23204995
35
Diagnostic In-Training Exam 2006 1 Section IX – Gastrointestinal Radiology 213. You are shown a contrast-enhanced CT of a 62-year-old man with left lower quadrant abdominal pain (Figure 1). What is the MOST LIKELY diagnosis? A. Omental infarct B. Diverticulitis C. Mesenteric panniculitis D. Epiploic appendagitis Section IX – Gastrointestinal Radiology Figure 1
-
Upload
radgirl -
Category
Health & Medicine
-
view
1.149 -
download
0
description
ACR Inservice Recall
Transcript of 23204995

Diagnostic In-Training Exam 2006 1
Section IX – Gastrointestinal Radiology
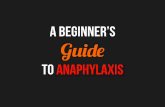
213. You are shown a contrast-enhanced CT of a 62-year-old man with left lower quadrant abdominalpain (Figure 1). What is the MOST LIKELY diagnosis?
A. Omental infarct
B. Diverticulitis
C. Mesenteric panniculitis
D. Epiploic appendagitis
Section IX – Gastrointestinal Radiology
Figure 1

Question #213
Rationales:
A. Incorrect. Omental infarct is usually right sided, presenting as a large fat-containing mass centeredin the omentum. It may or may not be adjacent to the colon. It is typically larger than the fatty massof epiploic appendagitis and is less well defined.
B. Incorrect. Diverticulitis demonstrates marked colonic wall thickening in addition to the surroundinginflammatory changes in the fat. It occurs more commonly in the sigmoid colon.
C. Incorrect. Mesenteric panniculitis is an idiopathic, chronic, nonspecific process usually presentingas a solitary mass of heterogeneous fat at the root of the jejunal mesentery. There are often shottylymph nodes.
D. Correct. Epiploic appendagitis presents with a paracolonic fat-containing mass with well circum-scribed hyperattenuating rim (“ring sign”) and central engorged/thrombosed vessel. It is locatedadjacent to the left colon in most cases and is typically smaller, more round, and better defined thanomental infarction.
American College of Radiology2
Section IX – Gastrointestinal Radiology

American College of Radiology3
Section IX – Gastrointestinal RadiologySection IX – Gastrointestinal Radiology
Figure 2A
Figure 2B

Diagnostic In-Training Exam 2006 4
Section IX – Gastrointestinal Radiology
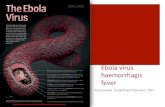
214. You are shown T2-weighted and pre- and post-contrast T1-weighted arterial and portal venousphase MR images (Figures 2A through 2D). Concerning the hepatic lesion, which one is TRUE?
A. It is the most common benign hepatic neoplasm.
B. It may increase in size with use of oral contraceptives.
C. It is associated with cirrhosis and viral hepatitis.
D. Predisposing conditions include primary sclerosing cholangitis.
Section IX – Gastrointestinal Radiology
Figure 2C
Figure 2D

Question #214
Rationales:
A. Incorrect. The images demonstrate typical findings of focal nodular hyperplasia, the second mostcommon benign hepatic neoplasm. Hemangioma is the most common.
B. Correct.
C. Incorrect. Hepatocellular carcinoma typically occurs in the setting of cirrhosis or chronic hepatitis.
D. Incorrect. These are associated with intrahepatic cholangiocarcinoma.
American College of Radiology5
Section IX – Gastrointestinal Radiology

American College of Radiology6
Section IX – Gastrointestinal Radiology
215. You are shown a spot view of the distal ileum (Figure 3) from a small bowel series in a 48-year-old man. What is the MOST LIKELY diagnosis?
A. “Backwash ileitis” of ulcerative colitis
B. “Pipestem bowel” of strongyloides infection
C. Tuberculosis
D. Crohn’s ileitis
Section IX – Gastrointestinal Radiology
Figure 3

