2H-Nuclear Magnetic Resonance Imaging of Tumor Blood …€¦ · mon injection of D20 is easily...
11
ICANCERRESEARCH 52, 6010-6019, November1, 19921 ABSTRACT 2H-Nuclear magnetic resonance imaging of deuteron accumulation in tissue following an i.v. bolus of deuterium oxide provides a noninvasive means of constructing maps of tissue perfusion. With a measured ante rial input function and a simple model for tissue-capillary exchange, these data can provide quantitative estimates of local flow. This tech nique was tested in rat brain and then applied to the study of spatial heterogeneity and temporal variation of blood flow in the tissue-isolated R3230AC mammary adenocarcinoma. Global flow from the brain aver aged 0.96 ml/min.g, in good agreement with results obtained from other methods; the perfusion of brain was relatively homogeneous. Global tumor blood flow averaged 0.32 ml/min.g, ranging from 0.11 to 0.96 ml/min.g. Imaging revealed variations in perfusion both within and between the tumors that far exceeded those expected from brain flow heterogeneity and uncertainty in the flow estimates. By obtaining re peated flow images at 30-mm intervals, it was possible to show that the regional blood flow shifted with time in single pixels and in multipixel regions. These experiments show that 2H-nuclear magnetic resonance may be useful in obtaining noninvasiveand quantitative measurement of temporal blood flow changes in a solid tumor in vivo. INTRODUCTION The blood flow within solid tumors often displays a marked spatial heterogeneity (1, 2). As tumors grow, large regions be come poorly perfused. This heterogeneity has important con sequences for both basic cancer research and clinical oncology (3). In regions where perfusion is poor, the delivery of such critical nutrients as oxygen and glucose cannot keep pace with the metabolic demands of the neoplastic cells (4). Nutrient concentrations in the poorly perfused regions fall. Blood flow heterogeneity thus leads to a heterogeneous extracellular envi ronment (5). Neoplastic cells subject to different perfusion and different extracellular environments may well respond differ ently to metabolic challenge or cancer therapy. The decreased efficacy ofradiation therapy in regions with low 02 levels is one example (6). More directly, blood flow is critical for the delivery of any blood-borne anticancer agent. However, despite its im portance, regional blood flow distribution is rarely measured because of the difficulties associated with perfusion measure ments. 3 measurement of exogenous D20 shows promise as a noninvasive means of measuring regional tumor blood flow (7). This method is similar in theory to other tracer techniques used Received 4/24/92; accepted 8/8/92. The costs of publicationof this article were defrayedin part by the paymentof pagecharges. Thisarticlemustthereforebeherebymarkedadvertisement inaccord ance with 18 U.S.C. Section 1734 solely to indicate this fact. I SupportedbyNationalCancer InstituteGrantCA37239(toR.K.J.)andNIH Regional Resources Grant 1 P41 RR03631 (to Pittsburgh NMR Center). We are grateful to the Richard King Mellon Foundation, the Lucille P. Markey Charitable Trust, the Ben Franklin Partnership Program of the Commonwealth of Pennsyl vania, and the Ralph M. Parsons Foundation for providing financial support for the establishment ofthe Pittsburgh NMR Center for Biomedical Research. Portions of this work were presented at the Society of Magnetic Resonance in Medicine, Ninth Annual Meeting, New York, NY, August 18—24, 1990. 2 To whom requests for reprints should be addressed, at Department of Radia tion Oncology, Massachusetts General Hospital, Boston, MA 02114. 3Theabbreviations usedare:NMR,nuclearmagnetic resonance; c.v.,thesquare root of the variance divided by the mean. to measure blood flow. The deuteron is a stable nuclide pos sessing a magnetic moment with spin 1 and is readily detected by NMR. As a small molecule, D2O has a large diffusion coef ficient, similar to that of water, enabling it to distribute rapidly in tissue. Administered acutely, it appears to have little toxicity (see Ref. 8 and references therein). Many measurements of whole organ blood flow distribution have been made using D2O and 2H-NMR spectroscopy (7) and this technique has been used for the measurement of tumor blood flow. Direct intratu mon injection of D20 is easily applied and yields global blood flows similar to those obtained by other methods (9). However, particularly in heterogeneous tumors, it suffers from the fact that it measures blood flow only in a small region about the site of injection, a region potentially traumatized by the injection itself(10). The measurement oftissue uptake of deuterons from the blood avoids these problems. This uptake, following i.v. or i.p. injection, has been used to study changes in global tumor blood flow (1 1, 12). A natural extension of these spectroscopic measurements is the NMR imaging of organ D20 accumula tion after exogenous administration. From the measurement of D20 accumulation within each volume element, it is possible to extract values for the local blood flows and create a map of the spatial blood flow distribution. For tumors, in which blood flow is often heterogeneous, such a measurement would be particu larly valuable. To date, D2O imaging has been used to obtain qualitative maps of relative blood flow from subcutaneous mu nine tumors (13). Further, the noninvasive nature of this tech nique makes it possible to monitor tumor blood flow over time. While it has been shown recently that regional tumor blood flow may vary on a short time scale (14), these acute variations have not been examined noninvasively or quantitatively in solid tumors. We present here the results of experimental efforts to quan titate spatial and temporal variations of the blood flow in a tissue-isolated mammary adenocarcinoma. The tissue-isolated tumor is a model tumor prepared so that it has a single artery and vein as its vascular connections to the host. This prepara tion allows one to isolate the tumor from surrounding tissue and ensures that the â€oeorgan― has a single arterial input, simpli fying the theoretical analysis. 2H imaging is used to monitor regional D20 accumulation in tissue following an i.v. bolus. Quantitative estimation of the blood flow is made possible with the measurement of the arterial input function for the tracer. The technique is tested through measurements of regional blood flow in a well-studied normal organ, the brain. The tech nique is used to quantitate the spatial distribution of flow in a series of the tumors. Repeated measures made in the same tumors are used to quantify the acute temporal changes that occur in the blood flow of these tumors. MATERIALS AND METHODS Preparation of Tumors. All tumor studies were performed using the R3230AC mammary adenocarcinoma (Biomeasure Laboratories, Hop kinton, MA). This tumor is maintained in our laboratory by serial s.c. 6010 2H-Nuclear Magnetic Resonance Imaging of Tumor Blood Flow: Spatial and Temporal Heterogeneity in a Tissue-isolated Mammary Adenocarcinoma' Clifford J. Eskey, Alan P. Koretsky, Michael M. Domach, and Rakesh K. Jam2 Departments ofChemical Engineering [C. I. E., M. M. D.J and Biological Sciences (A. P. K.], Pittsburgh NMR Centerfor Biomedical Research (C. J. E.. A. P. K.J, Carnegie Mellon University, Pittsburgh, Pennsylvania 15213, and Edwin L. Steele Laboratory, Department ofRadiation Oncology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 02114 (R. K. I.] on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of 2H-Nuclear Magnetic Resonance Imaging of Tumor Blood …€¦ · mon injection of D20 is easily...

