR and claims data typically deficient in key information about
Context of the test (indication, filtering)Test interpretation and findings Clinical characteristics of patientSubsequent diagnostic and therapeutic decisions
April 2016 CUTEheart Workshop
DiagnosticProcedure
OutcomesTHERAPY
Clinical Context

Limitations of Claims and EMR data
EMR and claims data typically deficient in key information about
Context of the test (indication, filtering)Test interpretation and findings Clinical characteristics of patientSubsequent diagnostic and therapeutic decisions
April 2016 CUTEheart Workshop
DiagnosticProcedure
OutcomesTHERAPY
Clinical Context
Defensivemedicine

Limitations of Claims and EMR data
EMR and claims data typically deficient in key information about
Context of the test (indication, filtering)Test interpretation and findings Clinical characteristics of patientSubsequent diagnostic and therapeutic decisions
April 2016 CUTEheart Workshop
DiagnosticProcedure
OutcomesTHERAPY
Clinical Context
Defensivemedicine
Creative Coding
National Oncologic PET Registry: A Nationwide Collaborative Program
Sponsored by
Managed by
Advisor
Goal: Assess the effect of PET on referring physicians’ plans of intended patient management.
• across a wide spectrum of cancer indications for PET, not covered currently by the Medicare program, •in relation to cancer‐type, indication, performance status, physician’s role in management, and scan type
April 2016 CUTEheart Workshop
http://www.cancerpetregistry.org
Biostatistics Center atBrown University

NOPR Accrual (Cases Completed/Business Day)
More than 200,000 patients registered

PET Changed Intended Management in 36.5% of Cases
Non-Treat Treat 23.2 31.6 28.6 29.2 28.3Treat Non-Treat 7.9 7.9 7.5 9.7 8.2Patients with change post-PET 31.1 39.5 36.1 39.0 36.5
Hillner et al J Clin Onc 2008
Clinical Indication for PET Study (Percent)
Pre-Pet Plan
Post-PET Plan
Dxn=5,616
Staging n=6,464
Restaging n=5,607
Recurrence n=5,388
Alln=22,975
Treat Same 16.0 46.5 15.8 20.4 25.5Non-Treat Same 52.9 14.0 48.0 40.7 37.9
April 2016 CUTEheart Workshop

Summary of NOPR Results (Before 2009 NCD)Overall Impact on Patient Management
– Diagnosis, Staging, Restaging, Recurrence– Data on 22,975 scans from May 8, 2006 – May 7, 2007– J Clin Oncol 2008; 26:2155‐61
Impact on Patient Management by Cancer Type– Confirmed Cancers– Staging, Restaging, Recurrence– Data on 40,863 scans from May 8, 2006 – May 7, 2008– J Nucl Med 2008; 49:1928‐35
Treatment Monitoring– Data on 10,447 scans from May 8, 2006 – Dec 31, 2007– Cancer 2009:115:410‐18
April 2016 CUTEheart Workshop

April 2016 CUTEheart Workshop
Do NOPR findings agree with those from • other studies or • other sources of information on the same participants
How does registry information compare to other sources?

Combining registries with administrative and insurance databases
– Linking NOPR and CMS claims data
April 2016 CUTEheart Workshop
Registry record
CMS claims, longitudinal
record

NOPR strengths
Provided extensive, timely, “real world” data, that are very difficult and expensive to collect in clinical trials.Prospectively organized and controlled data collectionRegistry data can be effectively linked to data from other information sourcesResults consonant with more tightly controlled studies (later in presentation)Supports the Coverage with Evidence Decisions approach of CMS
April 2016 CUTEheart Workshop

NOPR weaknesses (long list!)
April 2016 CUTEheart Workshop
Evidence documents change in intended management, not actualmanagementNo evaluation of whether management changes were appropriate.No information on whether the use of PET improved long‐term outcomesHow should PET should be used in the flow of patient care.Plus the concerns about generalizability and bias in data obtained from registries

Imaging Amyloid Plaques (PIB-PET)A harder case: Diagnosis ahead of therapy
April 2016 CUTEheart Workshop
18F-florbetaben (Piramal) March 2014 (Neuraceq)
18F-florbetapir (Avid/Eli Lilly) April 2012 (Amyvid)
18F-flutemetamol (GE) October 2013 (Vizamyl)

CMS National Coverage Decision
Insufficient evidence of clinical utility to justify coverage of Aβ PETReimbursement would be considered under coverage with evidence development (CED) in clinical studies designed to:• Develop better treatments or prevention strategies for AD
• Identify subpopulations at risk for developing AD• Resolve clinically difficult differential diagnoses (e.g., frontotemporal dementia versus AD)
• Must demonstrate Aβ PET improves health outcomes (short‐term outcomes related to changes in management as well as longer‐term dementia outcomes)CUTEheart WorkshopApril 2016

Combining registries with administrative and insurance databases
– Amyloid plaque imaging: Comparison of
• Registry of participants undergoing Dx, and
• Matched Controls identified from CMS claims data
April 2016 CUTEheart Workshop
?? ?
?