Question #215
Rationales:
A. Correct. The terminal ileum shows loss of mucosal folds and diffuse subtle nodularity with noulceration or stricture. The ileocecal valve is gaping, but the ileocecal angle is preserved. The cecumis normal contour and shows diffuse superficial ulceration. These findings are characteristic of back-wash ileitis of ulcerative colitis.
B. Incorrect. Strongyloides stercoralis infection is more common in the jejunum, with mucosal foldeffacement and areas of narrowing.
C. Incorrect. Tuberculosis of the ileum shows ulceration and hypertrophic changes. The mucosal foldsfirst thicken and then become effaced. Though the ileocecal valve is widely patent, this is usuallyaccompanied by loss of the ileocecal angle and shrinkage of the cecum (“coned cecum”).
D. Incorrect. Crohn’s disease involving this much ileum is unlikely to be this homogeneous. It is morelikely to show ulceration, more pronounced nodularity, stenosis, and eccentric bowel involvement.
Diagnostic In-Training Exam 2006 7
Section IX – Gastrointestinal Radiology

American College of Radiology8
Section IX – Gastrointestinal Radiology
216. You are shown a contrast-enhanced CT (Figure 4) of an elderly woman with chronic right upperquadrant pain. What is the MOST LIKELY diagnosis?
A. Acute calculous cholecystitis
B. Traumatic gallbladder rupture
C. Gallbladder carcinoma
D. Adenomyomatosis
Section IX – Gastrointestinal Radiology
Figure 4

Question #216
Rationales:
A. Incorrect. The CT scan demonstrates a gallstone with rim calcification in the gallbladder. There isabnormal gallbladder wall thickening. The gallbladder pathology is complicated by contiguousinvolvement of the adjacent hepatic parenchyma, but this appears more extensive than pericholecys-tic inflammatory changes. Acute calculous cholecystitis is a consideration in this case, but theabsence of fever and an elevated WBC makes this diagnosis unlikely.
B. Incorrect. Blunt abdominal trauma can cause gallbladder perforation or avulsion of the cystic duct.A traumatic perforation can result in either an intrahepatic or extrahepatic biloma. By CT, a bilomaappears as a homogeneous, low-density, thin-walled, round to oval to lobulated collection. Fig. 3does not show a discrete fluid collection typical of a biloma. In addition, no history of trauma isgiven.
C. Correct. Rationale: Gallbladder carcinoma is the most common cancer of the biliary tree. It is asso-ciated with cholelithiasis in 60 – 90% of cases. Gallbladder cancer is three times more common inwomen than in men, and it most often occurs in the eighth decade of life. Contiguous spread of neo-plasm into the adjacent liver is common. This usually obviates curative surgery. As a result, the five-year survival is only 3%.
D. Incorrect. Adenomyomatosis is a benign disorder of the gallbladder mucosa and muscular wall. Ithas two pathologic components that contribute to imaging findings. Intramural diverticula(Rokitansky-Aschoff sinuses) can appear as small hypoechoic spaces or can be filled with choles-terol crystals appearing as small echogenic foci with comet-tail acoustic artifact. Wall thickeningcan be circumferential (waist-like), diffuse, or focal. Focal adenomyomatosis usually occurs in thefundus and cannot be differentiated from a polypoid gallbladder carcinoma. However, because ade-nomyomatosis is benign, gallbladder wall disruption with contiguous invasion of the liver would notbe expected.
Diagnostic In-Training Exam 2006 9
Section IX – Gastrointestinal Radiology

American College of Radiology10
Section IX – Gastrointestinal Radiology
217. You are shown two images from an upper gastrointestinal examination (Figures 5A and 5B).What is the MOST LIKELY diagnosis?
A. Adenocarcinoma
B. Lymphoma
C. Marginal ulcer
D. Gastric remnant cancer
Section IX – Gastrointestinal Radiology
Figure 5A

Diagnostic In-Training Exam 2006 11
Section IX – Gastrointestinal RadiologySection IX – Gastrointestinal Radiology
Figure 5B

Question #217
Findings: There is a large benign ulcer in the efferent limb of the patient’s gastrojejunostomy.
Rationales:
A. Incorrect. This is a benign ulcer without any evidence of a malignant mass.
B. Incorrect. Lymphoma would typically have a large mass and/or enlarged distorted folds.
C. Correct. This is a classic benign appearing marginal ulcer post subtotal gastrectomy with a BillrothII anastomosis.
D. Incorrect. A gastric stump cancer occurs in the stomach, not in the jejunum.
American College of Radiology12
Section IX – Gastrointestinal Radiology

American College of Radiology13
Section IX – Gastrointestinal RadiologySection IX – Gastrointestinal Radiology
Figure 6A
Figure 6B