ICANCERRESEARCH52, 6010-6019, November1, 19921
ABSTRACT
2H-Nuclear magnetic resonance imaging of deuteron accumulation intissue following an i.v. bolus of deuterium oxide provides a noninvasivemeans of constructing maps of tissue perfusion. With a measured anterial input function and a simple model for tissue-capillary exchange,these data can provide quantitative estimates of local flow. This technique was tested in rat brain and then applied to the study of spatialheterogeneity and temporal variation of blood flow in the tissue-isolatedR3230AC mammary adenocarcinoma. Global flowfrom the brain averaged 0.96 ml/min.g, in goodagreement with results obtained from othermethods; the perfusion of brain was relatively homogeneous. Global
tumor blood flow averaged 0.32 ml/min.g, ranging from 0.11 to 0.96ml/min.g. Imaging revealed variations in perfusion both within andbetween the tumors that far exceeded those expected from brain flowheterogeneity and uncertainty in the flow estimates. By obtaining repeated flow images at 30-mm intervals, it was possible to show that theregional blood flow shifted with time in single pixels and in multipixelregions. These experiments show that 2H-nuclear magnetic resonancemay be useful in obtaining noninvasiveand quantitative measurement oftemporal blood flow changes in a solid tumor in vivo.
INTRODUCTION
The blood flow within solid tumors often displays a markedspatial heterogeneity (1, 2). As tumors grow, large regions become poorly perfused. This heterogeneity has important consequences for both basic cancer research and clinical oncology(3). In regions where perfusion is poor, the delivery of suchcritical nutrients as oxygen and glucose cannot keep pace withthe metabolic demands of the neoplastic cells (4). Nutrientconcentrations in the poorly perfused regions fall. Blood flowheterogeneity thus leads to a heterogeneous extracellular environment (5). Neoplastic cells subject to different perfusion anddifferent extracellular environments may well respond differently to metabolic challenge or cancer therapy. The decreasedefficacy ofradiation therapy in regions with low 02 levels is oneexample (6). More directly, blood flow is critical for the deliveryof any blood-borne anticancer agent. However, despite its importance, regional blood flow distribution is rarely measuredbecause of the difficulties associated with perfusion measurements.
3 measurement of exogenous D20 shows promise as a
noninvasive means of measuring regional tumor blood flow (7).This method is similar in theory to other tracer techniques used
Received 4/24/92; accepted 8/8/92.The costs of publicationof this articleweredefrayedin part by the paymentof
pagecharges.Thisarticlemustthereforebeherebymarkedadvertisementinaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
I SupportedbyNationalCancerInstituteGrantCA37239(toR.K.J.)andNIHRegional Resources Grant 1 P41 RR03631 (to Pittsburgh NMR Center). We aregrateful to the Richard King Mellon Foundation, the Lucille P. Markey CharitableTrust, the Ben Franklin Partnership Program of the Commonwealth of Pennsylvania, and the Ralph M. Parsons Foundation for providing financial support for theestablishment ofthe Pittsburgh NMR Center for Biomedical Research. Portions ofthis work were presented at the Society of Magnetic Resonance in Medicine, NinthAnnual Meeting, New York, NY, August 18—24,1990.
2 To whom requests for reprints should be addressed, at Department of Radia
tion Oncology, Massachusetts General Hospital, Boston, MA 02114.3Theabbreviationsusedare:NMR,nuclearmagneticresonance;c.v.,thesquare
root of the variance divided by the mean.
to measure blood flow. The deuteron is a stable nuclide possessing a magnetic moment with spin 1 and is readily detectedby NMR. As a small molecule, D2O has a large diffusion coefficient, similar to that of water, enabling it to distribute rapidlyin tissue. Administered acutely, it appears to have little toxicity(see Ref. 8 and references therein). Many measurements ofwhole organ blood flow distribution have been made using D2Oand 2H-NMR spectroscopy (7) and this technique has beenused for the measurement of tumor blood flow. Direct intratumon injection of D20 is easily applied and yields global bloodflows similar to those obtained by other methods (9). However,particularly in heterogeneous tumors, it suffers from the factthat it measures blood flow only in a small region about the siteof injection, a region potentially traumatized by the injectionitself(10). The measurement oftissue uptake of deuterons fromthe blood avoids these problems. This uptake, following i.v. ori.p. injection, has been used to study changes in global tumorblood flow (1 1, 12). A natural extension of these spectroscopicmeasurements is the NMR imaging of organ D20 accumulation after exogenous administration. From the measurement ofD20 accumulation within each volume element, it is possible toextract values for the local blood flows and create a map of the
spatial blood flow distribution. For tumors, in which blood flowis often heterogeneous, such a measurement would be particularly valuable. To date, D2O imaging has been used to obtainqualitative maps of relative blood flow from subcutaneous munine tumors (13). Further, the noninvasive nature of this technique makes it possible to monitor tumor blood flow over time.While it has been shown recently that regional tumor bloodflow may vary on a short time scale (14), these acute variationshave not been examined noninvasively or quantitatively in solidtumors.
We present here the results of experimental efforts to quantitate spatial and temporal variations of the blood flow in atissue-isolated mammary adenocarcinoma. The tissue-isolatedtumor is a model tumor prepared so that it has a single arteryand vein as its vascular connections to the host. This preparation allows one to isolate the tumor from surrounding tissueand ensures that the “organ―has a single arterial input, simplifying the theoretical analysis. 2H imaging is used to monitorregional D20 accumulation in tissue following an i.v. bolus.Quantitative estimation of the blood flow is made possible withthe measurement of the arterial input function for the tracer.The technique is tested through measurements of regionalblood flow in a well-studied normal organ, the brain. The technique is used to quantitate the spatial distribution of flow in aseries of the tumors. Repeated measures made in the sametumors are used to quantify the acute temporal changes thatoccur in the blood flow of these tumors.
MATERIALS AND METHODS
Preparation of Tumors. All tumor studies were performed using theR3230AC mammary adenocarcinoma (Biomeasure Laboratories, Hopkinton, MA). This tumor is maintained in our laboratory by serial s.c.