IDEAS Steering CommitteeCore Science TeamGil Rabinovici, UCSFMaria Carrillo, Alzheimer’s AssociationConstantine Gatsonis, Brown UBruce Hillner, VCUBarry Siegel, Wash URachel Whitmer, Kaiser Permanente
Additional committee membersWilliam Abbot, Piramal ImagingRosemarie Hakim, CMSMeredith Johnson, GE HealthcareMark Mintun, Avid RadiopharmaceuticalsDon Rosen, ACR
ACR OperationsCharlie ApgarCynthia Olson
MITA representative :Terri WilsonConsultant: Brian Carey, FoleyHoag LLP
Biostatistics Center (Brown U)Ilana GareenRoee GutmanErin GrecoLucy HannaBenjamin HermanRajesh Makineni
Scientific and logistical supportJim Hendrix, Alzheimer’s Association
CUTEheart WorkshopApril 2016

IDEAS (Imaging Dementia—Evidence for Amyloid Scanning)
Two main goals:Aim 1: To assess the impact of amyloid PET on the management of patients meeting Appropriateness Use Criteria – This aim will be addressed using a registry of
participants undergoing amyloid PET.Aim 2: To compare hospital admissions and emergency room visits within 12 months in patients enrolled in the registry to matched controls (no amyloid PET), to be identified from CMS claims data. – This aim will be addressed using linked registry and CMS claims data.
https://clinicaltrials.gov/ct2/show/NCT02420756?term=IDEAS&rank=1
April 2016 CUTEheart Workshop

Sample size considerations
Aim 1 Hypothesis: Determine whether amyloid PET imaging will lead to a ≥ 30% change between intended and actual patient management within 90 days in a composite measure consisting of the following:a) AD drug therapy; b) Other drug therapy; orc) Counseling about safety and future planningN=11,050 for 80% power (separate analyses for dementia and MCI subgroups)
Aim 2 Hypothesis: Determine whether amyloid PET is associated with a ≥ 10% relative reduction in registry patients in comparison to matched controls in the following endpoints: a) Inpatient hospital admissions over 12 months. b) Emergency room visits over 12 monthsN= 18,500 for 90% power (separate analyses for each endpoint)
April 2016 CUTEheart Workshop

April 2016 CUTEheart Workshop
In closing

(Can we assess) how effective is diagnosis in health care?
Current approaches can be enhanced: Linking tests to downstream outcomes is a challenging undertaking.Large secondary databases can be used, but may lack necessary information.Registries offer flexibility but typically have narrow focus.Combination of information from several sources holds promise.
April 2016 CUTEheart Workshop

CUTEheart WorkshopApril 2016
Solutions to the Problem: Coverage with Requirement for Data Collection through a National Registry or Registries1) Require Standardization of High Quality Testing2) Compare Back to Companion Diagnostics Where Available3) Collect Outcomes: High‐level clinical outcomes need to be collected and compared back to the new testing standard. 4) Attach Testing to Existing and Future Clinical Trials5) Aggregate All Data, Nationally and Internationally
Editorial by ASCO
CMS to Trim Spending on Diagnostic Lab TestsThe Centers for Medicare and Medicaid Services appear to be executing a two‐step strategy to shrink the $8 billion annual price tag of clinical diagnostic laboratory tests.On Sept. 25, CMS released a final payment determination for the Clinical Laboratory Fee Schedule that cuts payment by over 90 percent for some tests

New realities in health care:Integrated Systems, ACOs, etc
April 2016 CUTEheart Workshop
Comment in “Modern Health Care” The CMS stance on PET is an artifact of fee‐for‐service medicine. In a few years, as insurers in both the public and private sectors gravitate toward episode‐based and bundled care, the risk of using expensive and unproven technologies that don't improve outcomes won't fall on payers. It will fall on the purchasers of those expensive technologies which, for PET scanners, are mostly hospitals.
Decision Memo for Positron Emission Tomography (NaF-18) to Identify Bone Metastasis of Cancer (CAG-00065R)CMS has concluded that the evidence is not sufficient to determine that the results of NaF-18 PE imaging to identify bone metastases improve health outcomes of beneficiaries with cancer. Therefore we have determined that this use is not reasonable and necessary under §1862(a)(1)(A) of the Social Security Act.