Diagnostic In-Training Exam 2006 14
Section IX – Gastrointestinal Radiology
218. You are shown a contrast-enhanced CT (Figures 6A through 6C) in a 46-year-old woman. What is the MOST LIKELY diagnosis?
A. Metastatic ovarian carcinoma
B. Post-traumatic splenosis
C. Polysplenia
D. Lymphoma
Section IX – Gastrointestinal Radiology
Figure 6C

Question #218
Findings: Multiple splenic masses in left upper quadrant, no intrahepatic inferior vena cava, and anenlarged azygous vein and hemiazygous vein.
Rationales:
A. Incorrect. The multiple masses could represent enhancing metastases but other findings make thediagnosis.
B. Incorrect. There are too many splenic masses for splenules.
C. Correct. Multiple splenic masses, no intrahepatic IVC and an enlarged azygous vein.
D. Incorrect. There are no enlarged lymph nodes.
American College of Radiology15
Section IX – Gastrointestinal Radiology

American College of Radiology16
Section IX – Gastrointestinal Radiology
219. Concerning gastric lymphoma, which one is TRUE?
A. Accounts for 25% of all gastrointestinal lymphomas
B. Vast majority are Hodgkin’s lymphoma
C. Low-grade MALT lymphomas usually present as large bulky masses on upper gastrointestinalbarium studies
D. Advanced gastric lymphoma is usually large and involves the body and antrum
Question #219
Rationales:
A. Incorrect. Lymphoma involves the stomach more frequently than any other portion of the gastroin-testinal tract and accounts for 50% of all gastrointestinal lymphomas.
B. Incorrect. Almost all gastric lymphomas are non-Hodgkin’s lymphoma of B-cell origin.
C. Incorrect. Low-grade MALT lymphomas usually present as varied sized, rounded nodules on doublecontrast barium studies.
D. Correct. Advanced lymphoma is a large bulky mass and most commonly involves the gastric bodyand antrum.
Section IX – Gastrointestinal Radiology

Diagnostic In-Training Exam 2006 17
Section IX – Gastrointestinal Radiology
220. Concerning gastrojejunostomy, which one of the following is TRUE?
A. A Billroth I is a gastrojejunostomy.
B. A gastric stapling procedure incorporates a Roux-en-Y loop.
C. Internal hernias occur in up to 5% of patients following gastric bypass for weight reduction.
D. There is no increased risk for gastric cancer following partial gastrectomy for benignpeptic ulcer disease.
Question #220
Rationales:
A. Incorrect. A Billroth I is an antrectomy with a gastroduodenostomy.
B. Incorrect. A gastric partitioning stapling does not use any type of gastro-jejunal anastomosis.
C. Correct. Internal hernias have been reported in up to 5% of post gastric bypass operations.
D. Incorrect. There is a 3 to 6 fold increased chance of developing gastric remnant adenocarcinoma 15to 20 years following surgery for benign peptic ulcer disease.
Section IX – Gastrointestinal Radiology

221. Concerning splenic trauma, which one is TRUE?
A. The spleen is injured in 35% of penetrating abdominal trauma.
B. The spleen is the second most common solid organ injured in blunt trauma.
C. Grading splenic trauma is a reliable way to predict whether a patient will need splenectomy.
D. Embolization techniques can be used to control splenic hemorrhage.
Question #221
Rationales:
A. Incorrect. The spleen is injured less than 10%.
B. Incorrect. The spleen is the most common solid organ injured.
C. Incorrect. CT and surgical grading systems are not reliable methods to predict conservative vs. sur-gical management.
D. Correct. Embolization techniques can be useful in controlling splenic hemorrhage and obviatingsplenectomy.
American College of Radiology18
Section IX – Gastrointestinal RadiologySection IX – Gastrointestinal Radiology

Diagnostic In-Training Exam 2006 19
Section IX – Gastrointestinal Radiology
222. Concerning double-contrast upper GI examination, which one is TRUE?
A. Flow technique is useful for evaluation of the stomach but not the duodenum.
B. Compression views of the duodenum are obtained in the supine position.
C. The left posterior oblique view provides a double contrast view of the duodenum.
D. A barium suspension of 25% W/V concentration is used.
Question #222
Rationales:
A. Incorrect. Flow technique is useful for evaluating superficial lesions on the dependent surface of thestomach and duodenum.
B. Incorrect. Compression views of the duodenum are typically obtained in the prone position.
C. Correct.
D. Incorrect. A barium suspension of 250% W/V concentration is used.
Section IX – Gastrointestinal Radiology