6010
2H-Nuclear Magnetic Resonance Imaging of Tumor Blood Flow: Spatial andTemporal Heterogeneity in a Tissue-isolated Mammary Adenocarcinoma'
Clifford J. Eskey, Alan P. Koretsky, Michael M. Domach, and Rakesh K. Jam2
Departments ofChemical Engineering [C. I. E., M. M. D.J and Biological Sciences (A. P. K.], Pittsburgh NMR Centerfor Biomedical Research (C. J. E.. A. P. K.J,Carnegie Mellon University, Pittsburgh, Pennsylvania 15213, and Edwin L. Steele Laboratory, Department ofRadiation Oncology, Massachusetts General Hospital,Harvard Medical School, Boston, Massachusetts 02114 (R. K. I.]
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

2H-NMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
propagation in Fischer 344 weanlings. The tissue-isolated tumors wereprepared surgically using the procedure developed by Gullino (15) andmodified in our laboratory (16). Through an incision in the abdominalwall, the ovary is exposed and excised. In the fat pad that remains,tumor slurry is injected. The fat pad is then enveloped in a Parafilm bagand placed in a subcutaneous pouch. Tumor blood flow is supplied bythe ovarian artery; all venous outflow returns via the ovarian vein. Forthese studies, the tissue-isolated tumors were used for experiments12—17 days following implantation; at this age the tumors weighedbetween 0.6 and 1.2 g.
Animal, Anesthesia, Surgery, and Monitoring. All experiments wereperformed with Fischer 344 rats anesthetized with O2:N20 (1:1) contaming 1.4—1.6 volume % halothane administered via a small animalventilator. For all studies, the jugular vein was cannulated with polyethylene tubing (0.58 mm inside diameter, 0.97 mm outside diameter)and served as the entry site for infused D2O. Rectal temperature wasmaintained at 37 ±iT (SD) with an indicating controller connected toa circulating water bath/heating pad. For all animals used in tumorstudies, the carotid artery was cannulated and used to monitor bloodpressure. The subcutaneous pouch was opened, and the tumor, withinits Parafllm bag, was placed inside the radiofrequency probe. For allanimals used in brain studies, the carotid artery was not cannulated. Forarterial input measurements, a 40—45cm length oftubing was spliced inthe carotid artery.
Arterial Input Measurements. The time course of deuteron concentration in arterial blood was measured by 2H-NMR spectroscopy. A5-cm section of the tubing spliced into the carotid artery was placedinside a 4-turn, 1.0-cm inside diameter solenoid tuned to 2H (46.1MHz). When the spliced tubing was initially opened, the arterial bloodpassed through with a velocity ofapproximately 10 cm/s. Serial spectrawere collected using 56 acquisitions/spectrum and a total acquisitiontime ofroughly 8 s. After severalbaseline spectra had been acquired, 2.0ml of D2O saline were infused at a constant rate over 25—30s via thejugular cannula. Spectra were collected continuously for 10 mm. Themeasurements were performed three times, 30 mm apart, in each animal; three animals were studied. Signal intensity was determined fromthe integrated peak area.
2H-NMR Imaging. All 2H imaging and spectroscopy experimentswere performed on a 7.0 Tesla (‘Hresonance frequency, 300 MHz; 2Hresonance frequency, 46 MHz), 15-cm-bore Bruker Biospec II imagingspectrometer (Bruker Instruments, Billenica, MA). Serial 2H imageswere made with a gradient-recalled echo sequence. These images weremade with an echo time of 6 ms, a repetition time of 50 ms, a slicethickness of 8 mm, and in-plane resolution of 1 mm. The radiofrequency probe consisted of a 2.0-cm-diameter, 6-turn solenoid and oneor two fixed capillary tubes containing D2O that were used to determinethe tumor location and correct for machine instability. A single slicewas selected from the center of the tumor using the capillary tubepositions on a perpendicular slice. After a background image hadbeen obtained, the 2.0-mI bolus of D2O saline was administered to therat as described in the input function methods while imaging continued.A series of ten images from the same slice was obtained as D20 accumulated in the tumor. The acquisition time for each image was 55 s.The data from these serial images were used to create a map of bloodflow.
Analysis. From a simple mass balance on a tissue compartmentsubject to the assumptions that flow is constant and that the compartment is homogeneous with respect to D2O concentration, i.e.,tracer uptake is limited solelyby blood flow, one can readily derive that
i=a(@) 5 C,(t-r)e@)dr
where I is signal intensity from the compartment, a is the constantrelating concentration and signal, F is the blood flow per unit tissueweight, Xis the tissue:blood partition coefficient, t is time, and C, is theconcentration of tracer in arterial blood as a function of time. GivenC,(t) and A it is possible to obtain an estimate of blood flow fromleast-squares regression of the I versus t data. This approach to theanalysis of tissue perfusion was first introduced to biomedicine by Kety
(17). The assumptions upon which this analysis is predicated are cx
plored further under “Discussion.―The simplest method for incorporating the C,(t) data is to fit the time
course of arterial concentration to an analytic expression, substitute the
expression in Equation A, and solve. For the experimental protocolused in our studies, the arterial input data are well described by a linearrise in concentration, followed by a biexponential decay. This functioncan be expressed as
[H(l—r,)-H(1-r2)]-ci--Cmu \r2—r,
+ H(t —@2)1(1—c) [de.f(t_12)+ (1 —d) ee('72)] + ci
(B)
where c, d, 1@g, r1, and r2 are adjustable parameters determined fromthe experimental input function data and H(x) is the unit step function.Because the 2H signal intensity from the spectroscopy experiments isgiven by the sum ofthe signal over the 8-s collection period, the arterial
input data are best described by the integral of the input function overthe collection period
s=@e;J:'+@'@@—dr (C)
where S is the peak area from the 2H spectrum, p is a constant relatingnormalized concentration and signal, i@tis the length of the collectionperiod, and C, is given by Equation B. This integral was evaluatedanalytically and fit to the data from each input function experiment
using the nonlinear regression package MINSQ (MicroMath, Inc., SaltLake City, UT). Because the equation contains six adjustable parameters, the accuracy to which any individual parameter can be estimated ispoor. However, the values of the parameters have no significance in
themselves; rather, it is important that the input concentration be wellrepresented by the function.