New realities in health care:Integrated Systems, ACOs, Bundled Care etc
April 2016 CUTEheart Workshop
The CMS stance on PET is an artifact of fee‐for‐service medicine. In a few years, as insurers in both the public and private sectors gravitate toward episode‐based and bundled care, the risk of using expensive and unproven technologies that don't improve outcomes won't fall on payers. It will fall on the purchasers of those expensive technologies which, for PET scanners, are mostly hospitals.
• New incentives for health care systems to developmandexpand their own research efforts.
• Realistic hope for better data from more effective and efficient information systems.
• Continuous, integrated, enterprise‐wide data collection • Effectiveness questions posed from a “systemic” perspective in contrast to the current la carte evaluation of components of health care.
• Metrics and endpoints would be adapted to new realities.• Validity and Generalizability of findings may be a challenge.

April 2016 CUTEheart Workshop
Thank you!

April 2016 CUTEheart Workshop

Key challenges
Best target population (age range?; MCI vs. atypical dementia?)No established clinical management algorithms based on scan results (unlike situation for FDG‐PET in cancer)No good historical control dataSome patient‐centered outcomes will take quite long to be detectable (slowing of functional decline vs. avoiding futile Rx)
April 2016 CUTEheart Workshop

NOPR linked to CMS claims data
April 2016 CUTEheart Workshop
Approach
Construct health care utilization history using CMS claims dataCohort of 8640 consenting registry participants, age 65+, enrolled in 2007‐2008 undergoing PET for cancer restaging.Extensive database work involved to identify patterns of care and classify into post‐PET treatment categories.
(Med Care 2013;51: 361–367)

Australian Prospective Studies of Impact of PETAgreement in Post-PET Plan and Actual Care (2003-2006)
April 2016 CUTEheart Workshop
Cancer Pts Centers Indication Change in Plan
F/U (mo.
)
Agree-ment
Ovarian 90 3 SR 58.9 6 67.8 Esophagus 129 5 IS 38.0 12 53.2 Lymphoma 74 6 IS 34.0 6 74.3 Colorectal 93 4 SR 65.6 6 62.0 Colorectal 98 4 Resect
Hepatic 49.0
6
70.1
Head/Neck 71 3 IS 33.8 3 74.7 SR: Suspected Recurrence. IS: Initial Staging

Referring MD requests amyloid
PETPatient consent.
Visit 1 Pre‐PET
assessment and form completed
Visit 2PET done, interpreted
& reported.MD communicates results to participant
Visit 390‐day Post‐PET Assessment andform completed
Ongoingpatient
management
IDEAS Registry Workflow (main steps)
April 2016 CUTEheart Workshop

April 2016 CUTEheart Workshop
Additional material

Impact of PET Used for Treatment Monitoring
• Chemotherapy 82%, chemoRT 12%, RT 6%• Ovarian, pancreas, NSCLC, SCLC most frequent• Metastatic disease in 54%• PET findings led to:
– Switch to another therapy in 26%
– Adjust dose or duration of therapy in 17%
– Switch from therapy to observation/supportive care in 6%
• Management change more often if post-PET prognosis worse rather than improved/unchanged (70% vs. 40%)
Hillner et al., Cancer 2009; 115:410
April 2016 CUTEheart Workshop

