
2/7/2012 - Lancaster General Health · 2/7/2012 1 The New Era of ... –Atrial tumor resection...
13
2/7/2012 1 The New Era of Minimally Invasive Cardiac Surgery Jeffrey T. Cope, MD Division of Cardiothoracic Surgery Lancaster General Hospital February 23, 2012 10:30-11:30 AM Traditional Approach to Cardiac Surgery •Full median sternotomy •Cardiopulmonary bypass •Arrested heart Traditional Approach to Cardiac Surgery Advantages of Traditional Approach Sternotomy: •Has withstood the test of time •All surgeons comfortable with it •Provides full access to: –Pericardium –All chambers of the heart and great vessels –All 4 valves –All coronary arteries Advantages of Traditional Approach On-pump, arrested heart: •Provides ideal operating conditions •Allows surgical team full control of circulation and oxygenation Disadvantages of Traditional Approach Sternotomy: •Pain •Increased blood loss •Prolonged healing time (2-3 months) •Sternal wound complications •Cosmetically unappealing
Transcript of 2/7/2012 - Lancaster General Health · 2/7/2012 1 The New Era of ... –Atrial tumor resection...

2/7/2012
1
The New Era of Minimally Invasive
Cardiac Surgery
Jeffrey T. Cope, MD
Division of Cardiothoracic Surgery
Lancaster General Hospital
February 23, 2012
10:30-11:30 AM
Traditional Approach to Cardiac Surgery
•Full median sternotomy
•Cardiopulmonary bypass
•Arrested heart
Traditional Approach to Cardiac Surgery Advantages of Traditional Approach
Sternotomy:
•Has withstood the test of time
•All surgeons comfortable with it
•Provides full access to:
–Pericardium
–All chambers of the heart and great vessels
–All 4 valves
–All coronary arteries
Advantages of Traditional Approach
On-pump, arrested heart:
•Provides ideal operating conditions
•Allows surgical team full control of circulation
and oxygenation
Disadvantages of Traditional Approach
Sternotomy:
•Pain
•Increased blood loss
•Prolonged healing time (2-3 months)
•Sternal wound complications
•Cosmetically unappealing

2/7/2012
2
Disadvantages of Traditional Approach Disadvantages of Traditional Approach
On-pump, arrested heart:
•Stroke risk
•Injury to other organs (kidneys, lungs, etc.)
•Ventricular dysfunction
•Bleeding/blood transfusions
Minimally Invasive ApproachesAdvantages of
Minimally Invasive Approach
•Better cosmesis
•Less pain
•Less blood loss
•More rapid healing (2-4 weeks)
•Minimization/avoidance of sternal wound
complications
•Avoid deleterious effects of CPB/arrested
heart
Advantages of
Minimally Invasive Approach
•Reduced postop morbidity
•Shortened postop ICU and total hospital
length of stay
•More cost-effective (?)
Disadvantages of
Minimally Invasive Approach
•Technically very demanding
–Not appropriate for every surgical team
•Expensive technology
•Not appropriate for every patient

2/7/2012
3
Minimally Invasive Cardiac Surgery
at Lancaster General Hospital
•Via right anterolateral minithoracotomy:
–Mitral valve surgery
–Tricuspid valve surgery
–Atrial septal defect repair
–Atrial tumor resection (e.g. myxoma)
•Aortic valve replacement via upper
ministernotomy
Minimally Invasive Cardiac Surgery
at Lancaster General Hospital
•da Vinci robotic-assisted minimally invasive
direct coronary artery bypass (MIDCAB)
•Hybrid coronary revascularization
•Transcatheter aortic valve implantation
(TAVI)
Minimally Invasive Mitral Valve Surgery
•Approach via 6-8 cm right anterior minithoracotomy
in 4th intercostal space
•Venous cannulation for CPB via right common
femoral vein
•Arterial cannulation via right common femoral
artery or ascending aorta
•Mitral valve repair or replacement performed using
specialized equipment and long-shafted
instruments
Minimally Invasive Mitral Valve Surgery
Contraindications:
•Morbid obesity
•Previous right lung surgery or infection
•Severe LV dysfunction
•Other significant valve or coronary disease
Minimally Invasive Mitral Valve Surgery Minimally Invasive Mitral Valve Surgery

2/7/2012
4
Minimally Invasive Mitral Valve Surgery Minimally Invasive Mitral Valve Surgery
Minimally Invasive Mitral Valve Surgery Minimally Invasive Mitral Valve Surgery
Minimally Invasive Mitral Valve Surgery Minimally Invasive Mitral Valve Surgery

2/7/2012
5
Minimally Invasive Mitral Valve Surgery Minimally Invasive Mitral Valve Surgery
Minimally Invasive
Aortic Valve Replacement
•Approach via 6-8 cm upper ministernotomy incision
•Standard central aortic and right atrial cannulation
•Provides direct access to ascending aorta and
aortic valve
•AVR performed using standard instrumentation
Minimally Invasive
Aortic Valve Replacement
Contraindications:
•Morbid obesity
•Severe LV dysfunction
•Significant other valve or coronary disease
Minimally Invasive AVR
Partial upper ministernotomy:
Minimally Invasive AVR
2/7/2012
6
Minimally Invasive AVR Minimally Invasive AVR
Minimally Invasive AVR Minimally Invasive AVR
Minimally Invasive AVR Minimally Invasive AVR