The regional blood flow map was obtained from nonlinear regressionof the intensity in each pixel as a function of time. With the arterial
input given as Equation B, Equation A becomes
1= a'[H(t —r,) —H(t —T2)] 1@ _ k — (1 —LT2 @1 (r2 r,)
1(1-c)kd+a'H(l—r2) L k—f
(1— c k 1—@@ @,_T2) @k(I- r2)+@ 1—@k(i T2))+k—g
+ @k(i-r2)@ @k(i—@,)]
1T2—@—T, 1
r2 —T1 k(r2 —r1)
(D)
where the only adjustable parameters were k = F/A and a' = aCmax. Firstthe background intensity in a preinfusion image was subtracted fromeach image. Then a cutoff was placed on the lower limit of signaldetection; an estimate of the image noise was obtained from an emptyfield in one of the images and only those pixels which had an average
(A) signal (at times beyond 2 mm) greater than 1.5 times the standarddeviation of the noise were analyzed. The value of flow for pixelswith signal below the cutoff for analysis was set to zero. This filter
prevented the program from fitting the equation to any pixel the signalof which was composed chiefly of noise. The remaining pixels were fitindividually to Equation D using a FORTRAN program incorporatingthe IMSL routine RNLIN. The flow for each pixel was estimated fromthe value for k obtained from the fit for that pixel and an estimate of thepartition coefficient. For these studies, the partition coefficient was
6011
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Table 1 Arterial inpulfunctionparametersParametersfor Equation B were obtained from least-squares regressionsofdata
from each experimental trial to Equation C. Mean values were used intheanalysisof the imaging data. Maximum and minimum values were used to gen
crate values for the input sensitivitysimulations.Parameter
Mean SD MinimumMaximumc
0.0796 0.014 0.05640.0947d0.887 0.019 0.8610.914I0.227 0.094 0.0900.390g0.00669 0.00071 0.005540.00745T,5.45 2.55 2.038.94T2
34.6 3.90 28.7 40.2
100 2(0) 300 400 500
2HNMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
assumed to be 0.9 (9). The boundary of the tissue was determined
manually from borders apparent on the 10-mm 2H image.It should be noted that integration of Equation D is not appropriate
for analyzing the image data. Whereas the spectroscopy experimentrepresents a sum of pulses over the collection period, the image represents a sum over both time and phase-encoding gradient. Since most ofthe image intensity is determined by signal obtained for a phase gradi
ent of zero (the midpoint of the collection period for the imagingsequence used in these experiments), each image represents approximately a single time point. This point has been confirmed with numerical simulation (data not shown).
Data from the imaging experiments are also reported using the meanflow and flow variance. Mean flow was calculated from the leastsquares regression of the averaged accumulation data. Variance of flowwas calculated from the flow distribution shown in the images and is
reported as a c.v.Ratio Images. One means of demonstrating any changes in local
blood flow from the sequential flow images is to calculate, for eachimaging volume, the ratio of the flow values. If there is no change in
flow with time, the ratio for each pixel will equal unity. If there is acoherent change throughout the tissue, a ratio map will still be homo
geneous, but each pixel will have a value other than unity. Ifthe patternof flow changes, there will be a range of ratios. These images emphasize
relative changes in flow and should be interpreted with caution. Thevariance of this distribution of flow ratios represents a measure of theextent of temporal changes in the flow distribution. Of course, anyuncertainty present in the individual pixel flow estimates also increasesthe variance ofthe flow ratio distribution. This baseline variance may bedetermined from the variance of the parameter obtained by leastsquares regression and simple error propagation calculations (18). Suchestimates were made separately for brain and tumor from the experimental data.
RESULTS
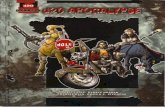
An accurate estimate of blood flow using tracers depends onthe determination of the arterial input function. Experimentalresults for the kinetics of the deuteron concentration in arterialblood following D2O infusion per the protocol described aboveare shown in Fig. 1A. During the infusion, the deuteron concentration rose rapidly to a peak and then decreased to a steadylevel. The data from all the trials were well approximated byEquation C; when the data were fitted to this equation, thecoefficients of variation for the estimated parameters were lessthan 20%, indicating a good fit to the data and relatively littlecross-correlation between parameters. The variation in the parameter estimates from one infusion to the next was greaterthan the parameter uncertainty between animals. Table 1 showsthe range and mean of the parameters obtained from the ninetrials. The arterial input function generated from Equation B
with mean parameters is shown by the heavy line in Fig. lB. Fora given flow rate the tissue accumulation curve can be calculatedfrom Equation D using the mean input parameters; the curvesgenerated for several flow rates are shown in Fig. lB. It is clearthat the shape of the accumulation function varies markedlywith flow rate. Fig. 1C shows the measured arterial concentration (integrated over 8-s periods) in three consecutive measurements in the same animal.
Some of the variability observed in arterial D20 kinetics mayarise from variable cardiovascular disturbances secondary to theD20 infusion. The rapid infusion of D20 into the jugular veincaused a brief drop of mean arterial pressure. This hypotensionbegan instantly and the pressure dropped 30—50mm Hg by theend of the 25—30-sinfusion. The pressure recovered rapidlywith a time constant of about 30 s. A simple simulation showsthat such a pressure drop would cause a flow of0.3 mi/mm .g to
A
Frequency
T@m (.)
C ‘.0
0.8
@ 0.6
@ 0.4
0.0
Time (s)
Fig. I. Arterial D20 concentration as a function of time. A, series of spectraobtained from the arterial input function experiments. The D2O infusion beganafter the third spectrum. B, simulated tissue accumulation curves obtained fromEquation D using the mean input parameters and a series of assumed flows(labeled in mi/mm .g). Heavy solid line, input function generated from EquationB with the mean parameter estimates given in Table 1. C, measured arterialconcentrations (integrated over 8-s periods) in three consecutive injections in thesame animal.
be underestimated by roughly 4% and a flow of 1.0 mI/mm •gtobe underestimated by roughly 10%.
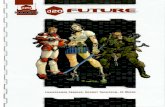
The effect of variations in the shape of the input functionswas explored with a simple simulation. The relative flow valueswithin each image are relatively insensitive to input functionvariations; however, the absolute flow estimates are dependenton precise knowledge ofthe arterial tracer concentration. Fromthe ranges of the parameters obtained from the fits of the cxperimental data, combinations of the parameters were chosenwhich yielded the inputs functions that (a) had the sharpestpeak and lowest steady-state level of deuterons [pulse-like
6012
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

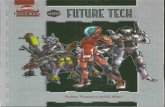
A proton image from a tissue-isolated R3230AC mammaryadenocarcinoma is shown in Fig. 3. The tumor is clearlyheterogeneous. However, it is difficult to give an interpretation to the intensity differences seen. They do not necessarilycorrespond to the areas of gross hypoperfusion or necrosis. The2H imaging of flow providesa more functional measureofheterogeneity.