NOPR Analysis by Cancer Types
Two years of data (40,863 scans)Confirmed Cancers
Initial staging, restaging, suspected recurrencesAll Cases Change in
Management95% C.I. Imaging adjusted
impact
Initial staging 39.8 39.0-40.6 13.4Restaging 35.9 35.1-36.7 12.6Suspected Recurrences 38.5 37.6-39.3 14.7
April 2016 CUTEheart Workshop
All Cases Initial Staging Restaging Suspected Recurrence
Prostate 32.0 34.0 39.4Ovary 43.1 37.7 44.5Bladder 39.9 36.4 36.7Pancreas 39.2 38.3 39.3
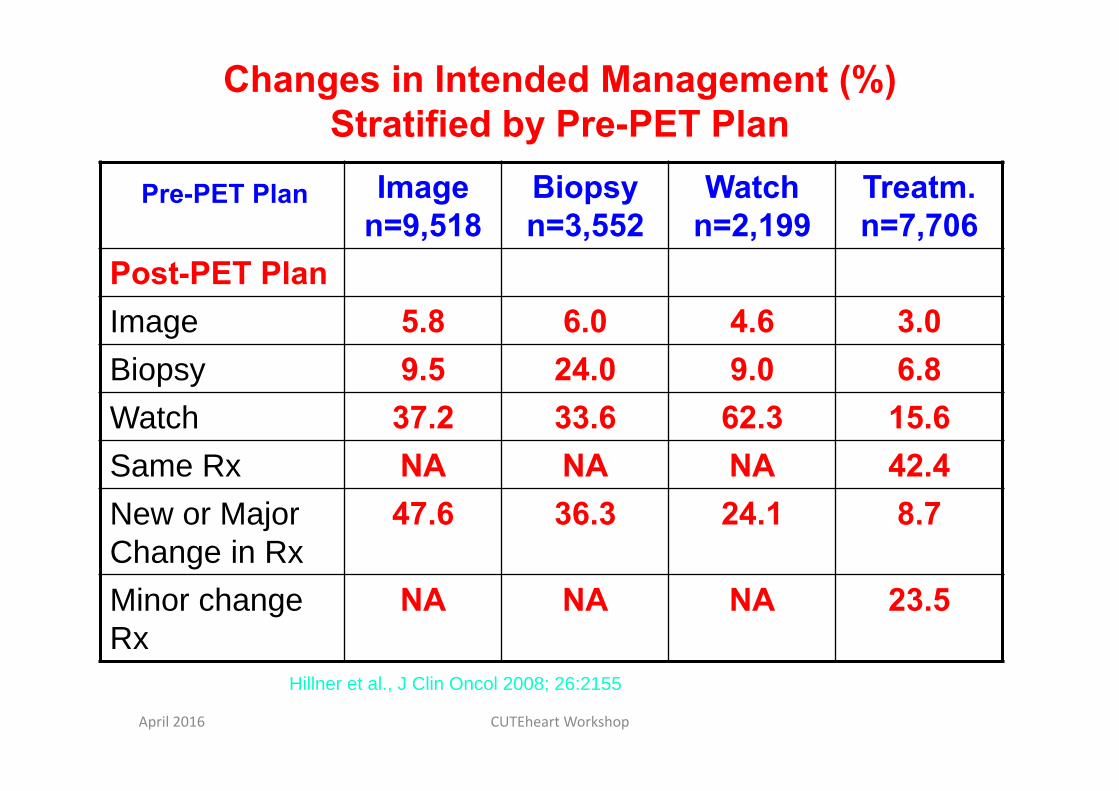
Changes in Intended Management (%) Stratified by Pre-PET Plan
Image n=9,518
Biopsy n=3,552
Watch n=2,199
Treatm. n=7,706
Post-PET PlanImage 5.8 6.0 4.6 3.0Biopsy 9.5 24.0 9.0 6.8Watch 37.2 33.6 62.3 15.6Same Rx NA NA NA 42.4New or Major Change in Rx
47.6 36.3 24.1 8.7
Minor change Rx
NA NA NA 23.5
Pre-PET Plan
Hillner et al., J Clin Oncol 2008; 26:2155
April 2016 CUTEheart Workshop

Patient presentation
Treatment Decisions
Diagnostic workup
Patient outcomes
April 2016 CUTEheart Workshop

The study of modalities for diagnosis and Prediction: Conceptual Framework
Fundamentally tests provide information for use in selecting course of care. Both long‐ and short‐term effects of tests materialize in context of available health care options, including therapeutic interventions.Not possible to define and measure test effects outside the particular health care context in which the test will be used. However, oftentimes diagnosis may be ahead of therapy: Diagnosis of DCIS; Amyloid plaque imaging for Alzheimer’s.
April 2016 CUTEheart Workshop

Pre‐PET Form: Intended Patient Management
Observation (with close follow‐up)Additional imaging (CT, MRI) or other non‐invasive diagnostic testsTissue biopsy (surgical, percutaneous, or endoscopic). Treatment (if treatment is selected, then also complete the following)Treatment Goal: (check one) Curative PalliativeType(s): (check all that apply)
– Surgical Chemotherapy (including biologic modifiers)– Radiation Other Supportive care
If PET were not available, your current management strategy would be (select one)?
Intended management, given PET findings, asked on post-PET form
April 2016 CUTEheart Workshop