223. Concerning duodenal inflammatory disease, which one is TRUE?
A. Duodenocolic fistulas are likely to occur in primary duodenal Crohn’s disease.
B. Radiation doses of 500 rad to the duodenum may cause radiation duodenitis.
C. Mucosal fold thickening is often more severe in dialysis patients.
D. Duodenal caustic injury is more likely to occur with alkali ingestion than acid ingestion.
Question #223
Rationales:
A. Incorrect. Duodenocolic fistulas rarely occur in primary duodenal Crohn’s disease, but will occa-sionally occur in primary colonic Crohn’s disease.
B. Incorrect. The dose threshold for injury is 5000 rad.
C. Correct.
D. Incorrect. The opposite is true.
American College of Radiology20
Section IX – Gastrointestinal Radiology

224. Concerning abdominal multidetector CT (MDCT), the z-axis resolution MOST LIKELY increaseswith decreasing:
A. slice thickness
B. radiation dose
C. mAs (product of tube current and scan time)
D. image noise
Question #224
Rationales:
A. Correct. Spatial resolution in CT is dependent on the image matrix (FOV) in transaxial plane andslice thickness in z- direction. One of the driving force in MDCT is to obtain high spatial resolutionand this is achieved by scanning very thin slice thickness.
B. Incorrect. The radiation dose per slice in CT increases with decreasing slice thickness. This is donein order to maintain lower image noise.
C. Incorrect. Decreasing mAs yeilds higher image noise and could degrade spatial resolution
D. Incorrect. See correct answer.
Diagnostic In-Training Exam 2006 21
Section IX – Gastrointestinal Radiology

225. Concerning selective immunoglobulin A deficiency, which one is TRUE?
A. It is an uncommon immunodeficiency in adults.
B. The majority of persons with IgA deficiency will present with malabsorption.
C. It is not associated with celiac disease.
D. It carries an increased risk of malignancy.
Question #225
Rationales:
A. Incorrect. It is the most common immunodeficiency in adults, occurring in 1 in 700 persons.
B. Incorrect. Most are asymptomatic because of a compensatory rise in IgM production. The remain-der will be symptomatic and may respond favorably to a gluten-free diet.
C. Incorrect. It has been reported in 1 in 40 patients with celiac disease.
D. Correct. Malignant tumors are more common in patients with IgA deficiency and in patients withother immunodeficiencies.
American College of Radiology22
Section IX – Gastrointestinal Radiology

226. Concerning acute pancreatitis on a helical CT with dynamic bolus contrast enhancement, which finding is the BEST prognostic indicator of morbidity and mortality?
A. Size of the pancreas
B. Location and size of fluid collections
C. Presence of biliary obstruction
D. Pancreatic parenchymal enhancement
Question #226
Rationales:
A. Incorrect. While this is one of the indicators of the severity of acute pancreatitis, it is not the mostpredictive of M & M.
B. Incorrect. While this is one of the indicators of the severity of acute pancreatitis, it is not the mostpredictive of M & M.
C. Incorrect. While this is a complication of acute pancreatitis, it is not the most predictive of M & M.
D. Correct. There is general agreement that the development and extent of pancreatic necrosis are themost important indicators of disease severity. Necrosis is diagnosed when portions of the gland donot enhance.
Diagnostic In-Training Exam 2006 23
Section IX – Gastrointestinal Radiology

227. Concerning microcystic cystadenoma of the pancreas, which one is TRUE?
A. Fluid aspirated from the cyst will contain mucin.
B. They usually appear as a solid mass on ultrasound exam.
C. They should be resected because they are potentially malignant.
D. They rarely calcify.
Question #227
Rationales:
A. Incorrect. Aspirate yields low viscosity fluid. The cysts are lined by glycogen-containing cells.Macrocystic cystadenomas and cystadenocarcinomas have mucinous fluid.
B. Correct. They have this appearance because the small cysts are depicted only as acoustic interfaces.
C. Incorrect. They are benign. Macrocystic adenomas are potentially malignant.
D. Incorrect. Microcystic adenoma calcifies more than any other pancreatic tumor, with central calcifi-cations seen in about one-third by conventional radiographs.
American College of Radiology24
Section IX – Gastrointestinal Radiology