A set of serial images showing the deuteron accumulation inone of the tissue-isolated tumors is shown in Fig. 4. Theseimages represent the raw data from which the calculatedflow images were made. Similar data were obtained from thebrain. These images demonstrate the signal-to-noise characteristic of the methods and imaging resolution used in thesestudies. This noise determines the uncertainty of the bloodflow estimates and contributes to apparent pixel-pixel heterogeneity in the flow image. It is thus important to obtain aquantitative estimate of the variation expected from imaging
0 100 200 300 400 500 600 noise alone.
Time (s) The flow images from rat brain reflect the relatively homo
geneous cerebral perfusion and provide an estimate of the nellability of the regional perfusion measurements. For reference,a proton image of a transverse section of the rat brain is shownin Fig. 5. A set of three brain flow images each made 30 mmapart in one rat is shown in Fig. 6 (top). Each image is accompanied by a histogram of the measured blood flows in Fig. 6(bottom). The flow is relatively homogeneous and stable in time.Some regions outside the brain, surrounding muscle and skin,demonstrate measurable but much slower flow. Within thebrain, some variations in flow may be discerned and appear toindicate a higher flow in the gray matter or meninges. The c.v.for the brain flows averaged 0.22. Only 23% of the variance inthis distribution can be accounted for by the uncertainty in theflow estimates (i.e., a c.v. of 0. 11). The global flow was calculated from a least-squares fit of the average raw image intensities. The global flow calculated from the 9 trials performed in 3rats ranged from 0.77 to 1.14 ml/ming with a mean of 0.96.These values are consistent with the range of brain blood flowsobtained with other tracer techniques (19). The variations inglobal flow with time in a single animal were within the variations expected from differences in arterial input. In order tobetter demonstrate potential flow shifts, ratio images were constructed. The ratio images and corresponding histograms forthe cerebral blood flow data depicted in Fig. 6 are shown in Fig.7. The temporal variability in the flow may be seen in the widthor standard deviation of the distribution of flow ratios. In brainthere were significant shifts in blood flow; the average c.v. of the
—1.0 0.0
2H-NMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
input, (Fig. 2A)1 and (b) the broadest peak and highest steadystate level of deuterons [step-like input, (Fig. 2A)J. These casesrepresent worst-case limits for variations in the input function.For each of these parameter sets and a series of assumed flowvalues, the output of a tracer accumulation experiment wasgenerated with Equation D. This output was then analyzed inthe same way as the experimentally determined tissue accumulation data from brain and tumor, using Equation D with themean input function parameter estimates. The deviations fromthe assumed flow are shown in Fig. 2B and they indicate themaximum errors in blood flow estimates that are likely to occurfrom variations in the arterial input. For the range of flowvalues expected in brain and tumors (0. 1 to 1.0 ml/min .g)the maximum error arising from variations in the input function is less than 40%. Because of this variability, one wouldideally measure both arterial and tissue tracer concentrationssimultaneously; however, this was not possible with the available hardware.
••@@‘:@ •@
@:‘@v-@.. •2 - •,.... -@,@- ,@- .e@
Fig. 3. ‘Himage of an excisedtissue-isolatedR3230AC mammaryadenocarcinoma. The image was obtained using a 180' pulse-refocused echo spin-warpimaging sequence. Echo time was 34 ms with a repetition time of 1 s and a slicethickness of 2 mm. The entire image frame represents a 2 cm x 2 cm field of view.
6013
1.0
0.8
0.6
0.4
0.2
0.0
250
200
150
100
50
0)
I.0I.I.
0I,aI.8)0.
0
—50
—100—2.0
Log[Flow (mug mm)]
Fig. 2. Sensitivityof flow estimates to uncertainty in the arterial input function. A, limits for the variation in the arterial input function. These curves weregenerated using parameters obtained by least-squares regression of the experimental data to Equation B. The heavy solid line was created from the meanarterial input parameters, while the thin lines were generated from the extremelimits of the parameters measured. All curves are normalized to make the peakconcentration 1. Experiments were simulated using these extreme limits of inputparameters for a wide range of flow values. These generated data were thenanalyzed using the mean arterial input to determine the flow that would beestimated for the imaging experiment. B, error in the flow estimate resulting atthese extremes of the input function.
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

2HNMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
BA
I
C 0
@ .@@@
Fig. 4. Serial 2H images of D20 accumulation. A—D,D20 levels in a tissue-isolated tumor at 0, 38, 93, and 203 s after the midpointof an i.v. bolus, respectively.
collection of venous outflow.4 The c.v. for the flows averaged0.72, 3-fold greater in the tumors than in brain (P < 0.001).Only 28% of the variance can be accounted for by uncertainty inthe flow estimates. The flow in the tumors not only varied inspace but also shifted with time. Three flow images from thesame tumor are shown in Fig. 9. This tumor had relative flowshifts in large (multipixel) regions. The upper left quarter of theimage has a flow of 0. 19 ±0.02 mI/mm . g in the first image; aflow of 0.28 ±0.04 in the second image made 30 mm later; anda flow of 0. 12 ±0.01 in the third. Several other tumors showedsimilar shifts. The spatial distribution of flow shifts are shownwith ratio images and corresponding histograms in Fig. 10. Asignificant fraction of the pixels had ratios of either zero orgreater than 1.5; this fraction arises from regions where flow atone time could not be differentiated from zero. The nonlinearcutoffused to identify these regions makes these regions appearas large, isolated peaks in the ratio histograms. When thosepixels with ratios of zero or infinity are excluded, the averagec.v. of these ratios was 1.4 (more than 4-fold that observed forbrain flow ratios). Here only 12% of the variance can be accounted for by uncertainty in the flow estimates. Since ratios ofzero or infinity were excluded, 1.4 represents only the lowestestimate of the relative variance.
DISCUSSION
NMR imaging of deuteron accumulation following i.v. administration of D2O (coupled with a model for tissue-capillaryexchange and knowledge ofthe arterial D20 concentration) canprovide quantitative estimates of regional tumor blood flow.
4 R. K. Jam and B. Bartel, unpublished observations.
Fig. 5. ‘Himage of a transverse slice through rat brain. The image was obtamed in the same manner as that of the tumor image in Fig. 3 but with a 4-mmslice thickness. The entire image frame represents a 3.25 cm x 3.25 cm field ofview.
flow ratios was 0.3 1. Again only one-fourth of the variancecould be accounted for by uncertainty in the flow estimates.However, these shifts were small relative to those observed inthe tumors.