Cohort Profile• First year of NOPR
(5/8/06 to 5/7/07)• 22,975 “consented”
cases from 1,519 facilities
• Technology profile – 84% PET/CT– 71% non-hospital– 76% fixed sites
Hillner et al., J Clin Oncol 2008April 2016 CUTEheart Workshop

Intended vs Inferred Care after PET for initial staging
April 2016 CUTEheart Workshop
J Nucl Med 201354:2024–2031
Cohort of 4661 consenting registry participants, age 65+, enrolled in 2007‐2008. PET for initial cancer restaging. N PPV Agreement KappaAny systemic txAll 3,030 79.3 74.1 0.40Bladder 676 79.0 73.0 0.42Ovarian 223 86.1 82.5 0.52Stomach 648 67.6 67.6 0.34
Any radiationAll 1,293 64.7 80.8 0.53Bladder 337 68.8 83.3 0.60Ovarian 23 30.4 91.6 0.32Stomach 250 48.8 79.0 0.39Any surgeryAll 1,031 63.6 77.9 0.43Bladder 248 56.9 75.8 0.36Ovarian 57 52.6 75.9 0.31Stomach 458 71.4 75.7 0.50
ConclusionBetter concordancethan in restaging PET

Clark et al. JAMA 2011, Lancet Neurol 2012
Pathology Validation: Florbetapir PET
Median 5 raters vs. autopsySensitivity 92%(69%-95%)Specificity 95%(90%-100%)
FDA approval:• Florbetapir
(AmyvidTM) 2012
• Flutemetamol(VizamylTM) 2013
• Florbetaben(NeuraceqTM) 2014
April 2016 CUTEheart Workshop

Amyloid vs. FDG-PET in Differential Diagnosis of AD vs. FTD
Rabinovici et al. Neurology 2011Rabinovici et al. AAN 2014
AD (N=62, age 65, MMSE 22)FTD (N=45, age 65, MMSE 22)Amyloid (PIB) PET visual reads
90% sensitivity, 83% specificityInter-rater agreement κ=0.96
FDG-PET visual reads78% sensitivity*, 84% specificityInter-rater agreement κ=0.72*
47 autopsy-proven casesPIB: Sensitivity 100%, Specificity 90%FDG: Sensitivity 87%, Specificity 78%
* ‐ p<0.05 vs. PIB
April 2016 CUTEheart Workshop

IDEAS study (under development)
Organization:
Working collaboration of researchers from NOPR Working Group, Alzheimer’s Association, SNMMI, American College of Radiology Imaging Network, and Brown Biostatistics.
Stakeholders from industry and professional organizations.
Support from industry and from CMS (coverage of scans)
April 2016 CUTEheart Workshop

Control group construction: Selection of superset
April 2016 CUTEheart Workshop
Criterion Factors/Examples Time1 New Diagnosis of MCI or
Dementia*CMS claims related to dementia and MCI in the 24 mo. prior to IDEAS Study initiation
≥24 mo.
1A MCI CODE 331.83 Mild cognitive impairment-other codes to be selected in sensitivity analysis
1B DEMENTIA CODE: Prior to structural imagingInconsistent claims patterns*
≥2 different categories of dementia codes or>2 claims with exclusively limited to non-specific dementia codes) occurring within a two year (24 month) time interval
2 Minimal Structural Brain Tests Minimal Blood Laboratory w/u
Head MRI or CT (+/-) CBC, standard blood chemistry profile, TSH, vitamin B12
<12 mo.
3 Exclude cases with unanticipated brain pathology on intake MRI/CT
Such as primary or metastatic cancers at time of match and at baseline for contemporaneous cohort
4 Exclude cases with:‐ All Non-Skin Cancers,
Lymphomas, Hematologic Malignancies
‐ Hip/Pelvic Fracture
<12 mo.