2/7/2012
7
da Vinci Robot-Assisted MIDCAB
Who is a candidate?
•A patient who needs bypass to LAD (not a small,
calcified, or intramyocardial vessel)
•EF > 30%
•No significant lung disease or pulmonary HTN
•No previous left chest surgery
•Not morbidly obese
•Not in the midst of an acute MI
da Vinci Robot-Assisted MIDCAB
The epitome of minimal invasiveness:
•No sternotomy
•No cardiopulmonary bypass
da Vinci Robot-Assisted MIDCAB
Disadvantages:
•Not everyone is a candidate
•Steep learning curve
•Anastomosis more difficult than sternotomy
approach
•Operation itself more costly than nonrobotic
approach (but lower LOS and complication rates)
da Vinci Robot-Assisted MIDCAB
da Vinci Robot-Assisted MIDCAB da Vinci Robot-Assisted MIDCAB

2/7/2012
8
da Vinci Robot-Assisted MIDCAB da Vinci Robot-Assisted MIDCAB
da Vinci Robot-Assisted MIDCAB da Vinci Robot-Assisted MIDCAB
da Vinci Robot-Assisted MIDCAB da Vinci Robot-Assisted MIDCAB
2/7/2012
9
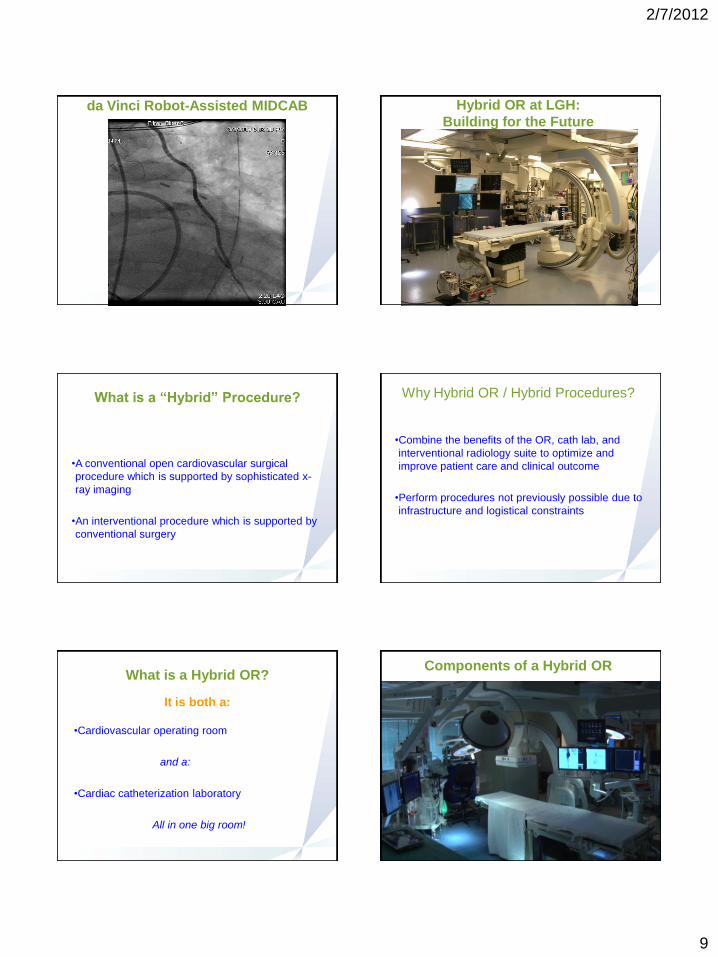
da Vinci Robot-Assisted MIDCAB Hybrid OR at LGH:
Building for the Future
What is a “Hybrid” Procedure?
•A conventional open cardiovascular surgical
procedure which is supported by sophisticated x-
ray imaging
•An interventional procedure which is supported by
conventional surgery
Why Hybrid OR / Hybrid Procedures?
•Combine the benefits of the OR, cath lab, and
interventional radiology suite to optimize and
improve patient care and clinical outcome
•Perform procedures not previously possible due to
infrastructure and logistical constraints
What is a Hybrid OR?
It is both a:
•Cardiovascular operating room
and a:
•Cardiac catheterization laboratory
All in one big room!
Components of a Hybrid OR
2/7/2012
10
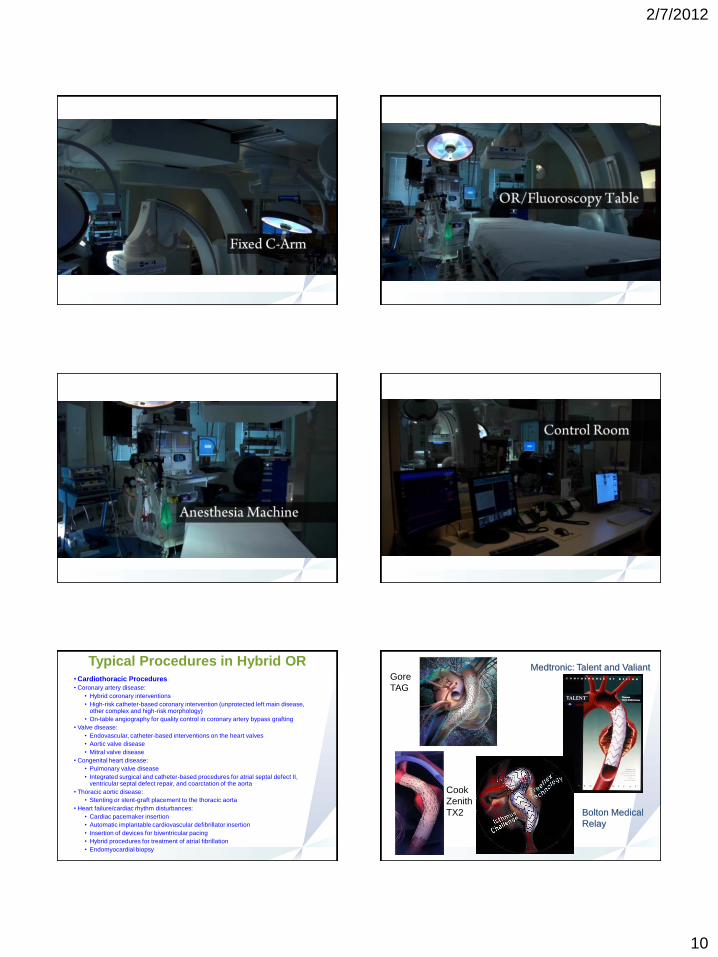
Typical Procedures in Hybrid OR• Cardiothoracic Procedures
• Coronary artery disease:
• Hybrid coronary interventions
• High-risk catheter-based coronary intervention (unprotected left main disease, other complex and high-risk morphology)
• On-table angiography for quality control in coronary artery bypass grafting
• Valve disease:
• Endovascular, catheter-based interventions on the heart valves
• Aortic valve disease
• Mitral valve disease
• Congenital heart disease:
• Pulmonary valve disease
• Integrated surgical and catheter-based procedures for atrial septal defect II, ventricular septal defect repair, and coarctation of the aorta
• Thoracic aortic disease:
• Stenting or stent-graft placement to the thoracic aorta
• Heart failure/cardiac rhythm disturbances:
• Cardiac pacemaker insertion
• Automatic implantable cardiovascular defibrillator insertion
• Insertion of devices for biventricular pacing
• Hybrid procedures for treatment of atrial fibrillation
• Endomyocardial biopsy
Gore
TAG
Cook
Zenith
TX2
Medtronic: Talent and Valiant
Bolton Medical
Relay