The flow images obtained from the tissue-isolated tumorsdemonstrate a marked spatial and temporal heterogeneity whencompared to brain. The flow images and corresponding histograms for three different tumors are shown in Fig. 8. The pattern and extent of the perfusion heterogeneity varied from onetumor to the next. Some tumors appeared to be largely homogeneous; others had large regions that were poorly perfused.The global blood flows and the variance of the blood flowdistribution for the tumors are given in Table 2. The averageglobal flow was 0.32 ml/g@min,in good agreement with previousmeasures of blood flow through these tumors obtained through
6014
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

. . I
0.5 .:.@ ,@ @, >5.s
@__ :S. S. 10 IS 5.5 ‘*5
2H-NMRIMAGINGOF HETEROGENEOUSTUMORBLOODFLOW
U
UU
a
a
I Is
I0
15
15
.:@ @5 ,:.@
“.5 (aug mIs)
Fig. 6. Three flow distribution images (lop) and histograms (bottom) obtained from a single rat brain at 30-mm intervals. The images are shown in order with the0—10-mmimage at the left. In the images, intensity is scaled linearly with the flow value; solid black pixels, flow of 0.0 ml/(min.g); solid white pixels, flow of 1.8ml/(min .g) or greater. In-plane resolution is I mm.
The method is relatively noninvasive and repeated measures inthe same subject are possible. The use of NMR spectroscopy tomonitor D2O has been shown to give proper estimates of theblood flow in such normal tissues as liver (8). The extension ofthis technique to imaging of relative blood flow (13, 20) yieldsinformation that is particularly valuable for the study of flowheterogeneity in solid tumors. With quantification of flow estimates the information allows one not only to distinguishchanges in flow within each tumor but also to better comparedifferent tumors. With the measured input function from theinfusion protocol used for these studies, flows ranging from0.01 to 5 ml/g . mm can be measured (with variable accuracy).With this method, the extent of both spatial and temporalheterogeneity in the tissue-isolated tumors (within the limitsimposed by spatial and temporal resolution) could be determined.
While the analysis of the raw accumulation data is simple inprinciple, in practice the analysis of the imaging experimentsmay become complex. The most straightforward means of ohtaming blood flow from accumulation data is least-squares fitting of the accumulation data to an equation determined fromthe input and a capillary-tissue exchange model. This fitting ismost reliable when the input concentration changes rapidlyrelative to the time constant for tissue tracer uptake. For thisreason a rapid i.v. bolus was chosen for the D20 delivery. Thearterial input function after i.v. bolus is complex and must bemeasured when one desires to quantify flow. Ideally, one wouldmeasure the input function and tissue accumulation simultaneously for each flow evaluation. With a well-mixed one-compartment model for tissue, only two parameters, the uptaketime constant and the steady-state signal intensity, are determined by the least-squares regression. In imaging experiments,one could assume that the steady-state intensity is uniform
throughout the organ of interest and fit only for the uptakeconstant. However, one can account for the effects of suchfactors as magnetic field inhomogeneity or partial filling byfitting for both parameters in each pixel. The uptake of thetracer is then scaled by the steady-state level.
The flow rates obtained from any tracer method are dependent upon the model used to describe tissue-capillary exchangeand relate tracer accumulation to blood flow. The most common model is the well-mixed compartment where tissue tracerconcentration is uniform and in equilibrium with the capillaryconcentration at all times. In order to approach this ideal, it isnecessary to use small tracers, the fast diffusion ofwhich allowsthem to distribute rapidly. In fact, models based on such assumptions are inadequate if the characteristic time for diffusion out of the vessels is not significantly less than the vesseltransit time (21). These assumptions have not been directlyevaluated in tumors. However, it is possible to gain a roughappreciation for the diffusion limitations by comparing the capillary transit time (capillary lengthdividedby velocity)andthecharacteristic time of diffusion (the square of one-half of theintercapillary distance divided by the diffusion coefficient).With morphological data obtained from casting studies of thesetumors (22) and a flow of0.5 mi/mm •g,the estimated capillarytransit time is 5 s; if one assumes a diffusion coefficient of 1 x10-s cm2/s, the diffusion time is 0.6 s. In brain, experimentaltransit time studies (23) and morphological data (24) yield acapillary transit time of 0.3—0.6s and a diffusion time of 0.2 s,respectively. Tracer studies also indicate that water may experience diffusion limitations in brain (25). It therefore appearsunlikely that diffusion limitations have much effect on the flowestimates in tumor but may cause some underestimation of flowin brain.
6015
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

40
a
“ow(mug mis)
@@JOO.* . . . I@ >@:@
Lc@ftisw
40a
a
aa
IS
r fl..fl..fl00 55 15 15 5.055 I, IS 5.0 ‘*5 , 5.1
2H-NMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
Fig. 7. Ratio images (top) and histograms(bottom) for the brain images of Fig. 6. Eachpixel represents the ratio of flow values fromthe corresponding pixel in two of the flow images. The image at the left represents the ratiosof the first two images in Fig. 6; the image atright represents the ratios of the second twoimages. The image intensity is scaled linearlywith the ratio; solid black pixels, flow ratio of0.0; solid white pixels, flow ratio of 2.0 orgreater.
5, K
Lo@(flow R@
U@U
a
a
I
Fig. 8. Images (top) and histograms (bottom) of blood flow in three tissue-isolated tumors. Intensity is scaled linearly with the flow value; solid black pixels, flow of0.0 ml/(min g); solid white pixels, flow of 1.2 ml/(min g) or greater. In-plane resolution is I mm
The potential heterogeneity in blood flow makes the tumors measurement of flow in brain was used to explore the reliabilitya poor choice of tissue for any attempt to determine the preci- of 2H imaging of deutenium accumulation and the analyticsion or accuracy of a perfusion measurement. An organ with scheme used to convert this information to blood flow. Themore reproducible, well-defined flow is required. Here, the values for global flow measured in this study are within the
6016
@UIIIIUI
IIUU UI
U UI@ UI IIIU UI UI
U UII@ IUIUI•
III U UUI U UI U rIIIM
U•U U U
UI Ut@@• U
UUUU UU
U UUUU U—UUU U U
U UU@ UU
U
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Table 2 GlobaJflow and coefficient of variation fromtissue-isolatedtumorsandbrainThe
globalflowwasobtainedfrom a fit ofthe summedimagedata toEquationD.The coefficientof variation wasobtained from the distributionof flowsintheflow
image. The values shown are the average of all measurements foreachtumor.Averagetumorandbrainvalues(±SDof the flowor c.v.fromdifferenttumors/brains)
are shown forcomparison.Global
blood flow Coefficient ofvariationTissue(ml/g mm) of flowdistributionTumor
V 0.250.47TumorW 0.370.68TumorX 0.300.51TumorY 0.490.62TumorB
0.111.29TumorD 0.350.72TumorL 0.270.78TumorM 0.440.71All
tumor 0.32 ±0.12 0.72 ±0.25Brain
0.96 0.22 ±0.07
.L
2H-NMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
similar measures made in other tumor models using positronemission tomography, radioactive tracers, thermal dilution, anddyes (26—29).The use of the tissue-isolated tumor as an experimental model is complicated by such heterogeneity. When oneobserves a change in global behavior, it is not possible to determine from input/output alone whether this change represents a change in flow distribution, a change in the behavior ofall cells, a change in a subpopulation of cells, or a shift in therelative size of different cell populations. However, the flowheterogeneity, which probably varies with cell line and tumorage or size, is qualitatively similar to that observed in manyhuman tumors (30), perhaps enhancing the value of these tumors as a model in studies of cancer therapy.