PET Amyloid Imaging
Imaging biomarkers for amyloid deposits have been approved by FDA:– 18F‐florbetapir in April 2012,– 18F‐flutemetamol in October 2013– 18F‐florbetaben in March 2014 CMS National Coverage Decision in September 2013Coverage for one study per patient, but only under CED to:– Develop better treatments or prevention strategies for AD, or,
as a strategy to identify subpopulations at risk for developing AD
– Resolve clinically difficult differential diagnoses (e.g., FTD vs. AD) with goal of improving health outcomes (including short term outcomes related to changes in management as well as longer term dementia outcomes).
April 2016 CUTEheart Workshop

Control group construction: Matching criteria
April 2016 CUTEheart Workshop
Criterion Factors/Examples Time1 Age Minimal age of 66 to 67 years +/-24mo.2 Gender N.A.3 Marital status N.A.4 Ethnicity N.A.5 Location/Service Area Hospital Referral Region (n=306) N.A.6 Match Chronic
Condition Warehouse per table below: Focus is on conditions related to hospitalizations
Match on number or specifics of associated CMS Codes. Non-CHF heart disease is an aggregate of Acute MI, A fib,, HTN, and CAD/IHD), CKD, COPD, diabetes
<24 mo.
7 Match for Chronic Neurological Conditions, not included in Warehouse
Prior stroke, TIA, PD, MS, epilepsy, TBI
<24 mo.
8 Hospitalization/Emergency Room Visits
Dementia or delirium <12 mo.
9 Medicare/Medicaid Eligibility
Single or dual eligibility N.A.

CUTEheart WorkshopApril 2016
rA1= rate of favorable outcomes for pts randomized to test A
rB2= rate of favorable outcomes for discordant cases randomized to be treated according to result of A
Difference between arms in simple randomized design
Difference between arms in randomized of discordant cases design
D1= rA1 ‐ rB1 =(r21-r11) x p x (SeB – SeA)+(r22-r12) x (1-p) x (SpA – SpB)
D2= rA2 – rB2 =[(r21-r11) x p x (SeB – SeA)+(r22-r12) x (1-p) x (SpA – SpB)]
= D1/ fwhere f = fraction of discordant cases

April 2016 CUTEheart Workshop
Collect Registry participant data
Select superset of potential matches from national CMS claims data using inclusion/exclusion criteria
Select matching cases from superset
Streamlined process flow of selection of controls
April 2016 CUTEheart Workshop
The Recent Reversal of the Growth Trend in MRI: A Harbinger of the Future?Richard Sharpe et al. JACR 2013
JACR 2012
CMS to Trim Spending on Diagnostic Lab TestsThe Centers for Medicare and Medicaid Services appear to be executing a two‐step strategy to shrink the $8 billion annual price tag of clinical diagnostic laboratory tests.On Sept. 25, CMS released a final payment determination for the Clinical Laboratory Fee Schedule that cuts payment by over 90 percent for some tests
October 2, 2015

Referring MD requests PET
Pre-PET Form
PETdone
PET interpreted& reported
Post-PETForm sent,
including question for referring MD consent
Post-PET Form completed.
Claim submitted
Ongoingpatient
management
NOPR Workflow
Ask patient for consent
April 2016 CUTEheart Workshop

Agreement of Post‐PET Plan and Claims‐inferred Actions at 30 Days
April 2016 CUTEheart Workshop
Bladder Ovary StomachPatients (total), n 1127 2075 632Systemic tx only planned, n 261 811 134
PPV (%) 66.7 65.0 51.5Raw agreement (%) 71.2 71.1 65.7k 0.33 0.40 0.17
Radiation only planned, n 71 46 34PPV (%) 74.6 67.4 35.3Raw agreement (%) 89.4 96.9 95.3k 0.42 0.48 0.23
Biopsy planned, n 150 176 85PPV (%) 64.7 55.1 48.2Raw agreement (%) 74.4 80.5 75.2K 0.27 0.23 0.21
Watching, n 473 804 320PPV (%) 70.8 74.1 66.3Raw agreement (%) 71.0 69.1 60.8k 0.41 0.38 0.21
Med Care 2013;51: 361–367
Conclusion: Moderate concordance

National coverage of NOPR registry (2006-2009)
April 2016 CUTEheart Workshop

April 2016 CUTEheart Workshop
Randomized designs in practice, cont.
Randomization to test only or to strategy with test?– Tradeoff between generalizability and efficiency
• Test only: “noisy” (hence larger sample sizes) but may be more generalizable
• Test as part of strategy : Less “noise” but results apply to specific strategies.
– Compliance is important factor to study.Paired test designs– Efficient but rarely adopted (see recent report in JClinEpi). MINDACT trial is example.
– Ethical issues‐ can positive or negative test results be ignored?
– Implementation difficulties.


