228. Concerning duodenal ulcers, which one is TRUE?
A. Free air is seen on conventional x-rays in up to 2/3 with perforation.
B. Duodenal peptic ulcers have a 5% chance of being malignant.
C. Multiple ulcers throughout the duodenum are most frequently associated with aspirin therapy.
D. Altered mucosal resistance is a major factor in the pathogenesis of duodenal peptic ulcers.
Question #228
Rationales:
A. Correct.
B. Incorrect. Gastric ulcers have a 5% chance of being malignant. In contrast, duodenal ulcers are vir-tually always benign.
C. Incorrect. Eighty-five percent of duodenal ulcers are solitary. Multiple ulcers in the postbulbar duo-denum should raise the possibility of Zollinger-Ellison syndrome. Chronic aspirin therapy is associ-ated with multiple gastric ulcers, seen in over 80% of these patients. It is not associated with duode-nal ulcers.
D. Incorrect. This is thought to be the major factor in gastric peptic ulcers. Duodenal ulcers are due toincreased peptic acid secretion.
Diagnostic In-Training Exam 2006 25
Section IX – Gastrointestinal Radiology

229. Concerning esophageal intramural pseudodiverticulosis, which one is TRUE?
A. Most commonly associated with Candida infection
B. Is a pre-malignant condition
C. Histologically represents dilated submucosal mucus glands
D. Outpouchings range in size from 1 cm to 2 cm
Question #229
Rationales:
A. Incorrect. Esophageal intramural pseudodiverticulosis (EIPD) is most commonly associated withreflux disease, but can be seen in Candidiasis, stricture, or esophageal carcinoma.
B. Incorrect.
C. Correct.
D. Incorrect. Outpouchings are usually on the order of 1 – 4 mm.
American College of Radiology26
Section IX – Gastrointestinal Radiology

230. What disease is associated with mesenteric desmoid tumors?
A. Gardner’s syndrome
B. Carcinoid tumors
C. Lymphoma
D. Peritoneal mesothelioma
Question #230
Rationales:
A. Correct. Desmoid tumors occur predominately in patients with Gardner’s syndrome who have hadabdominal surgery.
B. Incorrect. Carcinoid tumors may have a similar appearance to desmoid tumors but are not associat-ed with them.
C. Incorrect. No association.
D. Incorrect. No association.
Diagnostic In-Training Exam 2006 27
Section IX – Gastrointestinal Radiology

231. For an abdominal radiograph of a very large patient, which method is MOST LIKELY toimprove x-ray transmission?
A. Increasing mAs
B. Increasing the kVp
C. Increasing the tube-patient distance
D. Decreasing the tube-patient distance
Question #231
Rationales:
A. Incorrect. Increasing mAs will increase the number of photons generated and a proportionate num-ber of photons making it through the patient, however the photon energies and the fraction of inci-dent photons making it through the patient is unchanged.
B. Correct. Increasing kVp not only increases the number of x-ray photons generated, but also pro-duces higher energy photons with a maximum photon energy in keV equal to the kVp voltageacross the x-ray tube. The higher energy photons are more penetrating an a higher fraction of theincident photons will pass through the patient to the detector.
C. Incorrect. Increasing the tube-patient distance for a given technique does not change the penetratingability of the beam and will decrease the intensity of the beam.
D. Incorrect. Decreasing the tube-patient distance for a given technique will increase the incidentintensity of the beam, but will not change the penetrating ability of the beam. Note that decreasingthe tube-patient distance can significantly increase the entrance exposure to the patient.
American College of Radiology28
Section IX – Gastrointestinal Radiology

232. What is the MOST common malignant primary hepatic tumor?
A. Hepatocellular carcinoma
B. Lymphoma
C. Focal nodular hyperplasia
D. Intrahepatic cholangiocarcinoma
Question #232
Rationales:
A. Correct. HCC is the most common primary hepatic malignancy.
B. Incorrect. Hepatic lymphoma is uncommon and often undetectable by imaging.
C. Incorrect. FNH is benign.
D. Incorrect. Intrahepatic cholangiocarcinoma is the second most common primary hepatic malignancy.
Diagnostic In-Training Exam 2006 29
Section IX – Gastrointestinal Radiology