The presence of temporal variations in flow adds anotherdimension of complexity to tumor perfusion. There appear tobe significant fluctuations in flow on a time scale of 30 mm orless. These shifts are demonstrated from a calculation of theratio of flows in sequential images. Any changes which occurmore rapidly cannot be detected by the current experiments; theflow estimates represent a complex temporal average over anysuch fluctuations. The flow shifts occur on a scale large enoughto be detected with 2H imaging in single pixels and in multipixelregions. The measurements represent confirmation of a phenomenon seen during microscopy of window chamber preparations (31) and demonstrated in subcutaneous tumors using twofluorescent dyes, injected 20 mm apart (14). The 2H-NMRimaging technique used here has lower resolution than thesetechniques but makes it possible to obtain repeated measurements in the same tumor and suggests that the microscopicchanges are associated with changes at macroscopic levels.
Both spatial and temporal heterogeneities in blood flow haveimportant consequences for the design and interpretation ofexperiments in tumor pathophysiology. Global blood flow or
range of flows obtained from other methods (19). The varianceof flow within each brain was relatively small, with a c.v. of22%. If one assumes that the brain is homogeneously perfused,this variance represents the noise arising from random error oftechnique alone. Of course, brain perfusion is not homogeneous; therefore, this variance serves as an upper bound estimate of the dispersion that may arise from random error.
There are marked spatial variations of blood flow in thesetissue-isolated tumors. The c.v. of the flows in the tumors was72%, significantly greater than that observed in brain. It ispossible that some of the heterogeneity is induced by the transient hypoperfusion observed with D2O infusion; however, inorder for such an effect to be significant it would have to extendwell beyond the period ofthe flow disturbance. The observationof heterogeneous blood flow in the tumor is consistent with
U
U •uI@IIUU U
UUI U
a
aIs
Iso se 1.0 IS 1.0 >*S
now (mi/mis g)
Fig. 9. Three flow distribution images (top) and histograms (bottom) obtained from a single tissue-isolated tumor at 30-mm intervals. The images are shown in order,with the 0—10-mmimage at the left. Scale and resolution are the same as in Fig. 8.
6017
UUUUU
UUUU UUU UU
U UUU
U
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

. . n n A@ . . . n . I
or
40
35
30
@1L@@@ @os@@@.‘ IL
LogIFlowlab)
2H-NMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
IFig. 10. Ratio images (top) and histograms
(bottom) for the tumor images of Fig. 9. Theimage at the left represents the ratios of thefirst two images in Fig. 9; the image at rightrepresents the ratios of second two images.Scale and resolution are the same as in Fig. 7.
40
35
30
I
I10
so
III
[email protected],isLo@ @OWRabD)
perfusion have often been measured in experiments concernedwith the response oftumors to metabolite delivery or anticancertherapy. The methods available have forced researchers to relyupon an estimate of the global blood flow obtained at onemoment in time, using these data to correlate flow and anothermeasurement over a large number of animals. The correlationthus obtained is often poor, despite other evidence that flow hasa profound effect on that variable. One example is the relationship between flow and the energy status determined by 31P-NMR (32, 33). Another is the difficulty experienced relatingthe spatial distributions of a series of small metabolites on conrelating global measurements of blood flow with other biochemical or physical parameters (5). It is possible that an cxamination of not only global flow but also spatial and temporalvariation in flow might prove fruitful. It is possible that flowfluctuations on these short time and length scales are as important as the average flow rate in determining the behavior ofneoplastic cells in solid tumors.
The availability of such methods as 2H-NMR imaging nowmakes it possible to account for spatial and temporal variationsof perfusion. The quantitative assessment of regional bloodflow is of great importance in the understanding of both basalmetabolism and the response oftumors to therapy. The methoddescribed here offers a noninvasive means of providing thisinformation and thus might be extended to the study of humantumors. In humans, the arterial input function could be measured with each infusion from direct sampling or by monitoring2H intensity in major arterieswithin an image.In clinical nesearch, the combination of ‘H-NMR imaging (for structuraldetail and some discrimination of tumor from normal tissue)and 2H-NMR flow imaging would allow one to explore therelationship between tumor progression and flow changes, toevaluate differences between tumor types, and to study the effect of cancer therapy. The availability of noninvasive, spatially
discriminating techniques for flow measurement make suchstudies possible. The information thus obtained has importantpotential in clinical assessment of tumor type, tailoring of cancer therapy, and monitoring of response to therapy.
ACKNOWLEDGMENTS
We thank Dr. Paul Okunieff for his helpful comments and CarolLyons for her editorial assistance.
REFERENCES
1. Jam, R. K. Determinants of tumor blood flow: a review. Cancer Res., 48:2641—2658,1988.
2. Jam, R. K., and Ward-Hartley, K. Tumor blood flow—characterization, modifications, and role in hyperthermia. IEEE Trans. Sonics Ultrasonics, SU-31:504—526,1984.
3. Jam, R. K. Delivery of novel therapeutic agents in tumors: physiologicalbarriers and strategies. J. NatI. Cancer Inst., 81: 570—576,1989.
4. Shapot, V. S. Biochemical aspects of tumour growth. Moscow: MIR Publishers, 1980.
5. Vaupel, P., and Jam, R. K (eds.). Tumor blood flow and metabolic microenvironment: characterization and implications for therapy. New York: FischerPublications, 1991.
6. Coleman,C.N.Hypoxiaintumors:a paradigmfortheapproachtobiochemical and physiologic heterogeneity. J. Natl. Cancer Inst., 80: 310—317,1988.
7. Neil, J. J. The use offreely diffusible, NMR-detectable tracers for measuringorgan perfusion. Conc. Magn. Reson., 3: 1—12,1991.