2/7/2012
11
Hybrid Coronary
RevascularizationConcomitant Hybrid Minimally
Invasive AVR/PCI
By 2030, 20% of the U.S. Population Will
Be Over Age 65
Percentage of Populaton By Age Cohort
17%14%11%11%3%2%2%2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2000 2010 2020 2030
85+
65-84
45-64
20-44
5-19
0-4
Source: U.S. Census Bureau, 2004, "U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin," <http://www.census.gov/ipc/www/usinterimproj/>
Many Patients with Severe AS Are Not
Surgically Treated
40
6859
60
3241
0%
25%
50%
75%
100%
Charlson
2006
Iung 2003 Bouma 1999
Untreated
Surgically Treated
Severe AS*
Percent of Patients Treated
* EuroHeart Survey: Single Valve Disease (AS, MR)
1. Charlson E et al. Decision-making and outcomes in severe symptomatic aortic stenosis. J Heart Valve Dis2006;15:312-321
2. Iung B et al. A prospective survey of patients with valvular heart disease in Europe:
The Euro Heart Survey on Valvular Heart Disease. European Heart Journal 2003;24:1231-1243
3. Bouma B J et al. To operate or not on elderly patients with aortic stenosis:
the decision and its consequences. Heart 1999;82:143-148
EUUS
Rationale For Transcatheter Therapy
• High risk / Inoperable
• Age
• Depressed LVEF
• Stroke
• CRI
• Pulmonary insufficiency
• The frailty concept
• Quality of life
Transfemoral
Transapical
Edwards SapienTM Valve
Transcatheter Aortic Valve Implantation
(TAVI)
Transfemoral

2/7/2012
12
Other Routes of Access
• Transaortic
• Transsubclavian
Transapical
Exposure
Transapical Deployment Completion Angiogram
How to build a Hybrid OR?
•Planning!
•Planning!
•Planning!
•Design collaboration between LGH administrators,
cardiac surgeons, anesthesiologists, interventional
cardiologists, perfusionists, and OR/cath lab staff.
•Nothing like this has ever been built at LGH
before!

2/7/2012
13
Potential Impact of Hybrid OR at LGH
•Improve patient outcomes
•Foster sincere multidisciplinary collaboration
•Increase patient volumes
•Regional referral center
Questions?


