233. Concerning jaundice, which of the following is the MOST common etiology?
A. Choledocholithiasis
B. Pancreatitis
C. Benign stricture
D. Pancreatic carcinoma
Question #233
Rationales:
A. Incorrect. Choledocholithiasis accounts for 20% of cases of biliary obstruction.
B. Incorrect. Pancreatitis accounts for 8%.
C. Correct. Benign stricture form surgery, trauma, or biliary intervention accounts for almost half ofthe cases of biliary obstruction.
D. Incorrect. Pancreatic cancer does cause biliary obstruction, but less commonly than benign stricture.
American College of Radiology30
Section IX – Gastrointestinal Radiology

234. Concerning focal hepatic fatty sparing, what is its appearance on imaging studies?
A. Hypodense on CT relative to remaining liver
B. Hyperechoic on US relative to remaining liver
C. Demonstrates no signal loss on fat-suppressed MR images
D. Heterogeneous enhancement
Question #234
Rationales:
A. Incorrect. Areas of fatty sparing are hyperdense.
B. Incorrect. Fatty sparing is hypoechoic.
C. Correct.
D. Incorrect. Enhancement pattern is similar to the entire liver.
Diagnostic In-Training Exam 2006 31
Section IX – Gastrointestinal Radiology

235. Concerning ADULT intussusception, which one is TRUE?
A. Most surgical cases are caused by a structural lesion.
B. Carcinoid is the most common malignancy to cause a colocolic intussusception.
C. Symptomatic intussusception is more common in adults than children.
D. Asymptomatic small bowel intussusceptions commonly require surgery.
Question #235
Rationales:
A. Correct. In most adult cases, intussusception is associated with a bowel-related structural abnormality.
B. Incorrect. About 40% of adult intussusceptions are caused by malignant neoplasms. In the colon,primary adenocarcinoma is the most common.
C. Incorrect. Intussusception is most commonly a disease of childhood. Eighty-five to ninety-five per-cent of intussusceptions occur in children. Ninety-five percent of pediatric intussusceptions are idio-pathic. However, there is some evidence to suggest that viral infection causing Peyer patch enlarge-ment could be the underlying etiology in many cases.
D. Incorrect. A short-segment, relatively asymptomatic or incidental enteroenteric intussusception is fre-quently noted with abdominal CT and MR in adults. These are not associated with significant smallbowel obstruction, are usually self-limiting and transient, and do not require surgical intervention.
American College of Radiology32
Section IX – Gastrointestinal Radiology

236. Concerning Mirizzi syndrome, which one is TRUE?
A. Mirizzi syndrome is caused by gallstone impaction in the common hepatic duct.
B. Mirizzi syndrome is facilitated by an anatomic variant.
C. Cholecystocolonic fistula can complicate Mirizzi syndrome.
D. Bile duct injury at surgery is less likely in cases of Mirizzi syndrome.
Question #236
Rationales:
A. Incorrect. Mirizzi syndrome is a complication of longstanding cholelithiasis. It is caused byimpaction of a gallstone in the cystic duct or in the gallbladder neck. Extrinsic mass effect of thestone in the cystic duct on the common hepatic duct (CHD) or associated inflammatory changesextending to the CHD causes obstruction of the extrahepatic biliary tree
B. Correct. Mirizzi syndrome is defined as extrinsic obstruction of the common hepatic duct (CHD),usually caused by mass effect from a stone lodged in the adjacent cystic duct. CHD compression ismore likely in patients with low cystic duct insertions, because the cystic duct runs more paralleland in closer proximity to the CHD when this variant anatomy is present. Inflammatory changesextending from the cystic duct or gallbladder neck can also cause narrowing of the bile duct.
C. Incorrect. A cholecystocholedochal (not cholecystocolonic) fistula is a complication of Mirizzi syn-drome in 9 – 39% of cases. Fistula repair is required at the time of surgery. This requires eithercholedochoplasty or hepaticojejunostomy.
D. Incorrect. Because of adhesions, inflammation and variant bile duct anatomy, the surgical dissectionis more difficult in Mirizzi syndrome. Inadvertent injury to the biliary tree or hepatic artery is morelikely. Although laparoscopic cholecystectomy can be performed successfully in patients withMirizzi syndrome, more require open cholecystectomy than in cases of uncomplicated cholecystitis.
Diagnostic In-Training Exam 2006 33
Section IX – Gastrointestinal Radiology