8. Ackerman, J. J. H., Ewy, C. S., Becker, N. N., and Shalwitz, R. A. Deuteriumnuclear magnetic resonance measurements ofblood flow and tissue perfusionemploying 2H20 as a freely diffusible tracer. Proc. Natl. Aced. Sci. USA, 84:4099—4102,1987.
9. Kim,S-G.,and Ackerman,J. J. H. Quantitativedeterminationof tumorblood flow and perfusion via deutenum nuclear magnetic resonance spectroscopy in mice. Cancer Res., 48: 3449—3453,1988.
10. LarcombeMcDouall,J. B., and Evelhoch,J. L. Deuteniumnuclear magneticresonance imaging of tracer distribution in D20 clearance measurements oftumor blood flow in mice. Cancer Res., 50: 363—369,1990.
I 1. Mattiello, J., and Evelhoch, J. L. Relative volume-averagemurine tumorbloodflowmeasurementviadeuteriumnuclear magneticresonancespectroscopy. Magn. Reson. Med., 18: 320—334,1991.
12. Okunieff, P., Lee, J., Itoh, M., and Vaupel, P. Measurements oftumor bloodflowusing intraperitoneal deuterium and 2H-NMR spectroscopy.Adv.Exp.
6018
1@ .1@
I
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

2H-NMR IMAGING OF HETEROGENEOUS TUMOR BLOOD FLOW
lax systems within the brain. Magn. Reson. Med., 19: 217—220,1991.24. Pawlik, G., Rackl, A., and Bing, R. Quantitative capillary topography and
blood flow in the cerebral cortex of cats: an in vivo microscopic study. BrainRes., 208: 35—58,1981.
25. Larsoii K. B., Markham, J., and Raichle, M. Tracer-kinetic models formeasuring cerebral blood flow using externally detected radiotracers. J.Cereb. Blood Flow Metab., 7: 443—463,1987.
26. Lammertsma, A. A. Positron emission tomography and in vivo measurements of tumour perfusion and oxygen utilisation. Cancer Metastasis Rev., 6:521—539,1987.
27. Blasberg, R. G., Kobayashi, T., Patlak, C. S., Shinohara, M., Miyoaka, M.,Rice, J. M., and Shapiro, W. R. Regional Blood Flow, Capillary Permeability, and Glucose Utilization in Two Brain Tumor Models: Preliminary Observations and Pharmacokinetic Implications. Cancer Treat. Rep., 65 (Suppl.2):3—12,1981.
28. Gullino, P. M., Jam, R. K., and Grantham, F. H. Temperature gradients andlocal perfusion in a mammary carcinoma. J. Natl. Cancer Inst., 68: 5 19—533,1982.
29. Goldacre, R. J., and Sylven, B. On the access of blood-borne dyes to varioustumour regions. Br. J. Cancer, 16: 306-321, 1962.
30. Vaupel, P., Kallinowski, F., and Okunieff, P. Blood flow, oxygen and nutrientsupply, and metabolic microenvironment of human tumors. Cancer Res., 49:6449—6465,1989.
31. Intaglietta, M., Myers, R. R., Gross, J. F., and Reinhold, H. S. Dynamics ofmicrovascular flow in implanted mouse mammary tumours. BibI. Anat., 15:273—276,1977.
32. Evelhoch, J. L., Sapareto, S. A., Nussbaum, G. H., and Ackerman, J. J. H.Correlations between “PNMR spectroscopy and 150 perfusion measurements in the RIF-l munne tumor in vivo. Radiat. Res., 106: 122—131,1986.
33. Steen, R. G., and Graham, M. M. @‘Pmagnetic resonance spectroscopy issensitive to tumor hypoxia: perfusion and oxygenation of rat 9L gliosarcoma
after treatment with BCNU. NMR Biomed., 4: 117—124,1991.
Med. Biol., in press, 1992.13. Evelhoch, J. L., Larcombe McDouall, J. B., Mattiello, J., and Simpson, N.E.
Measurement of relative regional tumor blood flow in mice by deutçriumNMR imaging. Magn. Reson. Med., 24: 42—52,1992.
14. Trotter, M. J., Chaplin, D. J., Durand, R. E., and Olive, P. L. The use offluorescent probes to identify regions of transient perfusion in murine tumors. mt. J. Radiat. Oncol. Biol. Phys., 16: 931—934,1989.
15. Gullino, P. M. Techniques for the study of tumor physiopathology. In: H.Busch (ed.), Methods in Cancer Research, pp. 45—91.New York: AcademicPress, 1970.
16. Sevick, E. M., and Jam, R. K. Blood flow and venous pH of tissue-isolatedWalker 256 carcinoma during hyperglycemia.Cancer Res., 48: 1201—1207,1988.
17. Kety, S. S. The theory and applications of the exchange of inert gases to thelungs and tissues. Pharmacol. Rev., 3: 1—41,1951.
18. Meyer, S. L. Data Analysis for Scientists and Engineers. New York: JohnWiley and Sons, 1975.
19. Detre, J. A., Eskey, C. J. and Koretsky, A. P. Measurement ofcerebral bloodflow in rat brain by ‘9F-NMRdetection of tnifluoromethane washout. Magn.Reson. Med., 15: 45—57,1990.
20. Larcombe McDouall, J. B., Mattiello, J., McCoy, C. L., Simpson, N. E.,Seyedsadr, M. and Evelhoch, J. L. Size dependence ofregional blood flow inmurine tumours using deuterium magnetic resonance imaging. Int. J. Radiat.Biol.,60:109—113,1991.
21. Bassingthwaighte, J. B., and Goresky, C. A. Modeling in the analysis ofsolute and water exchange in the microvasculature. In: E. M. Renkin and C.C. Michel(ed.),Handbookof Physiology,Sect.2, pp. 549—626.Bethesda,MD:AmericanPhysiologicalSociety,1984.
22. Less, J. R., Skalak, T. C., Sevick, E. M., and Jam, R. K. Microvasculararchitecture in a mammary carcinoma: branching patterns and vessel dimensions. Cancer Res., 51: 265—273,1991.
23. Fenstermacher, J., Nakata, H., Tajima, A., Lin, S-Z., Otsuka, T., Acuff, V.,Wei, L., and Bereczki,D. Functional variations in parenchymalmicrovascu
6019
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1992;52:6010-6019. Cancer Res Clifford J. Eskey, Alan P. Koretsky, Michael M. Domach, et al. Mammary AdenocarcinomaSpatial and Temporal Heterogeneity in a Tissue-isolated H-Nuclear Magnetic Resonance Imaging of Tumor Blood Flow:2
Updated version
http://cancerres.aacrjournals.org/content/52/21/6010
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
on May 28, 2017. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from