237. Concerning intrahepatic cholangiocarcinoma, which one is TRUE?
A. It is usually hyperdense during the arterial phase of contrast enhancement.
B. It demonstrates washout during delayed CT imaging.
C. Postobstructive hepatic atrophy can be a prominent feature.
D. Extrahepatic spread of intrahepatic cholangiocarcinoma is uncommon.
Question #237
Rationales:
A. Incorrect. In the absence of primary sclerosing cholangitis, intrahepatic cholangiocarcinoma usuallypresents as a bulky mass. The lesion tends to be hypodense to background liver on noncontrast CTs.Following the dynamic administration of IV contrast, intrahepatic cholangiocarcinoma tends toremain relatively hypovascular (not hyperdense), particularly centrally.
B. Incorrect. Increased patchy enhancement can be observed during the portal venous phase. Retentionof contrast within the extracellular space of the central stoma at delayed CT imaging (5 – 10 min-utes) is relatively characteristic for these lesions.
C. Correct. High-grade obstruction from intrahepatic and hilar cholangiocarcinomas can cause atrophyof the hepatic parenchyma surrounding the pathologically dilated biliary tree. Capsular retractionoccurs in about 20% of cases. This retraction likely reflects the atrophy of a small volume of hepat-ic parenchyma beneath Glisson’s capsule. Surprisingly marked segmental and lobar atrophy canoccur when cholangiocarcinoma affects more central intrahepatic or hilar bile ducts.
D. Incorrect. The extrahepatic spread of peripheral, intrahepatic cholangiocarcinoma is not uncommon.In autopsy series, it is noted in about 50 – 70% of cases. Metastatic disease to regional celiac andleft gastric nodes occurs frequently. The prevalence of microscopic nodal disease with its tendencyto spread back to the liver makes the preoperative diagnosis of cholangiocarcinoma a contraindica-tion for hepatic transplantation.
American College of Radiology34
Section IX – Gastrointestinal Radiology

238. Concerning Crohn’s disease, which one is TRUE?
A. In the United States, ulcerative colitis is less common than Crohn’s disease.
B. Ulcerative colitis can affect any part of the alimentary tract.
C. Crohn’s disease is limited to the mucosa of the gastrointestinal tract.
D. Crohn’s disease does not contiguously affect the bowel.
Question #238
Rationales:
A. Incorrect. Among the general population of the United States, ulcerative colitis is more commonthan Crohn’s disease. The incidence of ulcerative colitis is 11 per 100,000. The incidence ofCrohn’s disease is about 7 per 100,000.
B. Incorrect. Crohn’s disease can affect any part of the gastrointestinal tract, from the mouth to theanus. About 75% of Crohn’s patients will have disease of the small intestine, without or with con-comitant disease elsewhere. Of all patients with small intestinal Crohn’s, 90% have involvement ofthe terminal ileum. Ulcerative colitis affects the colon. The terminal ileum can be secondarily affect-ed, backwash ileitis.
C. Incorrect. Crohn’s disease is associated with transmural inflammation of the bowel wall. At histol-ogy, noncaseating granulomas can be found throughout all layers, from the mucosa to the serosa.Granulomas, lymphoid aggregates, inflammatory changes and fissures can penetrate through thebowel wall to involve the adjacent mesentery (fibrofatty change) and mesenteric lymph nodes.
D. Correct. Crohn’s disease tends to have a discontinuous distribution. Lengths of involved gut willhave disease free segments or “skip areas”. Crohn’s disease often spares the rectum. This contrastswith ulcerative colitis, in which the rectum is almost always involved. In ulcerative colitis, diseaseextends upstream from the rectum and is continuous, without intervening normal segments.
Diagnostic In-Training Exam 2006 35
Section IX – Gastrointestinal Radiology